Back to Journals » Medical Devices: Evidence and Research » Volume 15
Assessment of an Articulating Laparoscopic Needle Holder (FlexDex™) Compared to a Conventional Rigid Needle Holder in 2-Dimension Vision Amongst Novices: A Randomised Controlled Study
Authors Motahariasl N, Farzaneh SB, Motahariasl S, Kokotkin I, Sousi S, Zargaran A, Zargaran D, Bijendra Patel
Received 7 November 2021
Accepted for publication 12 January 2022
Published 4 February 2022 Volume 2022:15 Pages 15—25
DOI https://doi.org/10.2147/MDER.S345140
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Nima Motahariasl,1 Sayed Borna Farzaneh,1 Sina Motahariasl,2 Ilya Kokotkin,3 Sara Sousi,4,5 Alexander Zargaran,5,6 David Zargaran,7 Bijendra Patel8
1St George’s Hospital NHS Trust, London, SW17 0QT, UK; 2Lewisham and Greenwich NHS Trust, London, SE13 6LH, UK; 3St George’s University of London, London, SW17 0RE, UK; 4Department of Surgery and Cancer, Imperial College London, Hammersmith Campus, London, W12 0NN, UK; 5King’s College London, London, SE1 1UL, Greater London, UK; 6Chelsea and Westminster Hospital, London, SW10 9NH, UK; 7Royal Free Hospital, London, NW3 2QG, UK; 8Barts Cancer Institute, Queen Mary University of London, London, UK
Correspondence: Sara Sousi
Department of Surgery and Cancer, Imperial College London, Hammersmith Campus, London, W12 0NN, UK
, Email [email protected]
Aim: This study aims to compare novice performance of advanced bimanual laparoscopic skills using an articulating laparoscopic device (FlexDex™) compared to a standard rigid needle holder amongst surgical novices in 2-dimension (2D) visualisation.
Methods: In this prospective randomised trial, novices (n = 40) without laparoscopic experience were recruited and randomised into two groups, which used either traditional rigid needle holders or the FlexDex™. Both groups performed 10 repetitions of a validated assessment task. Times taken and error rates were recorded, and results were evaluated based on completion times, error rates, and learning curves.
Results: The intervention group that used the FlexDex™ completed 10 attempts of the standardised laparoscopic task slower than the control group that used traditional rigid needle holder (415 s versus 267 s taken for the first three attempts and 283 s versus 187 s taken for the last three attempts, respectively). The difference in average time for the first three and last three attempts reached statistical significance (P < 0.001). Furthermore, the intervention group demonstrated a higher error rate when compared to the control group (9.3 versus 6.2 errors per individual).
Conclusion: When compared to the FlexDex™, the traditional rigid needle holder was observed to be superior in task performance speed, leading to shorter completion times and quicker learning effect, as well as fewer errors.
Key Statement: Traditional rigid needle holder leads to faster task completion times and lower error rates when compared with an articulating laparoscopic needle holder in 2D vision.
Keywords: laparoscopic skills, advanced bimanual skills, 2D, FlexDex™
Introduction
Instrument development has been shown to contribute to the healthcare system by offering improvements in surgical times and cost-efficiency.1 The emergence of minimally invasive laparoscopic surgery is one of the greatest of such. Laparoscopic procedures have been noted to have numerous advantages over traditional open surgery for both patients and surgeons.2 Despite these advantages, early laparoscopic instruments had numerous flaws which led to operative challenges and insufficiencies.3 The need for further innovation in this field has prompted biomedical companies to strive for novel designs to address the original flaws of these instruments. Whilst innovations have helped to further the technologies available within laparoscopic surgery, advances in operative techniques have brought about new challenges to facilitate more intricate and time-consuming surgical procedures. This has subsequently revealed novel design weaknesses and patterns of surgeon fatigue, which further create a demand for design refinements.2,3
The conventional rigid laparoscopic needle holders have been identified to propose challenges due to their restricted manoeuvrability; reducing manual dexterity and impairing haptic feedback during surgical procedures.4,5 Articulation of an instrument end effector, allows for higher degrees of freedom compared to the 4 degrees of conventional instruments, theoretically allowing for improved dexterity and instrument triangulation.6 Significant contributions to instrument articulation have been apparent through the revolution of robotic surgery. Robotic equipment such as the Da Vinci surgical system by Intuitive Surgical Inc. allowed for the development of fully articulating instruments mimicking movements that of the human hand.4 However, a major limitation impeding their widespread use is their cost and financial burden on health care organisations with an up-front cost of approximately $1.5 million, maintenance costs of $150,000 per annum and, per-patient costs of $1000.7,8 Ultimately this has led biomedical institutions to pursue the development of highly dexterous laparoscopic instruments with the advantages of robotic surgery but at a fraction of the price.
However, previous studies comparing conventional and articulating instruments have also shown that although articulating instruments allow for improved manoeuvrability and higher degrees of freedom, such benefits may be counterbalanced by their complexity of use and higher learning curve. Moreover, they explored the concept of orientation periods and demonstrated significant improvements in outcomes after a structured familiarisation period.9 Ultimately, this has pressured biomedical companies to produce new articulating instruments with minimal complexity, shorter learning curves and accompanying training programs.
A recent innovation in articulating laparoscopic needle holders is the FlexDex™ instrument produced by Awtar et al in affiliation with Michigan University and FlexDex™ Surgical Inc.10 The instrument’s handle houses a 3-axis gimbal and is attached to the surgeon’s forearm by a Velcro® wristband. This novel articulating instrument allows for higher degrees of freedom in comparison to the standard needle holder.4,11
Aims
This study compares the performance of advanced bimanual laparoscopic skills using an articulating laparoscopic device (FlexDex™), versus a standard rigid needle holder amongst surgical novices in 2-dimension (2D) visualisation.
Materials and Methods
Ethics
This study was granted ethical approval on 24/09/2021 by King’s College London Research Ethics Committee (MRA-21/22-26358).
Recruitment
A convenience sample of medical students was taken. Advertisements were listed at Surgical Society events. Participants registered their interests via a Google Form. No financial incentive was offered for participation in this study. Participants were randomised to either using articulating laparoscopic instruments (FlexDex™) versus a control group using standard rigid needle holders.
Randomisation
A sealed envelope method was used to randomise the subjects into either trial arm.
Inclusion and Exclusion Criteria
This included participants without prior surgical experience, particularly in the use of laparoscopic instruments. This was to identify participants who could be considered at the very beginning of the laparoscopic training journey. For inclusion in the study, participants had to be novices to laparoscopy with no previous training or exposure beyond camera handling. The participants who did not meet the inclusion criteria were excluded from the study. Furthermore, the exclusion criteria included: prior training in laparoscopic instrument handling beyond camera manipulation, lack of commitment and, absence during the introductory session.
Materials and Equipment
Laparoscopic box trainer by Zhejiang Shendasiao Medical Instruments Co., Ltd was used containing six skin-like access ports for the introduction of laparoscopic instruments. Finlux 42S7080 monitors were used (Display Size: 42 Inch (42”), Display Type: LED Full HD 1080p 2D monitor). The camera was a Sony camcorder (HDR-TD10 Handycam, (10X Zoom in 2D)) capable of recording in 2D, stabilised to a table in a fixed and non-guidable manner. Articulating laparoscopic grasper was the FlexDex™ laparoscopic needle holder provided by FlexDex™ Surgical™ and the laparoscopic grasper used was a 3mm laparoscopic grasper (Maryland) by LaproSurge®.
Laparoscopic Task
The assessment task was task 1 (Grasping and manipulation) of the LapPass® examination created by the Association of Laparoscopic Surgeons of Great Britain and Ireland (ALSGBI). Individuals in both the FlexDex™ and rigid group were asked to perform 10-repetitions with both time and number of errors being recorded for all 10 tries. To avoid data collection discrepancy, completion times were recorded by the same assessor (author) for all participants. Task errors were described as “Dropping rings outside the model surface” or “losing the ring”. In such cases, additional spare rings were available adjacent to the model surface (Supplementary Table 1).
Duration of Training
Individuals were asked to perform 10-repetitions with both time and number of errors being recorded for all 10 tries.
Assessment and Error Measurement
1. Completion times were measured for all 10 repetitions.
2. Learning curve assessment comparing completion time of first 3 and last 3 attempts.
3. Error scores were defined as dropping the rings outside the model surface or losing a ring outside the field of view at any point during the 4 steps of the bimanual manipulation. Each drop outside the model surface or loss outside the field of view was given a score of 1 and the accumulated error score was measured for each of the 10 attempts. No drop or loss of a ring during an attempt was given an error score of 0.
Study Pathway
Participants were required to attend two mandatory sessions. The first session was an introductory lecture and video demonstration, which provided information regarding the study and the task they will be requested to perform. Following the first session, the subjects were randomly allocated into two groups. Participants in group A were allocated to use the FlexDex™ needle holder, and the participants in group B were allocated to use standard needle holders. In the second session, subjects were given a 45-minute familiarisation period. During this time, six exercises were given to the subjects to help them acquaint themselves with the instruments (Supplementary Table 1). Subsequently, they undertook the validated assessment task. This validated assessment task was task number 1, “grasping and manipulation” of the LapPass® examination.12,13 The sequence of actions required to be performed by the participants is detailed in Supplementary Figure 1. It consisted of four steps that all needed to be done for 1 completed attempt.
For meaningful comparisons to be made between the performance of subjects, each participant was asked to carry out 10 repetitions of the assessment task. Two fundamental quantities, the completion time and the number of errors, were assessed for all 10 attempts. The mean time for successful completion of the first and last 3 attempts was used for statistical calculations. Furthermore, the mean total number of errors for all 10 attempts was calculated and compared between group A and group B, as well as the error rate per participant which was defined as the sum of errors over the 10 attempts.
Familiarisation Period
In session 2, participants in both groups were allocated an overall 45-minute time slot to become acquainted with the instruments they will be handling. A set of six training exercises designed according to videos provided by FlexDex™ surgical were used. Participants in both groups watched each of the designed 2-minute videos and were given 5 minutes to practice what had been demonstrated in each video. This process was repeated for each of the 6 videos. (Supplementary Table 1 and Supplementary Figure 2).
Consent
Written consent was taken from the subjects during the recruitment process, before the commencement of the trial.
Consort Diagram
The consort diagram is illustrated in Figure 1.
 |
Figure 1 Consort diagram illustrating the flow of subjects through the study. |
Data Collection and Statistical Analysis
Score sheets were made using Microsoft® Word for each participant to record completion times and the number of errors per attempt. Moreover, data was collected through spreadsheets using Microsoft® Excel version 16.21. Evaluation of task completion time between the two groups was through an inter-cohort comparison of completion times between the first and last three repetitions. Additionally, the average error throughout all 10 repetitions was used to compare error rates between the two trial arms. The data were analysed for normality of spread using the Shapiro–Wilk test. The F-test was implemented to assess whether the comparing samples had equal variance. Based on the p-values generated, the Two-Sample t-test, the Welch Two-Sample t-test, or the Wilcoxon rank-sum test was implemented to compare the differences between the two groups based on each test’s assumption. This was carried out for both the error rates and completion times. The significance level was set at 0.05 (a = 0.05) for this study. The statistical analyses were carried out using International Business Machines (IBM) SPSS® version 25 analytic software and R version 4.0.3.
Results
Seventy-one participants were recruited in the study. Following the implementation of the inclusion and exclusion criteria, 14 subjects were eliminated as they had previously received training in laparoscopic surgical skills. All the remaining 57 subjects were invited to attend the introductory lecture. Of the remaining participants, 17 failed to attend the introductory sessions, which led to their elimination from the study. Therefore, 40 individuals remained who participated in the study. The remaining 40 subjects were randomised into each study arm with 20 individuals present in each group; FlexDex™ (n=20) and Rigid (n=20). Table 1 below demonstrates the demographic information of the participants randomised to each arm of the study.
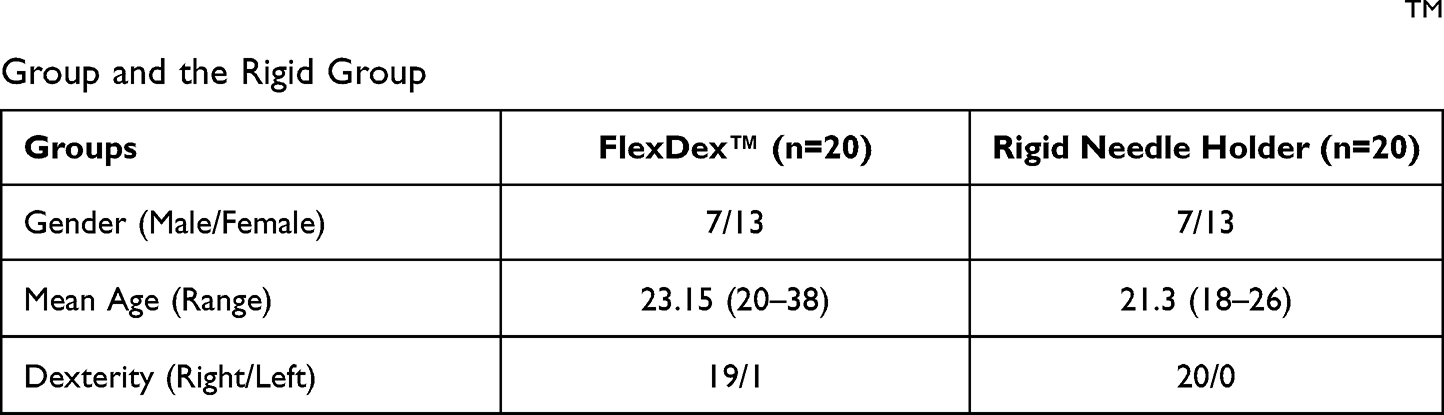 |
Table 1 Table Demonstrating Demographic Information of Participants in Both the FlexDexTM Group and the Rigid Group |
To demonstrate any pre-eminence of instrumentation, task completion time and accuracy were compared between the study arms. With regards to completion time, an inter-cohort comparison was conducted for the initial three attempts and the final three attempts. This method was chosen as it revealed an average for completion times at the beginning and towards the end of the assessments, therefore reducing the probability of comparison with single anomalous times. Moreover, using average times in the beginning and the end would demonstrate differences in the learning curve for each set of instruments and illustrate how readily participants can adapt to them.
Completion Times
Table 2 demonstrates the average completion time per attempt between the 20 participants in each of the cohorts. As shown in Table 3, analysis of results demonstrates an average of 415 seconds for the first 3 attempts and 283 seconds for the last 3 attempts in the FlexDex™ group. The Rigid group had an average of 267 seconds for the first 3 attempts and 187 seconds for the last 3 attempts. Figure 2C shows the boxplot of the average completion time of the attempts of the two groups, the results of the Two-Sample t-test are illustrated on the plot. A Two-Sample t-test was performed as the times are normally distributed (Shapiro–Wilk normality test p > 0.05) and of equal variance (F-test p > 0.05).
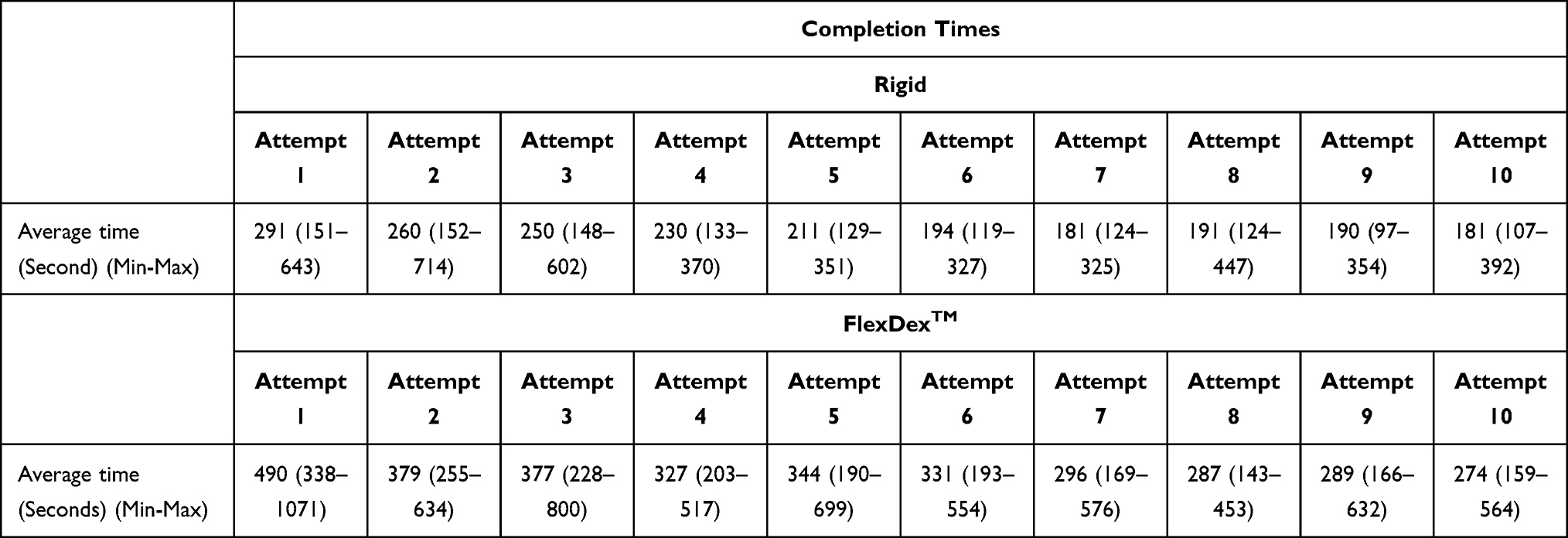 |
Table 2 Table Demonstrating the Average Time per Attempt Between All Individuals Within the FlexDex™ Group and the Rigid Needle Holder Group |
 |
Table 3 Table Demonstrating the Average Time, Standard Deviation, and Range of the First and Final 3 Attempts Between All Individuals Within the FlexDex™ Group and the Rigid Needle Holder Group |
 |
Figure 2 (A) Box plot of total average completion times in attempts 1, 2, 3 between the FlexDex™ and Rigid groups. The Wilcoxon Rank-Sum test results are displayed on the plot. (B) Box plot of total average completion times in attempts 8, 9, 10 between the FlexDex™ and Rigid groups. The Wilcoxon Rank-Sum test results are displayed on the plot. (C) Box plot of the average completion time of all attempts of the assessment task in participants allocated to the FlexDex™ and Rigid groups. |
Error Rates
A review of data regarding error rates demonstrates an average error rate of 6.2 errors between all participants throughout all 10 attempts in the Rigid group. Moreover, the analysis demonstrated an average of 9.3 errors between all participants throughout all 10 attempts in the FlexDex™ group (Table 4). Figure 3 demonstrates the boxplots of the average overall error rate in each of the two groups, where error rate is defined as the sum of errors of all the attempts. The results of the Welch Two-Sample t-test are illustrated on the plot; a Welch Two-Sample t-test was performed as the error rates are normally distributed (Shapiro–Wilk normality test p > 0.05) and have unequal variance (F-test p < 0.05).
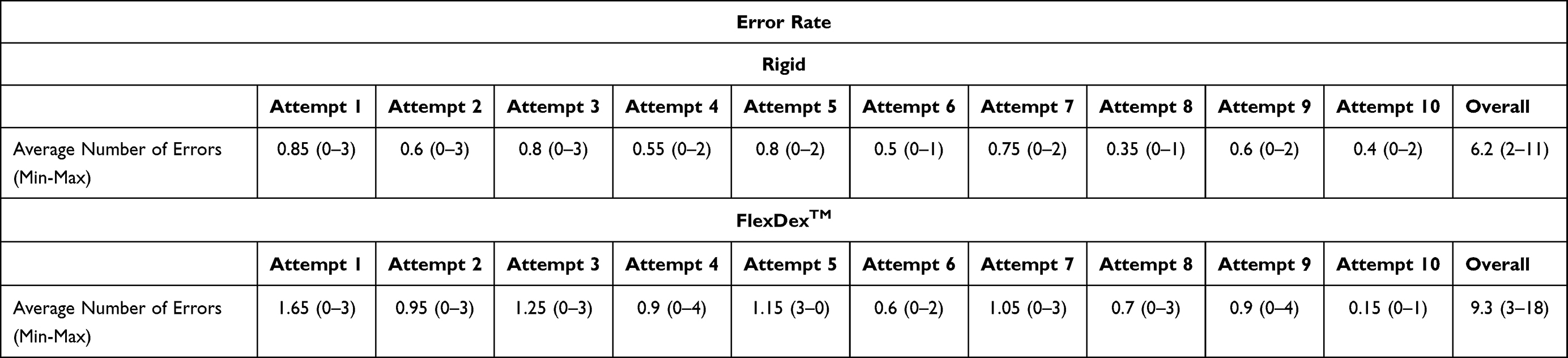 |
Table 4 Table Demonstrating the Average Error Rate per Attempt Between All Individuals Within the FlexDex™ Group and the Rigid Group |
 |
Figure 3 Box plot of the error rate over the 10 attempts of the assessment task in participants allocated to the Rigid and FlexDex™ groups. |
Learning Curve Assessment
Inter-cohort comparison of the first three attempts revealed statically significant (p < 0.001) quicker completion time in the Rigid group with a mean difference of 148.3 seconds. Analysis of the final three attempts also demonstrated statistically significant (p < 0.001) shorter completion times in favour of the Rigid combination with a mean difference of 95.7 seconds (Table 5). Figure 2A and B illustrate the boxplots for the first and last three attempts of each arm, respectively. Both reach statistical significance (p < 0.001) A Wilcoxon Rank-Sum test was performed as the times are not normally distributed (Shapiro–Wilk normality test p < 0.05).
 |
Table 5 This Table Demonstrates the Difference Between FlexDex™ and Rigid in the First 3 Attempts and Last 3 Attempts |
Discussion
This study aimed to compare the effect of utilising the wrist-like articulating laparoscopic instrument FlexDex™ on task performance speed and accuracy by surgical novices. Previously conducted studies aimed at assessing the performance of FlexDex™ demonstrated that this mechanical instrument may have an advantage over non-articulating laparoscopic needle holders in terms of manoeuvrability and performance speed. Other studies have further demonstrated similar outcomes to the conclusions of this trial. Xu et al compared the straight and articulating laparoscopic instruments in a laparoscopic single-site surgery setting. The findings of this study showed that due to the complexity of the instruments and a steep learning curve, articulating instruments are associated with longer operation time and higher workload when compared to conventional rigid laparoscopic instruments.14 Furthermore, the findings of a study by Martinec et al demonstrated that despite improvements in manoeuvrability and higher degrees of freedom in the use of articulating instruments, there is a steep learning curve in acquiring the skill to utilise such instruments.9
Completion Times
All participants were chosen from the same cohort of medical students with no prior laparoscopic training; therefore, the only variable between the study arms was the type of needle holder being used. When comparing the task completion times between the rigid needle holder and FlexDex™, there is a statistically significant difference favouring the rigid needle holder. When comparing the first 3 attempts, participants using the standard needle holder had statistically significant shorter completion time which means the learning curve for this instrument is quicker in comparison to FlexDex™. This finding suggests that the initial 45-minute familiarisation period, which utilised the guidance videos provided by FlexDex™ was not sufficient for overcoming the steep learning curve of this instrument. Furthermore, this can be further demonstrated when comparing the completion times of the last 3 attempts. The group utilising the standard needle holder completed the assessment task quicker compared to the FlexDex™ group. This could suggest that the attempts which took place between the initial and last 3 attempts did not provide enough exposure to the participants to help them overcome the learning curve of using FlexDex™. A study by Criss et al comparing the FlexDex™ to conventional laparoscopic instruments also demonstrated that for surgical tasks performed at more accessible locations, both surgical novices and experienced surgeons had quicker completion times with conventional laparoscopic instruments compared to the FlexDex™. However, they reported the FlexDex™ to be more ergonomic, with a significant reduction in physical fatigue during its use compared to conventional instruments.15
Error Rates
This study revealed a statistically significant lower average number of errors in participants using the rigid needle holder compared to FlexDex™ (6.2 versus 9.3). Therefore, it could be concluded that the participants utilising the standard needle holder demonstrated superior precision, efficiency, and safety compared to the participants utilising FlexDex™. These findings further reflect the steep learning curve involved in using FlexDex™. Inherent complexities associated with the FlexDex™ design such as the combination of a fulcrum effect in combination with end effector articulation create a complex pattern of movement to create the desired intracorporeal movement. This complexity leads to more frequent errors which necessitates a thorough training and familiarisation programme. Supporting this is a study by Tuncel et al comparing conventional and laparoscopic needle drivers which concluded that laparoscopy-naïve subject experience significant higher errors when completing tasks using articulating instruments as compared to conventional instruments.5 Currently no official training programme for utilising the FlexDex™ exists and it would be beneficial for further research to focus on developing an adequate training curriculum for this articulating instrument.
Learning Curve Assessment
Overall, subsequent attempts resulted in reduced completion times in both intervention and study groups. However, the results indicate that the participants in the Rigid group had a faster learning curve compared to the FlexDex™ group (line gradient 13.2 versus 9.2 respectively). In the FlexDex™ group, the difference in completion times between the first and last three attempts is 132 seconds, compared to 80 seconds in the Rigid group. This may indicate that although the participants in the experimental group had a more drastic difference in the performance times between the first and the last attempts, thus quicker learning curve, the participants in the Rigid group were faster throughout all 10 attempts compared to the FlexDex™ group. A study by Uysal et al comparing the learning curve between articulating and conventional laparoscopic instruments amongst surgical novices also found similar results in favour of conventional instruments.16 The longer learning curve could be attributed to factors such as the complexity of generating the desired movement with the FlexDex™, Its un-ergonomic hand placement when operating the device and finally difficulties in releasing the device from one’s hand.
Limitations
Several limitations were identified in conducting this study. For example, power calculations were not carried out for this study to determine the minimum number of participants per study arm. Furthermore, as there was no official FlexDex™ training programme available, the programme used in the familiarisation period was made by the researchers using the videos provided by FlexDex™. In the future, the use of a validated training routine can improve the reliability of the results. Moreover, the assessment used was a task with a moderate level of difficulty which may have inadvertently benefited the participants using the rigid instruments due to its inherent faster learning curve. Finally, participants in both groups used cameras that had been fixed in position and were non-manoeuvrable. Should a guidable camera had been used like those used in operating theatres, the results may have differed due to the ability to constantly visualise the articulating instrument tip.
Conclusion
The FlexDex™ laparoscopic needle driver is an FDA-approved surgical device that allows the surgeon to perform laparoscopic surgery with the same seven degrees of motion afforded by a robotic arm. This study showed that the traditional rigid needle holder resulted in reduced time taken to complete a laparoscopic task compared to FlexDex™. Additional randomised controlled trials and meta-analyses will be necessary to assess the generalisability of these initial results.
Disclosure
The authors report no conflicts of interest for this study. Authors have no relationship with FlexDex™.
References
1. Zheng J. Design and development of biomedical and surgical instruments in biomedical applications. In: Hudak R, editor. Biomedical Engineering – Technical Applications in Medicine. InTech; 2012. Available from: http://www.intechopen.com/chapters/38772.
2. Subido EDC, Pacis DMM, Bugtai NT. Recent technological advancements laparoscopic surgical instruments. Bali, Indonesia; 2018. 040007. Available from: http://aip.scitation.org/doi/abs/10.1063/1.5023977.
3. Berguer R. Surgical technology and the ergonomics of laparoscopic instruments. Surg Endosc. 1998;12(5):458–462. doi:10.1007/s004649900705
4. Anderson PL, Lathrop RA, Webster III RJ. Robot-like dexterity without computers and motors: a review of hand-held laparoscopic instruments with wrist-like tip articulation. Expert Rev Med Devices. 2016;13(7):661–672.
5. Tuncel A, Lucas S, Bensalah K, et al. A randomized comparison of conventional vs articulating laparoscopic needle-drivers for performing standardized suturing tasks by laparoscopy-naive subjects. BJU Int. 2008;101(6):727–730. doi:10.1111/j.1464-410X.2007.07220.x
6. Sieber MA, Fellmann-Fischer B, Mueller M. Performance of Kymerax© precision- drive articulating surgical system compared to conventional laparoscopic instruments in a pelvitrainer model. Surg Endosc. 2017;31(10):4298–4308. doi:10.1007/s00464-017-5438-8
7. Kockerling F. Robotic vs. standard laparoscopic technique - what is better? Front Surg. 2014;1. Available from: http://journal.frontiersin.org/article/10.3389/fsurg.2014.00015/abstract.
8. Anderson P, Lathrop R, Herrell S, Webster R. Comparing a mechanical analogue with the da Vinci user interface: suturing at challenging angles. IEEE Robot Autom Lett. 2016;1(2):1060–1065. doi:10.1109/LRA.2016.2528302
9. Martinec DV, Gatta P, Zheng B, Denk PM, Swanström LL. The trade-off between flexibility and maneuverability: task performance with articulating laparoscopic instruments. Surg Endosc. 2009;23(12):2697–2701.
10. FlexDex™ surgical – the MIS device that moves like you. [
11. Vigneswaran H, Crivellaro S. Perform renorrhaphy. Exp Tech Urol Nephrol. 2017;1(2). doi:10.31031/ETUN.2017.01.000506
12. LapPass ® [Internet]. ALSGBI. [cited May 25, 2019]. Available from: https://www.alsgbi.org/lappass/.
13. Fong M, Treglohan J, Selvasekar C, Sedman P, Leeder P, Francis N. TP8.2.9 development & evaluation of LapPass™: the laparoscopic passport. Br J Surg. 2021;108(Supplement_7). doi:10.1093/bjs/znab362.082
14. Xu AA, Zhu JF, Xie X, Su Y. Mechanical evaluation of articulating instruments and cross-handed manipulation in laparoendoscopic single-site surgery. Surg Innov. 2014;21(4):398–402. doi:10.1177/1553350613509727
15. Criss C, Jarboe M, Claflin J, Matusko N, Rooney D. Evaluating a solely mechanical articulating laparoscopic device: a prospective randomized crossover study. J Laparoendosc Adv Surg Tech A. 2019;29(4):542–550. doi:10.1089/lap.2018.0539
16. Uysal D, Gasch C, Behnisch R, et al. Evaluation of new motorized articulating laparoscopic instruments by laparoscopic novices using a standardized laparoscopic skills curriculum. Surg Endosc. 2020;35(2):979–988. doi:10.1007/s00464-020-08086-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.