Back to Journals » Journal of Inflammation Research » Volume 15
Assessment of Long-Term Effects on Pulmonary Functions Between Severe and Non-Severe Convalescent COVID-19 Patients: A Single-Center Study in China
Authors Tang YF, Han JY, Ren AM, Chen L, Xue TJ, Yan YH, Wang X ![]() , Wang Y, Jin RH
, Wang Y, Jin RH
Received 19 April 2022
Accepted for publication 1 August 2022
Published 19 August 2022 Volume 2022:15 Pages 4751—4761
DOI https://doi.org/10.2147/JIR.S371283
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ning Quan
Yan-Fen Tang,1,2,* Jun-Yan Han,2– 4,* Ai-Min Ren,1,2 Li Chen,1,2 Tian-Jiao Xue,1,2 Yong-Hong Yan,2– 4 Xi Wang,2– 4 Yu Wang,1,2 Rong-Hua Jin2,3,5
1Department of Respiratory, Beijing Ditan Hospital Capital Medical University, Beijing, 100015, People’s Republic of China; 2National Center for Infectious Diseases, Beijing Ditan Hospital, Capital Medical University, Beijing, 100015, People’s Republic of China; 3Institute of Infectious Diseases, Beijing Key Laboratory of Emerging Infectious Diseases, Beijing Ditan Hospital, Capital Medical University, Beijing, 100015, People’s Republic of China; 4Beijing Institute of Infectious Diseases, Beijing, 100015, People’s Republic of China; 5Changping Laboratory, Beijing, 102299, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Rong-Hua Jin, National Center for Infectious Diseases, Beijing Ditan Hospital, Capital Medical University, No. 8, Jingshun Dongjie, Chaoyang District, Beijing, 100015, People’s Republic of China, Tel +86 10 84322009, Fax +86 10 84322146, Email [email protected] Yu Wang, Department of Respiratory, Beijing Ditan Hospital, Capital Medical University, No. 8, Jingshun Dongjie, Chaoyang District, Beijing, 100015, People’s Republic of China, Tel +86 10 84322963, Fax +86 10 84322146, Email [email protected]
Objective: To explore the long-term effects of SARS-Cov-2 infection on the pulmonary function in the severe convalescent COVID-19 patients for 6 to 9 months follow-up in Beijing, China.
Methods: A total of 64 cases of COVID-19 patients were recruited for the study and discharged from the Beijing Ditan Hospital, Capital Medical University, for 6 to 9 months. COVID-19 patients were divided into non-severe (mild and moderate) and severe groups. The follow-up investigated the lung function tests, the novel coronavirus antibody (IgM and IgG), chest CT and blood tests.
Results: About 25.00% (16/64) patients had pulmonary ventilation dysfunction and 35.9% (23/64) had diffusion dysfunction. In the severe group, 56.50% (13/23) individuals showed decreased diffusion function. The diffusion dysfunction of the severe group was significantly decreased than the non-severe group (P = 0.01). Among 56 cases, the positive rate of IgG titers was 73.2% (41/56). The result of chest CT showed 55.36% (31/56) cases in nodules, 44.64% (25/56) in strip-like changes, 37.5% (21/56) in-ground glass shadow, and 5.36% (3/56) in grid shadow, which was significantly different between the severe group and the non-severe group. Patients tended to have ground glass changes in the severe group while nodules in the non-severe group.
Conclusion: For the 6 to 9 months in convalescent COVID-19 patients, 56.50% (13/23) of severe patients had pulmonary diffusion dysfunction. Convalescent COVID-19 patients should have their pulmonary function regularly tested, especially those with severe illness.
Keywords: COVID-19, pulmonary function, SARS-CoV-2 antibody, severe patients, chest CT, follow-up
Introduction
Similar to severe acute respiratory syndrome coronavirus (SARS-CoV) infection, SARS-CoV-2 infection triggers dysregulated immune-mediated processes that can lead to anatomical damage and fibrosis,1,2 influencing lung morphology and function beyond acute disease.3–7 Currently, some studies have reported the pulmonary function alteration of COVID-19 patients 3 to 12 months after they being discharged from the hospital. COVID-19 infection can cause pulmonary function impairment, manifested as restricted ventilation dysfunction, small airway dysfunction, and diffusion dysfunction.8 A meta-analysis showed the overall prevalence of abnormalities in pulmonary function was 20% (95% CI 13–17%) and included low diffusion capacity, reduced lung volume, or airflow obstruction.9 Diffusion dysfunction (DLCO <80%) was the most common abnormality, followed by reduced lung volume measurements, including TLC <80%, FVC <80%, and FEV1 <80%. Airflow obstruction (FEV1/FVC <70%) was relatively uncommon.10 There has been increasing focus on the diffusing capacity of the lungs for carbon monoxide (DLCO), a key measurement of pulmonary gas exchange. In addition to infection-related events, the increased mechanical stress caused by both prolonged positive pressure and mechanical ventilation may cause a direct mechanical insult, contributing to lung injury. Similarly, the intense inspiratory efforts of spontaneously breathing patients may also cause self-inflicted lung injury.11,12 Also, severe patients were more likely to suffer from persistent abnormal pulmonary functions.10 Follow-up of COVID-19 patients at 3 months, 6 months, or even 1 year after discharge has been reported.8,13–16 Pulmonary diffusion capacity was the most common impaired lung function in recovered patients with COVID-19. Several risk factors, such as female, altered chest CT, older age, higher D-dimer levels, and urea nitrogen, are associated with impairment of DLCO.17
However, the number of follow-up cases was limited and the patients had obvious geographical limitations, and most studies did not include the alteration of the pulmonary function. At present, pulmonary function detection is not a routine examination in the follow-up content because pulmonary function test requires the patient to repeatedly take out a forced breath action, which causes patients to cough and sputum; technicians should not only wear a complete set of personal protective equipment but also have strict requirements for air circulation time and room cleaning, which limits pulmonary function test, especially in COVID-19 epidemic phase. Persistent impairment of pulmonary function and exercise capacity have been known to last for months or even years in the recovered survivors with other coronavirus pneumonia (SARS (severe acute respiratory syndrome) and MERS (Middle East respiratory syndrome)). There are few reports on the recovery of pulmonary function in convalescent COVID-19 patients. So will the infection of COVID-19 patients lead to impaired pulmonary function or even pulmonary fibrosis? Therefore, the study aims to investigate the pulmonary function of convalescent COVID-19, especially in severe patients at 6 to 9 months of follow-up in Beijing, China.
Materials and Methods
Patients
This study collected 64 patients with COVID-19 who met the clinical cure criteria after hospitalization at Beijing Ditan Hospital, Capital Medical University from February 11, 2020, to June 14, 2020. Of the 64 patients with confirmed COVID-19 who were followed up for 6 to 9 months from November 13, 2020, to December 15, 2020, all patients had lung function tests, and 56 of them had their blood routine, liver function, blood coagulation, myocardial enzymes, new coronavirus nucleic acid, SARS-CoV-2 specific IgG, and IgM antibody, chest CT examination, and collected the clinical manifestations and comorbidities of patients at the time of onset (Figure 1). This study was approved by the Committee of Ethics at Beijing Ditan Hospital, Capital Medical University [No. JDLKZ (2020) D (042)-02] with informed consent. All patients signed informed consent. The patients were divided into mild (mild symptoms without the radiographic appearance of pneumonia, n = 10), moderate (having symptoms and the radiographic evidence of pneumonia, with no requirement for supplemental oxygen, n = 31, or n = 28), and severe group (having pneumonia, including one of the following: respiratory rate >30 breaths/minute; severe respiratory distress; or SpO2 ≤93% on room air at rest, and critical cases (eg, respiratory failure requiring mechanical ventilation, septic shock, other organ failure occurrence or admission into the ICU), n = 23 or n = 18) according to the WHO interim guidance18 and the guidance from China.19 For statistical purposes, we classified the mild and moderate groups as the non-severe group (n = 41 or n = 38).
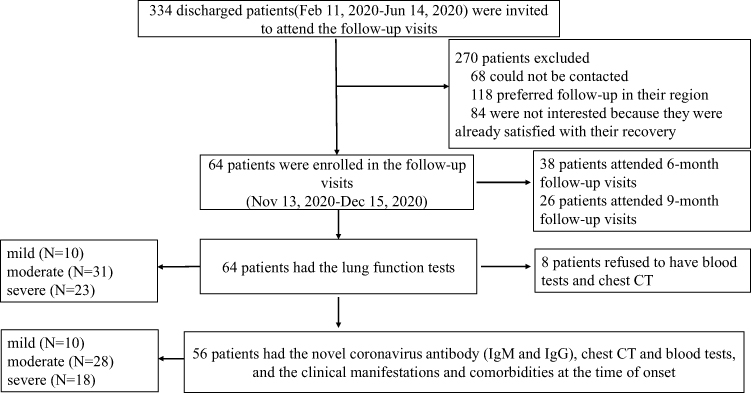 |
Figure 1 Enrollment of COVID-19 patients and follow-up after hospital discharge. 334 discharged patients were invited to attend the follow-up visits. 64 patients were enrolled in the follow-up visits. |
Detection of the SARS-CoV-2 Specific IgG and IgM Antibody
Novel coronavirus antibody detection was achieved by using the Novel Coronavirus antibody kit (Lizhu Pharmaceutical Group Co., Ltd. China). Novel coronavirus (2019-nCoV) antibody IgM (2019-nCoV IgM) and 2019-nCoV IgG were detected by the colloidal-gold method (Reovirus). 2019-nCoV IgM and IgG were shown in unit of S/CO, a value less than 0.79 was considered negative, a value of 0.80–1.20 was considered suspicious, and a value more than 1.21 was considered positive.
Determination of Pulmonary Function
According to the basic guidelines for routine pulmonary function examination (2018)20 and ATS-ERS guidelines,21 we use the MSDIFFUSION APS pulmonary function tester produced by Yegge Company, Germany, which measures the forced vital capacity (FVC), takes one-second forced expiratory volume (FEV1), one-second rate (FEV1/FVC) and measuring carbon monoxide dispersion with one breath (DLCO). The maximum expiratory flow at 50% of vital capacity is denoted by FEF50, and the maximum expiratory flow at 75% of vital capacity is denoted by FEF75. Pulmonary function criteria include the following: (1) pulmonary ventilation function—FEV1/pred <80% and FEV1/FVC <70% were pulmonary obstructive ventilation dysfunction; FEV1/pred <80% and FEV1/FVC >70% indicating restrictive ventilation dysfunction. (2) pulmonary diffusion dysfunction— DLCO/pred <80% was abnormal, and (3) small airway dysfunction—2 out of 3 items (FEF50%, FEF75%, FEF25–75% (MMEF)) are lower than 65% of the predicted value.
Chest CT Scan
CT scans were performed on a 64-slice spiral CTs (Philips, iCT, the Netherlands). The scan parameters are 120 kV (tube voltage), 210 mA (tube current), FOV 500 mmx500 mm, matrix 512x512, pitch 0.975, rotation time 0.35–0.5 s/circle, scanning layer thickness 5 mm, reconstruction layer thickness 1 mm.
Statistical Analysis
Statistical analysis was performed using SPSS 19.0. Continuous variables first pass through the Kolmogorov–Smirnov Test to assess the normality of the data distribution. Variables meeting the normal distribution were tested by the Student’s t-test (two sets of samples) or ANOVA analysis (multiple samples) combined with Tukey HSD post hoc test; non-normal distributed data Mann–Whitney U (two sets of samples) or Kruskal–Wallis H (multiple group samples) analysis. Categorical variables Chi-square tests or Fisher’s exact test was used and combined with Bonferroni correction. Binary logistic regression analysis was conducted to explore related factors associated with impaired pulmonary function in severe convalescent patients. All tests were two-sided, and a p-value less than 0.05 was statistically significant.
Results
General Information
Of the 56 follow-up patients, 37 were males and 19 were females aged (46.98 ± 14.09). The time from symptom onset to discharge was 33.11 ± 9.89 days. Age, time from hospital to discharge, fever, chills, sputum expectoration, and myalgia were statistically significant differences between the two groups (Table 1).
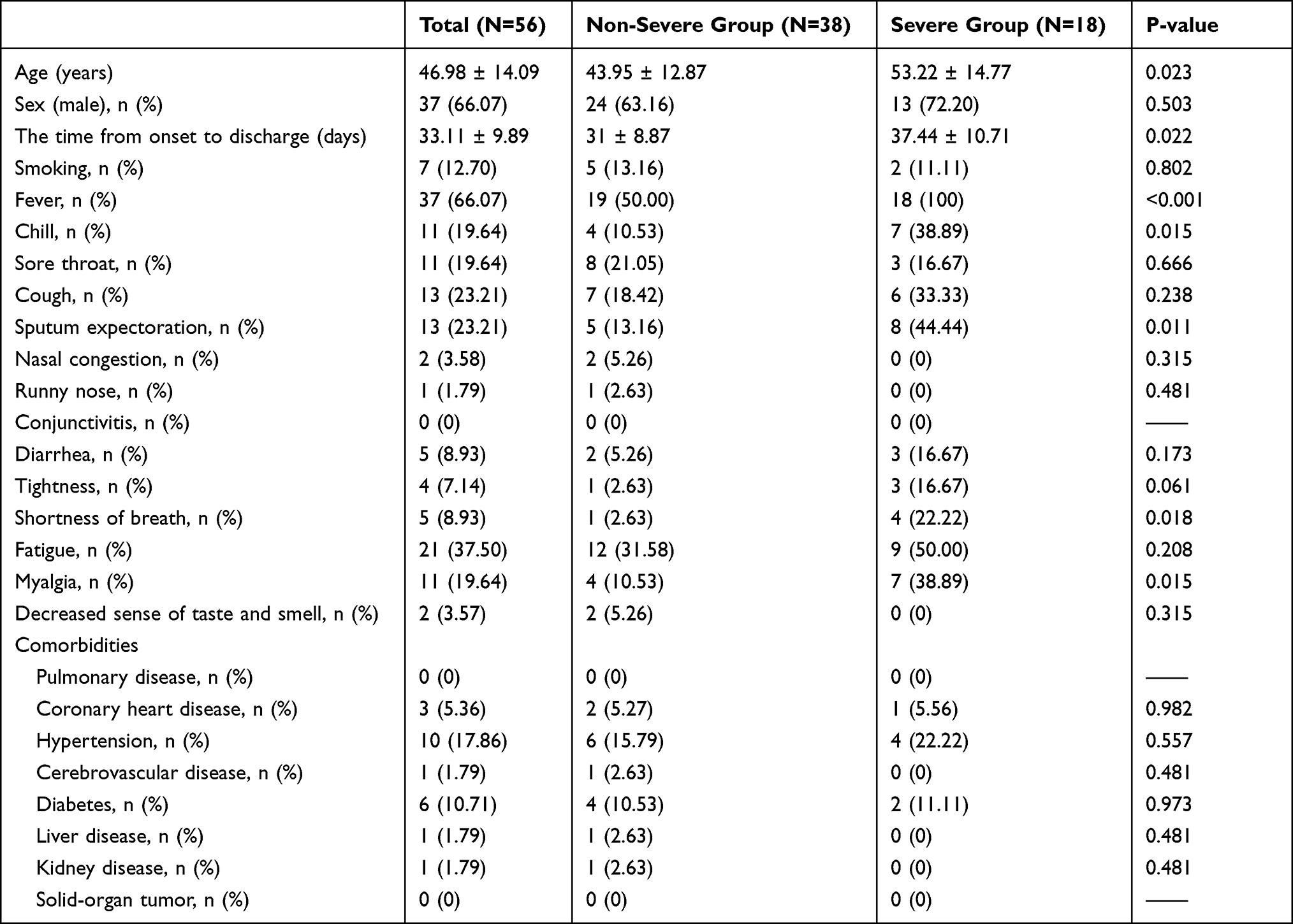 |
Table 1 Symptoms and Comorbidities of COVID-19 Patients in Different Groups |
SARS-Cov-2 IgG Positive Rates Were Comparable Among the Non-Severe and the Severe COVID-19 Patients
The novel coronavirus nucleic acid test of 56 cases of patients was negative. The SARS-Cov-2 IgM titer and the SARS-Cov-2 IgG titer were 0.39 (0.19–0.65) and 7.21 (0.78–18.42). The positive rates of SARS-Cov-2 IgM and IgG titer within 6 to 9 months after discharge were 17.86% and 73.21%, comparable among the non-severe and the severe patients (Table 2).
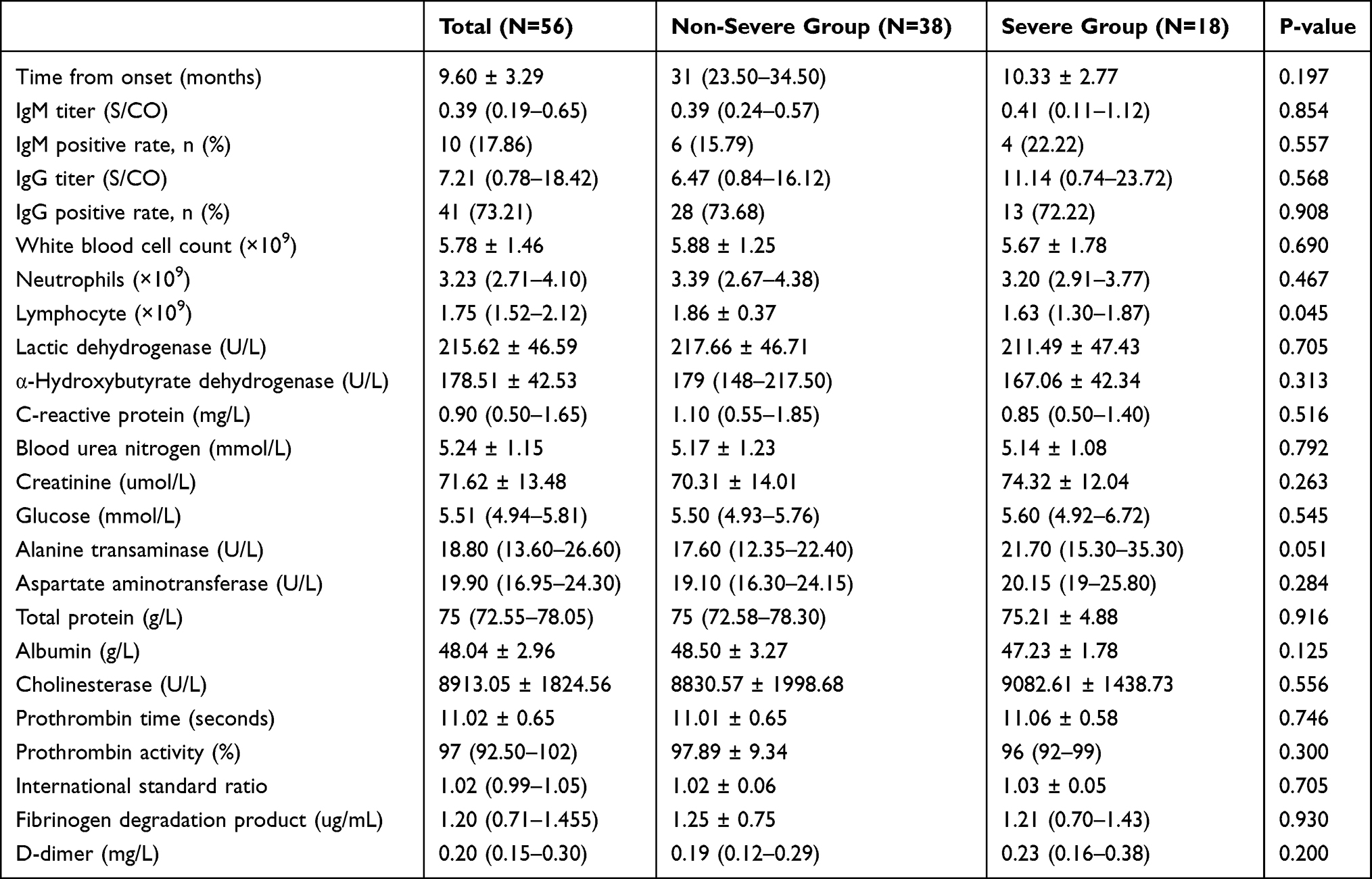 |
Table 2 Laboratory Test Results for COVID-19 Recovery with Different Groups |
Laboratory Results for COVID-19 Recovery with Different Groups
To explore the effect of SARS-Cov-2 infection on systemic organs, we showed the laboratory result of 56 patients during follow-up in Table 2. The counts of lymphocytes were significantly different in the two groups (P = 0.045, Table 2). Other laboratory results were similar among different groups, including liver, kidney, coagulation, and blood system.
Differential Pulmonary Functional Recovery from Severe COVID-19 and Impaired Diffusion Function in Recovered Severe COVID-19 Patients
Among the 64 patients with the pulmonary functional test, 39 (60.93%) were males and 20 cases (31.25%) of smokers. There were 16 cases (25.00%) with pulmonary ventilation dysfunction, including 15 cases (23.43%) with restrictive ventilation dysfunction and 1 cases (1.56%) with obstructive ventilation dysfunction, and 23 cases (35.94%) with diffusion dysfunction (Table 3). Table 3 shows a significant difference in restrictive ventilation dysfunctions between the severe and the non-severe group (p = 0.005); Similarly, diffusion dysfunction was observed among different groups, which accounted for 24.39% in the non-severe illness, including the mild and the moderate patients, and 56.5% in the severe group (p = 0.01). This trend of the gradual decrease in the level of DLCO among patients was identical to the degree of severity. In the severe group, DLCO% pred was lower than the average of the groups, indicating that the diffusion dysfunction in the severe group is significantly different from the non-severe group (P = 0.009). The value of TLC % pred in the severe group was much less than that of the non-severe group, suggesting a higher impairment of lung volume in severe COVID-19 patients. Thus, the difference in diffusion dysfunction is statistically significant between the two groups, and the diffusion dysfunction was especially decreased in the severe group.
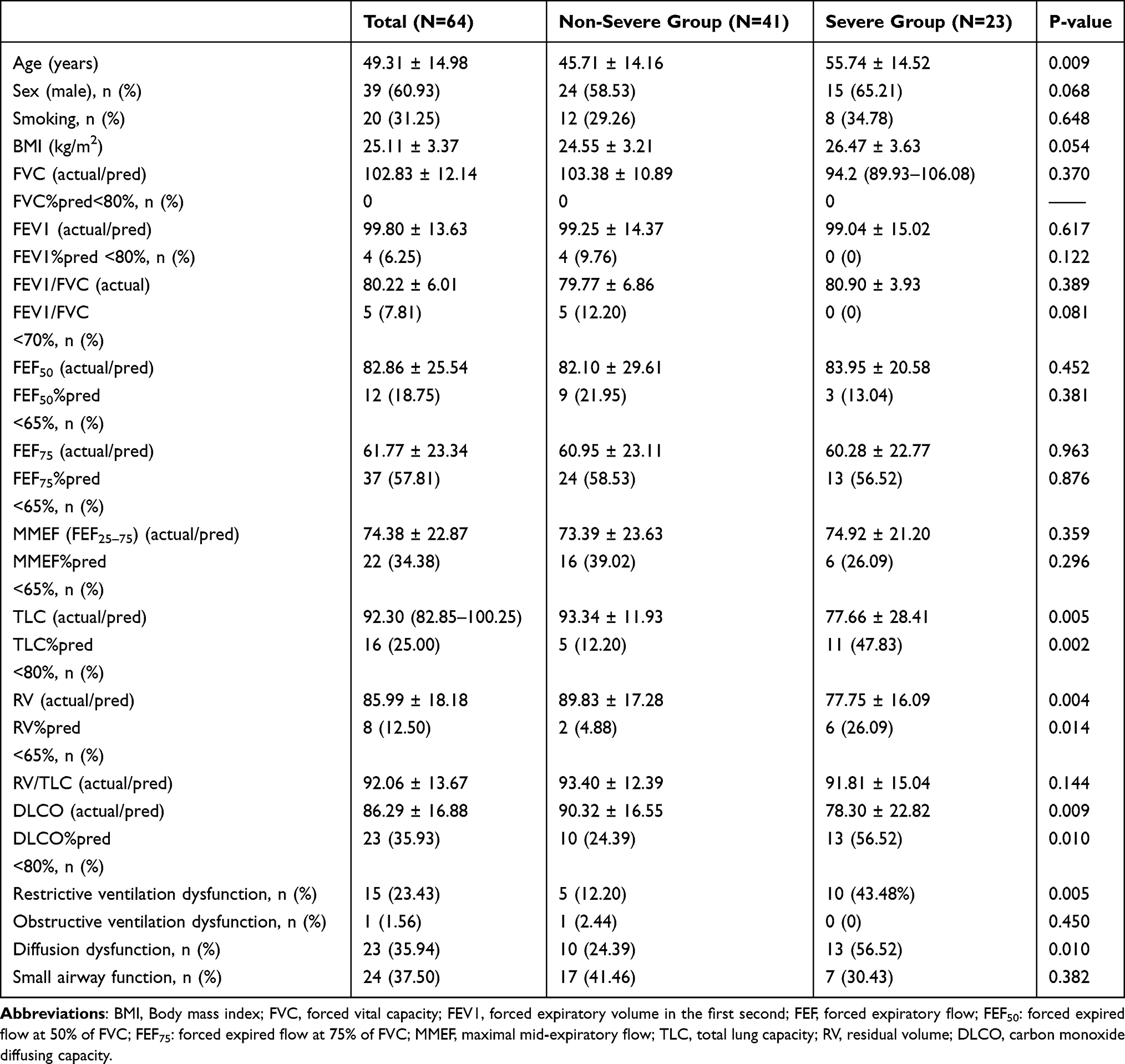 |
Table 3 Pulmonary Function in COVID-19 Recovery with Different Groups |
Female and Smoking Positively Correlated with Diffusion Dysfunction, and Age Was Correlated with Diffusion Dysfunction in Severe Patients
To explore the factors correlated with the decrease in the diffusion dysfunction in the convalescent COVID-19 patients, we divided the 56 cases into two groups (with and without diffusion dysfunction) according to the diffusion function. We observed no significant association between age, comorbidities, oxygen therapy, and treatment of hormone, antiviral, convalescent plasma, and immunoglobulin with diffusion impairment. Both females and smoking were risk factors for diffusion impairment (P = 0.013 and P = 0.022, Table 4).
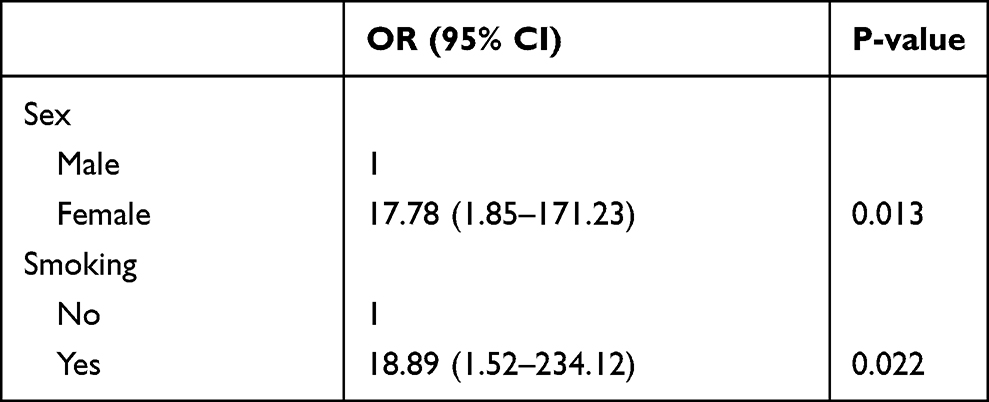 |
Table 4 Correlation of Diffusion Dysfunction Risk Factors |
Further, the pulmonary function of 18 severe cases was divided into two groups with the diffusion dysfunction. There was no significant association between sex, smoking, fever, comorbidities, oxygen therapy, hormone, convalescent plasma, and immunoglobulin with diffusion impairment. Age correlated with impaired diffusion in severe patients (P = 0.024, Table 5).
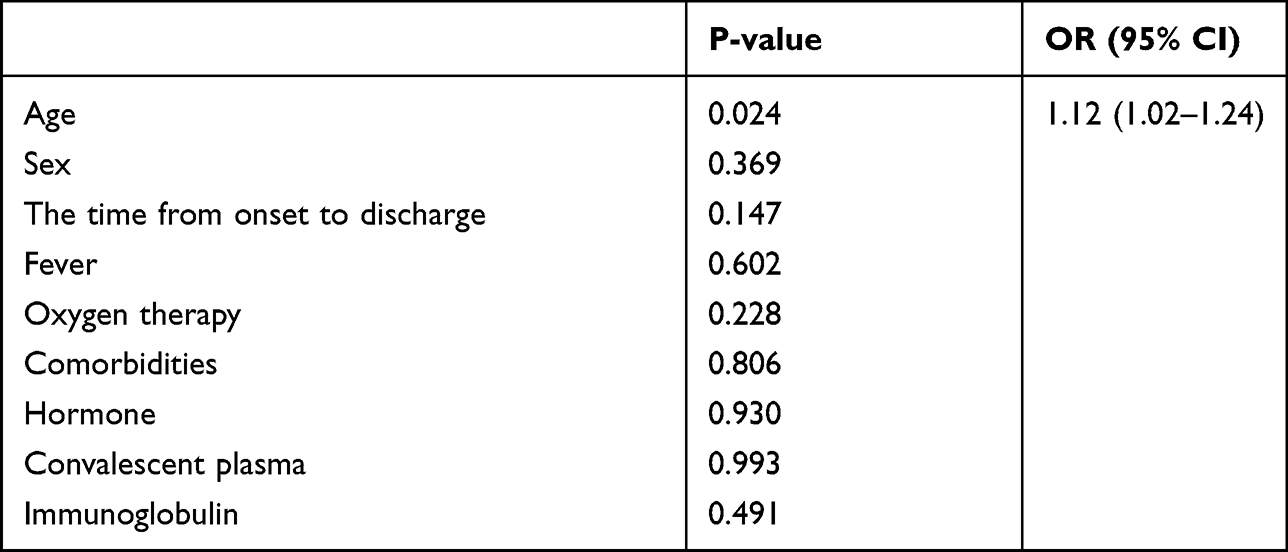 |
Table 5 Analysis of Correlated Factors of Diffusion Dysfunction in Severe Patients |
Chest CT Findings Were Incomparable Among Different Convalescent COVID-19 Patients
According to the chest CT imaging findings, the lung lesions of 56 patients were divided into glass shadow, stripe, grid shadow, nodular shadow, and new lesions. The study results found that more than half of the patients had lung lesions, and most of the lesions were located in the lower lungs. The main manifestations are nodular shadows, streaks, and ground glass shadows. Most of the severe group has strip-like changes (72.22%), ground glass (61.11%), and grid shadow (16.67%). Comparing the two groups, the differences in ground glass-like changes (P = 0.012), strip-like changes (P = 0.004), grid shadows (P = 0.010), and nodular shadows (P = 0.023) were statistically significant (Table 6).
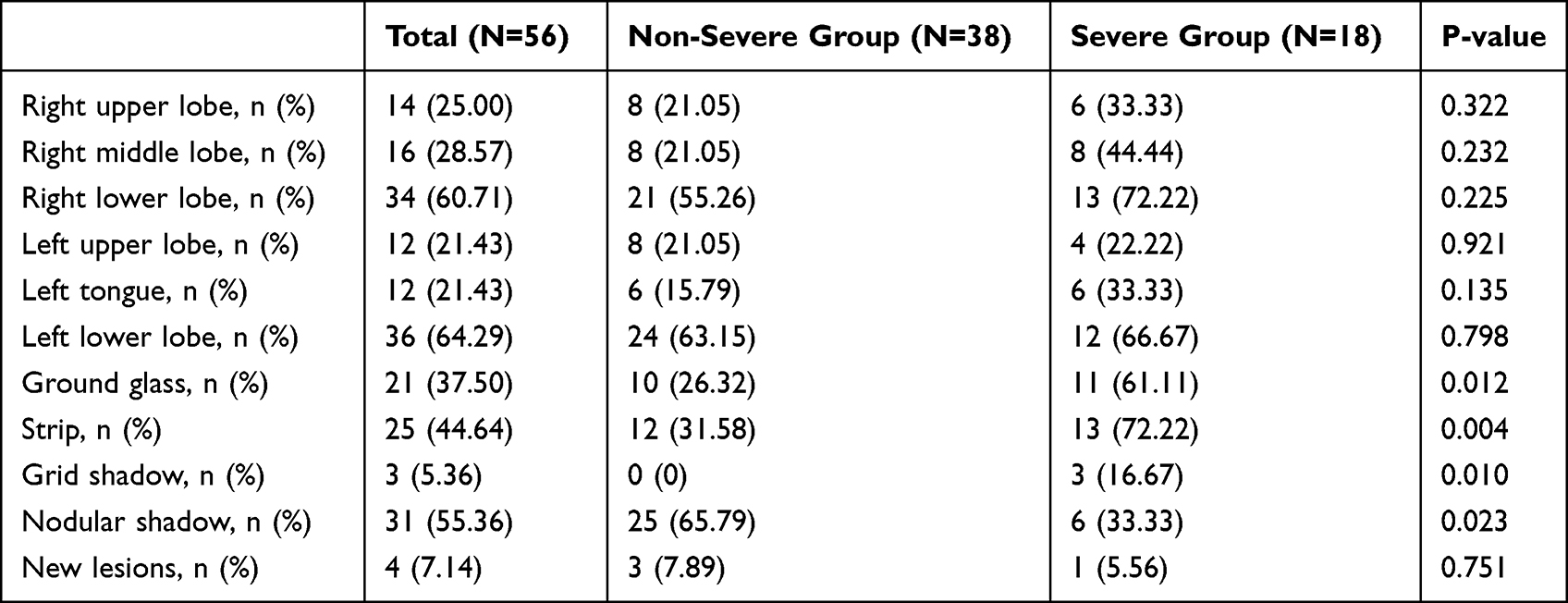 |
Table 6 Different Performances of Chest CT with Different Groups |
Discussion
The present study recruited 64 convalescent COVID-19 patients within 6 to 9 months of discharge. The positive rate of SARS-CoV-2 IgG was 73.21% (41/56). Twenty-three patients (35.94%) had diffusion dysfunction within 6 to 9 months of discharge. More than half of severe patients (56.50%, 13/23) have impaired diffusion function. Chest CT often occurs in lower lungs, among which the patients are mainly manifested as ground glass and strip in the severe convalescent patients.
Long-term follow-up studies for patients recovering from atypical infectious pneumonia (SARS and MERS) indicate that impaired pulmonary function may last for months or even years.22 SARS survivors’ exercise capacity and health status at 6 months are significantly lower than the standard.23 The changes in pulmonary fibrosis caused by SARS mainly occur in severe patients. When evaluating SARS pulmonary fibrosis, the dynamic DLCO score is more sensitive than HRCT.24 SARS survivors’ two-year follow-up results show significant defects in DLCO, athletic ability, and health status (6 minute walking test and 36 simple health adjustments).22 During the 1-year follow-up with MERS coronavirus infection, patients with severe pneumonia suffered more lung function damage than those without pneumonia or mild pneumonia. Severe pneumonia severely damaged pulmonary function and caused long-term radiation sequelae in MERS.25 There are varying degrees of decline in pulmonary function and reduced activity endurance with SARS and MERS who are followed up. It is related to the degree of pneumonia infected. Similarly, in our study, the pulmonary function is decreased in severe convalescent COVID-19 patients.
Most survivors of COVID-19 have abnormal diffusion function six weeks after discharge.26 There are 71.7% of patients who had significantly impaired DLCO (<80%), and 25% of patients who had severely impaired DLCO (<60% predictive value). Abnormal DLCO indicates pulmonary fibrosis or recovery late in the process. There is a significant correlation between the decline of DLCO and pneumonia severity. Two studies of the 3-month follow-up observed that 25% had a mainly abnormal DLCO pulmonary function.13,27 The severity of diffusion dysfunction also indicates that COVID-19 is more likely to be related to diffuse lung epithelial injury and small airway congestion.27 The pulmonary function of most patients was improved 3 months after clinical cure and discharge, and some patients remained with mild-to-moderate diffusion and small airway dysfunction.8 SARS-CoV-2 patients have gas-blood exchange barriers. There are 4–6 months follow-up studies pointed out that 22% to 56% had abnormal pulmonary diffusion function.14,28 DLCO% pred is the most critical factor related to the severity of COVID-19. DLCO has a more significant decline than DLCO/VA (carbon monoxide diffusing capacity corrected for alveolar volume), which indicates that the reduced lung volume and diffusion function may be more likely to cause pulmonary dysfunction. About one-third of patients have an abnormal residual pulmonary function and low DLCO in 12-month follow-up. The low DLCO may be caused by abnormal pulmonary interstitial or pulmonary vascular abnormalities.15
A 1-year cohort study showed that age, gender, and requiring HFNC (High Flow Nasal Cannula), NIV (Non-Invasive Ventilation), or IMV (Invasive Mechanical Ventilation) were positively associated with diffusion impairment, especially in females. However, there was no significant association between corticosteroid therapy and intravenous immunoglobulin therapy with diffusion impairment.16 The impaired diffusion capacity was more severe and recovered slower in females than in males.29 In the present study, females and smoking had more risk factors for diffusion impairment. Age correlated with impaired diffusion in severe patients. However, there was a small sample size. DLCO remains a complex lung function measurement, with emphysema, pulmonary vascular disease, and interstitial lung disease that contribute to DLCO impairment.9 The incidence of diffusion dysfunction was 47.2% to 54%, while the severe patients was 54% to 84.2%.27 The incidence of diffusion dysfunction in this study was lower than that in previous studies but consistent with the severe group. Most of the studies were conducted for 3 to 6 months of follow-up time. The pulmonary function of COVID-19 has not been recovered, while the lung function of severe patients has been damaged for a long time.
The most common chest CT findings of COVID-19 are bilateral ground-glass shadows with subpleural distribution and no pleural effusion. The CT range of symptoms progressed abnormally rapidly after the onset of symptoms, reaching a peak around 6 to 11 days, and then the abnormalities continued to be high. The temporal changes of various CT manifestations follow a specific pattern, which may indicate the progression and recovery of the disease.30 More than 80% of patients infected with SARS-CoV-2 have found varying degrees of lung damage on chest CT.30,31 SARS-CoV-2 affects extensive damage to alveolar epithelial and endothelial cells. The formation of serous fluid, fibrin exudation, and hyaline membrane formation in the alveolar cavity. The edema of the pulmonary interstitial, and the infiltration of inflammatory cells in the pulmonary interstitium with lymphocytes, lead to pulmonary interstitial fibrosis finally.32 About 24% of patients did not completely disappear after 6 to 9 months of discharge, with interstitial thickening and grid-like changes. Lung lesions in recovery patients are inconsistent with the degree of damage to the pulmonary diffusion function. Although HRCT scans did not clearly show the development of pulmonary fibrosis or progressive pulmonary interstitial changes, it required long-term dynamic monitoring of chest imaging.15 This study also found that more leftover lesions do not mean abnormal lung diffusion is more likely to occur. Therefore, SARS-CoV-2 infection leads to long-term lung disease. The mechanism of diffusion dysfunction remains to be further studied. It also suggests that no matter the chest CT, follow-up is intimately required for pulmonary diffusion function.
Multi-organ functional damage caused by SARS-CoV-2.33–35 D-dimer is an independent predictor of inpatient death in COVID-19 patients admitted to the hospital. Also, the D-dimer level is an important prognostic factor of the DLCO abnormality.25 The activity of the α-HBDH (α-Hydroxybutyrate dehydrogenase) in the heart is more than half of the total enzyme activity, so it is used to assess heart damage in clinical practice. COVID-19 could cause damage to the heart, α-HBDH may reflect the changes of disease more sensitively than LDH (Lactic dehydrogenase) in COVID-19 patients.36 In this study, we find that SARS-Cov-2 infection possibly did not affect the liver, kidney, and coagulation function in the convalescent patients. Though, the counts of lymphocytes were statistically different in the two groups. T cells from convalescent patients displayed continued alterations with the persistence of a cytotoxic program.37 However, there is no statistical baseline level for patients. It is impossible to evaluate the effect of counts of lymphocyte counts in COVID-19 recovery.
The positive rate of SARS-CoV IgG after 2 years of follow-up is 90%.38 In most COVID-19 patients, the SARS-Cov-2 IgG antibody in the serum and saliva is maintained at least 3 months after the onset. The positive rate of SARS-Cov-2 IgG titer is 70% in one year in Wuhan.39,40 A 12-month longitudinal study showed that the positive rate of SARS-Cov-2 IgG spike protein receptor-binding domain (RBD-IgG) exceeds 70% in the donors’ serum during the recovery period of COVID-19. The titer of RBD-IgG decreased with time and stabilized at 35.7% in the ninth month.39 At the same time, the SARS-CoV-2 IgG antibody disappeared in some patients.27 SARS-CoV-2 IgM disappears 4 to 6 weeks after the onset, and the degree of antibody level reduction is about 46%, mild or severe in patients. The SARS-CoV-2 antibodies may disappear within 18 months, which indicates the necessity of vaccination.41 Ten cases (17.8%) of SARS-CoV-2 IgM are positive, while the new coronavirus nucleic acid is negative. The reason is that coronaviruses causes other common respiratory infections and induces antibodies that cross-react with COVID-19.42 Therefore, the positive rate of SARS-CoV-2 IgM in the recovery period cannot represent a positive recurrence of nucleic acid.
This study has several limitations: most of the baseline data for lung function tests was unavailable because the test functions are limited or prohibited during the initial outbreak. Only a small number of patients suffer from chronic respiratory diseases; presumably, it is acceptable that the essential pulmonary function in most patients is expected. This cross-sectional analysis only provides short-term follow-up, and we should explore the long-term dynamic changes in pulmonary function in convalescent COVID-19 patients in the future study. Since the small sample size limits our research, we need to continue to expand the sample size in the future research.
Conclusion
About 72.22% of severe convalescent COVID-19 patients were still positive for SARS-CoV-2 IgG. About 56.52% of patients had abnormal diffusion function, and 61.11% had ground glass chest CT in the 6–9-month follow-up. Age correlated with impaired diffusion in severe patients. Pulmonary function tests should be considered in recovered COVID-19 patients during the follow-up, particularly in severe patients.
Ethical Approval
This study was approved by the Committee of Ethics at Beijing Ditan Hospital, Capital Medical University [No. JDLKZ (2020) D (042)-02] with informed consent. The study was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We thank the patients for their participation in this study and the doctors and nurses at Beijing Ditan Hospital, who cared for the patients, and provided the logistic support for the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; they took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is partially supported by Beijing Municipal Science and Technology Project (No. Z201100007920017).
Disclosure
We, the author of the submitted manuscript, declare that we do not have a commercial or other association that might pose a conflict of interest (eg, pharmaceutical stock ownership, consultancy, advisory board membership, relevant patents, or research funding).
References
1. Sigfrid L, Cevik M, Jesudason E, et al. What is the recovery rate and risk of long-term consequences following a diagnosis of COVID-19? A harmonised, global longitudinal observational study. BMJ Open. 2021;11:e043887. doi:10.1101/2020.08.26.20180950
2. Lopez-Leon S, Wegman-Ostrosky T, Perelman C, et al. More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. medRxiv. 2021. doi:10.1101/2021.01.27.21250617
3. Cheung OY, Chan JWM, Ng CK, Koo CK. The spectrum of pathological changes in severe acute respiratory syndrome (SARS). Histopathology. 2004;45(2):119–124. doi:10.1111/j.1365-2559.2004.01926.x
4. Lindsay McDonald T. Healing after COVID-19: are survivors at risk for pulmonary fibrosis? Am J Physiol Lung Cell Mol Physiol. 2021;320(2):L257–L265. doi:10.1152/ajplung.00238.2020
5. Wang F, Kream RM, Stefano GB. Long-term respiratory and neurological sequelae of COVID-19. Medical science monitor. Int J Clin Exp Med. 2020;26:e928996. doi:10.12659/MSM.928996
6. Zhao X, Nicholls JM, Chen YG. Severe acute respiratory syndrome-associated coronavirus nucleocapsid protein interacts with Smad3 and modulates transforming growth factor-β signaling. J Biol Chem. 2008;283(6):3272–3280. doi:10.1074/jbc.M7080.33200
7. Lal SK. Molecular biology of the SARS-coronavirus. Springer. 2010;1–328. doi:10.1007/978-3-642-03683-5
8. Lingyan Y, Yao G, Lin S, et al. The investigation of pulmonary function changes of COVID-19 patients in three months. J Healthc Eng. 2022;2022:9028835. doi:10.1155/2022/9028835
9. Long QY, Li JW, Hu XY, et al.Follow-ups on persistent symptoms and pulmonary function among post-acute COVID-19 patients: a systematic review and meta-analysis. Front med. 2021;8:702635. doi:10.3389/fmed.2021.702635
10. Balasubramanian A, MacIntyre NR, Henderson RJ, et al. Diffusing capacity of carbon monoxide in the assessment of COPD. Chest. 2019;156:1111–1119. doi:10.1016/j.chest.2019.06.035
11. Gattinoni L, Marini JJ, Busana M, et al. Spontaneous breathing, transpulmonary pressure and mathematical trickery. Ann Intensive Care. 2020;10(1):1–2. doi:10.1186/s13613-020-00708-1
12. Tobin MJ, Laghi F, Jubran A. Caution about early intubation and mechanical ventilation in COVID-19. Ann Intensive Care. 2020;10(1):4–6. doi:10.1186/s13613-020-00692-6
13. Lerum TV, Aaløkken TM, Bronstad E, et al. Dyspnoea, lung function and CT findings 3 months after hospital admission for COVID-19. Eur Res J. 2021;57(4). doi:10.1183/13993003.03448-2020
14. Huang C, Huang L, Wang Y, et al. 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet. 2021;397(10270):220–232. doi:10.1016/S0140-6736(20)32656-8
15. Xiaojun W, Liu X, Zhou Y, et al. 3-month, 6-month, 9-month, and 12-month respiratory outcomes in patients following COVID-19-related hospitalisation: a prospective study. Lancet Res Med. 2021;9(7):747–754. doi:10.1016/S2213-2600(21)00174-0
16. Huang L, Yao Q, Xiaoying G, et al. 1-year outcomes in hospital survivors with COVID-19: a longitudinal cohort study. Lancet. 2021;398(10302):747–758. doi:10.1016/S0140-6736(21)01755-4
17. Zhi H, Xiaolong J, Zhao Z, et al. Risk factors for impaired pulmonary diffusion function in convalescent COVID-19 patients: a systematic review and meta-analysis. E Clin Med. 2022;49:101473. doi:10.1016/j.eclinm.2022.101473
18. Clinical management of severe acute respiratory infection when COVID-19 is suspected. World Health Organization; 2020. Available from: https://www.who.int/publications-detail/clinical-management-of-severe-acute-respiratory-infection-when-novel-coronavirus-(ncov)-infection-is- suspected.
19. General Office of National Health Commission of the People’s Republic of China. Office of National Administration of Traditional Chinese Medicine. Diagnosis and treatment of coronavirus disease-19 (8th trial edition). China Med. 2020;15(10):1494–1499. Chinese.
20. Meiling J, Yuanlin S, Jinping Z, et al. Guideline for pulmonary function testing in primary care (2018). Chinese J Gen Pract. 2019;18(6):511–518.
21. Graham BL, Steenbruggen I, Miller MR, et al. Standardization of spirometry 2019 update. An official American Thoracic Society and European Respiratory Society Technical Statement. Am J Respir Crit Care Med. 2019;200(8):e70–88. doi:10.1164/rccm.201908-1590ST
22. Ngai JC, Ko FW, Ng SS, To KW, Tong M, Hui DS. The long-term impact of severe acute respiratory syndrome on pulmonary function, exercise capacity, and health status. Respirology. 2010;15(3):543–550. doi:10.1111/j.1440-1843.2010.01720.x
23. Hui DS, Joynt GM, Wong KT, et al. Impact of severe acute respiratory syndrome (SARS) on pulmonary function, functional capacity and quality of life in a cohort of survivors. Thorax. 2005;60(5):401–409. doi:10.1136/thx.2004.030205
24. Xie L, Liu Y, Xiao Y, et al. Follow-up study on pulmonary function and lung radiographic changes in rehabilitating severe acute respiratory syndrome patients after discharge. Chest. 2005;127(6):2119–2124. doi:10.1378/chest.127.6.2119
25. Park WB, Jun KI, Kim G, et al. Correlation between pneumonia severity and pulmonary complications in middle east respiratory syndrome. J Korean Med Sci. 2018;33(24):e169. doi:10.3346/jkms.2018.33.e169
26. Der Brugge SS, Stalman L, Winter B, et al. Pulmonary function and health-related quality of life after COVID-19 pneumonia. Respir Med. 2021;176:106272. doi:10.1016/j.rmed.2020.106272
27. Xiaoneng M, Jian W, Zhuquan S, et al. Abnormal pulmonary function in COVID-19 patients at time of hospital discharge. Eur Respir J. 2020;55(6). doi:10.1183/13993003.01217-2020
28. Guler SA, Ebner L, Aubry-Beigelman C, et al. Pulmonary function and radiological features 4 months after COVID-19: first results from the national prospective observational Swiss COVID-19 lung study. Eur Respir J. 2021;57(4). doi:10.1183/13993003.03690-2020
29. Chen M, Liu J, Peng P, et al. Dynamic changes of pulmonary diffusion capacity in survivors of non-critical COVID-19 during the first six months. E Clin Med. 2022;43:101255. doi:10.1016/j.eclinm.2021.101255
30. Wang Y, Dong C, Hu Y, et al. Temporal changes of CT findings in 90 patients with COVID-19 pneumonia: a longitudinal study. Radiology. 2020;296(2):E55–E64. doi:10.1148/radiol.2020200843
31. Dai H, Zhang X, Xia J, et al. High-resolution chest CT features and clinical characteristics of patients infected with COVID-19 in Jiangsu, China. Int J Infect Dis. 2020;95:106–112. doi:10.1016/j.ijid.2020.04.003
32. Zhe X, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Res Med. 2020;8(4):420–422. doi:10.1016/S2213-2600(20)30076-X
33. Zhao Y, Shang Y, Song W-B, et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. E Clin Med. 2020;25:100463. doi:10.1016/j.eclinm.2020.100463
34. Zheng Z, Peng F, Buyun X, et al. Risk factors of critical & mortal COVID-19 cases: a systematic literature review and meta-analysis. J Infect. 2020;81(2):e16–e25. doi:10.1016/j.jinf.2020.04.021
35. Zhang J, Wang X, Jia X, et al. Risk factors for disease severity, unimprovement, and mortality in COVID-19 patients in Wuhan, China. Clin Microbiol Infect. 2020;26(6):767–772. doi:10.1016/j.cmi.2020.04.012
36. Zhu H, Gaojing Q, Hui Y, et al. Features of α-HBDH in COVID-19 patients: a cohort study. J Clin Lab Anal. 2021;35(1):e23690. doi:10.1002/jcla.23690
37. Shuwa HA, Shaw TN, Knight SB, et al. Alterations in T and B cell function persist in convalescent COVID-19 patients. Med. 2021;2(6):720–735.e4. doi:10.1016/j.medj.2021.03.013
38. Yan H, Tan Y, Zhuang H, et al. A follow up study of total IgM, IgG, nucleoprotein and spike protein antibodies against severe acute respiratory syndrome (SARS) coronavirus in patients with SARS. Zhonghua Jiehe Zazhi. 2006;45(11):896–899.
39. Cesheng L, Ding Y, Xiao W, et al. Twelve-month specific IgG response to SARS-CoV-2 receptor-binding domain among COVID-19 convalescent plasma donors in Wuhan. Nat Commun. 2021;12(1):4144. doi:10.1038/s41467-021-24230-5
40. Isho B, Abe KT, Zuo M, et al. Persistence of serum and saliva antibody responses to SARS-CoV-2 spike antigens in COVID-19 patients. Sci Immunol. 2020;5(52). doi:10.1126/sciimmunol.abe5511
41. Zhang X, Suwen L, Hui L, et al. Viral and antibody kinetics of COVID-19 patients with different disease severities in acute and convalescent phases: a 6-month follow-up study. Virol Sin. 2020;35(6):820–829. doi:10.1007/s12250-020-00329-9
42. Jackson Turner S, Jane A, Kalaidina E, et al. SARS-CoV-2 mRNA vaccines induce persistent human germinal center responses. Nature. 2021;596(7870):109–113. doi:10.1038/s41586-021-03738-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Association Between Artificial Intelligence Based Chest Computed Tomography and Clinical/Laboratory Characteristics with Severity and Mortality in COVID-19 Hospitalized Patients
Ye J, Huang Y, Chu C, Li J, Liu G, Li W, Gao C
Journal of Inflammation Research 2024, 17:2977-2989
Published Date: 14 May 2024