Back to Journals » Infection and Drug Resistance » Volume 17
Assessment of Knowledge and Practice of Healthcare Providers in Saudi Arabia Regarding Clostridioides difficile Infection Diagnosis and Management: A Cross-Sectional Questionnaire-Based Study
Authors Almutairi MS ![]() , Alnezary FS, Alsuwaylim RO
, Alnezary FS, Alsuwaylim RO ![]() , Alsulaymi I, Almohammed OA
, Alsulaymi I, Almohammed OA ![]() , Thabit AK
, Thabit AK ![]()
Received 27 November 2023
Accepted for publication 7 February 2024
Published 14 February 2024 Volume 2024:17 Pages 583—594
DOI https://doi.org/10.2147/IDR.S450281
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Masaad Saeed Almutairi,1 Faris S Alnezary,2 Rasil O Alsuwaylim,1 Ibrahim Alsulaymi,1 Omar A Almohammed,3,4 Abrar K Thabit5
1Department of Pharmacy Practice, College of Pharmacy, Qassim University, Qassim, Saudi Arabia; 2Department of Pharmacy Practice, College of Pharmacy, Taibah University, Madinah, Saudi Arabia; 3Department of Clinical Pharmacy, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia; 4Pharmacoeconomics Research Unit, College of Pharmacy, King Saud University, Riyadh, Saudi Arabia; 5Pharmacy Practice Department, Faculty of Pharmacy, King Abdulaziz University, Jeddah, Saudi Arabia
Correspondence: Masaad Saeed Almutairi, Department of Pharmacy Practice, College of Pharmacy, Qassim University, Qassim, 51452, Saudi Arabia, Tel +966557523133, Email [email protected]
Introduction: Diagnosis of Clostridioides difficile infection (CDI) depends on clinical presentation and laboratory testing. Stool diagnostic tests are essential for effective detection of toxigenic C. difficile strains. No study to date has evaluated the readability of microbiology labs in Saudi Arabia to test for CDI and evaluated the knowledge and practice of healthcare providers regarding CDI management. Therefore, this study aimed to assess the knowledge and practice of healthcare providers in Saudi Arabia regarding CDI diagnosis and treatment.
Methods: A cross-sectional, descriptive, questionnaire-based study was conducted on healthcare providers in Saudi Arabia, primarily physicians and clinical pharmacists. The questionnaire was developed based on a literature review and input from infectious diseases experts. The questionnaire was administered online. Data were analyzed using descriptive and inferential statistics.
Results: Of 183 respondents, 27.9% had adequate knowledge on CDI diagnosis and management. The majority were internal medicine specialists (37.7%) working in governmental or semi-governmental hospitals (80.9%) in central (46.6%) or southern (30.1%) regions of Saudi Arabia. Most participants assessed laxative use (86.3%) and reported positive C. difficile specimens to infection control (67.2%). However, knowledge varied, with 57.4% supporting unnecessary retesting and 53% assuming positive PCR test indicates moderate CDI probability. Factors such as specialization, hospital accreditation status, and bed capacity influenced knowledge levels (p< 0.01 for all factors).
Conclusion: The study revealed a significant knowledge gap among Saudi healthcare providers regarding CDI diagnosis, management, and severity classification, highlighting the need for improved education and adherence to guidelines to improve patient outcomes and reduce recurrence risks.
Keywords: Clostridioides difficile, Clostridium difficile, diagnosis, polymerase chain reaction, knowledge, Saudi Arabia
Introduction
Clostridioides difficile infection (CDI) is caused by the toxigenicity of C. difficile, an anaerobic gram-positive bacterium. The spore-forming ability of C. difficile enables it to survive in unfavorable conditions, thus contributing to its dissemination and transmission in healthcare settings and occasionally in the community.1 Patients with CDI often have a history of recent antibiotic use, hospitalization, chronic diseases, or previous CDI episodes. Antibiotic treatment within the preceding 60 days, especially with third generation cephalosporins, penicillins with beta-lactamase inhibitors, chronic liver or kidney disease, malnutrition, and prior CDI are associated with an elevated risk of CDI.2 In a study conducted among hospitalized patients with inflammatory bowel disease, CDI was frequently associated with active inflammatory bowel disease. Furthermore, the prior intake of nonsteroidal anti-inflammatory medications was identified as a risk factor for CDI among these patients.3
The diagnosis of CDI is based on clinical signs and symptoms such as new onset diarrhea (≥3 loose stools in 24 hours), fever, abdominal pain, or leukocytosis.4 Moreover, CDI diagnosis can be determined by laboratory stool diagnostic tests. A polymerase chain reaction (PCR) or a multistep algorithm is recommended to effectively detect toxigenic C. difficile strains to facilitate the diagnosis of symptomatic CDI and minimize over-diagnosis of asymptomatic carriers.5 The Infectious Disease Society of America (IDSA) recommend using either PCR or a multistep algorithm, either glutamate dehydrogenase (GDH) and toxin, GDH and toxin then arbitrated by NAAT, or NAAT and toxin.6
Between 2009–2011, reported CDI incidence was 50–90 cases per 100,000 population in Europe, Canada, and the US. However, by 2017 incidence had risen to 145 cases per 100,000 population.7 In a tertiary care facility in Riyadh, Saudi Arabia, the incidence rate of CDI was 3.5 per 10,000 patient days, with a total of 106 episodes of CDI observed among 59 patients over a span of 137,230 patient-days.8 In another tertiary academic medical center in Saudi Arabia, among 170 patients included in the analysis, 10-year cumulative incidence of CDI was 8.4%.9
During the period from 2015 to 2019, a survey conducted in Slovakia revealed that 83.3% of clinicians reported requesting diagnostic testing for CDI both at the initiation and completion of CDI treatment.10 Another survey was conducted among 171 residents and faculty members at the University of New Mexico Health Sciences Center, with a significant proportion of respondents belonging to the internal medicine department. The survey encompassed a range of questions covering infection control knowledge and testing. The majority of participants (81%) indicated a preference for implementing contact precautions when isolating inpatients with new-onset diarrhea and a negative C. difficile test. Furthermore, 91% of respondents selected EIA for toxins A and B as the current laboratory test performed.11
Surveys of clinical laboratories found that EIA for toxin A and B was the primary assay for CDI diagnosis in 60–67% in Australia, New Zealand, and Spain.12,13 However, only one-third of laboratories had specific criteria, such as watery stool or history of antibiotic intake, for stool sample collection for CDI diagnosis.13 Additionally, a survey conducted in Korea, which encompassed 66 laboratories, revealed that the most widely utilized test for CDI was the EIA for toxin A and B. Out of the 66 laboratories, 51 of them employed this test either independently or in conjunction with other diagnostic methods. On the other hand, a combination of NAAT and C. difficile culture tests, either alone or in conjunction with other tests, was employed by 37 laboratories.14
In light of the limited available data in Saudi Arabia regarding utilized CDI diagnostics and the practice of CDI diagnosis and management by healthcare providers, we sought to conduct an evaluative study to address this gap. Therefore, the objective of this study was to evaluate the knowledge and practices pertaining to CDI diagnosis and treatment among healthcare providers in Saudi Arabia; thus, we aim to enhance our understanding of CDI management in the Saudi healthcare setting.
Materials and Methods
Study Design and Population
A cross sectional, descriptive, questionnaire-based study was conducted. The population were healthcare providers, physicians and clinical pharmacists, practicing in Saudi Arabia. The survey was administered from November 2021 to July 2022. Approval for the study protocol was obtained from the Regional Research Ethics Committee, Qassim region, Saudi Arabia (Approval number 1443–441,172).
Questionnaire Development
The questionnaire was developed based on a review of existing literature on healthcare providers’ knowledge and practices related to CDI diagnosis and treatment.11,15 The initial questionnaire draft was reviewed by three infectious disease experts to obtain their feedback on the layout and content. A pilot study on five participants was then conducted to evaluate the clarity and suitability of the questionnaire. All expert comments and edits from the pilot study were incorporated into the final version before distributing the questionnaire more broadly.
The questionnaire consisted of three sections. The first collected demographic data. The second section included questions assessing participants’ practices related to CDI diagnosis. The third section contained 11 knowledge-based items, with one point given for each correct answer and zero points for incorrect answers. Participants were considered to have adequate knowledge if they correctly answered at least 70% of these knowledge items; the 70% cutoff for adequate response was based on previous studies assessing the level of knowledge among healthcare workers.16,17
Administration of the Questionnaire
The questionnaire was converted into a web-based format using the online Google Forms platform. Informed consent was obtained and it was on the first page of the survey where it contained an informed consent statement, where participants were asked for their willingness and consent to participate. The questionnaire link was distributed to healthcare providers practicing in Saudi Arabia through the Saudi Commission for Health Specialties (SCFHS), which has a database of all registered healthcare providers in Saudi Arabia. An initial email was sent by the SCFHS, followed by a reminder email one month later.
Data Analysis
The questionnaire data were analyzed using SAS software (version 9.4; SAS Institute Inc., Cary, NC, USA). Descriptive statistics including frequencies and percentages were used to summarize participants’ knowledge and practices related to CDI diagnosis and management. Inferential statistics, specifically Chi-square test, was utilized to analyze differences in knowledge levels between participant groups.
Results
A total of 183 participants completed the survey. Table 1 shows the demographics of the participants. The most common specialties were internal medicine specialists (n=69; 37.7%), followed by infectious disease specialists (n=27; 14.8%), other medical specialists (n=31; 16.9%), and clinical pharmacists (n=23; 12.6%). Approximately half of participants (n=92; 50.3%) had 10 years of experience or less. In terms of location, the largest proportion were from the central region of Saudi Arabia (n=85; 46.6%), followed by the southern region (n=55; 30.1%).
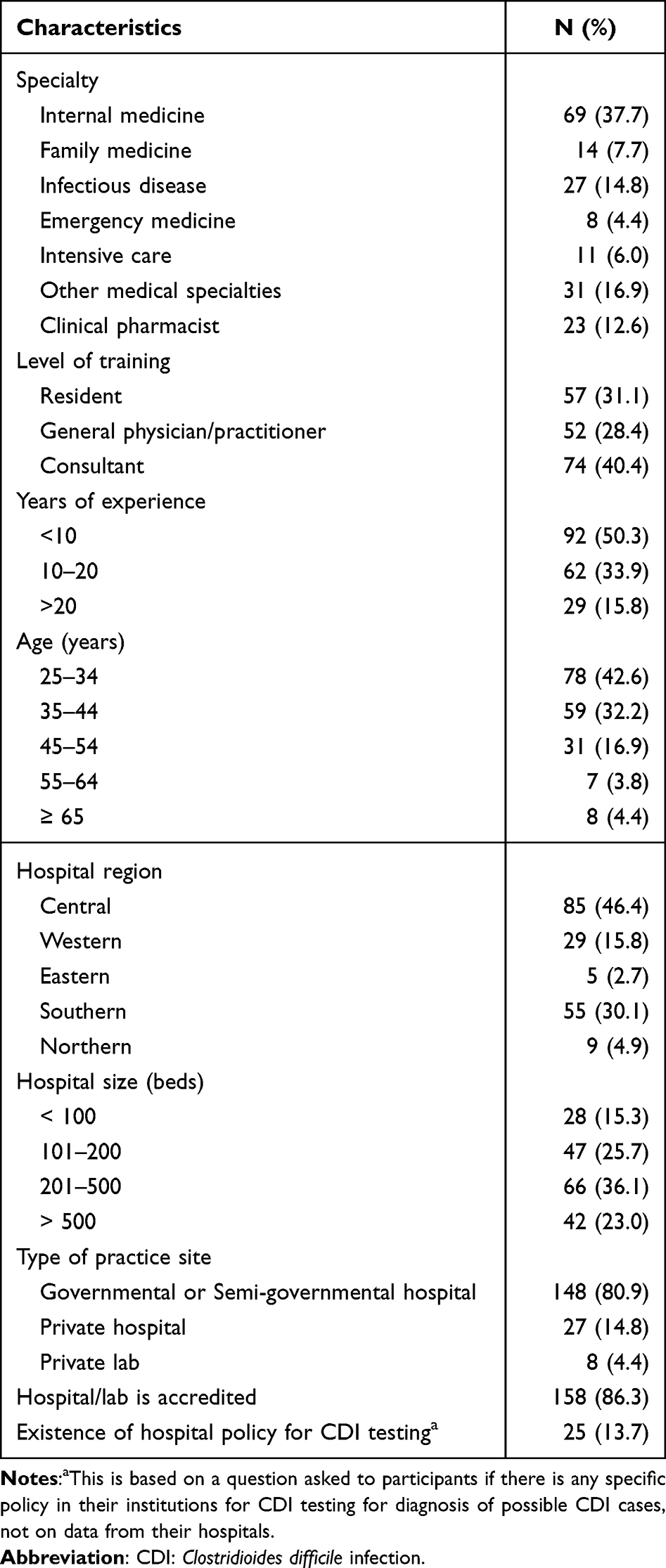 |
Table 1 Survey Demographics |
Regarding CDI diagnosis practices, most of the participants (n=158; 86.3%) reported inspecting laxative use history before ordering C. difficile testing. Half of participants selected at least one risk factor that would prompt CDI stool testing, while 36 (19.7%) correctly chose three triggering factors. Participants’ responses varied regarding the type of CDI diagnostic tests used at their institutions as shown in Table 2.
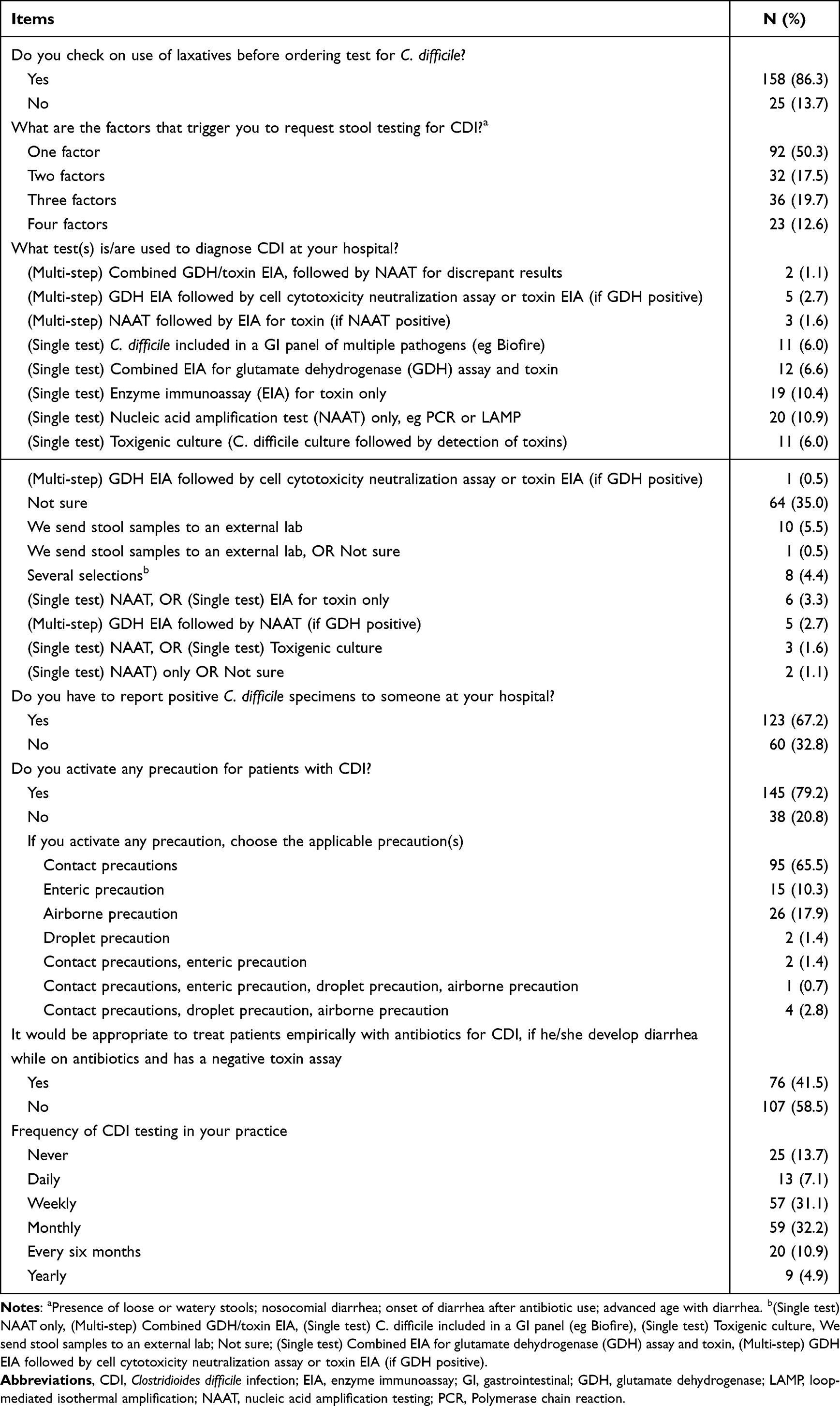 |
Table 2 Participants Responses to the Practice Items |
When specifically asked about the diagnostic tests used at their institution, 20 (10.9%) reported using NAAT only, whereas 19 (10.4%) reported using EIA for toxin only. Conversely, 64 (35.0%) were unsure of the test used for CDI diagnosis at their institution. Over half of participants (n=123, 67.2%) stated that positive C. difficile specimens were reported to the infection control department with 95 participants (65.5%) reported activating contact precautions for CDI patients. Interestingly, 76 participants (41.5%) indicated they would empirically treat patients for CDI despite negative toxin assay results. The remainder of the questionnaire items related to CDI diagnosis and management are summarized in Table 2.
Regarding the knowledge-based questions which are shown in Table 3, approximately half of participants (n=105, 57.4%) indicated that retesting at the end of CDI therapy is unnecessary. Moreover, 97 participants (53%) agreed that a positive PCR test indicates a moderate probability of CDI. The vast majority (n=165; 90.2%) correctly selected diarrhea with ≥3 episodes in 24 hours as a trigger for ordering CDI testing. Knowledge on CDI classification and risk factors showed some variability, where only 17 participants (9.3%) correctly selected four CDI classification factors, while 41 (22.4%) chose three factors, 55 (30.1%) chose two factors, and 48 (26.2%) chose one factor. For CDI risk factors, 91 participants (49.7%) correctly selected four or more, while 38 (20.8%) selected three correct risk factors. Regarding knowledge of antibiotics to discourage in patients with CDI risk factors, 52 (28.4%) selected one correctly, 50 (27.3%) selected two, 39 (21.3%) selected three, and 28 (15.3%) selected four. However, 14 (7.7%) selected incorrect options. Regarding CDI treatment, 119 participants (65%) supported using different treatment options based on CDI severity. The rates of choosing correct answers for the selection of antibiotic therapy for CDI varied based on the different severity classifications of CDI (Table 3). Regarding antibiotic treatment duration, 84 participants (45.9%) correctly selected “10 days” based on guidelines.
 |
Table 3 Participants’ Responses to the Knowledge Items |
Overall, 51 participants (27.9%) demonstrated adequate knowledge (>70% correct answers, while 65 (35.5%) had insufficient knowledge (50–69% correct) and 67 (36.6%) had inadequate knowledge (<50% correct). Groups with the highest proportion of adequate knowledge included infectious disease specialists (p<0.01), consultants (p<0.01), those working in hospitals with 201–500 beds (p<0.01) and >500 beds (p<0.01), practitioners in government or semi-government hospitals (p<0.01), and those in accredited hospitals (p<0.01). More details on the distribution and comparison of participants across the three knowledge levels are provided in Table 4.
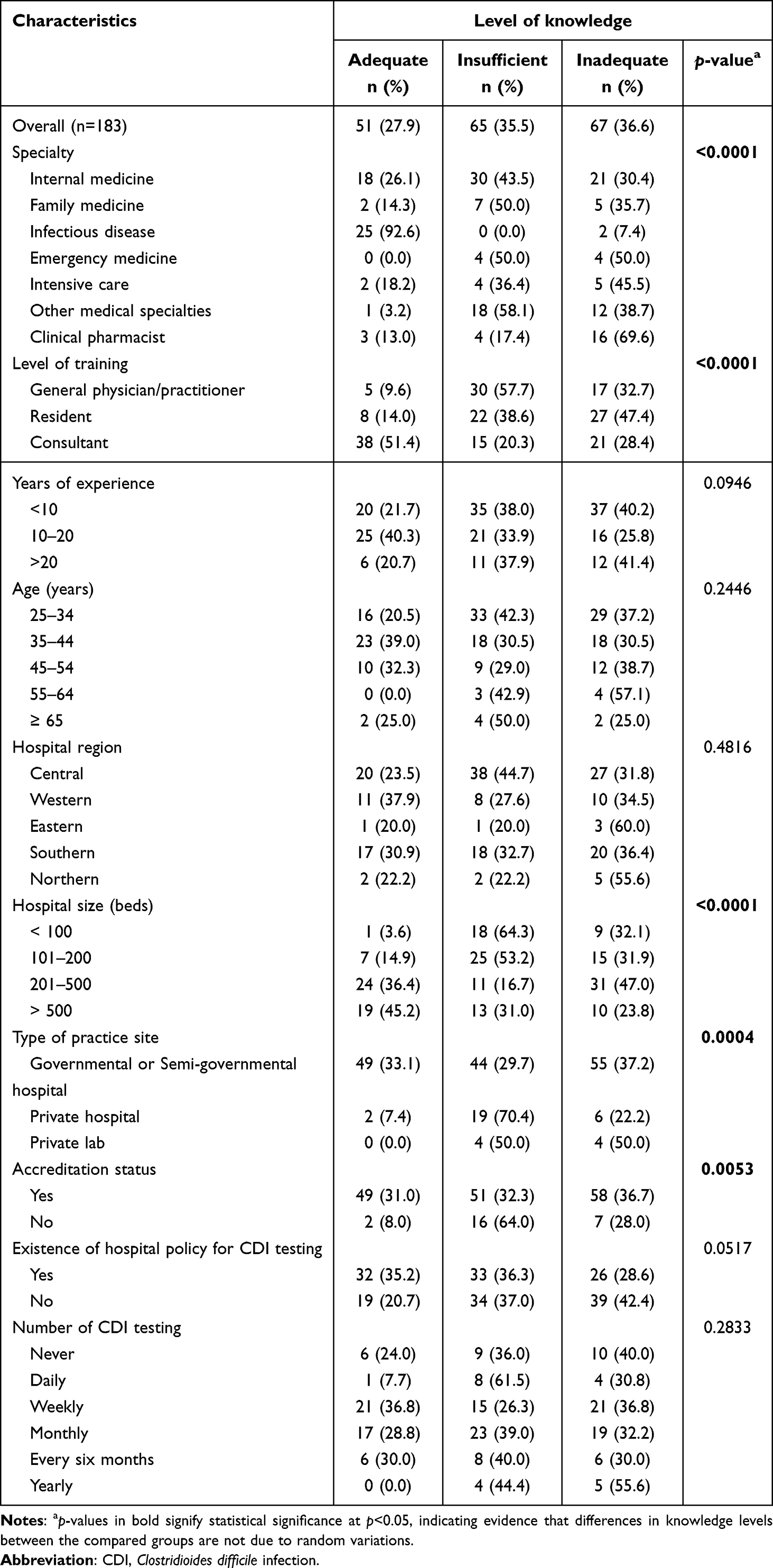 |
Table 4 Distribution and Comparison of Participants Based on the Level of Knowledge |
Discussion
To our knowledge, this is the first study to assess the knowledge and practice related to CDI diagnosis and management among healthcare providers in Saudi Arabia. Overall, the findings indicate that providers’ knowledge levels were suboptimal, with nearly two-thirds demonstrating insufficient or inadequate knowledge on CDI. These results align with a semi-structured interview study in South Africa which found limited CDI knowledge, with a median score of 3 out of 7.18 Compared to previous global studies, the level of CDI knowledge among healthcare providers in Saudi Arabia appears lower. For example, a study by Fayerberg et al in New Mexico, USA found almost half of participants lacked knowledge on CDI diagnosis at their institution. In contrast, nearly two-thirds of participants in our Saudi sample demonstrated insufficient or inadequate CDI knowledge. This indicates a greater knowledge gap in the Saudi context compared to what has been observed in some other regions.
Although the level of training indicates that the level of knowledge depends on the level of training, many of the highly trained staff are still having a concerning insufficient level of knowledge (only 51.4% of consultant had an adequate level of knowledge). However, we need to note that this concerning level of knowledge also depend on the practitioners’ specialty as our results indicate. Similarly, participants practicing in the private sector had a concerning low level of knowledge which indicate that their patients may not be receiving recommended therapy based on the best available evidence. This issue needs further investigation and instantaneous action plan to raise the level of knowledge among practitioners at different level of training and in the private sector to ensure that patients are receiving adequate therapy.
Clinical pharmacists, with their expertise in pharmacotherapy and antimicrobial stewardship, are uniquely positioned to play expanded roles in CDI prevention, detection, and management.19,20 As clinical pharmacists usually assume responsibilities related to appropriate antimicrobial use specially in facilities facing shortage in infectious disease specialists, they need to have adequate level of knowledge about this matter to fulfill this gap. Unfortunately, in our cohort clinical pharmacists demonstrated a concerning level of knowledge related to appropriate CDI diagnostic protocols and evidence-based treatment selections, particularly for severe cases. Thus, targeted educational initiatives focused on addressing the specific gaps identified in this group have potential to significantly enhance clinical pharmacists’ capabilities and empower them to collaborate more actively in institutional CDI stewardship efforts. Formal expansion of pharmacists’ responsibilities through updated policies and physician engagement, paired with closing knowledge gaps through rigorous training, can pave the way for clinical pharmacists to take on more impactful, guideline-concordant functions in tackling CDI.21
The current study revealed knowledge gaps regarding CDI diagnosis among the participants. Furthermore, 64 participants (35%) were unsure of the specific diagnostic test used at their institution. Notably, the most commonly selected response was NAAT only, with just 20 participants (10.4%) identifying this single test approach. According to guidelines, a NAAT alone is insufficient and requires a follow-up toxin test for confirmation. The uncertainty and overreliance on NAAT demonstrated in this sample indicates a need for providers to improve their understanding of appropriate CDI diagnostic methods. Targeted education and training could help address this knowledge gap and promote adherence to recommended testing protocols, which is essential for accurate CDI diagnosis. Alternatively, hospital-specific CDI guidelines can be developed and tailored based on the diagnostics available in the hospital’s microbiology lab. Such guidelines should be uploaded to the hospital’s intranet, and healthcare providers should be made aware of its availability. Consistent with our findings, a study by Aroori et al found that almost half of the participants were unaware of the CDI diagnostic test used at their institution.22 Implementing targeted interventions to increase providers’ familiarity with the recommended diagnostic protocols could help promote early and accurate detection of CDI cases. Furthermore, a study by Fayerberg et al in Mexico with 171 respondents found that nearly half failed to identify the CDI diagnostic test used at their hospital.11 Targeted education for healthcare workers on recommended diagnostic guidelines and the testing methods implemented at their facilities appears needed to address this gap. Increased familiarity with the appropriate use of toxin, molecular, and antigen assays could aid providers in accurate CDI diagnosis and treatment. In contrast, a survey of infectious disease specialists found that most respondents (98%) were aware of their hospital’s CDI diagnostic methods, with 62% using NAAT and 38% using toxin testing.15 The higher knowledge among infectious disease specialists compared to our sample may be attributed to the fact that only 15% of our participants specialized in infectious diseases.
According to the recent IDSA guidelines, CDI testing is recommended for patients with more than three diarrheal episodes within 24 hours.23 In this study, most respondents (90%) correctly answered this criterion for diagnosis and stool sample collection. In contrast, a recent Australian study found that two-thirds of nurses lacked knowledge on CDI identification.24 Our respondents demonstrated variable knowledge on other topics like IDSA severity classification and CDI risk factors. Over half identified at least four accurate risk factors, consistent with the results of a study by Comparcini et al where around half of the participants showed good risk factor knowledge.25 While our sample displayed appropriate awareness of key diagnostic criteria, there appear to be gaps in applying guidelines on CDI classification and risk factors that may be filled by targeted education and training across healthcare professions.
Regarding initial CDI management, almost half of the participants in our study correctly identified at least one appropriate option for non-severe cases (vancomycin or fidaxomicin orally) based on IDSA guidelines. However, only 5 (2.7%) demonstrated adequate knowledge of all suitable initial therapies for severe CDI (vancomycin or fidaxomicin orally, or metronidazole plus vancomycin IV). Still, most respondents (n=165; 90%) recognized at least one appropriate severe CDI treatment. Our study indicates knowledge gaps regarding CDI management, especially for severe CDI, which indicates the need for education on the recommended first-line treatments per guidelines.
A survey from Slovakia found the most commonly used CDI treatments were oral metronidazole (47.8%), oral vancomycin (21.7%), and a combination of oral vancomycin with intravenous metronidazole (17.4%). Fidaxomicin was used by 50% for severe or recurrent CDI.10 However, latest IDSA guidelines that were published after this study was published in 2021 recommend oral vancomycin or fidaxomicin alone as first-line treatment. Standardizing management based on current guidelines can help reduce CDI recurrence and clinical failure. One multicenter study found an 18% CDI clinical failure rate despite treatment.26 Optimizing evidence-based CDI protocols is crucial for improving outcomes and minimizing recurrence and relapse. It should be noted, however, that older IDSA guidelines recommending metronidazole as first-line therapy for non-severe CDI remains active in areas where CDI is not highly prevalent, such as in Saudi Arabia. Several previous studies from Saudi Arabia showed good clinical outcomes and reduced mortality when the older guidelines were followed.9,27
This study has several notable strengths. First, the cross-sectional design enabled collecting data from diverse healthcare providers across Saudi Arabia, allowing a snapshot of current practices and broader generalizability. Second, the rigorous questionnaire development using literature and experts supports data validity and reliability. However, some limitations should be acknowledged. First, self-reported data may introduce recall bias, although the online format improved efficiency and representativeness. Instructions and prompts also minimized errors. Second, self-reports may not fully reflect actual behavior or knowledge but remain a commonly accepted method for assessing perceptions. In addition, anonymity likely reduced social desirability biases. Third, the sample is primarily internal medicine specialists in government hospitals, which may limit generalizability. In addition, more residents and general practitioners were included in the study as they were more accessible and responsive to the participation invitation than senior practitioners in the workforce. Nonetheless, this provides valuable context-specific insights that can inform future research with more diverse samples. More research is needed to further understand the factors contributing to this knowledge deficiency and inform future educational and quality improvement interventions aimed at enhancing providers’ CDI competency in Saudi Arabia.
Conclusion
This study has highlighted notable gaps in the knowledge and management of CDI among healthcare providers in Saudi Arabia. The lack of comprehensive understanding, especially when compared to other global regions, underscores the urgent need for targeted educational interventions, as well as development of hospital-specific guidelines that should be adhered to. These interventions should focus on enhancing familiarity with recommended diagnostic protocols, understanding of IDSA classification, awareness of risk factors, and the ability to apply severity-based treatment. While the study does have some limitations, its findings are credible and significant, emphasizing a pressing requirement for action. Future research should focus on developing and implementing educational strategies tailored to address these identified deficiencies, with the ultimate aim of improving patient outcomes.
Statement of Ethics
This study protocol was reviewed and approved by the Regional Research Ethics Committee, Qassim region, Saudi Arabia (Approval number 1443-441172).
Acknowledgment
The authors extend their appreciation to the Deputyship for Research and Innovation, Ministry of Education in Saudi Arabia, for funding this research through project no. (IFKSUOR3–101–4).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The author (OAA) received funding from the Deputyship for Research and Innovation, Ministry of Education in Saudi Arabia through project no. (IFKSUOR3– 101–4), to support the publication of this manuscript. The funding agency plays no role in designing the study, conducting the analysis, interpreting the data, or writing the manuscript.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Abt MC, McKenney PT, Pamer EG. Clostridium difficile colitis: pathogenesis and host defence. Nat Rev Microbiol. 2016;14(10):609–620. doi:10.1038/nrmicro.2016.108
2. Khanafer N, Vanhems P, Barbut F, et al. Factors associated with clostridium difficile infection: a nested case-control study in a three year prospective cohort. Anaerobe. 2017;44:117–123. doi:10.1016/j.anaerobe.2017.03.003
3. Regnault H, Bourrier A, Lalande V, et al. Prevalence and risk factors of clostridium difficile infection in patients hospitalized for flare of inflammatory bowel disease: a retrospective assessment. Dig Liver Dis. 2014;46(12):1086–1092. doi:10.1016/j.dld.2014.09.003
4. Norris AH, Shrestha NK, Allison GM, et al. 2018 infectious diseases society of America clinical practice guideline for the management of outpatient parenteral antimicrobial therapy. Clin Infect Dis. 2019;68(1):e1–e35. doi:10.1093/cid/ciy745
5. Crobach MJ, Planche T, Eckert C, et al. European Society of clinical microbiology and infectious diseases: update of the diagnostic guidance document for clostridium difficile infection. Clin Microbiol Infect. 2016;22(Suppl 4:):S63–81. doi:10.1016/j.cmi.2016.03.010
6. McDonald LC, Gerding DN, Johnson S, et al. Clinical practice guidelines for clostridium difficile infection in adults and children: 2017 Update by the Infectious Diseases Society of America (IDSA) and society for healthcare epidemiology of America (SHEA). Clin Infect Dis. 2018;66(7):e1–e48. doi:10.1093/cid/cix1085
7. Guh AY, Mu Y, Winston LG, et al. Trends in U.S. burden of clostridioides difficile infection and outcomes. New England J Med. 2020;382(14):1320–1330. doi:10.1056/NEJMoa1910215
8. Alzouby S, Baig K, Alrabiah F, et al. Clostridioides difficile infection: incidence and risk factors in a tertiary care facility in Riyadh, Saudi Arabia. J Infect Public Health. 2020;13(7):1012–1017. doi:10.1016/j.jiph.2019.10.014
9. Aljafel NA, Al-Shaikhy HH, Alnahdi MA, et al. Incidence of Clostridioides difficile infection at a Saudi tertiary academic medical center and compliance with IDSA/SHEA, ACG, and ESCMID guidelines for treatment over a 10-year period. J Infect Public Health. 2020;13(8):1156–1160. doi:10.1016/j.jiph.2020.03.007
10. Stofkova Z, Novakova E, Sadlonova V. Survey on the diagnosis and treatment of Clostridium difficile infection. Bratisl Lek Listy. 2020;121(12):840–846. doi:10.4149/BLL_2020_138
11. Fayerberg E, Bouchard J, Kellie SM. Knowledge, attitudes and practice regarding Clostridium difficile: a survey of physicians in an academic medical center. Am J Infect Control. 2013;41(3):266–269. doi:10.1016/j.ajic.2012.03.013
12. Ferguson JK, Cheng AC, Gilbert GL, et al. Clostridium difficile laboratory testing in Australia and New Zealand: national survey results and Australasian society for infectious diseases recommendations for best practice. Pathology. 2011;43(5):482–487. doi:10.1097/PAT.0b013e328348c9b4
13. Alcalá L, Marín M, Martín A, et al. Laboratory diagnosis of clostridium difficile infection in Spain: a population-based survey. J Hosp Infect. 2011;79(1):13–17. doi:10.1016/j.jhin.2011.05.017
14. Chung H-S, Park JS, Shin B-M. Laboratory diagnosis of clostridium difficile infection in Korea: the first national survey. Ann Lab Med. 2019;39(3):317–321. doi:10.3343/alm.2019.39.3.317
15. Kociolek LK, Kutty PK, Polgreen PM, et al. Healthcare provider diagnostic testing practices for identification of clostridioides (clostridium)difficile in children: an emerging infections network survey. Infect Control Hosp Epidemiol. 2019;40(3):276–280. doi:10.1017/ice.2018.347
16. Almohammed OA, Aldwihi LA, Alragas AM, et al. Knowledge, attitude, and practices associated with COVID-19 among healthcare workers in hospitals: a cross-sectional study in Saudi Arabia. Front Public Health. 2021;9:643053. doi:10.3389/fpubh.2021.643053
17. Swed S, Bohsas H, Patwary MM, et al. Knowledge of mpox and its determinants among the healthcare personnel in Arabic regions: a multi-country cross-sectional study. New Microbes New Infect. 2023;54:101146. doi:10.1016/j.nmni.2023.101146
18. Legenza L, Barnett S, Rose W, et al. Clostridium difficile infection perceptions and practices: a multicenter qualitative study in South Africa. Antimicrob Resist Infect Control. 2018;7(1):125. doi:10.1186/s13756-018-0425-y
19. Bishop PA, Isache C, McCarter YS, et al. Clinical impact of a pharmacist-led antimicrobial stewardship initiative evaluating patients with clostridioides difficile colitis. J Invest Med. 2020;68(4):888–892. doi:10.1136/jim-2019-001173
20. Polisetty RS, Hoff BM, Moore WJ, et al. 180. Impact of a two-step diagnostic bundle on hospital-onset clostridioides difficile infection rates and treatment across a large health system. Open Forum Infect Diseases. 2022;9(Supplement_2): doi:10.1093/ofid/ofac492.258
21. Blythe D, Blythe D, Bork J, et al. SPARC-ing change—the Maryland statewide prevention and reduction of clostridioides difficile (SPARC) collaborative. Infect Control Hosp Epidemiol. 2020;41(S1):s80–s80. doi:10.1017/ice.2020.571
22. Aroori S, Blencowe N, Pye G, et al. Clostridium difficile: how much do hospital staff know about it? Ann R Coll Surg Engl. 2009;91(6):464–469. doi:10.1308/003588409X432310
23. Johnson S, Lavergne V, Skinner AM, et al. Clinical practice guideline by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA): 2021 focused update guidelines on management of clostridioides difficile infection in adults. Clin Infect Dis. 2021;73(5):e1029–e1044. doi:10.1093/cid/ciab549
24. Finnimore K, Smyth W, Carrucan J, et al. Nurses’ knowledge, practices and perceptions regarding Clostridioides difficile: survey results. Infect Dis Health. 2023;28(1):39–46. doi:10.1016/j.idh.2022.07.003
25. Comparcini D, Simonetti V, Segala FV, et al. Nurses’ knowledge, attitudes and practices on the management of clostridioides difficile infection: a cross-sectional study. Antibiotics (Basel). 2023;12(3): doi:10.3390/antibiotics12030529
26. Almutairi MS, Gonzales-Luna AJ, Alnezary FS, et al. Comparative clinical outcomes evaluation of hospitalized patients infected with Clostridioides difficile ribotype 106 vs. other toxigenic strains. Anaerobe. 2021;72:102440. doi:10.1016/j.anaerobe.2021.102440
27. Thabit AK, Aljedaani HJ, Alghamdi RH, et al. An insight into clostridioides difficile-associated diarrhea in Saudi children: diagnosis and treatment. Expert Rev Gastroenterol Hepatol. 2023;17(8):805–810. doi:10.1080/17474124.2023.2240704
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.