Back to Journals » Psychology Research and Behavior Management » Volume 18
Assessing Impulsivity in Adolescents with Borderline Personality Features via an Emotional Contextual Go/NoGo Paradigm
Authors Wang Q, Chen Y, Zhong J
Received 30 December 2024
Accepted for publication 9 July 2025
Published 7 August 2025 Volume 2025:18 Pages 1673—1683
DOI https://doi.org/10.2147/PRBM.S514799
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Qian Wang,1,2 Yizhou Chen,2,3 Jie Zhong2
1Department of Psychology, School of Humanities, Tongji University, Shanghai, People’s Republic of China; 2Beijing Key Laboratory of Behavior and Mental Health, Clinical and Health Psychology Department, School of Psychological and Cognitive Sciences, Peking University, Beijing, People’s Republic of China; 3Great Ormond Street Institute of Child Health, University College London, London, UK
Correspondence: Jie Zhong, Beijing Key Laboratory of Behavior and Mental Health, Clinical and Health Psychology Department, School of Psychological and Cognitive Sciences, Peking University, No. 5, Yi-He-Yuan Road, Haidian, Beijing, 100871, People’s Republic of China, Email [email protected]
Purpose: This study examined the influence of emotional contexts and invalidating family environment on impulsivity, especially response inhibition function, in adolescents with borderline personality features.
Methods: 483 Chinese adolescents (52.2% females; Mage = 15.54 years) from a community sample completed the scales of McLean Screening Instrument for Borderline Personality Disorder and Chinese Invalidating Family Scale for Adolescents and the Go/NoGo task under positive, neutral, and negative emotional conditions. Repeated measures ANCOVAs were performed without and with invalidating family environment as a covariate to compare the behavioral outcomes of the Go/Nogo task between participants with different levels of borderline personality features under different emotions.
Results: Adolescents with high borderline personality features made significantly more commission errors in the Go/NoGo task only in positive emotional conditions, and the group differences in commission error rates became non-significant after controlling invalidating family environment.
Conclusion: The results suggest the impaired response inhibition function particularly under positive emotions of adolescents high in borderline personality features and its close association to invalidating family environment, pointing to more targeted diagnostic and treatment strategies for adolescent borderline personality disorder.
Keywords: impulsivity, response inhibition, borderline personality disorder, invalidating family environment, emotions
Introduction
Borderline Personality Disorder in Adolescence
Borderline personality disorder (BPD) is a psychological disorder characterized by a pervasive pattern of emotion dysregulation, unstable interpersonal relationships, impulsivity, and identity disturbance.1 Although BPD patients are normally first diagnosed in early adulthood, the diagnosis of BPD in mid-adolescence has been proven to be comparable to that in adulthood in reliability and validity.2–4 A growing number of studies suggest high similarity and continuity between adult BPD and adolescent BPD, especially in terms of risk factors, pathological mechanisms, phenomenological features, and symptom stability.2,3,5,6
Adolescence has been considered a particularly delicate and critical period for BPD development, during which borderline personality features (BPF) emerge within a complex clinical picture.7 The developmental trajectory of BPF is heterogeneous during adolescence, with patterns of decrease,8 increase, or stability over time.9 However, one consistently observed trend of BPF is the high rank-order stability. Adolescents exhibiting the most severe BPF tend to remain the most symptomatic or even escalate in symptom severity.8,9 They also tend to consistently demonstrate lower levels of role functioning, social functioning, and life satisfaction that persist into mid-adulthood.10 BPF are significantly associated with increased risks of a later BPD diagnosis and general impairment in adulthood even when they decline with age.10,11 Therefore, studying BPF in adolescence can be an important means to identify the etiologic precursors of BPD and aid in the development of more effective prevention and treatment programs.12
Impulsivity and BPD
Impulsivity is a multidimensional concept manifested by rapid, unplanned behaviors without clear forethought and regard for the negative consequences.13 It is considered to be a central feature of BPD that was found to best predict BPD psychopathology across time, and its treatment can impact the course of BPD.14,15 Many studies have shown that BPD patients had significantly higher self-rated impulsivity than healthy controls, as well as other patients, with the exception of ADHD.16 Regarding impulsivity in adolescent BPD particularly, adolescents with heightened BPF have also been found to exhibit higher levels of impulsivity than control adolescents,17 and impulsivity was significantly positively correlated with BPF in nonclinical adolescents.18 Additionally, adolescents diagnosed with BPD were found to engage in more impulsive behaviors like recurrent self-injury and suicide compared to not only adolescents without BPD19 but also adults with BPD.20
Impulsivity is strongly relevant to the ability to inhibit an urgent wish to act, and response inhibition is seen as one important behavioral aspect of impulsivity,21 which can be measured through laboratory paradigms including the Go/NoGo task and stop signal task. However, the findings of previous studies on the performance of BPD individuals in these tasks have been mixed. Many studies employing behavioral tasks to measure response inhibition failed to find any performance deficits in BPD patients.16 Hence, some studies proposed that impulsive behavior in BPD might depend on emotional processing rather than solely impulsive traits.16 This view was supported by empirical studies which found that BPD patients displayed response inhibition deficits only in negative emotional conditions.22,23 In this respect, other BPD symptoms of impulse dysregulation, such as self-injury, suicide, and substance abuse, can be conceptualized as attempts to deal with negative emotions.24 However, there are also some other studies showing conflicting results, in which BPD patients still manifested reduced response inhibition function even under neutral emotions.25–27 Thus, the relationship between impulsivity and emotions in BPD individuals still remains unclear.
Invalidating Family Environment and Impulsivity in BPD
An invalidating family environment is a situation where caregivers are intolerant of children’s expression of private emotional experiences, responding with neglect, denial, or punishment.28 Family environments involving physical abuse, emotional abuse, or sexual abuse are extremely invalidating.29 According to Linehan’s biosocial model,28 family invalidation is a key contributing factor in the development of BPD. Prolonged exposure to such environments prevents children from acquiring effective emotional recognition and regulation strategies.29,30 As a result, children tend to inappropriately express their emotions with impulsive behaviors, which may aggravate their own emotional dysregulation and further reinforce the invalidating responses from caregivers, thereby creating a vicious cycle.29,31 This theoretical model is supported by a growing body of empirical evidence. For instance, a recent meta-analysis of 21 studies showed that childhood family invalidation was positively associated with BPF with small to moderate effect sizes.32 Additionally, Franssens et al conducted cross-lagged panel analyses that revealed not only the detrimental effects of parental invalidation on the development of BPF in children but also the child-driven effects that contributed to increasing invalidating parenting practices, highlighting the reciprocal influences between family invalidation and children’s BPD-related outcomes.33
Regarding impulsivity, research has demonstrated that childhood trauma, which is closely linked to invalidating family environments, can heighten impulsivity through emotional dysregulation in BPD34 and is positively correlated particularly with inhibitory deficits in BPD patients.35 There is also substantial evidence supporting the robust association between family invalidation and self-injury behavior, a common manifestation of impulsivity in BPD, among adolescents and young people.36–38 However, no research to date has directly explored the relationship between invalidating family environment and response inhibition function, especially in emotional contexts, of BPD adolescents.
The Current Study
This study investigated the relationship of impulsivity, especially response inhibition, to emotional processing and invalidating family environment in adolescents with BPF. We used an emotional Go/NoGo paradigm to measure and compare the response inhibition function of adolescents with different levels of BPF under positive, negative, and neutral emotional conditions. We further compared the differences before and after partialing out the variance of invalidating family environment to explore its effect on response inhibition. Given the heterogeneous results of previous adult studies, the analysis of response inhibition differences under different emotions was exploratory. But based on Linehan’s biosocial model,28 we hypothesized that invalidating family environment would be significantly positively correlated with response inhibition.
Method
Participants and Procedure
Participants were 536 adolescents recruited at their schools in the southern region of China. To rule out the effect of medication and provide better implications for early BPD screening, we selected all participants from community samples. After excluding participants who did not provide important demographic information and whose behavioral performance measures in the Go/NoGo task deviated from the mean by more than 3 standard deviations, 483 participants were included in the analysis. Participants were, on average, 15.54 years old (SD = 0.92) and 52.2% were female. The inclusion criteria comprised consent to participate, no history of DSM-5 diagnoses, no psychotherapy or medication treatment within the past 6 months, no history of neurological or severe medical illnesses, and no history of substance dependence or abuse. Following the example established in other studies,39,40 we used a cutoff score of 7 in McLean Screening Instrument for Borderline Personality Disorder41 to divide the participants into two groups. Participants with a total score of 7 or greater were assigned to the high-BPF group (n = 73), and the remaining 410 were assigned to the low-BPF group.
The study was approved by the ethical committee of Peking University (project reference number: #2022-02-06). After participants and their parents read the instructions presented and gave their informed consent, participants completed several self-report measures and then were assessed with the Go/NoGo task through an online assessment platform in their school’s computer labs. All participants were awarded a set of souvenirs for completing the study.
Measures
Demography
Basic demographic information was collected using a self-report survey, including gender and age.
McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD)
The MSI-BPD is a self-report screening scale based on the nine diagnostic criteria of BPD in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).1,41 It comprises ten yes-or-no items (criterion nine of DSM-5 is assessed with two questions), each scored on a 2-point scale, producing a range of sum scores from 0–10. Higher total scores indicate more severe BPF. A cutoff of 7 points has been identified with good sensitivity and specificity for BPD diagnosis, and those who scored 7 or higher are individuals with subthreshold features of borderline pathology.41 The MSI-BPD was found to be a valid tool for BPD screening and assessment of BPF in adolescents and is particularly suitable for initial BPD screening in large samples.42,43 To be noted, the MSI-BPD was employed solely as a screening tool to identify potential BPF in the current study, not for clinical diagnosis. Formal BPD diagnosis requires structured interviews, detailed developmental history, and assessment of symptom persistence. Cronbach’s internal consistency reliability coefficient of the Chinese version of MSI-BPD used in this study was good (α = 0.83).
Chinese Invalidating Family Scale for Adolescents (CIFS-A)
The CIFS-A, a revised version of the Chinese Invalidating Family Scale (CIFS) more applicable to adolescents, was confirmed to be a reliable and valid instrument to evaluate the invalidating family environment in Chinese culture.44 The CIFS-A consists of two subscales, a father and a mother, measuring the extent of parenting invalidation of the father with 20 items and the mother with 27 items. Each item is scored on a 4-point scale. Positively worded items are reverse-scored. Higher total scores indicate a higher level of invalidating family environment. In the present study, the internal consistency was found to be good (α = 0.86 for the overall score).
Go/NoGo Task
The Go/NoGo task is an experimental paradigm commonly used to measure impulsivity, especially response inhibition, with high ecological validity.45,46 In the present study, the Go/NoGo task was applied under three emotional conditions: positive, negative, and neutral. The specific procedure for each trial is shown in Figure 1. Each trial started with a 500 ms fixation in the center of the screen, and then an emotional picture was presented for 1800 ms. After another 500 ms of fixation, the Go/NoGo target stimuli (letter M or W) were presented for 200 ms, followed by a blank screen for 800 ms for the participants to respond. Participants were instructed to respond by pressing the space bar when they saw M and to withhold the response when they saw W. After that, 200 ms of feedback was provided regarding whether the response was correct. If the participant responded correctly, the word “Correct” in Chinese would be displayed, and if the response was incorrect or the participant had not responded to M for more than 800 ms, then the word Error in Chinese would appear. At the end of the trial, there was a blank screen for another 500 ms as the transition to the next trial.
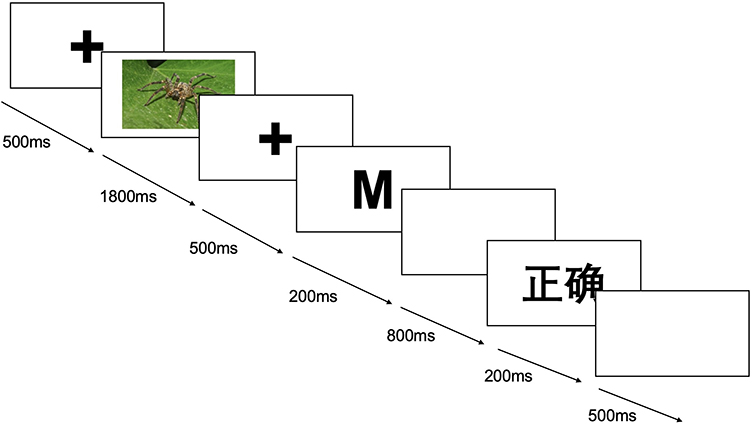 |
Figure 1 The procedure of each trial in the emotional Go/NoGo task. The Chinese character means “Correct”. |
Only one type of emotional picture was presented in one round to prevent interference between different types of emotional stimuli. The order of the three types of emotional conditions was randomized. Each round of testing presented 36 stimuli (18 Go, 18 NoGo) in total. The omission error rate (percentage of Go trials erroneously followed by no response), commission error rate (percentage of NoGo trials erroneously followed by a response), and hit response time (average response time of correct Go trials) of each participant in each condition were recorded.
The emotional pictures (36 positive/neutral/negative pictures each) employed in this task were previously validated by the study of Wang.47 Their content included people, places, animals, food, and other objects. Based on the two-dimensional theory of emotional valence-arousal, the pictures were categorized into positive, neutral, and negative according to their valence and 23 students from Peking University rated the valence and arousal of all the pictures using a 9-point Likert scale. The three categories differed significantly from each other in valence (M±SD: positive = 6.62±1.61; neutral = 5.22±1.58; negative = 2.78±1.72). Positive and negative pictures had similar arousal levels that were both significantly higher than that of neutral ones (M±SD: positive = 4.82±2.24; neutral = 3.56±2.09; negative = 4.52±2.34). Each of the 36 emotional pictures in each group appeared only once in a random order in the corresponding task round. Examples of the pictures are presented in Figures S1–S3.
Data Analysis
Data were analyzed using SPSS Version 25.0. Chi-square (χ2) tests were used for categorical variables and t-tests for continuous variables to compare demographic characteristics and invalidating family environment between the groups. Demographic variables with a significant difference between the groups were included as covariates in these analyses.
The sensitivity index d’ of the Go/NoGo task was calculated as a measure of discrimination: d’ = z (reaction rate of Go trials) − z(reaction rate of NoGo trials). Rates of 0 were replaced with 0.5/n, and rates of 1 were replaced with 1−0.5/n, where n was the number of Go or NoGo trials.48 The sensitivity index d’, rates of omission and commission errors, and hit response time of the Go/NoGo task were compared in a series of repeated measures ANCOVAs using a two-factor design (BPF group: high/low; emotional condition: positive/ neutral/ negative). To further explore the effect of invalidating family environment, extra ANCOVAs, including invalidating family environment as a covariate, were performed. All post-hoc tests were performed using the Bonferroni correction. Significance levels were adjusted when necessary using Greenhouse–Geisser epsilon correction. All p values were two-sided, and findings at the p < 0.05 level were considered significant.
Results
Participant Characteristics
Demographic and psychometric characteristics comparing the high-BPF and low-BPF groups are presented in Table 1. There were no significant differences in gender composition between the two groups, but a significant difference in age was found. Thus, age was incorporated as a covariate in all the following analyses. High-BPF participants scored significantly higher in BPF and invalidating family environment than the low-BPF group.
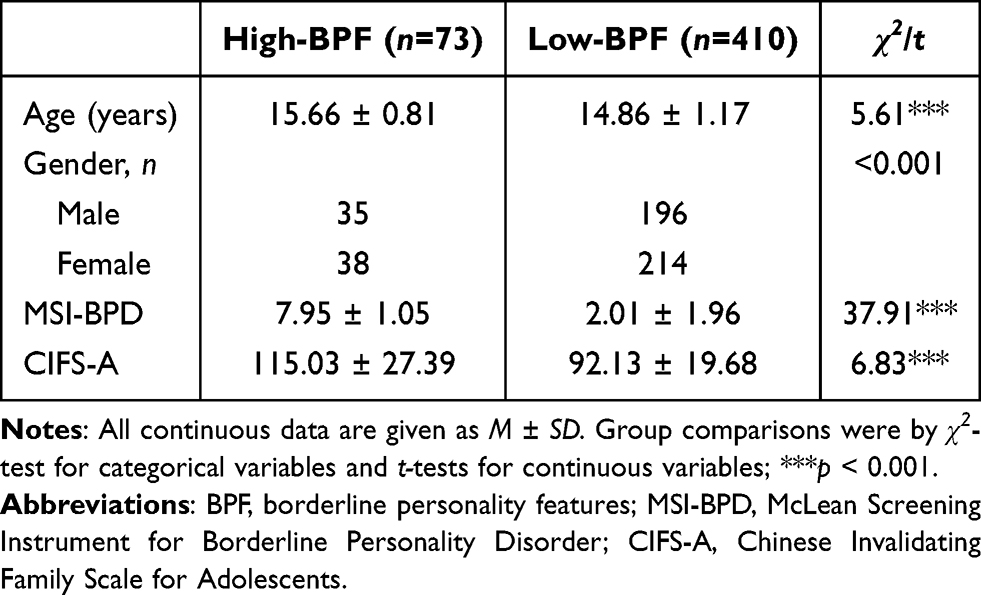 |
Table 1 Demographic and Psychometric Characteristics by BPF Group |
ANCOVA without Invalidating Family Environment
To examine group differences in behavioral data of the Go/NoGo task (Table 2), four repeated measures ANCOVAs were performed.
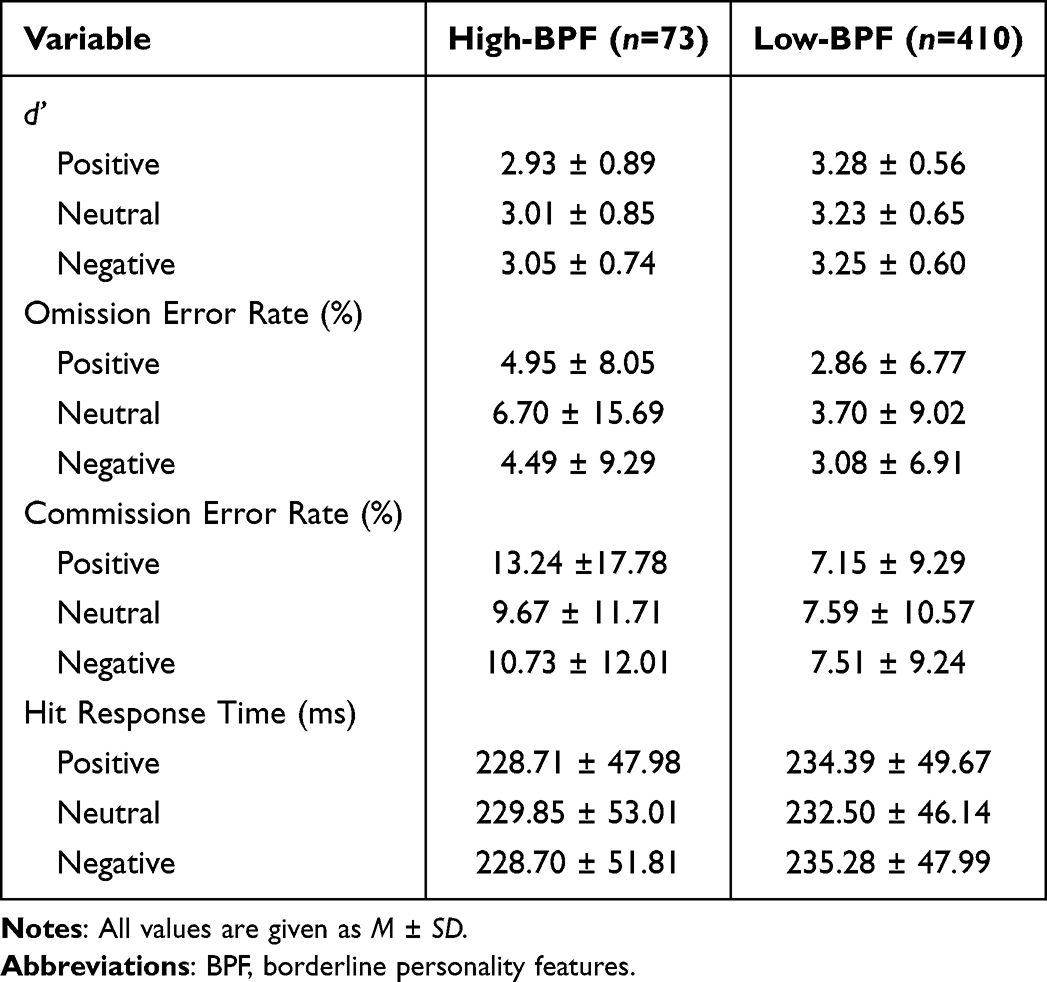 |
Table 2 Behavioral Data of the Go/Nogo Task in Positive, Neutral, and Negative Emotional Conditions by BPF Group |
No significant main effects of emotional conditions were found. The sensitivity index d’, omission error rate, commission error rate, and hit response time all showed a significant main effect of group (F(1, 480) = 8.81, p = 0.003, η2 = 0.018; F(1, 480) = 6.92, p = 0.009, η2 = 0.014; F(1, 480) = 5.568, p = 0.019, η2 = 0.011; F(1, 480) = 4.01, p = 0.046, η2 = 0.008, respectively), indicating that high-BPF group had overall lower d’, higher omission and commission error rates, and shorter hit response time. The interaction between group and type of emotions was significant only for commission error rate (F(2, 960) = 3.25, p = 0.039, η2 = 0.007). Bonferroni post hoc tests showed that the commission error rate of high-BPF group was significantly higher with positive emotional stimuli (p = 0.002) than that of low-BPF group. The differences with negative (p = 0.079) and neutral (p = 0.441) emotional stimuli were not significant.
ANCOVA with Invalidating Family Environment
After controlling invalidating family environment, the main effects of group on d’ (F(1, 479) = 5.76, p = 0.017, η2 = 0.012) and omission error rate (F(1, 479) = 6.38, p = 0.012, η2 = 0.013) were still significant. However, for commission error rate, there was no longer a significant group effect (F(1, 479) = 2.40, p = 0.122, η2 = 0.005) or group × emotional condition interaction (F(2, 958) = 2.19, p = 0.112, η2 = 0.005). The group effect on hit response time was also not significant (F(1, 479) = 3.04, p = 0.082, η2 = 0.006).
The effect of invalidating family environment was significant only on commission error rate (F(1, 479) = 4.48, p = 0.035, η2 = 0.009). It was significantly positively correlated with commission error rate under positive (r = 0.167, p < 0.001) and negative emotional conditions (r = 0.143, p = 0.002) but showed no significant correlation with commission error rate with neutral emotions (r = 0.074, p = 0.104). No other effects were significant.
Discussion
Our study investigated the difference in response inhibition function between adolescents with different levels of BPF under positive, neutral, and negative emotional conditions using the Go/NoGo paradigm. We also explored the influence of invalidating family environment. Results showed that high-BPF participants displayed poorer overall performance with higher rates of omission error and quicker reaction to stimuli than low-BPF ones in all conditions. However, their higher commission error rates only occurred under positive emotions, and this group difference became non-significant after controlling the invalidating family environment. Taken together with its significant effect on commission error rates, invalidating family environment appears to be highly relevant to the formation of high-BPF adolescents’ response inhibition deficit. Given the diagnostic complexities associated with adolescent BPD, our findings offer only a preliminary framework of relevant risk factors. Further research involving clinically diagnosed samples is essential to validate and extend these observations.
Impulsivity in BPF in Emotional Contexts
The sensitivity index d’ measures participants’ ability to distinguish between stimuli with higher values representing higher performance levels.49 In our study, high-BPF adolescents’ overall lower d’ values suggest that they had greater difficulty with the task demands. Further, high-BPF participants made more omission errors regardless of the emotional conditions. The omission error rate in the Go/NoGo paradigm is regarded as a measurement of sustained attention.50,51 Based on the structure of impulsivity proposed by the Barratt Impulsiveness Scale,52 the attention deficit belongs to the factor of attentional impulsivity, indicating poor cognitive control and inattention. Therefore, our findings demonstrate that high-BPF adolescents display a higher level of attentional impulsivity, which is relatively stable across different emotional contexts.
Regarding commission error rates, the most sensitive indicator of response inhibition function,25,50,51 we found that the values of high-BPF adolescents were significantly higher only under positive emotional conditions. This expressly highlights the prominent role of positive emotions in eliciting impulsive behaviors in adolescents high in BPF.
The study by Fossati et al17 investigating BPF among Italian nonclinical adolescents found that while the difference in positive urgency (the tendency to act rashly when experiencing intense positive affect) remained significant between high-BPF adolescents and controls after controlling negative urgency (the tendency to act impulsively when experiencing negative affect), the difference in negative urgency became insignificant when controlling positive urgency. They thus proposed that positive urgency might be relevant particularly to adolescent BPF. Our study provided some behavioral evidence for this view, suggesting that high-BPF adolescents may be more easily influenced by positive emotions to perform impulsive behaviors, and this might be an important component of adolescent BPF.
The urge to act more impulsively when confronted with positive rather than negative emotional stimuli was also found among healthy individuals by the study of Albert et al.53 They found that participants made more commission errors to positive emotion-arousing stimuli than to negative and neutral ones in a Go/NoGo task. They explained that the natural association between pleasant stimuli and approach-related behaviors made inhibiting responses to them more difficult. In light of their view, we could suppose likewise that high-BPF adolescents might be especially attracted to positive stimuli, have a stronger tendency to approach pleasant and reward-related events, and find it harder to resist such a tendency. This tendency may even have a possible link with their chronic feelings of emptiness and desperate need of others, one of the symptoms most relevant to the diagnosis of adolescent BPD.54 Future research might specifically explore their relationships. Albert et al also demonstrated that the anterior cingulate cortex (ACC), the structure involved in emotional response inhibition, consumed greater resources to withhold responses to positive stimuli than non-positive ones.53 Research has revealed a reduction in ACC volume in adolescents with BPD,55 which is possibly the neural basis of the participants’ inhibition deficit under positive emotional contexts in this study.
Our findings are inconsistent with some previous studies using the Go/NoGo paradigm in which BPD patients were observed to make more commission errors only in negative emotional conditions22 or display no deficits at all.56,57 One possible reason is that all studies above selected participants from adult clinical populations, but the participants in our study are a community adolescent sample. It is possible that it may indicate an important divergence of BPF between adults and adolescents. More research is necessary to specifically compare the inhibition function of high-BPF adolescents and adults under different emotional contexts to validate this point.
Regarding hit response time, high-BPF adolescents in this study showed a quick reaction style regardless of emotional conditions. While faster responses fit naive ideas of impulsive behaviors, most previous studies found that clinical groups with higher impulsivity displayed longer reaction time.27,58,59 Some researchers proposed high impulsivity may lead to shorter reaction time in simple tasks but prolonged deliberation time in more complex ones.26 Therefore, the shorter hit response time of high-BPF participants in this study may be related to the relatively simple demands of our tasks.
The Effect of Invalidating Family Environment
After including invalidating family environment as a covariate, the difference between groups in omission error rate remained significant. In contrast, the difference in commission error rate became non-significant. Moreover, invalidating family environment had no significant effects on omission error rate, but a significant positive correlation was found between it and commission error rate under positive emotions. These findings suggested that attentional impulsivity might be relatively independent of family environments, and that response inhibition deficit observed under positive emotional contexts could be partly explained by their invalidating family environment.
Based on the biosocial theory, it is the reciprocal transactions between biological vulnerability and invalidating environments that lead to aggravating emotional dysregulation and behavioral dyscontrol.28,29 Faced with caregivers’ invalidating responses to their emotions, children, especially those with biological vulnerabilities for BPD, fail to study the proper way of regulating emotional arousal. They have no alternative but to exploit extreme behaviors to elicit helpful responses from their caregivers, and in the long run, their emotional sensitivity and impulsive behavior tendencies are intermittently reinforced.29,31 On the contrary, an environment with strong family support can protect biologically vulnerable children so as not to induce manifestations of their vulnerability.29
Additionally, the neurodevelopmental alterations may mediate the relationship between invalidating environment and deficits in response inhibition. There is evidence that early life stress, including invalidating family environment, could affect the development of frontostriatal circuits and regulatory networks encompassing the amygdala, therefore predisposing to the inability of inhibitory control and emotional regulation.60 Childhood trauma could also portend impairment of the function and activation of ACC,61,62 which has been proven to play a vital role in the inhibition of emotional responses, especially positive ones.53 This is a possible explanation why high-BPF adolescents’ inhibition function was observed to be most prominently damaged in positive emotional conditions when ACC is required to integrate more resources.
Limitations
The results of our study must be considered in light of several limitations. First, measures of BPF were only administered using MSI-BPD, a self-report screening tool without clinical confirmation, and no clinical assessment interviews were conducted. As a screening measure, MSI-BPD is tooled to be highly sensitive and not particularly specific and accordingly may lead to a high rate of false positives. Also, the scores within the low-BPF group as measured by the MSI-BPD ranged from 0 to 6, indicating considerable heterogeneity within this group. Future research should assess different dimensions of BPF using multiple measures of psychopathology, and further incorporate clinically diagnosed BPD samples using structured clinical interviews as the gold standard, to establish diagnostic accuracy and generalizability. Second, BPF are heterogeneous, but our study did not take other symptomatology characteristics of relevant disorders into account. Future research needs to investigate the extent to which comorbidity could moderate the association between BPF and impulsivity. Third, regarding the Go/NoGo paradigm, the low overall error rates indicate that its task might be too simple. Future studies should therefore set a higher rate of Go trials to NoGo trials. Finally, owing to the cross-sectional design, our study could not provide concrete causal conclusions.
Conclusions
The current study provides preliminary evidence that response inhibition deficits under positive emotions may be uniquely relevant to adolescent BPF and influenced by invalidating family environment. Despite the limitations, our study offers novel insights into the phenomenological features and pathological mechanisms underlying adolescent BPF. Our findings have important clinical implications for more targeted diagnostic and treatment strategies for adolescent BPD. We recommend that future studies further investigate whether inhibitory deficits under positive emotions could serve as a valid early indicator of BPD for adolescents through longitudinal tracking. Also, clinicians need to carefully assess patients’ impulsive behaviors occurring during times of positive affect, which might be less likely to be reported as problematic, especially during adolescence, and highlight the handling of positive emotions in the treatment of adolescents with salient BPF.
Data Sharing Statement
Data and materials are available upon request from the corresponding author.
Ethics Approval and Informed Consent
This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki. Ethical approval was granted by the Ethical Committee of Peking University (project reference number: #2022-02-06). Written informed consent was obtained from all participants and their parents.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the National Science Foundation of China (project number: 30900401). The funding was awarded to Dr. Jie Zhong.
Disclosure
The authors have no conflicts of interest relevant to this article.
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5.
2. Chanen A, Sharp C, Hoffman P. Global alliance for prevention and early intervention for borderline personality disorder. Prevention and early intervention for borderline personality disorder: a novel public health priority. World Psychiatry. 2017;16(2):215–216. doi:10.1002/wps.20429
3. Kaess M, Brunner R, Chanen A. Borderline personality disorder in adolescence. Pediatrics. 2014;134(4):782–793. doi:10.1542/peds.2013-3677
4. Miller AL, Muehlenkamp JJ, Jacobson CM. Fact or fiction: diagnosing borderline personality disorder in adolescents. Clin Psychol Rev. 2008;28(6):969–981. doi:10.1016/j.cpr.2008.02.004
5. Pinto A, Grapentine WL, Francis G, Picariello CM. Borderline personality disorder in adolescents: affective and cognitive features. J Am Acad Child Adolesc Psychiatry. 1996;35(10):1338–1343. doi:10.1097/00004583-199610000-00021
6. Sharp C, Pane H, Ha C, et al. Theory of mind and emotion regulation difficulties in adolescents with borderline traits. J Am Acad Child Adolesc Psychiatry. 2011;50(6):563–573.e1. doi:10.1016/j.jaac.2011.01.017
7. Guilé JM, Boissel L, Alaux-Cantin S, de La Rivière SG. Borderline personality disorder in adolescents: prevalence, diagnosis, and treatment strategies. Adolesc Health Med Ther. 2018;9:199–210. doi:10.2147/AHMT.S156565
8. Bornovalova MA, Hicks BM, Iacono WG, McGue M. Longitudinal twin study of borderline personality disorder traits and substance use in adolescence: developmental change, reciprocal effects, and genetic and environmental influences. Personal Disord. 2013;4(1):23–32. doi:10.1037/a0027178
9. Haltigan JD, Vaillancourt T. Identifying trajectories of borderline personality features in adolescence: antecedent and interactive risk factors. Can J Psychiatry Rev Can Psychiatr. 2016;61(3):166–175. doi:10.1177/0706743715625953
10. Winograd G, Cohen P, Chen H. Adolescent borderline symptoms in the community: prognosis for functioning over 20 years. J Child Psychol Psychiatry. 2008;49(9):933–941. doi:10.1111/j.1469-7610.2008.01930.x
11. Belsky DW, Caspi A, Arseneault L, et al. Etiological features of borderline personality related characteristics in a birth cohort of 12-year-old children. Dev Psychopathol. 2012;24(1):251–265. doi:10.1017/S0954579411000812
12. Chanen AM. Outcomes in women diagnosed with borderline personality disorder in adolescence: early detection and timely intervention are fundamental. J Can Acad Child Adolesc Psychiatry J Acad Can Psychiatr Enfant Adolesc. 2011;20(3):175.
13. Moeller FG, Barratt ES, Dougherty DM, Schmitz JM, Swann AC. Psychiatric aspects of impulsivity. Am J Psychiatry. 2001;158(11):1783–1793. doi:10.1176/appi.ajp.158.11.1783
14. Lieb K, Zanarini MC, Schmahl C, Linehan MM, Bohus M. Borderline personality disorder. Lancet. 2004;364(9432):453–461. doi:10.1016/S0140-6736(04)16770-6
15. Links PS, Heslegrave R, van Reekum R. Impulsivity: core aspect of borderline personality disorder. J Personal Disord. 1999;13(1):1–9. doi:10.1521/pedi.1999.13.1.1
16. Sebastian A, Jacob G, Lieb K, Tüscher O. Impulsivity in borderline personality disorder: a matter of disturbed impulse control or a facet of emotional dysregulation? Curr Psychiatry Rep. 2013;15(2):339. doi:10.1007/s11920-012-0339-y
17. Fossati A, Gratz KL, Maffei C, Borroni S. Impulsivity dimensions, emotion dysregulation, and borderline personality disorder features among Italian nonclinical adolescents. Borderline Personal Disord Emot Dysregulation. 2014;1(1):5. doi:10.1186/2051-6673-1-5
18. Fossati A, Gratz KL, Maffei C, Borroni S. Emotion dysregulation and impulsivity additively predict borderline personality disorder features in Italian nonclinical adolescents. Personal Ment Health. 2013;7(4):320–333. doi:10.1002/pmh.1229
19. Muehlenkamp JJ, Ertelt TW, Miller AL, Claes L. Borderline personality symptoms differentiate non-suicidal and suicidal self-injury in ethnically diverse adolescent outpatients. J Child Psychol Psychiatry. 2011;52(2):148–155. doi:10.1111/j.1469-7610.2010.02305.x
20. Lawrence KA, Allen JS, Chanen AM. A study of maladaptive schemas and borderline personality disorder in young people. Cogn Ther Res. 2011;35(1):30–39. doi:10.1007/s10608-009-9292-4
21. Hochhausen NM, Lorenz AR, Newman JP. Specifying the impulsivity of female inmates with borderline personality disorder. J Abnorm Psychol. 2002;111(3):495–501. doi:10.1037/0021-843X.111.3.495
22. Silbersweig D, Clarkin JF, Goldstein M, et al. Failure of frontolimbic inhibitory function in the context of negative emotion in borderline personality disorder. Am J Psychiatry. 2007;164(12):1832–1841. doi:10.1176/appi.ajp.2007.06010126
23. Yang H, Liu Q, Peng W, et al. Impaired impulse inhibition of emotional stimuli in patients with borderline personality disorder. Sci Rep. 2021;11(1):16628. doi:10.1038/s41598-021-96166-1
24. Brown MZ, Comtois KA, Linehan MM. Reasons for suicide attempts and nonsuicidal self-injury in women with borderline personality disorder. J Abnorm Psychol. 2002;111(1):198–202. doi:10.1037/0021-843X.111.1.198
25. Albert J, López-Martín S, Arza R, et al. Response inhibition in borderline personality disorder: neural and behavioral correlates. Biol Psychol. 2019;143:32–40. doi:10.1016/j.biopsycho.2019.02.003
26. Rentrop M, Backenstrass M, Jaentsch B, et al. Response inhibition in borderline personality disorder: performance in a Go/Nogo task. Psychopathology. 2008;41(1):50–57. doi:10.1159/000110626
27. Sinke C, Wollmer MA, Kneer J, Kahl KG, Kruger THC. Interaction between behavioral inhibition and emotional processing in borderline personality disorder using a pictorial emotional go/no-go paradigm. Psychiatry Res. 2017;256:286–289. doi:10.1016/j.psychres.2017.06.046
28. Linehan MM. Cognitive-Behavioral Treatment of Borderline Personality Disorder. New York: Guilford Press; 1993.
29. Crowell SE, Beauchaine TP, Linehan MM. A biosocial developmental model of borderline personality: elaborating and extending linehan’s theory. Psychol Bull. 2009;135(3):495–510. doi:10.1037/a0015616
30. Fruzzetti AE, Shenk C. Fostering validating responses in families. Soc Work Ment Health. 2008;6(1–2):215–227. doi:10.1300/J200v06n01_17
31. Beauchaine TP, Neuhaus E. Impulsivity and vulnerability to psychopathology. In: Beauchaine TP, Neuhaus E, editors. Child and Adolescent Psychopathology. John Wiley & Sons, Inc; 2008:129–156.
32. Lee SSM, Keng SL, Yeo GC, Hong RY. Parental invalidation and its associations with borderline personality disorder symptoms: a multivariate meta-analysis. Personal Disord. 2022;13(6):572–582. doi:10.1037/per0000523
33. Franssens R, Abrahams L, Brenning K, Van leeuwen K, De Clercq B. Unraveling prospective reciprocal effects between parental invalidation and pre-adolescents’ borderline traits: between- and within-family associations and differences with common psychopathology-parenting transactions. Res Child Adolesc Psychopathol. 2021;49(10):1387–1401. doi:10.1007/s10802-021-00825-w
34. Krause-Utz A, Erol E, Brousianou AV, et al. Self-reported impulsivity in women with borderline personality disorder: the role of childhood maltreatment severity and emotion regulation difficulties. Borderline Personal Disord Emot Dysregulation. 2019;6:6. doi:10.1186/s40479-019-0101-8
35. Ernst M, Mohr HM, Schött M, et al. The effects of social exclusion on response inhibition in borderline personality disorder and major depression. Psychiatry Res. 2018;262:333–339. doi:10.1016/j.psychres.2017.03.034
36. Adrian M, Berk MS, Korslund K, Whitlock K, McCauley E, Linehan M. Parental validation and invalidation predict adolescent self-harm. Prof Psychol Res Pract. 2018;49(4):274–281. doi:10.1037/pro0000200
37. Holden RR, Lambert CE, La Rochelle M, Billet MI, Fekken GC. Invalidating childhood environments and nonsuicidal self-injury in university students: depression and mental pain as potential mediators. J Clin Psychol. 2021;77(3):722–731. doi:10.1002/jclp.23052
38. Santo MA, Dell’Aglio DD. Self-injury in adolescence from the bioecological perspective of human development. Psicol Teor E Prática. 2022;24(1):1–24. doi:10.5935/1980-6906/ePTPHD13325.en
39. Vivarini P, Jenkins ZM, Castle DJ, Gwee K. Borderline personality disorder symptoms in individuals with eating disorder: association with severity, psychological distress, and psychosocial function. Personal Ment Health. 2023;17(2):109–116. doi:10.1002/pmh.1565
40. Yoshimatsu K, Rosen BH, Kung S, Palmer BA. Improvements in depression severity in hospitalized patients with and without borderline personality features. J Psychiatr Pract. 2015;21(3):208–213. doi:10.1097/PRA.0000000000000068
41. Zanarini MC, Vujanovic AA, Parachini EA, Boulanger JL, Frankenburg FR, Hennen J. A screening measure for BPD: the McLean Screening Instrument for Borderline Personality Disorder (MSI-BPD). J Personal Disord. 2003;17(6):568–573. doi:10.1521/pedi.17.6.568.25355
42. Mirkovic B, Speranza M, Cailhol L, et al. Validation of the French version of the McLean screening instrument for borderline personality disorder (MSI-BPD) in an adolescent sample. BMC Psychiatry. 2020;20(1):222. doi:10.1186/s12888-020-02643-8
43. Noblin JL, Venta A, Sharp C. The validity of the MSI-BPD among inpatient adolescents. Assessment. 2014;21(2):210–217. doi:10.1177/1073191112473177
44. Io L, Wang Q, Wong OL, Li Z, Zhong J. Development and psychometric properties of the Chinese Invalidating Family Scale. Fam Process. 2023;62(3):1161–1175. doi:10.1111/famp.12818
45. Bari A, Robbins TW. Inhibition and impulsivity: behavioral and neural basis of response control. Prog Neurobiol. 2013;108:44–79. doi:10.1016/j.pneurobio.2013.06.005
46. Dougherty DM, Bjork JM, Andrew Harper R, et al. Behavioral impulsivity paradigms: a comparison in hospitalized adolescents with disruptive behavior disorders. J Child Psychol Psychiatry. 2003;44(8):1145–1157. doi:10.1111/1469-7610.00197
47. Wang Z. Impulsivity among Passionate criminals: The role of Emotional interference [dissertation]. Beijing: Peking University; 2020.
48. Stanislaw H, Todorov N. Calculation of signal detection theory measures. Behav Res Methods Instrum Comput J Psychon Soc Inc. 1999;31(1):137–149. doi:10.3758/bf03207704
49. Tschan T, Peter-Ruf C, Schmid M, In-Albon T. Temperament and character traits in female adolescents with nonsuicidal self-injury disorder with and without comorbid borderline personality disorder. Child Adolesc Psychiatry Ment Health. 2017;11:4. doi:10.1186/s13034-016-0142-3
50. Berwid OG, Curko Kera EA, Marks DJ, Santra A, Bender HA, Halperin JM. Sustained attention and response inhibition in young children at risk for attention deficit/hyperactivity disorder. J Child Psychol Psychiatry. 2005;46(11):1219–1229. doi:10.1111/j.1469-7610.2005.00417.x
51. Trommer BL, Hoeppner JA, Lorber R, Armstrong KJ. The go-no-go paradigm in attention deficit disorder. Ann Neurol. 1988;24(5):610–614. doi:10.1002/ana.410240504
52. Patton JH, Stanford MS, Barratt ES. Factor structure of the Barratt impulsiveness scale. J Clin Psychol. 1995;51(6):768–774. doi:10.1002/1097-4679(199511)51:6<768::aid-jclp2270510607>3.0.co;2-1
53. Albert J, López‐Martín S, Tapia M, Montoya D, Carretié L. The role of the anterior cingulate cortex in emotional response inhibition. Hum Brain Mapp. 2011;33(9):2147–2160. doi:10.1002/hbm.21347
54. Westen D, Betan E, Defife JA. Identity disturbance in adolescence: associations with borderline personality disorder. Dev Psychopathol. 2011;23(1):305–313. doi:10.1017/S0954579410000817
55. Goodman M, Hazlett EA, Avedon JB, Siever DR, Chu KW, New AS. Anterior cingulate volume reduction in adolescents with borderline personality disorder and co-morbid major depression. J Psychiatr Res. 2011;45(6):803–807. doi:10.1016/j.jpsychires.2010.11.011
56. Ramos-Loyo J, Juárez-García C, Llamas-Alonso LA, Angulo-Chavira AQ, Romo-Vázquez R, Vélez-Pérez H. Inhibitory control under emotional contexts in women with borderline personality disorder: an electrophysiological study. J Psychiatr Res. 2021;132:182–190. doi:10.1016/j.jpsychires.2020.10.014
57. van Zutphen L, Siep N, Jacob GA, et al. Impulse control under emotion processing: an fMRI investigation in borderline personality disorder compared to non-patients and cluster-C personality disorder patients. Brain Imaging Behav. 2020;14(6):2107–2121. doi:10.1007/s11682-019-00161-0
58. Keilp JG, Sackeim HA, Mann JJ. Correlates of trait impulsiveness in performance measures and neuropsychological tests. Psychiatry Res. 2005;135(3):191–201. doi:10.1016/j.psychres.2005.03.006
59. Kertzman S, Lowengrub K, Aizer A, Vainder M, Kotler M, Dannon PN. Go-no-go performance in pathological gamblers. Psychiatry Res. 2008;161(1):1–10. doi:10.1016/j.psychres.2007.06.026
60. Pechtel P, Pizzagalli DA. Effects of early life stress on cognitive and affective function: an integrated review of human literature. Psychopharmacology. 2011;214(1):55–70. doi:10.1007/s00213-010-2009-2
61. Ansell EB, Rando K, Tuit K, Guarnaccia J, Sinha R. Cumulative adversity and smaller gray matter volume in medial prefrontal, anterior cingulate, and insula regions. Biol Psychiatry. 2012;72(1):57–64. doi:10.1016/j.biopsych.2011.11.022
62. Zhai ZW, Yip SW, Lacadie CM, Sinha R, Mayes LC, Potenza MN. Childhood trauma moderates inhibitory control and anterior cingulate cortex activation during stress. NeuroImage. 2019;185:111–118. doi:10.1016/j.neuroimage.2018.10.049
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.