Back to Journals » Patient Preference and Adherence » Volume 20
Assessment of Factors Associated with Treatment Adherence Among Elderly Patients with Multimorbid Type 2 Diabetes Mellitus Using Lasso-Logistic Regression
Authors Ma R ![]() , Zhou B
, Zhou B ![]() , Liu T, Wang Y
, Liu T, Wang Y
Received 16 November 2024
Accepted for publication 1 December 2025
Published 13 January 2026 Volume 2026:20 506859
DOI https://doi.org/10.2147/PPA.S506859
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Ruijie Ma,1,* Baiyun Zhou,1,* Ting Liu,2 Yanmei Wang1
1Department of Nursing, Pudong Gongli Hospital, Shanghai University of Medicine & Health Sciences, Shanghai, People’s Republic of China; 2Shanghai Health Commission Key Lab of Artificial Intelligence (AI)-Based Management of Inflammation and Chronic Diseases, Department of Central Laboratory, Pudong Gongli Hospital, Shanghai University of Medicine & Health Sciences, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yanmei Wang, Department of Nursing, Pudong Gongli Hospital, Shanghai University of Medicine & Health Sciences, No. 219 Miao Pu Road, Shanghai, 200135, People’s Republic of China, Email [email protected]
Aims and Objectives: This study aimed to investigate treatment adherence among elderly patients with multimorbid type 2 diabetes mellitus (T2DM), and analyze the influencing factors.
Design: A single-centre, cross-sectional study design.
Methods: In this study, convenience sampling was used to examine elderly patients with multimorbid T2DM seeking treatment at six community health service centers within the Jinqiao Medical Alliance in the Pudong New Area of Shanghai between May and July 2024. Demographic and disease-related data were collected including treatment adherence, self-care activities, social support, cognitive function, and depression. Factors influencing treatment adherence were investigated through three machine learning approaches: random forest algorithm for detecting non-linear patterns, multiple linear regression for linear relationship analysis, and Lasso-Logistic regression with L1 regularization to optimize feature selection while controlling multicollinearity. This tripartite methodology synergistically combines ensemble learning, parametric modeling, and sparse logistic regression to ensure robust predictor identification.
Results: This study found that the average treatment adherence score for elderly patients with multimorbid T2DM was 45.30 (SD = 5.99). Integrated machine learning (random forest, Lasso-Logistic regression, and linear regression) identified four key determinants: elevated HbA1c (β = − 4.417, P < 0.01) and depression (β = − 1.207, P < 0.01) significantly reduced adherence, whereas improved self-care (β = 0.081, P < 0.01) and higher income (β = 0.589, P < 0.01) enhanced compliance. This multi-method approach validated predictors through both linear and non-linear modeling frameworks.
Conclusion: This study quantifies adherence in elderly T2DM patients (Mean=45.30) and identifies four modifiable predictors through advanced modeling. Prioritized interventions should focus on enhancing glycemic control through intensified HbA1c monitoring for upward trends and integrating depression management into diabetes care plans, while leveraging self-care capacity and economic support as foundational enhancers through tailored guidance and support programs to improve treatment adherence, optimize health outcomes, and minimize morbidity in this population.
Keywords: type 2 diabetes mellitus, multimorbidity, treatment adherence, cross-sectional study, random forest algorithm
Introduction
The term “multimorbidity” denotes the simultaneous presence of two or more chronic health conditions within a patient,1 characterized by elevated prevalence, recurrent incidence, and significant disability rates, particularly among the elderly population.2,3 With the acceleration of population aging, the incidence of multimorbidities among elderly individuals is steadily increasing.4–6 According to the findings of the 2020 Seventh National Population Census in China, the elderly populace reached 260.4 million, with a staggering 61.0% of individuals aged over 70 exhibiting multimorbid conditions. Prevalence rates varied significantly, spanning from 21.0% to 69.5%, depending on the evaluation criteria and regional differences; however, the overall scenario remains of grave concern.7
Diabetes mellitus (DM) is central conditions within the realm of multimorbidities,7,8 which has undergone a marked and persistent rise in prevalence over the past four decades.9–11 Projections estimate an increase in prevalence to 11.3% by 2030, posing significant challenges to socio-economic progress.11 In 2017, the economic ramifications of DM management in China reached $110 billion, accounting for 15.1% of the global economic impact of the disease. T2DM stands as the most prevalent form of diabetes in China, drawing substantial scholarly attention, particularly in research focusing on elderly diabetic multimorbidities.12
Elderly patients with multimorbid T2DM face compounded clinical challenges due to prolonged disease progression and complex pathophysiological interactions.13 These dynamics not only heighten risks of psychological comorbidities and socioeconomic burden but also strain healthcare systems’ capacity for effective chronic disease management. Within this context, treatment adherence – defined as patients’ sustained engagement with pharmacotherapy, dietary modifications, physical activity regimens, and scheduled clinical evaluations14 – emerges as a critical mediator of health outcomes and disease burden mitigation. However, treatment adherence behaviors are profoundly influenced by demographic, cultural, and systemic factors.15–17 Existing studies demonstrate that demographic variables—including age, educational attainment, employment status, and polypharmacy—significantly affect treatment adherence among older adults with comorbidities: advancing age correlates negatively with adherence, higher education levels exhibit positive associations, retirees or unemployed individuals demonstrate better compliance compared to their employed counterparts, while polypharmacy exacerbates nonadherence due to intensified comorbidity burdens.15 Within Shanghai’s unique cultural context, dietary traditions and familial structural shifts jointly create systemic barriers to adherence. The culinary culture of “thick oil and red sauce” perpetuates elderly preferences for high-glycemic-index dishes like braised pork, fostering rigid dietary habits that directly conflict with medical guidance.16 Concurrently, the empty-nest phenomenon, amplified by advanced aging, undermines household monitoring mechanisms, allowing entrenched unhealthy eating patterns to persist and intensify due to inadequate external intervention. These dual cultural determinants interact synergistically, culminating in chronic disease management challenges emblematic of the region’s sociocultural landscape.17
Previous interventions aimed at improving treatment adherence in similar populations have been explored. Some studies focused on educational programs to enhance patients’ knowledge about diabetes and its management, while others emphasized the role of social support systems. However, these interventions often had limitations, the evidence remains fragmented, with predominant focus on medication adherence in single-disease contexts, significant knowledge gaps persist regarding: (a) Multidimensional adherence behaviors encompassing nutrition, self-care, and preventive monitoring; (b) Context-specific determinants within aging populations with multimorbidity; (c) Advanced analytical approaches to disentangle complex predictor interactions.14 To address these gaps, this investigation adopted the Health Ecological Model (HEM), which provided a comprehensive framework to systematically identify and analyze multilevel determinants of treatment adherence across five hierarchical dimensions—intrapersonal, interpersonal, organizational/community, public policy, and physical environment.18 Building on this multilevel framework, the study employed three sequentially integrated machine learning approaches: the random forest algorithm first identified non-linear interactions and prioritized critical predictors by evaluating feature importance among factors through Gini impurity analysis; subsequently, multiple linear regression quantified directional relationships between refined predictors and adherence behaviors, estimating risk magnitudes via β-coefficients; concurrently, LASSO-logistic regression applied L1 regularization to eliminate redundant features arising from complex interactions factors, resolving multicollinearity while preserving clinically interpretable determinants.19 The aim was to investigate the current status of treatment compliance in elderly patients with multimorbid T2DM and analyze the main influencing factors, to provide insights and references for developing personalized medical and nursing strategies for this demographic.
Methods
Study Design
The study was designed as a single-centre, cross-sectional research. It was conducted and reported in compliance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines throughout the process.
Sample
According to the sample size estimation formula for cross-sectional surveys20

Where n is the sample size, µ is a statistical measure, and π is the incidence. After conducting a literature review, it was found that the prevalence of multimorbidities in elderly individuals with type 2 diabetes in China was identified as 40.32%,7 which can be expressed as π = 0.40. Setting α = 0.05 and  . By selecting 10% of the estimated population proportion, which δ was set to 4% (10% of 40.32%), the necessary sample size (n) was estimated to be 576. Considering a 20% inefficiency rate, the targeted sample size was estimated to 691 participants, and we ultimately received 856 valid responses.
. By selecting 10% of the estimated population proportion, which δ was set to 4% (10% of 40.32%), the necessary sample size (n) was estimated to be 576. Considering a 20% inefficiency rate, the targeted sample size was estimated to 691 participants, and we ultimately received 856 valid responses.
Participants and Procedure
Utilizing a convenience sampling method, this research focused on elderly patients diagnosed with multimorbid T2DM who sought treatment at six community health service centers affiliated with the Jinqiao Medical Alliance in the Pudong New Area of Shanghai, spanning from May to July 2024. Other inclusion criteria include: (1) Compliance with the diagnostic standards for elderly type 2 diabetes outlined in the Guideline for the Prevention and Treatment of Type 2 Diabetes Mellitus in China (2020 edition); (2) One or more chronic diseases in addition to diabetes mellitus; (3) Age ≥ 60 years; (4) patients were conscious; (5) voluntary criteria. The exclusion criteria: (1) Patients with other serious chronic diseases; (2) Participation in other intervention studies within the last three months that could influence the results; (3) Patients with severe disabilities preventing cooperation in the investigation.
Instruments
General Information Questionnaire
This study, based on previous literature review and the Health Ecology Theory, designed a general information questionnaire that includes the following aspects: (1) Personal traits: gender, age, complications, number of multimorbidities, family history of diabetes, disease duration, body mass index (BMI), HbA1c, fasting plasma glucose (FPG), postprandial blood glucose (PBG); (2) Psychological and behavioral characteristics: smoking, alcohol consumption, nighttime sleep time, physical activity status (≥3 times a week, each time > 30 min); (3) Interpersonal networks: marital status, living alone status; (4) Work and living conditions: education level, personal monthly income; (5) Policy environment: type of medical insurance. Among them, data for age, type of medical insurance, complications, number of multimorbidities, BMI, HbA1c, FPG, and PBG were retrieved from medical records.
Diabetes Treatment Adherence Questionnaire
The questionnaire was adapted by Chinese scholars Chen et al21 from the Diabetes Adherence Questionnaire originally developed by another group of Chinese scholars, Li et al.22 It comprises five dimensions: medication, diet, exercise, self-monitoring, and regular review, with four items for each dimension, totaling 20 items. Each item employs a 3-point scoring system: often (1 point), occasionally (2 points), and never (3 points). The maximum score is 60, with higher scores indicating better adherence; scores between 40–60 suggest good adherence, while scores below 40 indicate poor adherence. The Cronbach’s α of the Diabetes Treatment Adherence Questionnaire was 0.86 in diabetic population.21
Summary of Diabetes Self-Care Activities
The Summary of Diabetes Self-Care Activities (SDSCA), originally developed by Toobert et al23 was subsequently translated into Chinese and culturally adapted through a standardized forward-backward translation protocol by Wan et al.24 It consists of six dimensions: general diet (2 items), special diet (2 items), exercise (2 items), blood glucose monitoring (2 items), foot care (2 items), and medication (1 item), summing up to 11 items with a total score of 77. Item 4 is reverse scored, while the others are positively scored; higher scores reflect better self-care activities. Given the varying number of items across different dimensions, a scoring index was used for dimension comparison, calculated as follows: scoring index = (actual score of the dimension / possible maximum score of the dimension) × 100%. A dimension scoring index of > 80% was considered a high level. 60%–80% asmedium level, and < 60% as low level.22 In the cultural adaptation work carried out by Wan et al, the Cronbach’s α of the SDSCA for patients with type 2 diabetes was 0.89.24
Social Support Rate Scale
The Social Support Rate Scale (SSRS) was designed by Chinese scholar Xiao et al to understand the characteristics of participants’ social support.25 It comprises a total of 10 items, which include subjective support (items 1, 3, 4, and 5, totaling 4 items, with scores ranging from 8 to 32), objective support (items 2, 6, and 7, with scores ranging from 1 to 22), and the degree of utilization of social support (items 8, 9, and 10, with scores ranging from 3 to 12). The maximum possible score is 66; a higher score indicates greater support received. This scale can objectively reflect an individual’s level of social support. It has demonstrated good reliability and validity within the Chinese population, with social support levels categorized as low to moderate (≤ 44 points) and high (> 45 points). The test-retest reliability of the SSRS was 0.92.25 The Cronbach’s alpha ranged from 0.800 to 0.844.14,26
Mini-Mental State Examination
The Mini-Mental State Examination (MMSE), originally developed by Folstein et al27 was subsequently translated and culturally adapted for Chinese populations through a standardized linguistic validation process by Zhou et al.28 It assesses five dimensions: orientation (10 items), memory (3 items), attention and calculation (5 items), recall (3 items), and language (9 items), comprising a total of 30 items. Each item is scored as 1 or 0, resulting in an overall score ranging from 0 to 30, where a higher score indicates better cognitive ability. For illiterate individuals, a score of 17 or less is indicative of cognitive decline. Similarly, for those with less than nine years of education, a score of 20 or less suggests cognitive decline. For individuals with more than nine years of education, a score of 24 or less indicates cognitive decline. The Cronbach’s α of the MMSE was reported to be 0.833.28
5-Item Geriatric Depression Scale
The 5-item Geriatric Depression Scale (GDS-5) was adapted and simplified by scholars including Hoyl et al from the 15-item Geriatric Depression Scale (GDS-15).29,30 It consists of 5 items, with a score of 2 or more indicating the presence of depressive symptoms. In this study, a binary classification method was employed to assign scores based on the scale: a score of 2 or higher indicated the presence of depressive symptoms, recorded as 1 point (yes); otherwise, recorded as 0 points (no). The Cronbach’s α of the GDS-5 was reported to be 0.810.31
Data Collection Procedures
Five nursing graduate students were trained prior to the survey to ensure the accuracy and consistency of data collection. After communicating with the administrators of six community health service centers, the research team conducted questionnaires at the sites of health education activities organized for diabetic patients in the communities. The survey was conducted face-to-face, with participants fully informed about the completion process. For those unable to complete the survey independently, researchers assisted while avoiding any suggestive or leading language. Upon completion of the survey, the data were promptly verified for completeness and validity. All questionable items were double-checked and corrected, and any obvious errors were removed.
Data Analysis
Data analysis was conducted using SPSS 27.0 and R Studio software. Normally distributed continuous data were presented as the Mean (SD), while non-normally distributed continuous data were expressed as the Median (P10, P90). Categorical data are described using frequencies and proportions. The comparison of normally distributed continuous data between two groups was conducted using the independent-samples t-test. In contrast, the comparison of two groups with skewed distribution was performed using the Mann–Whitney U-test. When comparing multiple groups, Analysis of Variance (ANOVA) was used for normally distributed continuous data, whereas the Kruskal–Wallis test was employed for skewed continuous data. The random forest algorithm in R software was employed to construct a Random forest plot and rank the importance of the initially included variables. Lasso analysis was used for variable selection, and the identified variables were subsequently analyzed using multiple stepwise regression. All significance levels were set at P < 0.05 (two-tailed).
To address potential confounding factors, we implemented a rigorous multi-stage analytical approach. Initial variable screening was conducted through univariate analysis with a significance threshold of p < 0.05, eliminating variables showing no preliminary association with adherence outcomes. Subsequently, LASSO regression was performed using the glmnet package in R, with the lambda parameter optimized via 10-fold cross-validation to balance model complexity and predictive accuracy. This process retained 10 variables with non-zero coefficients from an initial pool of 14 candidates. The selected variables were then incorporated into a multivariable linear regression model.
Ethical Considerations
This study received approval from Gongli Hospital of Shanghai Pudong New Area ethics committee (Approval No. GLYY1s2024-025, approval date: May 15, 2024). Participation was entirely voluntary for all subjects. This study complies with the Declaration of Helsinki.
To ensure the confidentiality and data security of the participants, several measures were implemented: (1) Anonymization: Personal identifiers were removed from the data to ensure anonymity. Participants were assigned unique study IDs to facilitate data management without compromising their privacy. (2) Data Handling and Analysis: Data handling and analysis were performed in compliance with data protection regulations. Only aggregated data were used for reporting and publication purposes, ensuring that individual participants could not be identified. (3) Confidentiality Agreement: All researchers involved in the study signed a confidentiality agreement, committing to the protection of participants’ personal information and study data. (4) Secure Communication: Communication regarding study-related information was conducted through secure channels to prevent unauthorized access or disclosure.
Results
Participant Characteristics
A total of 856 elderly patients with multimorbid T2DM participated in the survey. The ages of the participants ranged from 60 to 85 years, with a mean age of 69.39 years (SD = 6.22). The sample includes 445 males (52%) and 411 females (48%). Among the participants, 478 (55.8%) were diagnosed with one additional disease alongside T2DM, whereas 378 (44.2%) presented with two or more additional diseases. These findings are summarized in Table 1.
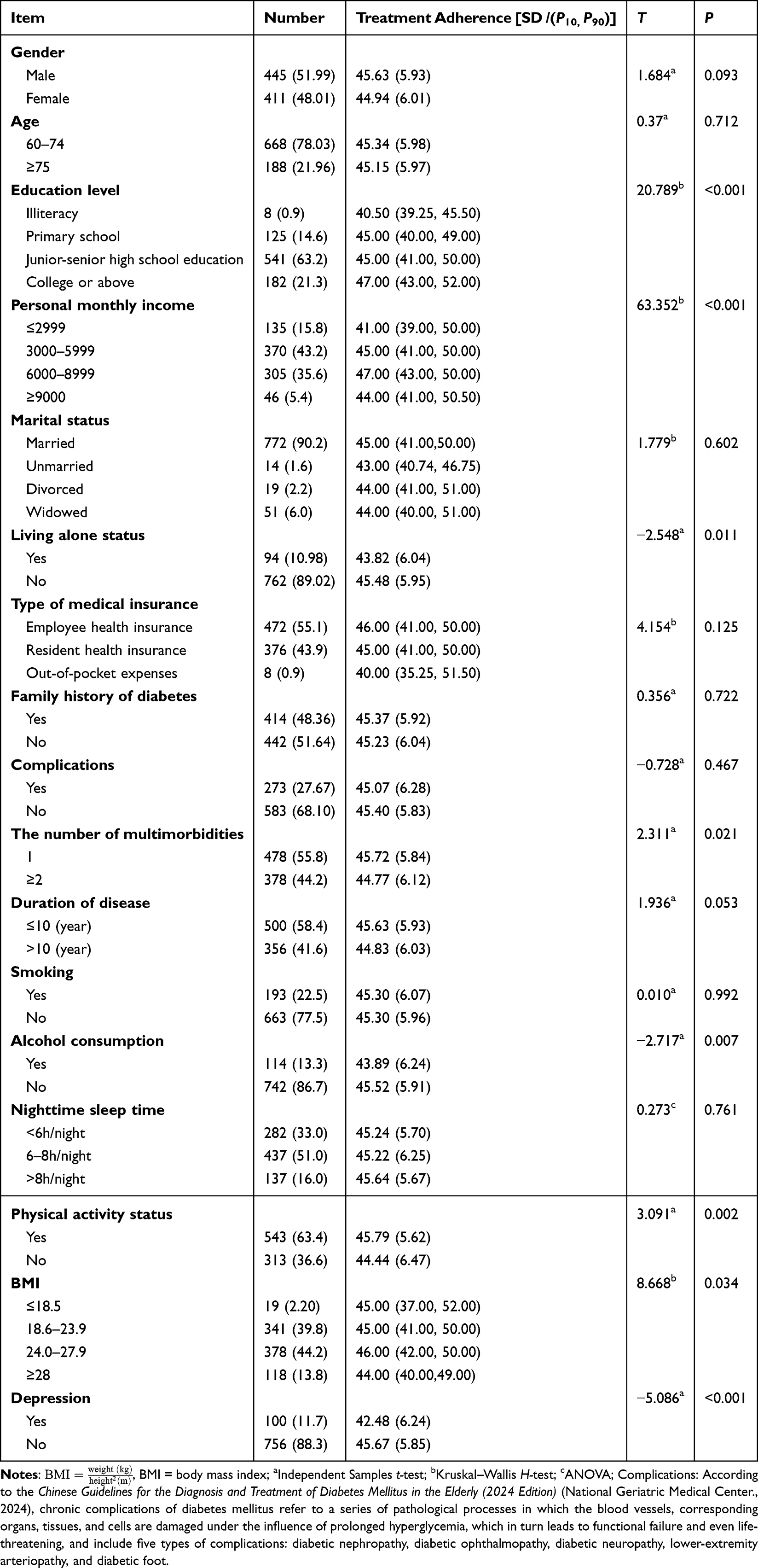 |
Table 1 General Data and Univariate Analysis of Treatment Adherence in Elderly Patients with Multimorbid T2DM (n = 856) |
Univariate Analysis of the Level of Treatment Adherence and Its Associated Factors
We defined those who had lost their partner and did not live with their children as “living alone” status, “smokers”/ “drinkers” as smoking/drinking more than or equal to 3 times per week, and those who were “physically active” as exercising more than or equal to 3 times per week for more than 30 minutes per session. Univariate analysis showed that living alone status, the number of multimorbidities, alcohol consumption, physical activity status, education level, personal monthly income, BMI, and depression are statistically significant differences in score of the treatment adherence among elderly patients with multimorbid T2DM. (P < 0.05) (Table 1).
Scores on the Diabetes Treatment Adherence Questionnaire and Other Scales
The mean score for the Diabetes Treatment Adherence Questionnaire among elderly patients with multimorbid T2DM is 45.30 (SD = 5.99). The highest mean score in the medication dimension is 2.58 (SD = 0.45), while the exercise dimension has the lowest mean score of 1.87 (SD = 0.49). The total score for SDSCA does not conform to a normal distribution, represented as a Median (P10, P90) of 37.00 (24.00, 50.00), with the highest mean score of 7.00 (5.00, 7.00) for the medication dimension and the lowest mean score of 1.00 (0.00, 3.50) for the foot care dimension. The mean score for the level of social support is 34.03 (SD = 5.56), with the highest mean score of 4.81 (SD = 0.84) for subjective support items. The mean score for MMSE is 27.83 (SD = 2.82). Scores on the Diabetes Treatment Adherence Questionnaire and other scales are presented in Table 2.
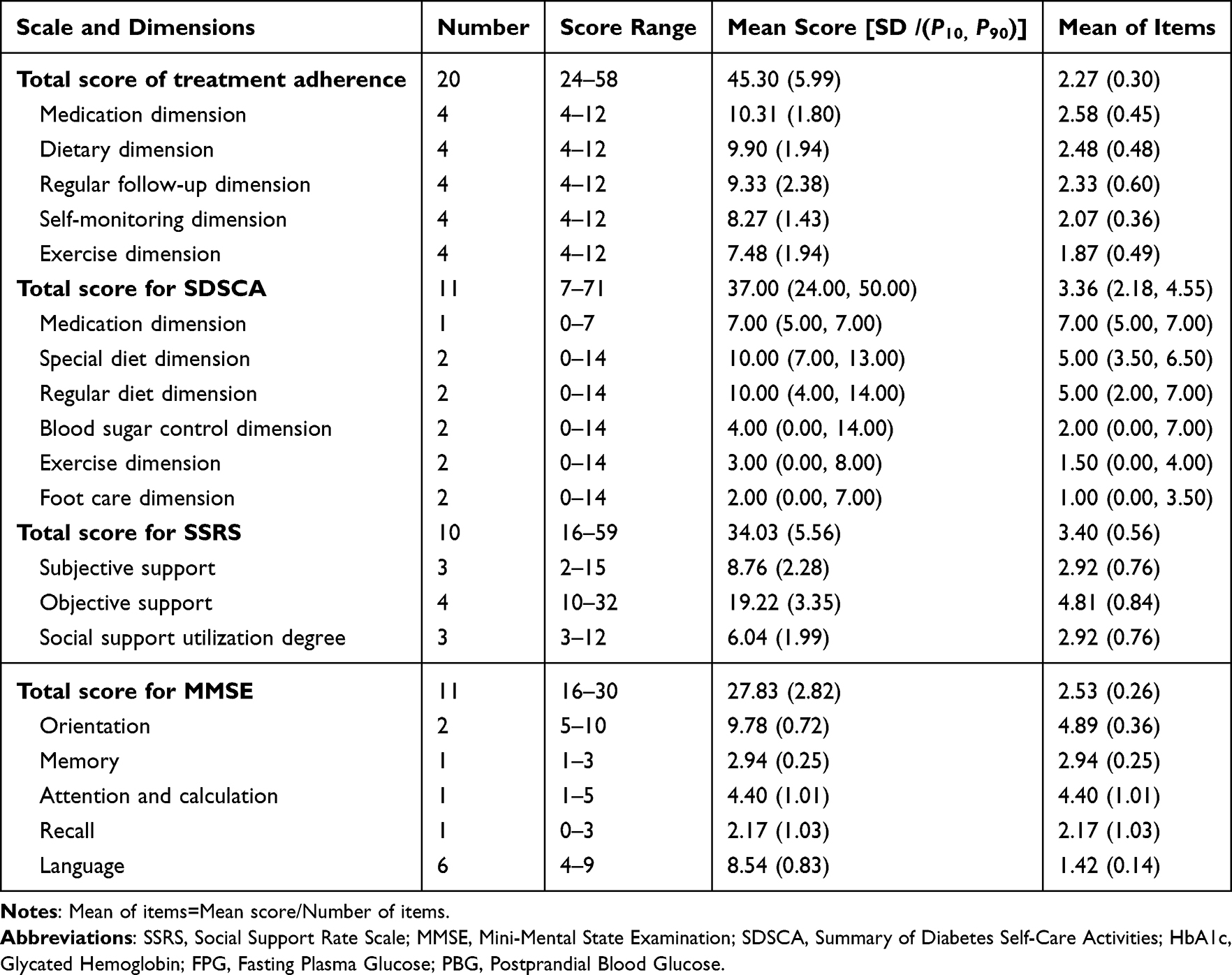 |
Table 2 Scores on Diabetes Treatment Adherence Questionnaire and Other Scales (n = 856) |
Correlation Analysis of Continuous Variables
The results of the Spearman correlation analysis indicated significant correlations between treatment adherence and various factors in elderly patients with multimorbid T2DM. Specifically, treatment adherence is positively correlated with cognitive (rs = 0.189, P < 0.001), self-care activities (rs = 0.358, P < 0.001), and social support level (rs = 0.186, P < 0.001). Conversely, it is negatively correlated with the key metabolic indicators, including FPG (rs = −0.892, P < 0.001), PBG (rs = −0.880, P < 0.001), and HbA1c (rs = −0.865, P < 0.001). These findings are summarized in Table 3.
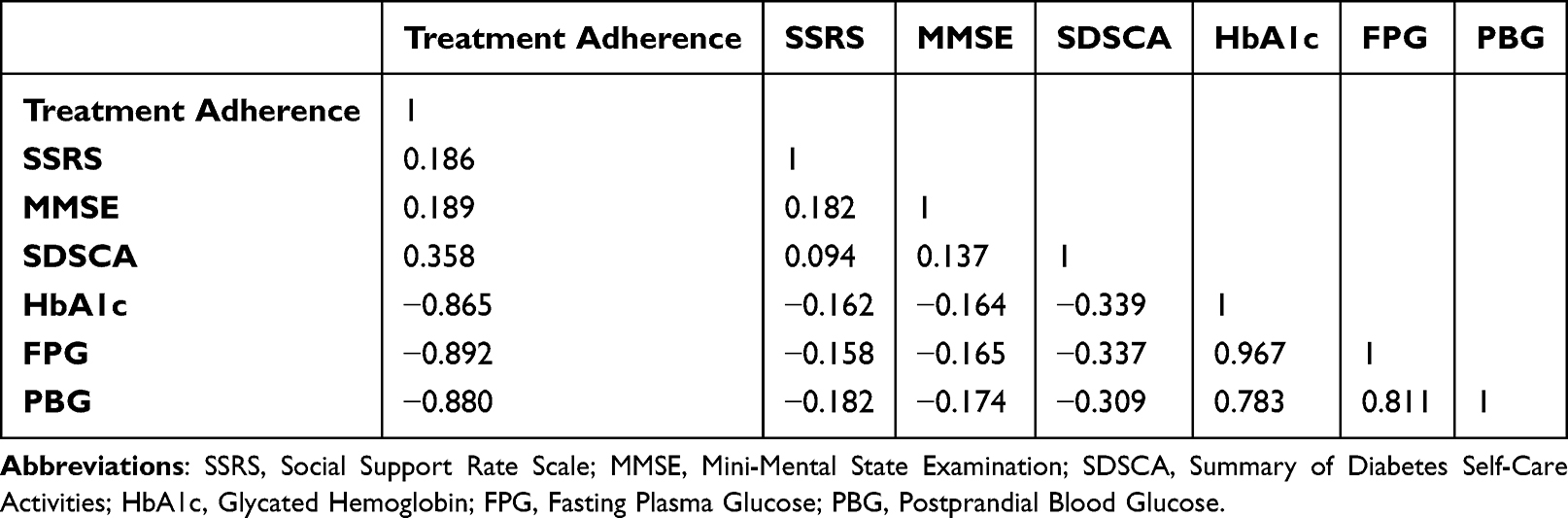 |
Table 3 Correlation Analysis of Continuous Variables (n = 856) |
Screening the Influencing Factors
Ranking of Variable Importance
Using the treatment adherence questionnaire scores as the dependent variable, We incorporated 14 statistically significant variables from univariate and correlation analyses into a Random Forest model. We utilized R Studio with the Random Forest package to generate the results. The %IncMSE (Increase in Mean Squared Error) indicates the average reduction in precision; a larger %IncMSE signifies greater importance of the variable in influencing factors. The results showed the importance of the variables ranked from highest to lowest as follows: FPG, PBG, HbA1c, personal monthly income, education level, social support level, self-care activities level, alcohol consumption, physical activity status, the number of multimorbidities, BMI, cognitive level, depression, living alone status among the variables with the greatest impact on adherence to treatment in elderly patients with multimorbid T2DM are PBG, FPG, and HbA1c, with a %IncMSE of 20–50%, which is 2–5 times higher than that of the other variables, as demonstrated in Figure 1.
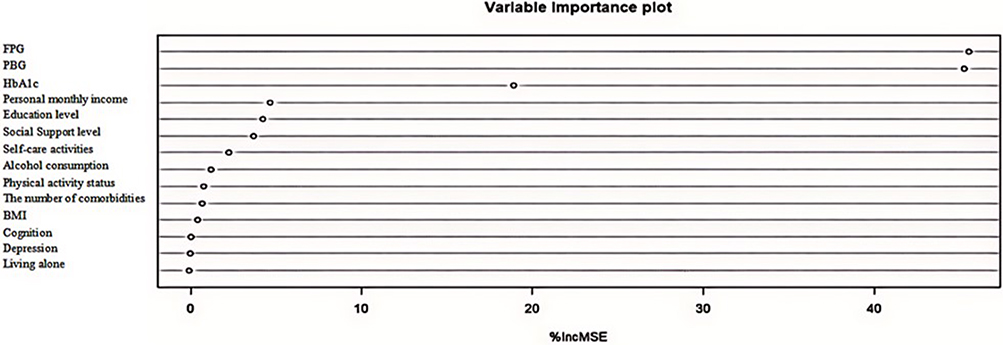 |
Figure 1 Importance ranking of factors affecting treatment adherence in elderly patients with Comorbidities of T2DM. |
Identifying Variable
Based on the variable importance ranking, we conducted a LASSO analysis on 14 statistically significant variables from the univariate analysis using the “glmnnet” function in R Studio (See Figure 2). The vertical dashed line on the left represents “λ-min”, while the vertical dashed line on the right denotes “λ-1se”. The result showed minimal variation in bias within the interval [λ-1se, λ-min]. At the optimal λ, the result identified 10 significant predictors. As a result, the following top 10 factors—PBG, FPG, HbA1c, self-care activities level, personal monthly income, depression, alcohol consumption, living alone status, the number of multimorbidities, and physical activity status—were incorporated into the multiple linear regression analysis.
 |
Figure 2 Feature variable selection based on LASSO analysis. |
Multivariate Analysis of the Level of Treatment Adherence and Its Associated Factors
The variables HbA1c, PBG, and FPG are commonly used to evaluate glycemic control in patients, but they may present collinearity. Moreover, HbA1c served as the gold standard for assessing a patient’s glycemic control. To minimize the impact of collinearity on the regression results, this study included only HbA1c in the analysis. Taking treatment adherence as the dependent variable, the top eight variables identified by the random forest algorithm were used as independent variables in a multiple-stepwise regression analysis. Since personal monthly income is an ordinal categorical variable and the other categorical variables are binary, there is no necessity for dummy variable creation. The analysis results indicated that HbA1c, depression, self-care activities, and personal monthly income are the main influencing factors of treatment adherence in elderly patients with multimorbid T2DM (P < 0.001), with VIF values all less than 10, showing the absence of confounding interference among the variables, as presented in Table 4.
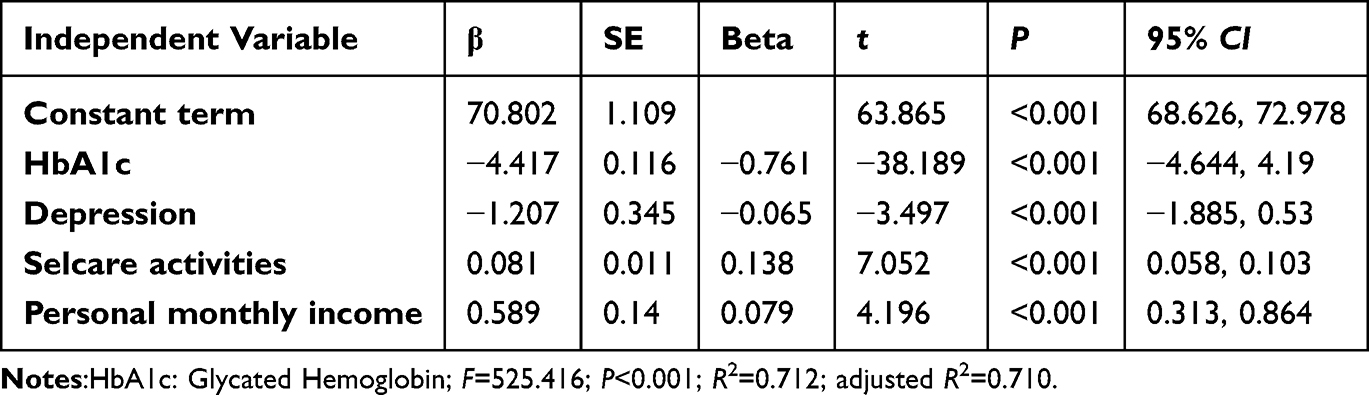 |
Table 4 Multivariate Analysis of the Level of Treatment Adherence and Its Associated Factors (n = 856) |
Discussion
The Treatment Adherence Levels Among Elderly Patients with Multimorbid T2DM
In this research, the treatment adherence levels among elderly patients with multimorbid T2DM were observed to be moderately high, with a mean score of 45.30 (SD = 5.99). This score surpassed the established threshold of 40 according to the adherence scale and was slightly higher than the results from Fei Ji’s 2019 research,32 which indicated a score of 42.25 (SD = 7.09) among elderly patients with type 2 diabetes residing in a rural community in Jinan. The variations might stem from differences in geographical locations, demographic characteristics, and timeframes.32 However, both investigations reported elevated scores in the areas of medication adherence and dietary compliance. This concordance reflects the impact of traditional Chinese cultural beliefs that intertwine medicinal and dietary practices, leading most elderly patients with multimorbid T2DM to prioritize both pharmacological and nutritional interventions, thereby enhancing their capacity for diet self-regulation and consistent medication intake.
In the study, only 15.5% of elderly patients with multimorbid T2DM had attained an educational level of primary school or below, while those holding university degrees or higher comprised 21.3% of the participants, indicating generally high educational attainment. This elevated educational background facilitates a comprehensive understanding of treatment guidelines and fosters an eagerness to pursue diabetes-related knowledge and comply with treatment protocols. Additionally, 55.8% of participants had a singular multimorbidity, resulting in the utilization of fewer medications with minimal adverse effects such as insomnia, daytime drowsiness, nausea, or vomiting, and a sustained commitment to following medical advice regarding timely medication intake. Importantly, 89% of patients lived with family members, and robust familial support—a vital component of social support—showed a significant correlation with treatment adherence, positively affecting patients’ adherence behaviors. The majority of elderly patients with multimorbid T2DM in this study embraced a healthy lifestyle.33 Specifically, 86.7% refrained from alcohol consumption or had ceased drinking, 63.4% participated in regular physical activity, and 39% maintained an optimal weight. This commitment to a healthy lifestyle contributes to achieving closer alignment with ideal management standards, as the prior behaviors of patients align well with treatment recommendations, reflecting a generally strong adherence to prescribed protocols.
Moreover, a robust alliance among healthcare professionals, patients, and caregivers serves as a vital cornerstone for improving patient adherence to treatment protocols.34,35 This highlights the imperative for medical and nursing personnel to acknowledge patient preferences and subjective experiences in the provision of healthcare services. Embracing a patient-centered methodology for shared decision-making is crucial, as it facilitates timely communication that fosters patient trust and enhances their sense of accountability and intrinsic motivation. The pivotal roles of primary healthcare settings and family support should be fully leveraged, with synergistic strengths cultivated through a collaborative “Hospital-Community-Home” model to collectively oversee and enhance treatment adherence among elderly patients with multimorbid T2DM, thereby supporting more effective disease management.
Factors Influencing Treatment Adherence in Elderly Patients with Multimorbid T2DM
HbA1c
HbA1c is widely regarded as the benchmark for evaluating an individual’s glycemic control. This study highlighted an HbA1c threshold of less than 7.0% as the desired standard. The results indicated that the HbA1c achievement rate for elderly patients with multimorbid T2DM stood at 49.18%, which displayed a negative correlation with treatment adherence. This finding corroborates the research by DaSantos et al emphasizing that HbA1c is a critical determinant of patient compliance with treatment regimens.36
Elderly patients with multimorbid T2DM face substantial challenges in long-term pharmacotherapy due to the progressive nature of the disease. Chronic macrovascular and microvascular complications inevitably increase medication complexity, healthcare costs, and risks of glycemic fluctuations. These factors collectively hinder treatment adherence and amplify psychological burdens for patients and caregivers. However, growing recognition of the benefits of healthy lifestyle modifications—such as reducing alcohol intake to mitigate its adverse effects on insulin secretion and glucose utilization—and strict adherence to medical regimens can foster proactive glucose management. Regular follow-up, continuous glucose monitoring, and structured interventions (eg, balanced nutrition, physical activity, and medication compliance) are critical for stabilizing metabolic parameters and delaying disease progression. Healthcare providers must prioritize patient education to address barriers to adherence, reinforce the importance of sustained behavioral changes, and empower patients to align their daily practices with clinical guidelines, thereby optimizing long-term outcomes.37–40
Depression
The study revealed depressive symptoms in 11.7% of older adults with multimorbid T2DM. Their treatment adherence scores 42.48 (SD = 6.24) were significantly lower than those without depressive symptoms 45.67 (SD = 5.85), a pattern consistent with prior findings by Du et al.41 Additionally, research conducted by Shamim et al42 suggests that specific antidiabetic medications elevate the likelihood of developing depressive disorders. The physical manifestations associated with depressive states, such as fatigue, weakness, and headaches, directly impact patients’ self-care activities and adherence to treatment guidelines, which in turn exacerbates blood glucose regulation issues and creates a harmful cycle of declining health. Elderly patients with multimorbid T2DM frequently endure protracted health challenges accompanied by intricate pathophysiological factors. The persistent hurdles posed by the illness, along with the associated medical complications, may lead to a decrease in the quality of life for both patients and their families, giving rise to psychological distress, feelings of guilt, intensified depressive symptoms, and further diminished compliance with treatment regimens.43 Moreover, the presence of social support emerges as a critical element in mitigating stress and adverse health outcomes.44 Family support, a fundamental aspect of social support, plays an indispensable role in daily patient monitoring, emotional recognition, and management, as well as in providing positive reinforcement and encouragement. Such support has the potential to substantially improve patients’ perceptions of familial warmth and create a secure and comfortable treatment atmosphere.
In this investigation, it was observed that 10.98% of elderly patients with multimorbid T2DM were living in isolation, highlighting an alarming lack of social support and inadequate assistance in emotional, material, and various other domains. This scenario predisposes them to emotional challenges such as anxiety and depression, manifesting as diminished life enthusiasm, reluctance to participate in social engagements, denial regarding the gravity of their condition, passive coping mechanisms in response to pain, self-neglect, and non-compliance with prescribed medical guidance. Consequently, this situation hampers timely treatment and care opportunities, complicates treatment efforts, and escalates the rates of disability and mortality among these patients. These findings corroborate the research conducted by Song et al,45 which performed a meta-analysis examining the incidence of depression and its contributing factors among solitary elderly individuals in China. Therefore, healthcare practitioners must evaluate the psychological well-being of elderly patients with multimorbid T2DM and extend psychological support to mitigate anxiety and depressive symptoms. It is crucial to promote familial support and enhance social interactions, provide training and health consultations, and engage in routine reassessments to address evolving needs, which will ultimately improve adverse emotional states and optimize patient adherence to treatment regimens.
Self-Care Activities
Self-care activities among elderly patients with multimorbid T2DM are vital for effective disease management and the mitigation of complications. Our study showed a strong positive relationship with treatment adherence, marking them as indispensable for productive diabetes care. The outcome of this investigation revealed that across the five dimensions of self-care activities measured by the SDSCA, the medication, and dietary aspects received notably high scores (> 4.45), whereas glycemic control and physical activity dimensions presented moderate scores (2.36–4.45), and foot care was rated low (< 2.36). These findings align with the research conducted by He et al regarding self-care activities and their influencing factors among Chinese youth with T2DM.46 The data suggest that older adults in China living with multimorbid T2DM and additional health conditions exhibit commendable adherence to medication protocols and the maintenance of a balanced diet, possibly attributable to the direct impact of pharmacological treatments and dietary practices on glucose metabolism, coupled with the insights gained from personal experiences and the health education provided by healthcare practitioners. This comprehension fosters a stronger focus on dietary and medication compliance, yielding improved scores in these specific areas.
Effective regulation of blood glucose levels and a comprehensive exercise regimen are acknowledged as fundamental components of diabetes health management. This study observed elderly patients with multimorbid T2DM experiencing a gradual deterioration in physical function, exercise capacity, and metabolic efficiency as they age and encounter increased multimorbidities. Notably, 36.6% of participants were physically inactive, while the remaining 63.4% engaged in self-care practices using conventional exercise regimens and blood glucose monitoring technologies. However, these patients demonstrated limited understanding of the critical role that healthcare-recommended moderate-intensity aerobic exercise plays in optimizing metabolic outcomes and stabilizing blood glucose concentrations. They exhibited an insufficient understanding of the specifics regarding exercise modalities, duration, assessment methods, and safety considerations linked to aerobic resistance training, leading to an incomplete implementation of thorough blood glucose management, and slightly relaxed the rigor of blood sugar control, culminating in only moderate evaluation scores. Additionally, diabetic foot ulcers are a significant complication associated with diabetes; however, the findings revealed suboptimal self-care activities among patients concerning foot care, the mean score [SD /(P10, P90)] was 2.00 (0.00, 7.00). This may be ascribed to the advanced age of certain elderly patients with multimorbid T2DM, which can impair the timely acquisition of relevant knowledge and adaptation processes. Consequently, these patients may struggle to comprehend the etiological factors, progression, and severity of diabetic foot complications, often failing to detect early indicators in the absence of overt complications or when only mild symptoms are present, thereby overlooking critical foot care practices. A segment of patients has acknowledged the importance of foot care through educational initiatives delivered by healthcare providers; however, they have not fully comprehended the appropriate techniques for care. Erroneous practices, such as washing feet with excessively hot water and overlooking the cleaning of the spaces between the toes, may hasten the development of complications, resulting in skin damage, increased bacterial growth, and elevated infection risks.
The self-care activities exhibited by elderly patients with multimorbid T2DM showed a positive correlation with their treatment adherence, and the facets defining these behaviors closely resembled one another. This correlation indicates that emphasizing patients’ self-care efforts concerning blood glucose regulation, physical activity, and foot care could significantly enhance their treatment adherence. Healthcare professionals need to prioritize these elements and convey current self-care strategies to patients. Crafting personalized health management plans that correspond with the severity of their conditions and individual needs can facilitate the standardization of patients’ self-care activities and ultimately improve their treatment adherence.
Personal Monthly Income
In recent years, the swift advancement of the economy and cultural aspects has resulted in a notable surge in the prevalence of diabetes, presenting a considerable public health challenge. In 2022, the economic implications of diabetes in China were estimated to be $165.3 billion.47 In Shanghai, China the personal average annual expenditure for diabetes treatment and management increased from $1,292.72 in 2014 to $2,092.87 in 2019. This escalation not only imposes a financial strain on patients but also reflects the overall status of local economic development, healthcare availability, and consumption patterns.47 To alleviate the healthcare burden faced by individuals with chronic diseases, the Chinese government has initiated a series of chronic disease prevention and management strategies since 2009. Our study conducted in Shanghai involved participants covered by the municipal medical insurance system. The results indicated that the average monthly income of elderly patients with multimorbid T2DM along with multimorbid conditions was above the national average monthly income exceeded the national average by 4500 RMB,48 specifically, 41% of these patients had an average monthly income of at least 6,000 RMB, with various income streams, including pensions, governmental support, and familial assistance.49 A positive correlation existed between patients’ economic standing and their adherence to treatment regimens. Possible explanations for this correlation encompass the provision of substantial economic support, an overall elevated economic environment, and advantageous governmental policies, which reduce the economic burden of type 2 diabetes multimorbidity on individuals and families. This enhancement contributes to improved patient outcomes and a heightened awareness of chronic disease prevention. Consequently, patients exhibit a greater willingness to allocate time and resources towards disease management, proactively pursue medical treatment, adhere to long-term therapeutic approaches, and comply with medical recommendations for routine examinations and healthcare access. Such adherence fosters early identification, diagnosis, and intervention in disease progression, which benefits overall health outcomes.
Strength
Our study holds several distinct strengths. First, we specifically targeted a population—elderly patients with multimorbid T2DM—that has received insufficient attention in previous fragmented research, filling an important niche in the field. Second, our research extended the scope of treatment adherence research from single - disease medication focus to multidimensional adherence behaviors, including nutrition, self - care, and preventive monitoring. This allowed for a more comprehensive understanding of the complex factors influencing adherence among this patient group. Third, by integrating the Health Ecological Model (HEM), we adopted a holistic approach to understanding treatment adherence, comprehensively addressing the identified knowledge gaps. Fourth, the utilization of three sequentially integrated machine - learning approaches—the random forest algorithm, multiple linear regression, and LASSO - logistic regression—enabled us to identify non - linear interactions, quantify relationships, and eliminate redundant features, enhancing the depth of our analysis.
Limitation
This study has certain limitations. Firstly, the results were specific to a particular geographic region within the medical alliance in Shanghai, China, which restricted the generalizability. Secondly, the use of convenience sampling may introduce selection bias, as it may not represent the broader population of elderly patients with multimorbid T2DM. Future investigations should incorporate large-scale, multi-center studies to examine the levels of treatment adherence and associated influencing factors among elderly patients with multimorbid T2DM. By emphasizing the importance of these factors, we can identify clinical interventions that ultimately provide more robust research evidence to enhance treatment adherence and improve health outcomes for this vulnerable population. In addition, Our cross - sectional study neither fully explored the complex interactions between identified factors nor elucidated the long - term trajectory of treatment adherence. Thus, future research should employ advanced statistical approaches like structural equation modeling and longitudinal designs to comprehensively understand factor interactions, adherence patterns, and the long - term effectiveness of interventions.
Conclusion
The treatment adherence levels among elderly patients with multimorbid T2DM were observed to be at a moderately high standard. Significant determinants of adherence included HbA1c levels, depression, self-care activities, and personal monthly income. HbA1c levels directly reflect disease control, motivating patients to adhere to treatment; depressive symptoms act as a barrier, undermining patients’ motivation to engage with treatment plans; self-care activities empower patients to better manage their conditions, positively influencing adherence; and higher personal income may provide access to better resources, contributing to improved treatment compliance.
Relevance To Clinical Practice
This research delineated the adherence levels to treatment adherence among elderly patients with multimorbid T2DM and examined the determinants influencing these adherence rates. Employing a random forest algorithm, the study evaluated and ranked the significance of these determinants, thereby offering essential insights for the formulation of pharmaceutical medical and nursing strategies. The results underscored the imperative for healthcare providers to consistently evaluate treatment adherence among patients within clinical settings. By focusing on the key influencing factors, critical elements such as HbA1c, depression, self-management activities, and personal monthly income are discerned. Moreover, it becomes paramount to manage the modifiable components of these critical variables, specifically HbA1c, depression, and self-management practices, while also addressing stable factors like personal monthly income. The study advocates for the investigation of effective medical and nursing frameworks that provide affordable and high-efficacy personalized care plans for elderly patients with multimorbid T2DM, enhancing health outcomes, boosting adherence rates and patient satisfaction, curtailing healthcare expenses, and optimizing cost-effectiveness amidst constrained healthcare resources. Additionally, our research calls for the International Diabetes Federation to implement relevant strategies to alleviate the treatment burden on this substantial group of elderly patients with multimorbid T2DM, thereby improving their treatment adherence and fostering socio-economic development.
Consent for Publication
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR.
Funding
1. The Medical Discipline Construction Program of Shanghai Pudong New Area Health Commission. 2. The Healthcare Talents Elite Program of Shanghai Pudong New Area.
Disclosure
The authors report no conflicts of interest in ths work.
References
1. World Health Organization. The World Health Report 2008: Primary Health Care Now More Than Ever: Introduction and Overview. World Health Organization: Geneva, Switzerland; 2008. Available from: https://iris.who.int/handle/10665/69863.
2. Zhao Q, Wang J, Nicholas S, et al. Health-Related Quality of Life and Health Service Use among Multimorbid Middle-Aged and Older-Aged Adults in China: a Cross-Sectional Study in Shandong Province. Int J Environ Res Public Health. 2020;17(24):9261. doi:10.3390/ijerph17249261 PMCID: PMC7764479.
3. Wang Z, Peng W, Li M, et al. Association between multimorbidity patterns and disability among older people covered by long-term care insurance in Shanghai, China. BMC Public Health. 2021;21(1):418. doi:10.1186/s12889-021-10463-y PMID: 33639902; PMCID: PMC7912511.
4. Acar Tek N, Mş K-E. Determinants of Health Related Quality of Life in Home Dwelling Elderly Population: appetite and Nutritional Status. J Nutr Health Aging. 2018;22(8):996–16. doi:10.1007/s12603-018-1066-9 PMID: 30272105.
5. Wang HH, Wang JJ, Wong SY, et al. Epidemiology of multimorbidity in China and implications for the healthcare system: cross-sectional survey among 162,464 community household residents in southern China. BMC Med. 2014;12(1):188. doi:10.1186/s12916-014-0188-0 PMID: 25338506; PMCID: PMC4212117.
6. Chen H, Cheng M, Zhuang Y, Broad JB. Multimorbidity among middle-aged and older persons in urban China: prevalence, characteristics and health service utilization. Geriatr Gerontol Int. 2018;18(10):1447–1452. doi:10.1111/ggi.13510 PMID: 30178629.
7. Li YN, Wang YQ. Prevalence and Patterns of Multimorbidity Among Chinese Elderly People. Chinese General Practice. 2021;24(31):3955–3962,3978. doi:10.12114/j.issn.1007-9572.2021.00.295
8. Zemedikun DT, Gray LJ, Khunti K, Davies MJ, Dhalwani NN. Patterns of Multimorbidity in Middle-Aged and Older Adults: an Analysis of the UK Biobank Data. Mayo Clin Proc. 2018;93(7):857–866. doi:10.1016/j.mayocp.2018.02.012 PMID: 29801777.
9. Chinese Diabetes Society. Guideline for the Prevention and Treatment of Type 2 Diabetes Mellitus in China (2020 Edition). Chin J Diabetes Mellitus. 2021;13(4):315–409. doi:10.3760/cma.j.cn311282-20210304-00142
10. Magliano DJ, Boyko EJ. IDF Diabetes Atlas 10th edition scientific committee. In: IDF DIABETES ATLAS.
11. Ma Y, Kong XJ, Peng W, et al. Disease Burden and Time Trends of Diabetes in China. Chin Prev Med. 2023;24(4):281–286. doi:10.16506/j.1009-6639.2023.04.001
12. Yan W, Lu Y, Zhang R, Chang F. Multimorbidity status of the elderly in China-research based on CHARLS data. Chin J Dis Control Prevent. 2019;23(4):426–430. doi:10.16462/j.cnki.zhjbkz.2019.04.012
13. Chinese Elderly Type. Diabetes Prevention and Treatment of Clinical Guidelines Writing Group; Geriatric Endocrinology and Metabolism Branch of Chinese Geriatric Society; Geriatric Endocrinology and Metabolism Branch of Chinese Geriatric Health Care Society; Geriatric Professional Committee of Beijing Medical Award Foundation; National Clinical Medical Research Center for Geriatric Diseases (PLA General Hospital), Zhonghua Nei Ke Za Zhi. 2022;61(1):12–50. doi:10.3760/cma.j.cn112138-20211027-00751 PMID: 34979769
14. Zhang ZX, He FP, Zhang CH, et al. Latent Class Analysis and Influencing Factors of Medication Adherence in Multiple Chronic Conditions Patients[J]. Chinese General Practice. 2022;25(31):3904–3913. doi:10.12114/j.issn.1007-9572.2022.0340
15. Wang W, Luan W, Zhang Z, Mei Y. Association between medication literacy and medication adherence and the mediating effect of self-efficacy in older people with multimorbidity. BMC Geriatr. 2023;23(1):378. doi:10.1186/s12877-023-04072-0
16. Zang J, Yu H, Zhu Z, et al. Does the Dietary Pattern of Shanghai Residents Change across Seasons and Area of Residence: assessing Dietary Quality Using the Chinese Diet Balance Index (DBI). Nutrients. 2017;9(3):251. doi:10.3390/nu9030251
17. Wei Y, Sun Y, Li Y, et al. Investigation and research on elderly people’s willingness to combine medical and health care and related factors in coastal cities in eastern China. PeerJ. 2022;10:e14004. doi:10.7717/peerj.14004
18. Hou D, Sun Y, Liu Z, et al. A longitudinal study of factors associated with cognitive frailty in middle-aged and elderly population based on the health ecology model. J Affect Disord. 2024;352:410–418. doi:10.1016/j.jad.2024.02.014
19. Breiman L. Random Forests. Machine Learning. 2001;45(1):5–32. doi:10.1023/A:1010933404324
20. Sun ZQ. Medical Statistics. 2010. Available from: https://xueshu.baidu.com/usercenter/paper/show?paperid=7ce8f29723e973783dd8107181fe0c6d&site=xueshu_se.
21. Chen YM, Huang J. Compliance of Re-hospitalization Diabetic Patients. J Nursing Sci. 2008;23(23):34.
22. Li XQ, Cai HW. Investigation on Compliance Behavior of Diabetic Patients in Out-of-Hospital Treatment. Chin J Nurs. 2004;39(7):500–502.
23. Toobert DJ, Hampson SE, Glasgow RE. The summary of diabetes self-care activities measure: results from 7 studies and a revised scale. Diabetes Care. 2000;23(7):943–950. doi:10.2337/diacare.23.7.943 PMID: 10895844.
24. Wan QQ, Shang SM, Lai XB, Pan J. Study on the Reliability of Summary of Diabetes Self-Care Activities for Type 2 Diabetes Patients. Chin J Pract Nurs. 2008;24:26–27. doi:10.3760/cma.j.issn.1672-7088.2008.07.009
25. Xiao S. Theoretical Basis and Research Application of Social Support Rating Scale. J Clini Psych. 1994;4(2):98.
26. Sun J, Sun R, Jiang Y, et al. The relationship between psychological health and social support: evidence from physicians in China. PLoS One. 2020;15(1):e0228152. doi:10.1371/journal.pone.0228152 PMID: 31995601; PMCID: PMC6988930.
27. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6 PMID: 1202204.
28. Zhou XX. A Preliminary Study of the Validity and Reliability of the Chinese Version of the Mini-Mental State Examination in Stroke Patients. Master’s Degree Dissertation. Fujian University of Chinese Medicine; 2015.
29. Hoyl MT, Alessi CA, Harker JO, et al. Development and testing of a five-item version of the Geriatric Depression Scale. J Am Geriatr Soc. 1999;47(7):873–878. doi:10.1111/j.1532-5415.1999.tb03848.x PMID: 10404935.
30. Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): recent Evidence and Development of a Shorter Version. Clin Gerontologist. 1986;5(1–2):165–173. doi:10.1300/J018v05n01_09
31. Rinaldi P, Mecocci P, Benedetti C, et al. Validation of the five-item geriatric depression scale in elderly subjects in three different settings. J Am Geriatr Soc. 2003;51(5):694–698. doi:10.1034/j.1600-0579.2003.00216.x PMID: 12752847.
32. Ji F. Relationship Between Self-Perceived Aging, Family Flexibility, and Treatment Compliance in Elderly Patients With Type 2 Diabetes in Rural Communities. Master’s Thesis. Shandong University of Traditional Chinese Medicine; 2019. Doi: 10.27282/d.cnki.gsdzu.2019.000898
33. Foley L, Larkin J, Lombard-Vance R, et al. Prevalence and predictors of medication non-adherence among people living with multimorbidity: a systematic review and meta-analysis. BMJ Open. 2021;11(9):e044987. doi:10.1136/bmjopen-2020-044987 PMID: 34475141; PMCID: PMC8413882. [published correction appears in BMJ Open. 2022 Jul 18;12(7):e044987. doi: 10.1136/bmjopen-2020-044987corr1].
34. van Velsen L, Flierman I, Tabak M. The formation of patient trust and its transference to online health services: the case of a Dutch online patient portal for rehabilitation care. BMC Med Inform Decis Mak. 2021;21(1):188. doi:10.1186/s12911-021-01552-4 PMID: 34118919; PMCID: PMC8199797.
35. Xu XX, Li P, Hou M, et al. Status Quo of Nurse Job Crafting in Tertiary A Hospitals in Xinjiang and Its Influencing Factors. Mil Nurs. 2023;40(09):14–17. doi:10.3969/j.issn.2097-1826.2023.09.004
36. DaSantos A, Goddard C, Ragoobirsingh D. Self-care adherence and affective disorders in Barbadian adults with type 2 diabetes. AIMS Public Health. 2021;9(1):62–72. doi:10.3934/publichealth.2022006 PMID: 35071669; PMCID: PMC8755965.
37. Ley SH, Hamdy O, Mohan V, Hu FB. Prevention and management of type 2 diabetes: dietary components and nutritional strategies. Lancet. 2014;383(9933):1999–2007. doi:10.1016/S0140-6736(14)60613-9 PMID: 24910231 PMCID: PMC4751088.
38. Kenate S, Tesfaye T, Berhanu Mogas S, et al. Validity of Anthropometric Cut-Offs for Early Diagnosis of Dyslipidemia Among Ethiopian Adults. Diabetes Metab Syndr Obes. 2020;13:3831–3837. doi:10.2147/DMSO.S278291 PMID: 33116730; PMCID: PMC7585828
39. Teixeira CR, Zanetti ML, Landim CA, et al. Self-Monitoring Blood Glucose at Home: integrative Literature Review. Rev Eletrônica de Enfermagem. 2009;11(4):1006–1017. doi:10.5216/ree.v11i4.33257
40. Khalafi M, Habibi Maleki A, Symonds ME, Rosenkranz SK, Rohani H, Ehsanifar M. The effects of intermittent fasting on body composition and cardiometabolic health in adults with prediabetes or type 2 diabetes: a systematic review and meta-analysis. Diabetes Obes Metab. 2024;26(9):3830–3841. doi:10.1111/dom.15730 PMID: 38956175.
41. Du Y, Zheng Q, Ou ZH, et al. Efficacy and safety of Morinda officinalis oligosaccharide capsules for depressive disorder: a systematic review and meta-analysis. Braz J Psychiatry. 2021;43(3):306–313. doi:10.1590/1516-4446-2020-0945 PMID: 32997072; PMCID: PMC8136385.
42. Shamim MA, Shukla R, Swami MK, et al. Targeting self-care adherence for glycaemic control in multimorbid type 2 diabetes mellitus with depression using bupropion: a protocol for cross-over randomised controlled trial. BMJ Open. 2024;14(6):e077975. doi:10.1136/bmjopen-2023-077975 PMID: 38834315; PMCID: PMC11163640.
43. Bobo WV, Grossardt BR, Virani S, St Sauver JL, Boyd CM, Rocca WA. Association of Depression and Anxiety With the Accumulation of Chronic Conditions. JAMA Network Open. 2022;5(5):e229817. doi:10.1001/jamanetworkopen.2022.9817 PMID: 35499825; PMCID: PMC9062691.
44. Wang X, Guo J, Liu H, Zhao T, Li H, Wang T. Impact of Social Participation Types on Depression in the Elderly in China: an Analysis Based on Counterfactual Causal Inference. Front Public Health. 2022;10:792765. doi:10.3389/fpubh.2022.792765 PMID: 35433576; PMCID: PMC9010741.
45. Song C, Yao L, Chen H, Song Y, Liu L. Prevalence and factors influencing depression among empty nesters in China: a meta-analysis. BMC Geriatr. 2023;23(1):333. doi:10.1186/s12877-023-04064-0 PMID: 37254062; PMCID: PMC10228112.
46. He Q, Liu Y, Lin K, Zhao F, Guo H, Shen Y. Diabetes self-management and its related factors among Chinese young adults with type 2 diabetes mellitus. Nursing Open. 2023;10(9):6125–6135. doi:10.1002/nop2.1834 PMID: 37221986; PMCID: PMC10416073.
47. Liu X, Zhang L, Chen W. Trends in economic burden of type 2 diabetes in China: based on longitudinal claim data. Front Public Health. 2023;11:1062903. doi:10.3389/fpubh.2023.1062903 PMID: 37143967; PMCID: PMC10151735.
48. Zeng W, Wang C, Chen H, et al. Health status and public health education for internal older migrants in China: evidence from a nationally representative survey. Front Public Health. 2022;10:937361. doi:10.3389/fpubh.2022.937361
49. Gu H, Kou Y, You H, et al. Measurement and decomposition of income-related inequality in self-rated health among the elderly in China. Int J Equity Health. 2019;18(1):4. doi:10.1186/s12939-019-0909-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Cross-Sectional Study of the Correlation Between the Atherogenic Index of Plasma and Nonalcoholic Fatty Liver Disease in Patients with Type 2 Diabetes
Lin J, Li H, Wan Q
Diabetes, Metabolic Syndrome and Obesity 2022, 15:2227-2234
Published Date: 30 July 2022
Diabetes Distress in Adults with Type 2 Diabetes and Multimorbidity: A Scoping Review
Aziz MA, Juniarti N, Kurniawan T, Afriana R
Journal of Multidisciplinary Healthcare 2026, 19:588965
Published Date: 16 February 2026