")
Back to Journals » Psoriasis: Targets and Therapy » Volume 12
Assessing and Improving Psychological Well-Being in Psoriasis: Considerations for the Clinician
Authors Blackstone B, Patel R, Bewley A
Received 23 November 2021
Accepted for publication 2 February 2022
Published 25 March 2022 Volume 2022:12 Pages 25—33
DOI https://doi.org/10.2147/PTT.S328447
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Uwe Wollina
Brittany Blackstone,1,* Radhika Patel,1,* Anthony Bewley2
1Bart’s Health NHS Foundation Trust, London, UK; 2Barts Health NHS Trust, Queen Mary University London, London, UK
*These authors contributed equally to this work
Correspondence: Brittany Blackstone, Department of General Internal Medicine, The Royal London Hospital, Whitechapel Road, London, E1 1FR, UK, Email [email protected]; Radhika Patel, Bart’s Health NHS Foundation Trust, London, UK, Email [email protected]
Abstract: Psoriasis is a common chronic, systemic inflammatory disease, affecting approximately 2% of the population worldwide. Psoriasis is associated with profound psychosocial comorbidity with a burden that extends well beyond the physical signs and symptoms. Psychosocial comorbidities strongly associated with psoriasis include anxiety and depression, suicidal ideation, and substance misuse. There is a substantial unmet need for access to psychological support for people with skin disease in the UK. Recent reports found that while up to 98% of patients felt that their skin disease had affected their emotional or psychological well-being, only 18% sought help. This care gap is largely due to a lack of awareness about the limited available services alongside poor recognition, diagnosis, and triaging. Addressing psychosocial support needs starts with early identification, which can be complex and challenging. Once patients who need further support are identified, outcomes can be improved through prompt and effective treatment of inflammation, cognitive behavioural therapy, meditation and mindfulness-based therapy (including motivational interviewing), and to some extent psychotropic medication. Finally, resources for mental health support are notoriously limited, with dire consequences for patients. It is imperative that a proportion of the new funding promised for mental health services is bookmarked for dermatology patients and adequate provision of multidisciplinary psychodermatology teams to best serve the needs of this population. Ultimately, psoriasis is a complex condition with multifactorial psychological and biological drivers. Psoriasis is associated with high levels of distress, which is often under-recognized. Fully addressing this condition requires a holistic approach to the physical and psychosocial aspects to maximise adherence, efficacy, and optimise patient quality of life.
Keywords: dermatology, chronic illness, psychosocial impact, mental health, stigmatization, quality of life
Introduction
Psoriasis is a common chronic, systemic inflammatory disease, affecting approximately 2% of the population worldwide, resulting in keratinocyte hyperproliferation.1 Men and women are equally affected by symptom onset occurring at any age. There are various clinical phenotypes; however, the most common presentation is chronic plaque psoriasis, which is characterised by well-demarcated, erythematous plaques covered with silvery scales. Lesions classically affect the scalp, extensor surfaces of the knees, elbows and lower back. There may also be nail involvement.
The pathogenesis of disease is complex and not fully understood. Over the past two decades, immunological studies have highlighted the key role of cytokines, particularly IL-17 and IL-23, in epidermal hyperproliferation as well as the role T helper cells type 17 (Th17), TNFα and interferons. Furthermore, genome-wide association studies have helped identify over 80 at risk loci, accounting for about 30% of disease heritability.2–4 This risk of developing psoriasis is two to three times higher in monozygotic compared with dizygotic twins. There is consensus that psoriasis expression is a consequence of genetic susceptibility combined with immunological factors and environmental triggers, such as stress, infection (often streptococcal), smoking, alcohol consumption and exposure to certain drugs. The exact mechanism between immunogenetic factors and environmental triggers is yet to be discovered.5
Due to various elevated proinflammatory interleukins, psoriasis is a multisystem disorder and is associated with several medical conditions including psoriatic arthritis, coronary heart disease, diabetes, malignancies, inflammatory bowel disease and depression.6
Psychosocial Co-Morbidities Overview
As a relapsing and remitting lifelong disease, psoriasis has a detrimental impact on the quality of life (QoL) of patients. Psychosocial comorbidities strongly associated with psoriasis include anxiety and depression, suicidal ideation and substance misuse.
A recent report published by the All-Party Parliamentary Group on Skin (APPGS) highlights the magnitude of the mental health burden skin diseases pose in the UK. Patients reported feelings of embarrassment, shame, anxiety, depression and suicidal thoughts. 93% of patients stated their skin condition affected their self-esteem.7 As a consequence of these feelings and/or perception of stigmatisation related to their appearance, many patients adopt avoidance and concealment as coping strategies leading to social isolation. Individuals struggle to form or maintain intimate relationships, withdraw from friends, family and society.
The clinical severity of psoriasis, as measured by a Psoriasis Area and Severity Index (PASI) score, has no significant correlation between QoL and daily functioning. However, patients with visible psoriatic lesions are significantly negatively impacted in terms of lower QoL scores.8
These negative psychosocial factors, in particular stigma, caused by psoriasis, paradoxically perpetuate a vicious cycle of poor adherence to treatment, thus worsening skin and mental health.9
Depression and Anxiety
Depending on the screening tool used, depression affects 9–55% of patients with psoriasis, with a higher prevalence in those with more severe disease.10 Contrastingly, the prevalence of anxiety ranges from 7% to 48% and is unrelated to disease severity.11 Several studies have concluded a significantly higher prevalence of depression and anxiety amongst psoriasis patients compared to those without psoriasis or other severe skin conditions.
Both human studies and mice models demonstrate that depression may have a systemic inflammatory component to its aetiology. Proinflammatory cytokines such as interleukin (IL)-1 and IL-6 are elevated in both psoriasis and depression, indicating that the inflammatory process may be contributing to account for these psychological comorbidities rather than being a result of the psychosocial impact of psoriasis itself.
There are various hypothesized mechanisms by which inflammatory cytokines can lead to anxiety and depression that are beyond the scope of this review.
Functional magnetic resonance imaging (MRI) brain studies in which participants are shown images of disgusted faces have demonstrated lower levels of activity in the bilateral insular cortex of psoriasis patients compared to controls.12 This area is known to be activated in response to the feeling and observation of disgust. The authors hypothesise that the lower level of activity may be the result of learned coping mechanisms, in order to protect oneself during negative social experiences. On the other hand, positron emission tomography (PET) scan studies have shown no significant difference in neuroinflammatory signals between psoriasis patients and controls, suggesting the blood–brain barrier may have a role in protecting against peripheral circulating inflammatory mediators.13
Investigating the role of biologics and new biosimilar therapies on depressive symptoms in patients with psoriasis is an emerging area of research. A systematic review of 3 randomised controlled trials showed patients with moderate-to-severe psoriasis treated with adalimumab, etanercept and ustekinumab had significantly lower depressive symptom scores.14 Similarly, both depression and anxiety significantly decreased in patients with psoriasis treated with brodalumab compared with placebo (P < 0.0001).15 However, it is difficult to distinguish whether this is a result of the direct anti-inflammatory effect of the medication or indirectly through improved psoriasis leading to improved quality of life.
Suicide
It is estimated that approximately 350 suicides per year in the UK are attributed to psoriasis.16 5% of survey respondents in the APPGS inquiry spontaneously described thoughts of suicidal ideation (n = 29), even though this was not specifically asked in the survey. One study has shown up to a 44% higher rate of suicide compared with the general population. In those with severe disease, there is reported to be a 69% greater likelihood of attempting suicide, and a 30% greater likelihood of completing suicide, despite controlling for possible confounders.
Despite several studies reporting a higher prevalence of suicidal ideation and behaviour (SIB), suicide attempts and completed suicide in patients with psoriasis the current literature base is limited. Many of these were of poor quality, and use different tools to assess mental health disorders, making comparison between studies more challenging; hence further research is warranted.17
Alcohol and Smoking Misuse
Patients with psoriasis consume more alcohol and have higher rates of alcoholism compared to the general population.18 The reason for this is complex and multifactorial; however, it is likely that many patients use alcohol as a coping mechanism to deal with the psychosocial distress related to their chronic health condition.
There is evidence demonstrating that alcohol consumption leads to increased severity of psoriasis through several pathways, such as increased susceptibility to infections, stimulation of lymphocyte and keratinocyte proliferation and production of proinflammatory cytokines.19,20 Such patients also have poor treatment compliance and often become trapped in a cycle of poor disease control, leading to lower quality of life, which further fuels alcohol and substance misuse as a coping strategy.
Smoking is twice as prevalent amongst patients with psoriasis compared to controls, with heavy smoking (more than 20 cigarettes per day) contributing to a two-fold increase in the severity of disease.21 Smoking is also a well-recognised risk factor for developing the psoriatic arthritis, a comorbidity that affects approximately 20% of patients with psoriasis. Patients with psoriasis who smoke are more likely to develop psoriatic arthritis, and at an earlier age.
A large Finnish cohort study found patients with moderate-severe psoriasis have excess mortality attributed to alcohol and to a lesser extent smoking-related.22 Patients should be encouraged to reduce their alcohol intake as it has been shown to improve skin disease, with abstinence inducing remission in some cases. Similarly, smoking cessation should be encouraged.
Access to Mental Health Services: Current Situation
There is a substantial unmet need for access to psychological support for people with skin disease in the UK. The APPGS report found 98% of survey respondents stated that their skin disease had affected their emotional or psychological well-being, however only 18% sought help.7 This care gap is largely due to a lack of awareness about the limited available services alongside poor recognition, diagnosis and triaging. Patients with skin conditions often trivialise their problems as they feel that their health condition is non-life limiting or important enough to seek medical help for. Therefore, clinicians need further training, resources and support to actively explore and evaluate the severity of psychosocial impact of skin disease.
It is well known that the COVID-19 pandemic has exacerbated the mental health crisis and limited access further. Given the increased risk of mental health disease amongst patients with psoriasis, compounded by the psychosocial impact of social distancing, self-isolating and shielding (especially those taking immunosuppressant medications), we expect to see higher rates of anxiety, depression, poor compliance with treatment and reduced physical attendance in healthcare. This in turn may lead to a vicious cycle of acute flares of the skin condition with further deterioration in mental health.23
Early identification of patients with additional psychological support needs
- Direct questioning techniques
Addressing the psychosocial and support needs in patients with psoriasis starts with early identification of the patients who need support, which can be complex and challenging. It is a common misconception that the severity of skin disease correlates with psychological difficulties, as measuring the extent of the psoriasis is often not an accurate measure of psychosocial disease.24
There are several techniques that can be used to overcome these challenges and identify patients with additional support needs. Simple interventions such as open questioning specific to psychological states can be very effective. The American Academy of Dermatology suggests questions such as:
- How does having psoriasis affect the patient’s daily life at home, work or at school?
- How is the patient coping with psoriasis and are they using any treatments?
- How does the patient feel – depressed, anxious, worthless, lonely?
- How is psoriasis affecting the patient’s relationship with their partner, family, friends, and carers?
- Does the patient need further advice or support?25
In addition to these broader questions, a large multinational study was undertaken by Bewley et al to help develop statements that could assist the consultation process by identifying the relative importance of factors related to effective management of psoriasis for patients.24 Statements derived from this study highlighted the questions that may help identify patients who feel that psoriasis “controls their daily life”. The questions that were found to be most correlated with psychological distress for patients include:
- Whether their psoriasis is “usually visible”
- If they feel others understand the effect psoriasis has had on them
- If they feel others avoid them
- If they take any measures to hide their psoriasis
- If they feel helpless with regard to their disease
- If they feel unable to participate in activities due to their disease.
Questioning whether these statements apply to a patient could help to identify those with further support needs but could also help to highlight specific issues regarding the patient’s individual problems, beliefs, and symptoms, which could be addressed with targeted interventions.
Compounding the challenge of identifying patients who need psychological support is the high presence of alexithymia in patients with psoriasis. A large, multicentre study showed that 25% of patients with psoriasis have alexithymia, or a reduced ability to recognise and describe internal emotions, often resulting in a difficulty identifying feelings and distinguishing them from physical sensations.26 Clearly, this presents a difficulty in identifying and discussing psychological treatment modalities, as patients may themselves be unable to express their emotions adequately and communicate their feelings with healthcare professionals. Hence, quality of life measurement is important to properly assess the full effect of psoriasis on a patient.
High scores on quality of life questionnaires should prompt clinicians to investigate further whether patients could benefit from psychological interventions. Examples of some of the more commonly used questionnaires in psoriasis are listed in Table 1.
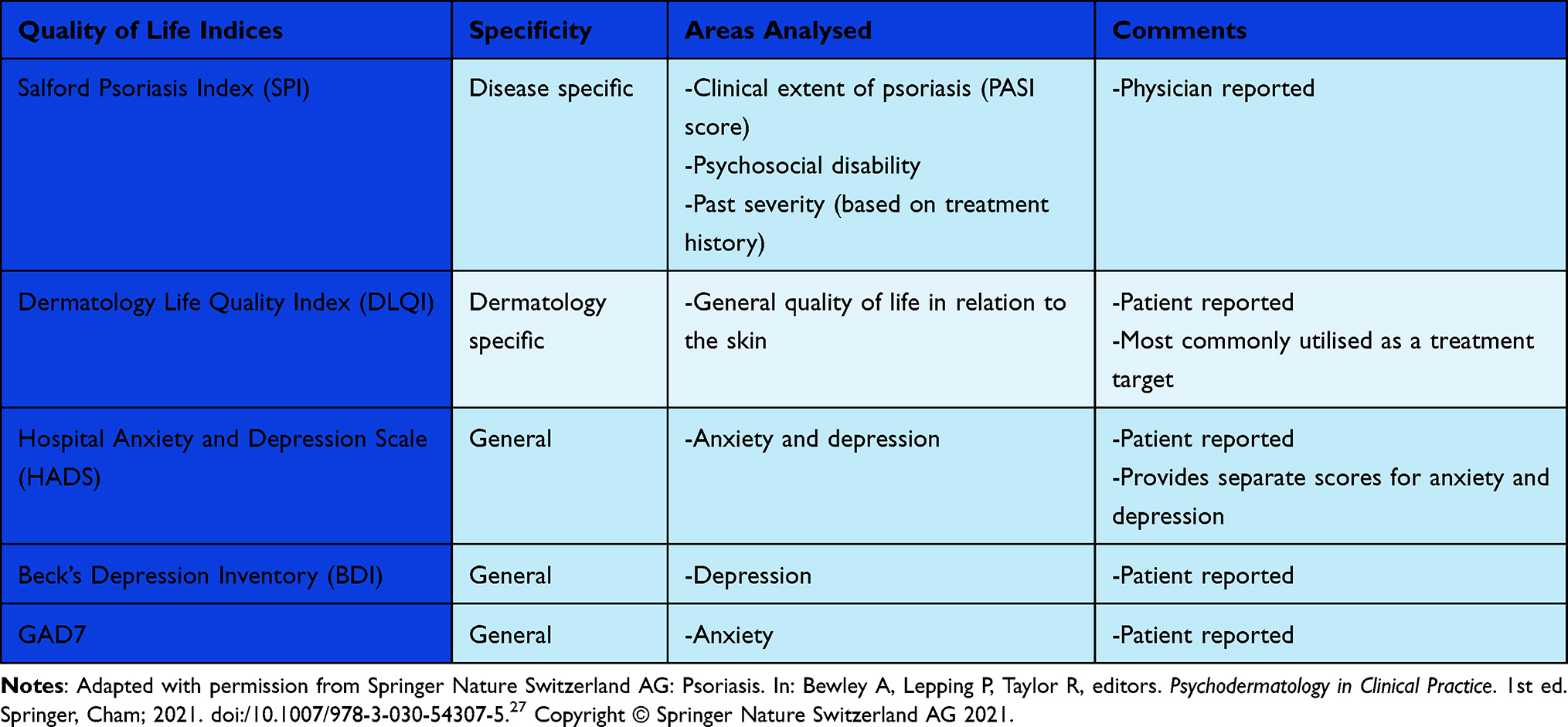 |
Table 1 Quality of Life Questionnaires |
Improving Outcomes
As we have discussed above, psoriasis is a condition with a complex interplay between physical and psychological components. While treating the skin is important, a holistic approach, taking under consideration psychological health and well-being, is required to manage patients optimally. Three tools to improve psychological health in psoriasis, namely, prompt and effective treatment of inflammation, cognitive behavioural therapy, meditation, and mindfulness-based therapy (including motivational interviewing), and to some extent psychotropic medication, are addressed below.
- Treatment of the skin: importance of adherence, limiting inflammation, and skin clearance
Skin clearance of clear/nearly clear has been defined by the BAD guideline development group as “critical” given its importance to patients with psoriasis.28 As discussed above, there is a direct link between inflammation and psychological distress. Treatment for inflammation, for example, in patients undergoing anti-TNF treatment, has shown a significant improvement in depression when compared to placebo, irrespective of clinical severity.29 This suggests that treating systemic inflammation is important in treating psychological distress.
An important caveat when discussing treatment of the skin is that it is psychologically important for patients to be aware that, while psoriasis is treatable, there is no cure. Successful management also depends on patients understanding the chronic nature of psoriasis, the therapeutic options available to them, and that several agents may be needed to achieve skin clearance It is key for patients to understand that psoriasis often has an unpredictable clinical course, with fluctuating severity over time.
It is key for physicians to introduce these concepts early to avoid patient frustration and treatment burnout, as one of the main impediments to complete skin clearance is adherence, with some studies showing up to 40% of patients not using their medication as recommended.30 Patients often felt that topical medications were of minimal help in managing their psoriasis, a feeling that was compounded by the fact that many had gone through a long process of trial and error before trying more potent options, leading to a loss of faith in topical options (as well as in the medical professionals who had been treating them). This often leads to a vicious cycle where patients are less likely to be adherent (and less likely to tolerate side effects of treatments) due to perceived lack of effectiveness, which then itself leads to worse outcomes.
Cognitive behavioural therapy (CBT) is another key treatment for patients with psoriasis. Patients with psoriasis can often experience negative and unrealistic thoughts, which cause further distress and skew the way they interpret situations. This has further negative knock-on effects on the actions they take. Patients are often aware that stress can worsen their psoriasis, which can cause them anxiety about being stressed (which can cause a feedback loop ultimately resulting in a worsening of the physical and psychological state). CBT aims to break this cycle by helping patients become aware of their negative thoughts and helps them develop alternative ways of thinking and behaving, hence reducing their psychological distress.
As discussed earlier, it is common for patients with psoriasis to fixate on their condition, with cognitive distortions that skew the way they perceive themselves and their interactions with others. There is evidence that just 6 weeks of CBT sessions, in addition to standard treatment, has significant improvement in the clinical severity of the skin, and improves symptoms of anxiety, depression, stress, and disability. These results can persist in the long term, with one study showing that 64% of patients treated with CBT and standard therapies achieving 75% improvement in their psoriasis, and only 23% of patients treated with standard therapies alone achieving this improvement.31 Promising results have also been demonstrated using internet-based electronic CBT interventions, with improvements seen in anxiety and quality of life.
Mindfulness-based therapies, including mindfulness-based stress reduction (MBSR) therapy, are commonly used psychological interventions, which have shown some efficacy in treating patients with psoriasis. These therapies focus on the inner experience, including sensations and behaviours, as well as introducing other stress-reduction techniques. A systematic review of psychological therapies in dermatology identified three major studies applying mindfulness-based therapies in 90 total patients with psoriasis; all three studies provided evidence for disease improvement.32–34 Fordham et al conducted the largest trial investigating mindfulness-based therapy in psoriasis to date, investigating 29 patients either receiving 8-week mindfulness group therapy in addition to traditional psoriasis therapy vs usual therapy alone. While mindfulness therapy resulted in a statistically lower Self-Administered Psoriasis Area Severity Index (SAPASI) (p = 0.05) and Dermatology Life Quality Index (DLQI) impairment scores than usual therapy alone, no difference was found in perceived stress or distress.32
Hypnosis has also been suggested as a possible therapy for psoriasis; proponents have argued that during the hypnotic state, suggestions can be introduced to increase mental and physical relaxation. In one study by Boncz et al, 27 patients with chronic plaque psoriasis were treated with either hypnosis, hypnosis and PUVA, or PUVA alone.35 After three treatment sessions, skin symptoms and related sleeping disorders decreased and later disappeared, with combination therapies of PUVA and hypnosis showing the best outcomes. However, this study, as with other studies investigating hypnosis as a treatment modality, was limited by sample size and lack of statistical analysis. Hence, further studies are needed to investigate the potential benefits of hypnosis in psoriasis patients.
Finally, motivational interviewing has been suggested as a potentially effective therapy for psoriasis. Motivational interviewing (MI) is very commonly used in other diseases, such as chronic obstructive pulmonary disease, and uses a guiding style to engage patients and use their own motivations to invoke change. MI is designed to empower patients by drawing on their own rationales and capacity for change. Larsen et al published a study of 169 patients with psoriasis and examined the effects of traditional therapy vs traditional therapy + MI. Results showed significantly greater SAPASI improvement at 3 months in the group receiving MI compared to the control group; in addition, beneficial effects were maintained at the 6-month follow-up.36 While the number of studies investigating MI in psoriasis is limited, a small number of trials to date have demonstrated promise as an adjunctive therapy.
There is mixed evidence regarding the use of psychotropic medication to treat patients with psoriasis. One double-blind placebo-controlled study by Alpsoy et al of 60 patients with psoriasis were randomised to Moclobemide (MAO inhibitor antidepressant) plus topical corticosteroids, with the control group receiving only corticosteroids.37 Those treated with antidepressants and topical steroids showed improvements in the clinical severity of their psoriasis as well as improvements in their depression and anxiety compared to the control. There is some evidence that psychotropic medication is most effective in psoriasis when combined with psychotherapeutic treatment; another small study in 38 psoriasis patients compared treatment with Escitalopram (a SSRI antidepressant) and treatment with psychotherapeutic treatment alone; the patients treated with medication and therapy had greater improvement in their skin and reduction in symptoms of anxiety and depression.38
While to date there is limited evidence that psychotropic medication has clinical benefits for cutaneous psoriasis, there is growing evidence that anxiety/depression, when co-morbidity with cutaneous psoriasis, may be, to some extent, caused by neuro-inflammation.39–41 Given this, it follows that systemic treatment with biologics in psoriasis may independently act as an antidepressant by reducing psoriatic neuroinflammation; research is ongoing in this field.
However, healthcare practitioners should also be aware that there is significant evidence that several psychotropic medications can themselves cause flares in psoriasis, and should be used with caution. These well-known agents include lithium, fluoxetine, and bupropion.
The above discussion is summarised in Table 2
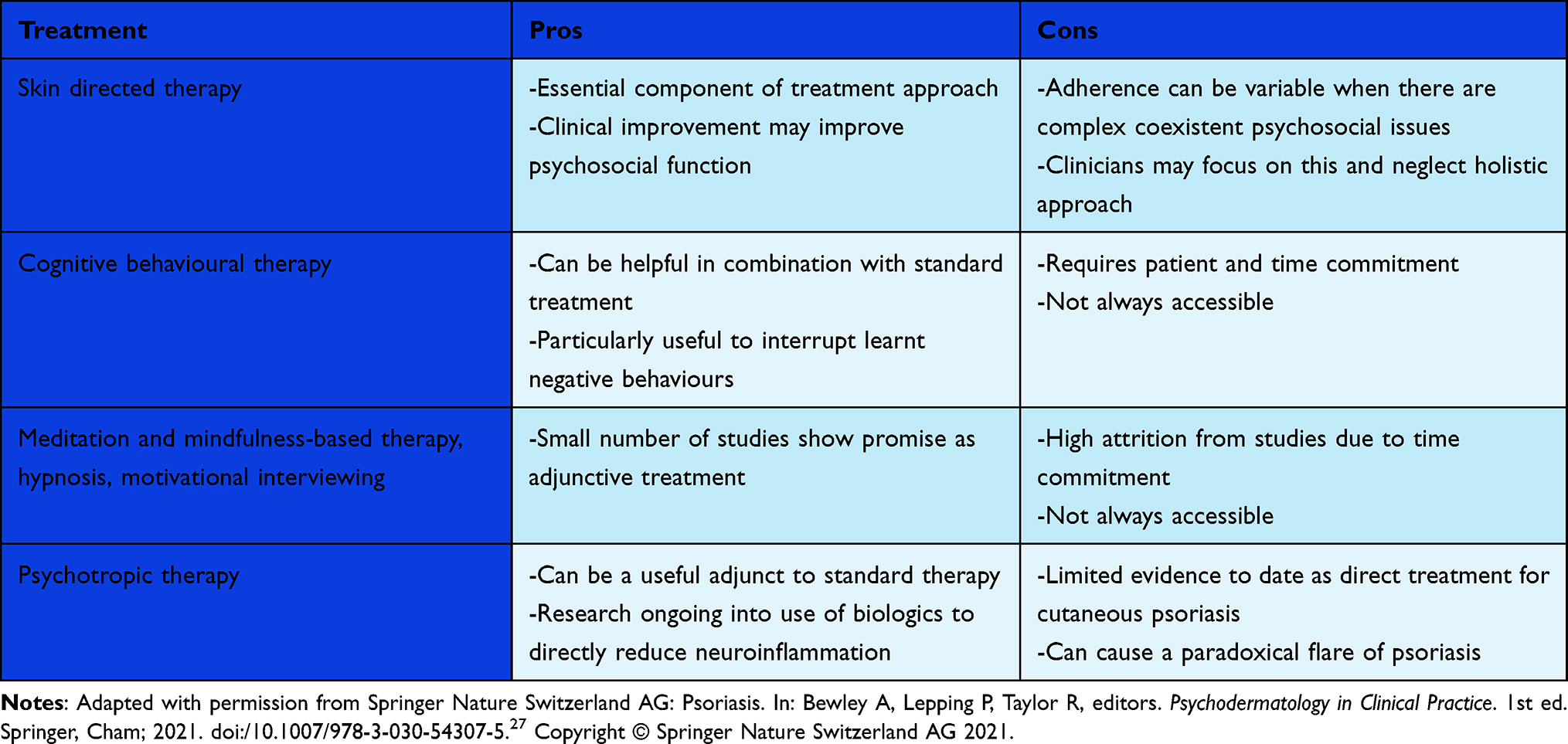 |
Table 2 Treatment Options |
Key Interventions at the Policy Level
Resources for mental health support are notoriously limited in the UK, with dire consequences for patients. As discussed above, these limitations have been exacerbated throughout the Covid-19 pandemic, which has worsened many mental health issues. Thankfully, new funding for Clinical Commissioning Groups (CCGs) has been promised for mental health services throughout the UK. It is imperative that a proportion of this funding is bookmarked for dermatology patients. This clinical need is supported by the discussion above, namely that 98% of skin disease patients report that their condition affects their emotional and psychological well-being, while only 18% have received psychological support.
Furthermore, it is imperative that commissioners understand that comprehensive multidisciplinary psychodermatology teams providing care to patients with all facets of psychodermatology must be commissioned. In addition to the clinical benefit of such services, it has been shown that psychodermatology clinics are cost-effective when compared to managing dermatology patients with co-morbid psychological issues in other less specialist settings, with some studies showing average cost of management as more than double in generalist vs psychodermatology clinics for these specific patients.42,43 The 2020 All-Party Parliamentary Group on Skin (APPGS) noted that HCPs can spend a disproportionate amount of time attempting to manage patients with co-morbid skin and psychological conditions in generalist settings. This is not only disadvantageous from a resource perspective but a longer duration of untreated mental health distress has been shown to be associated with worse clinical outcomes.44
To provide this service most effectively, it is important that each new Integrated Care System reviews its regional service provision in dermatology and psychodermatology, carrying out regular audits to assess needs within the local area. These assessments can be used to inform decision-making regarding resource allocation in different areas.
Finally, despite the tools listed above, it is currently difficult to compare outcomes across studies to determine what is the most effective identification and treatment strategies for patients with psoriasis and psychosocial support needs. A unifying dermatology-specific screening tool for depression would help compare treatment options and develop evidence-based algorithms in the future.
We recommend that in order to most effectively implement these suggestions, NHS England should create a National Clinical Director for Skin to provide the NHS with clinical leadership, advice, and support on dermatology care. This position would provide the leadership and direction needed to bring together this comprehensive reorganisation and appropriately utilise resources.
Conclusion
Ultimately, psoriasis is a complex condition with multifactorial psychological and biological drivers. Fully addressing this condition requires a holistic approach to the physical and psychosocial aspects, to maximise adherence, efficacy, and optimise patient quality of life. Adequate funding and support for multidisciplinary psychodermatology teams from a policy perspective is also necessary to best serve the needs of this population.
Acknowledgment
Brittany Blackstone and Radhika Patel are joint-first authors.
Disclosure
Professor Anthony Bewley reports personal fees from AbbVie, Almirall, Eli Lilly, Galderma, Janssen, Leo Pharma, Novartis, Sanofi, and UCB, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med. 2009;2009(361):496–509. doi:10.1056/NEJMra0804595
2. Tsoi LC, Stuart PE, Tian C, et al. Large scale meta-analysis characterizes genetic architecture for common psoriasis associated variants. Nat Commun. 2017;1:15382. doi:10.1038/ncomms15382
3. Tang H, Jin X, Li Y, et al. A large-scale screen for coding variants predisposing to psoriasis. Nat Genet. 2014;46(1):45–50. doi:10.1038/ng.2827
4. Sun L-D, Cheng H, Wang Z-X, et al. Association analyses identify six new psoriasis susceptibility loci in the Chinese population. Nat Genet. 2010;42(11):1005–1009. doi:10.1038/ng.690
5. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. The Lancet. 2021;397(10281):1301–1315. doi:10.1016/S0140-6736(20)32549-6
6. Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases. J Am Acad Dermatol. 2017;76(3):377–390. doi:10.1016/j.jaad.2016.07.064
7. All-Party Parliamentary Group on Skin. Mental Health and Skin Disease [Internet]. Available from: http://www.appgs.co.uk/wp-content/uploads/2020/09/Mental_Health_and_Skin_Disease2020.pdf.
8. Heydendael VMR, de Borgie CAJM, Spuls PI, Bossuyt PMM, Bos JD, de Rie MA. The Burden of psoriasis is not determined by disease severity only. J Investig Dermatol Symp Proc. 2004;9(2):131–135. doi:10.1111/j.1087-0024.2004.09115.x
9. Ginsburg IH, Link BG. Feelings of stigmatization in patients with psoriasis. J Am Acad Dermatol. 1989;20(1):53–63. doi:10.1016/S0190-9622(89)70007-4
10. Korman AM, Hill D, Alikhan A, Feldman SR. Impact and management of depression in psoriasis patients. Expert Opin Pharmacother. 2016;17(2):147–152. doi:10.1517/14656566.2016.1128894
11. Fleming P, Bai JW, Pratt M, Sibbald C, Lynde C, Gulliver WP. The prevalence of anxiety in patients with psoriasis: a systematic review of observational studies and clinical trials. J Eur Acad Dermatol Venereol. 2017;31(5):798–807. doi:10.1111/jdv.13891
12. Elise kleyn C, McKie S, Ross AR, et al. Diminished neural and cognitive responses to facial expressions of disgust in patients with psoriasis: a functional magnetic resonance imaging study. J Invest Dermatol. 2009;129(11):2613–2619. doi:10.1038/jid.2009.152
13. Hunter HJA, Hinz R, Gerhard A, et al. Brain inflammation and psoriasis: a [(11) C]-(R)-PK11195 positron emission tomography study. Br J Dermatol. 2016;175(5):1082–1084. doi:10.1111/bjd.13788
14. Fleming P, Roubille C, Richer V, et al. Effect of biologics on depressive symptoms in patients with psoriasis: a systematic review. J Eur Acad Dermatol Venereol. 2015;29(6):1063–1070. doi:10.1111/jdv.12909
15. Papp KA, Reich K, Paul C, et al. A prospective Phase III, randomized, double‐blind, placebo‐controlled study of brodalumab in patients with moderate‐to‐severe plaque psoriasis. Br J Dermatol. 2016;175(2):273–286. doi:10.1111/bjd.14493
16. Olivier C, Robert PD, Daihung D, et al. The risk of depression, anxiety, and suicidality in patients with psoriasis: a population-based cohort study. Arch Dermatol. 2010;146(8). doi:10.1001/archdermatol.2010.186
17. Chi -C-C, Chen T-H, Wang S-H, Tung T-H. Risk of suicidality in people with psoriasis: a systematic review and meta-analysis of cohort studies. Am J Clin Dermatol. 2017;18(5):621–627. doi:10.1007/s40257-017-0281-1
18. Brenaut E, Horreau C, Pouplard C, et al. Alcohol consumption and psoriasis: a systematic literature review. J Eur Acad Dermatol Venereol. 2013;27:30–35. doi:10.1111/jdv.12164
19. Á F, Kemény L. Psoriasis and alcohol: is cutaneous ethanol one of the missing links?: possible link between psoriasis and alcohol misuse. Br J Dermatol. 2010;162(4):711–716. doi:10.1111/j.1365-2133.2009.09595.x
20. Farkas Á, Kemény L. Alcohol, liver, systemic inflammation and skin: a focus on patients with psoriasis. Skin Pharmacol Physiol. 2013;26(3):119–126. doi:10.1159/000348865
21. Fortes C, Mastroeni S, Leffondré K, et al. Relationship between smoking and the clinical severity of psoriasis. Arch Dermatol. 2005;141:5. doi:10.1001/archderm.141.12.1580
22. Poikolainen K, Karvonen J, Pukkala E. Excess mortality related to alcohol and smoking among hospital-treated patients with psoriasis. Arch Dermatol. 1999;135(12). doi: 10.1001/archderm.135.12.1490
23. Lada G, Talbot PS, Bewley A, Kleyn CE. Mental health and dermatology practice in the COVID‐19 pandemic. Clin Exp Dermatol. 2020;45(7):816–817. doi:10.1111/ced.14330
24. Bewley A, Burrage DM, Ersser SJ, Hansen M, Ward C. Identifying individual psychosocial and adherence support needs in patients with psoriasis: a multinational two‐stage qualitative and quantitative study. J Eur Acad Dermatol Venereol. 2013;28(6):763–770. doi:10.1111/jdv.12174
25. American Academy of Dermatology. Psoriasis Clinical Guideline. American Academy of Dermatology; n.d. Available from: https://www.aad.org/member/clinical-quality/guidelines/psoriasis.
26. Sampogna F, Puig L, Spuls P, et al. Prevalence of alexithymia in patients with psoriasis and its association with disease burden: a multicentre observational study. Br J Dermatol. 2017;176(5):1195–1203. doi:10.1111/bjd.15243
27. Psoriasis. In: Bewley A, Lepping P, Taylor R, editors. Psychodermatology in Clinical Practice. 1st ed. Springer, Cham; 2021:89-103. doi:10.1007/978-3-030-54307-5;
28. Smith CH, Jabbar‐Lopez ZK, Yiu ZZ, et al. British Association of Dermatologists guidelines for biologic therapy for psoriasis 2017. Br J Dermatol. 2017;Suppl 2. doi:10.1111/bjd.15665
29. Kannan S, Heller MM, Lee ES, Koo JYM. The role of tumor necrosis factor-alpha and other cytokines in depression: what dermatologists should know. J Dermatolog Treatment. 2011;24(2):148–152. doi:10.3109/09546634.2011.619159
30. Augustin M, Holland B, Dartsch D, et al. Adherence in the treatment of psoriasis: a systematic review. Dermatology. 2011;222:363–374. doi:10.1159/000329026
31. Qureshi AA, Awosika O, Baruffi F, Rengifo-Pardo M, Ehrlich A. Psychological therapies in management of psoriatic skin disease: a systematic review. Am J Clin Dermatol. 2019;20(5):607–624. doi:10.1007/s40257-019-00437-7
32. Fordham B, Grifths CEM, Bundy C. A pilot study examining mindfulness-based cognitive therapy in psoriasis. Psychol Health Med. 2015;20:121–127. doi:10.1080/13548506.2014.902483
33. Kabat-Zinn J, Wheeler E, Light T, et al. Influence of a mindfulness meditation-based stress reduction intervention on rates of skin clearing in patients with moderate to severe psoriasis undergoing photo therapy (UVB) and photochemotherapy (PUVA). Psychosom Med. 1998;60:625–632. doi:10.1097/00006842-199809000-00020
34. Gaston L, Crombez JC, Lassonde M, Bernier-Buzzanga J, Hodgins S. Psychological stress and psoriasis: experimental and prospective correlational studies. Acta Dermato Venereol. 1991;156:37–43.
35. Boncz I, Farkas B, Hunyadi J. Experiences with group hypnotherapy of psoriatic patients. Aust J Clin Hypnother Hypn. 1990;11:15–20.
36. Larsen MH, Krogstad AL, Aas E, Moum T, Wahl AK. A telephone-based motivational interviewing intervention has positive effects on psoriasis severity and self-management: a randomized controlled trial. Br J Dermatol. 2014;171(6):1458–1469. doi:10.1111/bjd.13363
37. Alpsoy E, Özcan E, Çetin L, et al. Is the efficacy of topical corticosteroid therapy for psoriasis vulgaris enhanced by concurrent Moclobemide therapy? J Am Acad Dermatol. 1998;38(2):197–200. doi:10.1016/S0190-9622(98)70240-3
38. D’Erme AM, Zanieri F, Campolmi E, et al. Therapeutic implications of adding the psychotropic drug escitalopram in the treatment of patients suffering from moderate-severe psoriasis and psychiatric comorbidity: a retrospective study. J Eur Acad Dermatol Venereol. 2012;28(2):246–249. doi:10.1111/j.1468-3083.2012.04690.x
39. González-Parra S, Daudén E. Psoriasis and depression: the role of inflammation. Actas Dermo-Sifiliográficas (English Edition). 2019;110(1):12–19. doi:10.1016/j.adengl.2018.05.035
40. Nadeem A, Ahmad SF, Al-Harbi NO, et al. IL-17A causes depression-like symptoms via NFΚB and p38mapk signaling pathways in mice: implications for psoriasis associated depression. Cytokine. 2017;97:14–24. doi:10.1016/j.cyto.2017.05.018
41. Patel N, Nadkarni A, Cardwell LA, et al. Psoriasis, depression, and inflammatory overlap: a review. Am J Clin Dermatol. 2017;18(5):613–620. doi:10.1007/s40257-017-0279-8
42. Mental health and skin disease (2020) - APPGS [Internet]. All-Party Parliamentary Group on Skin (APPGS); 2020 [cited 2021Oct18]. Available from: http://www.appgs.co.uk/publication/view/mental-health-and-skin-disease-2020/.
43. Mohandas P, Bewley A, Taylor R. Dermatitis artefacta and artefactual skin disease: the need for a psychodermatology multidisciplinary team to treat a difficult condition. Br J Dermatol. 2013;169(3):600–606. doi:10.1111/bjd.12416
44. Romanov D, Lepping P, Bewley A, et al. Longer duration of untreated psychosis is associated with poorer outcomes for patients with delusional infestation. Acta Dermato Venereol. 2018;98(9):848–854. doi:10.2340/00015555-2888
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.