")
Back to Journals » International Journal of General Medicine » Volume 15
Assessment of Patient Knowledge Level Towards MRI Safety Before the Scanning in Saudi Arabia
Authors Alahmari DM, Alsahli FM, Alghamdi SA , Alomair OI , Alghamdi A, Alsaadi MJ
Received 22 April 2022
Accepted for publication 18 July 2022
Published 28 July 2022 Volume 2022:15 Pages 6289—6299
DOI https://doi.org/10.2147/IJGM.S368652
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Dhafer M Alahmari,1 Fahad M Alsahli,1 Sami A Alghamdi,2 Othman I Alomair,2 Abdulrahman Alghamdi,3 Mohammed J Alsaadi4
1Department of Medical Imaging, King Saud Medical City, Riyadh, Saudi Arabia; 2Department of Radiological Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia; 3Department of Medical Imaging, Aseer Central Hospital, Abha, Saudi Arabia; 4Department of Radiology and Medical Imaging, College of Applied Medical Sciences, Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia
Correspondence: Mohammed J Alsaadi, Department of Radiology and Medical Imaging, College of Applied Medical Sciences, Prince Sattam bin Abdulaziz University, 145, PO Box 422, Al-Kharj, 11942, Saudi Arabia, Tel +00966541001006, Email [email protected]
Purpose: Magnetic resonance imaging (MRI) is an important diagnostic method in modern clinical medicine. Patients’ knowledge about MRI is of utmost importance for optimizing the workflow, safety, and patient comfort and saving valuable time for the MRI department. This study investigates patient knowledge levels regarding MRI safety before an MRI examination.
Patients and Methods: A cross-sectional survey was completed by 200 patients who required MRI. Recruitment occurred over eight weeks in governmental and private hospitals in Saudi Arabia; both hospitals and participants were selected randomly. The questionnaire was given to the patients prior to their MRI scans. Descriptive statistics and chi-square tests were performed to identify relationships between knowledge of MRI safety and selected demographic groupings (age, gender, education level, income level). It also evaluates their source of information and assesses the patient’s previous experience regarding MRI scans.
Results: The study sample consisted of 200 patients from 230 surveys distributed in Saudi Arabia, and the response rate was ∼ 87%. Depending on the P-values of the chi-square statistical test to find the relationship between socio-demographic factors and patient’ knowledge level, the results showed a significant association (p-value=0.006) between age and gender and the level of knowledge relating to MRI safety issues. A similar significance (p-value=0.042) is observed between the knowledge level of patients and their educational level and annual income. In addition, a highly significant association (p-value< 0.001) is found between education level or previous experience and whether people seek information about MRI safety.
Conclusion: The study findings suggest that a complex combination of factors affects patient knowledge regarding MRI safety before an MRI examination. Hence, the hospital and radiological department must provide the patient with accurate information about MRI.
Keywords: safety, knowledge, assessment, MRI, environment
Introduction
Magnetic resonance imaging (MRI) has been widely used in many areas of clinical medicine.1 Maintaining a safe MRI environment is a daily challenge for MRI healthcare providers. This was noted due to the growing number of clinical MRI applications. In addition, the increasing magnetic field strengths that are utilized in examinations. Moreover, an expanding variety of biomedical implants and in vivo devices are in use. Consequently, patient knowledge regarding MRI examinations, procedures, equipment, and safety is more important than ever. Indeed, it has become an essential part of the practice of all healthcare providers.2
Patient knowledge is information that influences a patient behaviour and produces changes in knowledge, attitudes, and skills that contribute to maintaining and improving the patient’s health.3 Generally, the purpose of providing information to patients is to inform and prepare them, which may, in turn, reduce patient anxiety, encourage comfort and conformity, and expedite the delivery of healthcare services. All efforts aim to equip patients with necessary and desired information that is crucial to promote awareness and assist them in dealing with their disease and its prognosis.2 Prior to an MRI, patients are encouraged to learn as much as possible about the examination and how to protect themselves from all risks associated with MRI examinations.4 The patient’s knowledge and understanding of what to expect during MRI scanning would improve patient preparation. Advanced MRI safety knowledge will reduce the anxiety-related MRI diagnostic performance.5 Information on MRI, safety concerns and associated risks are critical elements for a patient’s acceptance to undergo MRI investigations and helps provide a good understanding of how these procedures are performed and their consequences.4 Several factors would lead to cancelling an MRI exam, such as loud noise exposure, limited space inside the pore, and length of scanning time. Furthermore, image artifacts will occur more when the patient moves during the scan.4–6 Thus, patient knowledge is a vital determinant of the quality of care and among the most significant factors for improving the effectiveness and efficiency of care.6
No previously published studies have investigated patient knowledge regarding MRI safety before an MRI examination. However, research in health practice has examined patient knowledge of treatment and health procedures. For example, Abbate et al4 have reported that patients may have a lower chance of infection if they understand the risks that can increase the potential of contracting an infection. In addition, knowledgeable patients are more confident and willing to question healthcare workers who do not use gloves or face masks during treatment.7 Meanwhile, Yacel et al have investigated patient knowledge of breast cancer and its diagnosis process.8 The authors concluded that women have insufficient knowledge of mammography; for instance, most participants were aware that x-rays are employed in mammography, but few knew that x-rays could be dangerous for their breasts. Furthermore, the study identified patient perceptions of the pain, discomfort, and effects of radiation due to a mammogram as barriers that lead to non-compliance.8
The challenge of maintaining a safe MRI environment for patients has continued because of the absence of MRI safety information. Patient knowledge of the issues around MRI safety is imperative to overcoming this challenge. Therefore, this study measures the patient knowledge concerning MRI safety before an MRI scan in Saudi Arabia.
Materials and Methods
This research entailed a cross-sectional electronic self-reported survey. The participants provided written consent before starting the survey, and this study was conducted in accordance with the declaration of Helsinki. The studies involving human participants were reviewed and approved by the Ethics Committee at King Saud Medical City (ref no. H1RI-13-Jan21-03). An information sheet was given to all participants with their MRI appointment. Before the MRI scan, the participants were asked whether agreed to participate in the study. Those who agreed were asked to sign the consent form. Hence, signed informed consent was obtained from all participants. Participants were asked to complete a questionnaire that gathered information about their knowledge of MRI safety before undergoing an MRI examination. Therefore, this study measures patient knowledge of MRI procedures and the associated risks and benefits as well as how each patient’s level of education, sources of information, and previous MRI experience impact their knowledge of MRI safety and the procedure. Participants were recruited from MRI departments at different governmental and private hospitals in the Kingdom of Saudi Arabia. The survey instrument was administered over eight weeks (January–February 2021). The respondents completed a hard-copy questionnaire on only one occasion.
Recruitment Method
The target population consisted of male and female adults of at least 18 years of age in the community who required an MRI. People who were unconscious or unable to complete the questionnaire without supervision were excluded. Patients were able to complete the questionnaire in either English or Arabic as some Saudi citizens speak only Arabic, and the other citizen speak English language. Simple random sampling was applied to ensure an equal probability of selection for everyone. The questionnaires were distributed to patients who were attending for MRI scans at the general medical imaging departments of 13 hospitals (seven governmental hospitals and six private hospitals) in various cities in the Kingdom of Saudi Arabia.
Survey Design
The questionnaire was designed specifically to measure patient knowledge and understanding of the safety issues associated with an MRI procedure. Participants were asked to complete a questionnaire to gather information about a patient’s knowledge of MRI safety before undergoing an MRI examination. This study measures the patient’s knowledge of the MRI procedure and associated risks and benefits. Besides, the patient’s level of education, sources of information, and previous experiences of undergoing an MRI procedure would impact their knowledge of MRI safety and the procedure. Part A targeted demographic variables (age, gender, education level, and socio-economic status), while Part B assessed patient knowledge of MRI safety and their perceptions regarding items that are not safe inside the MRI examination room. For instance, 21 metallic items that are prohibited inside the MRI room were listed in the section B questions such as watch, rings, coins, pacemaker and mobile. Part C quantified the sources of information that patients sought and preferred, and Part D determined patients’ previous experiences of undergoing an MRI procedure. All patients utilized the Arabic and English version of the survey. Prior to the data analysis, the completed surveys were checked for any invalid entries (incomplete responses, repeated answers across items, and dummy entries).
Pilot Study
Before starting the project, a pilot study was conducted with 12 people in different public areas in Saudi Arabia to assess the content validity of the survey and estimate the amount of time that participants would need to complete all the items. All ambiguities and areas in need of clarification were addressed so that future participants could complete the questionnaire with relative ease.
Data Analysis
Descriptive statistics, including frequencies and percentages, were calculated. Normality was tested with histograms. Inferential statistics such as chi-squared tests were used to compare subject groups, and p-values of less than 0.05 were considered significant. General linear models were fitted to the data to demonstrate the variance in responses in different subject groups. All statistical analyses were performed with SPSS version 26.0 (IBM, Chicago, Illinois, USA).
Results
A total of 230 questionnaires were distributed, and 200 were returned, which represents a response rate of ~ 87%. Table 1 presents the demographic data of the participants.
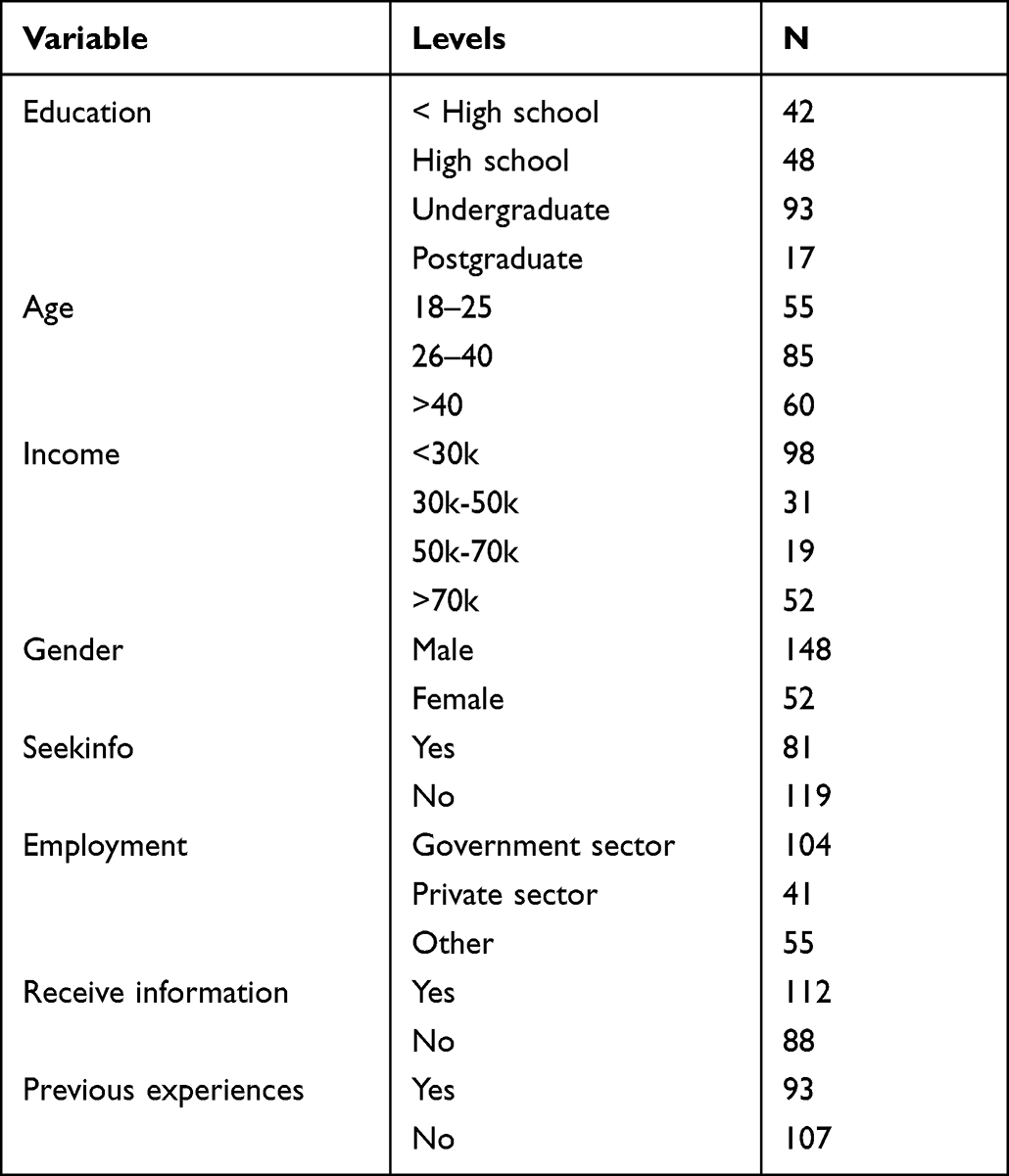 |
Table 1 Demographic Data of the Participants |
Knowledge
The surveys yielded data on two types of knowledge. The first relates to MRI safety (11 questions), and the second concerns items that are safe to take into an MRI examination (21 questions). For each set of questions, the response of each participant was taken as the total number of correct answers. All explanatory variables were categorized, and two-way interactions were fitted. The results are discussed below.
- MRI safety issues: Significant two-way interactions were observed between age and gender (p-value=0.006), age and income (p-value=0.021), education and income (p-value=0.042), and gender and patient information-seeking (SeekInfo; p-value=0.042). The interaction plots were obtained for several interesting patterns.
- Age and gender: Male participants over the age of 40 had the lowest mean number of correct responses, while female participants over 40 years of age had the highest mean number of correct responses. There was a significant difference between the other two age groups (Figure 1).
- Age and income: In the over-40 age group, the highest mean number of correct responses was achieved by the 50k–70k (k=1000; 1 Saudi Riyal=$0.32AUD/0.16GBP) income group followed by the above-70k income group. In the 26–40 age group, the 50k–70k income group had the highest mean number of correct responses, while the above-70k and below-30k income groups had the lowest means (Figure 2).
- Education and income: The 50k–70k group of postgraduates had a significantly higher mean number of correct responses. Once again, there was very little difference between the other age groups at all education levels (Figure 3).
- Gender and SeekInfo: Female participants had the same average number of correct responses regardless of whether they sought information about the MRI. In contrast, males who sought information had a substantially higher mean number of correct responses compared to males who did not seek information (Figure 4).
- Items safe in an MRI: The only significant interactions occurred between age and education (p-value=0.012), age and income (p-value=0.031), and education and income (p-value=0.040). The patterns of the interaction plots are discussed below. Notably, no postgraduates below the age of 26 were included in the study. Furthermore, the main effect of SeekInfo was significant (p-value=0.005), with those who sought information registering a slightly higher mean. Interestingly, participants in the 18–25 age group who had not completed high school did not seek information about the MRI. The interaction plots of the linear model for items safe in the MRI were obtained.
- Age and education: Postgraduates above the age of 40 had the highest mean number of correct responses. Of those who had finished high school, the 18–25 age group had the lowest mean (Figure 5).
- Age and income: The highest means were recorded for the two middle income groups in the 26–40 age group. The mean declined from the 26–40 age group to the above-40 age group for the three lower income levels, with the sharpest decrease for the 30k–50k income group. In contrast, the mean for the above-70k income group increased across the age range, with the highest mean for the above-40 age group (Figure 6).
- Education and income: The middle-income groups exhibited similar behaviour, with higher means at the extreme education levels. The highest means were obtained for the middle-income groups with postgraduate qualifications. In comparison, the other two income groups had almost steady means across age groups (Figure 7).
 |
Figure 1 Interaction plots for the linear model for MRI safety between gender and age. |
 |
Figure 2 Interaction plots for the linear model for MRI safety between age and income. |
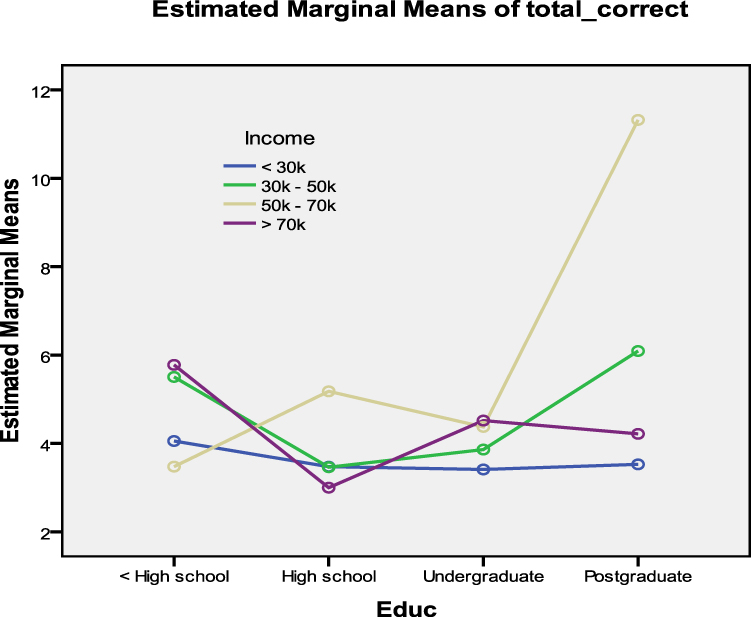 |
Figure 3 Interaction plots for the linear model for MRI safety between education and income. |
 |
Figure 4 Interaction plots for the linear model for MRI safety between gender and Seekinfo. |
 |
Figure 5 Interaction plots of the linear model for items safe in an MRI between age and education. |
 |
Figure 6 Interaction plots of the linear model for items safe in an MRI between age and income. |
 |
Figure 7 Interaction plots of the linear model for items safe in an MRI between education and income. |
Information and Education
A chi-squared test was conducted to examine the association between the participants’ education level and whether they sought information about MRI safety. The results support a positive association (p-value<0.001), which indicates that people with higher education levels are more likely to seek information about MRI safety compared to those with lower education levels. More than half (56.2%) of the patients reported that they had previously received information about MRI safety. Figure 8 showed the association between the education level and incidence of seeking information with regards of MRI safety.
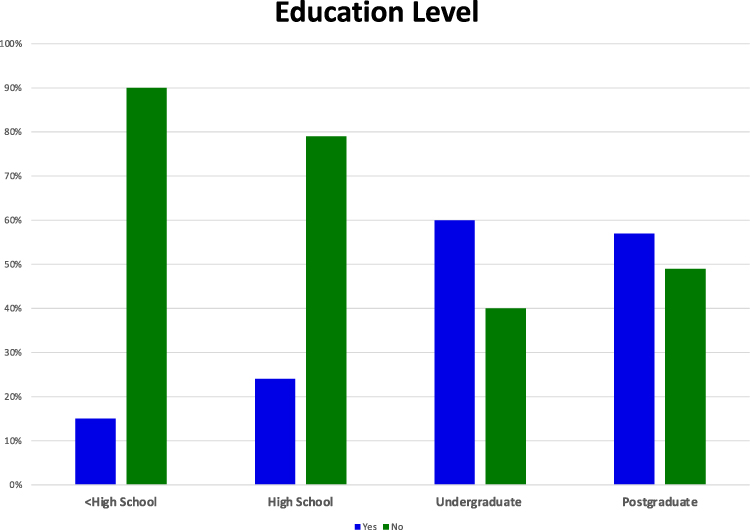 |
Figure 8 Association between education levels and incidence of seeking information about MRI safety. |
Previous MRI Experience and Information
The analysis also assessed the association between previous MRI experience and the decision of whether to seek information about MRI safety. The chi-squared test results reveal a highly significant association (p-value<0.001). Of the participants who sought information regarding MRI safety, 63% reported previous experience, whereas 35% of the patients who had not sought information identified no previous MRI experience.
Discussion
The present study aims to identify the levels of patient knowledge regarding MRI safety before an MRI scan. Depend on the knowledge assessment section consists of eleven questions related to MRI scan information, Table 2. This study suggests that patients do not have sufficient knowledge of the diagnostic procedures they will undergo. This conclusion is consistent with that of Yacel et al, who have investigated patient knowledge concerning breast cancer and its diagnosis and prevention.8
 |
Table 2 Examples of the Questions Towards Patient Knowledge of MRI Safety and Patient Perceptions of Items That are Safe in MRI Examinations |
Demographic and Socio-Economic Variables
Key demographic factors were utilized to determine the differences in patient knowledge levels regarding MRI safety prior to undergoing an MRI. The results reflect a significant association between age and gender (p-value=0.006) and the level of knowledge about the procedure and safety. Older male participants (>40 years) tended to be less knowledgeable than their younger counterparts. In addition, females under the age of 40 were lacking in knowledge of MRI safety issues. Kamel et al, have similarly observed a linear association between age and sex and the level of patient knowledge of how to control diabetes.9
The current study also identifies a highly significant association between the knowledge level of patients and their education level and annual income (p-value=0.042). Highly educated patients (postgraduates) who earned more than 70k and patients over the age of 40 who earned between 50k and 70k displayed substantially more knowledge of MRI safety. In contrast, several studies have identified perceptions that patients of a low socioeconomic status are less informed, in worse health, and have poorer prognoses compared to patients of high socioeconomic status.10 Lane et al have reported that patient comprehension of the nature and consequences of an MRI examination is essential to optimize the outcome of their medical investigation.11 Therefore, the level of the knowledge regarding MRI safety is influenced by demographic factors, such as age, gender, education level, and socio-economic factors (eg annual income).
The responses concerning items that are safe in an MRI examination indicate more knowledge of this topic among postgraduate patients between 26 and 40 years of age who earned between 50k and 70k and among participants below a high school level of education who earned between 50k and 70k. These results are affirmed by the majority of experts who agree that patients with a higher education level and higher annual income are more likely to be capable of effectively managing their own care.11–13 A possible explanation for this trend is that a higher education level and higher socioeconomic status afford individuals greater access to useful sources of information (eg internet, books, and brochures) to learn which items are safe in an MRI examination.
Sources of Information and Previous MRI Experience
Actively seeking information about health investigations is central to improving one’s health and is a vital tenet in promoting the health of patients.14 The results of the present study reveal that participants above the age of 25 who sought information demonstrated significantly more knowledge of MRI safety issues. Both this study and the research by Smart and Burling evidence that highly educated patients are more strongly disposed to seek information about their health, diagnosis, and treatment from multiple sources.14 Being informed can in turn increase the choices and options available to them. Interestingly, gender also influences the extent to which patients pursued information. Males were consistently less likely to seek information and thus had poorer overall knowledge of MRI safety compared to women. This disparity may be explained by social norms, culture, and behavioural paradigms.15
Despite the expectation that previous experience would grant patients sufficient information about the MRI process and safety issues, this assumption is incorrect. Previous experience with MRI led to two possible scenarios. The first is that the experience made the patient more inquisitive and therefore more likely to seek further information to supplement their prior experience. In the second scenario, the level of information that the patient received both before and during the MRI examination was insufficient, so the patient felt the need to supplement their knowledge and alleviate their concerns.
Previous research has identified an influence of higher education on the level of knowledge of MRI safety.12 However, the present results imply that this influence is enhanced by not only opportunity but also an increased willingness of highly educated patients to seek further information.
Limitation and Recommendations
A limitation of this study is that it was conducted in only one country (Saudi Arabia). Thus, there is a need for further adaptations of this research to other locations to ensure that societal and cultural factors are not biasing the results.
It is evident that the provision of information to patients is essential for effective care in any health setting. This research has observed considerable variation between groups in terms of which sources of information were used and the degree to which the information was sought. Providing adequate information is an ongoing challenge for all healthcare providers; however, given the complex combination of factors in this study, it may be beneficial to profile patients before an MRI. This process can assist in identifying groups for correlation to the style and format of the resources they prefer. Each department and referring physician should provide patients with access to multiple resources (eg websites, printed material, face-to-face information sessions) that match their profile. In this way, patients could be equipped with the most suitable sources of information well in advance of the procedure, which would allow them to more fully understand the potential issues of which they must be aware.
Conclusion
The present study reveals that the combination of factors contributing to patient knowledge of MRI safety in the Saudi population is complex. In particular, the combination of education, age group, income, gender, and whether the information was sought prior to an MRI examination determines the level of patient knowledge. By profiling patients concerning these factors and delivering information in various formats, healthcare providers can more effectively target patients who should receive information before the examination and increase their readiness to cooperate with an MRI examination. While the target population of this study was the Kingdom of Saudi Arabia, the results may have broader implications.
Acknowledgments
The research team would like to express their gratitude to all individuals who have encouraged and assisted with this research. In addition, we would like to thank all those who supported and participated in the data collection from the MRI departments in Saudi Arabia as well as Dr. Nazeem, who assisted with the statistical analysis process.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Duru FLR, Scheidegger MB, Lüscher TF, Boesiger P, Candinas R. Pacing in magnetic resonance imaging environment: clinical and technical considerations on compatibility. Eur Heart J. 2001;22(2):113–124. doi:10.1053/euhj.2000.2149
2. De Wilde JP, Grainger D, Price DL, Renaud C. Magnetic resonance imaging safety issues including an analysis of recorded incidents within the UK. Prog Nucl Magn Reson Spectrosc. 2007;51(1):37–48. doi:10.1016/j.pnmrs.2007.01.003
3. Briggs J. Knowledge Retention from Pre-operative Patient Information. Best Practice. 2000;4(6):1–6.
4. Bolejko A, Sarvik C, Hagell P, Brinck A. Meeting patient information needs before magnetic resonance imaging: development and evaluation of an information booklet. J Radiol Nurs. 2008;27(3):96–102. doi:10.1016/j.jradnu.2008.05.001
5. Ajam AA, Tahir S, Makary MS, et al. Communication and team interactions to improve patient experiences, quality of care, and throughput in MRI. Top Magn Reson Imaging. 2020;29(3):131–134. doi:10.1097/RMR.0000000000000242
6. Laidlaw SH. Patients with multiple sclerosis: their experiences and perceptions of the MRI investigation. J Diagnostic Radiography Imaging. 2003;5(1):19–25. doi:10.1017/S146047280300004X
7. Abbate R, Di Giuseppe G, Marinelli P, Angelillo IF. Patients’ knowledge, attitudes, and behavior toward hospital-associated infections in Italy. Am J Infect Control. 2008;36(1):39–47. doi:10.1016/j.ajic.2007.01.006
8. Yacel ABD, Acar M, Elludokuz H, Albayrak R, Haktanir A. Knowledge About Breast Cancer and Mammography in Breast Cancer Screening Among Women Awaiting Mammography. Turk J Med Sci. 2005;35(42):35–42.
9. Kanal EBA, Bell C, Borgstede JP, et al. ACR Guidance Document for Safe MR Practices: 2007. Am j Roentgenol. 2007;188(6):1447–1474. doi:10.2214/AJR.06.1616
10. Kamel NMBY, el-Zeiny NA, Merdan IA. Sociodemographic determinants of management behaviour of diabetic patients Part II. Diabetics’ knowledge of the disease and their management behaviour. Eastern Mediterranean Health Journal. 1999;5(5):974–983. doi:10.26719/1999.5.5.974
11. Woo JKH, Ghorayeb SH, Lee CK, Sangha H, Richter S. Effect of patient socioeconomic status on perceptions of first- and second-year medical students. CMAJ. 2004;170(13):1915–1919. doi:10.1503/cmaj.1031474
12. Lane DA, Ponsford J, Shelley A, Sirpal A, Lip GYH. Patient knowledge and perceptions of atrial fibrillation and anticoagulant therapy: effects of an educational intervention programme: the West Birmingham Atrial Fibrillation Project. Int J Cardiol. 2006;110(3):354–358. doi:10.1016/j.ijcard.2005.07.031
13. Berg S. The well-informed patient: a new breed of health care consumer: the advantages (and pitfalls) of seeking health information. Asthma Magazine. 2005;10(4):28–30.
14. Smart JM, Burling D. Radiology, and the Internet: a Systematic Review of Patient Information Resources. Clin Radiol. 2001;56(11):867–870. doi:10.1053/crad.2001.0738
15. Alelyani M, Gameraddin M, Alasmari A, Alshahrani F, Alqahtani N, Musa A. Patients’ perceptions and attitude towards MRI safety in Asir Region, Saudi Arabia. Patient Prefer Adherence. 2021;15:1075–1081. doi:10.2147/PPA.S309186
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.