Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
Assessing Determinants of Online Medical Services Adoption Willingness of General Hospital Physicians Using the Information-Motivation-Behavioral Skills Model: A Multi-Group Structural Equation Modeling Approach
Authors Peng X ![]() , Li Z, Zhang C
, Li Z, Zhang C ![]() , Wu Q, Gu J, You H
, Wu Q, Gu J, You H ![]()
Received 28 October 2021
Accepted for publication 10 December 2021
Published 21 December 2021 Volume 2021:14 Pages 3453—3462
DOI https://doi.org/10.2147/JMDH.S346675
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xueqing Peng,1 Zhiguang Li,2 Chi Zhang,3 Qifeng Wu,1 Jinghong Gu,4 Hua You1,3,5
1School of Public Health, Nanjing Medical University, Nanjing, 211166, People’s Republic of China; 2The First Affiliated Hospital with Nanjing Medical University, Nanjing, 210029, People’s Republic of China; 3School of Nursing, Nanjing Medical University, Nanjing, 211166, People’s Republic of China; 4College of Art and Sciences, University of Washington, Seattle, WA, 98195, USA; 5Institute of Healthy Jiangsu Development, Nanjing Medical University, Nanjing, 211166, People’s Republic of China
Correspondence: Hua You
Institute of Healthy Jiangsu Development, Department of Social Medicine and Health Education, School of Public Health, Nanjing Medical University, 101 Longmian Avenue, Jiangning District, Nanjing, 211166, People’s Republic of China
Tel +86-13382772548
Email [email protected]
Purpose: Physician adoption of online medical services (OMS) has been hastened by the COVID-19 pandemic, but their adoption willingness still requires to be improved. This study aims to construct a physician’s OMS adoption willingness model based on the information-motivation-behavioral skill (IMB) theory, explore the determinants affecting adoption willingness and its influencing pathways, and evaluate the moderating effects of OMS use experience on willingness through multi-group analysis.
Participants and Methods: A cross-sectional survey was conducted among physicians in three public hospitals of Jiangsu province, China, from June to July 2020, using a multi-stage sampling method. Structural equation modeling was applied to analyze the valid data from 531 respondents.
Results: Physicians’ willingness to adopt OMS was at a moderate level, with an average score of 14.27± 3.34 (range: 4– 20). The behavior model for physician’s OMS adoption willingness fitted well. Information (In), motivation (Mo), and behavioral skill (BS) explained 69% of the variance in adoption willingness (AW). Information could only exert completely indirect effect on willingness via behavioral skills (b = 0.202, 95% CI[0.122, 0.314]); motivation could both generate direct effect (β=0.368, p < 0.001) and partial indirect effect on willingness via behavioral skills (b = 0.160, 95% CI[0.092, 0.248]); and behavioral skills had a positive effect on willingness (β=0.424, p < 0.001). Furthermore, OMS use experience showed a significant moderating effect on the Mo → AW pathway, with inexperienced physicians’ willingness being significantly stronger influenced by motivation compared to experienced ones.
Conclusion: Findings from this study revealed the role of IMB model in interpreting and predicting physicians’ willingness to adopt OMS and the moderating effect of uptake experience, providing practitioners with a theoretical foundation and intervention framework for supporting OMS development efforts.
Keywords: online medical services, physician, information-motivation-behavioral skills (IMB) model, structural equation modeling
Introduction
The COVID-19 pandemic posed great challenges to health-care services.1 When conventional medical services are unavailable, online medical services (OMS) can deliver varieties of essential treatments via Internet. OMS refers to a new sort of health service mode formed by taking the Internet as the carrier, information technology as the means and deep integration with traditional medical and health services. It contains a variety of medical services, such as disease consultation, telemedicine, online re-examination, chronic disease management, health management, rehabilitation guidance, etc.2,3 Profited by its cross-time-and-space convenience merits, it not only promoted the allocation of medical resources and solved the dilemma of medical inconvenience for non-COVID-19 patients, but also contained the spread of the pandemic.4 Telemedicine, in Hollander’s opinion, is a near-perfect solution to cope with COVID-19.5 In China, despite the increased utilization of OMS driven by the COVID-19 pandemic,6 the overall utilization rate continues to be poor. According to the China Internet Network Information Center,3,7,8 before the COVID-19 pandemic, China had only 195 million OMS users; during the pandemic, it grew to 276 million; but it fell to 239 million in the post-pandemic era. And OMS was used by 26.6%, 29.4%, and 23.7% of Internet users at these three points, respectively. Thus, the utilization of OMS needs to be improved.
Physicians are the stakeholders and main users of OMS. They serve as gatekeepers, deciding whether or not to provide OMS; and their sentiments towards OMS profoundly influence the development of OMS.9 As a result, boosting physicians’ preparedness to embrace OMS appears to be a vital initial step in furthering OMS development. Hence, research is greatly needed to establish the determinants that influence physicians’ willingness to use OMS for targeted intervention.
Some researchers have already applied health behavior theories to explain physicians’ readiness to adopt OMS. Rho et al, for example, using technology acceptance model (TAM), pointed out that perceived usefulness and ease of use can significantly promote physicians’ telemedicine uptake intention;9 Using improved TAM, Saigi-Rubio et al discovered that medical expenses, information security, and patients’ attitudes all affect physicians’ willingness to use OMS;10 In their application of the theory of planned behavior (TPB), Pikkemaat et al found that attitude and perceived behavior control were important predictors of willingness to use telemedicine.11 Most of these aforementioned theories studied the behavior from the standpoint of individuals adopting new technologies, with a focus on individual attitudes and perceptions. However, other factors, like how well physicians are aware of OMS-related information,12 may also have an impact on OMS uptake.
Fisher et al proposed that three elements primarily influence behavior in their information-motivation-behavioral skill (IMB) model. In these factors, information is highly relevant to behaviors, the motivations drive the occurrence of behaviors (individual attitudes and subjective norms), and the behavioral skills are required to implement behaviors.13 These three can not only have direct effects on behavior, in which information and motivation can also indirectly influence behavior via behavioral skills.13 This model has been used by many researchers to investigate a wide range of health behaviors.14–17 But to the best of our knowledge, no previous studies have applied it in the field of OMS research. Whether physicians are willing to adopt OMS is the subject of the health behavior research. As a result, we intend to use it as a framework to build an IMB hypothesis model of physicians’ propensity to embrace OMS (Figure 1) and test it with existing data.
 |
Figure 1 Conceptual framework of physician’s OMS adoption willingness based on IMB model. Abbreviation: OMS, online medical services. Notes: Pathway tests: “+” represents the positive relationships between IMB factors and OMS adoption willingness. Mediation tests: Test 1 (1—>3—>4) and Test 2 (2—>3—>4). |
Taking into account important moderating variables aids in a better understanding of causation. According to Duplaga et al, nurses’ prior experience in information technology is the main determinant in their acceptance of e-health solutions;18 While Pynoo et al discovered that doctors’ acceptance of picture archiving and communication systems is unaffected by experience.19 Kuo et al emphasized the effects of previous telemedicine experience, and they were able to demonstrate that the presence or absence of experience affected physicians’ telemedicine perception and intention differently.20 Evidence from these studies suggests that the OMS use experience may be an important moderating factor. Hence, in this study, it is included as a moderating variable in the model of this study.
Specifically, we employed the structural equation modeling (SEM) to verify: (1) whether the hypothetical model is established and to investigate the determinants and pathways of physician’s OMS adoption willingness (2) moderating effects of OMS use experience on the relationship between IMB factors and physician’s adoption willingness.
Materials and Methods
Design and Sample
We used multistage stratified sampling to perform a cross-sectional survey on the physicians’ OMS utilization in Jiangsu province, China, from June to July 2020. Jiangsu province, located in the coastal area of eastern China, is a city with high economic and medical levels. To begin with, three prefecture-level cities from Jiangsu’s southern, central, and northern regions were selected by their geographic location and economic status. Second, a tertiary public hospital was randomly selected from each city. Thus, a total of three hospitals were selected. Thirdly, the qualified physicians (excluded interns) were recruited from each hospital.
After the qualified physicians agreed to participate in this investigation, the specially trained investigators distributed the questionnaire and instructed them how to understand the self-administered questionnaire and fill it out within 20 minutes. We determined the sample size according to the criterion of 1:10 observations per indicator,21 and taken into account 15% of invalid questionnaires. Because the questionnaire lists 23 observed variables, a minimum sample size of 318 was required. Therefore, a total of 550 respondents received survey questionnaires. After excluding the invalid questionnaires that were not completely filled out or had obvious logic errors, a total of 531 (more than the minimum sample size) were finally included in the analysis. The effective response rate was 96.5%. Oral informed consent was approved by the Ethics Review Committee of Nanjing Medical University.
Measures
Basic Information
This section included demographic characteristics (gender, age, education, working years, job title, specialty) and OMS use experience (Have you ever used OMS?). “Experienced” physicians were defined as those who had used any service function within the scope of the OMS definition.
Scale Questionnaire Based on IMB Model
This section of the measure was self-designed with reference to some relevant studies and government documents,10,22–24 as well as the review comments and suggestions of experts. The scale has 16 items (Table S1), comprising four subscales: information, motivation, behavioral skills, and adoption willingness. Each subscale contains four items respectively. The information subscale consists of information related to carrying out OMS, eg, “Physicians can register multiple online medical platforms at the same time”; the motivation subscale assesses physicians’ personal and social motivations (subjective norms) for OMS, eg, “I think performing OMS can broaden my medical business”; the behavioral skills subscale is concerned with the skills required to carry out OMS, eg, “I can independently use OMS to provide diagnosis and treatment services for patients”; and the adoption willingness subscale is used to measure the willingness to adopt OMS, eg, “I have a high probability of using OMS in the future”. Regarding the information subscale, the answer options of each item are assigned to the corresponding scores according to a 5-level Likert scale: 1 = “absolutely unknown”, 2 = “unknown”, 3 = “a little known”, 4 = “mostly known”, and 5 = “absolutely known”. Similarly, for remaining three subscales, the answer options are set as: 1 = “absolutely disagree”, 2 = “disagree”, 3 = “a little agree”, 4 = “mostly agree”, and 5 = “absolutely agree”. Each subscale has a total score range of 4–20. A higher score signals higher level of information mastery, greater OMS adoption motivation, more OMS operation skills, and stronger OMS adoption willingness.
The Cronbach’s α coefficients of the four subscales range from 0.799 to 0.925. For the entire scale, the Cronbach’s α coefficient is 0.931, the Kaiser-Meyer-Olkin (KMO) value is 0.929, and the p value of Bartlett’s test is <0.001. The scale has good reliability and validity.
Data Analysis
The SPSS 25.0 software was used for performing descriptive statistics, Pearson’s correlation analysis, and t-test. The AMOS 23.0 software was applied to perform maximum likelihood SEM to test the hypothesis model developed in this study.
In SEM, confirmatory factor analysis (CFA) was employed to ensure that each measurement model was valid. The factor loadings (>0.6 acceptable), composite reliability (CR, >0.7 acceptable), and average variance extracted (AVE, >0.5 acceptable) were used to evaluate the pros and cons of the measurement model.25 In structural model, we tested the direct and indirect effects of the IMB components on the OMS adoption willingness. The significance of the indirect effect (namely behavioral skills’ mediating effect) is judged by running the bias-corrected bootstrap for 5000 times to obtain a 95% confidence interval (CI); if the CI does not contain zero, the indirect effect is significant.26
To see if OMS use experience had a moderating influence, we performed SEM multi-group analysis. First, we compared the experienced and inexperienced groups’ factor loading equivalence of the measurement models. Then, under the constraints of equal factor loadings and structural pathways, we looked to see if the proposed model differed significantly different between the two groups; if p < 0.05, then moderating effect existed.26 Next, significance comparison on direct path differences between the two groups is determined by the parameter critical ratios for differences (CRD). An absolute CRD value higher than 1.965 indicates that there is a significant difference at p < 0.05 level. The behavioral skills’ moderated mediation was tested by calculating the 95% bias-corrected CI of the mediating effect difference value between the two groups.26
All of our data met the criteria for univariate normality (skew <2.0 and kurtosis <0.7). But it did not obey multivariate normality, since the multivariate kurtosis’ critical ratio is 50.966, higher than 5.27 Violation of multivariate normality results in an overestimation of χ2 and a deterioration in model fit.28 Therefore, we performed 5000 times Bollen-Stine bootstrap procedure to correct the model fit. The model fit was evaluated by the following indicators:29 Goodness-of-Fit Index (GFI), Adjust Goodness-of-Fit Index (AGFI), and Comparative Fit Index (CFI) (recommended to be >0.9, but >0.8 acceptable); Root Mean-Square Error of Approximation (RMSEA) (recommended to be <0.08). The determinate coefficient R2 should generally be higher than 0.33 (as recommended, (0.19 (small), 0.33 (medium), 0.67 (high)).30
The significance level was set at α = 0.05.
Results
Basic Characteristics
Of the 531 valid respondents, 51.0% were male and 49.0% were female, with an average age of 35.0±7.1 years. The education level was dominated by masters, accounting for 253 (47.6%). Regarding job title, attending physicians accounted for the largest proportion (192 (36.2%)). Two hundred and seventy-four physicians (51.6%) reported ever using OMS. The mean scores of each IMB construct (range: 4–20) were at a moderate level: information (12.90±3.26), motivation (13.59±3.22), behavioral skills (12.98±3.53) and adoption willingness (14.27±3.34) (Table 1).
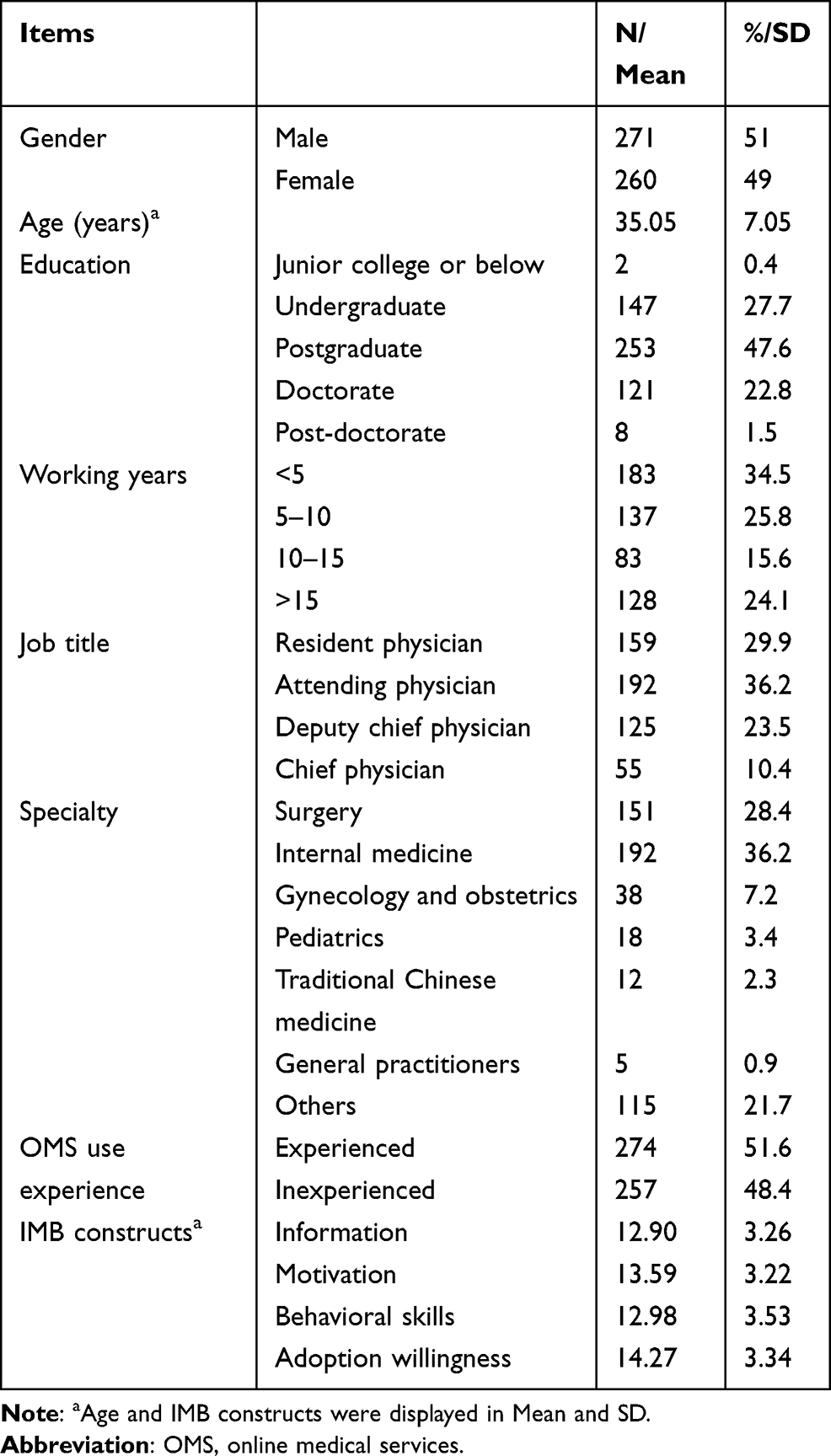 |
Table 1 Basic Characteristics |
Results of Bivariate Correlations and Comparison Tests
Information (r = 0.450), motivation (r = 0.693), and behavioral skills (r = 0.657) all had significant correlations with OMS adoption willingness (p < 0.01) (Table 2). In comparison to inexperienced physicians, experienced physicians had higher information (t = 6.939), motivation (t = 3.951), behavioral skills (t = 8.098), and adoption willingness (t = 5.703) p < 0.001 (Table 3).
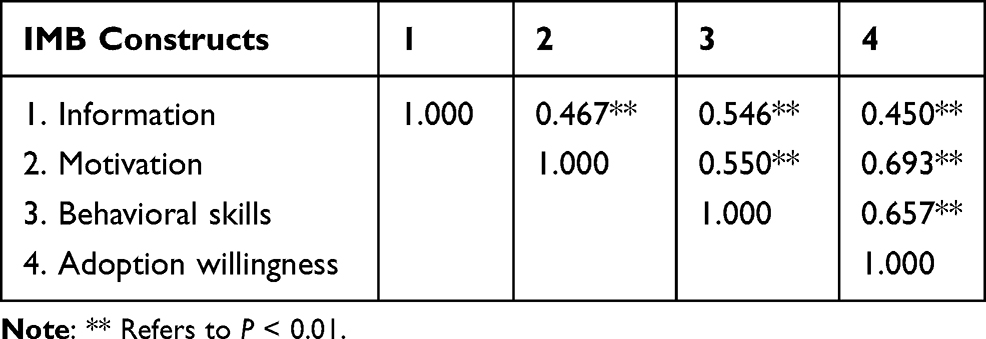 |
Table 2 Bivariate Correlations Among IMB Constructs |
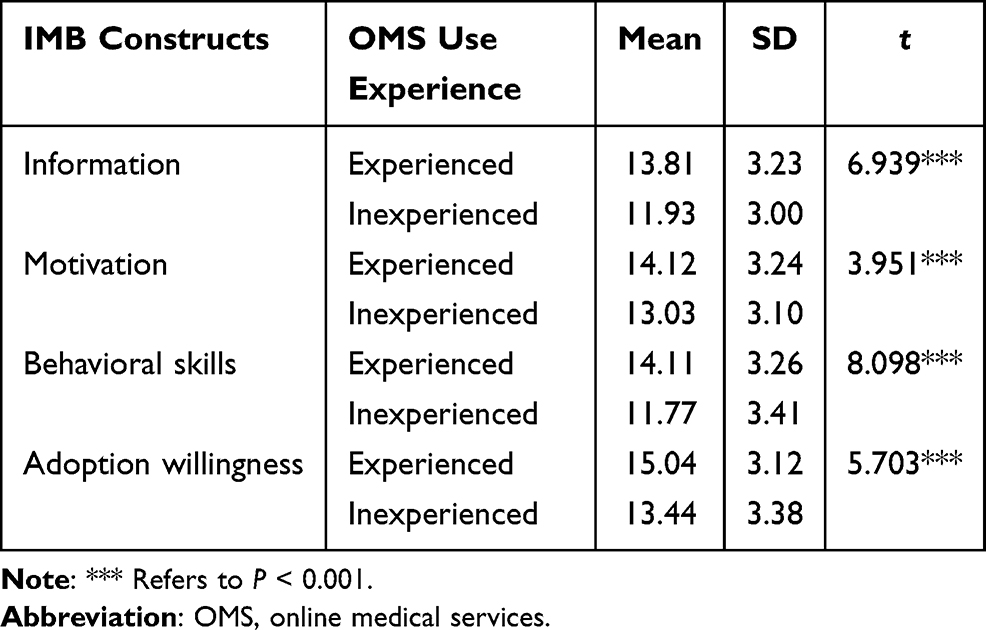 |
Table 3 Comparison of IMB Constructs on OMS Use Experience Groups |
Measurement Model
The CFA results revealed that observed variables can reflect the corresponding IMB constructs well. The factor loading ranges of the four constructs were information (0.639–0.777), motivation (0.706–0.875), behavioral skills (0.740–0.877), and adoption willingness (0.830–0.902); all these factor loadings were significant. All latent facets had good internal consistency (CR >0.7) and convergent validity (AVE >0.5) (Table S2).
Structural Model
The structural model fitted well: χ2=304.045, df =98, CFI=0.965, GFI=0.932, AGFI=0.906, RMSEA=0.063. In Table 4 and Figure 2. For the full sample model, motivation (β=0.495) and behavioral skills (β=0.424) could directly and positively affect physicians’ OMS adoption willingness, but information could not directly affect it, p<0.001. Information (β=0.431) and motivation (β=0.368) can also directly and positively influence behavioral skills, p<0.001. Both information (b=0.202, 95% CI [0.122, 0.314]) and motivation (b=0.160, 95% CI [0.092, 0.248]) can affect OMS adoption willingness indirectly via behavioral skills, as shown in Table 5. Information had a complete indirect effect, while motivation showed a partial one. Information and motivation accounted for 49% of the variance in behavioral skills; and information, motivation, and behavioral skills accounted for 69% of the variance in OMS adoption willingness.
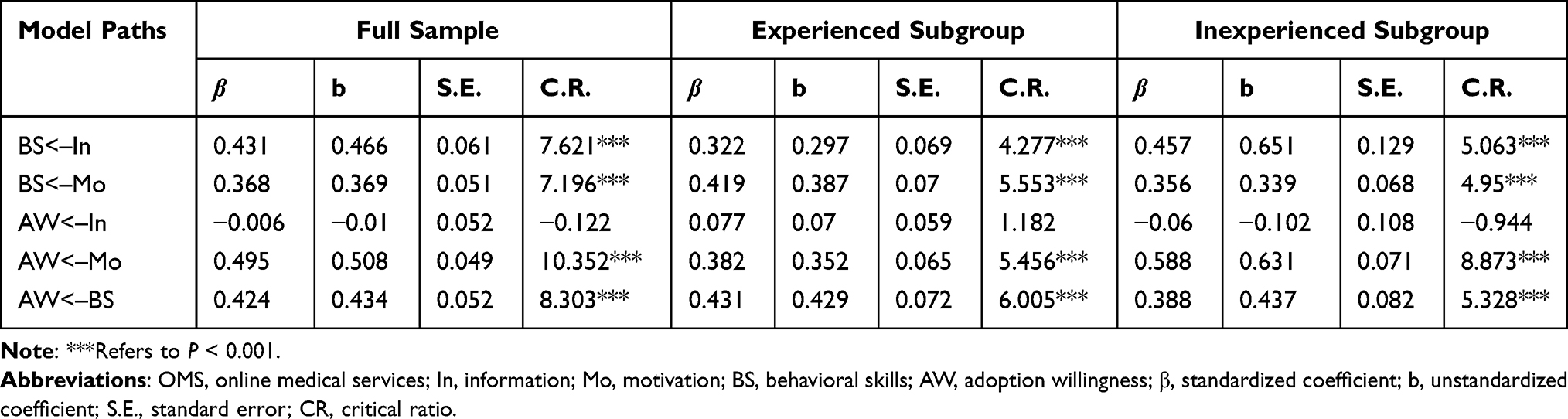 |
Table 4 Results of Structural Model for Full Sample and OMS Use Experience Subgroups |
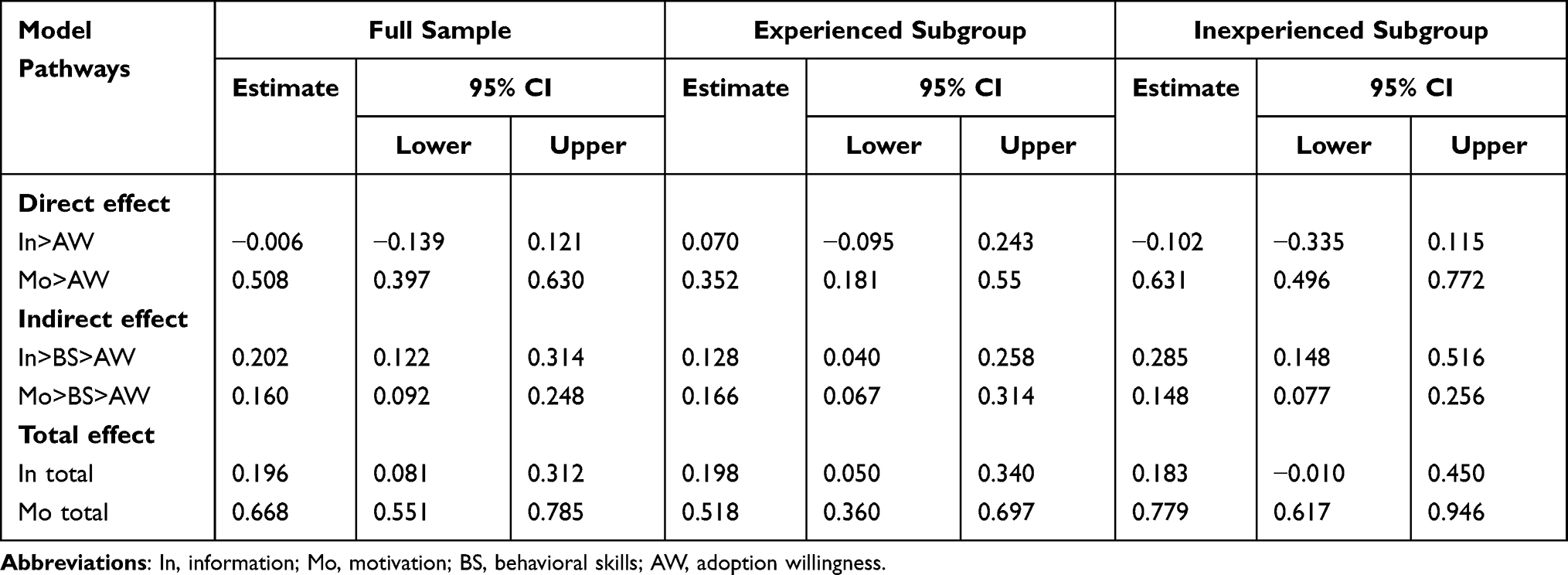 |
Table 5 Direct and Indirect Effects and 95% Confidence Intervals (CI) |
 |
Figure 2 Standardized structural model of OMS adoption willingness (full sample). Abbreviations: OMS, online medical services; ns, non-significant. Note: ***Refers to P < 0.001. |
Multi-Group Analysis of OMS Use Experience
The path results of the OMS experience subgroup are shown in Table 5 and Figure 3. The two groups’ factor loadings were equivalent at the measurement level (p = 0.768). The testing results from constrained model with equal factor loadings and path coefficients revealed a statistically significant difference between the two experience groups (p = 0.020). That is, OMS use experience had significant moderating effect.
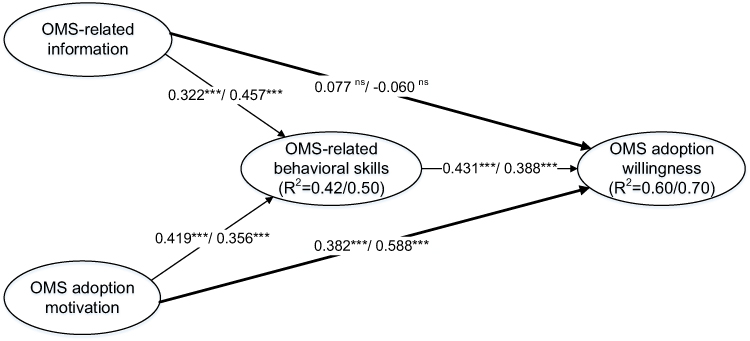 |
Figure 3 Standardized structural model of OMS adoption willingness (group comparison by OMS use experience). Abbreviations: OMS, online medical services; ns, non-significant. Notes: Structural model with standardized estimates for experienced/inexperienced groups. The paths in bold yield significant differences between the two groups. ***Refers to P < 0.001. |
In Figure 3, both the Mo—>AW pathway coefficients in experienced (β=0.382) and inexperienced (β=0.588) group were significant, p < 0.001. In addition, there is a significant difference between the two groups in the Mo—>AW pathway (CRD = 2.901, p < 0.05). That is, the direct association between Mo—>AW was moderated by the OMS use experience, as seen by the fact that inexperienced physicians’ motivation had a stronger positive impact on adoption willingness compared with experienced ones. Furthermore, there was a significant difference in the In—>AW route between the two groups (CRD = 2.422, p < 0.05). Although experience moderated the In—>AW relationship, the information showed no significant effect on adoption willingness in both groups. The remaining direct paths between the two groups were not significantly different.
The mediation effect difference value of information between the two groups was not significant (diff b=−0.157, 95% CI [−0.408, 0.018]). The same goes for motivation (diff b= 0.018, 95% CI [−0.127, 0.178]). That is, the OMS usage experience did not moderate the mediation effect on behavioral skills.
Discussion
In this study, physicians’ OMS adoption willingness showed a moderate level. It is similar to some previous findings. For example, a study in Senegal showed that physicians’ willingness to utilize telemedicine was moderate;31 Hu and Chau found that physicians working in public tertiary hospitals had a moderate intention to use telemedicine technology.32 In the current promotion of Internet medicine, it is vital to pay attention to improving physician’s uptake intention. Using IMB model, we explored the determinants of physicians’ OMS adoption willingness and examined the route interaction between these factors. The high R2 value (0.69) indicated a great explanatory power of these factors. Meanwhile, the applicability of the proposed model was supported by the good model fit. Furthermore, due to diverse OMS use experiences, several route outcomes revealed some fluctuation. These findings offer fresh insights into how to boost physicians’ OMS adoption willingness.
Unlike Fisher’s IMB model,13 the OMS-related information showed only a completely indirect effect on adoption willingness via behavioral skills, rather than a direct effect. Previous studies have shown that if the behavior is particularly complex, the direct pathway of information effects on behavior would not exert.33,34 OMS is a relatively young technology as a revolutionary health service paradigm. Furthermore, various types of OMS involved different operational techniques. Telemedicine, for example, necessitates a thorough understanding of modern communication technology, computer multimedia, and other equipment; online rehabilitation counseling requires mastering the various operating functions provided by the online medical platform, etc. Thus, users need to be proficient in multiple operating skills. This could explain the mechanism of information on adoption willingness. Information is a necessary condition for generating behavior.35 Although our study does not indicate a direct association between information and adoption willingness, it did show that information can influence behavioral skills. Furthermore, this study showed that physicians had only a moderate knowledge of OMS-related information. Therefore, strengthening the visibility and popularization of OMS-related information among physicians is essential.
Even with abundant information and proficient behavioral skills, strong motivation is still required to produce and maintain behaviors.36 Our findings supported the direct and indirect effect of motivation on adoption willingness, as predicted by IMB. Physicians with a high level of motivation were more likely to have relevant behavioral skills and, further, were more likely to have OMS uptake intention. Several other researchers have also confirmed this positive association between them.37–39 This finding suggests that enhancing physicians’ motivation regarding adopting OMS is also a profitable measure. In this paradigm, motivation in this model includes both personal motivation and social motivation. The benefits of conducting OMS, such as expanding business and boosting efficiency, prompt physicians’ willingness to use.40,41 Incentives from peers and patients can also strengthen their desire to adopt. For example, Shoaib et al found that reasons for health-care professionals to use e-health are being recommended by peers and experts;42 Han et al claimed that better communication with patients through m-health had an incentive effect.43 As a result, tailored interventions can be considered for boosting both personal motivation and social motivation. For example, to publicize OMS’s benefits, to increase incentive mechanism on physicians, and to urge those who work with physicians to play a positive role (ie, peers, patients).
A positive association between behavioral skills and adoption willingness was also discovered in this study. Familiarity with skills can facilitate physicians’ uptake willingness. This is consistent with the findings of prior studies.44,45 A lack of skills in conducting OMS has been identified as a major impediment for physicians in numerous research.46–48 To conduct OMS, it demands more than just basic operational skills (ie, proficiently using electronic devices and website functions). Physicians must also need to coordinate their online and offline working time and own adequate self-efficacy to overcome difficulties encountered during the OMS process.37 Given that behavioral skills also act as a mediator, it exerts a critical role in affecting OMS adoption willingness. Hence, enhancing physicians’ behavioral skills is a key measure, and practitioners should place great emphasis on the intervention of behavioral skills.
Finally, the multi-group analysis results of OMS use experience displayed that the aforementioned information and behavioral skills results were applicable for both physicians with and without experience. However, it showed a moderating effect on the pathway between motivation and willingness. Similar to Kuo et al’s findings,20 inexperienced physicians’ adoption willingness was significantly stronger influenced by motivation compared to experienced physicians. Older staff members may be more likely to have relevant experience using OMS. However, previous studies have shown that years of work experience was negatively correlated with physicians’ telemedicine uptake willingness.31 That implies, older staffs could be less eager to engage with OMS. This may explain why experienced physicians are less impacted by motivation than inexperienced physicians. This finding may serve as a reminder that experienced physicians can be fully leveraged to persuade inexperienced physicians of the advantages and benefits of using OMS, so as to arouse interest and even desire to adopt OMS.
Several limitations: first, the respondents were enrolled from tertiary public hospitals. Therefore, extending the results to physicians in secondary hospitals or primary medical units may be erroneous. In subsequent research, the sample population can be expanded to validate the results among physicians in other hospital types. Second, the information was gathered using a cross-sectional survey, which can only indicate a connection observed at a single time point and cannot establish a strong causal relationship. This requires further longitudinal study to verify. Third, OMS contains a wide variety of types. Different types of OMS functions may have been hampered by different obstacles. We just looked at the broad determinants of OMS; the influencing factors of specific OMS types need to be further investigated. Also, our classification of “experience” is a little nebulous. The potential influence of physicians’ differing OMS usage experience with telemedicine programs might confound the result. Fourth, the COVID-19 pandemic has resulted in a temporary surge in the utilization of OMS in China. This study was conducted during the COVID-19 pandemic, and did not examine how physicians’ uptake willingness change in the COVID-19 post-pandemic era. Therefore, further research is needed to determine the lasting impact of the COVID-19 pandemic on physicians’ OMS uptake willingness.
Conclusion
In summary, based on the IMB model, this study is the first to propose and test the determinants of physicians’ OMS adoption willingness, as well as the mechanism among these factors. It offered a theoretical foundation and intervention framework for supporting OMS development efforts; and it also enriched the existing application of IMB model in the field of behavioral research. In addition, it revealed a moderating effect of physicians’ OMS experience on the relationship between motivation and willingness to use OMS. In terms of practical application, findings from this study provide practitioners fresh insights to more effectively boosting the development of OMS.
Ethics Approval
This study was approved by the Ethics Review Committee of Nanjing Medical University (No. (2020)592). All participants in this study provided oral informed consent.
Acknowledgments
We would like to thank all the physicians for their participation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China [grant number 72074122]; and Cultivation Project of Decision-making Consultation, Institute of Healthy Jiangsu Development, Nanjing Medical University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang YN, Chen Y, Wang Y, et al. Reduction in healthcare services during the COVID-19 pandemic in China. BMJ Glob Health. 2020;5(11):e003421. doi:10.1136/bmjgh-2020-003421
2. Shaw T, McGregor D, Brunner M, Keep M, Janssen A, Barnet S. What is eHealth (6)? Development of a conceptual model for ehealth: qualitative study with key informants. J Med Internet Res. 2017;19(10):e324. doi:10.2196/jmir.8106
3. China Internet Network Information Center. The 39th China statistical report on internet development. Available from: http://www.cnnic.net.cn/hlwfzyj/hlwxzbg/hlwtjbg/201701/P020170123364672657408.pdf.
4. Hong Z, Li N, Li DJ, et al. Telemedicine during the COVID-19 pandemic: experiences from Western China. J Med Internet Res. 2020;22(5):e19577. doi:10.2196/19577
5. Hollander JE, Carr BG. Virtually perfect? Telemedicine for Covid-19. N Engl J Med. 2020;382(18):1679–1681. doi:10.1056/NEJMp2003539
6. Health people.cn. National Health Commission: internet diagnosis and treatment in commission-managed hospitals increased by 17 times compared with the same period last year. Available from: http://health.people.com.cn/n1/2020/0320/c14739-31647877.html. Accessed September 29,2021.
7. China Internet Network Information Center. The 46th China statistical report on internet development. Available from: http://www.cnnic.net.cn/hlwfzyj/hlwxzbg/hlwtjbg/202009/P020210205509651950014.pdf.
8. China Internet Network Information Center. The 48th China statistical report on internet development. Available from: http://www.cnnic.net.cn/hlwfzyj/hlwxzbg/hlwtjbg/202109/P020210915523670981527.pdf.
9. Rho MJ, Choi IY, Lee J. Predictive factors of telemedicine service acceptance and behavioral intention of physicians. Int J Med Inform. 2014;83(8):559–571. doi:10.1016/j.ijmedinf.2014.05.005
10. Saigi-Rubio F, Jimenez-Zarco A, Torrent-Sellens J. Determinants of the intention to use telemedicine: evidence from primary care physicians. Int J Technol Assess. 2016;32(1–2):29–36. doi:10.1017/S0266462316000015
11. Pikkemaat M, Thulesius H, Nymberg VM. Swedish primary care physicians’ intentions to use telemedicine: a survey using a new questionnaire - Physician Attitudes and Intentions to Use Telemedicine (PAIT). Int J Gen Med. 2021;14:3445–3455. doi:10.2147/IJGM.S319497
12. Dunnebeil S, Sunyaev A, Blohm I, Leimeister JM, Krcmar H. Determinants of physicians’ technology acceptance for e-health in ambulatory care. Int J Med Inform. 2012;81(11):746–760. doi:10.1016/j.ijmedinf.2012.02.002
13. Fisher JD, Fisher WA. Changing AIDS-risk behavior. Psychol Bull. 1992;111(3):455–474. doi:10.1037/0033-2909.111.3.455
14. Green SM, Turner D, Baldwin JA, et al. Towards an information motivation and behavioral skills model for new sex partners: results of a study of condom use as an HIV prevention method for emerging adults who met partners on dating and sex-seeking platforms or offline. AIDS Behav. 2019;23(5):1115–1134. doi:10.1007/s10461-018-2349-1
15. Wang HW, Chang RJ, Shen QM, et al. Information-motivation-behavioral skills model of consistent condom use among transgender women in Shenyang, China. BMC Public Health. 2020;20(1):1–9.
16. Tsamlag L, Wang HW, Shen QM, et al. Applying the information-motivation-behavioral model to explore the influencing factors of self-management behavior among osteoporosis patients. BMC Public Health. 2020;20(1):1–8. doi:10.1186/s12889-020-8292-x.
17. Nelson LA, Wallston KA, Kripalani S, et al. Assessing barriers to diabetes medication adherence using the information-motivation-behavioral skills model. Diabetes Res Clin Pract. 2018;142:374–384. doi:10.1016/j.diabres.2018.05.046
18. Duplaga M, Carpenter DO. Searching for a role of nursing personnel in developing landscape of Ehealth: factors determining attitudes toward key patient empowering applications. PLoS One. 2016;11(4):e0153173. doi:10.1371/journal.pone.0153173
19. Pynoo B, Devolder P, Duyck W, van Braak J, Sijnave B, Duyck P. Do hospital physicians’ attitudes change during PACS implementation? A cross-sectional acceptance study. Int J Med Inform. 2012;81(2):88–97. doi:10.1016/j.ijmedinf.2011.10.007
20. Kuo KM, Talley PC, Lee CM, Yen YC. The influence of telemedicine experience on physicians’ perceptions regarding adoption. Telemed E-Health. 2015;21(5):388–394. doi:10.1089/tmj.2014.0091
21. Chin WW. The partial least squares approach for structural equation modeling. In: Marcoulides GA, editor. Modern Methods for Business Research. Lawrence Erlbaum Associates Publishers; 1998:295–336.
22. The State of Council of the People's Republic of China. Notice on printing and distributing three documents including the measures for the administration of Internet diagnosis and treatment (Interim). Available from: http://www.gov.cn/gongbao/content/2019/content_5358684.htm. Accessed September 29,2021.
23. Yada N, Head M. Attitudes toward health care virtual communities of practice: survey among health care workers. J Med Internet Res. 2019;21(12):e15176. doi:10.2196/15176
24. Kissi J, Dai BZ, Dogbe CSK, Banahene J, Ernest O. Predictive factors of physicians’ satisfaction with telemedicine services acceptance. Health Inform J. 2020;26(3):1866–1880. doi:10.1177/1460458219892162
25. Hair JF, Ringle CM, Sarstedt M. PLS-SEM: indeed a silver bullet. J Mark Theory Pract. 2011;19(2):12.
26. Jiang S, Liang ZR. Mediator of school belongingness and moderator of migration status in the relationship between peer victimization and depression among Chinese children: a multi-group structural equation modeling approach. J Affect Disord. 2021;278:382–389. doi:10.1016/j.jad.2020.09.075
27. Byrne BM. Structural Equation Modeling with AMOS:Basic Concepts, Applications, and Programming. Taylor and Francis; 2016.
28. Kline RB. Principles and Practices of Structural Equation Modeling.
29. Doll WJ, Xia WD, Torkzadeh G. A confirmatory factor analysis of the end-user computing satisfaction instrument. MIS Q. 1994;18(4):8. doi:10.2307/249524
30. Urbach N, Ahlemann F. Structural equation modeling in information systems research using partial least squares. J Inf Technol Theory Appl. 2010;11(2):34.
31. Ly BA, Kristjansson E, Labonte R, Bourgeault IL. Determinants of the intention of senegal’s physicians to use telemedicine in their professional activities. Telemed E-Health. 2018;24(11):879–898. doi:10.1089/tmj.2017.0276
32. Hu PJ, Chau PY. Physician acceptance of telemedicine technology: an empirical investigation. Top Health Inf Manage. 1999;19(4):20–35.
33. John SA, Walsh JL, Weinhardt LS. The information-motivation-behavioral skills Model revisited: a network-perspective structural equation model within a public sexually transmitted infection clinic sample of hazardous alcohol users. AIDS Behav. 2017;21(4):1208–1218. doi:10.1007/s10461-016-1446-2
34. Zhu CD, Cai Y, Ma J, et al. Predictors of intention to smoke among junior high school students in Shanghai, China: an empirical test of the Information-Motivation-Behavioral Skills (IMB) model. PLoS One. 2013;8:11.
35. Alzghoul BI, Abdullah NA. Pain management practices by nurses: an application of the Knowledge, Attitude and Practices (KAP) model. Glob J Health Sci. 2015;8(6):154–160. doi:10.5539/gjhs.v8n6p154
36. Fisher JD, Fisher WA, Misovich SJ, Kimble DL, Malloy TE. Changing AIDS risk behavior: effects of an intervention emphasizing AIDS risk reduction information, motivation, and behavioral skills in a college student population. Health Psychol. 1996;15(2):114–123. doi:10.1037/0278-6133.15.2.114
37. Guo X, Han X, Zhang X, Dang Y, Chen C. Investigating m-Health acceptance from a protection motivation theory perspective: gender and age differences. Telemed J E Health. 2015;21(8):661–669. doi:10.1089/tmj.2014.0166
38. Zhang X, Guo X, Lai KH, Guo F, Li C. Understanding gender differences in m-health adoption: a modified theory of reasoned action model. Telemed J E Health. 2014;20(1):39–46. doi:10.1089/tmj.2013.0092
39. Nov O, Schecter W. Dispositional resistance to change and hospital physicians’ use of electronic medical records: a multidimensional perspective. J Am Soc Inf Sci Tec. 2012;63(4):648–656.
40. Lord S, Moore SK, Ramsey A, Dinauer S, Johnson K. Implementation of a substance use recovery support mobile phone app in community settings: qualitative study of clinician and staff perspectives of facilitators and barriers. JMIR Ment Health. 2016;3(2):e24. doi:10.2196/mental.4927
41. Duhm J, Fleischmann R, Schmidt S, Hupperts H, Brandt SA. Mobile electronic medical records promote workflow: physicians’ perspective from a survey. JMIR Mhealth Uhealth. 2016;4(2):e70. doi:10.2196/mhealth.5464
42. Shoaib SF, Mirza S, Murad F, Malik AZ. Current status of e-health awareness among healthcare professionals in teaching hospitals of Rawalpindi: a survey. Telemed J E-Health. 2009;15(4):347–352. doi:10.1089/tmj.2008.0124
43. Han KJ, Subramanian R, Cameron GT. Listen before you leap: Sri Lankan health professionals’ perspectives on m-health. Health Inform J. 2019;25(3):858–866. doi:10.1177/1460458217725903
44. Gagnon MP, Ngangue P, Payne-Gagnon J, Desmartis M. m-Health adoption by healthcare professionals: a systematic review. J Am Med Inform Assoc. 2016;23(1):212–220. doi:10.1093/jamia/ocv052
45. Jacob C, Sanchez-Vazquez A, Ivory C. Social, organizational, and technological factors impacting clinicians’ adoption of mobile health tools: systematic literature review. JMIR Mhealth Uhealth. 2020;8(2):e15935.
46. Tintorer DL, Dominguez JMM, Pujol-Rivera E, Beneyto SF, Tuduri XM, Saigi-Rubio F. Keys to success of a community of clinical practice in primary care: a qualitative evaluation of the ECOPIH project. BMC Fam Pract. 2018;19. doi:10.1186/s12875-017-0674-5
47. Sinclair C, Holloway K, Riley G, Auret K. Online mental health resources in rural Australia: clinician perceptions of acceptability. J Med Internet Res. 2013;15(9):e193. doi:10.2196/jmir.2772
48. Jungwirth D, Haluza D. Information and communication technology and the future of healthcare: results of a multi-scenario Delphi survey. Health Informatics J. 2019;25(1):161–173. doi:10.1177/1460458217704256
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.