Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Assessing Lifestyle Goal Setting in Patients with COPD
Authors Born CDC ![]() , Beijers RJHCG, van Iersel LEJ, Muijrers IHMJE, Schuurman LT, Gerards SMPL, Simons SO
, Beijers RJHCG, van Iersel LEJ, Muijrers IHMJE, Schuurman LT, Gerards SMPL, Simons SO ![]() , Gosker HR
, Gosker HR ![]() , van Helvoort A, Schols AMWJ
, van Helvoort A, Schols AMWJ ![]() , Crutzen R
, Crutzen R
Received 14 November 2025
Accepted for publication 9 March 2026
Published 31 March 2026 Volume 2026:21 579191
DOI https://doi.org/10.2147/COPD.S579191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Charlotte DC Born,1 Rosanne JHCG Beijers,1 Lieke EJ van Iersel,1 Imke HMJE Muijrers,1 Lisanne T Schuurman,1 Sanne MPL Gerards,2 Sami O Simons,1 Harry R Gosker,1 Ardy van Helvoort,1,3 Annemie MWJ Schols,1 Rik Crutzen4
1Department of Respiratory Medicine, NUTRIM Institute of Nutrition and Translational Research in Metabolism, Maastricht University Medical Centre+, Maastricht, the Netherlands; 2Department of Health Promotion, NUTRIM Institute of Nutrition and Translational Research in Metabolism, Maastricht University Medical Centre+, Maastricht, the Netherlands; 3Danone Research & Innovation, Utrecht, the Netherlands; 4Department of Health Promotion, Care and Public Health Research Institute (CAPHRI), Maastricht University Medical Centre+, Maastricht, the Netherlands
Correspondence: Rosanne JHCG Beijers, NUTRIM Institute of Nutrition and Translational Research in Metabolism, Department of Respiratory Medicine, Universiteitssingel 50, Room 5.228, P.O. Box 5800, Maastricht, 6202 AZ, the Netherlands, Email [email protected]
Purpose: Healthy lifestyle changes can reduce symptoms and slow disease progression in patients with chronic obstructive pulmonary disease (COPD). To tailor strategies supporting long-term behavior change, this study investigated patients’ willingness to set lifestyle goals during personalized counseling. Goal focus and content, goal adjustments over time, reasons for unwillingness, barriers and facilitators, and differences between goal setters and non-goal setters were also examined.
Patients and Methods: As part of an ongoing randomized controlled trial (NCT03807310), patients received monthly phone calls over 12 months, offering lifestyle counseling on diet and physical activity (PA) using motivational interviewing. Data were analyzed for a subset of patients who had completed the trial by 12 February 2025. Baseline trial data were used for patient characterization, and counseling notes were analyzed to assess willingness and factors affecting goal setting.
Results: Data from 103 patients (61.2% male, mean age 68.3± 6.5 years, body mass index 26.3± 4.9 kg/m2, FEV1 56.6± 18.1% predicted), were analyzed. Overall, 71% were willing to set lifestyle goals, most often focused on PA. About one-quarter adjusted their goals during follow-up due to achievement or health complaints (PA) and previous unsuccessful attempts (diet). Patients unwilling to set goals mainly reported satisfaction with current habits or no perceived need for change. Experienced facilitators included accountability and favorable weather (PA) and visual reminders, social support, and seasonal influences (diet). Barriers were mainly health complaints (PA) and low motivation (diet). No differences were found between goal setters and non-goal setters in demographic, physiological, lifestyle or motivational characteristics.
Conclusion: A majority of patients with COPD were willing to set lifestyle goals, particularly related to PA, but satisfaction with current behaviors and health-related barriers often limited engagement. These findings provide input for the design of future interventions to support sustainable lifestyle change in COPD care.
Plain Language Summary: People with chronic obstructive pulmonary disease (COPD) often benefit from healthy lifestyle changes, such as being more active and improving their diet. These changes can reduce symptoms and help slow disease progression. However, patients may need support to make lifestyle changes by breaking them into manageable steps, or “goals”.
This study looked at how willing patients with COPD were to set goals concerning changes in lifestyle when offered personalized counseling over the phone. Patients received monthly calls for 12 months, focusing on physical activity and diet, using supportive conversation techniques to encourage behavior change. Notes from these calls were analyzed to understand goal setting, reasons for reluctance, and factors that helped or hindered progress.
Among 103 patients, about 7 out of 10 were willing to set goals, most often related to physical activity. Some patients adjusted their goals during the study due to achieving or struggling with initial goals, or because of health issues. Those who did not want to set goals usually felt satisfied with their current habits or saw no need to change. Factors that helped patients work on their goals included, for example, accountability (eg, a dog that needs walking) and social support, while barriers included health complaints and low motivation.
These results show that most patients are willing to set goals, but satisfaction with current habits and health challenges can limit engagement. Understanding these factors can help healthcare providers improve programs to encourage sustainable lifestyle changes and improve quality of life for people with COPD.
Keywords: chronic respiratory disease, physical activity, nutrition, behavior change, counseling
Introduction
Chronic obstructive pulmonary disease (COPD) is a common and heterogenous lung disease, affecting approximately 10.3% of the global population and accounting for nearly 5% of all deaths.1,2 The burden of COPD is expected to grow due to an aging population and ongoing exposure to risk factors.1 Although COPD is a progressive, incurable disease, it is both preventable and treatable. While smoking and air pollution are the most well-established risk factors, growing evidence highlights the critical role of lifestyle in COPD prevention and management.3 A healthy lifestyle, including regular physical activity (PA) and good dietary quality, has been shown to reduce symptoms and slow disease progression in patients with COPD.4,5
PA levels in patients with COPD are significantly lower than in healthy populations. These levels decline further as the disease progresses, and physical inactivity is associated with higher hospital readmission rates and mortality.4,6–8 In parallel, the quality of dietary intake of patients with COPD is generally poor, and literature suggests this may be particularly pronounced in those with disturbed body composition, such as low fat-free mass or abdominal obesity.9 A Western diet is also associated with accelerated decline in pulmonary function.5 Furthermore, recent evidence shows the potential beneficial role of healthy dietary patterns on clinical outcomes including fatigue, sleep quality, depression, activities of daily living, and disease severity in patients with COPD.10
Factors such as older age and low socioeconomic status (SES), respiratory disease severity, dyspnea, fatigue and co-morbidities are associated with reduced PA and dietary quality in patients with COPD.11–13 Certain clinical phenotypes such as sarcopenic obesity (SO), have been linked to worse health-related quality of life (QoL) and increased physical limitations, which may also influence engagement in PA.14 A qualitative study identified several barriers to PA engagement in patients with COPD that were closely related to self-efficacy beliefs and symptom severity, including health related (eg fatigue, mobility problems, breathing issues caused by the weather), psychological (eg embarrassment, fear, frustration/disappointment), attitudinal (feeling in control of their condition, PA perception, older age perception), and motivational aspects.15 Taken together, these findings suggest that effective tailoring of interventions for patients with COPD should address both clinical characteristics and individual differences in psychological, attitudinal, and motivational factors.
In recent years, COPD management programs are focusing more on stimulating and supporting behavioral change in PA and diet through counseling, moving beyond exercise training and nutritional supplementation.16 The incorporation of counseling, supported by motivational interviewing (MI) techniques, is considered essential for achieving sustainable behavior change.17 MI is a person-centered counseling approach designed to enhance intrinsic motivation for behavior change. Through goal-setting techniques, patients are guided to identify lifestyle changes that align with their personal values and to break these down into manageable steps.18–20 In this process, the initiative shifts to the patient, who is encouraged to take an active role in setting personal goals, in contrast to the traditionally physician-led approach often seen in COPD management.
Although the effects of counseling interventions on PA levels and dietary outcomes in populations with COPD remain inconsistent, two systematic reviews concluded that studies incorporating individual goal setting (that was regularly revised) were more successful.12,21–23 The potential benefits suggest that integrating lifestyle counseling into COPD care is essential for improving patient reported outcomes. In its latest official position statement on PA in COPD, the European Respiratory Society recommended assessing readiness and motivation for change, incorporating behavior-change techniques, and ensuring frequent contact time to enhance the effectiveness of behavioral interventions.4 Despite a growing number of counseling interventions being implemented in research settings, little is known about patient willingness to engage in lifestyle goal setting. One study evaluating a self-management intervention using MI reported that goals were set in 83% of counseling sessions, suggesting high engagement when prompted.24 However, less is known about patient willingness when counseling is offered voluntarily, meaning optional counseling that patients may accept or decline, rather than as part of a structured intervention. Gaining insight into patient willingness to engage in lifestyle goal setting, and the factors influencing this process, may be a first step to help tailor more effective counseling strategies and interventions to support sustained behavior change.
To better understand patient engagement in lifestyle counseling and the factors influencing goal setting, we conducted an explorative, inductive sub-study. The primary aim was to investigate the willingness of patients with COPD to set lifestyle-related goals during personalized counseling. Secondary aims were to describe the focus (PA, diet or both) and content of goals, and the adjustment of goals over time; explore reasons for unwillingness to set goals, as well as barriers and facilitators to pursuing goals; and examine differences between goal setters and non-goal setters in demographic, physiological, lifestyle, and motivational characteristics.
Materials and Methods
Study Population
This was a sub study of the ongoing randomized controlled NUTRECOVER trial (NCT03807310), primarily investigating the effects of 1-year targeted nutrient supplementation on PA level and health-related QoL in patients with COPD. A detailed description of the NUTRECOVER trial has been described elsewhere.25
The NUTRECOVER trial began data collection on 16 October 2020 and aims to include 166 patients with COPD. For the current study, we used data from a subset of patients who, by 12 February 2025, had either completed the NUTRECOVER trial or dropped out. Patients were recruited via multiple hospitals, including the Maastricht University Medical Centre+ (MUMC+), VieCuri, and Zuyderland, in the province of Limburg, the Netherlands. Included patients had moderate to very severe COPD (GOLD stage II–IV) based on extensive lung function measurements recorded in hospital records. Patients were clinically stable and had no comorbid conditions that could affect the intervention, such as a history of lung cancer within the past five years, neurodegenerative disorders, or gastrointestinal disorders. All patients included in the NUTRECOVER trial were eligible for lifestyle counseling.
Study Design and Lifestyle Counseling
Patients received monthly phone calls from one of the counsellors (LvI, LS, CB, TT, or IM), with the initial call occurring one month after the NUTRECOVER trial inclusion (Figure 1). These phone calls continued throughout the 12-month study period, allowing for a maximum of 11 calls per patient. The calls were intended to last no more than 30 minutes. During these calls, the occurrence of possible adverse events was checked, and supplement intake was monitored. Additionally, lifestyle counseling was offered. In case patients were open to lifestyle counseling, they were asked to construct goals based on their PA level and/or dietary pattern. Every following month, the goals were subsequently discussed and potentially adjusted. In case patients were not open to lifestyle counseling and initially declined to set a goal, they were offered the possibility again in the following months. This offer was repeated at least once during the study. This also means that goals could be established at a later stage during the study.
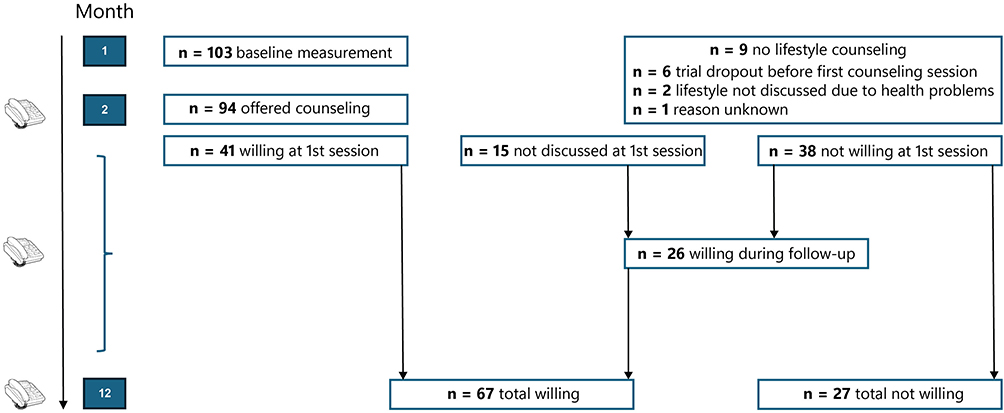 |
Figure 1 Overview of the study timeline and participant flow regarding lifestyle counseling. Patients received monthly phone calls offering lifestyle counseling, with the initial call occurring one month after the NUTRECOVER trial baseline measurement. These phone calls continued throughout the 12-month study period. A total of 103 participants completed the baseline measurement; 94 were offered lifestyle counseling. Of these, 41 were willing to set lifestyle goals during the first session, 15 did not discuss lifestyle changes at that time, and 38 were not initially willing. During follow-up, 26 additional participants became willing, resulting in overall 67 participants willing to set a goal and 27 not willing to set a goal by the end of the study. Nine participants did not receive lifestyle counseling due to dropout, health problems, or unknown reasons. |
Lifestyle counseling was guided by the Self-Determination Theory, a psychological framework emphasizing autonomy, competence, and relatedness in behavior change.26 MI techniques were employed to encourage self-directed goal setting, which has been shown to enhance intrinsic motivation and long-term behavior change, also in COPD management.17,27 These included the use of open-ended questions, reflective listening, affirmations, and summarizing, as well as exploring ambivalence, supporting self-efficacy by encouraging achievable goals, and emphasizing patient autonomy. Counsellors refrained from giving direct advice, instead helping patients to identify their own motivations for change and reinforcing positive experiences. The primary aim of the lifestyle counseling was to encourage patients to adopt healthier behaviors.
During the counseling sessions, notes were drafted based on a guidance document (see Supplementary Material 2) with open-ended questions on predefined topics, including lifestyle habits, barriers, facilitators, and goals, to ensure consistency across patients. In the first session, the counseling notes included detailed records of patients’ current lifestyle habits, identified healthy and unhealthy behaviors, and the specific goals set around PA and/or diet. Even if patients chose not to set goals, their lifestyle patterns and motivations were still explored and recorded. During the following sessions, notes captured patients’ progress toward their goals, reflections on facilitators and barriers, and any adjustments made to their goals.
Data Extraction
To ensure consistency in data extraction, two researchers (CB and IM) independently analyzed the counseling notes of an initial 10% of patients in duplicate (data extraction form available on OSF). Consensus meetings were held to resolve discrepancies and establish standardized rules for further extraction. To assess inter-rater reliability after initial alignment, the researchers independently extracted data for two additional patients. For the two independently analyzed patients, agreement was assessed across the available variables. For the first patient, agreement was 88.7% across 115 variables. For the second patient, who dropped out at session 5, agreement was 97.3% across 37 variables. This resulted in an overall agreement of 90.8%. Given this high level of agreement, both researchers proceeded to extract data from the remaining counseling notes independently. Data-extraction of the counseling notes was never done by the same researcher that also drafted the notes.
Extracted data for the first phone call session included (1) whether patients were willing to set (a) goal(s) (yes/no), (2) if not, the reason for unwillingness, (3) whether the goal(s) was/were related to PA, diet or both, and (4) the specific goal constructed. For the following sessions it was also recorded whether goals were adjusted (yes/no), and if mentioned, the reasons for adjustment. Barriers and facilitators for reaching goals were also extracted from the counseling notes. Elements were considered facilitators if the patient explicitly indicated that a factor helped them adhere to a goal, and barriers if the patient reported a factor that made adherence more difficult. A goal was defined not only when it was explicitly named as such but also when patients expressed an intention to try or achieve something specific. In cases of uncertainty for the researcher, the determination of a goal was verified by checking whether it was followed up in subsequent sessions; if it was, it was classified as a goal. Patients were considered goal setters if they set at least one goal at any point during the 12-month counseling period, regardless of whether it occurred during the first session or later in the study.
Baseline Characteristics
This study used baseline data from the NUTRECOVER trial, collected during a measurement day at the MUMC+. This visit included assessments of PA level, QoL, physical performance, exercise performance, body composition, lung function, dietary intake, and motivation towards exercising as described in Beijers et al, (2022).25
Additionally, sarcopenia was defined according to the European Working Group on Sarcopenia in Older People (EWGSOP) guidelines, using the following criterion: low muscle quantity (Appendicular Skeletal Muscle Mass Index (ASMI) < 7.0 kg/m2 for men and <5.5 kg/m2 for women).28 Patients with co-existing obesity (≥ 30 kg/m2) and sarcopenia were classified as having SO.29,30 SES was determined using SES-WOA scores based on 4-digit postal codes.31 The score is based on financial wealth, educational level, and recent employment history of private households on January 1, 2019. The average SES-WOA score for the Netherlands is 0. Positive scores (> 0) indicate a higher-than-average SES and negative scores (< 0) a lower-than-average SES. More details on all measurements can be found in Supplementary Material 1.
Data Analysis
Descriptive statistics (means and frequencies) were first computed to summarize baseline characteristics. Data normality was assessed by visual inspection of histograms and the Shapiro–Wilk test. Continuous variables were summarized using means and standard deviations (SD) if normally distributed, or medians and interquartile ranges (IQR) if not normally distributed.
To address the primary aim of investigating patients’ willingness to set lifestyle goals, absolute frequencies and percentages of goal setters and non-goal setters were calculated.
For the secondary aim of describing the focus and content of goals, the number and proportion of goals targeting PA, diet, or both were summarized. Representative examples of patient-set goals were also selected and presented according to their goal focus. Adjustments to goals over time were analyzed descriptively by reporting absolute frequencies and percentages of participants who adjusted their goals, along with the reasons for these adjustments when provided. Representative examples of adjusted goals were included.
To explore reasons for goal adjustment, unwillingness to set goals, and barriers and facilitators to pursuing goals, participant statements were categorized into themes using a data-driven, inductive approach. The frequency of occurrence for each theme was quantified, and illustrative statements were presented.
Finally, to examine differences between goal setters and non-goal setters across baseline characteristics, including demographic, physiological, lifestyle, and motivational variables, independent t-tests or Mann–Whitney U-tests were used for continuous variables (depending on distribution), and chi-square tests were used for categorical variables.
Statistical analyses were conducted in IBM SPSS, version 28. Two-sided p-values <0.05 were considered statistically significant.
Results
Baseline Characteristics
A total of 103 patients had completed the trial by February 12, 2025, and were included in this study. Patients had a mean age of 68.3 ± 6.5 years and 61.2% were male, see Table 1 for baseline characteristics. Socio-economic status (−0.1±0.2) was slightly lower than the national average (SES-WOA score of 0). Mean BMI was 26.2 ± 4.9 kg/m2, with 35.9% of patients classified as overweight and 18.4% as obese. Among the patients, 30.1% were sarcopenic, but no one was classified as having SO. While 46.6% of patients were categorized as having moderate COPD (GOLD II), nearly 40% had severe or very severe disease (GOLD III–IV). The mean FEV1 was 56.6 ± 18.1% predicted. Patients had a median daily step count of 4026.0 steps [IQR: 2652.0–6788.5]. Median daily energy intake was 24.9 kcal/kg body weight [IQR: 18.3–28.6] in men and 26.6 kcal/kg body weight [IQR: 19.2–34.8] in women. Prior to the start of the counseling sessions, the median scores for intrinsic and identified regulation towards exercising were 4.0 [IQR: 3.0–5.0] and 4.0 [IQR: 4.0–5.0] out of 5, respectively.
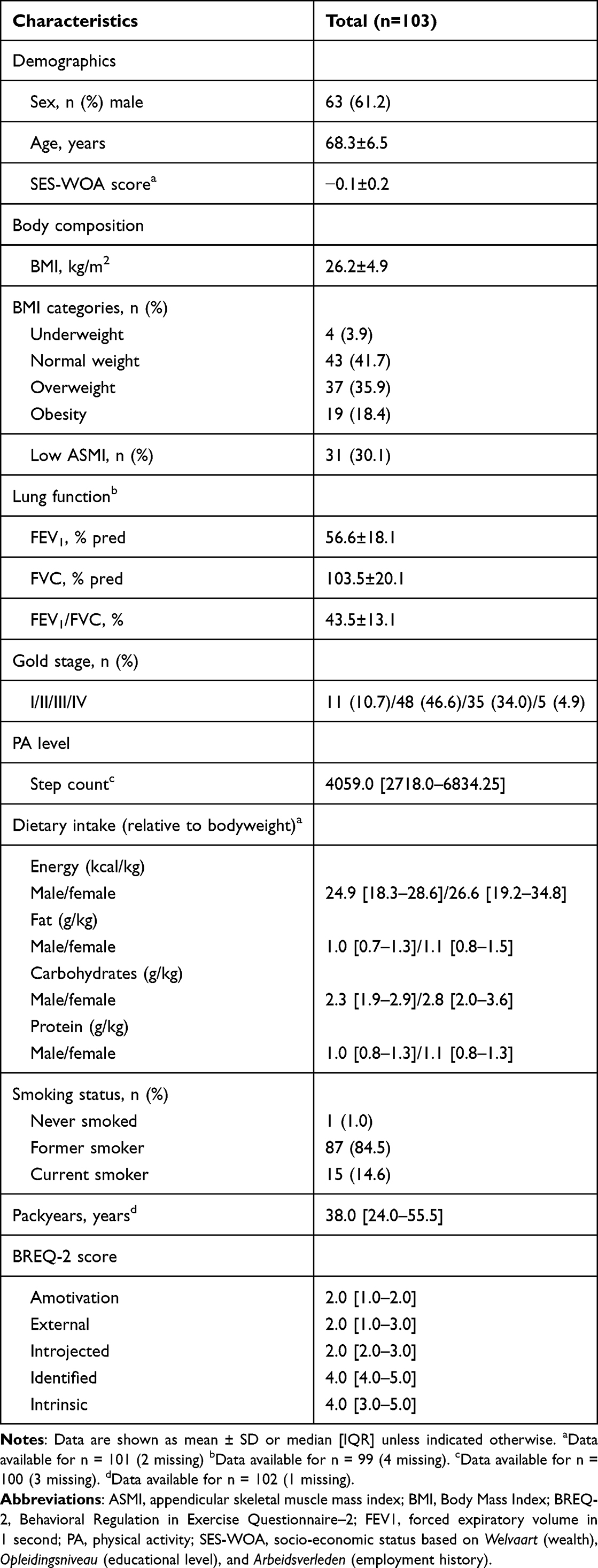 |
Table 1 Baseline Characteristics of the Total Study Sample (n=103) |
Willingness to Set Goals, Goal Focus and Examples of Set Goals
For nine patients (8.7%), lifestyle goal setting was never discussed due to dropout from the trial, either dropout before the first counseling session (66.7%) or later in the study, at a point when lifestyle had not yet been addressed (eg because of significant health issues) (Figure 1).
Out of the 94 patients who were given the opportunity to set lifestyle goals, 41 were willing and 38 were not willing to set a goal during the first counseling session, while goal setting was not discussed for 15 patients. For these 15 patients, lifestyle was not discussed due to health complaints (n = 2), the scheduled call not taking place (n = 2), the patient having no time to discuss lifestyle during the call (n = 4), or unknown reasons (n = 7). During subsequent counseling sessions, 26 patients who were initially unwilling or for whom goal setting was not discussed during the first session became willing to set a goal. Overall, 67 patients (71.3%) were willing to set at least one lifestyle goal related to either PA or diet, whereas 27 patients (28.7%) remained unwilling to set a goal. The maximum number of goals set during a single session was four. Among patients who set goals, 52.2% set a goal related to PA, 22.4% set a dietary goal, and 25.4% set goals addressing both PA and diet.
Table 2 shows a selection of patient-set PA and dietary goals, illustrating the wide range and personalized nature of these goals. Regarding PA, some goals focused on step counts, varying from as low as 3000 steps per day to as high as 7000 steps per day. Other goals emphasized maintaining independence through daily household activities, resuming physiotherapy, increasing outdoor activity when weather permitted, or maintaining physical fitness and activity levels. Regarding diet, some patients aimed to increase healthy food intake, such as eating more fruit or vegetables, while others focused on reducing intake of specific items like snacks, fried foods, or sugar-sweetened beverages. Several goals involved strategies for hydration, portion control, or regular meal patterns, including eating lunch daily or maintaining three meals per day. These examples reflect both specific and broader intentions related to dietary behavior.
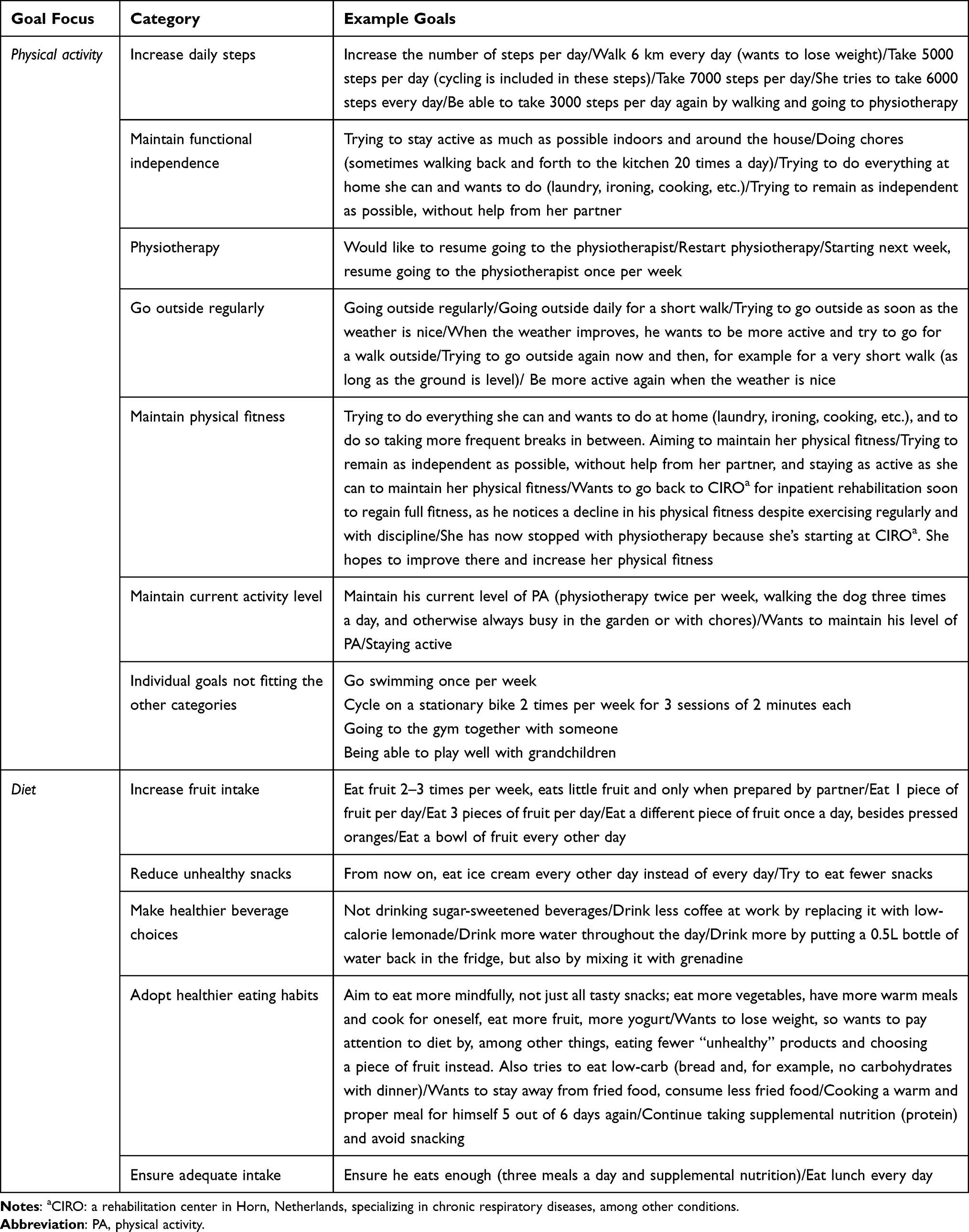 |
Table 2 Examples of Patient-Set Goals by Goal Focus (Physical Activity or Diet) |
Adjustment of Goals Over Time
Among the 67 patients who set goals, 25.4% adjusted their goals over the course of the 12-month period (across a total of 11 counseling sessions). Adjustments to PA goals were made for various reasons, with the main reasons being achievement of a previous goal and experiencing health complaints. Other reported reasons included recovery from health complaints, time constraints, changes in personal circumstances, a desire to increase weight loss, or to enhance enjoyment of the goal. These adjustments involved either increasing or decreasing the difficulty or frequency of the goal, modifying the start time, or making practical changes such as shifting the location of the activity. The latter occurred, for example, due to the reopening of gyms following COVID-19 restrictions, a transition from regular physiotherapy to pulmonary rehabilitation, or a desire to maintain physical fitness after completing rehabilitation. In some cases, goals remained similar in difficulty but were revised for greater specificity, with no clearly stated reason for the change.
Dietary goals were adjusted for reasons including the achievement of previous goals, adaptation following earlier unsuccessful attempts (ie, making the goal more achievable), and receiving recommendations from health professionals. Table 3 presents examples of adjusted PA and dietary goals, along with the type of adjustment (eg increase or decrease in difficulty), and the reasons for these adjustments.
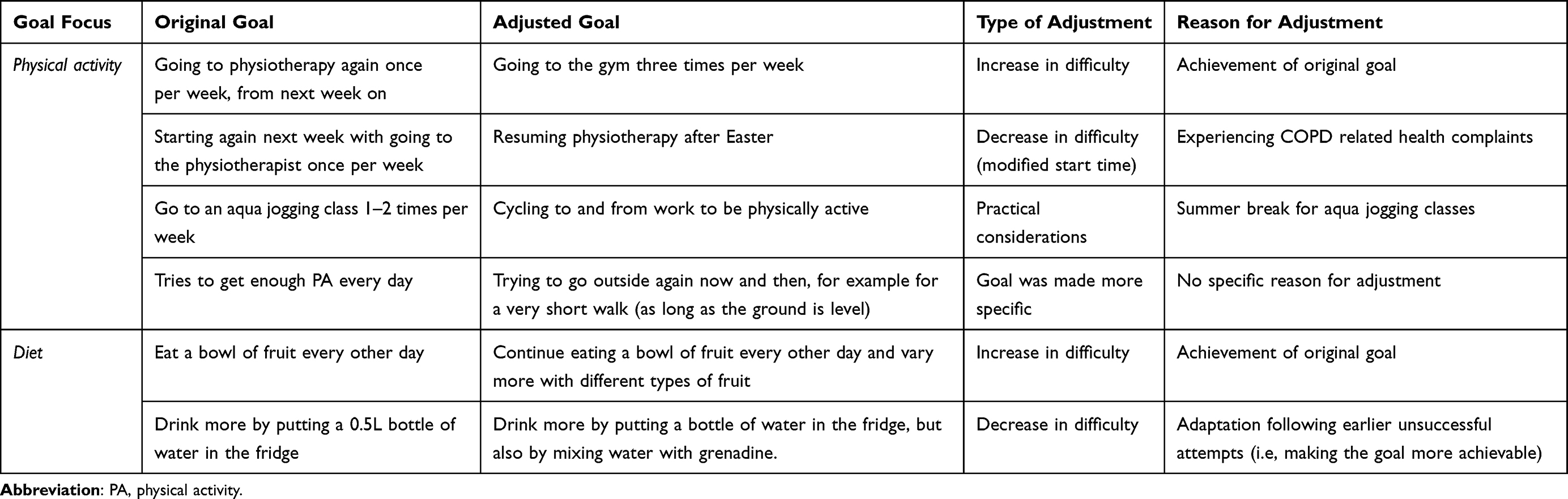 |
Table 3 Examples of Adjusted Physical Activity and Dietary Goals, the Type of Adjustment, and Corresponding Reasons for Adjustment |
Insights into Goal-Setting Behavior
Reasons for Unwillingness to Set Goals
Among patients who never set a goal (n=27), the most frequently reported reason was being satisfied with their current PA behavior (48.1%) and eating behavior (33.3%). One participant, for example, stated being satisfied with his activity level (walking well over 10,000 steps daily) and being content with his diet, which included adequate intake, plenty of fruit, whole grain bread, and dairy. As a result, he felt there were no specific goals to pursue. A perceived lack of need for change was also a commonly reported reason for not setting goals, mentioned by 22.2% of patients for PA and by 29.6% for diet. For example, a participant stated that he wanted to keep everything as it was. Additional reasons for not engaging in goal setting included receiving concurrent lifestyle support through pulmonary rehabilitation (PA: 7.4%), experiencing health complaints, either general (diet: 7.4%) or related to COPD (PA: 11.1%, diet: 7.4%), and a preference for self-management (7.4% for both PA and diet), meaning patients indicated they were already working on their lifestyle independently and did not feel the need for help. A small proportion (3.7%) indicated a lack of time for engaging in lifestyle change. No specific reason was provided in 22.2% of cases for refraining from goal setting related to either PA or diet.
In addition to some of the reasons reported by patients who never set goals, including satisfaction with PA or eating behavior, no perceived need for change, already receiving lifestyle support, health complaints (lung-related or general), or lack of time, patients who did set goals at some point during the 12-month period also reported additional reasons for not setting a goal during specific sessions. These included being unable to identify goals, experiencing health complaints due to a COVID-19 infection, financial constraints (eg physiotherapy only being reimbursed once instead of twice per week), lack of a sense of accountability (eg absence of scheduled appointments with a physiotherapist), psychological burden, feeling they had already reached their maximum effort, and not being open to change.
Barriers and Facilitators to Pursuing Goals
Physical Activity
When working on PA goals, the most frequently reported facilitators were being held accountable (eg having a dog that needs to go for a walk) and favorable weather conditions. Additional facilitators included support from healthcare professionals, perceived progress and importance of goals, the motivation to maintain independence, self-regulation of activity and rest (eg one participant described that she could remain active if she took sufficient breaks), support from loved ones (eg exercising together), a good balance between work and daily activity, enjoyment of PA (eg enjoying walking), engaging in meaningful activity to prevent boredom, and fear of job loss as a motivator (eg needing to stay active for work).
Conversely, health complaints, both pulmonary and non-pulmonary, were the most reported barriers to working on PA goals. Bad weather (eg rain, cold, heat, or high humidity) was also frequently mentioned. Other barriers included fear of COVID-19 (eg vaccination not yet available), emotional distress or grief, financial limitations (eg physiotherapy only being reimbursed once instead of twice per week), lack of access to facilities, an unfavorable work-life activity balance, unrealistic goal setting, no perceived progress, decreased physical fitness, weekend-related sedentary behavior, being busy with other responsibilities, absence of follow-up after rehabilitation, and fatigue.
Diet
For dietary goals, key facilitators included the use of visual reminders (eg placing a glass of water on the kitchen counter), support from loved ones, and seasonal influences such as the increased availability of appealing fruits during the summer. Other facilitators mentioned were perceived importance and understanding of healthy eating, exposure to health education provided by the counsellors, experienced health benefits, the substitution of unhealthy foods with healthier alternatives, taste preference (eg choosing fruits one enjoys), convenient food choices, alternating between different types of fruit, and easy access to healthy options.
The most frequently reported barrier while working on a dietary goal was lack of motivation. Additional barriers included forgetfulness, a low perceived importance of dietary change, considering dietary change a low priority, a lack of availability (eg one participant was noted to skip eating fruit for a day if he had forgotten to add it to the shopping list, and therefore did not have any at home), being busy with other responsibilities, seasonal influence leading to less healthy food choices (eg greater temptation to eat ice cream during summer), food cravings, and a lack of cooking skills that make preparing healthy meals difficult.
Differences Between Goal- and Non-Goal Setters
Table 4 presents differences between goal setters (n=67) and non-goal setters (n=27) across demographic, physiological, lifestyle and motivational characteristics. No differences were seen in any of these characteristics. Additionally, there were no differences in motivation towards exercise, as measured by BREQ-2 scores, between patients who set a PA goal and those who did not.
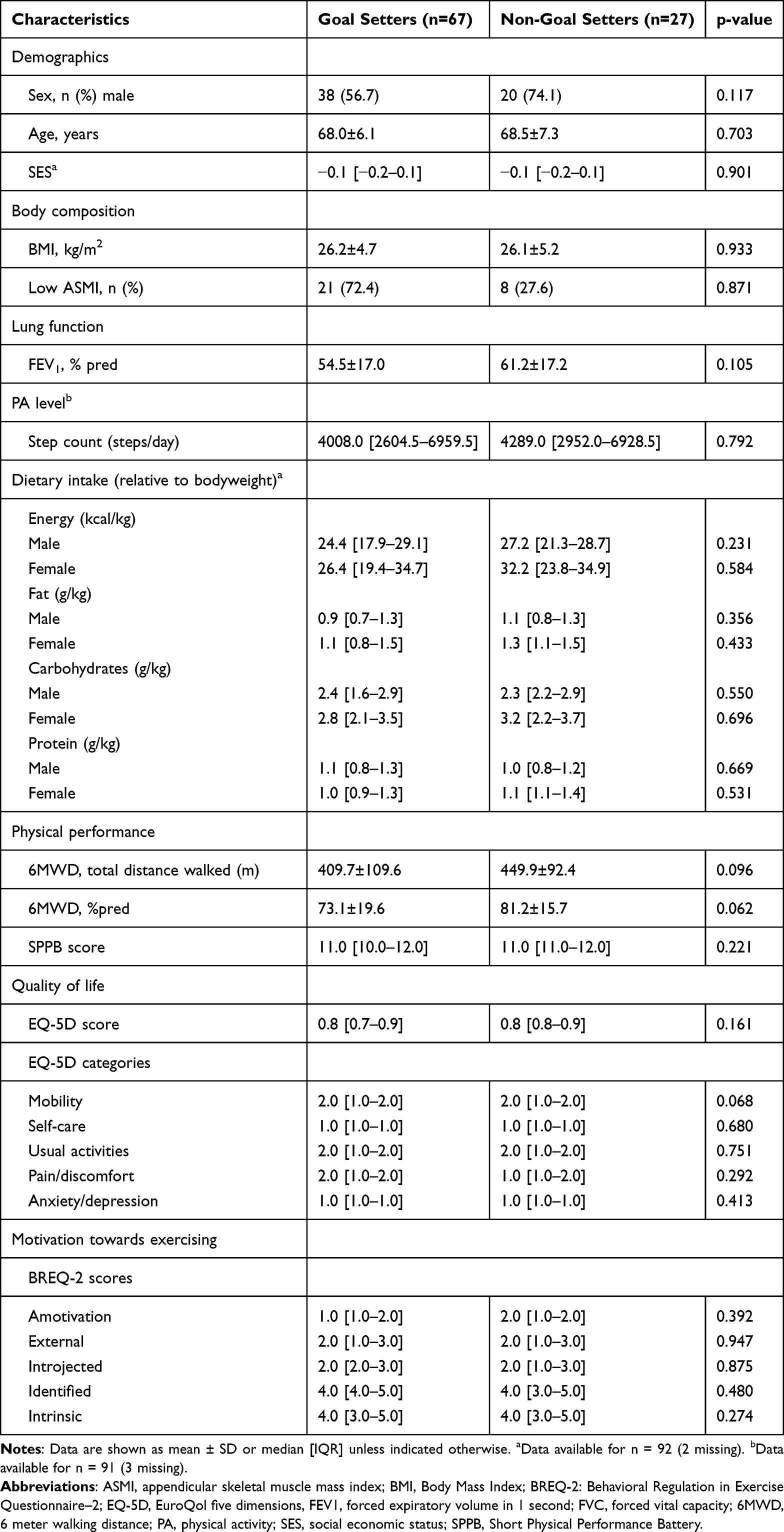 |
Table 4 Differences Between Goal Setters (n=67) and Non-Goal Setters (n=27) in Demographic, Physiological, Lifestyle and Motivational Characteristics |
Discussion
In this study, we examined the willingness of patients with COPD to engage in lifestyle goal setting as part of personalized counseling and the factors influencing this process. The majority of patients were willing to set at least one lifestyle goal, with a particular focus on PA, either alone or in combination with diet. Over the course of the counseling period, some patients adjusted their goals, most often because they had achieved their initial goal or faced health complaints in the case of PA goals, and because of previous unsuccessful attempts in the case of dietary goals. Patients who chose not to set goals mainly reported being satisfied with their current lifestyle habits or perceiving no need for change. When working on goals, patients reported various facilitators, such as being held accountable and favorable weather conditions for PA, and the use of visual reminders, social support, and seasonal influences for diet. Key barriers included health complaints, both pulmonary and non-pulmonary, which most often hindered progress on PA goals, while lack of motivation emerged as the most frequently reported barrier for pursuing dietary goals. No differences in demographic, physiological, lifestyle, or motivational characteristics were identified between goal setters and non-goal setters.
Despite counseling not being the primary focus of the NUTRECOVER trial and participation in goal setting being entirely voluntary, a high proportion of patients were willing to set lifestyle goals. This suggests that, even in the context of a placebo controlled RCT, primarily investigating the effect of a specific nutritional supplement, many patients with COPD are open to engaging in conversations about behavior change when given the opportunity. This openness aligns with findings from a self-management program provided as the main intervention, in which motivational interviewing and goal setting were key components.24 Within the same study, 41% of the goals set focused on PA, a slightly lower percentage than in our study, likely reflecting the broader focus of self-management interventions, which often also address topics such as breathing techniques, stress management, and smoking cessation. In our study, dietary goals were less frequently set than PA goals. This may be partly explained by the nutritional supplement being the core intervention of the NUTRECOVER trial, potentially increasing awareness of healthy eating and reducing perceived need for further change. It also reflects a broader trend seen in COPD care, where the role of nutrition is often underemphasized compared to PA, seen in both high- and low-income countries.17,22 Moreover, the link between nutrition and lung health may be less well known among patients, and the effects of dietary changes may be perceived as less direct or immediate than those of PA, which could further reduce motivation to set dietary goals. The most common reasons given for not setting dietary goals, being satisfied with current habits and perceiving no need for change, mirror this pattern. Continuation of an active lifestyle and functional purposes like gardening or travelling to another location have been identified as perceived reasons for PA among people with mild to very severe COPD.32 This is reflected in the types of goals set by patients in our study, particularly those aimed at maintaining their current activity level and functional independence.
Our findings regarding barriers support previous research indicating that the most frequently reported reason to be sedentary was the weather, followed by health problems.32 In addition, lack of motivation has been highlighted in the literature as an important barrier for adherence to dietary changes.33 Lack of time was reported by only one patient as a reason for not wanting to set goals and by four patients as barrier to working on lifestyle goals (being busy with other responsibilities and work-life activity balance). This also aligns with findings from previous literature, and may be explained by the fact that populations with COPD tend to be older, with many individuals retired or incapacitated for work due to illness.32 Fear of movement and feelings of shame were additional barriers to PA identified in that study, though these were not frequently mentioned and did not emerge in our sample. It is possible that such factors also played a role in our patients’ willingness to set goals but were not explicitly reported during the counseling sessions.
We did not identify any major differences between goal setters and non-goal setters in demographic, physiological, lifestyle or motivational characteristics. This may be due to the wide variability in the types of goals set and the differences in how counseling was delivered, both across patients and between different counsellors. Additionally, the relatively small sample size, particularly in the group of patients who did not set goals, may also have limited the ability to detect statistically significant group differences. Contrary to expectations, motivation towards exercise did not differ between groups, not even between patients who set a PA goal and those who did not.
For both PA and diet, the most frequently cited reasons for not setting a goal were satisfaction with current behaviors and a perceived lack of need for change. However, this perception does not fully align with the objective baseline data from our study sample. For example, patients typically recorded step counts characteristic of a sedentary lifestyle (<5000 steps/day), with a median of 4026 steps.34 This reflects a potential mismatch between perceived and actual lifestyle behaviors. Similarly, a study examining lifestyle factors as risks for dementia found that many participants were unaware of their non-adherence to recommended guidelines, underscoring the widespread gap between perceived and actual lifestyle adherence.35 This highlights the importance of incorporating awareness-raising components into interventions, aiming not only at facilitating behavior change but also at addressing possible misperceptions regarding health behaviors in patients with COPD. Although health complaints were regularly reported as reasons for not setting or for adjusting PA goals, perceived health benefits were not mentioned as facilitators for engaging in PA in our study. This contrasts with previous literature, which has identified health benefits as an important facilitator.15 However, this absence does not necessarily indicate a lack of awareness among participants, as the benefits of PA for managing COPD symptoms and overall health are now widely recognized and consistently emphasized by pulmonologists. Health benefits were mentioned as a facilitator for pursuing dietary goals, although these referred to general health rather than COPD-related health, for example, improved bowel movements after increasing fruit and water intake.
Although counseling was not the primary aim of this study, including it in an extensive RCT provided highly relevant data. Nevertheless, several limitations of this study must be acknowledged. First, selection bias should be considered when interpreting the findings. Individuals who enrolled in a nutritional supplementation trial may have already been more motivated to engage in lifestyle changes than the general COPD population. This potential bias is reflected in the relatively high baseline levels of intrinsic and identified motivation and may limit the generalizability of the results. In addition, the counseling sessions were conducted by different counsellors and were not strictly standardized in content or delivery, which may have introduced variability in how goal setting and follow-up were carried out. As a result, techniques central to MI, such as consistently exploring barriers and facilitators when difficulties in goal pursuit arose, were not always applied systematically. This may have led to underreporting of relevant challenges or supports. However, evidence does indicate that therapist flexibility within MI, rather than strict adherence, is associated with improved outcomes and client engagement.36
Notable strengths that underpin this research are its detailed examination of the willingness of patients with COPD to engage in lifestyle goal setting. This is done alongside a qualitative exploration of goal content, reasons for adjustment or unwillingness, and experienced barriers and facilitators, offering a nuanced understanding of patients’ goal-setting behaviors. The longitudinal design allowed for monitoring of changes in goals over time, as well as exploration of barriers and facilitators encountered during goal pursuit. Overall, the study provides real-world insights into the implementation of lifestyle counseling embedded within a long-term trial, contributing valuable knowledge to the practical application of such interventions in future COPD care.
Once the NUTRECOVER trial is completed, it may be possible to investigate whether willingness to set goals, or the types of goals set, are associated with changes in PA or dietary behavior over time. In the meantime, the current results already highlight key considerations for tailoring counseling strategies in patients with COPD namely, the importance of raising awareness about actual versus perceived lifestyle behaviors, explicitly addressing potential health benefits of lifestyle change, and integrating practical strategies to overcome common barriers such as health complaints, lack of motivation, and environmental factors.
Conclusion
This study provides new insights into the willingness of patients with COPD to engage in lifestyle goal setting and the factors influencing this process. A majority of patients were open to discussing and setting lifestyle goals, particularly related to PA. However, perceived satisfaction with current behaviors and health-related barriers often limited goal setting. Our findings highlight the need for tailored counseling strategies that not only promote behavior change but also address common misperceptions, emphasize potential (COPD related) health benefits, and provide practical support for overcoming common barriers.
Abbreviations
ASMI, appendicular skeletal muscle mass index; BMI, body mass index; BREQ-2, Regulation in Exercise Questionnaire-2; COPD, chronic obstructive pulmonary disease; EQ-5D, EuroQol five dimensions; EWGSOP, European Working Group on Sarcopenia in Older People; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; IQR, interquartile range; MUMC+, Maastricht University Medical Centre+; MI, motivational interviewing; PA, physical activity; QoL, quality of life; RCT, randomized controlled trial; SES, low socioeconomic status; SES-WOA, socio-economic status based on Welvaart (wealth), Opleidingsniveau (educational level), and Arbeidsverleden (employment history); 6MWT, Six-Minute Walk Test; SPPB, Short Physical Performance Battery; SO, sarcopenic obesity.
Data Sharing Statement
Data extraction form available on OSF (in Dutch).
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
The NUTRECOVER trial was approved by the Medical Ethics Committee from MUMC+, Maastricht, The Netherlands (NL66543068.18/METC18-011), and was conducted in accordance with the principles of the Declaration of Helsinki (Fortaleza, Brazil, 2013) and with the Dutch Regulations on Medical Research Involving Human Subjects Act (WMO). All subjects gave written informed consent before participation. The study has been registered at clinicaltrials.gov (NCT03807310).
Acknowledgments
The authors are grateful to all participants for their time and commitment to this study.
The authors acknowledge the use of ChatGPT (GPT-5, OpenAI) for language improvement during the preparation of this manuscript. The model was used to help refine phrasing and improve clarity of expression, but all conceptual content, analysis, and final revisions were made by the authors. The abstract of this paper was presented at the European Respiratory Society Conference as a poster presentation with interim findings. The poster’s abstract was published in European Respiratory Journal 2025 Vol 66 Issue suppl 69: https://doi.org/10.1183/13993003.congress-2025.PA526.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The NUTRECOVER trial was supported by a LSH-TKI Lung Foundation grant 10.2.16.119, 2017 “Food for thought and active lifestyle in COPD”, which was co-funded by Danone Research & Innovation, Maastricht University, Utrecht University and the Dutch Lung Foundation.
Disclosure
Sami Simons reports grants from Roche, grants from Dutch Research Council (NWO), grants from Dutch Lung Foundation (Longfonds), consulting fees and honoraria for presentations, and lecture. Participation on Advisory Board (all payments to institution) from AstraZeneca, consulting fees and honoraria for presentations, and lecture. Participation on Advisory Board (all payments to institution) from Chiesi, non-financial support from P4O2 foundation, non-financial support from eVoiceNet, outside the submitted work. Ardy van Helvoort is employed by Danone Research & Innovation, Utrecht, Netherlands. The authors report no conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. GLOBAL STRATEGY FOR PREVENTION, DIAGNOSIS AND MANAGEMENT OF COPD: 2025 Report. 2025. Available from: https://goldcopd.org/2025-gold-report/.
2. Institute for Health Metrics and Evaluation (IHME). Global burden of disease 2021: findings from the GBD 2021 study. 2024.
3. Born CDC, Bhadra R, D’Souza G, et al. Combined lifestyle interventions in the prevention and management of asthma and COPD: a systematic review. Nutrients. 2024;16(10). doi:10.3390/nu16101515
4. Watz H, Pitta F, Rochester CL, et al. An official European Respiratory Society statement on physical activity in COPD. Eur Respir J. 2014;44(6):1521–16. doi:10.1183/09031936.00046814
5. van Iersel LEJ, Beijers R, Gosker HR, Schols A. Nutrition as a modifiable factor in the onset and progression of pulmonary function impairment in COPD: a systematic review. Nutr Rev. 2022;80(6):1434–1444. doi:10.1093/nutrit/nuab077
6. Waschki B, Kirsten AM, Holz O, et al. Disease progression and changes in physical activity in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2015;192(3):295–306. doi:10.1164/rccm.201501-0081OC
7. Pitta F, Troosters T, Probst VS, Spruit MA, Decramer M, Gosselink R. Physical activity and hospitalization for exacerbation of COPD. Chest. 2006;129(3):536–544. doi:10.1378/chest.129.3.536
8. Garcia-Aymerich J, Lange P, Benet M, Schnohr P, Antó JM. Regular physical activity reduces hospital admission and mortality in chronic obstructive pulmonary disease: a population based cohort study. Thorax. 2006;61(9):772–778. doi:10.1136/thx.2006.060145
9. van de Bool C, Mattijssen-Verdonschot C, van Melick PP, et al. Quality of dietary intake in relation to body composition in patients with chronic obstructive pulmonary disease eligible for pulmonary rehabilitation. Eur J Clin Nutr. 2014;68(2):159–165. doi:10.1038/ejcn.2013.257
10. Carlotto CI, Bernardes S, Zanella P, Silva FM. Dietary patterns and risk of Chronic Obstructive Pulmonary Disease (COPD) and clinical outcomes in diagnosed patients: a scoping review. Respir Med. 2024;233:107773. doi:10.1016/j.rmed.2024.107773
11. Grönberg AM, Slinde F, Engström CP, Hulthén L, Larsson S. Dietary problems in patients with severe chronic obstructive pulmonary disease. J Hum Nutr Diet. 2005;18(6):445–452. doi:10.1111/j.1365-277X.2005.00649.x
12. Burge AT, Cox NS, Abramson MJ, Holland AE. Interventions for promoting physical activity in people with chronic obstructive pulmonary disease (COPD). Cochrane Database Syst Rev. 2020;4(4):Cd012626. doi:10.1002/14651858.CD012626.pub2
13. Gimeno-Santos E, Frei A, Steurer-Stey C, et al. Determinants and outcomes of physical activity in patients with COPD: a systematic review. Thorax. 2014;69(8):731–739. doi:10.1136/thoraxjnl-2013-204763
14. Wang Z, Zhou X, Deng M, et al. Clinical impacts of sarcopenic obesity on chronic obstructive pulmonary disease: a cross-sectional study. BMC Pulm Med. 2023;23(1):394. doi:10.1186/s12890-023-02702-2
15. Kosteli MC, Heneghan NR, Roskell C, et al. Barriers and enablers of physical activity engagement for patients with COPD in primary care. Int J Chron Obstruct Pulmon Dis. 2017;12:1019–1031. doi:10.2147/copd.S119806
16. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13–64. doi:10.1164/rccm.201309-1634ST
17. Williams MT, Effing TW, Paquet C, et al. Counseling for health behavior change in people with COPD: systematic review. Int J Chron Obstruct Pulmon Dis. 2017;12:2165–2178. doi:10.2147/copd.S111135
18. Miller WR, Rollnick S. Motivational Interviewing: Preparing People to Change Addictive Behavior. The Guilford Press; 1991.
19. Resnicow K, McMaster F. Motivational Interviewing: moving from why to how with autonomy support. Int J Behav Nutr Phys Act. 2012;9:19. doi:10.1186/1479-5868-9-19
20. Cole SA, Sannidhi D, Jadotte YT, Rozanski A. Using motivational interviewing and brief action planning for adopting and maintaining positive health behaviors. Prog Cardiovasc Dis. 2023;77:86–94. doi:10.1016/j.pcad.2023.02.003
21. Hanrahan C, Broderick J, O’Connor TM, McVeigh JG. Behaviour change interventions for physical activity in adults with chronic obstructive pulmonary disease; A systematic review and meta-analysis. Respir Med Res. 2024;85:101068. doi:10.1016/j.resmer.2023.101068
22. Bell K, Lawson J, Penz E, Cammer A. Systematic review of tailored dietary advice and dietitian involvement in the treatment of chronic obstructive pulmonary disease (COPD). Respir Med. 2024;225:107584. doi:10.1016/j.rmed.2024.107584
23. Long H, Howells K, Peters S, Blakemore A. Does health coaching improve health-related quality of life and reduce hospital admissions in people with chronic obstructive pulmonary disease? A systematic review and meta-analysis. Br J Health Psychol. 2019;24(3):515–546. doi:10.1111/bjhp.12366
24. Benzo R, Vickers K, Ernst D, Tucker S, McEvoy C, Lorig K. Development and feasibility of a self-management intervention for chronic obstructive pulmonary disease delivered with motivational interviewing strategies. J Cardiopulm Rehabil Prev. 2013;33(2):113–123. doi:10.1097/HCR.0b013e318284ec67
25. Beijers RJ, van Iersel LEJ, Schuurman LT, et al. Effect of targeted nutrient supplementation on physical activity and health-related quality of life in COPD: study protocol for the randomised controlled NUTRECOVER trial. BMJ Open. 2022;12(3):e059252. doi:10.1136/bmjopen-2021-059252
26. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychol. 2000;55(1):68–78. doi:10.1037//0003-066x.55.1.68
27. Lindner H, Menzies D, Kelly J, Taylor S, Shearer M. Coaching for behaviour change in chronic disease: a review of the literature and the implications for coaching as a self-management intervention. Austr J Primary Health. 2003;9(2&3):9.
28. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48(1):16–31. doi:10.1093/ageing/afy169
29. Donini LM, Busetto L, Bauer JM, et al. Critical appraisal of definitions and diagnostic criteria for sarcopenic obesity based on a systematic review. Clin Nutr. 2020;39(8):2368–2388. doi:10.1016/j.clnu.2019.11.024
30. World Health Organization. Obesity and overweight. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
31. Centraal Bureau voor de Statistiek. Sociaal-economische status per postcode, 2019. CBS.nl. 2025. https://www.cbs.nl/nl-nl/maatwerk/2022/26/sociaal-economische-status-per-postcode-2019.
32. Hartman JE, ten Hacken NH, Boezen HM, de Greef MH. Self-efficacy for physical activity and insight into its benefits are modifiable factors associated with physical activity in people with COPD: a mixed-methods study. J Physiother. 2013;59(2):117–124. doi:10.1016/s1836-9553(13)70164-4
33. Deslippe AL, Soanes A, Bouchaud CC, et al. Barriers and facilitators to diet, physical activity and lifestyle behavior intervention adherence: a qualitative systematic review of the literature. Int J Behav Nutr Phys Act. 2023;20(1):14. doi:10.1186/s12966-023-01424-2
34. Cheng SWM, Alison JA, Stamatakis E, Dennis SM, McKeough ZJ. Validity and accuracy of step count as an indicator of a sedentary lifestyle in people with chronic obstructive pulmonary disease. Arch Phys Med Rehabil. 2023;104(8):1243–1252. doi:10.1016/j.apmr.2023.01.020
35. Bruinsma J, Loukas VS, Kassiotis T, et al. Socio-cognitive determinants of lifestyle behavior in the context of dementia risk reduction: a population-based study in the Netherlands. J Alzheimers Dis. 2024;99(3):941–952. doi:10.3233/jad-231369
36. Hettema JE, Hendricks PS. Motivational interviewing for smoking cessation: a meta-analytic review. J Consult Clin Psychol. 2010;78(6):868–884. doi:10.1037/a0021498
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.