Back to Journals » Psychology Research and Behavior Management » Volume 16
Assessing Anxiety and Depression Among Students Post-COVID-19: Exploring Associating Factors
Authors Basheti IA, Assaraira TY, Obeidat NM, Al‐Abed Al‐haq F, Refai M
Received 22 February 2023
Accepted for publication 29 April 2023
Published 12 May 2023 Volume 2023:16 Pages 1797—1810
DOI https://doi.org/10.2147/PRBM.S409632
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Iman A Basheti,1,2 Thafer Yusif Assaraira,3 Nathir M Obeidat,4 Fawwaz Al‐Abed Al‐haq,5 Mashhoor Refai6
1Department of Clinical Pharmacy and Therapeutics, Faculty of Pharmacy, Applied Science Private University, Amman, Jordan; 2School of Pharmacy, Faculty of Medicine and Health, The University of Sydney, Sydney, NSW, Australia; 3English Department, Mutah University, Al‐Karak, Jordan; 4Department of Internal Medicine, The University of Jordan, Amman, Jordan; 5Department of English Language and Literature, Hashemite University, Zarqa, Jordan; 6King Abdullah II School of Engineering, Princess Sumaya University for Technology, Amman, Jordan
Correspondence: Iman A Basheti, Department of Clinical Pharmacy and Therapeutics, Applied Science Private University, Amman, 11931, Jordan, Email [email protected]
Background: The COVID-19 pandemic has had a large impact on global mental health including anxiety and depression rates, many factors affected the vulnerability to these psychological conditions amongst university students.
Aim: To explore the level of anxiety and depression of university students living in Jordan.
Methods: A cross-sectional study design was conducted in which an electronic survey was created and distributed, university students residing in Jordan participated in the study.
Results: A total of 1241 students were enrolled in the study. The mean anxiety score among males and females was (9.68 (SD = 4.10)) and (10.46 (SD = 4.14)), respectively. 42.1% of males had “abnormal” anxiety score compared to 48.4% females. The mean depression score among males (7.77 (SD = 4.31)) was similar to that for the females (7.64 (SD = 4.14)), and 26.0% of the males had “abnormal” depression score compared to 22.6% of the females. Factors affecting anxiety scores included younger age, being a female, taking medication/s, or drinking two cups of coffee or more a day.
Conclusion: With 46% and 24% of students suffering from abnormal anxiety and depression respectively, it is important for education policy makers to take immediate measures to allocate students in need of psychological assessment and help to deliver suitable interventions.
Keywords: anxiety, depression, students, Jordan, psychological assessment
Introduction
Coronavirus disease 2019 (COVID-19) is a viral respiratory disease caused by the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that primarily spreads via inhalation of respiratory droplets or direct contact with contaminated surfaces.1 During the last few years, the pandemic has led to a significant global crisis owing to the rapid spread and high morbidity and mortality rates of the COVID-19 virus.2 As such, the World Health Organization (WHO) declared the COVID-19 outbreak as a global pandemic on March 11, 2020.3 Until October 26, 2022, there were 633,963,548 reported cases and 6,586,483 reported deaths worldwide.4 The symptoms of COVID-19 vary depending on the viral load5 and vaccination status of patients,6 ranging from asymptomatic to mild, moderate, or severe symptoms; such symptoms either self-resolve or require hospitalization and monitoring.
Several interventions have been implemented to limit the spread and rise of COVID-19 cases, such as travel restrictions, border measures, social distancing, use of masks, isolation and quarantine, and various mobility and lockdown strategies which effectively decreased COVID-19 cases.7 However, although quarantine deemed an effective way in reducing the spread of the virus globally,8 and health-care professionals worldwide were aware about route of transmission and clinical symptoms,9,10 several significant negative economic, social, and psychological impacts caused as a consequence.11 As a result, people faced a myriad of challenges and issues, including psychological pressure.12,13
It is now well documented that the COVID-19 pandemic has had a large and uneven impact on global mental health.14 According to studies conducted at the start of the lockdown due to COVID-19 pandemic, stress directly related to the viral infection, in addition to concerns about the disruptions that affected the health-care services and employment contributed to psychological anguish.15–17 Post-traumatic stress disorder (PTSD) symptoms, stress, anxiety, and depressive symptoms were among of the common psychological effects of the pandemic. The risk of contracting the virus, the type of daily living restrictions, patient’s gender, COVID-19 information-seeking behavior, educational level, income level, and age of patients, were all personal and contextual factors that affected the vulnerability to and severity of these psychological issues in different population segments.18,19
One of the fundamental elements of a community that deserves to receive proper attention during this pandemic is university students.20 Higher education students tended to experience various psychological difficulties because of the significant changes in the teaching and learning methods that took place during the pandemic.18,19,21 Many universities throughout the world have transferred their courses online to maintain their academic routines after lengthy lockdowns and school closures. As most students have goals and aspirations for the future, these conditions have had an unparalleled impact on them. Students’ lives and education were severely disrupted during the pandemic, which has made their futures even more uncertain, leading to heightened stress.18,19
Numerous researches have examined the pandemic’s effects on university students’ mental health and the factors associated with higher levels of distress. For example, 195 undergraduate students from one university in the United States of America who participated in an interview survey about the COVID-19 pandemic acknowledged the negative effects and the urgent need for developing interventions and preventive techniques.22 Another study of 162 undergraduate students found high levels of mental health distress, with depression being associated with difficulties focusing on academic work, job loss, and higher levels of anxiety in students seeking more information on COVID-19.23 High levels of depression were also reported in a July 2020 online survey of 255 students at a university in Hong Kong, and depressive symptoms were found to exist and adversely correlated with perceived availability of peer support.24 Another online study conducted in February 2020 involving 11,787 Chinese college students revealed that the prevalence rates of depression and anxiety symptoms were 25.9% and 17.8%, respectively.25
A cross‑sectional online survey conducted in December 2020 at a nursing college attached to a tertiary care teaching hospital in North India involving 251 bachelor’s degree in nursing showed that coronavirus pandemic caused significant distress among nursing students.26 Being able to minimize the anxiety and depression symptoms among university students, it would be essential to assess their mental health condition and possible ways to mitigate such symptoms. No previous study has assessed the rate of anxiety and depression amongst students in Jordan post COVID-19 pandemic and changes that took place in the tertiary education process.
This study was designed to analyze the level of anxiety and depression of university students living in Jordan in relation to the learning process changes that happened post the COVID-19 pandemic.
Methods
Study Design and Participants
The study objectives were addressed through an observational cross-sectional study design. Data collection took place from the 29th of June to the 12th of September 2022, in which an open survey was open for every visitor of the site. The electronic survey was created and distributed using the Google Forms platform. The target population were tertiary education students in Amman, Jordan. A convenience sample of students were involved in the study. The initial contact with the potential participants was through email while allowing web-based data entry and CHERRIES guidelines.27 The survey was posted on the website. Content of the website was not prepared to preselect the respondents or influence the results. Respondents were able to review and change their answers through a back button. The timeframe that was used as a cut-off point was given and described why.
To be eligible, students had to be residing in Jordan, over the age of 18, and enrolled in a Jordanian university, including both private and public universities. Potential participants were informed that their participation is entirely voluntary and do not pose any risk to them. The study aim was clarified in the introduction of the survey, and students were requested to approve an electronic informed consent before filling out the study survey. A statement of survey anonymity, voluntary participation, and the right to submit their response whenever they wished were all included in the electronic informed consent. No names, personal information, or other identifiers of the participants were gathered, in order to preserve the respondents’ anonymity. In addition, purpose of the study, length of the survey (five minutes) was stated, and the fact that data provided would be stored in a password protected computer that is only accessed by the primary researcher for the purpose of analysis were all stated up front before the student proceeded to complete the online survey.
Survey Development
The first version of the survey was developed after an extensive review of the literature, and was created using the general principles of good survey design.28 The survey consisted of 30 closed-ended items, with pre-defined answers (16 demographic items and 14 items related to Hospital Anxiety and Depression Scale). To ensure the content and face validity of the survey, the first draft was assessed by five independent academic researchers and experts in the field. Where appropriate, the provided comments on the relevance of each item, the clarity of the word, and reading comprehension were incorporated.
After editing the survey according to the provided feedback, it was pilot tested on a convenience sample of 50 students in order to guarantee the readability and clearness of the questions, as well as its applicability to the students enrolled in Jordanian universities. Moreover, it was confirmed by the students that the survey is free from difficult terminology and medical jargon. The survey was also tested for usability and technical functionality of the electronic questionnaire. The pilot-phase results were not included in the study analysis.
The final version of the survey consisted of two main sections. In the first section, participants’ demographic data were collected, while the second section students’ anxiety and depression data were collected through the validated published Hospital Anxiety and Depression Scale (HADS).29,30
This online survey reported outcomes according to the CHERRIES statement which provides readers a better understanding of the sample, with regard to participants’ self-selection and its possible differences from a “representative” sample and multiple entries from the same person.
The Hospital Anxiety and Depression Scale (HADS)
The HADS is a well-validated, reliable, and published 14-item instrument designed to assess respondents’ anxiety (7-item) and depression (7-item). The HADS was devised by Zigmond and Snaith (1983), it is divided into two 7-item subscales.29 Each item had four possible score options ranging from zero to three; where a higher score indicates higher anxiety or depression scores, ie, higher severity of symptoms. The score of the questionnaire ranges between 0 and 21, with 0–7 indicating a “normal” case, 8–10 indicating “borderline abnormal” case, and 11–21 indicating “abnormal” case.
The overall Cronbach alpha measures of internal consistency were 0.7836 and 0.8760 for anxiety and depression, respectively. Spearman rank correlations of all items of the scale were significantly above zero.30
Survey Implementation
The survey link was distributed through several platforms (eg, Facebook and WhatsApp) or by sending e-mails outlining the purpose of the study. Potential participants were able to open a link in order to view the study’s ethical review board-approved information. Despite being created in English originally; the survey was given to the students in Arabic (the formal language in Jordan). The translated previously published questionnaire was used.30 In addition, two independent researchers who were considered fluent in both languages back-translated the survey from English to Arabic to confirm accuracy for the Jordanian population.30 The research team designed the survey to be completed in approximately five minutes.
Ethical Approval
The Applied Science Private University Ethics Committee provided the ethical approval (study approval number: 2022-PHA-15) of the study. In addition, The World Medical Association’s Declaration of Helsinki guideline was followed in the study design.
Sample Size
The sample size was calculated using the Epi Info software, with a 95% confidence level, 50% expected frequency, 5% acceptable margin of error, and a design effect of 1.0, the study required a minimum of 384 participants to be representative of the population.
Statistical Analysis
Participant responses were coded and entered into a customized database using the Statistical Package for the Social Sciences (SPSS), Version 24.0 (IBM Corp., Armonk, New York, USA). The qualitative variables were presented as frequency and percentages, while continuous variables were presented as mean (standard deviation). In order to determine the factors that influence students’ anxiety and depression scores (dependent variable), simple linear regression, followed by multiple regression was performed. Using univariate linear regression analysis, variables that had a p-value of less than 0.25 were added to the multiple linear regression. After checking that the variables are independent, those with a tolerance value >0.1 and variance inflation factor value of 5 or more were chosen to guarantee the absence of multicollinearity between the independent variables. In the multiple linear regression, a variable that has a p-value of 0.052 or less was considered statistically significant. Both complete and partially completed questionnaires were analyzed.
Results
The mean age of the students was 21.02 (SD = 3.616), with 60.2% being females (n = 747). More than three-quarters of the students were living in Amman (n = 979). The majority were single (n = 1178), non-smokers (n = 938), had no chronic disease/s (n = 1172), and did not use any medication/s (n = 1120). About 23.0% consumed two cups or more of coffee (with caffeine) each day. Only 17.5% (n = 217) reported having a family member diagnosed previously with anxiety or depression. More than 60.0% of the students were studying in a private university, and 70.8% (n = 879) were in their 1st, 2nd, or 3rd academic year (Table 1).
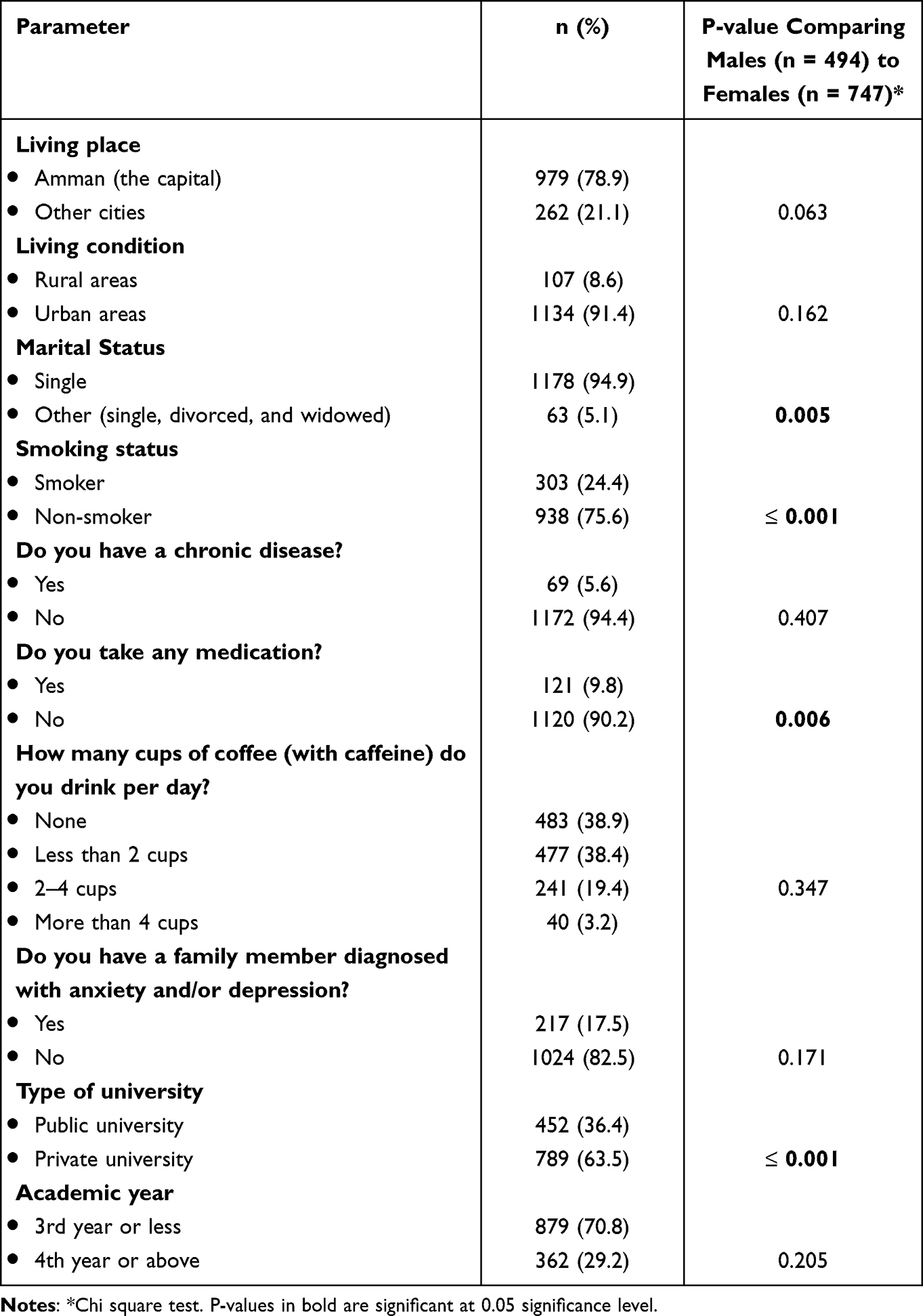 |
Table 1 Demographic Characteristics of the Study Participants (n = 1241) |
Results found that significantly more females were studying in public universities (40.8%, n = 301) than males (30.2%, n = 149), and a higher proportion were married (4.9%, n = 36) than males (1.8%, n = 9). As for the smoking status, surprisingly, significantly more females (87.0%, n = 641) reported to be smoking than males (58.0%, n = 286) and more females were taking medications (11.7%, n = 86 vs 6.9%, n = 34).
Assessing students’ anxiety revealed that 22.7% of the students (n = 282) felt tense or wound up “most of the time” (Table 2). About 19.0% (n = 239) reported getting a sort of frightened feeling as something awful was about to happen “very definitely and quite badly”. As for worrying thoughts going through the student’s mind, 28.3% of the students (n = 351) responded with yes during “a great deal of the time”. Only 34.9% of the students (n = 434) responded with “definitely” with regards to sitting at ease and feeling relaxed. Regarding getting a sort of frightened feeling like “butterflies” in the stomach, 17.3% of the students (n = 214) answered with “not at all”, and about 22.0% reported feeling restless (ie, n = 267) answered with “very much indeed”. Only 10.9% of the students (n = 135) reported getting sudden feeling of panic (they answered with “very often indeed”). Significant differences were noted in the following three anxiety questionnaire items; item 4 “I can sit at ease and feel relaxed” (p-value= 0.042) where less males answered with “not at all” and “not often” (2.8% and 19.1%) compared to females (3.5% and 18.0%). As for item 6, “I feel restless as I have to be on the move” (p-value ≥0.001), less males answered with “very much indeed” and “quite a lot” (15.4% and 28.2%) compared to females (25.5% and 34.9%). With regard to item 7, “I get sudden feelings of panic” (p-value ≥0.001), less males answered with “very often indeed” and “quite often” (8.1% and 17.6%) compared to females (12.8% and 23.9%); answers to the previous three items indicate that females felt significantly more anxious than males (Table 2).
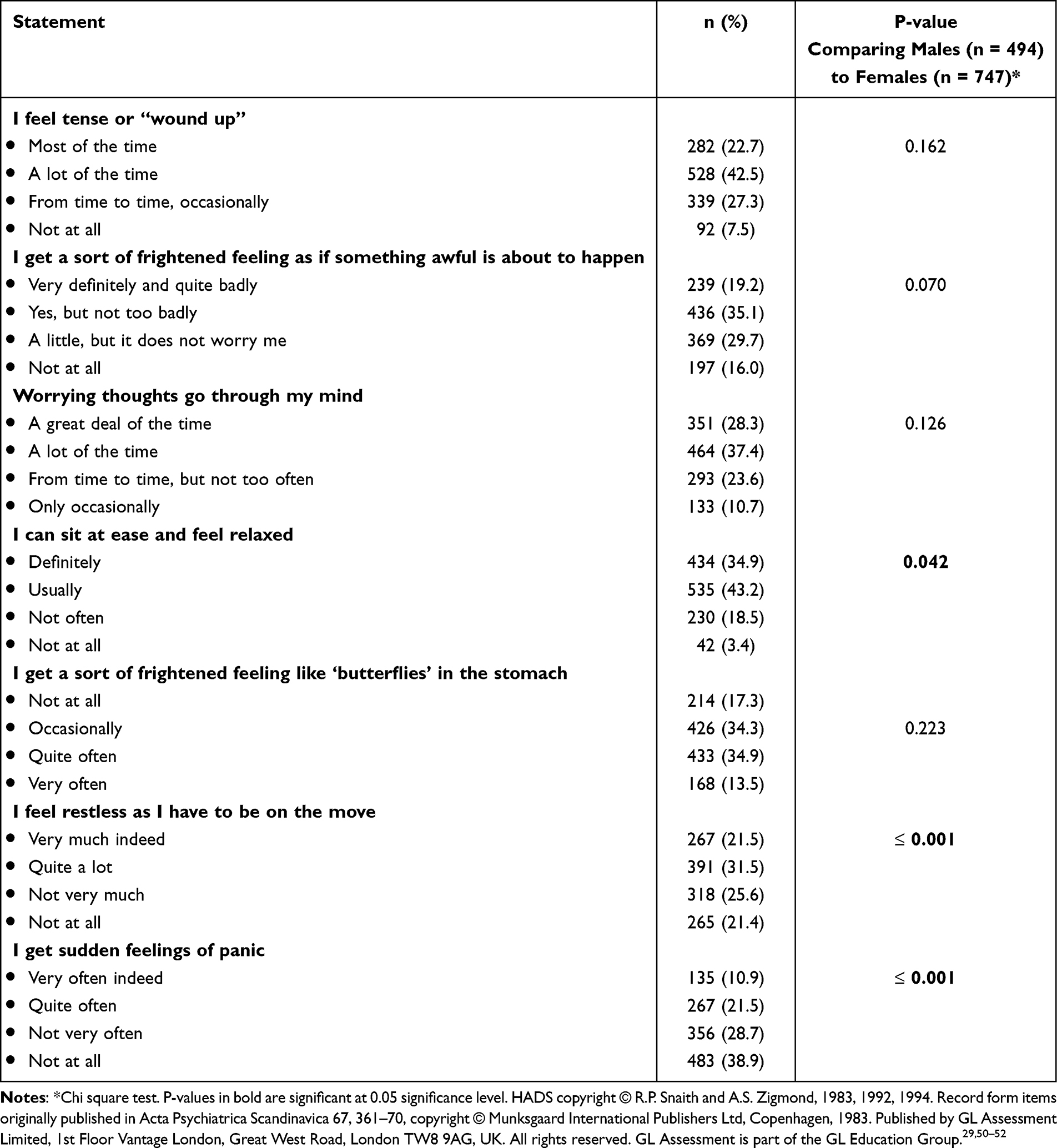 |
Table 2 Assessment of Students’ Anxiety (n = 1241) Using the Hospital Anxiety and Depression Scale (HADS) |
Assessing students’ depression score (Table 3) showed that 34.6% of the students still enjoyed the things they used to enjoy previously (ie, n = 429 answered with “definitely as much”). More than half of the students (52.9%, n = 657) answered with “as much as I always could” when asked whether they can laugh and see the funny side of things. Only 3.6% of the students (n = 45) reported “not at all” regarding feeling cheerful. More than one-third of the students (37.5%, n = 465) responded with “nearly all the time” when asked whether they felt as if they were slowed down. In terms of losing interest in appearance, 12.7% of the students (n = 157) responded with “definitely” yes. Concerning looking forward with enjoyment to things, 31.7% of the students (n = 393) answered “as much as I ever did”. Many of the students (40.7%, n = 505) reported that they can enjoy a good book or radio or TV program “often”.
 |
Table 3 Assessment of Students’ Depression (n = 1241) Using the Hospital Anxiety and Depression Scale (HADS) |
In the depression questionnaire items, significant differences were noted between both genders in all of the 7 items, as more males gave responses that indicated higher depressive feelings. This was mostly apparent for item 1 “I still enjoy the things I used to enjoy”, as more males answered with “hardly at all” and “only a little” compared to females (males: 8.1% and 22.5% vs females: 6.6% and 20.6%). The case was similar for the rest of the items (Table 3).
With regard to the anxiety scores interpretations obtained from the HADS, as shown in Figure 1, 27.3% of the students (n = 339) had a “normal” anxiety score (score = 0–7), whereas 26.9% (n = 334) had “borderline abnormal” anxiety score (score = 8–10), and 45.8% (n = 568) had “abnormal” anxiety score (score = 11–21). On the other hand, with regard to the depression scores interpretations obtained from the HADS, 52.4% of the students (n = 650) had a “normal” depression score (score = 0–7), whereas 23.6% (n = 293) had “borderline abnormal” depression score (score = 8–10), and 24.0% (n = 298) had “abnormal” depression score (score = 11–21).
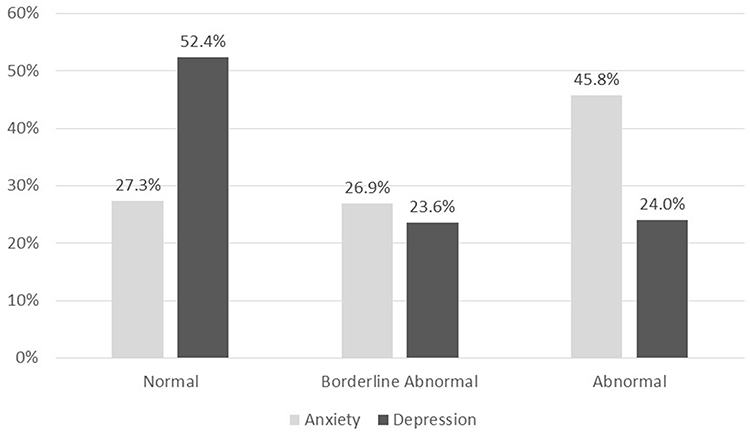 |
Figure 1 Interpretation of students’ (n = 1241) proportions of those with normal vs borderline abnormal vs abnormal symptoms using the Hospital Anxiety and Depression Scale (HADS). |
The mean anxiety score among males (n = 494) was 9.68 (SD = 4.10), and 31.3% (n = 155) of the participants had a “normal” anxiety score, whereas 26.6% (n = 131) had “borderline abnormal” anxiety score, and 42.1% (n = 208) had “abnormal” anxiety score. On the other hand, females (n = 747) had a mean anxiety score of 10.46 (SD = 4.14). Yet, 24.5% (n = 183) of the participants had a “normal” anxiety score, and 27.2% (n = 203) had “borderline abnormal” anxiety score, and 48.4% (n = 361) had “abnormal anxiety” score (Figure 2).
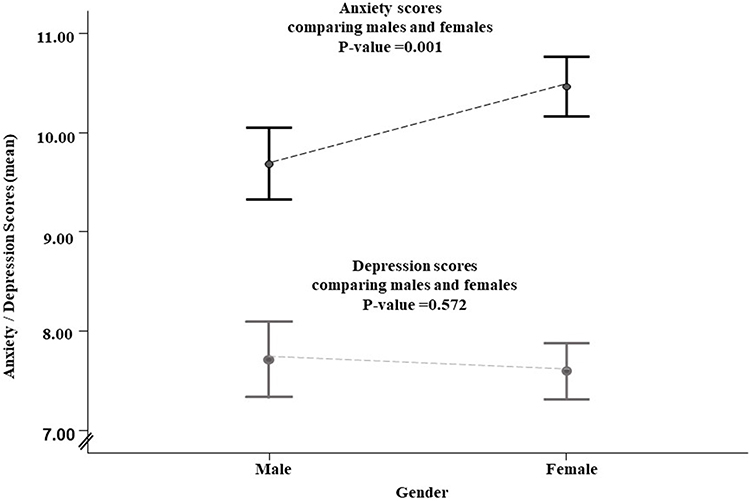 |
Figure 2 Comparing the anxiety and depression mean scores of male (n = 494, 39.8%) and female (n= 747, 60.2%) participant students. |
The mean depression score among males (n = 494) was 7.77 (SD = 4.31), while 52.8% (n = 261) of the participants had a “normal” depression score, 21.1% (n = 104) had “borderline abnormal” depression score, and 26.0% (n = 129) had “abnormal” depression score. As for females (n = 747), the mean depression score was 7.64 (SD = 4.14), 52.2% (n = 390) of the participants had a “normal” depression score, whereas 25.3% (n = 189) had “borderline abnormal” depression score, and 22.6% (n = 168) had “abnormal” depression score (Figure 2). Multiple linear regression analysis of factors affecting anxiety scores among students (Table 4) revealed that being younger (Beta = −0.014, P-value= 0.036), being a female (Beta = 0.116, P-value= 0.017), taking medication/s (Beta = 0.222, P-value= 0.006), or drinking two cups of coffee with caffeine or more a day (Beta = 0.111, P-value= 0.049) is significantly associated with having a higher anxiety score. Multiple linear regression analysis of factors affecting depression scores among students (Table 5) revealed that being younger (Beta = −0.013, P-value= 0.038), being a non-smoker (Beta = −0.123, P-value= 0.025), taking medication/s (Beta = 0.267, P-value= 0.002), drinking two cups of coffee with caffeine or more (Beta = 0.188, P-value= 0.001), or having a family member diagnosed with anxiety or depression (Beta = 0.316, P-value= ≤ 0.001) is significantly associated with having a depression score indicating depressive symptoms.
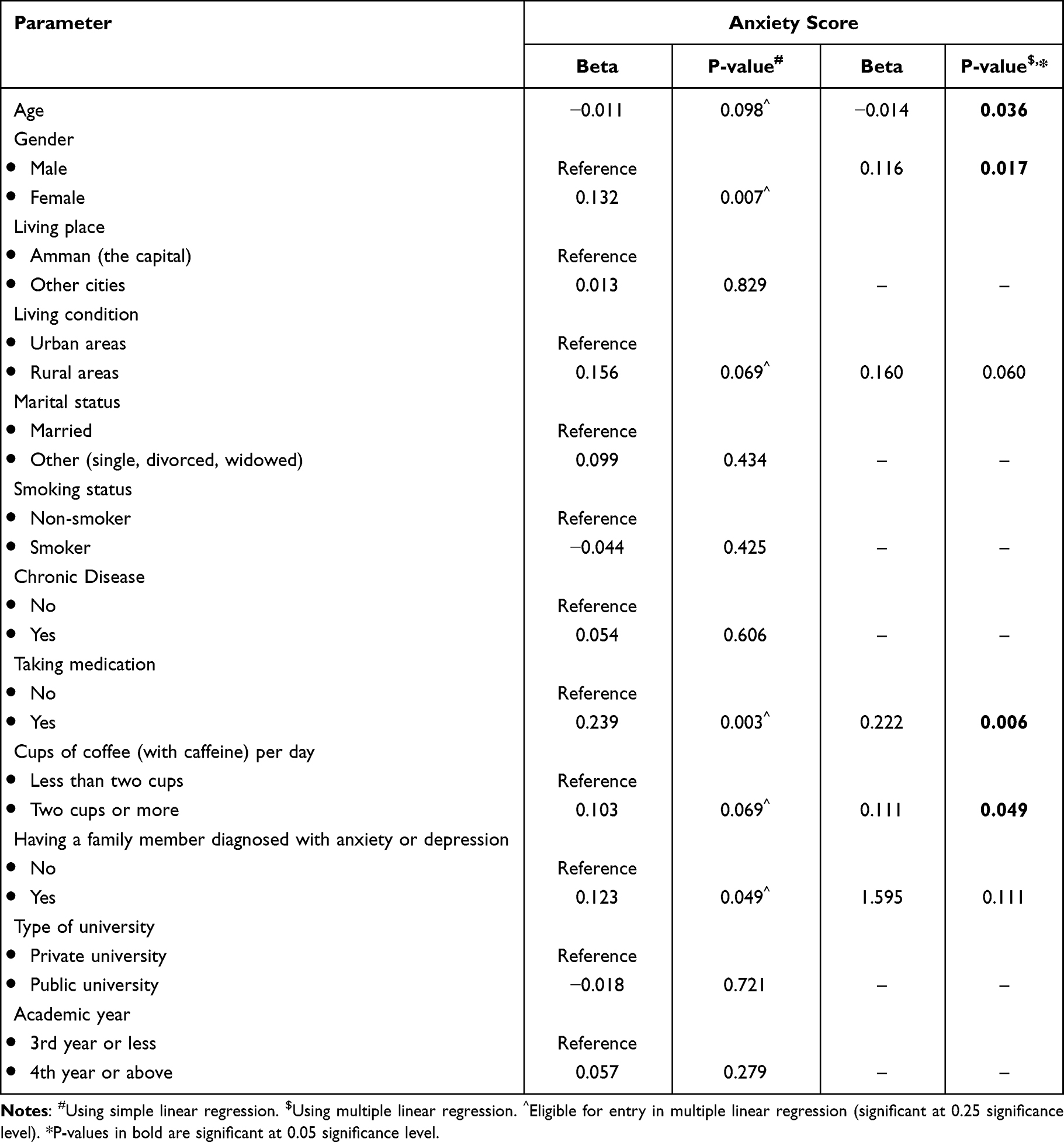 |
Table 4 Assessment of Factors Affecting Anxiety Scores Among the Study Participants (n = 1241) |
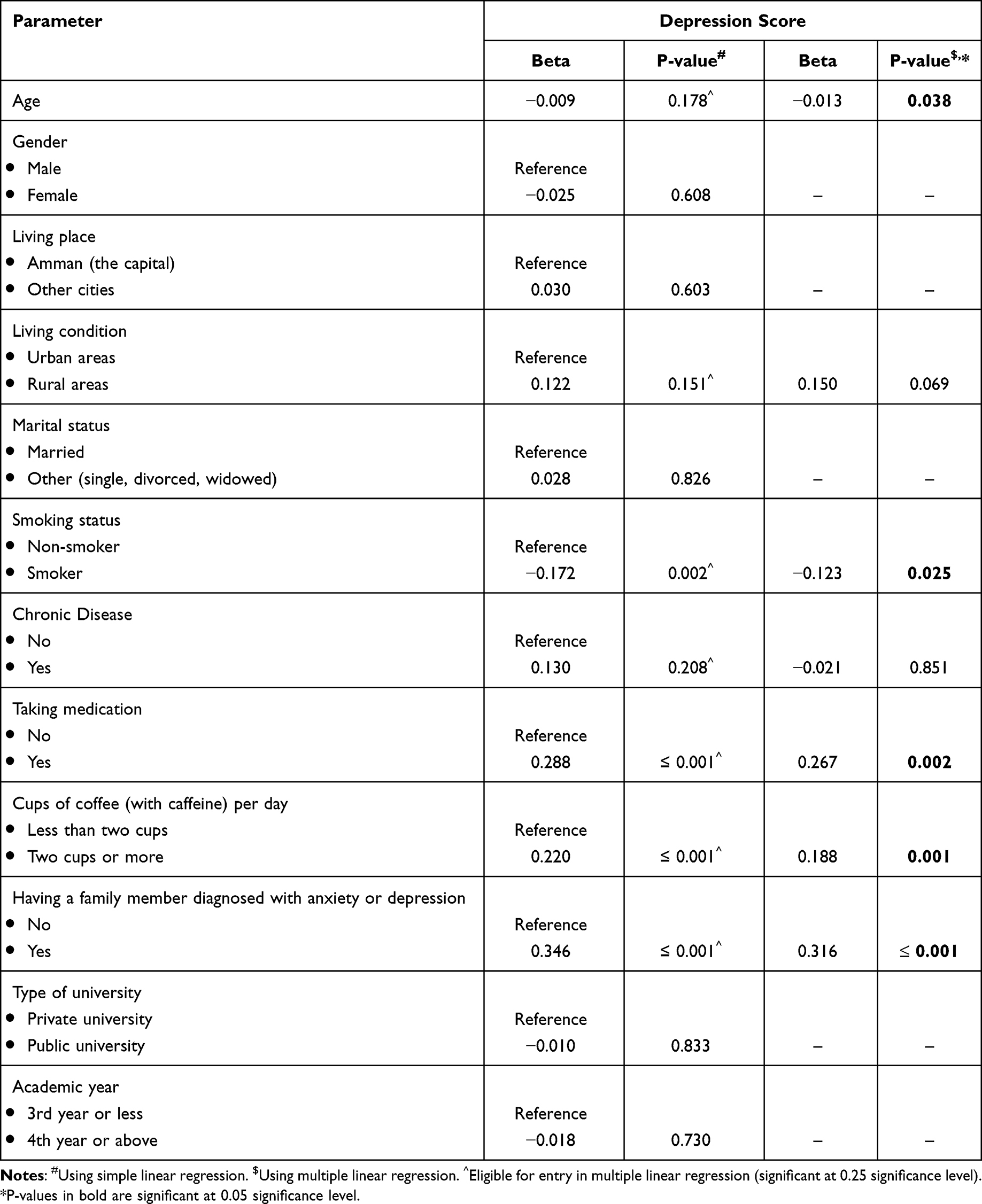 |
Table 5 Assessment of Factors Affecting Depression Scores Among the Study Participants (n = 1241) |
Discussion
The stability of families and individuals was impacted throughout the current global crisis and pandemic,31 which is a key issue that might significantly affect students’ anxiety and depression levels. This is the first study to report the degree of anxiety and depression experienced by university students in Jordan post the COVID-19 pandemic, and its effects on their education. Borderline anxiety and depression levels were found to affect 26.9% and 23.6% of students, and abnormal anxiety and depression affected 45.8% and 24.0% of students. Such high rates were surprising and knowing the associated factors can help target certain vulnerable groups in the future. Higher levels of anxiety and depression were significantly associated with younger ages, medication use, consuming two or more cups of caffeinated coffee a day and having a family history of anxiety or depression.
This study used the HADS assessment to determine the levels of anxiety and depression amongst students during the pandemic. The HADS questionnaire is the most suitable tool for the bi-dimensional assessment of anxiety and depression symptoms among the study participants due to its validity, reliability, and availability, as it has been published in many countries.32 Additionally, because it only has 14 questions, 7 of which are related to anxiety symptoms and 7 to depressive symptoms- The questionnaire can be completed online in a short time. Since each item on the questionnaire is graded from 0 to 3, this tool offers an anxiety score and a depression score, as the scores vary from 0 to 21.32
The pandemic had an impact on the psychological states of university students all around the world.33 Similar to the findings of this study, a recent study assessing the psychological impact of COVID-19 on university students in Saudi Arabia reported that 38.6% of participants showed anxiety symptoms, while 33.1% showed depression symptoms.34 According to reports, in addition to social and financial losses, the lack of resources, forced social and physical distance, and self-quarantining contributed to students’ emotional discomfort.11,12 The pandemic’s high rates of financial instability and resource (food and housing) insecurity increased college students’ psychological distress, such as anxiety and depression.35 Also, a study performed by Hamaideh et al on Jordanian students during COVID-19 “home-quarantine” found that the prevalence of anxiety and depression was 67.9% and 78.7%.36
The transition from face-to-face learning to online learning becoming a common modality of education meant more social isolation, prolonged screen time, affected studies, worries about future employment, all factors leading to increased stress, burnout, anxiety and depression levels.37,38 A study conducted on online learning students in Brazil showed that most students reported emotional impact in online learning, followed by learning impact, financial impact, social impact and technological impact.39 Another study, conducted via an online survey among 5100 medical students engaged in online learning from Wannan Medical College in China showed the prevalence of anxiety and stress to be as high as 32.9% and 14.6%, respectively.40 Another study included 1210 respondents from 194 cities in China found that 53.8% of respondents rated the psychological impact of the pandemic as moderate or severe; 16.5% reported moderate to severe depressive symptoms while 28.8% reported moderate to severe anxiety symptoms.41 A recent meta-analysis conducted by Ebrahim et al on a total of 46,284 cases showed an overall pooled prevalence rate of 29.1% for anxiety symptoms and 23.2% for depression symptoms showing significant impact on university students’ psychological well-being.42 A previous study conducted in North India involving nursing students also found significant associations between stress levels and students being in the first-year academic level, as well as students having family members in the medical profession.26 Hence, it is apparent that the pandemic has increased the rates and level of anxiety and depression amongst students, and that moving forward to online learning may have an association with such increase.
A cross-sectional study was conducted during the COVID-19 pandemic (July 2020) to assess anxiety and depression levels among Jordanian medical students. From the study participants (n = 450), 43.8% had a “normal” anxiety score, and 40.0% had a “normal” depression score. The current study’s findings reported a lower level of “normal” anxiety (27.3% vs 43.8%), but a higher level of “normal” depression scores (52.4% vs 40.0%). In addition, comparing the level of “abnormal” anxiety and “abnormal” depression scores, the current study reported a higher level of “abnormal” anxiety score (45.8% vs 33.8%), and a lower level of “abnormal” depression score (24.0% vs 26.2%).43
Family history of anxiety or depression and being of a female gender are important when it comes to assessing the liability of individuals to develop the condition.36,44 In this study, results showed that higher depression scores were associated with a family history. This finding was in concordance with studies that demonstrated that anxiety and depression have genetic ties.45,46 Females were also found to be at higher risk of anxiety. This finding is in accordance with those of previous studies that demonstrated that females were more likely to develop mood disorders and stress-related mental illnesses including depression and anxiety.47 This sex difference in developing mental diseases is likely due to genetics and sex steroid hormones.44
Although this study provides valuable information about depression and anxiety, and the way changes in the learning process following the pandemic affected such psychological symptoms of students, the study was composed only by self-reported questionnaires that are not deepened with clinical and instrumental examinations. Secondly, there may be a selection bias because the respondents self-selected to respond to the survey; yet, since a large sample size of participants completed the questionnaire, this helped to mitigate the effect of this bias. Also, the results may not accurately reflect the intensity of anxiety and depression symptoms among students because the research approach followed was unable to reach participants with medically examined anxiety and depression symptoms. Another limitation of this study is not using the tools designed specifically for the COVID-19 pandemic, such as the coronavirus anxiety scale (CAS),48 yet, the HADS assessment scale is an accurate tool to use and was suitable to answer the objectives of this study. Meanwhile, it could be useful to undertake a prospective study on the same individuals using tools designed specifically for the COVID-19 pandemic to provide a tangible result and support the need for a targeted public health strategy. Finally, the study did not assess for the participation rate (unique number of people who filled in the first page of the survey (or agreed to participate by checking a checkbox) divided by visitors who visited the first page of the survey) nor for the completion rate (number of people submitting the last questionnaire page divided by the number of people who agreed to participate (or submitted the first survey page)). Measures to prevent multiple entries from the same individual were not applied such as the use of cookies which prevents the users from entering the survey twice, or use of IP check where no two entries from the same IP address is allowed.
Conclusion
In conclusion, this research shows how crucial it is for organizations and decision-makers to assess the mental health status of tertiary education students, and how changes in the educational process following the pandemic have affected such status. This study has shown that 26.9% of university students in Jordan had “borderline abnormal” anxiety score, and 45.8% had “abnormal” anxiety score. Results were also alarming for depression scores, as 23.6% had “borderline abnormal” depression score, and 24.0% had “abnormal” depression score.
Factors affecting anxiety scores among students included younger age, being a female, taking medication/s, or drinking two cups of coffee or more a day. As for depression, such factors included younger age, being a non-smoker, taking medication/s, drinking two cups of coffee, or having a family member diagnosed with anxiety/depression. Unveiling such factors can help policy makers target the groups affected most by anxiety and depression symptoms, devising plans to help the students who have fell victims to such mental problems following the pandemic and the resultant changes that took place in the educational system.
Receiving sufficient training on pandemics can play a vital role in improving self-efficacy and reducing anxiety which would eventually prepare educators and students to face future pandemics in a much better and more efficient manner.9,47,49 Higher education institutions are well-positioned to offer training and support to educators and students. Students in need of mental health support can also benefit from comprehensive care offered by the University Psychology Clinic during their higher education study years, helping them overcome the new challenges and the post trauma of the pandemic. Referral of students in need of further mental help to more specialized health-care facilities is also vital. Tertiary education institutions can build bridges with other institutions in the country to react to the encounters of recent times as the globe continues to struggle with the far-reaching effects of the deviations faced following COVID-19 pandemic.
Data Sharing Statement
Data are available upon request from the corresponding author.
Funding
This research was funded by the Deanship of Research and Higher Studies of the involved universities, grant number [DRG‐2021‐2022‐16], Applied Science Private University (ASU), the University of Jordan (UJ), the Hashemite University (HU), and Princess Sumaya University for Technology (PSUT).
Disclosure
Authors declare no conflict of interest.
References
1. Sharma A, Tiwari S, Deb MK, Marty JL. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2): a global pandemic and treatment strategies. Int J Antimicrob Agents. 2020;56(2):106054. doi:10.1016/j.ijantimicag.2020.106054
2. Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020;8(5):475–481. doi:10.1016/S2213-2600(20)30079-5
3. Listings of WHO’s response to COVID-19. Available from: https://www.who.int/news-room/detail/29-06-2020-covidtimeline.
4. Worldometer - real time world statistics. Available from: https://www.worldometers.info/.
5. Fajnzylber J, Regan J, Coxen K, et al. SARS-CoV-2 viral load is associated with increased disease severity and mortality. Nat Commun. 2020;11(1):1–9. doi:10.1038/s41467-020-19057-5
6. Huang YZ, Kuan CC. Vaccination to reduce severe COVID-19 and mortality in COVID-19 patients: a systematic review and meta-analysis. Eur Rev Med Pharmacol Sci. 2022;26(5):1770–1776. doi:10.26355/eurrev_202203_28248
7. Ayouni I, Maatoug J, Dhouib W, et al. Effective public health measures to mitigate the spread of COVID-19: a systematic review. BMC Public Health. 2021;21(1):1–14. doi:10.1186/s12889-021-11111-1
8. Day T, Park A, Madras N, Gumel A, Wu J. When is quarantine a useful control strategy for emerging infectious diseases? Am J Epidemiol. 2006;163(5):479–485. doi:10.1093/aje/kwj056
9. Kumar R, Singh V, Mohanty A, Bahurupi Y, Gupta PK. Corona health‑care warriors in India: knowledge, attitude, and practices during COVID-19 outbreak. J Educ Health Promot. 2023;12(February). doi:10.4103/jehp.jehp_419_22
10. Basheti IA, Nassar R, Barakat M, et al. Pharmacists’ readiness to deal with the coronavirus pandemic: assessing awareness and perception of roles. Res Soc Adm Pharm. 2021;17(3):514–522. doi:10.1016/j.sapharm.2020.04.020
11. Brooks SK, Webster RK, Smith LE, et al. The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet. 2020;395(10227):912–920. doi:10.1016/S0140-6736(20)30460-8
12. Duan L, Zhu G. Psychological interventions for people affected by the COVID-19 epidemic. Lancet Psychiatry. 2020;7(4):300–302. doi:10.1016/S2215-0366(20)30073-0
13. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
14. Holmes EA, O’Connor RC, Perry VH, et al. Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science. Lancet Psychiatry. 2020;7(6):547–560. doi:10.1016/S2215-0366(20)30168-1
15. Salari N, Hosseinian-Far A, Jalali R, et al. Prevalence of stress, anxiety, depression among the general population during the COVID-19 pandemic: a systematic review and meta-analysis. Global Health. 2020;16(1):1–11.
16. Fancourt D, Steptoe A, Bu F. Trajectories of anxiety and depressive symptoms during enforced isolation due to COVID-19 in England: a longitudinal observational study. Lancet Psychiatry. 2021;8(2):141–149. doi:10.1016/S2215-0366(20)30482-X
17. Santomauro DF, Mantilla Herrera AM, Shadid J, et al. Global prevalence and burden of depressive and anxiety disorders in 204 countries and territories in 2020 due to the COVID-19 pandemic. Lancet. 2021;398(10312):1700–1712. doi:10.1016/S0140-6736(21)02143-7
18. Xiong J, Lipsitz O, Nasri F, et al. Impact of COVID-19 pandemic on mental health in the general population: a systematic review. J Affect Disord. 2020;277:55–64. doi:10.1016/j.jad.2020.08.001
19. Passavanti M, Argentieri A, Barbieri DM, et al. The psychological impact of COVID-19 and restrictive measures in the world. J Affect Disord. 2021;283:36–51. doi:10.1016/j.jad.2021.01.020
20. Basheti IA, Nassar RI, Halalşah İ. The impact of the coronavirus pandemic on the learning process among students: a comparison between Jordan and Turkey. Educ Sci. 2022;12(5):365. doi:10.3390/educsci12050365
21. Kumar R, Beniwal K, Bahurupi Y. Pandemic fatigue in nursing undergraduates: role of individual resilience and coping styles in health promotion. Front Psychol. 2022;13(August). doi:10.3389/fpsyg.2022.940544
22. Son C, Hegde S, Smith A, Wang X, Sasangohar F. Effects of COVID-19 on college students’ mental health in the United States: interview survey study. J Med Internet Res. 2020;22(9):e21279. doi:10.2196/21279
23. Kecojevic A, Basch CH, Sullivan M, Davi NK, Vickers K. The impact of the COVID-19 epidemic on mental health of undergraduate students in New Jersey, cross-sectional study. PLoS One. 2020;15(9):e0239696. doi:10.1371/journal.pone.0239696
24. Sun Y, Lin SY, Chung KKH. University students’ perceived peer support and experienced depressive symptoms during the COVID-19 pandemic: the mediating role of emotional well-being. Int J Environ Res Public Health. 2020;17(24):1–13. doi:10.3390/ijerph17249308
25. Wu X, Tao S, Zhang Y, et al. Geographic distribution of mental health problems among Chinese college students during the COVID-19 pandemic: nationwide, web-based survey study. J Med Internet Res. 2021;23(1):e23126. doi:10.2196/23126
26. Sharma A, Kumar R. Psychological distress and coping styles among baccalaureate nursing students: promoting mental health of future nurses in COVID-19 pandemic. J Educ Health Promot. 2023;11:331.
27. Turk T, Elhady MT, Rashed S, et al. Quality of reporting web-based and non-web-based survey studies: what authors, reviewers and consumers should consider. PLoS One. 2018;13(6):1–15. doi:10.1371/journal.pone.0194239
28. Boynton PM, Greenhalgh T. Selecting, designing, and developing your questionnaire. BMJ. 2004;328(7451):1312–1315. doi:10.1136/bmj.328.7451.1312
29. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
30. El-Rufaie OEF, Absood GH. Retesting the validity of the Arabic version of the Hospital Anxiety and Depression (HAD) scale in primary health care. Soc Psychiatry Psychiatr Epidemiol. 1995;30(1):26–31. doi:10.1007/BF00784431
31. Araújo FJDO, De lima LSA, Cidade PIM, Nobre CB, Neto MLR. Impact of Sars-Cov-2 and its reverberation in global higher education and mental health. Psychiatry Res. 2020;288:112977. doi:10.1016/j.psychres.2020.112977
32. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the hospital anxiety and depression scale: an updated literature review. J Psychosom Res. 2002;52(2):69–77. doi:10.1016/S0022-3999(01)00296-3
33. Basheti IA, Assaraira TY, Obeidat NM, Al-abed Al-haq F, Refari M. Assessing learning preferences of tertiary education students in Jordan post COVID-19 pandemic and the associated perceived stress. Educ Sci. 2022;12(11):829. doi:10.3390/educsci12110829
34. Alkahtani RF, Alomar AA, Alkanhal AF, et al. Prevalence of anxiety, depression, and sleep disturbances associated with the COVID-19 outbreak in Riyadh, Saudi Arabia. Cureus. 2022;14(5):1.
35. Jones HE, Manze M, Ngo V, Lamberson P, Freudenberg N. The impact of the COVID-19 pandemic on college students’ health and financial stability in New York City: findings from a Population-based sample of City University of New York (CUNY) students. J Urban Health. 2021;98(2):187–196. doi:10.1007/s11524-020-00506-x
36. Hamaideh SH, Al-Modallal H, Tanash M, Hamdan-Mansour A. Depression, anxiety and stress among undergraduate students during COVID-19 outbreak and “home-quarantine.”. Nurs Open. 2022;9(2):1423–1431. doi:10.1002/nop2.918
37. Mheidly N, Fares MY, Fares J. Coping with stress and burnout associated with telecommunication and online learning. Front Public Health. 2020;8. doi:10.3389/fpubh.2020.574969
38. Višnjić A, Veličković V, Sokolović D, et al. Relationship between the manner of mobile phone use and depression, anxiety, and stress in university students. Int J Environ Res Public Health. 2018;15(4):697. doi:10.3390/ijerph15040697
39. Pelucio L, Simões P, Dourado MCN, Quagliato LA, Nardi AE. Depression and anxiety among online learning students during the COVID-19 pandemic: a cross-sectional survey in Rio de Janeiro, Brazil. BMC Psychol. 2022;10(1). doi:10.1186/s40359-022-00897-3
40. Chang WW, Shi LX, Zhang L, Jin YL, Yu JG. The mental health status and associated factors among medical students engaged in online learning at home during the pandemic: a cross-sectional study from China. Front Psychiatry. 2021;12. doi:10.3389/fpsyt.2021.755503
41. Wang C, Pan R, Wan X, et al. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int J Environ Res Public Health. 2020;17(5):1.
42. Ebrahim AH, Dhahi A, Husain MA, Jahrami H. The psychological well-being of university students amidst COVID-19 pandemic: scoping review, systematic review and meta-analysis. Sultan Qaboos Univ Med J. 2022;22(2):179–197. doi:10.18295/squmj.6.2021.081
43. Basheti IA, Mhaidat QN, Mhaidat HN, Saqr M. Prevalence of anxiety and depression during COVID-19 pandemic among healthcare students in Jordan and its effect on their learning process: a national survey. PLoS One. 2021;16(4):e0249716. doi:10.1371/journal.pone.0249716
44. Songtachalert T, Roomruangwong C, Carvalho AF, Bourin M, Maes M. Anxiety disorders: sex differences in serotonin and tryptophan metabolism. Curr Top Med Chem. 2018;18(19):1704–1715. doi:10.2174/1568026618666181115093136
45. Hettema JM, Neale MC, Kendler KS. A review and meta-analysis of the genetic epidemiology of anxiety disorders. Am J Psychiatry. 2001;158(10):1568–1578. doi:10.1176/appi.ajp.158.10.1568
46. Sullivan PF, Neale MC, Kendler KS. Genetic epidemiology of major depression: review and meta-analysis. Am J Psychiatry. 2000;157(10):1552–1562. doi:10.1176/appi.ajp.157.10.1552
47. McLean CP, Asnaani A, Litz BT, Hofmann SG. Gender differences in anxiety disorders: prevalence, course of illness, comorbidity and burden of illness. J Psychiatr Res. 2011;45(8):1027–1035. doi:10.1016/j.jpsychires.2011.03.006
48. Silva WAD, de Sampaio Brito TR, Pereira CR. COVID-19 anxiety scale (CAS): development and psychometric properties. Curr Psychol. 2022;41(8):5693. doi:10.1007/s12144-020-01195-0
49. Dharra S, Kumar R. Promoting mental health of nurses during the coronavirus pandemic: will the rapid deployment of nurses’ training programs during COVID-19 Improve Self-Efficacy And Reduce Anxiety? Cureus. 2021;13:5.
50. Snaith RP. The Hospital Anxiety and Depression Scale. Health Qual Life Outcomes. 2003;1(1):29. doi:10.1186/1477-7525-1-29
51. White D, Leach C, Sims R, Atkinson M, Cottrell D. Validation of the hospital anxiety and depression scale for use with adolescents. Br J Psychiatry. 1999;175(5):452–454. doi:10.1192/bjp.175.5.452
52. Herrmann C. International experiences with the hospital anxiety and depression scale-a review of validation data and clinical results. J Psychosom Res. 1997;42(1):17–41. doi:10.1016/S0022-3999(96)00216-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Digital Therapy: Alleviating Anxiety and Depression in Adolescent Students During COVID-19 Online Learning - A Scoping Review
Yosep I, Suryani S, Mediani HS, Mardhiyah A, Maulana I
Journal of Multidisciplinary Healthcare 2023, 16:1705-1719
Published Date: 21 June 2023
Depression Among University Students in Jordan After the COVID-19 Pandemic: A Cross-Sectional Study
Alhemedi AJ, Qasaimeh MG, Abdo N, Elsalem L, Qaadan D, Alomari E, lssa Q, Alhadeethi M, Abdul Kareem HM, Almasri A, Elkhateeb O, Naser AY
Psychology Research and Behavior Management 2023, 16:4237-4249
Published Date: 18 October 2023
AI Technology panic—is AI Dependence Bad for Mental Health? A Cross-Lagged Panel Model and the Mediating Roles of Motivations for AI Use Among Adolescents
Huang S, Lai X, Ke L, Li Y, Wang H, Zhao X, Dai X, Wang Y
Psychology Research and Behavior Management 2024, 17:1087-1102
Published Date: 12 March 2024
Impact of Anxiety and Depression on the Level of Asthma Control Among Jordanian Adults with Asthma
Abu Al Karsaneh O, Al Anber A, Al Shboul S, Alrjoub M, Almashaqbeh OI, Alqaisi M, Abuatieh R, Ananzeh SM, Hamad AM, Almomani R, Tommalieh MM
Journal of Asthma and Allergy 2024, 17:463-476
Published Date: 19 May 2024
Mushrooms, Microdosing, and Mental Illness: The Effect of Psilocybin on Neurotransmitters, Neuroinflammation, and Neuroplasticity
Kinderlehrer DA
Neuropsychiatric Disease and Treatment 2025, 21:141-155
Published Date: 29 January 2025