")
Back to Journals » Infection and Drug Resistance » Volume 16
Assessment of Enrofloxacin Usage and Residue Levels of Enrofloxacin-Ciprofloxacin in Breast and Liver Tissues of Commercial Broilers Sold in Kampala-Uganda
Authors Munanura EI , Ntale M, Wasswa J, Kaggwa B
Received 6 June 2023
Accepted for publication 6 December 2023
Published 12 December 2023 Volume 2023:16 Pages 7629—7639
DOI https://doi.org/10.2147/IDR.S419793
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Edson Ireeta Munanura,1 Muhammad Ntale,2 John Wasswa,2 Bruhan Kaggwa1
1Department of Pharmacy, School of Health Sciences, College of Health Sciences, Makerere University, Kampala, Uganda; 2Department of Chemistry, School of Physical Sciences, College of Natural Sciences, Makerere University, Kampala, Uganda
Correspondence: Edson Ireeta Munanura, Tel +256740511609, Email [email protected]
Background: Human exposure to veterinary drugs like fluoroquinolones occurs due to the presence of their residues in foods from animal sources in varying concentrations. The existence of antibiotic residues in foodstuffs can pose great public health problems to consumers. This study aimed to assess enrofloxacin use patterns and assess residue levels of enrofloxacin/ciprofloxacin in breast muscle and liver tissues of broiler chickens sold for consumption in Kampala capital city.
Methods: This was a cross-sectional study that involved both field survey and laboratory-based methods. The field study involved the use of qualitative and semi-quantitative data collection tools to interview 34 broiler farmers and 10 veterinary drugs vendors. For the determination of enrofloxacin/ciprofloxacin levels, 68 chicken breast and liver tissue samples were collected from main markets in Kampala over one month and analyzed using HPLC-UV.
Results: Enrofloxacin was the most used antibiotic (100%) for the management of poultry diseases, majorly respiratory diseases (100%), salmonella infections (40%), and disease prevention (60%). Over 76% of the farmers knew the meat withdrawal time (WDT) for enrofloxacin, but none of them adhered to this. Over 70% of the farmers reported that the veterinary drugs vendors were not providing meat WDT information. Enrofloxacin/ciprofloxacin residues were identified in 35.3% (12/34) of the muscle and 38.2% (13/34) of the liver tissues analyzed. Of those muscle and liver tissue samples that tested positive, 25% (3/12) and 38.5% (5/13) respectively had drug concentrations higher than the recommended Maximum Residue Limits. The overall mean enrofloxacin/ciprofloxacin concentration in the chicken muscle and liver tissues was 83.6 (± 34.5) μg/kg and 171.5 (± 75.9) μg/kg.
Conclusion: This observed presence of enrofloxacin/ciprofloxacin levels above safety requirements is attributable to inadequate medicines use information provided by veterinary drugs vendors to farmers and also to the non-compliance of some farmers to meat WDT due to the economic implications.
Keywords: withdrawal time, maximum residue limits, enrofloxacin, food safety
Introduction
Enrofloxacin is a fluorinated quinolone carboxylic acid derivative. It is one of the most extensively used quinolones in animal husbandry.1 Quinolones are synthetic antimicrobial agents that have a wide spectrum of activity and are highly efficacious against various bacterial infections especially those caused by gram-negative bacteria in humans and animals.2–6
The antimicrobial activity of quinolones is through inhibition of the DNA gyrase enzyme resulting in inhibition of cell division through the formation of unstable condensation of the DNA configuration.7,8 Enrofloxacin is partly de-ethylated in-vivo to its active form, ciprofloxacin. Ciprofloxacin is used widely in the management of various severe bacterial infections in humans such as typhoid, urinary tract infections, and respiratory tract infections.9,10
In humans, quinolones are extensively used for the treatment of urinary tract infections and enteric infections.3,11 In veterinary medicine, quinolones are routinely used for the treatment of and prophylaxis against bacterial infections in farm animals, especially cattle, pigs, pets, and poultry. Enrofloxacin is widely used in poultry for the treatment of respiratory, renal, and digestive infections at oral doses of 10 mg per body weight per day for 3–10 days.2,3
Human exposure to veterinary drugs like fluoroquinolones occurs due to the presence of their residues in foods from animal sources in varying concentrations. The existence of antibiotic residues in foodstuffs can pose great public health problems to consumers, and so needs to be regulated. These health problems include: microbial resistance to similar drugs used in humans, sensitivity to antibiotics, allergic reactions, and intestinal microflora imbalances. More so, their presence in foodstuffs beyond recommended limits causes great losses to the food industry through product recalls, bans, and legal suits.7,8,11–13
To limit the risks from such exposure, Maximum Residue Levels (MRLs) standards for specific drugs have been set for various animal products in various countries and continental bodies. For instance, in the European Union countries, the enrofloxacin/ciprofloxacin MRL value is 30 ng/g of muscle, liver, and kidney.9,14,15 To achieve the recommended MRL targets, Withdrawal Time (WDT) for animal products for human consumption has been set by manufacturers for their products based on drug residue level studies and regulatory requirements for specific countries or continental bodies. The WDT is the time recommended to allow tissue concentrations of the drug and its metabolite(s) to reduce to levels below the drug’s MRL.2,16 The WDT recommended by the manufacturer for a given product depends on its formulation process, the dose given, the duration of treatment, and the route of administration.2
However, the lack of stringent monitoring mechanisms, the weak regulations in various developing countries, and the lack of will by farmers to comply due to financial implications involved has seen a lot of violations of the WDTs resulting in human exposure to these drugs in doses above the recommended MRLs. For instance, in a study carried out in 2007 in Tehran (Iran) on 270 liver, kidney, and muscle tissue samples of chicken, all the samples tested positive for enrofloxacin. More so, it was discovered that 8.88% of muscle, 13.33% of the liver, and 24.44% of the kidney samples contained enrofloxacin levels higher than the MRL recommended.10,17
Bacterial resistance in humans towards fluoroquinolones has greatly increased, with the driving force being their high-level use in veterinary animals in developing countries without complying with set WDTs.3,4,7,18 Inappropriate use of antibiotics by animal health professionals was estimated to be at 68%, and this improper use was mainly due to non-compliance to recommended doses. This has led to drug inefficiencies also in animals, especially in poultry and cattle, estimated to stand at 47% and 21%, respectively.19 An increase in ciprofloxacin-resistant strains of Campylobacter jejuni and Salmonella enterica in humans has been reported in several countries since the licensing of enrofloxacin for veterinary use.3,4,7,18 Cross-resistance between fluoroquinolones has also been reported among a vast range of microorganisms including both gram-positive and negative bacteria.17
Monitoring of fluoroquinolone drug residues in edible animal products is crucial for proper assessment of human exposure through food to mitigate the resulting human health hazards.8 This study thus focused on the assessment of enrofloxacin use practices amongst broiler farmers, veterinary doctors, and veterinary drug vendors. It also focused on the determination of enrofloxacin/ciprofloxacin residue levels in muscle and liver samples of chickens sold in selected markets within four (4) administrative divisions of Kampala capital city, ie Kawempe, Nakawa, Makindye, and Rubaga.
Materials and Methods
Study Design
This study involved both field and laboratory-based methods. The field study was a cross-sectional study that involved the use of qualitative and semi-quantitative data collection tools to obtain enrofloxacin use practices information from selected veterinary drugs vendors and broiler farmers. The laboratory study involved determining residue levels of enrofloxacin/ciprofloxacin in the liver and breast muscle broiler tissues using HPLC-UV alongside appropriate positive and negative controls.
Sub-Study 1: Assessing Enrofloxacin Use Practices by Selected Veterinary Drugs Vendors and Broiler Chicken Farmers in Kampala’s Capital City
Procedure
From the list of registered poultry farmers in Kampala that was provided by the office of the Director of veterinary services - Kampala Capital City Authority, the leaders of poultry farmers were identified with the help of divisional veterinary extension workers, and from these, 34 boiler farmers were selected randomly for in-depth interviewing. These were from Kawempe, Makindye, and Nakawa divisions. To achieve saturation, 16–24 in-depth interviews are required for qualitative research.20 Ten (10) veterinary personnel practicing in veterinary drugs outlets that were mentioned most by the farmers were also interviewed. The data on enrofloxacin use practices amongst the 34 farmers was collected with the assistance of veterinary officers working in each division by using a farmer’s semi-structured questionnaire. A different semi-structured questionnaire was used to collect data from veterinary drugs vendors (veterinary personnel). For quality assurance purposes, the tools were pre-tested in the Nakawa division using ten (10) chicken farmers, in line with the minimum recommendation of 5–15 participants for pretesting of tools.21 Furthermore, research assistants were adequately trained to ensure consistency throughout the data collection process.
Statistical Data Analysis
Qualitative data was transcribed, coded, and analyzed for emergent themes using thematic analysis, as per recommended approach and steps.22 The data was managed using NVivo (version 10). The descriptive statistical data (means and percentages) was generated for enrofloxacin use practices among broiler farmers regarding; years in the poultry business, antibiotics commonly used, information obtained on the usage of the drug, adherence to MRLs, and challenges encountered when using this drug.
Sub-Study 2: To Determine Residue Levels of Enrofloxacin/Ciprofloxacin in Liver and Breast Muscle Tissues of Broiler Chicken of Selected Markets in Kampala Capital City
Collection and Storage of Samples
Thirty-four (34) broiler chickens (from which 34 muscle and 34 liver tissue samples were obtained) were randomly purchased from four (4) markets in Kampala capital city; ie Kalerwe (Kawempe Division), Kasubi (Rubaga Division), Kibuye (Makindye Division) and Nakawa (Nakawa Division) in two batches separated by a period of three (3) weeks. The data regarding each sample was entered in the samples collection tool. These were slaughtered immediately at the slaughterhouses in these markets and transferred into separate self-sealing bags and transported to the analytical laboratory at the Department of Pharmacy (Makerere University) for sample processing. Samples of breast tissue (10 g) and liver tissue (10 g) were then aseptically obtained from each chicken, placed in a labeled self-sealing bag, and stored at −20 °C. For chicken to provide drug-free tissue samples (Blanks), five (5) birds were purchased from a poultry farm in Bulenga (Wakiso district), with a history of not recently using enrofloxacin, and isolated from the rest for 14 days before being slaughtered and the samples were prepared following the same process described above. Three (3) samples of these were spiked with enrofloxacin 50 µg/kg and quantification was done to confirm absence of residues following the procedures described below.
Chemicals and Reagents
Standards of enrofloxacin and ciprofloxacin of purity of 99.9% and triethylamine (TEA) of purity of 99% were purchased from Alfa Aesar. Acetonitrile (CAN) supra gradient HPLC grade and methanol gradient HPLC grade were purchased from Scharlau Chemie-SA. Sodium hydrogen phosphate (99%), dibasic sodium phosphate (98%), orthophosphoric acid (85%), and hydrochloric acid were purchased from Central Drug house-India.
Equipment and Instrumentation
The chromatographic system comprised a Shimadzu HPLC-UV machine (LC-10AT VP-LC), a Waters Nova-pak® C18 column (4 μm, 3.9mm × 150 mm), and running Shimadzu Class VP software for Windows. Other instruments included a sonicator, weighing balance (Shimadzu), portable pH meter (Thermo scientific Russel RL0600), centrifuges (Biofuse fresco-iteraeus and R23 REMI-research centrifuge), vortex (Stuart scientific sutovortex mixer SA1), Varian® SPE column holder, and a nitrogen evaporator (N-EVPTM 112).
Preparation of Drug Standard Stock Solution, Working Standards, and Quality Control Samples
Stock standard solutions of enrofloxacin (100 μg/mL) were prepared by dissolving enrofloxacin standard (1.0 mg) in methanol (5 mL) in an ultrasonic bath and the final volume was adjusted to 10 mL with de-ionized water. Stock standard solutions of ciprofloxacin were prepared by dissolving ciprofloxacin standard (1.0 mg) in 85% orthophosphoric acid (0.5 mL) in an ultrasonic bath and the final volume was adjusted to 10 mL with de-ionized water. These were stored at 4 °C in volumetric flasks wrapped with aluminum foil. Working standard solutions of enrofloxacin and ciprofloxacin of 10 μg/mL were prepared by dilution of the standard stock solutions with water containing 6.7% methanol-hydrochloric acid (92:2 v/v). Working solutions of enrofloxacin and ciprofloxacin were used to spike muscle and liver blanks to obtain calibration standards at concentrations of 5–500 µg/kg. Quality control samples were made from drug-free muscle and liver samples spiked with a known amount of both enrofloxacin and ciprofloxacin at concentrations of 50, 100, and 500 µg/kg.17,23
Extraction of Samples
Minced muscle sample (2 g) and liver sample (2 g) were weighed and placed in a separated plastic centrifuge tube (12 mL) and phosphate buffer (10 mL) at pH 7.4 was added to each of the muscles and liver tissue samples. The samples were vortexed for 2 min and then centrifuged for 10 min at 4400 g. The sample supernatant was filtered using a syringe filter (FilterBio® PES, 33 mm, 0.45 um). Filtrate (0.5 mL) was applied to a C18 SPE cartridge (Starlab Scientific 40–60 μm, 120 Å, 100 mg/mL, carbon content: 17.6%, Surface area: 300 m2/g) previously activated with methanol (2 mL) followed by de-ionized water (2 mL). Washing was done with water (0.25 mL), then water (0.5 mL), and then acetonitrile (0.5 mL). The cartridges were properly dried by running nitrogen through them for two (2) min and then eluted with methanol containing 2% hydrochloric acid (0.1 mL) followed by de-ionized water (1.4 mL) and mixture transferred to autosampler vials.24 Drug-free muscle and liver samples were also fortified with enrofloxacin/ciprofloxacin to obtain concentrations of 5 −500 µg/kg,23 allowed to stand for 15 min, and extracted following the same procedure described above. The blank (muscle and liver free of drug) samples were extracted after adding deionized water instead of the drug mixture.
Chromatographic Conditions
Analysis was done using a Shimadzu HPLC-UV machine and a Waters Nova-pak® RP-C18 column (4 μm, 3.9 mm × 150 mm) maintained at a temperature of 25 °C. The mobile phase consisted of; water: CAN: TEA (83:14:0.45). To make this mobile-phase mixture, water, and triethylamine (TEA) were mixed and pH adjusted to 2.3 using orthophosphoric acid (85%), and then acetonitrile (CAN) was added. Separation was done in gradient elution mode at a flow rate (1.0 mL/min) with detection set at 277 nm, injection volume (20 µL), and runtime of 12 min.
Identification and Quantitative Analysis
Enrofloxacin and ciprofloxacin were identified using the retention time of unknown substances in comparison with standard drugs. The quantity of enrofloxacin and ciprofloxacin residues was calculated using the formula below:

AUCsample = area under the curve of sample; AUCStd = area under the curve of standard
The total enrofloxacin and ciprofloxacin in each sample were obtained by summing up the concentration of each drug in the specific broiler chicken tissue.
Data Entry and Analysis
The concentrations of enrofloxacin/ciprofloxacin in muscle and liver tissues were entered in Microsoft Excel 2013. The data were then imported into GraphPad Prism Ver 7.0 and mean concentrations plus standard deviations were generated.
Quality Assurance/Control
A calibration curve of the area under the peak versus the nominal concentration of enrofloxacin or ciprofloxacin was plotted and the correlation coefficient (R2) was determined. The Limit of Quantification (LOQ) was defined as the lowest drug concentration, which can be determined with an accuracy of 80–120% and a precision below 20%. The Limit of detection (LOD) was determined by using a method of signal-to-baseline noise (S/N > 3).24
Precision was recorded as the percentage coefficient of variation (CV) set at not more than 15% of nominal concentration. Accuracy was expressed as the percentage of error (PE). Intra-day and inter-day precision and accuracy were determined by analyzing samples 3-fold on the same day and once a day during the 6 days of analysis, respectively.24
Recoveries to test the performance of the method were carried out as follows: samples of meat and liver samples were spiked with enrofloxacin to achieve concentrations of 75, 150, and 250 µg/kg and then processed following the extraction procedure already stated above. The concentrations were obtained from areas of the curve and the result was expressed as a percentage ie (C1 / C2) x 100; Where C1 is measured content and C2 is fortification level.25
Results
Sub-Study 1: Documentation of Enrofloxacin Use Practices by Selected Veterinary Drugs Vendors and Broiler Chicken Farmers in Kampala’s Capital City
The farmers had broiler birds ranging from 50 to 1200 birds (Mean 389.1; SD 289.9) and had on average 11.1 years in the poultry business (SD 7.5; Range 2–30). Most of the farmers interviewed had ordinary-level education and above 26/34 (76.5%). Of the 34 farmers, 55.9% had completed ordinary level, 5.9% had completed advanced level and 14.7% had completed tertiary-level training.
Enrofloxacin (34/34; 100%) and oxytetracycline (22/34; 82.4%) were reported by the farmers as the antibiotics they mostly used in the management of poultry conditions especially respiratory diseases and salmonella infections (Figure 1), and over 80% of these farmers interviewed had used enrofloxacin in the last three months.
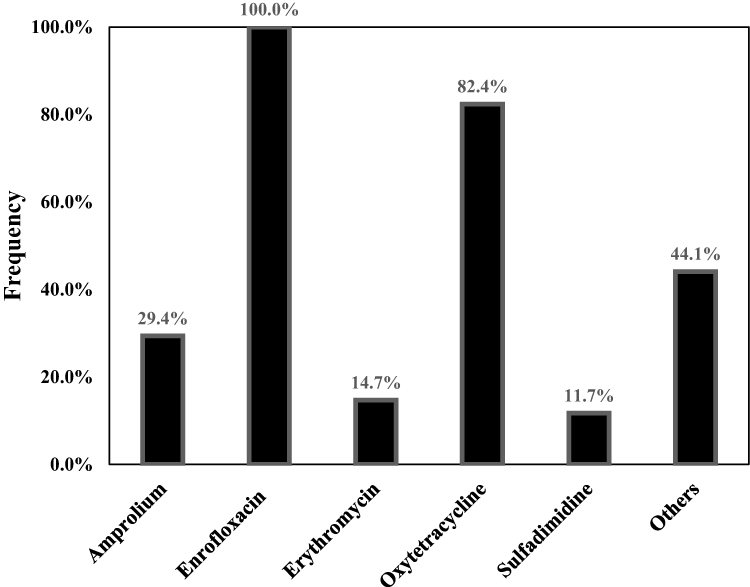 |
Figure 1 Common antibiotics used by farmers to manage poultry diseases. |
The drug vendors reported recommending to farmers enrofloxacin for the management of respiratory diseases (10/10; 100%) for 3–5 days (8/10; 80%), salmonella infections (4/10; 40%) for 5–7 days (3/10; 30%) and disease prevention (6/10; 60%). This was majorly in poultry (10/10; 100%), goats/sheep/cattle (6/10; 60%), and swine (4/10; 40%). The use of enrofloxacin was suggested to an average of 15.6 farmers (± 15.7) a week, and it was requested by on average 15.7 (± 11.8) farmers.
Over 80% of the farmers interviewed reported having used enrofloxacin in the last three months. More so, an average of 16 farmers a week were reported by veterinary drug vendors as having their birds prescribed for enrofloxacin, while an average of 16 farmers a week requested enrofloxacin to manage poultry diseases.
Most of the farmers (24/34; 70.6%) reported that they are never told by the veterinary vendors whether or not they are supposed to wait to slaughter or sell their broiler chickens for some days after treating them using enrofloxacin. Of the 10 vendors interviewed, only 4 (40%) reported giving withdrawal time information to farmers. Over 76% (26/34) of the farmers believed that the meat withdrawal time should be at least 7 days (Figure 2) and most believed that if this was not done, this would pose some health risks to one who consumes such meat.
 |
Figure 2 The meat withdrawal time that farmers thought was appropriate. |
Sub-Study 2: Determination of Enrofloxacin/Ciprofloxacin Residues in Breast Muscle and Liver Tissues of Broiler Chicken in Selected Markets of Kampala Capital City
At a flow rate of 1 mL/min, enrofloxacin and ciprofloxacin were successfully eluted with retention times of 7.7 and 5.5 min, respectively, with no interference from the matrix. The calibration curves for enrofloxacin and ciprofloxacin were linear with a correlation coefficient (R2) range of 0.995 to 0.9999 over the concentrations of 50–500 µg/kg (Figure 3).
 |
Figure 3 Standard curves for ciprofloxacin (a and b) and enrofloxacin (c and d) at concentrations 10–500 µg/kg in muscle and liver matrix, respectively. |
The mean analytical spike recovery was 86.5% (SD = 7.5%, n = 3) and this was within the acceptable range of 80–120%. The Intra and inter-day precision, and accuracy were done using ciprofloxacin and enrofloxacin standards, respectively (Table 1). The LOQ for ciprofloxacin and enrofloxacin was 55 and 52 µg/kg, respectively.
 |
Table 1 Intra and Inter-Day Precision and Assessment Variation (n = 5) |
The broiler chicken collected for analysis in this study had a weight range of 0.91–1.56 kg (Mean = 1.1 kg; SD = 0.193). The liver and muscle tissues were obtained from chicken purchased from Nakawa, Kibuye, Kasubi, and Kalerwe markets in Kampala capital city. The overall mean concentration of enrofloxacin/ciprofloxacin in the broiler chicken muscle and liver tissues was found to be 83.6 (±34.5) µg/kg and 171.5 (±75.9) µg/kg respectively (n = 34). The mean enrofloxacin/ciprofloxacin concentration ±SD in the different chicken samples from the different markets is shown in Table 2.
 |
Table 2 Chicken Samples Tissue Collection Sources and Mean Tissue Concentrations |
Of the 34 samples of muscle and 34 liver analyzed, 35.3% (12) and 38.2% (13) respectively tested positive for enrofloxacin/ciprofloxacin. Furthermore, of those samples of muscle and liver that tested positive for enrofloxacin/ciprofloxacin, 25% (3/12) and 38.5% (5/13) respectively had drug concentrations higher than the MRLs (Table 3, Figures 4 and 5).
 |
Table 3 Enrofloxacin/Ciprofloxacin Residue Data in Broiler Breast Muscle and Liver Tissue Samples Analyzed |
 |
Figure 4 Enrofloxacin/ ciprofloxacin concentrations (µg/kg) in breast muscle tissues analyzed (n=34). |
 |
Figure 5 Enrofloxacin/ ciprofloxacin concentrations (µg/kg) in Liver tissues of broiler chicken analyzed (n=34). |
Discussion
Enrofloxacin is one of the most used antibiotics in the management of various diseases in poultry in Uganda and the world over. In our study, 100% of the farmers were using enrofloxacin as the primary antibiotic of choice to manage respiratory and gut infections. In related studies in Ghana and Cameroon, 11% and 57.1% of farmers respectively were reported to be using enrofloxacin for the management of poultry diseases, ie treatment and prevention.26,27
The occurrence of high levels of drugs such as enrofloxacin/ciprofloxacin in foods from animal sources beyond set Maximum Residue Levels (MRLs) is a clear indication of non-adherence to recommended withdrawal times by farmers and lack of stringent mechanisms by the concerned regulatory agencies mandated to ensure compliance. Antibiotics like enrofloxacin, erythromycin, doxycycline, and others are heat stable and thus will be present in substantial amounts in cooked food made from recently drug-exposed animals.28 Enrofloxacin and its metabolite ciprofloxacin remain unchanged when boiled in water at 100 °C for three (3) hours, and the method of cooking (ie microwaving, roasting, boiling, grilling, or frying) does not have a significant effect on the levels of enrofloxacin residues in chicken.10 The withdrawal period for animal products post-treatment with such antibiotics as such cannot be avoided.
In this study, 8.8% and 14.7% of the chicken muscle and liver tissues respectively had total fluoroquinolone (enrofloxacin-ciprofloxacin) levels higher than the EU recommended limits 100 and 200 µg/kg in muscle and liver tissues, respectively.29 This limit is less stringent than that of the USA of 30 µg/kg2 and Japan of 10 µg/kg30 for all chicken tissue. The number of samples positive for enrofloxacin/ciprofloxacin, the proportion of positive samples with levels higher than the MRLs, and the mean concentrations determined in our study were lower than those reported by a related study by Aslam et al and but comparable with a study done in Iran by Mogahadam et al.
In the study by Aslam et al, 52% of the muscle and 78.7% of the liver tissues were positive for enrofloxacin, with 58.3% and 71.2% of these muscle and liver tissues respectively having values higher than the MRLs. In that same study, the average concentrations in muscle and liver tissues respectively were 208 and 527 µg/kg respectively31 as compared to those found by our study which were 83.6 µg/kg and 171.5 µg/kg respectively. In the study by Mogahadam et al, 52% of the liver tissues were positive for enrofloxacin/ciprofloxacin, with a mean concentration of 156.4 µg/kg.
Our study involved using broiler chicken kept at the stalls in markets. Such broiler chickens are not slaughtered immediately when delivered from the farm and can be in cages for weeks and as such may have enough time to metabolize the drugs before they are purchased for slaughter unlike those procured for slaughter directly from the farms. This could explain why the study by Aslam et al found higher fluoroquinolone residue levels as compared to our study. However, there is also the possibility that chicken market vendors could treat the birds at their stalls in case they get infections before they are bought off.
The high chicken tissue positivity rates for enrofloxacin-ciprofloxacin levels found in this study relate to the high non-adherence to recommended withdrawal time that was at 100% (34/34 farmers). Non-adherence rates in related studies in Ghana and Cameroon were reported to be at 42% and 43%, respectively.26,27 The high non-adherence rate in our study is not driven by a lack of emphasis by veterinary medicine vendors on recommended meat withdrawal times to farmers during medicine purchases but rather by the reluctance of farmers to adhere precipitated by the absence of enforcement mechanisms in Uganda. Most of the farmers (76%) were aware of the enrofloxacin brands’ meat withdrawal time of at least 7 days and the related health risks to humans. In a related study in Uganda, despite 53.3% of farmers being aware of meat withdrawal time, most were still selling or consuming poultry products during the withdrawal period.32 The non-adherence is majorly driven by the unwillingness to undertake the extra cost of feeding already mature birds for the extra days of the withdrawal period since this would make the business less profitable. Such challenges associated with non-adherence are the reasons enrofloxacin was banned in 2005 in the USA for use in chickens and has never been licensed for use in chickens in Australia.3,33
Conclusion
Chicken sold in markets within Kampala capital city potentially contain enrofloxacin/ciprofloxacin residues, with a small proportion having levels above the maximum residue limit of 100 and 200 µg/kg for muscle and liver tissues, respectively. Veterinary medicine vendors largely do not give broiler farmers the pre-requisite information regarding meat withdrawal times. Even though over 76% of the farmers were aware of the appropriate meat withdrawal time, all were not adhering to this health safety recommendation, and this as such creates serious health concerns for humans who consume these broiler chickens with drug levels above the MRLs. Considering the high non-compliance of farmers with meat withdrawal time recommendations, there is a need for routine monitoring of antibiotic residues in foods from animal sources, and this can be achieved through using portable and easy-to-use methods of analysis such as antibiotics ELISA test kits.
Ethics Approval and Informed Consent
Written informed consent was obtained from the survey respondents to participate in this study and for the publication of this report and accompanying images. Research approval was provided by the Uganda National Council of Science and Technology (A538) and the Makerere University School of Health Sciences-Institutional Review Board (#SHSREC REF:2016-020).
Acknowledgments
This manuscript originates from an MSc. Chemistry thesis submitted to Makerere University.34 We acknowledge the support of the analytical laboratory staff and administration at the Department of Pharmacology and Department of Pharmacy, Makerere University which provided the infrastructure and technical support for the laboratory analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by the Pharmaceutical Society of Uganda (PSU) and One Health Central and Eastern Africa (OHCEA).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Grabowski Ł, Gaffke L, Pierzynowska K, et al. Enrofloxacin-the ruthless killer of eukaryotic cells or the last hope in the fight against bacterial infections? Int J Mol Sci. 2022;23(7):3648. doi:10.3390/ijms23073648
2. San Martin B, Cornejo J, Lapierre L, et al. Withdrawal time of four pharmaceutical formulations of enrofloxacin in poultry according to different maximum residues limits. J Vet Pharmacol Ther. 2010;33(3):246–251. doi:10.1111/j.1365-2885.2009.01127.x
3. Cheng AC, Turnidge J, Collignon P, Looke D, Barton M, Gottlieb T. Control of fluoroquinolone resistance through successful regulation, Australia. Emerg Infect Dis. 2012;18(9):1453–1460. doi:10.3201/eid1809.111515
4. Piddock LJ. Fluoroquinolone resistance: overuse of fluoroquinolones in human and veterinary medicine can breed resistance British. Med J. 1998;317(7165):1029–1030. doi:10.1136/bmj.317.7165.1029
5. Roybal J, Walker CC, Pfenning AP, et al. Concurrent determination of four fluoroquinolones in catfish, shrimp, and salmon by liquid chromatography with fluorescence detection. J AOAC Int. 2002;85(6):1293–1301. doi:10.1093/jaoac/85.6.1293
6. Reyes-Herrera I, Schneider MJ, Blore PJ, Donoghue DJ. The relationship between blood and muscle samples to monitor for residues of the antibiotic enrofloxacin in chickens. Poult Sci. 2011;90(2):481–485. doi:10.3382/ps.2010-01057
7. Malorny B, Schroeter A, Helmuth R. Incidence of quinolone resistance over the period 1986 to 1998 in veterinary salmonella isolates from Germany. Antimicrob Agents Chemother. 1999;43(9):2278–2282. doi:10.1128/AAC.43.9.2278
8. Sheng W, Xia X, Wei K, Li J, Li QX, Xu T. Determination of marbofloxacin residues in beef and pork with an enzyme-linked immunosorbent assay. J Agric Food Chem. 2009;57(13):5971–5975. doi:10.1021/jf900940n
9. Lucchetti D, Fabrizi L, Guandalini E, et al. Long depletion time of enrofloxacin in rainbow trout (Oncorhynchus mykiss). Antimicrob Agents Chemother. 2004;48(10):3912–3917. doi:10.1128/AAC.48.10.3912-3917.2004
10. Lolo M, Pedreira S, Miranda JM, et al. Effect of cooking on enrofloxacin residues in chicken tissue. Food Addit Contam. 2006;23(10):988. doi:10.1080/02652030600904894
11. Yu H, Tao Y, Chen D, et al. Simultaneous determination of fluoroquinolones in foods of animal origin by a high performance liquid chromatography and a liquid chromatography tandem mass spectrometry with accelerated solvent extraction. J Chromatogr B Biomed Sci. 2012;885–886:150–159.
12. Qiao F, Sun H. Simultaneous extraction of enrofloxacin and ciprofloxacin from chicken tissue by molecularly imprinted matrix solid-phase dispersion. J Pharm Biomed Anal. 2010;53(3):795–798. doi:10.1016/j.jpba.2010.06.008
13. Morales-Gutiérrez FJ, Hermo MP, Barbosa J, Barrón D. High-resolution mass spectrometry applied to the identification of transformation products of quinolones from stability studies and new metabolites of enrofloxacin in chicken muscle tissues. J Pharm Biomed Anal. 2014;92:165–176. doi:10.1016/j.jpba.2014.01.014
14. Le Boulaire S, Bauduret J-C, Andre F. Veterinary drug residues survey in meat: an HPLC method with a matrix solid phase dispersion extraction. J Agri Food Chem. 1997;45(6):2134–2142. doi:10.1021/jf9604192
15. Posyniak A, Zmudzki J, Niedzielska J. Liquid chromatography analysis of enrofloxacin and ciprofloxacin in chicken blood spotted on filter-paper disks. Anal Technol Biomed Life Sci. 2002;780(2):309–314. doi:10.1016/S1570-0232(02)00540-8
16. Paschoal JA, Quesada SP, Goncalves LU, Cyrino JE, Reyes FG. Depletion study and estimation of the withdrawal period for enrofloxacin in pacu (Piaractus mesopotamicus). J Vet Pharmacol Ther. 2013;36(6):594–602. doi:10.1111/jvp.12043
17. Salehzadeh F, Salehzadeh A, Rokni N, Madani R, Golchinefar F. Enrofloxacin residue in chicken tissues from Tehran slaughterhouses in Iran. Pak J Nutr. 2007;6(4):409–413. doi:10.3923/pjn.2007.409.413
18. Attari VE, Abbasi MM, Abedimanesh N, Ostadrahimi A, Gorbani A. Investigation of enrofloxacin and chloramphenicol residues in broiler chickens carcasses collected from local markets of tabriz, Northwestern Iran. Health Promot Perspect. 2014;4(2):151–157. doi:10.5681/hpp.2014.020
19. Mouiche MMM, Njingou BZN, Moffo F, Mpouam SE, Feussom JMK, Awah-Ndukum J. Veterinary pharmacovigilance in sub-Sahara Africa context: a pilot study of adverse reactions to veterinary medicine in Cameroon. BMC Veter Res. 2019;15(1):301. doi:10.1186/s12917-019-2043-1
20. Hagaman AK, Wutich A. How many interviews are enough to identify metathemes in multisited and cross-cultural research? Another perspective on Guest, Bunce, and Johnson’s (2006) landmark study. Field Methods. 2017;29(1):23–41. doi:10.1177/1525822X16640447
21. Perneger TV, Courvoisier DS, Hudelson PM, Gayet-Ageron A. Sample size for pre-tests of questionnaires. Qual Life ReS. 2015;24(1):147–151. doi:10.1007/s11136-014-0752-2
22. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
23. Moghadam RN, Arefhosseini SR, Javadi A, et al. Determination of enrofloxacin and ciprofloxacin residues in five different kinds of chicken tissues by dispersive liquid-liquid microextraction coupled with HPLC. Iran J Pharma Res. 2018;17(4):1182–1190.
24. Manceau J, Gicquel M, Laurentie M, Sanders P. Simultaneous determination of enrofloxacin and ciprofloxacin in animal biological fluids by high-performance liquid chromatography. Application in pharmacokinetic studies in pig and rabbit. J Chromatogr B Biomed Sci. 1999;726(1–2):175–184. doi:10.1016/S0378-4347(99)00026-2
25. de Assis DCS, da Silva GR, Lanza IP, et al. Evaluation of the presence and levels of enrofloxacin, ciprofloxacin, sulfaquinoxaline and oxytetracycline in broiler chickens after drug administration. PLoS One. 2016;11(11):e0166402. doi:10.1371/journal.pone.0166402
26. Boamah V, Agyare C, Odoi H, Dalsgaard A. Antibiotic practices and factors influencing the use of antibiotics in selected poultry farms in Ghana. J Antimicrob Agents. 2016;2016:1.
27. Kamini MG, Keutchatang FT, Mafo HY, Kansci G, Nama GM. Antimicrobial usage in the chicken farming in Yaoundé, Cameroon: a cross-sectional study. Int J Food Contam. 2016;3(1):10. doi:10.1186/s40550-016-0034-6
28. Lim WS, Kim DH, Jin SY, et al. A case of fixed drug eruption due to doxycycline and erythromycin present in food. Allergy Asthma Immunol Res. 2013;5(5):337–339. doi:10.4168/aair.2013.5.5.337
29. EU-No37/2010. Commission RegulatioN (EU) No 37/2010 of 22nd December 2009 on pharmacologically active substances and their classification regarding maximum residue limits in foodstuffs of animal origin. Brussels: Official Journal of the European Union; 2010:1–71.
30. MHWJp. Specifications and standards for food, food additives. Notification no. 499; 2005. Available from: https://www.mhlw.go.jp/english/topics/foodsafety/positivelist060228/dl/n03.pdf.
31. Aslam B, Kousar N, Javed I, et al. Determination of enrofloxacin residues in commercial broilers using high performance liquid chromatography. Int J Food Prop. 2016;19(11):2463–2470. doi:10.1080/10942912.2015.1027922
32. Bashahun DGM, Odoch TA. Assessment of antibiotic usage in intensive poultry farms in Wakiso District, Uganda. Livest Res Rural Dev. 2015;27:12.
33. Nelson JM, Chiller TM, Powers JH, Angulo FJ. Fluoroquinolone-resistant campylobacter species and the withdrawal of fluoroquinolones from use in poultry: a public health success story. Clin Infect Dis. 2007;44(7):977. doi:10.1086/512369
34. Munanura EI. Assessing Enrofloxacin Use Practices and Residue Levels of Enrofloxacin/Ciprofloxacin in Breast and Liver Tissues of Broiler Chicken Sold in Selected Markets in Kampala Capital City-Uganda [MSC]. Kampala: Department of Chemistry, Makerere University; 2022.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.