Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Assessing Swallowing Function is Important Upon Admission to Community-Based Integrated Care Wards. A Retrospective Observational Study
Authors Okubo M ![]() , Morishita M
, Morishita M ![]() , Ohno T, Sakaguchi H, Kokabu S
, Ohno T, Sakaguchi H, Kokabu S
Received 29 September 2025
Accepted for publication 8 December 2025
Published 26 December 2025 Volume 2025:18 Pages 8257—8265
DOI https://doi.org/10.2147/JMDH.S571210
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Masahiko Okubo,1,2 Motoyoshi Morishita,3 Tomohisa Ohno,4 Hideo Sakaguchi,4 Shoichiro Kokabu5
1Department of Dentistry and Oral Surgery, Ongata Hospital, Hachioji, Tokyo, Japan; 2Department of Dentistry, Yokohama Izumidai Hospital, Yokohama, Kanagawa, Japan; 3Department of Physical Therapy, Faculty of Rehabilitation, Reiwa Health Sciences University, Fukuoka, Fukuoka, Japan; 4Department of Dentistry, Ryohoku Hospital, Hachioji, Tokyo, Japan; 5Department of Biochemistry, Kyushu Dental University, Kitakyushu, Fukuoka, Japan
Correspondence: Masahiko Okubo, Department of Dentistry and Oral Surgery, Ongata Hospital, 105 Nishiterakata, Hachioji, Tokyo, 192-0153, Japan, Tel +81-42-651-3411, Fax +81-42-659-2164, Email [email protected]
Purpose: This study aimed to evaluate patients’ swallowing ability at the time of admission to community-based integrated care wards and to assess the importance of this evaluation.
Patients and Methods: 77 older adult patients admitted to the wards between April 2023 and March 2024 participated in the study. Within 48 h of admission, an original screening tool and meal rounds were collaboratively administered by a multidisciplinary team to assess patients’ oral and pharyngeal function and their mode of nutritional intake. Dysphagia diets were classified according to the Dysphagia Diet Classification 2021 and compared with the International Dysphagia Diet Standardization Initiative. Oral and pharyngeal function were assessed using the Food Intake LEVEL Scale (FILS) and standardized meal rounds. Fiberoptic endoscopic evaluation of swallowing was performed when necessary. Associations between changes in food intake routes and discharge destinations were analyzed using the chi-squared test, while changes in FILS scores were evaluated using the Wilcoxon signed-rank test.
Results: Aspiration pneumonia and cerebrovascular disorders were the most common illnesses. Many patients were safely transitioned from total or peripheral parenteral nutrition to oral intake, accompanied by significant improvements in FILS scores. The findings demonstrate the effectiveness of assessing swallowing ability and determining appropriate feeding routes in community-based integrated care wards.
Conclusion: This study could contribute to better establishing appropriate feeding methods and managing patient nutrition during hospitalization. By using multidisciplinary shared swallowing-assessment tools, safe transition to oral intake can be promoted without necessarily performing detailed examinations.
Keywords: deglutition, aging, community-based integrated care, dysphagia, nursing care, quality of life, swallowing ability
Introduction
Community-based integrated care wards are a medical system unique to Japan, designed to support patients in transitioning smoothly from acute treatment to home or other facilities, with the ultimate goal of promoting independent living following discharge. Established during the 2014 medical revision fees in response to Japan’s super-aging society, these wards serve as an intermediary step between acute care and returning home.1,2 The system primarily targets older adults who have completed acute treatment but require additional medical care, rehabilitation, or support before returning home. Admission criteria are determined by medical category and activities of daily living assessments.3 Furthermore, discharge planning is strategically coordinated by a multidisciplinary team, and previous studies have highlighted collaboration not only among physicians, nurses, and rehabilitation specialists but also among dental practitioners, dental hygienists, and nutritionists.4,5
However, the operational structure of community-based integrated care wards and the conditions of admitted patients vary by facility. Patients with diverse medical histories, including fracture surgery, disuse syndrome, cerebrovascular diseases, and aspiration pneumonia, may be admitted. Without appropriate nutritional management and rehabilitation prior to discharge, the risk of readmission or post-discharge aspiration pneumonia increases, along with the care burden placed on family members or home-care staff.6–8
Nutritional management is a key determinant of patients’ quality of life after discharge. Aspiration prevention and appropriate selection of nutritional intake methods support stable oral food feeding, particularly in patients with dysphagia.9
Dysphagia is a condition in which food or liquid cannot be safely and smoothly transported from the pharynx to the stomach because of abnormalities in one or more of the oral, pharyngeal, or esophageal phases of swallowing. Its causes are diverse and include structural abnormalities (such as tumors or postoperative changes), neurological and neuromuscular disorders (e.g., stroke, Parkinson’s disease, and myopathies), age-related functional decline, drug-induced effects, and disturbances of consciousness or cognition, which often interact in a multifactorial manner.
And it is usually found among older individuals due to various age-related diseases.10 When oral intake cannot be maintained, prolonged use of parenteral nutrition, such as total parenteral nutrition (TPN) or peripheral parenteral nutrition (PPN), increases the risk of catheter-related bloodstream infections (CRBSI) and metabolic complications. Conversely, when switching to enteral nutrition (eg, via a nasogastric tube or gastrostomy), new risks may arise, including aspiration pneumonia, gastroesophageal reflux, local subcutaneous infection at the insertion site, and tube obstruction. In addition, interruption of oral intake can lead to disuse-related decline in orofacial and pharyngeal muscle function, reduced salivary secretion, and deterioration of oral hygiene, which may in turn increase the risk of pneumonia and other infections. Therefore, when introducing enteral or parenteral nutrition, it is essential to provide comprehensive management that includes maintaining oral intake function and continuing oral care.11 Several studies have been conducted on dysphagia in older adults and its impact on their daily living. Ohta et al examined the relationship between dysphagia and discharge to home in older patients in a rural rehabilitation unit. They found that the presence of dysphagia was negatively associated with home discharge, as effective interventions to manage multimorbidity are lacking.10 Mori et al’s study found that severe dysphagia impacted caregiver well-being and recommended that new multidisciplinary approaches should be incorporated into dysphagia rehabilitation strategies.12 A scoping review was conducted to assess nutritional assessment items in adult patients with oropharyngeal and esophageal dysphagia.13
However, evidence remains limited regarding optimal swallowing evaluation methods and multidisciplinary nutritional management strategies in community-based integrated care wards. In addition, no widely established or directly comparable swallowing screening tool exists.
Therefore, in this study, we aimed to examine whether a swallowing function assessment system consisting of screening tools and meal rounds, administered at the time of admission, can promote safe and appropriate oral intake, contribute to aspiration prevention, lower readmission risk, and reduce caregiving burdens at home. In addition, we propose an operational model for the effective implementation of this system in community-based integrated care wards. This study adds to the existing literature by introducing a novel system to support patients with dysphagia and their caregivers, which may serve as a basis for future approaches aimed at relieving physical discomfort associated with aspiration pneumonia and breathing, distress related to enteral nutrition, and the psychological suffering caused by loss of oral intake, as well as reducing caregiver burden.
Materials and Methods
Research Design
This study was a retrospective observational study conducted in accordance with the STrengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Participants
All patients admitted to the community-based integrated care ward of Yokohama Izumidai Hospital between April 2023 and March 2024 were eligible for inclusion, regardless of age, sex, medical history, primary diagnosis, or level of care at admission. Patients were excluded if they declined participation, were unable to undergo swallowing assessment within 48 h of admission due to medical circumstances (eg, rapid clinical deterioration or emergency discharge), or had severe restrictions on nutritional route changes, such as those admitted solely for palliative care.
Research Procedure
Within 48 h of admission, an original screening tool (developed by a multidisciplinary team and administered at the time of admission) and meal rounds were collaboratively administered by nutritionists, speech-language-hearing therapists, and dental hygienists to assess patients’ oral and pharyngeal function and mode of nutritional intake (Figure 1). The professionals were certified by the Japanese Society of Dysphagia Rehabilitation, each with over 10 years of clinical experience.
 |
Figure 1 Swallowing screening tool at the time of admission. This comprehensive screening tool was developed and administered by a multidisciplinary team of certified nutritionists, speech-language-hearing therapists, and dental hygienists within 48 hours of patient admission to community-based integrated care wards. The assessment comprises six main domains: (1) patient demographic and clinical information; (2) medical history screening for dysphagia-associated conditions; (3) nutritional intake mode before admission and expected discharge destination; (4) communication ability and oral function, including oral cavity environment, molar occlusion, and tongue movement; (5) comprehensive swallowing ability evaluation, including current nutritional intake route (oral, gastronomy, nasogastric tube, TPN, or PPN), dietary form, liquid viscosity requirements, feeding posture, and swallowing-related symptoms; and (6) clinical decision-making regarding FEES, swallowing training, and dental treatment. Multiple evaluation columns allow for serial assessments throughout the admission period. This systematic evaluation enabled identification of discrepancies between prescribed nutritional intake methods and actual swallowing capacity, facilitating appropriate interventions and safe transitions from parenteral nutrition to oral feeding. |
Based on previous studies, meal rounds focused on mandibular movement during mastication (simple elevation/depression, weak rotational movements, or normal rotational movements) and observation of posterior occlusal support.14,15 In the present study, dysphagia diets were classified according to the Dysphagia Diet Classification 2021 (codes: 0t, 0j, 1j, 2–1, 2–2, 3, 4), originally established by the Japanese Society of Dysphagia Rehabilitation in 2013 and revised in 2021. We also examined the relationship between the Japanese Dysphagia Diet 2021 and the International Dysphagia Diet Standardization Initiative, an international standardized benchmark (Table 1).16,17 In cases where pharyngeal residue or silent aspiration was suspected, fiberoptic endoscopic evaluation of swallowing (FEES) was performed for detailed assessment of aspiration risk.18–21
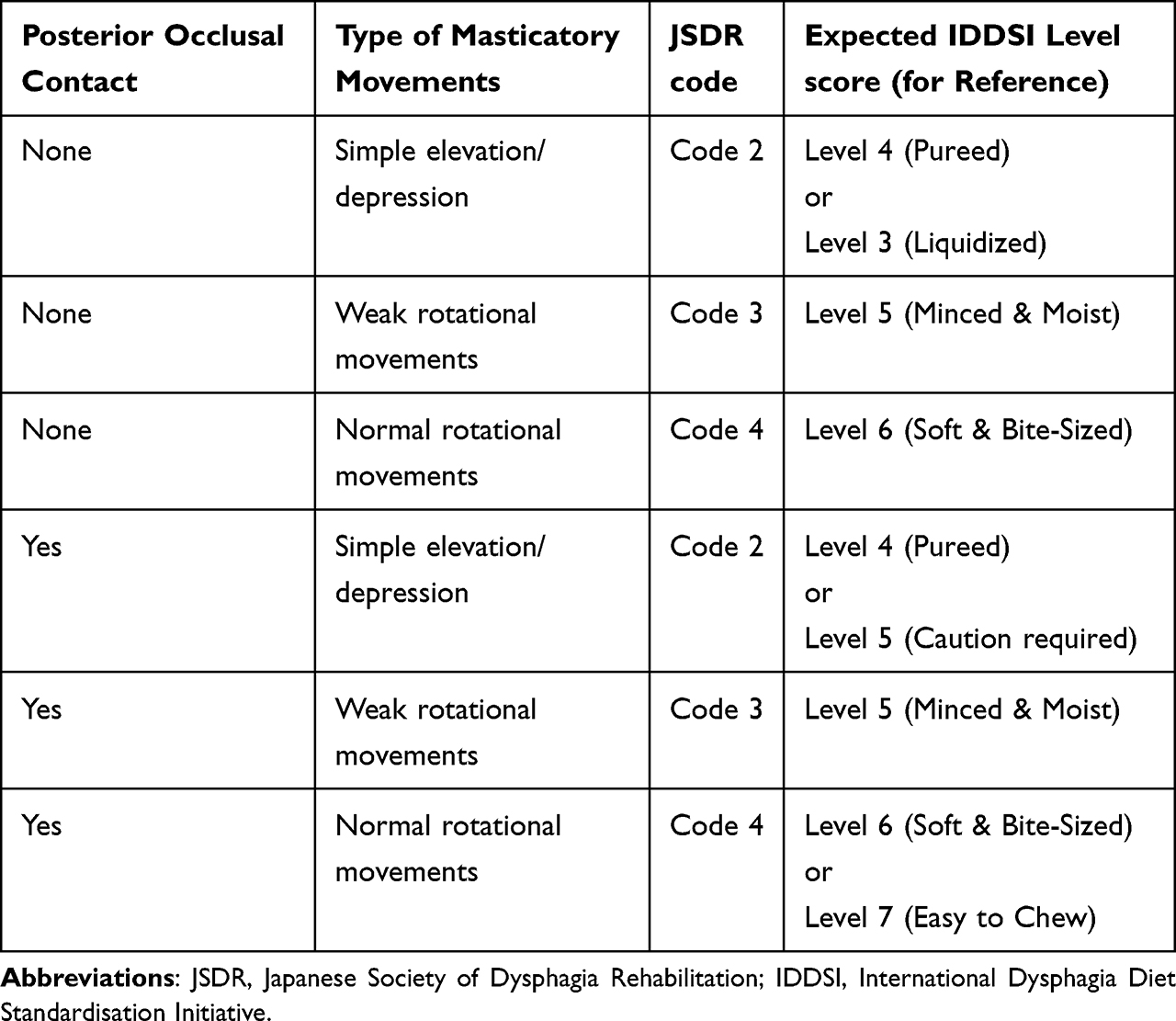 |
Table 1 Correspondence of Posterior Occlusal Support and Mandibular Movements with JSDR and IDDSI Texture Levels |
Patient symptoms were shared among a multidisciplinary team, including physicians, dental practitioners, nurses, dental hygienists, speech-language-hearing therapists, and nutritionists, during weekly conferences, and interventions were implemented as needed.22 First, the mode of nutritional intake, such as pureed food (IDDSI Level 4), soft food, or thickened liquids, was selected and adjusted according to each patient’s swallowing ability. Second, swallowing training and oral rehabilitation were provided to maintain and improve oral and tongue muscle strength. Third, toothbrushing instruction and thorough oral hygiene management were implemented. Fourth, for patients receiving TPN or PPN, transitions to oral intake were made when safety was confirmed through FEES and meal rounds. The primary evaluation items were: (1) types of nutrition delivery routes (oral intake, nasogastric tube feeding, PPN, or TPN); (2) changes in Food Intake LEVEL Scale (FILS) scores before and after the intervention; and (3) discharge destination (home, nursing facility, transfer to another medical institution, such as a rehabilitation or long-term care ward, or death). The FILS is a standardized scale for the quantitative and qualitative assessment of oral food intake, ranging from 1 to 10.23
Statistical Analysis
Using the chi-square test, we examined changes in routes of nutritional supply before and after the intervention and their difference in discharge destinations based on the presence or absence of the intervention. Additionally, changes in FILS scores before and after the intervention were compared using the Wilcoxon signed-rank test. We calculated the effect size r from the Z-value in the Wilcoxon signed-rank test and Cramer’s V in the chi-squared test. Statistical significance was set at p<0.05.
Ethical Statement
The study protocol was approved by the Ethics Committee of Yokohama Izumidai Hospital (approval number: 20240805–1). Written informed consent was obtained from all participants or their legally authorized representatives following a full explanation of the study procedures.
Results
Descriptive Statistics
From April 2023 to March 2024, a total of 77 patients (mean age, 83.9±7.4 years; 38 men and 39 women) admitted to the hospital’s community-based integrated care ward were enrolled as study participants. Aspiration pneumonia (20.8%) was the most common illness, followed by cerebrovascular disorders (18.2%) (Table 2).
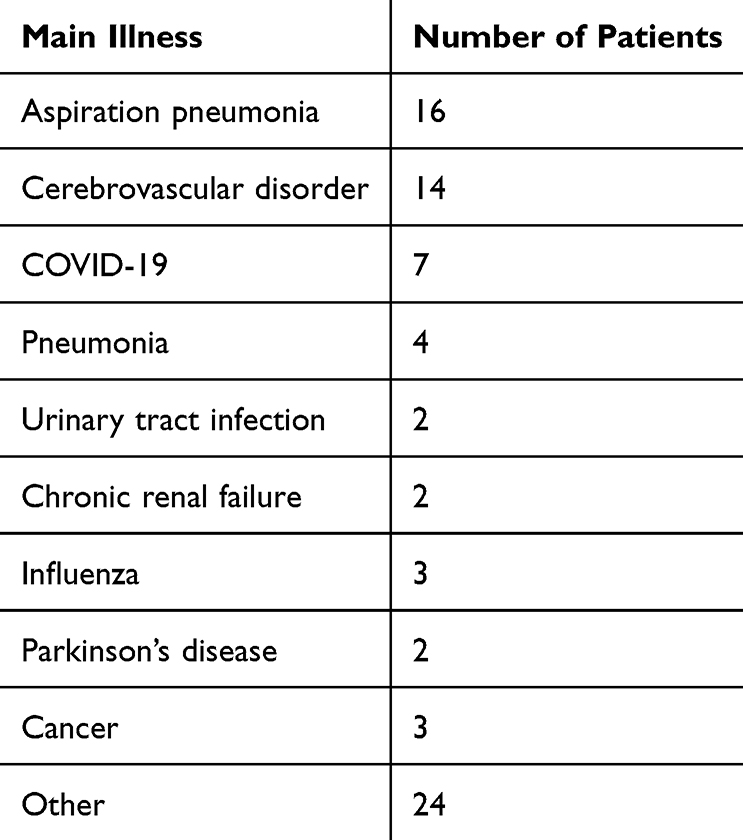 |
Table 2 Distribution of Main Illnesses Among Patients Admitted to the Community-Based Integrated Care Wards |
The results of the chi-square test revealed a significant association between the intervention and route of nutrition supply (χ2(3)=8.40, p<0.05, Cramer’s V = 0.23). Based on swallowing evaluations and meal rounds performed collaboratively by multiple professionals, with interventions tailored to patient symptoms, numerous patients were transitioned to oral intake following FEES and oral rehabilitation. Considering the adjusted residual values among the changes in route of nutrition supply before and after intervention, TPN decreased while oral intake increased. (Table 3).
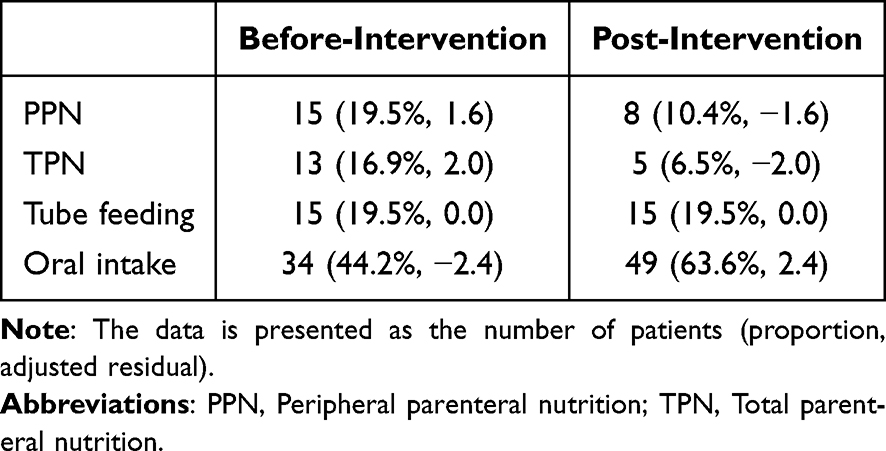 |
Table 3 Changes in Route of Nutritional Supply Before and After Intervention |
Of the 77 patients screened, 62 (81%) had their FILS modified This indicates a mismatch between prescribed diets and actual swallowing ability. After the intervention, the median FILS score improved from Level 4 (restricted oral intake requiring supplemental nutrition) to Level 7 (three oral meals per day with easily consumable foods) (Z=5.757, p<0.05, r=0.66). The number of patients who do not require supplemental nutrition has increased. (Table 4).
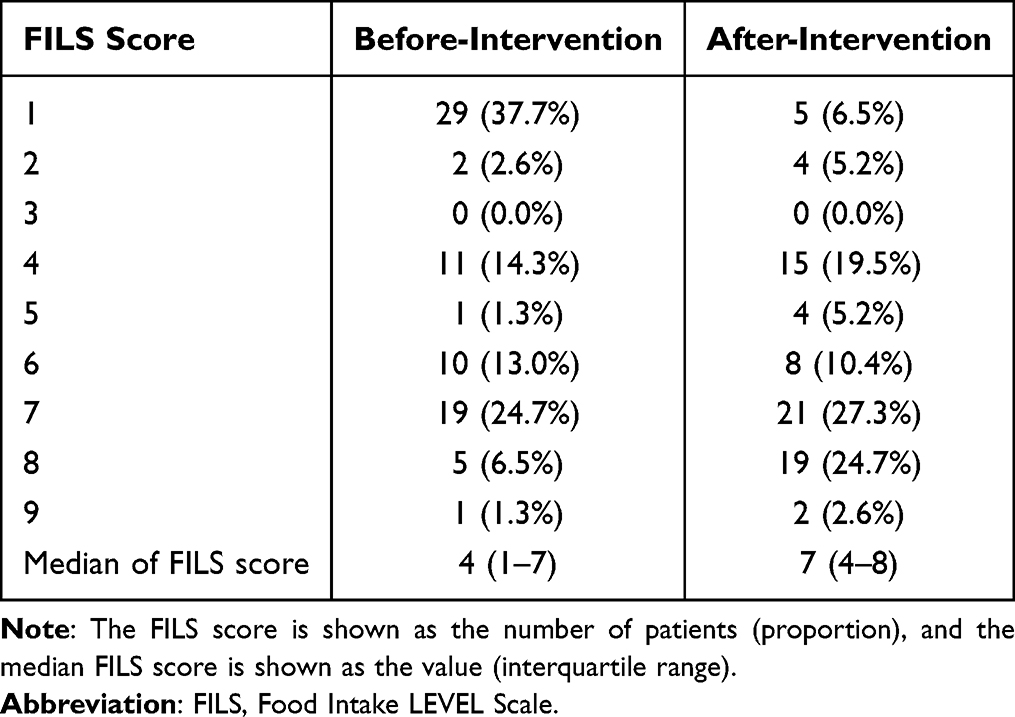 |
Table 4 Changes in Food Intake LEVEL Scale Scores Before and After Intervention |
The results of the chi-square test revealed a significant association between the intervention and discharge outcomes (χ2(3)=24.04, p<0.01, Cramer’s V =0.38). Considering the adjusted residual values for the presence or absence of intervention and differences in discharge destinations, the intervention group had fewer transfers to other hospitals and more discharges to home. For comparison, a non-intervention group was also evaluated. This group consisted of 88 patients who had been admitted to the same community-based integrated care ward during the corresponding period one year earlier (April 2022–March 2023), before the introduction of the current multidisciplinary swallowing-assessment intervention. Their discharge outcomes were compared with those of the intervention group. (Table 5).
 |
Table 5 Difference in Discharge Destinations Based on the Intervention Presence |
Discussion
Our study revealed a very high rate (81%) of diet–texture mismatches, highlighting a substantial clinical gap between the physician- or nurse-ordered diet and patients’ actual swallowing ability at admission. This finding suggests that, even when oral intake has already been initiated, a swallowing assessment may identify the need for texture modification or safer routes of intake. Our discrepancy rate appears substantially higher than adjustment rates reported in previous studies. For instance, Martino et al found that a considerable proportion of acute stroke patients required modification of their prescribed diet or feeding route following swallowing screening (Martino R et al, 2005). Similarly, Beck et al reported that although texture-modified diets and thickened liquids are widely used among adults with dysphagia, the evidence supporting their clinical appropriateness remains limited (Beck AM et al, 2018).
Standardized swallowing screening tools and meal rounds were jointly administered by professionals from multiple disciplines, and patient symptoms were further evaluated during multidisciplinary conferences. The results demonstrated that oral food intake in community-based integrated care wards could be initiated early, with improvements in safety. Although community-based integrated care wards play an important intermediary role in supporting patients’ smooth transition to home or care facilities following acute treatment, operational practices vary across wards, and methods for evaluating swallowing ability and modes of food intake have not been fully standardized.6–8
In the present study, through meal rounds, more appropriate dietary intake modes were selected, and when necessary, FEES and rehabilitation programs were implemented to enhance the safety of oral intake. These interventions supported the transition from TPN and PPN to oral feeding and contributed to improvements in FILS scores. Stable oral intake not only helps prevent aspiration pneumonia but also reduces caregiver burden after discharge.24 In addition, it is likely to lessen the psychological burden on family members and contribute to lower medical costs.11
This study had several limitations. First, this was a retrospective, observational study conducted at a single facility. To improve generalizability to patients with diverse backgrounds, future prospective studies across multiple facilities are warranted. In addition, the validity and reliability of the unique screening tool used were not assessed against other standardized evaluation methods; thus, further research is required to confirm its reproducibility and to follow patients longitudinally after discharge. Nevertheless, in community-based integrated care wards, where patients with various conditions receive intensive care over a short period of time, this tool may support comprehensive evaluations of swallowing ability and facilitate the selection of appropriate dietary intake methods. This may, in turn, contribute to higher rates of patients returning home and lower rates of death prior to discharge. Moreover, the tool has potential to reduce the burden on family members and staff providing in-home nursing care. Multidisciplinary approaches, such as those applied in the present study, highlight the importance of nutritional management and swallowing rehabilitation following acute care, particularly in aging societies. As community-based integrated care wards are unique to Japan, cross-institutional studies should be conducted in these wards and comparable facilities, ideally through collaboration between Japanese and international researchers. Standardization and stronger evidence may ultimately support the development of a global care model for swallowing management.
Our current study suggests that using a multidisciplinary shared swallowing-assessment tool can promote a safe transition to oral intake without the need for detailed instrumental examinations. This approach was associated with improvements in FILS scores and may also help increase rates of discharge to home or care facilities, reduce mortality-related discharges, prevent aspiration pneumonia and readmissions, and lessen caregiver burden. However, further research is needed to confirm these potential benefits.
Conclusions
In the present study, professionals from multiple disciplines administered swallowing screening tools and meal rounds to patients in community-based integrated care wards. Swallowing ability at admission was assessed and, together with interventions planned during multidisciplinary conferences, supported transition from TPN or PPN to oral intake. This method appears feasible for supporting the early and safe initiation of oral food intake. It may help to reduce the risk of aspiration pneumonia and readmission, increase the likelihood of discharge to home or other facilities, and ease caregiver burden; however, these potential benefits should be interpreted with caution. Further evaluation of the effectiveness and reproducibility of such multidisciplinary approaches in prospective, multicenter collaborative studies would therefore be desirable. In addition, efforts are needed to refine their implementation in community-based integrated care wards and to strengthen the evidence base for these practices. Taken together, our findings suggest that a standardized, multidisciplinary assessment of swallowing function at the time of admission to community-based integrated care wards may be a useful approach for promoting a safe and appropriate transition to oral intake.
Declaration
This study adhered to the principles of the Declaration of Helsinki.
Abbreviations
FEES, fiberoptic endoscopic evaluation of swallowing; FILS, Food Intake LEVEL Scale; IDDSI, International Dysphagia Diet Standardisation Initiative; JSDR, Japanese Society of Dysphagia Rehabilitation; TPN, total parenteral nutrition; PP, peripheral parenteral nutrition.
Data Sharing Statement
Additional unpublished data related to this study are available from the corresponding author upon reasonable request. These data are not currently deposited in a public repository but can be shared individually upon reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Yokohama Izumidai Hospital (approval number: 20240805-1). Written informed consent was obtained from all participants or their legally authorized representatives following a full explanation of the study procedures.
Acknowledgments
We would like to acknowledge Editage (https://www.editage.com/) for English language editing.
Funding
This study did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ministry of Health.Labour and Welfare. Ideal Form of Community-Based Integrated Care Wards (From the Viewpoint of Hospital Function).Japanese.Tokyo MHLW.
2. Tsutsui T. Implementation process and challenges for the community-based integrated care system in Japan. Int J Integr Care. 2014;14:e002. doi:10.5334/ijic.988
3. Ministry of Health. Labour and Welfare. Handling of community-based integrated care ward admission fees [in Japanese]. Tokyo: MHLW; March 2020. Available from: https://www.mhlw.go.jp/content/12404000/000638365.pdf.
4. Ministry of Health. Labour and Welfare. Further advancement and promotion of the community-based integrated care system [in Japanese]. Tokyo: MHLW; 2021. Available from: https://www.mhlw.go.jp/content/12300000/000938163.pdf.
5. Ministry of Health. Labour and Welfare. Towards a new vision for regional medical care [in Japanese]. Tokyo: MHLW; 2022. Available from: https://www.mhlw.go.jp/content/10800000/001245115.pdf.
6. Ministry of Health. Labour and Welfare. Regarding community-based integrated care ward admission fees and management fees [in Japanese]. Tokyo: MHLW; March 2020. Available from: https://www.mhlw.go.jp/content/12404000/000864874.pdf.
7. Ministry of Health, Labour and Welfare.Survey Results on Inpatient and Outpatient Medical Care. (Preliminary Report).Japanese.Tokyo.MHLW;2022.Available fromhttps://www.mhlw.go.jp/content/12404000/001110850.pdf.
8. Ministry of Health. Labour and Welfare. New regional medical care vision [in Japanese]. Tokyo: MHLW; October 2023. Available from: https://www.mhlw.go.jp/content/10800000/001309842.pdf.
9. Chu YH, Chao -JC-J. Effectiveness of diet modification on dietary nutrient intake, aspiration, and fluid intake for adults with dysphagia: a meta-analysis of randomized controlled trials. J Nutr Health Aging. 2025;29(4):100486. doi:10.1016/j.jnha.2025.100486
10. Ohta R, Weiss E, Mekky M, Sano C. Relationship between dysphagia and home discharge among older patients receiving hospital rehabilitation in rural Japan: a retrospective cohort study. Int J Environ Res Public Health. 2022;19(16):10125. doi:10.3390/ijerph191610125
11. Çabuk F, Çetiner M. Perspective chapter: parenteral nutrition in intensive care. In: Jalili M, editor. Nutrition During Intensive Care. 2024. doi:10.5772/intechopen.1007799
12. Mori H, Nakane A, Yokota Y, Tohara H, Nakayama T. “Caregiver burden and eating‐related guilt during dysphagia rehabilitation: a descriptive cross‐sectional time series study.”. J Parenter Enteral Nutr. 2024;48(7):818–826. doi:10.1002/jpen.2679
13. Ueshima J, Momosaki R, Shimizu A, et al. nutritional assessment in adult patients with dysphagia: a scoping review. Nutrients. 2021;13(3):778. doi:10.3390/nu13030778
14. Kikutani T. Determination for modified food for the elderly patients with motor masticatory disorders. Ann Jpn Prosthodont Soc. 2016;8(2):126–131. doi:10.2186/ajps.8.126
15. Tagashira I, Tohara H, Wakasugi Y, et al. A new evaluation of masticatory ability in patients with dysphagia: the Saku-Saku Test. Arch Gerontol Geriatr. 2018;74:106–111. doi:10.1016/j.archger.2017.10.010
16. Kayashita J, Fujishima I, Fujitani J. Dysphagia Diet Committee of the Japanese Society of Dysphagia Rehabilitation. et al. The Japanese dysphagia diet of 2021 by the Japanese society of dysphagia rehabilitation. Jpn J Compr Rehabil Sci. 2022;13:64–77. doi:10.11336/jjcrs.13.64
17. Cichero JA, Lam P, Steele CM, et al. Development of international terminology and definitions for texture-modified foods and thickened fluids used in dysphagia management: the IDDSI framework. Dysphagia. 2017;32(2):293–314. doi:10.1007/s00455-016-9758-y
18. Giraldo-Cadavid LF, Insignares D, Velasco V, et al. Fiberoptic endoscopy evaluation of swallowing (FEES) findings associated with high pneumonia risk in a cohort of patients at risk of dysphagia. Dysphagia. 2025;40(1):282–291. doi:10.1007/s00455-024-10727-w
19. Nordio S, Di Stadio A, Koch I, Stritoni P, Meneghello F, Palmer K. The correlation between pharyngeal residue, penetration/aspiration and nutritional modality: a cross-sectional study in patients with neurogenic dysphagia. Acta Otorhinolaryngol Ital. 2020;40(1):38–43. doi:10.14639/0392-100X-2136
20. Neubauer PD, Rademaker AW, Leder SB. The yale pharyngeal residue severity rating scale: an anatomically defined and image-based tool. Dysphagia. 2015;30(5):521–528. doi:10.1007/s00455-015-9631-4
21. Ramsey D, Smithard D, Kalra L. Silent aspiration: what do we know? Dysphagia. 2005;20(3):218–225. doi:10.1007/s00455-005-0018-9
22. Aoki S, Hosomi N, Hirayama J, et al. The multidisciplinary swallowing team approach decreases pneumonia onset in acute stroke patients. PLoS One. 2016;11(5):e0154608. doi:10.1371/journal.pone.0154608
23. Kunieda K, Ohno T, Fujishima I, Hojo K, Morita T. Reliability and validity of a tool to measure the severity of dysphagia: the Food Intake LEVEL Scale. J Pain Symptom Manage. 2013;46(2):201–206. doi:10.1016/j.jpainsymman.2012.07.020
24. Yamaguchi K, Miyagami T, Imada R, et al. Effect of pre-hospital living setting on nutritional intake route upon discharge in older adults with aspiration pneumonia: a prospective cohort study. BMC Geriatr.;25(1):10. doi:10.1186/s12877-024-05659-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Involvement of Older Adults, the Golden Resources, as a Primary Measure for Fall Prevention
Arkkukangas M
Clinical Interventions in Aging 2023, 18:2165-2170
Published Date: 22 December 2023
Caregiver Burden in Bladder Cancer Patients with Urinary Diversion Post-Radical Cystectomy and the Need for Comprehensive Nursing Education: A Narrative Literature
Zhang T, Qi X
Journal of Multidisciplinary Healthcare 2024, 17:3825-3834
Published Date: 7 August 2024
Yoga Practice as a Potential Sarcopenia Prevention Strategy in Indonesian Older Adults: A Cross-Sectional Study
Meiliana A, Dewi NM, Latarissa IR, Barliana MI, Alfian SD, Yulianti T, Wijaya A
Open Access Journal of Sports Medicine 2025, 16:3-13
Published Date: 10 January 2025
Nursing Interventions in Palliative Care for Advanced Dementia: A Systematic Review of Symptom, Relief, Comfort, and Caregiver Support
Pujante VGB, Sami W, Al-Kuwari NF, Rizvi MR
Journal of Multidisciplinary Healthcare 2025, 18:6545-6564
Published Date: 9 October 2025