Back to Journals » Risk Management and Healthcare Policy » Volume 15
Assessment of Nurses’ Knowledge and Confidence Regarding Tracheostomy Care in a Pediatric Long Term Care Hospital in Saudi Arabia
Authors Mosalli R, Aboumoustafa GA, Khayyat W, Bokhari AN, Almatrafi MA, Ghazi M, Paes B
Received 14 May 2022
Accepted for publication 13 September 2022
Published 22 September 2022 Volume 2022:15 Pages 1809—1821
DOI https://doi.org/10.2147/RMHP.S374730
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Haiyan Qu
Rafat Mosalli,1,2 Gamal A Aboumoustafa,1 Wed Khayyat,3 Aziza N Bokhari,3 Mohammed A Almatrafi,2 Mohammed Ghazi,1,4 Bosco Paes5
1Department of Pediatrics, International Extended Care Center, Jeddah, Saudi Arabia; 2Department of Pediatrics, Umm Al-Qura University, Makkah, Saudi Arabia; 3Medical College, Umm Al-Qura University, Makkah, Saudi Arabia; 4Department of Pediatrics, Division of Critical Care, King Abdulaziz University, Jeddah, Saudi Arabia; 5Department of Pediatrics (Neonatal Division), McMaster University, Hamilton, Ontario, Canada
Correspondence: Rafat Mosalli, Department of Pediatrics, Umm Al-Qura University, P.O. Box 7607, Makkah, Saudi Arabia, Tel +966 561182222, Fax +966 252-70000 Ext 4110, Email [email protected]
Background: The incidence of tracheostomy insertion in pediatric patients has increased over the last few decades. Tracheostomized pediatric patients need daily, meticulous care by qualified nurses to minimize severe, avoidable complications. Adequately trained nurses facilitate patients’ stability, accelerate weaning from the ventilator, and reduce potential tracheostomy dislodgement.
Methods: A cross-sectional, retrospective cohort survey was conducted in September 2021, using an electronic version of a self-questionnaire, to assess nurses’ knowledge and comfort level regarding tracheostomy care of pediatric patients at the International Extended Care Center in Jeddah, Saudi Arabia. Statistical analysis of the accrued data was performed using the SPSS 21.0 software package and a P-value < 0.05 calculated by t-Test, was considered significant.
Results: Among 43 nurses included in the study, 14 (32.6%) were very comfortable taking care of tracheostomized patients, 13 (30.2%) were comfortable, and 16 (37.2%) were uncomfortable. Regarding knowledge, three main aspects of tracheostomy care were correctly answered (%) by all the nurses: knowledge of routine tracheal care (55%), tracheal care skills (11.6%), and tracheal emergency care (2.3%). The study showed a significant positive correlation between nurses’ comfort level with tracheal care and academic degree, duration of pediatric experience, completion of more than one life support course, and attendance at the annual local tracheostomy care competency learning program (TCCLP; all P < 0.05).
Conclusion: Deficits exist in nurses’ knowledge of tracheostomy care. Improved knowledge garnered through repetitive participation in tracheostomy competency programs and life support courses correlate with greater comfort and more than 5 years of pediatric experience. Nurses’ deficits in emergency care knowledge and skills should be addressed through a structured educational program and a simulation, hands-on based TCCLP course, irrespective of comfort level with tracheostomy care.
Keywords: pediatric nurses, tracheostomy, training skills, children, extended care, Jeddah
Introduction
A tracheostomy is a well-established and frequently used procedure across all age groups to overcome upper airway obstruction, facilitate mechanical ventilatory support, and/or removal of tracheobronchial secretions.1
The incidence of tracheostomy has increased over the last few decades. The procedure is mostly performed on pediatric intensive care patients who are dependent on chronic ventilatory support, prior to transfer to extended care facilities with a long-term acute care service or admission to a non-critical area such as a step-down unit. The management of a tracheostomy is a complex activity with several potential complications if the nurse lacks the essential knowledge and skills to provide appropriate care.2,3
A systematic review conducted in 2020, reported that the most common complications of the surgical operation were cutaneous lesions and granulomas at the tracheostomy site.4 Mortality related to the procedure was as high as 6% in children and was mainly associated with cannula obstruction or accidental decannulation.4 The largest prospective series of tracheostomy patients demonstrated a four-fold higher mortality in pediatric patients with hemorrhage versus those without hemorrhage (P<0.001).5 Higher mortality rates were also evident in neonates, children aged 1–5 months, and those aged greater than 10 years compared to children 1–3 years of age.5 Post-operative complications such as tube occlusion, infection of the stoma site, aspiration, hemorrhage, or excessive granulation of the trachea may occur. Compromised breathing following the removal of a tracheostomy is described as a late complication.6
At the International Extended Care Center (IECC), about 75% of the admitted pediatric patients are tracheostomized and ventilator dependent and require continuous monitoring and rigorous multidisciplinary care. Nurses are considered front-line health-care providers hence, proper knowledge of tracheostomy care and skills are critical to ensure patients’ stability and safety. Expert, well-coordinated care reduces the incidence of unwanted complications such as laryngeal injuries and mechanical obstruction, accelerates weaning from the ventilator, and concurrently reduces the potential risk of malpractice litigation.7,8
The main objective of this study is to assess nurses’ knowledge and comfort level with tracheostomy care of pediatric patients at the IECC in Jeddah, Saudi Arabia.
Materials and Methods
Study Design
We conducted a cross-sectional, retrospective cohort survey in September 2021 at the IECC. The IECC is one of the largest centers in the entire western province of Saudi Arabia, with more than a 150-bed capacity, accommodating both adult and pediatric patients. The center provides an optimal level of long-term and acute care services and care for chronic ventilated patients. The study was designed to evaluate the knowledge, skills, and emergency response in tracheostomy care using a questionnaire with key items extrapolated from the published literature.9–11 Participants provided informed consent to join the study, and data collection for analysis was accrued after full agreement by the participants. The project was approved by the IECC Institutional Review Board (IECC IRB) Jeddah, Saudi Arabia.
Population
The questionnaire was distributed to all the 43-nursing staff at the IECC involved in the long-term care of tracheostomized pediatric patients. Medical records of the recruited subjects were reviewed, and pertinent demographic characteristics were assembled.
Assessment Tool
A two-part questionnaire was utilized for the study. The first section included demographic data of both the patients and nurses. The second section comprised 3 main domains: First, a composite of 20 true and false questions assessing tracheal care knowledge;9 second, ten multiple-choice questions to assess tracheal care skills;10,11 last, two scenarios assessed background knowledge in emergency tracheostomy care. A written response to three additional open-ended questions following the two case scenarios, sought general knowledge about the contents of the tracheostomy kit, indications for suctioning the tracheostomy and the meaning of the mnemonic HME (heat, moisture, exchanger) and its function. Each of the correct responses to ten multiple choice questions on tracheal skills was awarded a score of 2 points with a total score of 20. Similarly, each affirmative and correct response to the questions in the case scenarios was allotted a score of 2 points for a total score of 20. The questionnaire was reviewed for content validity by four expert intensivists other than the authors of the study. Finally, we asked the nurses about their comfort level working with tracheostomized pediatric patients who required ventilator assistance.10
Statistical Analysis
We conducted a descriptive analysis of the assembled data; Frequencies are reported for categorical data. Mean, and median indicate measures of central tendency. Responses were designed to measure confidence and comfort in the management of a tracheostomy during routine care and emergency situations. A four-point Likert scale (from 1- very comfortable, 2 - comfortable, 3 - uncomfortable, 4 - completely uncomfortable) was used for the question that assessed the subjective comfort level of nurses with tracheostomy care.12 Data analysis was performed using the SPSS 21.0 software package, and a P -value ≤ 0.05, calculated by t-test, was considered significant.
Results
Demographic Data
Table 1 presents the general characteristics of the surveyed nurses. All 43 pediatric nurses who participated in this study completed the survey (100%); 40 (93%) were female, and 3 (7%) were male. The mean (± standard deviation) age of the respondents was 32.5 years (6.52). Regarding the level of education, the majority, 27 (62.8%), had a bachelor’s degree. Forty-two nurses (97.7%) procured their nursing qualification outside the kingdom of Saudi Arabia, apart from one nurse (2.3%). Regarding experience, there was almost an equal distribution of nurses with less than one year (n=14; 32.6%) and more than 5 years’ experience (n=17; 39.5%). All the nurses had attended a basic life support (BLS) course, more than half had participated in either a pediatric advanced life support (PALS) or combined BLS and PALS courses, while 6 (13.9%) were trained in BLS, PALS, and advanced cardiac life support (ACLS). Skills in all the life support courses were acquired internationally. Nurses are mandated to attend the annual tracheostomy care competency learning program (TCCLP) at the local center. Program attendance ranged from one (n=14, 32.6%) to greater than five times (n=17; 39.5%; Table 1).
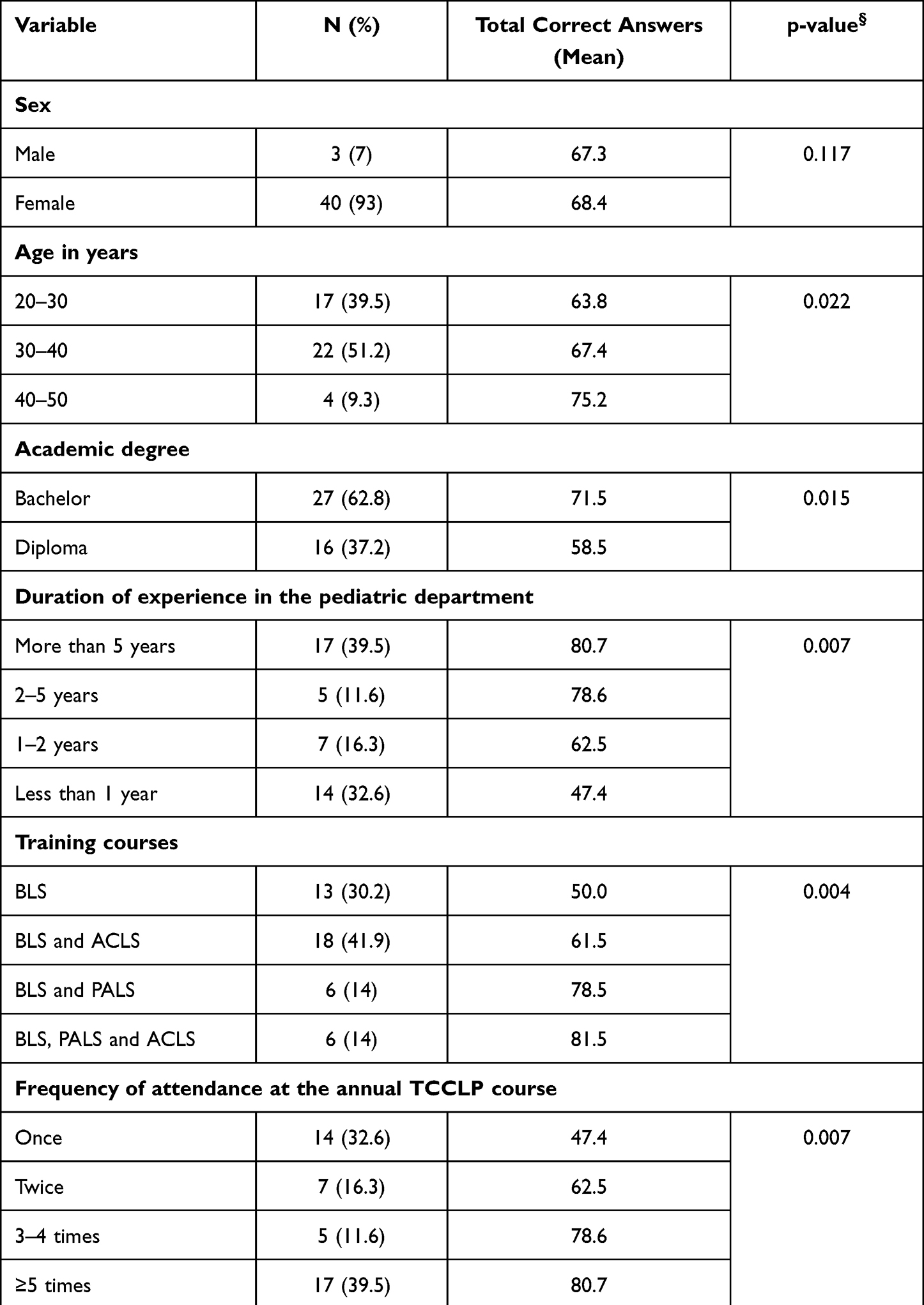 |
Table 1 Demographic Data of the Nurses (n=43) and the Relationship Between the Variables and Total Correct Answers |
The demographic characteristics of the tracheostomized patients are outlined in Table 2. Among the enrolled subjects, the sex distribution was similar. The primary diagnosis in most patients was neurologic (n=35; 76%) and all the patients in this category required prolonged mechanical ventilation. Overall, 89.1% (41/46) of the subjects who required a tracheostomy had acquired their primary illness at birth and the duration of the tracheostomy ranged from less than one year to greater than 5 years.
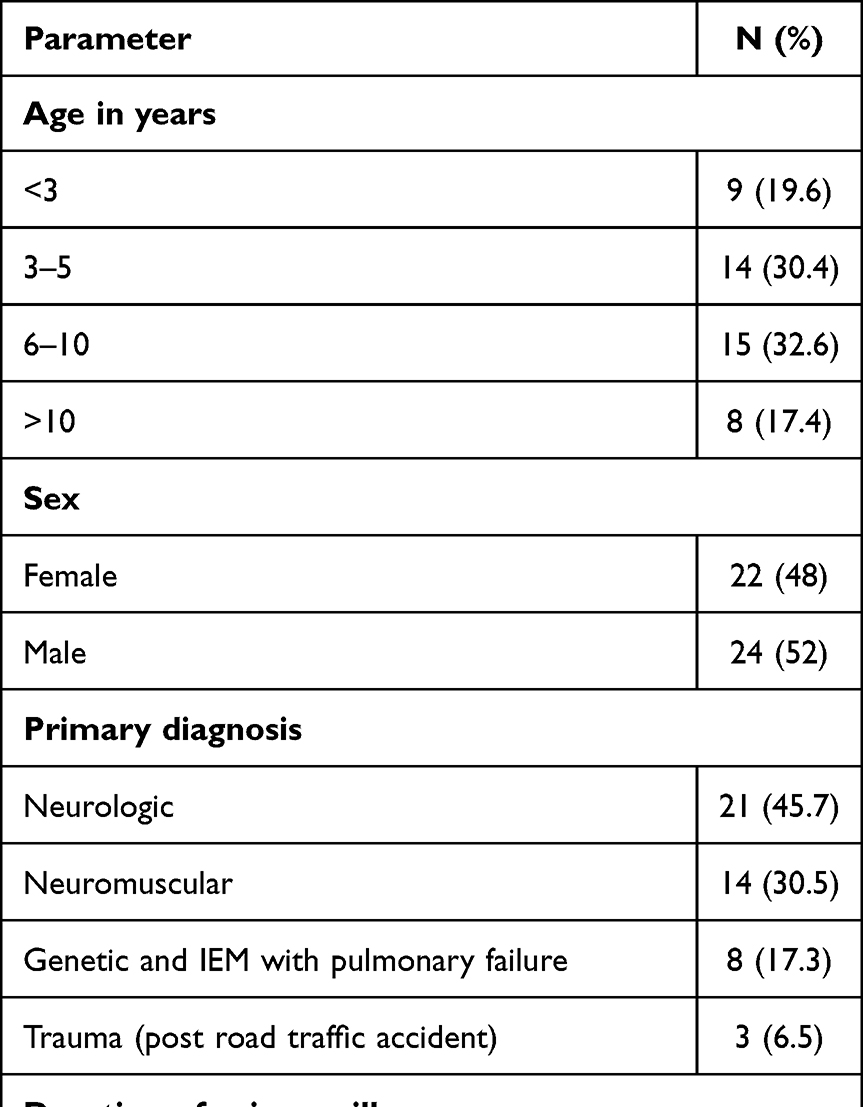 |
Table 2 Demographic Characteristics and Outcome Data for Pediatric Tracheostomized Patients (n=46) |
Knowledge
A true and false section was designed to assess tracheal care knowledge. Eleven of the 20 questions (55%) were answered correctly by all the nurses. Overall, the true and false responses ranged from 27.9% −100% and 39.5% −100% respectively. The other responses of the respondents are summarized and compared in Table 3.
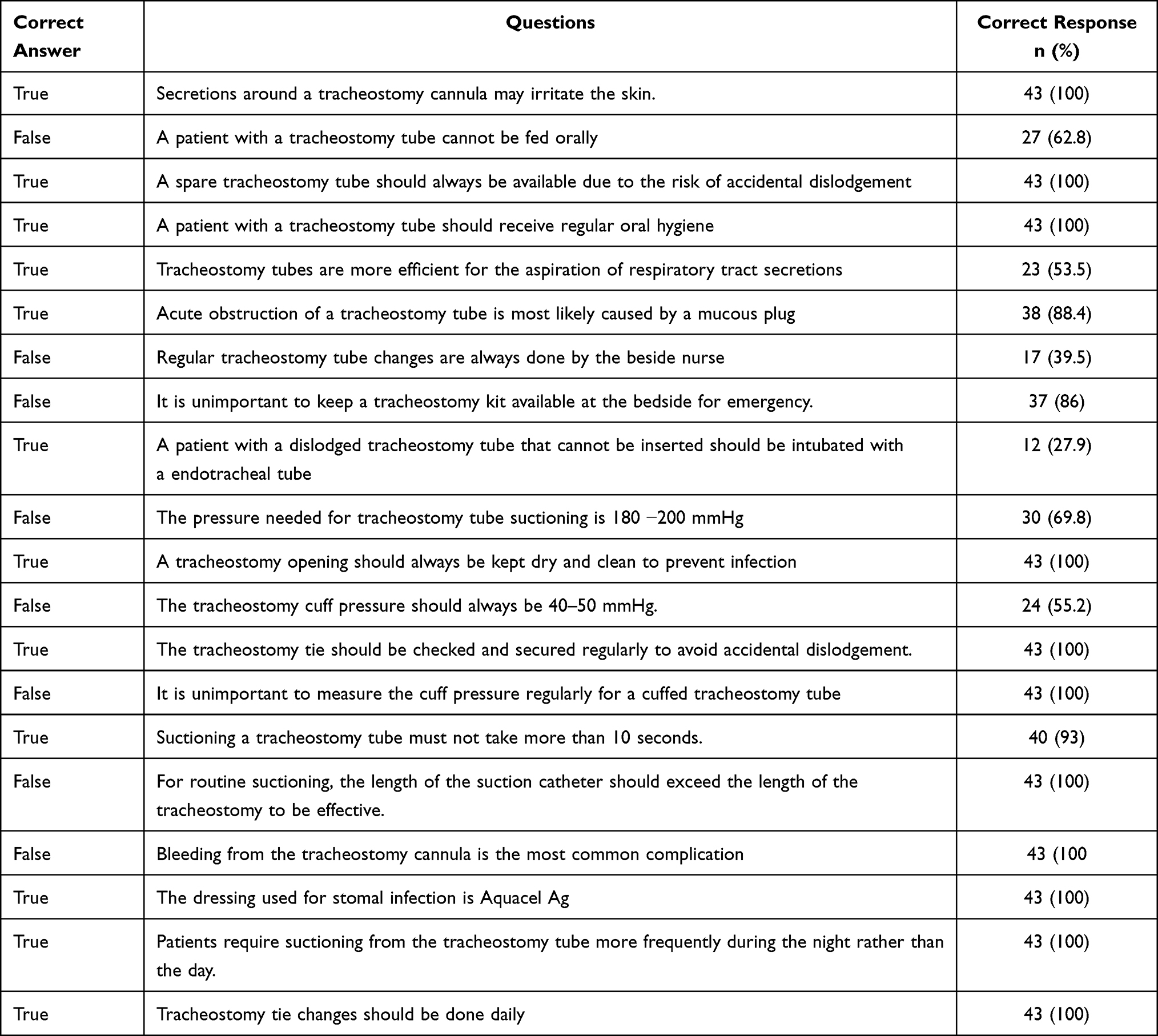 |
Table 3 Tracheal Care Knowledge Among the Study Participants (n=43) |
Skills
Nursing tracheal skills were assessed by multiple choice questions and the findings are depicted in Table 4. Five (11.6%) nurses provided all the correct answers, and the total group scores for majority of the nurses ranged between 14–18 out of 20. Thirty (69.8%) erroneously stated that a tracheostomy is usually performed between the 3rd and 4th tracheal ring. Of note, only eleven nurses (25.6%) did not know all the information that should be included as part of the hand-off of a patient with a tracheostomy tube to another nurse.
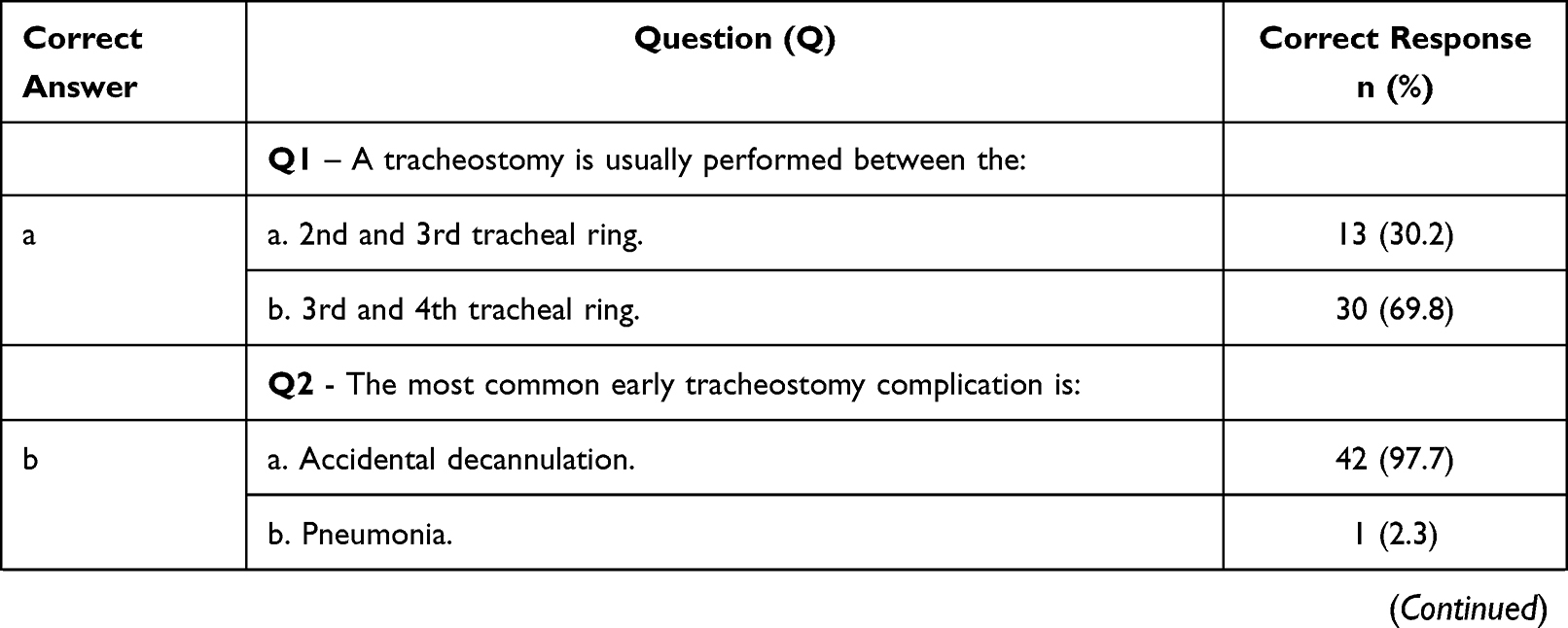 | 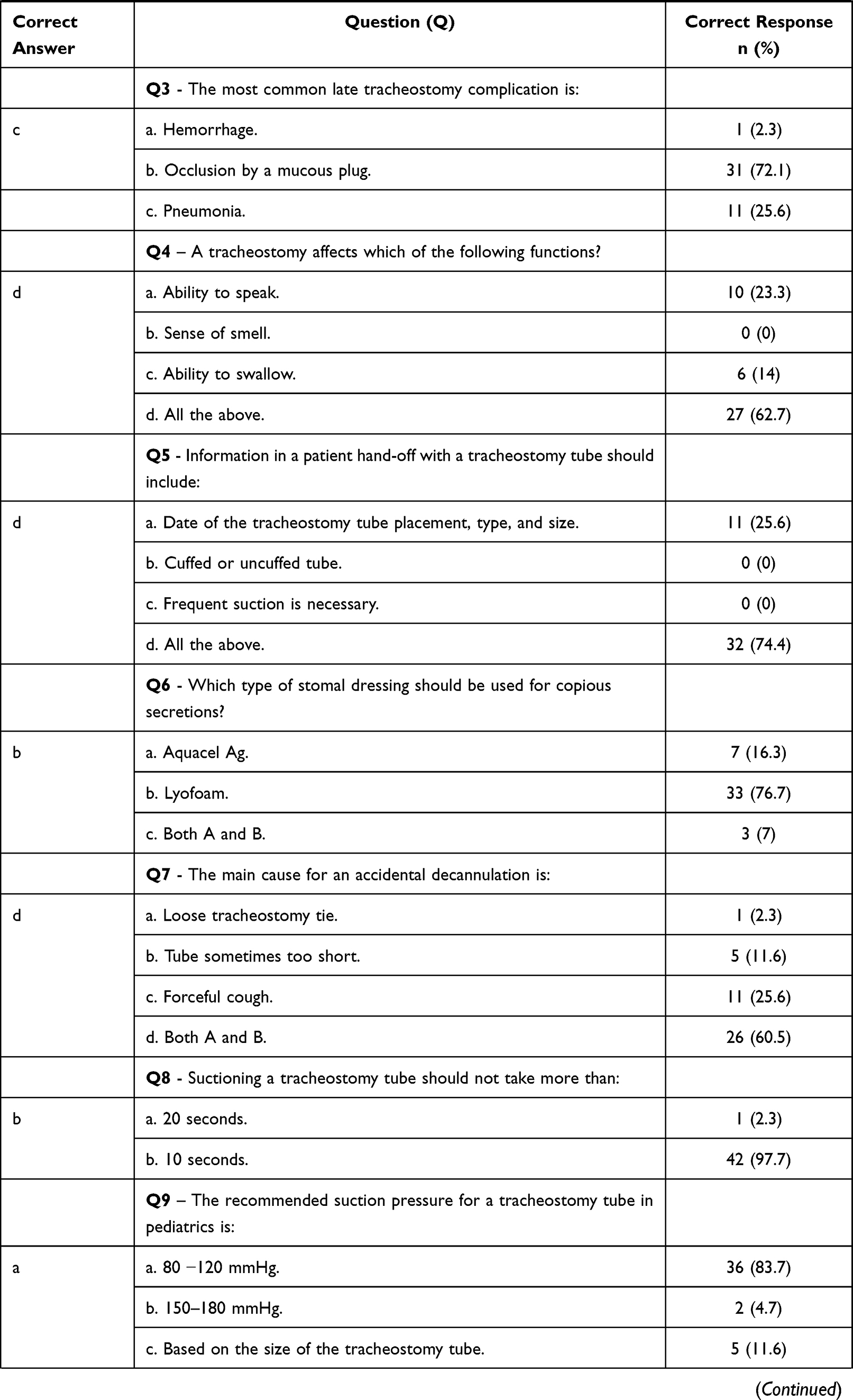 | 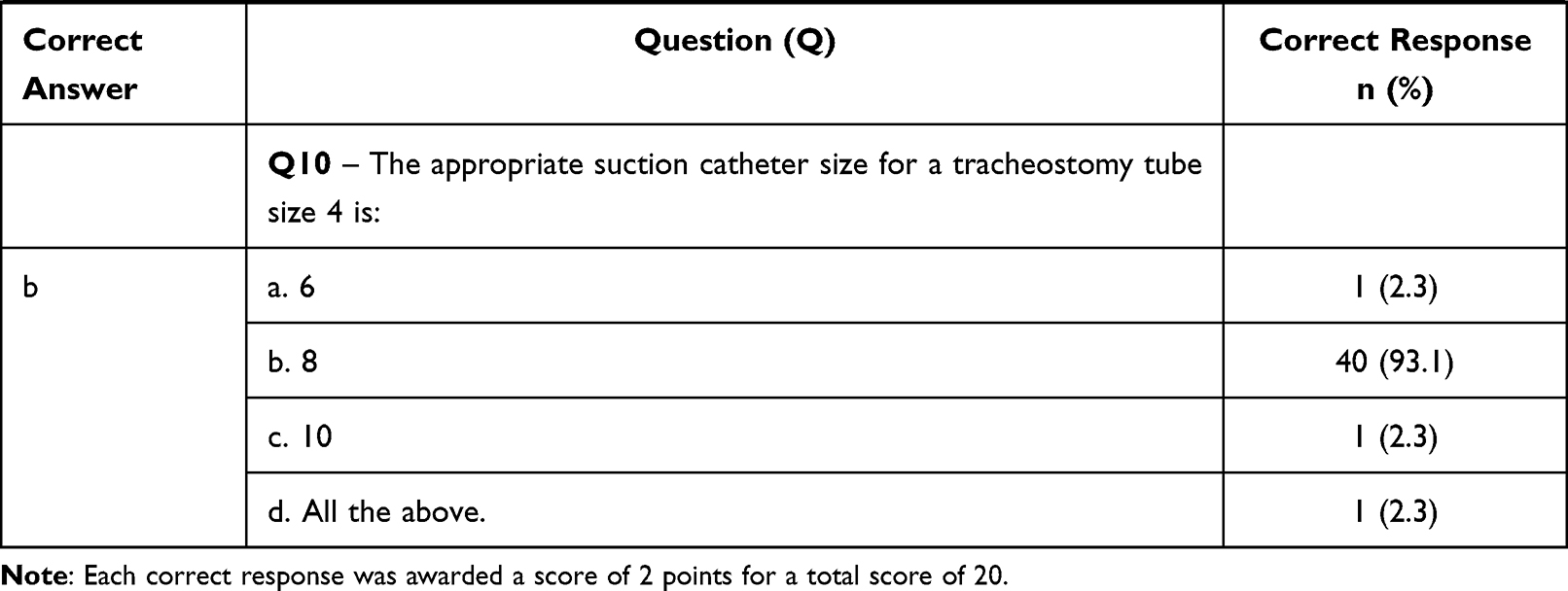 |
Table 4 Tracheal Care Skills of the Study Participants (n=43) |
Background Knowledge in Emergency Tracheostomy Care
Two case scenarios (Table 5) evaluated nurses’ responses in emergency cases. Only one nurse got all the answers correct (2.3%), and the overall scores ranged between 9–20 (median:14). Sixty-five percent of the nurses (n=28) did not know what to do with an introducer or obturator. Although 81% - 94% of the nurses had experienced the respective acute scenarios in their clinical practice, disappointingly only 13 (30%) were comfortable dealing with such emergencies if they arose.
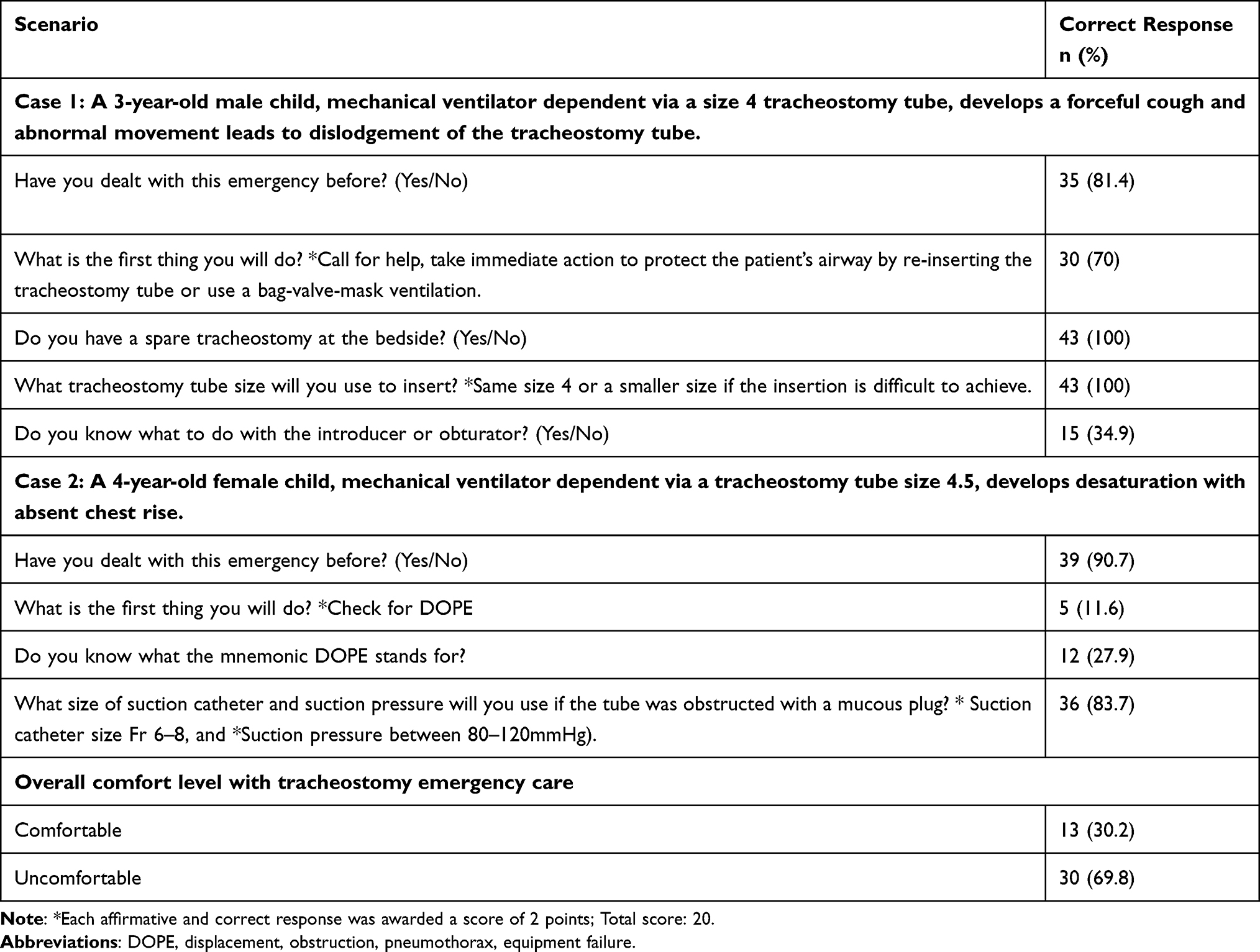 |
Table 5 Scenarios to Assess Knowledge of the Emergency Care of a Tracheostomy (n=43) |
Responses to the Open-Ended Questions
Of the three open-ended questions, none of the nurses were able to identify the entire contents of the tracheostomy kit. Among the indications for tracheostomy suction, 9 nurses (20.9%) would execute the procedure for excessive secretions, 11 (25.6%) for respiratory distress or desaturation and 23 (53.5%) for any combination thereof. Thirty-four nurses (79%) did not understand what HME implied or its function. Moreover only 12 (28%) appreciated the meaning and implications of displacement or obstruction of the endotracheal tube, pneumothorax, and ventilator or equipment failure (DOPE).
Subjective Comfort Level
At the end of the questionnaire, we asked the nurses if they were well updated and felt comfortable working with tracheostomized pediatric patients requiring ventilator assistance or not. To assess the level of confidence, we compared their answers to this question (subjective confidence) with their objective total score. Among 33 (76.7%) nurses who confirmed that they were well updated and confident, 54% scored above average, 35% were average, and 11% were below average (P=0.005). Among the ten (23.3%) nurses who responded negatively to the question and were uncomfortable with tracheostomy care; 33 (76.7%) scored below average, and 10 (23.3%) had pass scores (P=0.002). Finally, among the 43 nurses, 14 (32.6%) were very comfortable working with tracheostomy patients, 13 (30.2%) were comfortable, and 16 (37.2%) were uncomfortable. Of interest, we found no clear relationship between nurses’ age and confidence level with tracheostomy care, which ranged from 64.7%, 54.4% and 100% in those aged 20–30 years, 30–40 years, and 40–50 years respectively.
Discussion
Among intensive care patients, 10–24% will need a tracheostomy.13 The most common indications for tracheostomy in children with chronic disorders are neurologic and neuromuscular illnesses.14 Although tracheostomy is a simple, safe procedure when proactively planned, it may involve serious complications postoperatively if a proper care plan is not instituted by qualified nurses.15,16 Nurses are the front-line staff in tracheostomy care which mainly involves dressing, tube changing, suctioning, and managing potential emergencies. A nurse-to-patient ratio of 1:1 is recommended to ensure optimal care in an intensive care unit and a ratio of 1:2 in high dependency patients.17 While the tracheostomy care of children is the responsibility of nurses in their primary unit of practice, multidisciplinary, collaborative interprofessional teamwork should be strongly encouraged to achieve optimal patient outcomes.15
Among the subjects enrolled in our study, the primary diagnosis in most patients who required a tracheostomy was neurologic 21 (45.7%) and neuromuscular 14 (30.5%) disease. Overall, most patients had the procedure performed between one and five years of age (n= 22; 47.8%) and 18 (39.1%) had a tracheostomy instituted at greater than 5 years. Veder et al reported that the primary reasons for a tracheostomy were airway obstruction comprising laryngotracheal obstruction and craniofacial anomalies and those requiring respiratory support for cardio-pulmonary and neurological diseases.18 The group of children with airway obstruction were younger when tracheostomized (3.0 months vs 31.0 months, P < 0.05) and were dependent for a longer duration (median 21.5 months vs 2.0 months, P < 0.05) than the pulmonary support group.
Regarding overall tracheostomy complications, the rate in our study was low (Table 2), and in the main were of late onset manifesting as obstruction with a mucous plug or stoma infection and because of timely intervention, were uneventful. Accidental decannulation occurred in 17.3% of patients. Elective decannulation was performed in 8.7% of the patients, which correlated with children who were tracheotomized post road traffic accidents, and who were discharged to home care. Mortality occurred in 30.4% of the patients due to underlying illnesses such as acute respiratory distress syndrome and septic shock and was unrelated to tracheostomy complications. Our findings align with a low tracheostomy-related mortality of 1.43% in a recent pediatric, population-based study.19
The IECC provides orientation and an annual comprehensive and competency-based learning program for all nurses involved in the care of tracheostomized pediatric patients who are chronically ventilator dependent. The TCCLP is a mandatory course for all nurses. We found that nurses who attended more than five courses were highly comfortable with tracheostomy care.
Hands-on care for tracheostomized pediatric patients is commonly taught by the transmission of knowledge and experience from one nurse to another.10 In our study, we found that there was a significant relationship between years of experience and level of knowledge and comfort with the management of a tracheostomy. Nurses with more than five years of experience had higher scores in knowledge and comfort compared to nurses with experience of less than one year. The findings differ from Mungan et al who reported an insignificant relationship either between duration of experience or academic qualifications.9 Paul et al found that graduate nurses who acquired knowledge in their undergraduate studies were more confident than those who received it during their practice.20
Our analysis showed no clear relationship between nurses’ age and percent confidence level with tracheostomy care, which was lowest among nurses aged 30–40 years (54.4%) and highest in those who were 40–50 years of age (100%). This is consistent with the findings by Mungan and Sreeja et al where there were insignificant differences in knowledge across the age groups.9,21
Regarding academic degree qualifications and the comfort level of nurses with tracheostomized patients, 74.1% (n=20/27) had a bachelor’s degree, and most of the uncomfortable nurses (56.3%; n=9/16) had a general nurse diploma. There was a significant association between academic degree and comfort level (P=0.015). This could be either due to the difference in the curriculum or self-confidence backed by a higher academic degree. The results contrast with the report by Sreeja et al who found no significant difference in knowledge relative to educational qualifications.21 Additionally, Al Nemare et al,22 found no difference in the confidence level between nurses who graduated from outside or inside Saudi Arabia, while in our study, we had only one nurse who graduated from Saudi Arabia and was uncomfortable with tracheostomy care.
BLS, ACLS, and PALS are required courses for resuscitation and are now mandatory for all health care providers. Interestingly, in our study, we found a significant relationship between nurses who were certified in more than one course and their comfort level with tracheostomy care. The nurses who were only BLS certified felt uncomfortable, while the nurses who were additionally certified in PALS or ACLS were comfortable as were those certified in both PALS and ACLS.
In our study, nurses were more knowledgeable and skilled with routine daily tracheostomy care compared to dealing with emergencies, which is consistent with the documentation by Mungan et al.9 This deficit is a major concern that may lead to compromised outcomes and merits consideration when designing the next TCCLP course. A study conducted in 2016 to assess nurses’ confidence level with tracheostomy care in two tertiary care centers in Jeddah, showed that 88.6% were not very confident in the care of patients with a tracheostomy, and providing ventilatory assistance.23 Similarly, in Turkey, Mungan et al found in three tertiary state hospitals that the level of nurses’ knowledge with tracheostomy care was below expectations.9 In contrast, Al Nemare reported that 60% of the nurses were confident and that 47% of the nurses did not feel or were unsure if they were up to date with recent information regarding tracheostomy care. More than half of the participants seemed to have inadequate training and support, and most of the practice was experience-based, rather than evidence-based, as confidence level correlated with years of experience.22 We compared the subjective and objective comfort levels with tracheostomy care, and of the 76.7% of nurses who felt they were comfortable, 89% were truly comfortable, according to their scores. Eleven percent thought they were comfortable and well updated but had a below-average score which shows an apparent deficit in nurses’ perspective of their knowledge and skills. Pritchett et al reported that intensive care nurses were significantly more comfortable in the management of both a fresh and established tracheostomy compared to non-intensive care nurses.24 Additionally, non-intensive care nurses with more than five years of pediatric experience were statistically more comfortable handling accidental tracheal decannulations.24
Insufficient knowledge regarding tracheostomy care is a widely reported issue that impacts outcomes and may result in increased mortality in such patients. Our study showed that multiple factors play a significant role in nurses’ comfort level with tracheostomy care such as academic degree, experience duration, and training courses. To improve nurses’ comfort level, we suggest that all centers with tracheotomized patients encourage nurses to procure a bachelor or higher degree, undergo mandatory training for a prescribed number of hours, motivate nurse’s with more than five years of experience to nurture and mentor nurses with less experience and to be certified in PALS and ACLS courses. Parker et al also recommended the addition of tracheostomy care skills into BLS.1 We noted that 32 (74.4%) of 43 nurses knew all the information to be included in the medical record when handling tracheostomized patients and fully appreciated the significant impact of bedside hand-off using the Situation, Background, Assessment, Recommendation (SBAR) technique that Abbaszade et al reported in their study.25 Nurses should familiarize themselves with this framework to optimize communication between members of the health care team about a patient’s condition and enhance the quality of nursing care across all dimensions.
Finally, we strongly recommend a continuous quality improvement project with an auditing process. This should perhaps become the traditional theoretical teaching module of tracheostomy care with a well-structured, pediatric disease focused program, using high fidelity simulation methods to increase nurses’ knowledge, skills, and ultimately comfort level.26–29
There are several limitations of this study that merit consideration. First, we included only one center with a small, specific sample size of pediatric patients. However, there was no selection bias since all the nurses in the center participated in the survey, which is a major strength and our questionnaire covered more than one practical aspect of tracheostomy care. Second, the questionnaire was adopted from the available literature but was not internally or externally validated for robustness before implementation, although the components were uniformly agreed upon by the local intensivists. Third, although the findings in part were replicated in other studies, our findings are applicable and generalizable to similar long term care facilities. Last, we did not address safety recommendations for children who received a tracheostomy during the COVID-19 pandemic. In a state-of-the-art review, Meister et al outlined modified protocols for tracheostomy care, albeit predominantly in adults, stressing the importance of safety across multidisciplinary teams and healthcare providers with the use of personal protective equipment and being more vigilant for potential complications.30
Conclusion
Nurses’ performance in this study showed a significant positive correlation between nurses’ comfort level with tracheal care and academic degree, duration of pediatric experience, completion of more than one life support course, and attending the annual local tracheostomy care competency learning program. Our study confirms that nurses with more pediatric experience, repetitive participation in tracheostomy care programs and advanced life support courses, achieve greater competency with tracheostomy care. The disappointing revelation is that nurses often score the competency and confidence of dealing with a tracheostomy higher than their knowledge-based answers support. The gap in nurses’ knowledge and skills regarding emergency care of a tracheostomy needs to be fully addressed in the next annual educational program using a proper structured and valid simulation model with a continuous quality auditing tool.
Data Sharing Statement
Data supporting the findings of this study are available upon request from the corresponding author.
Ethical Approval
Data collection for analysis was accrued with participants’ agreement and was approved by the IECC Institutional Review Board (IECC IRB) Jeddah, Saudi Arabia, dated 13/09/2021.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for-profit sectors.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Parker V, Giles M, Shylan G, et al. Tracheostomy management in acute care facilities—a matter of teamwork. J Clin Nurs. 2010;19(9–10):1275–1283. doi:10.1111/j.1365-2702.2009.03155.x
2. Heafield S, Karnik A, Rogers M. Tracheostomy management in ordinary wards. Hosp Med. 1999;60(4):261–262. doi:10.12968/hosp.1999.60.4.1092
3. Garrubba M, Turner T, Grieveson C. Multidisciplinary care for tracheostomy patients: a systematic review. Crit Care. 2009;13(6):177. doi:10.1186/cc8159
4. Lubianca Neto JF, Castagno OC, Schuster AK. Complications of tracheostomy in children: a systematic review. Braz J Otorhinolaryngol. 2020. PMID: 33472759. doi:10.1016/j.bjorl.2020.12.006.
5. Brenner MJ, Pandian V, Milliren CE, et al. Global tracheostomy collaborative: data-driven improvements in patient safety through multidisciplinary teamwork, standardisation, education, and patient partnership. Br J Anaesth. 2020;125(1):e104–e118. doi:10.1016/j.bja.2020.04.054
6. Cheung NH, Napolitano LM. Tracheostomy: epidemiology, indications, timing, technique, and outcomes. Respir Care. 2014;59(6):895–915. doi:10.4187/respcare.02971
7. Dorton LH, Lintzenich CR, Evans AK. Simulation model for tracheotomy education for primary health-care providers. Ann Otol Rhinol Laryngol. 2014;123(1):11–18. doi:10.1177/0003489414521144
8. Farida JP, Lawrence LA, Svider PF, et al. Protecting the airway and the physician: aspects of litigation arising from tracheotomy. Head Neck. 2016;38(5):751–754. doi:10.1002/hed.23950
9. Mungan İ, Kazancı D, Bektaş Ş, Sarı S, Çavuş M, Turan S. The evaluation of nurses’ knowledge related to tracheostomy care in tertiary intensive care units. Int Med. 2019;1(6):313–318. doi:10.5455/im.54258
10. Smith-Miller C. Graduate nurses comfort and knowledge level regarding tracheostomy care. J Nurses Prof Dev. 2006;22(5):222–229. doi:10.1097/00124645-200609000-00003
11. Hickey M. Focus on tracheostomy. Perspectives—Recovery strategies from the OR to home. Philadelphia: Lippincott Williams & Wilkins; 2002: 1–8.
12. DeVellis R. Scale development: theory and applications (Applied Social Research Methods Series No. 26). NewburyPark, CA: Sage Publications; 1991.
13. Esteban A, Anzueto A, Alía I, et al. How is mechanical ventilation employed in the intensive care unit? An international utilization review. Am J Respir Crit Care Med. 2000;161(5):1450–1458. doi:10.1164/ajrccm.161.5.9902018
14. Raimonde AJ, Westhoven N, Winters R. Tracheostomy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021.
15. Bedwell JR, Pandian V, Roberson DW, McGrath BA, Cameron TS, Brenner MJ. Multidisciplinary tracheostomy care: how collaboratives drive quality improvement. Otolaryngol Clin North Am. 2019;52(1):135–147. doi:10.1016/j.otc.2018.08.006
16. Strychowsky JE, Albert D, Chan K, et al. International Pediatric Otolaryngology Group (IPOG) consensus recommendations: routine peri-operative pediatric tracheotomy care. Int J Pediatr Otorhinolaryngol. 2016;86:250–255. doi:10.1016/j.ijporl.2016.03.029
17. Australian College of Critical Care Nurses Ltd (ACCCN). Position statement on intensive care nursing staffing. Aust Crit Care. 2002;15(1):6–7. doi:10.1016/S1036-7314(02)80037-6
18. Veder LL, Joosten KFM, Zondag MD, Pullens B. Indications and clinical outcome in pediatric tracheostomy: lessons learned. Int J Pediatr Otorhinolaryngol. 2021;151:110927. doi:10.1016/j.ijporl.2021.110927
19. Kang KT, Lin YS, Lin CY, Lee CH, Hsu WC. Epidemiology of pediatric tracheotomy: a population-based study using National Health Insurance Research Database in Taiwan. Int J Pediatr Otorhinolaryngol. 2022;152:110989. doi:10.1016/j.ijporl.2021.110989
20. Paul F. Tracheostomy care and management in general wards and community settings: literature review. Nurs Crit Care. 2010;15(2):76–85. doi:10.1111/j.1478-5153.2010.00386.x
21. Sreeja TP Knowledge assessment of nurses about tracheostomy care; 2007. Available from: http://dspace.sctimst.ac.in/jspui/handle/123456789/1573.
22. Alnemare AK. Nurses training and confidence in management of tracheostomy patients in a community hospital in Saudi Arabia. J Res Med Dent Sci. 2020;8(5):110–118.
23. Al-Khatib T, Mahfoz TB, Arif R. Nurses training, clinical support and confidence in management of tracheostomy patients in Jeddah, Saudi Arabia. Saudi J Otorhinolaryngol Head Neck Surg. 2017;19(2):51–57. doi:10.4103/1319-8491.275316
24. Pritchett CV, Foster Rietz M, Ray A, Brenner MJ, Brown D. Inpatient nursing and parental comfort in managing pediatric tracheostomy care and emergencies. JAMA Otolaryngol Head Neck Surg. 2016;142(2):132–137. doi:10.1001/jamaoto.2015.3050
25. Abbaszade A, Assarroudi A, Armat MR, et al. Evaluation of the impact of handoff based on the SBAR technique on quality of nursing care. J Nurs Care Qual. 2021;36(3):E38–E43. doi:10.1097/NCQ.0000000000000498
26. McCoy JL, Williams KA, Senkinc JL, Westerman J, Tobey AB. Pediatric tracheostomy care simulation: real-life scenarios in a safe learning environment. Respir Care. 2021. doi:10.4187/respcare.09201
27. Shah SJ, Cusumano C, Ahmed S, Ma A, Jafri FN, Yang CJ. In situ simulation to assess pediatric tracheostomy care safety: a novel multicenter quality improvement program. Otolaryngol Head Neck Surg. 2020;163(2):250–258. PMID: 32450759. doi:10.1177/0194599820923659
28. Wooldridge AL, Carter KF. Pediatric and neonatal tracheostomy caregiver education with phased simulation to increase competency and enhance coping. J Pediatr Nurs. 2021;60:247–251. doi:10.1016/j.pedn.2021.07.011
29. Uyan ZS, Atag E, Ergenekon AP, et al. Efficacy of standardized tracheostomy training with a simulation model for healthcare providers: a study by ISPAT team. Pediatr Pulmonol. 2022;57(2):418–426. doi:10.1002/ppul.25772
30. Meister KD, Pandian V, Hillel AT, et al. Multidisciplinary safety recommendations after tracheostomy during COVID-19 pandemic: state of the art review. Otolaryngol Head Neck Surg. 2021;164(5):984–1000. doi:10.1177/0194599820961990
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Nurses’ Lived Experiences of Assessing Pain in Hospitalized Children in Indonesia: A Qualitative Phenomenological Study
Ramdhanie GG, Wanda D, Agustini N, Nurhaeni N, Mediani HS, Abuzairi T, Akbar MA, Nugraha BA
Journal of Multidisciplinary Healthcare 2026, 19:600334
Published Date: 18 May 2026