Back to Journals » International Journal of General Medicine » Volume 16
Assessment of Electrocardiographic Changes and Associated Factors Among Thyroid Dysfunction Patients Attending Jimma Medical Center, Southwest Ethiopia: A Cross-Sectional Study
Authors Zeleke M, Badanie A, Asefa ET, Reta Demissie W ![]() , Chala G
, Chala G ![]() , Aman H, Feyisa TO
, Aman H, Feyisa TO ![]() , Habte ML
, Habte ML ![]()
Received 7 February 2023
Accepted for publication 23 May 2023
Published 26 May 2023 Volume 2023:16 Pages 2035—2046
DOI https://doi.org/10.2147/IJGM.S407513
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Mastewal Zeleke,1 Almaz Badanie,2 Elsah Tegene Asefa,3 Wondu Reta Demissie,2 Getahun Chala,1 Husen Aman,4 Teka Obsa Feyisa,5 Mezgebu Legesse Habte5
1Department of Medical Physiology, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 2Department of Biomedical Sciences, College of Medicine and Health Sciences, Jimma University, Jimma, Ethiopia; 3Department of Medicine, College of Medicine and Health Sciences, Jimma University, Jimma, Ethiopia; 4Department of Human Anatomy, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 5Department of Medical Biochemistry, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Mastewal Zeleke, Department of Medical Physiology, College of Health and Medical Sciences, Haramaya University, P.O.Box:235, Harar, Harari Regional State, Ethiopia, Tel +251911142917, Email [email protected]
Background: Thyroid dysfunction (TD) is a metabolic manifestation related to either excessive or inadequate production of thyroid hormones. It has been widely proven to have comorbidities like cardiovascular disease. An electrocardiograph is a simple investigative instrument used to assess cardiac status to prevent complications in the later stages of the disease.
Objective: To assess electrocardiogram (ECG) changes and associated factors among TD patients.
Methods: An institution-based cross-sectional study was conducted among 273 TD patients attending Jimma Medical Center from October 11 to December 11, 2021. An ECG tool with 12 leads was used to assess the cardiac status, and a semi-structured questionnaire was used to assess sociodemographic, behavioral, and comorbidity variables. Bodyweight, height, waist circumference (WC), hip circumference (HC), and blood pressure variables were recorded, and body mass index (BMI) and waist-to-hip ratio (WHR) were calculated.
Results: Out of a total of 273 analyzed and interpreted ECG results by the cardiologists, 185 (67.8%) had ECG alterations. The most common types of ECG changes were arrhythmia 153 (56%), followed by myocardial infarction 74 (27.1%), ventricular hypertrophy [left 20 (7.3%) and right 15 (5.5%)], left atrial enlargement 3 (1%), axis deviation, and other abnormalities 24 (8.8%) and 18 (6.6%), respectively. The identified predictor variables for the ECG changes were the age group of 41 to 60 years old [AOR = 2.5, 95% CI: 1.25, 5.05], being female [AOR = 2.7, 95% CI: 1.28, 5.59], having diabetes mellitus [AOR = 4.25, 95% CI: 1.6, 11.2], and not starting the treatment [AOR = 8.6, 95% CI: 3.45, 21.6].
Conclusion: This study revealed that the prevalence of ECG changes was high among TD patients. The most common type of ECG change observed was arrhythmia followed by myocardial infarction. The age range of 41– 60 years old, being female, having diabetes mellitus, and not starting the treatment were significantly associated with the ECG changes. Implementing an efficient noninvasive screening of cardiac status can detect unrecognized and asymptomatic cardiac impairment in TD patients.
Keywords: cardiovascular disease, electrocardiogram, Ethiopia, thyroid dysfunction
Introduction
Thyroid dysfunction (TD) is a metabolic manifestation related to either excessive or inadequate production of thyroid hormones by the thyroid gland.1 This condition results in hyperthyroidism or hypothyroidism, which resulted due to pathological processes within the thyroid gland.2 Thyroid dysfunction is a global health problem that significantly impacts well-being, as it is one of the most common endocrine disorders next to diabetic mellitus accounting for about 30% to 40%3 of the endocrine disorders. According to the World Health Organization (WHO) report, the prevalence of TD was highest in Africa, which represents over 25% of the global burden of the disease.4 In Ethiopia, goiter is a major public health problem accounting for more than 30%.5 The risk factors such as age, sex, genetics, smoking status, alcohol consumption, and exposure to therapeutic drugs influence the global epidemiology of thyroid disease.6,7
Thyroid dysfunction is widely documented to be associated with a variety of cardiovascular disorders, which are the leading cause of death worldwide.8 Cardiovascular disorders are one of the most common noncommunicable diseases, which are the leading cause of death worldwide, accounting for 73.4% of all deaths in the world.9 A systematic review and meta-analysis studies revealed that the prevalence of cardiovascular diseases was around 20% in Ethiopia.10
Universally, the spread of TD is at the highest rate in developing nations including Ethiopia. This will exacerbate the risk of developing cardiovascular complications, which is a major public health concern. To our knowledge, in Ethiopia, there is a limited study conducted to assess electrocardiographic changes and associated factors among TD patients. Thus, this study aimed to assess the spectrum of electrocardiographic changes and associated factors among TD patients.
Materials and Methods
Study Population
A hospital-based cross-sectional study design was conducted on randomly selected 273 TD patients attending Jimma Medical Center (JMC) follow-up clinic, Jimma, Oromia regional state, Ethiopia from October 11 to December 11, 2021. The study was conducted following the guidelines laid down in the Declaration of Helsinki, and all procedures involving human subjects were approved by the ethical review board of Jimma University, Institute of Health, with the reference number PGC/510/202. After outlining the study’s objectives and purpose, written informed consent was obtained from all subjects before participation, and was informed about the confidentiality of the information they gave. All TD patients, who were willing to take part in the study, attended the JMC follow-up clinic were included in the study. The TD patients with age less than 18 years old, with known cardiac disease and undergone thyroidectomy, and pregnant women were excluded from the study.
Operational Definitions
Physically Active
Consumption of greater than 600 metabolic equivalents of energy per week (150 minutes of moderate and 75 minutes of vigorous physical activity in a week).11
Normal Sinus Rhythm
A regular heart rate between 50 and 100 beats per minute with normal P-wave, PR-interval, QRS complex, T-waves, and P-waves before each QRS complex.12
ECG Alterations
Any changes in the ECG beyond the normal sinus rhythm based on Minnesota coding criteria.13
Data Collection Tool and Technique
The data were collected by trained BSc nurses at the JMC follow-up clinic. The data collectors have given orientation about the objectives and purpose of the study to the respondents and took informed written consent before data collection. The data collection was conducted through a face-to-face interview using semi-structured questionnaires for assessing the risks of CVDs among TD patients. The sociodemographic factors, behavioral factors, and comorbidity data were collected, and information related to medical conditions was reviewed from patients’ medical charts. The data were collected by applying all COVID-19 prevention protocols such as wearing a face mask, gloves, gown, hand washing, and using sanitizer before and after each procedure.14
Supine resting ECG was assessed using a standard 12 lead ECG machine (NIHON KOHDEN, CARDIOFAX S, INDIA) and calibrated on 1mv for a 10mm (0.1Mv/mm) at a speed of 25mm/sec. The suggested procedure for electrocardiography followed the standard manual for Minnesota as a reference. The ECG results were analyzed for recording errors and manually interpreted by a cardiologist.15 The participants who had ECG alterations were referred to a cardiac clinic for further screening and treatment. Blood pressure (BP) was measured three times in a sitting position from the left arm using accuracy validated automated BP monitoring devices after the patient rests for 5 minutes before taking the measurement and 3 minutes before repeating the subsequent measurements.16 Body mass index (BMI) (kg/m2) was computed from the client’s height (m) and weight (kg). The weight was measured with a validated weighing Scale with a stadiometer (VMED, TAIWAN), and height was measured for standing patients with no shoes with their back against the wall, heels together, and eyes focused forward. Waist circumference (WC) at a midpoint between the costal margin and iliac crest at the end of expiration, and hip circumference (HC) was measured at a maximum circumference at the level of the greater trochanter on both sides using a non-stretchable measuring tape.17
Statistical Analysis
After the template was created, the data were checked, coded, and entered into Epi data version 4.6, and exported to SPSS version 25 for analysis. The descriptive statistics such as frequency, percentage, mean, and standard deviation were used to describe the findings. Binary logistic regression analysis was done to observe the association of each independent variable to the dependent variable and variables with p-values of less than 0.25 were identified. The identified variables were entered into a multivariable logistic regression model to identify the independent factors associated with the ECG alterations. The 95% confidence interval (CI) and an associated factor with a p-value of less than 0.05 were considered statistically significant.
Results
Socio-Demographic Characteristics of the Participants
Out of a total of 273 TD patients, 210 (76.9%) were females, 170 (62.3%) were in the age group of 41–60 years old, 170 (62.3%) were married and 147 (53.8%) were rural dwellers. The average age of the respondents was 47.02 ±10.47 years with a minimum age of 22 years and a maximum age of 68 years old. Regarding the educational status of the respondents, 125 (45.8%) were not attended formal education (Table 1).
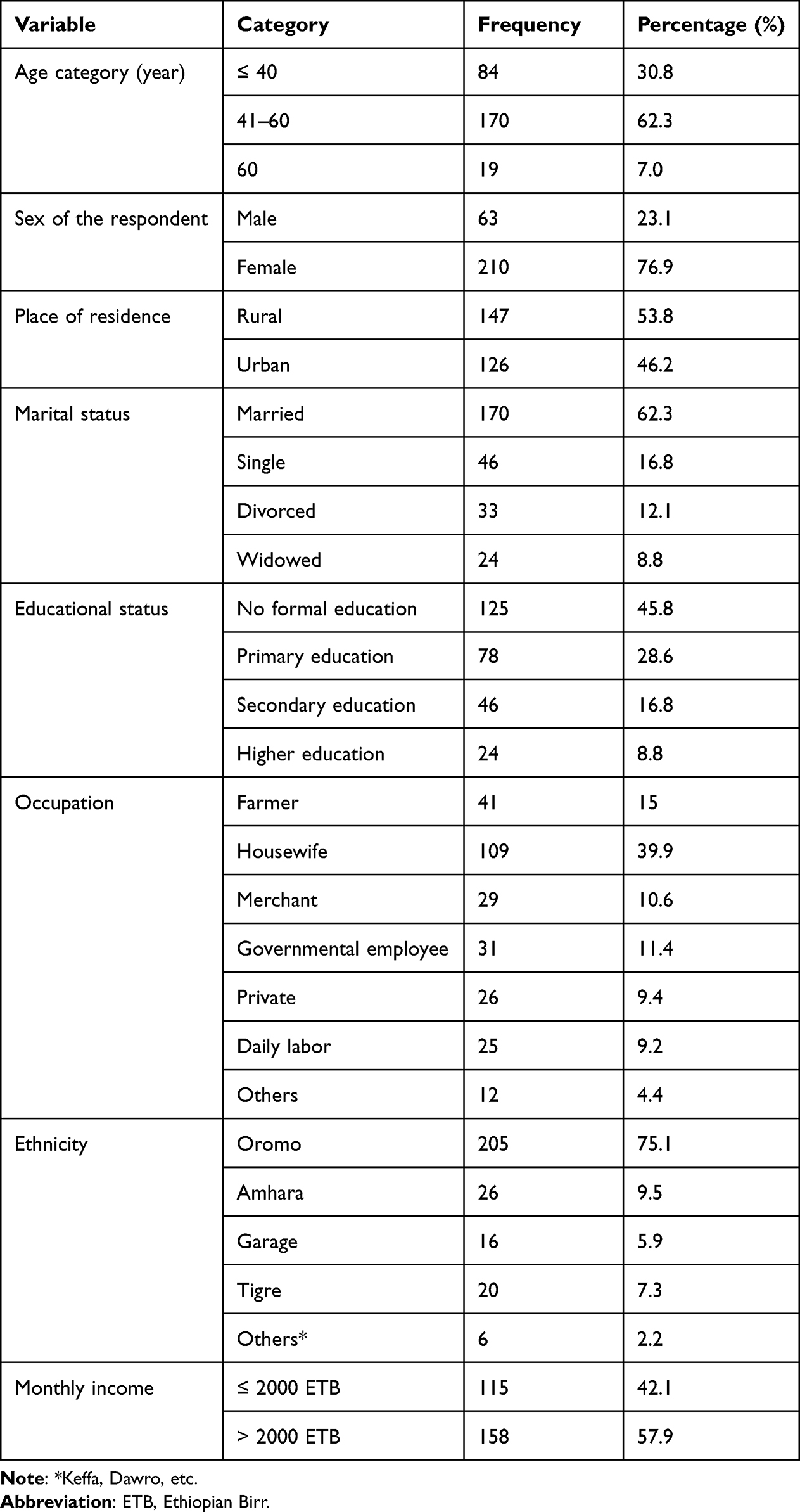 |
Table 1 Sociodemographic Characteristics of TD Patients Attending JMC Follow-Up Clinics from October–December 2021 (N = 273) |
Behavioral Characteristics of the Respondents
Most of the respondents, 209 (76.6%), were nonsmokers and 168 (61.5%) were non-alcohol users. Non-khat chewer accounts for 124 (45.4%) of the respondents. One hundred thirty-two (48.4%) of the physically active respondents consume greater than 600 metabolic equivalents of energy per week (150 minutes of moderate and 75 minutes of vigorous physical activity in a week) (Table 2).
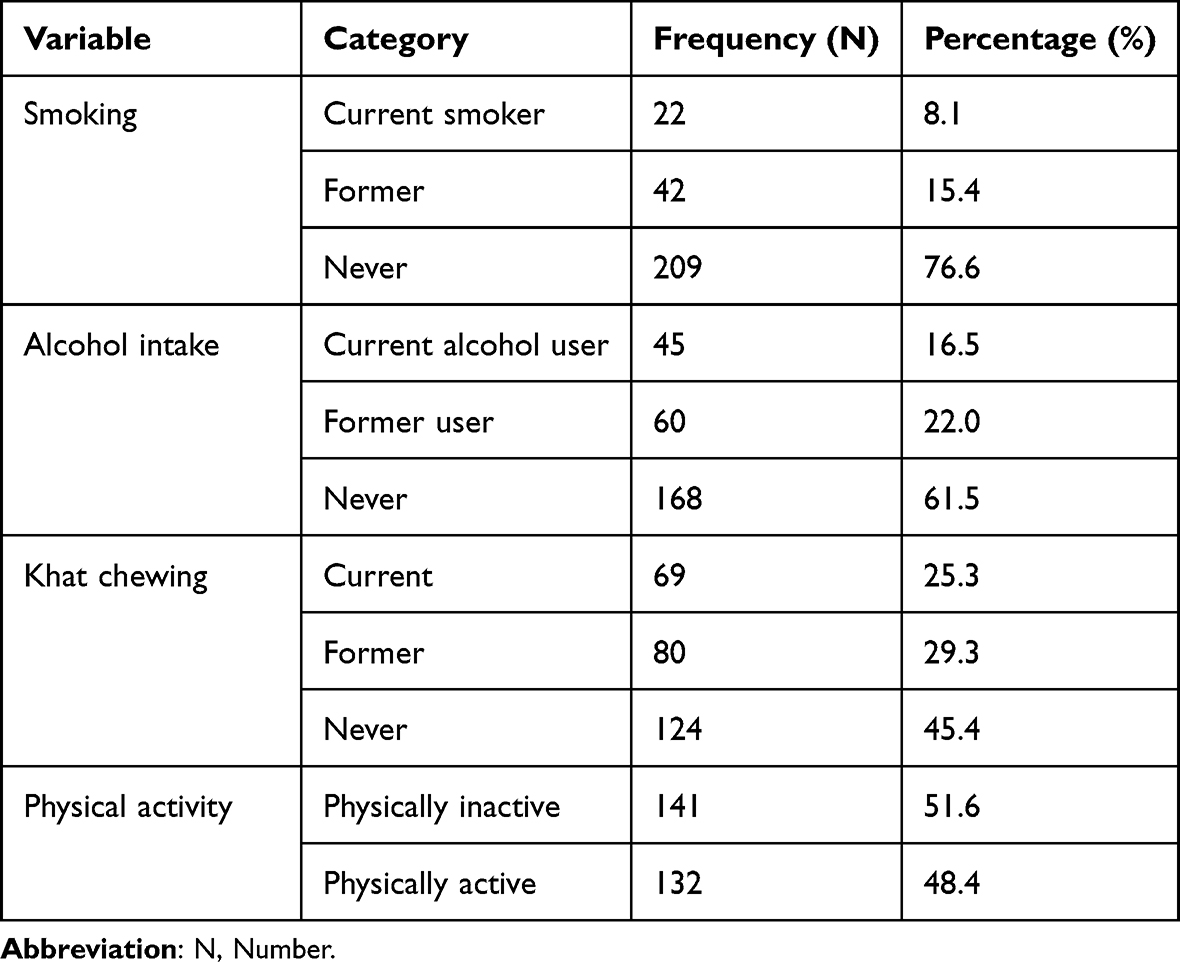 |
Table 2 Behavioural Characteristics of TD Patients Attending JMC Follow-Up Clinics from October–December 2021 (N = 273) |
Anthropometric and BP Measurements of the Respondents
In this study, the average weight, height, and BMI of the 273 TD patients were 55 ± 10.72 kg, 1.58 ± 0.06m, and 21.96 ± 3.82 kg/m2, respectively. The average systolic BP (SBP) was 122.87 ±16.75 mmHg, while the average diastolic BP (DBP) was 76.17 ± 9.31 mmHg (Table 3).
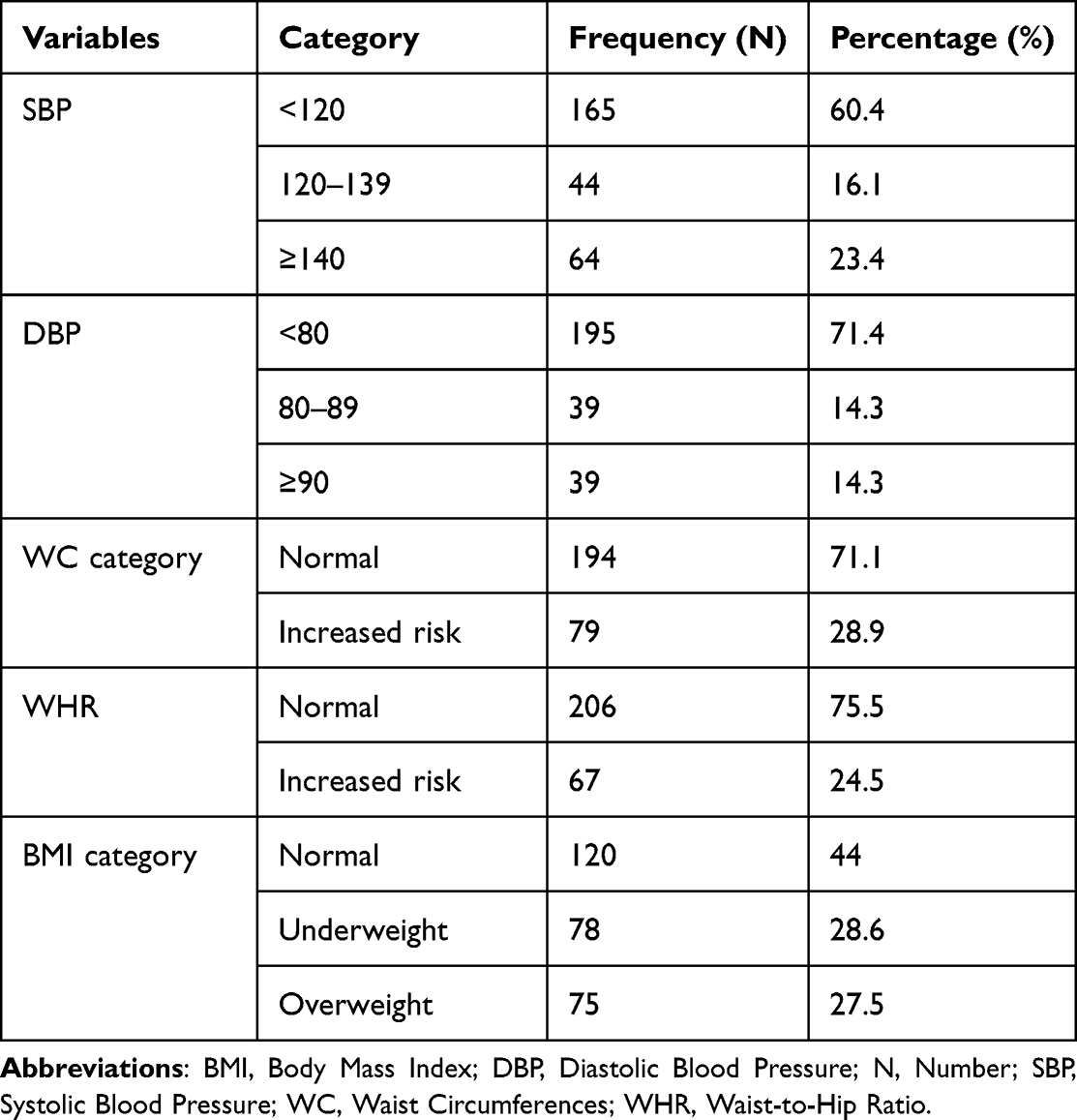 |
Table 3 Distribution of Anthropometric and BP of TD Patients Attending JMC Follow-Up Clinics from October–December 2021 (N = 273) |
Thyroid Dysfunction Status of the Respondents
Of the total of 273 TD patients, about 72.5% were hyperthyroid. The patients who had not started antithyroid medication account for 104 (38%), and the patients who had started the treatment account for 169 (62%). In this study, newly diagnosed TD patients account for 81 (29.7%), and comorbidities like hypertension and diabetes mellitus account for 64 (23.4%) and 56 (20.5%), respectively (Table 4).
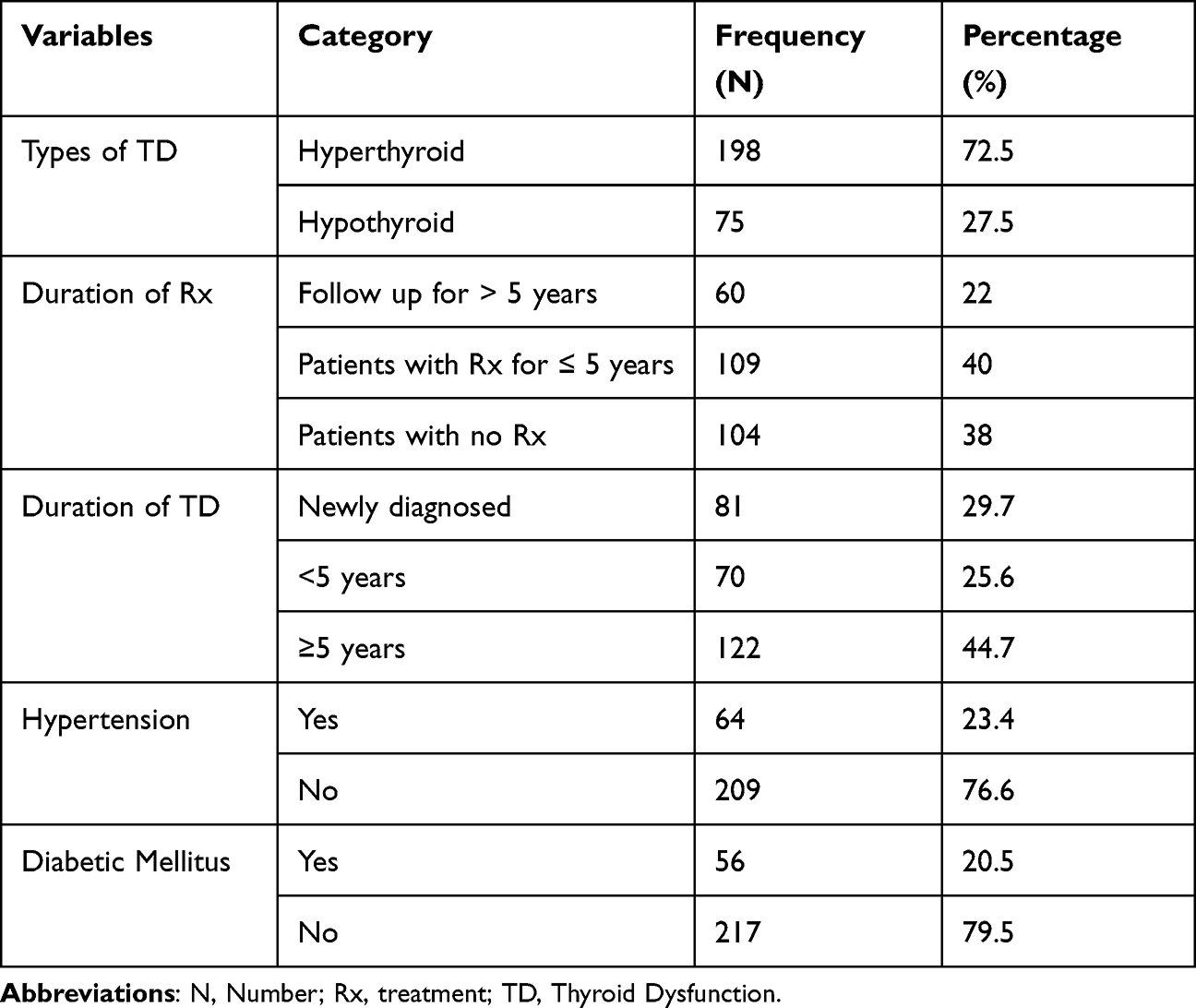 |
Table 4 Thyroid Dysfunction Status of the TD Patients Attending JMC Follow-Up Clinics from October–December 2021 (N = 273) |
ECG Alterations Among TD Patients
Out of a total of 273 analyzed and interpreted ECG results by the cardiologists, about 185 (67.8%) had ECG alterations, while 88 (32.2%) of patients had normal ECG. From this, a higher prevalence (57.9%) was observed in female participants, 50.2% in hyperthyroid patients, 48.7% in participants with the age range of 41–60 years old, and 36.6% of patients with more than five years of TD.
Types of ECG Alterations Among TD Patients
In this study, based on Minnesota coding criteria, the most common forms of ECG alterations observed were Arrhythmia,153 (56%), followed by myocardial infarction (MI), 74 (27.1%), enlargements of heart chamber as Left atrial enlargement (LAE), 3 (1%), ventricular hypertrophy (VH) [Left VH, 20 (7.3%), and right VH, 15 (5.5%)] and axis deviation, 24 (8.8%). It was observed that one patient might have more than one type of ECG alterations. Among the arrhythmia as one type of ECG alterations, different subtypes were evaluated as per Minnesota coding criteria from this sinus origin arrhythmia, supraventricular origin arrhythmia, conduction blocks, and Preexcitation Syndromes (PES)/ Wolff-Parkinson White Syndrome (WPWS) were interpreted with the frequency of 25.3%, 16.4%, 9.5%, and 1.5%, respectively. The other interpreted ECG alterations were MI (ST-wave changes (15%), T-wave inversion (9.5%), and prolonged QTc-interval (2.5%)). Heart chamber enlargements and hypertrophy as left and right VH account for 7.3% and 5.5%, respectively, while LAEs account for 1%. The axis deviations, which are right- and left-axis deviations, were seen among 24 TD patients and interpreted by frequencies of 5.1% and 3.6%, respectively (Table 5).
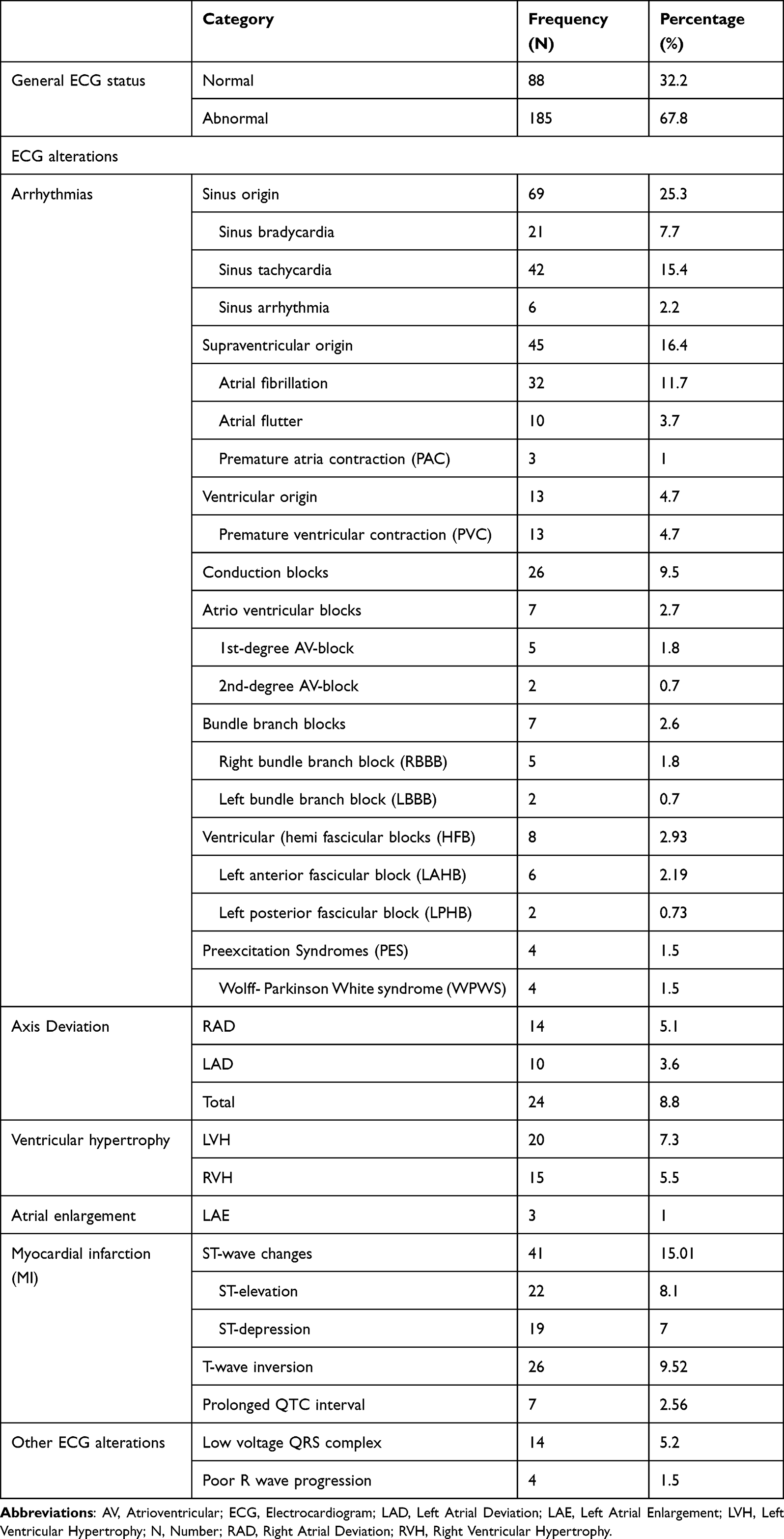 |
Table 5 Patterns of ECG Alterations Among TD Patients Attending JMC Follow-Up Clinics from October–December 2021 (N = 273) |
Factors Associated with the ECG Alterations
In bivariate analysis, the variables, which had a p-value <0.25 were selected for the multivariate logistic regression model. Accordingly, variables like age category, sex, educational status, monthly income, BMI category, diabetes mellitus, hypertension, khat chewing, smoking, duration of treatment, and duration of the disease were identified as expected factors associated with the ECG alterations using binary logistic regression analysis. After adjusting independent variables, the multivariate logistic regression model estimated that age, sex, treatment duration, and diabetes mellitus were significantly associated with the ECG alterations among TD patients. By making all other variables constant, the likelihood of developing ECG alterations in TD patients was 2.5 times more among the age group of 40–60 years old than aged less than 41 and above 60 years old, 2.7 times more among female participants than men, 4.25 times more among diabetic than non-diabetic patients, and 8.6 times more among new case-patient than follow-up patients (Table 6).
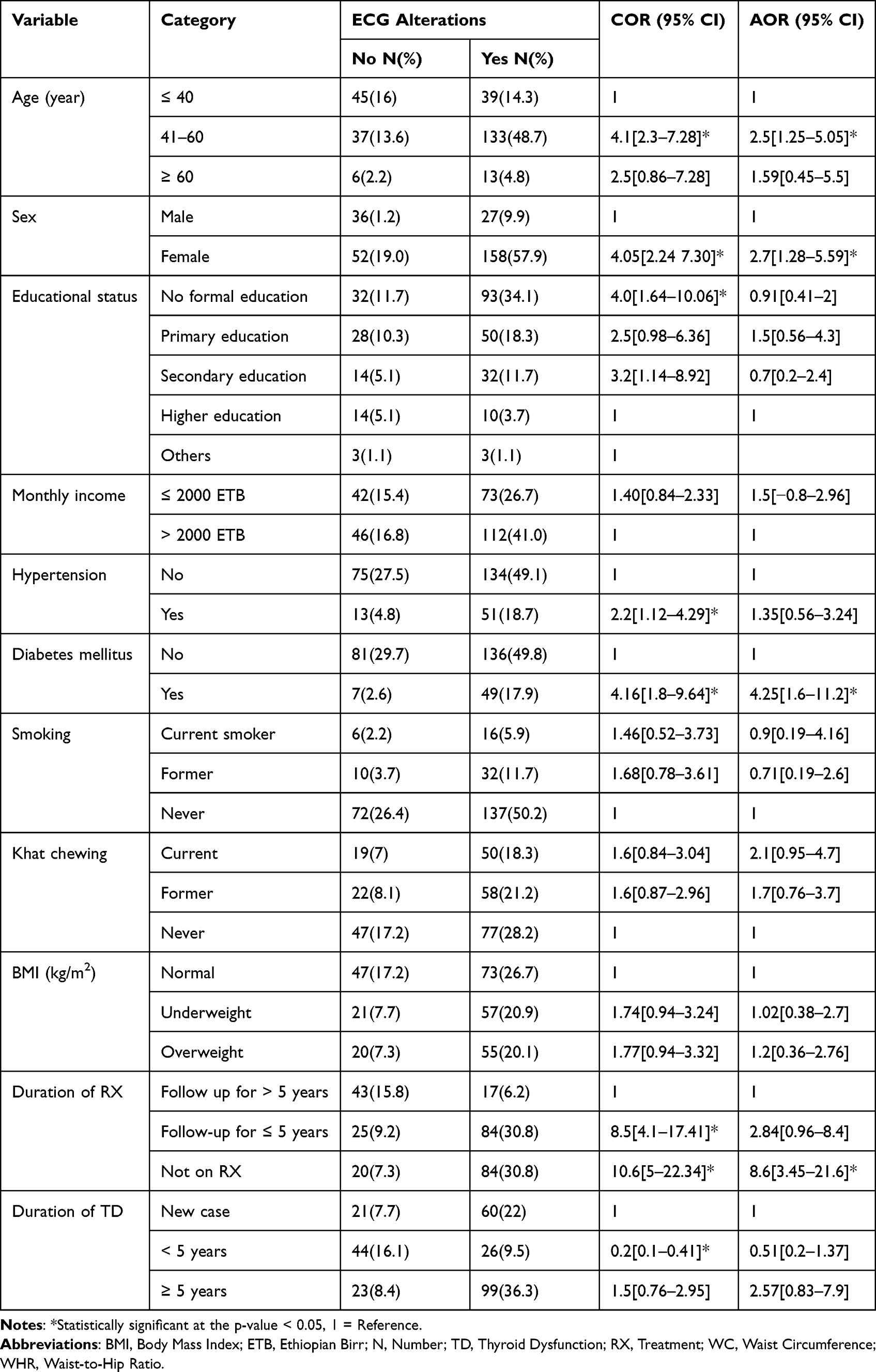 |
Table 6 ECG Alterations and Associated Factors by Bivariate and Multivariate Logistic Regression Among TD Patients Attending JMC Follow-Up Clinics from October–December 2021 (N = 273) |
Discussion
In this study, ECG alterations were interpreted among 67.8% of TD patients [CI = 63.1–73.3%]. This finding is in line with the study done in Pakistan, which found 71.5%,18 and India, which reported ECG alteration in 70%.19 However, it is higher than two studies done in India as they reported a magnitude of ECG alterations of 40.38%20 and 57%,21 respectively. These differences might be due to geographical differences, the largest burden for iodine deficiency found in Ethiopia, which predisposes to developing thyroid complications that exacerbate the risk for developing cardiac impairment, and lifestyle variances.
In the present study, the predominant patterns of ECG alterations were arrhythmia that observed in 56% of TD patients followed by myocardial infarction (MI) (26.7%), heart chamber enlargement, and hypertrophy accounted for 12.8% and 1%, respectively, and axis deviation (8.8%). From different subtypes of arrhythmias, the most observed ECG alterations include sinus tachycardia (15.4%), atrial fibrillation (11.7%), and sinus bradycardia (7.7). From MI, the most observed ECG alterations were ST-wave changes (15%), T-wave inversion (9.5%), and prolonged QTc-interval (2.5%). From the hypertrophy of the heart chambers, LVH was 7.3%, and LAE was 1%. These findings were supported by some studies done in India and Pakistan.19,20,22,23
Regarding factors associated with ECG alteration in the present study, it was observed that age was an independent predictor of ECG alteration. Thyroid dysfunction patients with the age range of 41–60 years old had a 2.5 times higher chance of developing ECG alterations compared to those aged less than 41 and above 60 years old [AOR = 2.5, 95% CI = 1.25–5.0]. This finding is supported by the study done in Denmark24 and Khane et al.25 The possible mechanisms could be due to anatomical, biochemical, and electrophysiological changes in the aging process that cause a change in greater freedom of motion of the heart within the thorax in the elderly subject and an imbalance between sympathetic and parasympathetic activity. In general, the normal physiological properties of the heart become altered and produce greater excitability, irritability, and slowed conduction.
In the present study, sex was another identified predictor variable of ECG alteration. The odds of having ECG alteration were more than two times higher in female patients than in males [AOR = 2.7, 95% CI: 1.28–5.5]. This finding is supported by the study done in Copenhagen and England.24,26 Women have faster resting heart rates and longer QTc intervals than men, which appear to evolve after puberty, suggesting that sex hormones influence cardiac electrophysiology. Estrogen may be a key factor in susceptibility to ventricular arrhythmias, altering cardiac contractility, and repolarization by altering cardiac ion channels and transporters.27,28
Diabetic mellitus was also another identified predictor variable of ECG alterations. Thyroid dysfunction patients with DM had around four times higher odds of having ECG alterations compared to non-DM TD patients [AOR = 4.25, 95%, CI = 1.6–11.2]. This finding is in line with the study done by Kumar et al.29 The relationship between DM and cardiovascular diseases is multifactorial including autonomic dysfunction, atrial and ventricular remodeling, and molecular alterations. In addition, dysglycemia, dyslipidemia, and hyperinsulinemia change the metabolic profiles and cellular signaling of the cardiovascular system.12
The other predictor variable for ECG alteration was the duration of treatment [AOR = 8.6, 95% CI: 3.45–21.6]. In the present study, it has been found that TD patients who did not start the treatment had an 8.6 times higher chance of developing ECG alterations as compared to follow-up patients. This finding is in line with the study done by Ohal et al30 and in England.26 Thyroid dysfunction has direct effects on cardiac rate, cardiac mass, myocardial contractility, and cardiac output, which may ultimately lead to heart failure.31 In untreated TD patients, the risk of cardiovascular disease was found to be increased. The ECG changes such as sinus bradycardia, prolonged QTc interval, changes in the morphology of the T-wave, QRS duration, and low voltage are increased in hypothyroidism, whereas atrial arrhythmias and duration of QT interval are increased in hyperthyroidism.24
Implications
Thyroid dysfunctions have a known influence on cardiomyocytes with increased cardiac contractility and rate, and risk of proarrhythmic effects.32 This study shows the ECG changes in TDs that make it easier for physicians to apply in routine clinics. Moreover, it tries to link the pathophysiological changes in ECG changes with TD. This study shows that age and gender are significantly associated with ECG changes in TD. Further findings on the physiology behind this interaction will improve our knowledge of the effect of TD on cardiovascular morbidity and mortality. Moreover, early treatment of TD decreases cardiovascular complications. Further studies focusing on the prognostic implication of these ECG changes in thyroid dysfunction would be clinically relevant.
Limitations of the Study
To the best of our knowledge, there is a limited study conducted in Ethiopia to show the prevalence of ECG alterations among TD patients. The study also addressed factors like socioeconomic factors, comorbidity, and behavioral factors, which were not included in the previous studies. Despite this, it is also important to note that there are some limitations since it was a simple cross-sectional study design and the patient could not be followed up on whether the ECG alterations were resolved after attaining a euthyroid state or not. Biochemical measurements such as lipid profiles and serum electrolytes, and an echocardiographic examination were also not performed due to budget shortage.
Conclusion
This study revealed that the prevalence of ECG changes was high, which was 67.8% among TD patients. The most common type of ECG change observed was arrhythmia followed by myocardial infarction. The age range of 41–60 years old, being female, having DM, and not starting treatment of TD had a significant association with the ECG changes. Implementing an efficient noninvasive screening of cardiac status as a routine diagnosis can detect unrecognized and asymptomatic cardiac impairment in TD patients.
Abbreviations
AOR, Adjusted Odds Ratio; BMI, Body Mass Index; BP, Blood Pressure; COR, Crude odds ratio; DM, Diabetes Mellitus; ECG, Electrocardiogram; TD, Thyroid Dysfunction; WHO, World Health Organization.
Data Sharing Statement
All data obtained are available in this manuscript. However, any reasonably required data will be available per the corresponding author on request.
Acknowledgments
First and foremost, we would like to thank Haramaya University and Jimma University Institute of Health, Department of Biomedical Sciences, for providing the opportunity to conduct this paper. We extend our appreciation to the data collectors’ nurses for their unlimited support from the start to the accomplishment of data collection, and to our families and friends for their technical and emotional support. Last, but not least, we would like to thank all the study participants who took part in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in conceiving the idea, study design, and managing the overall progress of the study in the acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that there is no competing interests.
References
1. Alaa H, Alsayed R, Yousif E. Thyroid gland and its rule in human body research journal of pharmaceutical, biological and chemical sciences thyroid gland and its rule in human body. J Pharm Biol Chem Sci. 2016;7(11):6.
2. Persani L. Central Hypothyroidism: Pathogenic, Diagnostic and Therapeutic Challenges. Vol. 97, Journal of Clinical Endocrinology and Metabolism. USA: The Endocrine Society; 2012:3068–3078.
3. Madariaga AG, Santos Palacios S, Guillén-Grima F, Galofré JC. The incidence and prevalence of thyroid dysfunction in Europe: a meta-analysis. J Clin Endocrinol Metab. 2014;99(3):923–931. doi:10.1210/jc.2013-2409
4. Toyib S, Kabeta T, Dendir G, Bariso M, Reta W. Prevalence, clinical presentation and patterns of thyroid disorders among anterior neck mass patients visiting Jimma Medical Center, Southwest Ethiopia. Biomed J Sci Tech Res. 2019;18(2):13431–13435.
5. Abuye C, Berhane Y. The goitre rate, its association with reproductive failure, and the knowledge of iodine deficiency disorders (IDD) among women in Ethiopia: cross-section community based study. BMC Public Health. 2007;7(1):1–7. doi:10.1186/1471-2458-7-316
6. Gruppen EG, Kootstra-Ros J, Kobold AM, et al. Cigarette smoking is associated with higher thyroid hormone and lower TSH level. Endocrine. 2020;67(3):613–622. doi:10.1007/s12020-019-02125-2
7. Borissova AM. Management of thyroid dysfunction during pregnancy and postpartum: an endocrine society clinical practice guideline - screening for thyroid dysfunction during pregnancy. Endokrinologya. 2009;14(1):56–61.
8. Selmer C, Olesen JB, Hansen ML, et al. The spectrum of thyroid disease and risk of new onset atrial fibrillation: a large population cohort study. BMJ. 2012;345(7885):e7895. doi:10.1136/bmj.e7895
9. Roth GA, Johnson C, Abajobir A, et al. Global, regional, and national burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70(1):1–25. doi:10.1016/j.jacc.2017.04.052
10. Angaw DA, Ali R, Tadele A, Shumet S. The prevalence of cardiovascular disease in Ethiopia: a systematic review and meta-analysis of institutional and community-based studies. BMC Cardiovasc Disord. 2021;21(1):1–10. doi:10.1186/s12872-020-01828-z
11. WHO. Global Physical Activity Questionnaire (GPAQ) Analysis Guide. Geneva: World Health Organization; 2012:1–22.
12. Bedane DA, Tadesse S, Bariso M, Reta W, Desu G. Assessment of electrocardiogram abnormality and associated factors among apparently healthy adult type 2 diabetic patients on follow‑up at Jimma Medical Center, Southwest Ethiopia: cross‑sectional study. BMC Cardiovasc Disord. 2021;21(3):1–9. doi:10.1186/s12872-021-02110-6
13. Prineas RJ, Crow RS, Zhang ZM. The Minnesota Code Manual of Electrocardiographic Findings, Standards and Procedures for ECG Measurement in Epidemiologic and Clinical Trials. London: Springer-Verlag London Limited; 2010:1–338.
14. Cirrincione L, Plescia F, Ledda C, et al. COVID-19 pandemic: prevention and protection measures to be adopted at the workplace. Sustainability. 2020;12(9):1–18. doi:10.3390/su12093603
15. Prineas RJ, Crow RS, Zhang ZM. The Minnesota Code Manual of Electrocardiographic Findings Standards and Procedures for ECG Measurement in Epidemiologic and Clinical Trials. New York: springer; 2010.
16. Jevon P. Blood pressure 2: procedures for measuring blood pressure. Nurs Times. 2020;116(8):26–28.
17. World Health Organization. Waist circumference and waist–hip ratio. Report of a WHO Expert Consultation. Geneva; 2008;8–11.
18. Baladi IH, Rai AA, Ahmed SM. ECG changes in patients with primary hyperthyroidism. Pan Afr Med J. 2018;30(12):1–5. doi:10.11604/pamj.2018.30.246.12244
19. Ramesh K, Nayak BP. A study of cardiovascular involvement in hypothyroidism. Int Arch Integr Med. 2016;3(5):74–80.
20. Panwar M, Saikia BJ, Shreya P. Assessment of cardiovascular manifestations of hyperthyroid disorder patients. Eur J Mol Clin Med. 2020;07(11):9414–9417.
21. Sureshbabu KP, Gireesh Oswal A. Cardiac manifestations in hypothyroidism - a cross sectional study. Res J Pharm Biol Chem Sci. 2014;5(3):966–975.
22. Satpathy P, Singh H, Agarwal A, Diggikar P, Laddha M, Sachdeva V. Lipid profile and electrocardiographic changes in thyroid dysfunction. Med J DY Patil Univ. 2013;6(3):250. doi:10.4103/0975-2870.114647
23. Goyal V, Goyal S. A study of electrocardiographic changes in thyroid disorders a study of electrocardiographic changes in thyroid disorders. Int J Med Res Rev. 2016;4(4):486–490. doi:10.17511/ijmrr.2016.i04.04
24. Tayal B, Graff C, Selmer C, et al. Thyroid dysfunction and electrocardiographic changes in subjects without arrhythmias: a cross-sectional study of primary healthcare subjects from Copenhagen. BMJ Open. 2019;02(3845):e023854.
25. Khane RS, Surdi AD, Bhatkar RS. Changes in ECG pattern with advancing age. J Basic Clin Physiol Pharmacol. 2011;22(4):97–101. doi:10.1515/JBCPP.2011.017
26. Osman F, Franklyn JA, Holder RL, Sheppard MC, Gammage MD. Cardiovascular manifestations of hyperthyroidism before and after antithyroid therapy. A matched case-control study. J Am Coll Cardiol. 2007;49(1):71–81. doi:10.1016/j.jacc.2006.08.042
27. Ravens U. Sex differences in cardiac electrophysiology. Can J Physiol Pharmacol. 2018;96(10):985–990. doi:10.1139/cjpp-2018-0179
28. Murphy E, Kelly DP. Estrogen signaling and cardiovascular disease. Circ Res. 2011;109(6):687–696. doi:10.1161/CIRCRESAHA.110.236687
29. Kumar A, Kumar R, Mehra D, Chaturvedi A, Sharma M. ECG changes in thyroid dysfunction in diabetes mellitus. J Med Sci Clin Res. 2019;07(01):77–82.
30. Ohal SS, Bhagchandani RA, Phatak MS. Electrocardiographic changes in hypothyroidism–a cross-sectional study. Natl J Physiol Pharm Pharmacol. 2019;9(5):459.
31. Abdel-Moneim A, Gaber AM, Gouda S, et al. Relationship of thyroid dysfunction with cardiovascular diseases: updated review on heart failure progression. Hormones. 2020;19(3):301–309. doi:10.1007/s42000-020-00208-8
32. Ulivieri A, Lavra L, Magi F, et al. Thyroid hormones regulate cardiac repolarization and QT-interval related gene expression in hiPSC cardiomyocytes. Sci Rep. 2022;12(1):568. doi:10.1038/s41598-021-04659-w
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Profiles of Cardiovascular Diseases and Predictors of Outcome of Hospitalization in a Tertiary Teaching Hospital, Ethiopia: A Prospective Observational Study
Hailu A, Gidey K, Mohamedniguss Ebrahim M, Berhane Y, Baraki TG, Hailemariam T, Negash A, Mesele H, Desta T, Tsegay H, Assefa M, Bayray A
Research Reports in Clinical Cardiology 2023, 14:69-83
Published Date: 29 September 2023