")
Back to Journals » Journal of Blood Medicine » Volume 15
Risk of Intracranial Hemorrhage in Persons with Hemophilia A in the United States: Real-World Retrospective Cohort Study Using the ATHNdataset
Authors Hu J , Chandler M, Manuel CM, Caicedo J, Denne M, Ewenstein B , Mokdad AG , Xing S, Recht M
Received 15 November 2023
Accepted for publication 27 March 2024
Published 24 April 2024 Volume 2024:15 Pages 191—205
DOI https://doi.org/10.2147/JBM.S443380
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Jianzhong Hu,1 Martin Chandler,1 Christopher Matthew Manuel,1 Jorge Caicedo,2 Michael Denne,2 Bruce Ewenstein,2 Ali G Mokdad,2 Shan Xing,3 Michael Recht1,4,5
1American Thrombosis and Hemostasis Network, Rochester, NY, USA; 2Rare Diseases and Hematology, Takeda Pharmaceuticals, U.S.A., Inc, Lexington, MA, USA; 3US Value and Evidence Generation, Takeda Pharmaceuticals, U.S.A., Inc, Lexington, MA, USA; 4Yale Center for Bleeding and Clotting Disorders, Yale University School of Medicine, New Haven, CT, USA; 5National Bleeding Disorders Foundation, New York, NY, USA
Correspondence: Michael Recht, National Bleeding Disorders Foundation, 7 Penn Plaza, New York, NY, 10001, USA, Tel +1 800-360-2846, Email [email protected]
Introduction: Intracranial hemorrhage (ICH), a serious complication in persons with hemophilia A (PWHA), causes high rates of mortality and morbidity. Identified ICH risk factors from patient data spanning 1998– 2008 require reassessment in light of changes in the current treatment landscape.
Aim and methods: PWHA identified in the ATHNdataset were evaluated retrospectively to assess incidence of ICH and determine the association between ICH risk and key characteristics using time-to-event analyses (Cox proportional-hazards models, survival curves, and sensitivity analyses).
Results: Over a median follow-up time of 10.7 patient-years, 135 of 7837 PWHA over 2 years of age in the ATHNdataset (1.7%) experienced an ICH. Stratification by prophylaxis status and inhibitor status resulted in an incidence rate (IR) ratio (IRR) (IR+/IR−) of 0.63 (95% confidence interval [CI], 0.43– 0.94; P=0.020) and 1.76 (95% CI, 0.97– 3.20; P=0.059), respectively. Characteristics associated with greater risk of developing ICH include being aged 2– 12 years; being covered by Medicaid; having had HIV, hepatitis C, or hypertension; and never having received factor VIII or prophylactic treatment. In multivariable analysis with interaction, the estimated hazard ratio for PWHA never receiving prophylaxis was 7.67 (95% CI, 2.24– 26.30), which shrunk to 2.03 (95% CI, 1.30– 9.12) in bootstrapping analysis and 3.09 in the highest-penalty ridge-regression analysis but was still significant. Inhibitor status was found not to be statistically associated with ICH in all analyses.
Conclusion: These results align with previous studies demonstrating that prophylaxis confers a protective effect against ICH. Previously, inhibitor positivity had been shown to increase risk for ICH; however, this study did not corroborate those findings.
Keywords: bleeding, factor VIII, health insurance, hematologic disease, prophylaxis, risk factors
Introduction
Hemophilia A (HA) is an X-linked recessive bleeding disorder caused by a deficiency of factor VIII (FVIII).1,2 There are an estimated 24,000–26,400 males with hemophilia A in the United States; approximately 75% of persons with hemophilia A (PWHA) have moderate or severe forms of the disease.3,4 Intracranial hemorrhage (ICH) in PWHA is associated with a high rate of mortality and morbidity.5 ICH risk is 10–20 times higher in people with hemophilia (PWH) than the general population.5 Incidence of ICH from select European countries is estimated at 13.9–38.6 per 100,000 males, while the reported incidence in PWHA is 290–540 per 100,000 PWHA.5
In a US-based study, 1.9% of the cohort with hemophilia, which included individuals with hemophilia A or B, experienced an ICH, resulting in an incidence rate of 390/100,000 patient-years.6 Witmer et al used data from the Universal Data Collection project, collected by the Centers for Disease Control and Prevention, from >20,000 people with bleeding disorders from May 1998 through March 2008.6 This study found that prophylaxis was associated with a significant risk reduction for ICH occurrence in people with severe hemophilia who were negative for HIV or inhibitors.6 Prophylaxis with clotting factor concentrates is currently an established standard of care for people with severe hemophilia A (factor levels <0.01 IU/mL; <1% of normal) and some people with moderate hemophilia A (0.01–0.05 IU/mL; 1–5% of normal).1,2 FVIII inhibitors can develop in response to treatment with FVIII concentrate and are associated with increased mortality and decreased effectiveness of factor concentrate; however, the effect of inhibitor status on bleeding phenotype is unclear.7–9
Risk factors for ICH identified by Witmer et al included being between 2 and 9 years of age or >41 years of age, presence of a high-titer inhibitor, prior ICH, severe hemophilia, and hepatitis C (HCV) infection.6 A 2011 study of an Italian cohort of PWH also identified an increased risk of ICH in young children, adults aged >40 years, people with severe hemophilia diagnosis, and people with inhibitors.10 People with hemophilia A or hemophilia B were included in both studies.6,10
Since publication of the Witmer study in 2010, the standard of care and treatment landscape for PWHA have changed.2 Here, we used contemporary ATHNdataset data to investigate risk factors for ICH and identify possible associations between time to developing ICH and various analyzed characteristics in individuals with hemophilia A.
Methods
Study Design
This retrospective cohort study included male (assigned at birth) PWHA in the ATHNdataset, with visit information from January 1, 2010 through September 30, 2020. The American Thrombosis & Hemostasis Network (ATHN) is the steward of the ATHNdataset, a Health Insurance Portability and Accountability Act–compliant, de-identified patient health dataset containing data from individuals with bleeding and clotting disorders receiving care in the United States at ATHN-affiliated treatment centers. Individuals may opt in or consent to contribute their data to help establish a better understanding of blood disorders, including complications, social and economic costs, and the effectiveness of treatments and interventions. With data contributed by >61,000 individuals, ~17,000 of whom have HA, the ATHNdataset is the largest source of health data of PWH in the world.
Only individuals with moderate (FVIII levels 1–5%)/severe (FVIII levels <1%) HA who opted in or consented to enrollment in the ATHNdataset were included in this study. While individuals with factor deficiencies other than HA were not ruled out from this dataset, those with a history of any bleeding disorder as primary diagnosis other than HA were excluded. Individuals with mild HA or with missing FVIII clotting activity levels were also excluded. ICH cases were not discriminated as spontaneous or trauma related. ICH status was based on documentation in real-world medical records, which were extracted anonymously into the ATHNdataset. There is no independent verification of the data in the ATHNdataset.
Demographics, Variables, and Outcome
The variables assessed in this study included race, ethnicity, age, mortality, Medicaid coverage, HCV status, HIV status, hypertension (HTN) status, FVIII treatment (plasma derived [pd] and/or recombinant [r]), bypassing agent treatment, non-factor treatment, prophylaxis status, and inhibitor status. Subgroups for each variable were defined based on relevant criteria. Mortality, assessed at study end, was evaluated for impact on ICH incidence during the study period. History of or current HCV/HIV infection and/or HTN were documented in real-world medical records, which were, in turn, anonymously extracted into the ATHNdataset. Individuals were described as “ever having received prophylaxis” if at any time in their medical history they received prophylaxis, defined as the use of any treatment product on a regular basis to prevent bleeds and/or maintain tolerance to factor. Individuals receiving episodic treatment were classified as never having received prophylaxis. Information on patient clinical data, individual prophylactic regimens related to frequency and dose, or temporally restricted inhibitor positivity and inhibitor titers were unavailable for this study.
The primary outcome of interest was time from first recorded visit in the ATHNdataset to the first incidence of ICH or right-censor (death or end of study period).
Statistical Methods
Unadjusted Analysis
ICH events were evaluated for frequency over the study period by linear regression. Significance was determined by P-value of the F-test, with a cutoff of 0.05. The association between incidence of ICH and each individual variable was measured in a contingency table analysis. Incidence rates (IRs; reported per 1000 patient-years) were calculated for prophylaxis and inhibitor in subgroup analyses by removing individuals with unknown status for either characteristic. The incidence rate ratio (IRR) was then calculated using the IR values for individuals with or without history of prophylaxis and FVIII inhibitors, respectively. Significance was determined through chi-square test with α=0.05.
Unadjusted univariate Cox proportional-hazards (CoxPH) analysis, which considers time to occurrence and incidence of ICH, was assessed for each subgroup associated with a variable across the cohort. Hazard ratios (HRs) were estimated and plotted for each variable using the CoxPH model against the subgroup reference. Survival curves were plotted for key subgroup variables, and significance was determined by P-value of the log rank test, with a cutoff of 0.05.
Multivariable Analyses
All assessed variables were used to develop a multivariable CoxPH model. Three more multivariable CoxPH models were developed: one included only significant covariates from the unadjusted CoxPH analysis, one additionally included inhibitor status (regardless of significance in the unadjusted analysis), and one further incorporated an interaction between inhibitor and prophylaxis. Significance for subgroups associated with a variable was determined using α=0.05 against the reference subgroup for the variable analyzed.
Sensitivity Analyses
Sensitivity analyses were conducted because of the small number of PWHA who experienced ICH in proportion to the cohort and were compared with their respective original models. A stratified bootstrapping model was applied to the unadjusted univariate and multivariable CoxPH models. This approach was done by defining the estimate or coefficient for bootstrapping specific to the model. Three hundred individuals were randomly sampled from the ICH and no-ICH populations and were bootstrapped 1000 times. Bootstrap statistics included a mean of estimates, bias, and confidence interval (CI) and were compared with their respective original model using the full dataset. Three ridge-regression penalties (small: θ=1, medium: θ=5, large: θ=10) were applied to the CoxPH multivariable model to address bias that could occur when the number of events of interest is rare, using all data to generate the model. Significance for subgroups associated with a variable was determined using α=0.05 against the reference subgroup for the variable analyzed.
Results
Patient Characteristics
The initial cohort consisted of 8065 PWHA. Only male (assigned at birth) PWHA aged between 2 and 75 years with and without ICH were included (n=7863). PWHA <2 years of age and >75 years of age were excluded because of the lack of comparator individuals within each age group; all 22 PWHA <2 years of age had a documented ICH incident, and none of the 95 PWHA >75 years of age experienced an ICH incident. Sixteen PWHA with ICH from this cohort were excluded from the final analysis because ICH occurrence was before the study period and therefore could not be used to identify risk factors for new-onset ICH. An additional 10 PWHA were excluded from the final analysis because they did not have a visit during the study timeframe (n=7837; Supplementary Figure 1). Demographic, clinical, and treatment characteristics of the final cohort are summarized in Table 1. ICH incidence rate significantly decreased during the 10-year study period (coefficient: –19.66; P<0.001; Figure 1).
 |
Table 1 Demographic, Clinical, and Treatment Characteristics of the Cohort and Incidence of ICH |
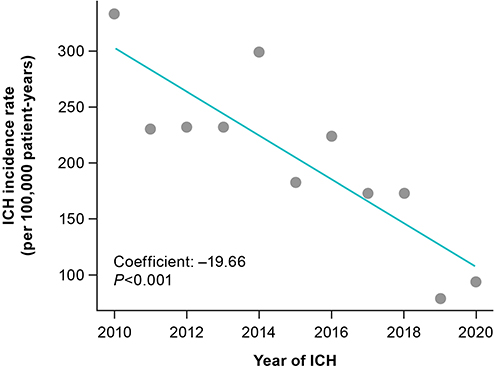 |
Figure 1 ICH incidence rate during the study period (2010–2020). Abbreviation: ICH, intracranial hemorrhage. |
Incidence of ICH
Unadjusted contingency table analysis was performed to test the association between incidence of ICH and each variable (Table 1). Because of small sample size, pdFVIII and rFVIII treatments were combined (FVIII combined). Bypassing agent and non-factor treatment parameters were not further analyzed because of low utilization rates in the study cohort.
Over 10 years and 9 months of collected data, 135 of 7837 PWHA (1.7%) had an ICH, with a median follow-up time of 10.7 patient-years. ICH incidence was found to be dependent on age (P<0.001), Medicaid status (P=0.018), mortality status (P=0.011), HCV status (P=0.011), HIV status (P<0.001), HTN status (P=0.001), and combined FVIII treatment status (P=0.001) and not found not to be dependent on race (P=0.200) or ethnicity (P=0.700). No dependence was found between incidence of ICH and prophylactic treatment (P=0.120) or ICH and inhibitor status (P=0.200).
IRR by prophylactic status (0.63; 95% CI, 0.43–0.94) was significant (P=0.020), showing increased incidence of ICH among individuals never receiving prophylaxis; the IR for individuals receiving prophylaxis and not receiving prophylaxis was 162 and 255 per 100,000 patient-years, respectively. IRR by inhibitor status (1.76; 95% CI, 0.97–3.20) was nonsignificant (P=0.059) but showed a numerically increased incidence of ICH among individuals with inhibitors; IR for individuals with and without inhibitors was 303 and 172 per 100,000 patient-years, respectively. No significant associations were found in the five age groups when stratified by prophylaxis status (Supplementary Table 1).
Most significant variables in the contingency table analysis remained significant in the unadjusted univariate CoxPH analysis, which provided additional insights into differential ICH risk in analyzed subgroups (Figure 2). Covariates with a significant protective effect on ICH risk (HR <1) include age >12 years (P<0.001) and no prior HCV (P=0.011), HIV (P<0.001), or HTN (P=0.049; Figure 3); availability of a start date for the three assessed comorbidities had no apparent bearing on ICH risk relative to having a history of that comorbidity. Past/current absence of an inhibitor was found not to have a significant effect on ICH risk (P=0.067; Figure 3) but showed a numerically decreased HR. Covariates indicating a significantly greater ICH risk (HR >1) include mortality after an ICH (P=0.010), current or past Medicaid coverage (P=0.017), and absence of pdFVIII or rFVIII treatment (P<0.001; Figure 3). Individuals who had never received prophylactic treatment were found to carry significantly greater risk of developing ICH than individuals receiving prophylactic treatment (HR 1.56; 95% CI, 1.06–2.30; P=0.024; Figure 2). Neither race nor ethnicity had a significant impact on risk of developing ICH (Figure 2).
 |
Figure 2 Risk of ICH in univariate analysis. Abbreviations: CI, confidence interval; FVIII, factor VIII; HCV, hepatitis C virus; HIV, human immunodeficiency virus; HR, hazard ratio; HTN, hypertension; ICH, intracranial hemorrhage. |
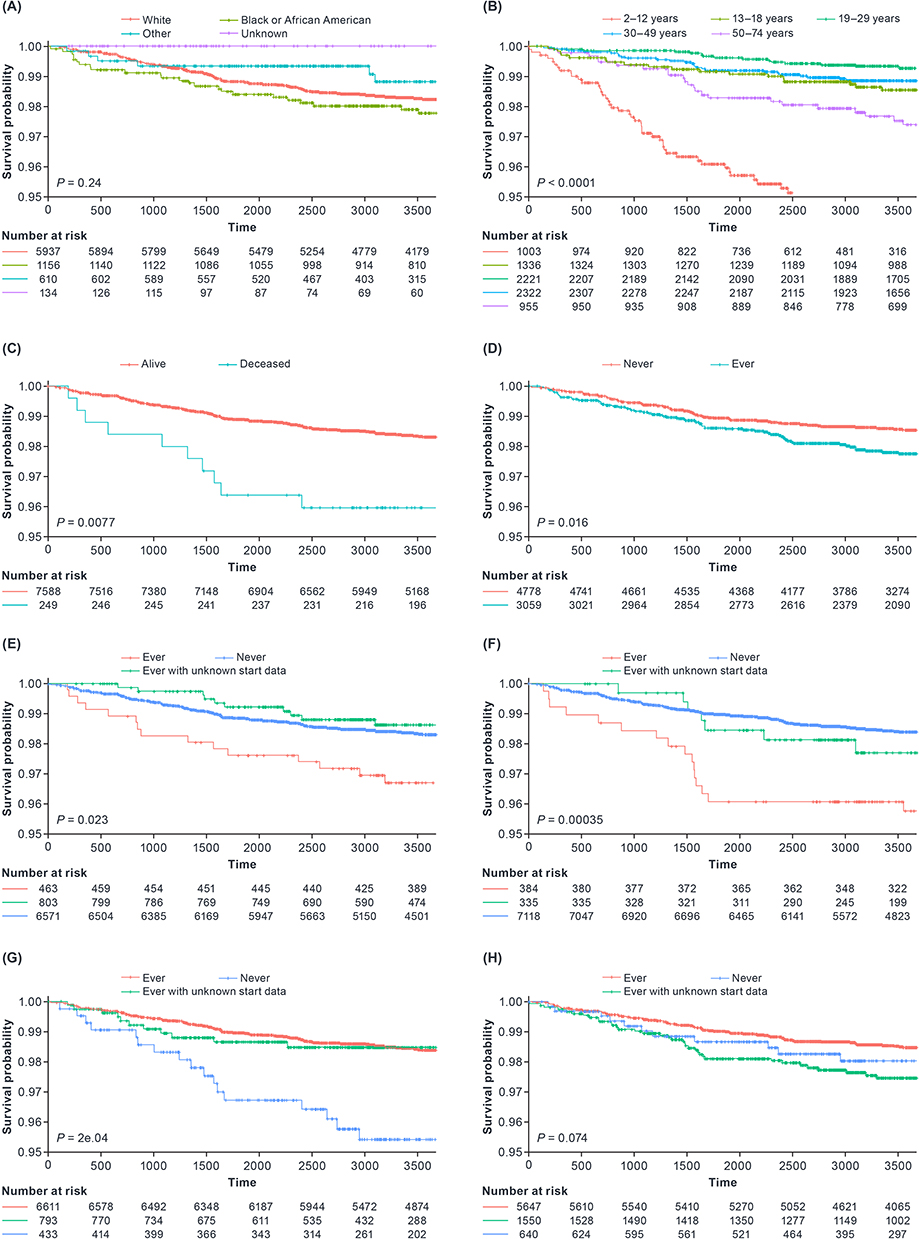 |
Figure 3 Kaplan–Meier curves of key characteristics. (A) Race; (B) Age; (C) Mortality; (D) Medicaid; (E) Hepatitis C; (F) HIV; (G) Any FVIII treatment (pdFVIII and rFVIII); (H) Prophylaxis. Abbreviations: FVIII, factor VIII; HCV, hepatitis C virus; HIV, human immunodeficiency virus; pdFVIII, plasma-derived factor VIII; rFVIII, recombinant factor VIII. |
Kaplan–Meier plots largely corroborated the unadjusted univariate CoxPH HR analyses (Figure 3); however, there were only marginal differences in the survival curves for the three prophylaxis subgroups (P=0.074). Bootstrapping sensitivity analysis of the unadjusted univariate CoxPH model analysis corroborated significance and directionality of most key characteristics; however, never having had HCV or HTN no longer had a significant protective effect on ICH development (Supplementary Table 2).
Multivariable Analysis
Multivariable CoxPH survival analysis with all variables was largely consistent with previous contingency table and univariate analyses. Although the effect of never receiving prophylaxis was found to be nonsignificant (P=0.070), the HR was numerically increased when compared with the reference group (Supplementary Figure 2). The risk of developing ICH was also not significantly associated with a negative history of HCV (P=0.06) or with mortality in this analysis (P=0.257; Supplementary Figure 2).
Two additional multivariable CoxPH models were generated, one including only covariates found to be significant in the unadjusted population CoxPH analysis and another also including inhibitor status (Supplementary Figure 3; Supplementary Figure 4). In the former, never having received prophylaxis (P=0.064) and never having had HCV (P=0.072) were both nonsignificant, although HR directionality matched previous analyses (Supplementary Figure 3). In the latter, similar results were observed in subgroups that never received prophylaxis (P=0.060) and never had HCV (P=0.071); never having had HTN was also found to be nonsignificant (P=0.051), with a numerically decreased HR compared with the reference group (Supplementary Figure 4).
Finally, multivariable CoxPH analysis, built using all significant covariates from the unadjusted analysis, inhibitor status, and with a prophylaxis:inhibitor interaction, was considered (Figure 4). Although most of the covariates were consistent in both significance and directionality of effect on ICH with the previously analyzed model, the HR for never having received prophylactic treatment increased exponentially to 7.67, while never having had HCV was found to be nonsignificant (P=0.098; Figure 4). This analysis also considered the joint impact of prophylaxis and inhibitor status on ICH risk; compared with the reference group (having had inhibitors [with unknown start date] and having received prophylaxis [with unknown start date]), never having received prophylaxis and never having had inhibitors, jointly, was significantly protective against ICH risk (P=0.005; Figure 4).
 |
Figure 4 Risk of ICH in multivariable analysis with significant covariates (univariate analysis) and prophylaxis:inhibitor interaction. Abbreviations: CI, confidence interval; FVIII, factor VIII; HCV, hepatitis C virus; HR, hazard ratio; HIV, human immunodeficiency virus; HTN, hypertension; ICH, intracranial hemorrhage. |
Bootstrapping and penalty-based ridge-regression sensitivity analyses were conducted on a multivariable model with interaction to confirm results (Table 2 and Table 3). Overall, the bootstrapping analysis minimized HR estimates; however, directionality and significance were largely maintained compared with the original model (Table 2). Based on the estimated 95% CI, not having had HTN no longer had a significant protective effect on ICH occurrence. The HR of not having received prophylactic treatment decreased from 7.67 to 2.03 following bootstrapping analysis but was significant based on the estimated CI.
 |
Table 2 Multivariable CoxPH Model with Interaction and Bootstrap Sensitivity Analyses |
 |
Table 3 Multivariable CoxPH Model with Interaction and Penalty-Based Ridge-Regression Analyses |
Ridge-regression penalties were also applied to the multivariable CoxPH model with a prophylaxis:inhibitor interaction; as expected, smaller penalties impacted HR estimates less than larger penalties (Table 3). Compared with the original model, mortality and HCV remained nonsignificant, and HTN status went from significant to nonsignificant. Penalty-based ridge regression minimized HR estimates while maintaining directionality and significance compared with the population-based multivariable CoxPH model with an interaction term for other variables. The HR of never having received prophylactic treatment decreased from 7.67 to 3.09 following application of the largest ridge-regression penalty.
Discussion
ICH is a serious complication for PWH. Identifying factors associated with increased ICH risk is critical for its prevention. Our study identified the following risk factors for ICH in PWHA using the ATHNdataset: being between 2 and 12 years of age, having ever received Medicaid coverage, having had certain comorbidities (HIV and HTN), never having received factor treatment, and never having received prophylactic treatment.
This is the first US study in over a decade to identify risk factors for ICH and associations between risk factors and time to developing ICH. Witmer et al reported that any of the following conditions confer significant risk of ICH: age 2–9 or >41 years, being of Black (non-Hispanic) descent, and having HCV, high-titer inhibitors, severe hemophilia, or prior ICH.6 A significant interaction between prophylaxis and both inhibitor and HIV status could only be found in people with severe hemophilia, not in the entire cohort; absence of an inhibitor and no documented HIV infection were found to be protective against development of ICH.6,10
Since the Witmer study, the standard of care and the overall hemophilia treatment landscape have evolved, necessitating our follow-up study using more recent ATHNdataset data.2 Additionally, the Witmer study population included those with either hemophilia A or B; therefore, the findings in that study are not specific to either type.6 Our study looks at risk factors for ICH specifically in individuals with moderate/severe hemophilia A.
Results from multivariable analysis with an interaction term indicated being aged 13–74 years or never having had HIV were associated with lower risk of ICH, while ever being covered by Medicaid or never having received either FVIII treatment or prophylactic treatment were associated with greater risk of ICH during the study period. These results were largely consistent in directionality and significance following sensitivity analyses. Mortality after study end was found to increase ICH risk, and never having HTN or HCV was found to decrease ICH risk only in the univariate analyses.
Our findings are in agreement with other real-world studies.5,6,10–14 Hypertension is a known risk factor for ICH in the broad population and was the most common comorbidity among adult PWHA with ICH.11,15 Prevalence of HTN was higher in PWHA versus those without, especially among older individuals.11 While HTN was found to be significant only in the univariate analysis, further analysis of ICH cases by age and hypertensive status may illuminate a role in mediating ICH risk. Mortality caused by ICH is higher in PWH when compared with the general population (estimated at 20%) and is yet higher in young children and in developing countries, emphasizing the need to better understand risk factors for ICH.5,14 In our study, mortality at study’s end was found to be significant only in the univariate analysis and was assessed as a risk factor for ICH, not an outcome.
Analyses from this study demonstrate that PWHA who have ever been covered by Medicaid have a higher risk of developing an ICH. Therefore, Medicaid-insured PWHA could represent an important population for ICH risk mitigation. Medicaid is a public health insurance option in the United States.16 It has previously been shown that people with Medicaid insurance have worse outcomes after ICH than privately insured individuals;12 whether this disparity in outcomes exists in Medicaid-insured PWHA requires further study. Given that Medicaid insurance is linked to socioeconomic status, this finding could be further suggestive of an existing health disparity by income and a barrier to achieving health equity.16,17 Socioeconomic status was not fully captured in the ATHNdataset, opening the possibility that the impact of Medicaid insurance on ICH incidence could be explained by disparities in health equity. Intriguingly, this analysis found no effect of race or ethnicity, both notable contributors to health inequity, on ICH incidence,18 suggesting that health inequity, alone, does not fully describe the factors contributing to ICH incidence.
Inhibitor status was not found to be a significant risk factor for ICH in this study, but previous studies have demonstrated that presence of inhibitors, particularly high-titer inhibitors, significantly increases ICH risk.6,10 This could be related to the changing landscape of immune tolerance induction. Over time, variations on the original Bonn protocol and other novel immune tolerance induction regimens have been used to treat persons with FVIII inhibitors.19 Synchronously, a wider breadth of hemophilia treatments, including extended–half-life factor products and emicizumab, have also been available, although their respective effectiveness in immune tolerance induction has not been definitively established.20 Altogether, these advances may enable increased use of immune tolerance induction, which may, in turn, preclude establishing a statistically significant link between ICH incidence and inhibitor status.
Previous studies have also demonstrated the ICH protective effect of prophylactic treatment in people with severe hemophilia6 and in children and adolescents with hemophilia A, corroborating findings from this study.13 As of 2018, the standard of care for congenital hemophilia A has evolved to include emicizumab, a humanized antibody that mimics activated FVIII to allow continuation of the coagulation cascade.21 This study’s period includes data from before and after emicizumab approval in 2018. The ICH rate significantly decreased across the study period, but data from the periods before and after emicizumab approval cannot be conclusively analyzed because of the limited sample size after emicizumab approval and the inability to account for all possible confounders (Figure 1).
As in the Witmer study,6 results are only generalizable to people receiving specialized care at hemophilia treatment centers (HTCs). In a study from 1998, HTCs were estimated to treat 60–70% of PWH in the United States; however, there are no data to confirm this.22 Newer data suggest that close to 80% of PWH are treated at HTCs.3 The ATHNdataset, which contains data from all ATHN-affiliated treatment centers, only contains information from people who consent or opt in to contribute their data. Therefore, these data may not be generalizable to all PWHA receiving care through the United States HTC Network or the broader population of PWHA in the United States.
Adherence to a prophylactic regimen can dictate whether PWHA experience improved outcomes.2 In a 2010 survey of US HTC nurses, 80% of people with severe HA were found to be adherent to their prescribed prophylactic regimen. Data related to prophylaxis adherence were not available for the people in this study; however, the inclusion of non-compliant individuals or individuals with a less rigorous prophylactic regimen could lead to an underestimation of the effect of prophylaxis on occurrence of ICH. This suggests that prophylactic treatment may have a more protective effect on risk of developing ICH than assessed in this study.
Although only participants with moderate or severe HA were included in this study, hemophilia severity data were not analyzed because of suspected interactions with clinical and treatment characteristics. Severe hemophilia is a known risk factor for ICH, and prophylaxis is the standard of care for severe hemophilia.2,6 In a French survey using data from 1991 through 2001, two-thirds of ICH cases were in people with severe hemophilia, and prophylaxis was associated with improved ICH-associated outcomes in PWH.2,23
This analysis did not distinguish individuals who have active HIV or HCV infections, or currently have HTN or FVIII inhibitors, from those who have previously had but do not currently have either comorbidity. This will cause an underestimation of the effect of either HCV, HIV, HTN, or inhibitor status on development of ICH, suggesting that not having either comorbidity may be more protective against ICH occurrence than assessed.
While the Witmer study found a relationship between prophylaxis and inhibitor status in people with severe hemophilia, in our study prophylaxis:inhibitor subgrouping characteristics and sample sizes prevent strong conclusions regarding the joint risk of prophylaxis and inhibitor status on ICH, with the notable exception of inhibitor-negative individuals who have never received prophylaxis.6
Conclusions
This study, using data from the ATHNdataset, identified the following risk factors for ICH in PWHA: being aged between 2 and 12 years, having ever received Medicaid coverage, having had certain comorbidities (HIV and HTN), never having received factor treatment, and never having received prophylactic treatment. These risk factors will need to be continually reevaluated as the treatment landscape for hemophilia evolves to include increased use of non-factor products and gene therapy.
Data Sharing Statement
The data supporting the findings of this study originate from the ATHNdataset and are available from ATHN. Restrictions apply to the availability of these data, which were used under license for this study. Data inquiries can be made by emailing ATHN at [email protected].
Ethics Statement
The ATHNdataset is a Health Insurance Portability and Accountability Act–compliant, de-identified patient health dataset containing data from individuals with bleeding and clotting disorders receiving care in the United States at ATHN-affiliated treatment centers who have consented to contribute their data voluntarily. Per ethics review by Advarra (www.advarra.com), the ATHNdataset has been deemed non-human research.
Acknowledgments
This study was sponsored by Takeda Pharmaceuticals U.S.A., Inc., Lexington, MA, USA. Medical writing support was provided by Nivedita Saxena, an employee of Parexel, and was funded by Takeda Pharmaceuticals U.S.A., Inc.
Findings from this manuscript were presented in part as a poster presentation at the American Society of Hematology Annual Meeting; December 10–13, 2022. The poster’s abstract was published in Volume 140, Issue Supplement 1 in Blood: doi.org/10.1182/blood-2022-163861.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all of these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Takeda Pharmaceuticals U.S.A., Inc., Lexington, MA, USA.
Disclosure
JC, MD, AGM, and SX are currently employees and stockholders of Takeda. BE was an employee of Takeda at the time of the study and is currently a stockholder of Takeda. MR was affiliated with American Thrombosis and Hemostasis Network at the time of the study and receives research funding from Bayer, BioMarin, CSL Behring, Genentech, Grifols, Hema Biologics, LFP, NovoNordisk, Octapharma, Pfizer, Sanofi, Sparke, Takeda, and uniQure; is a consultant for BioMarin, Catalyst Biosciences, CSL Behring, Genentech, Hema Biologics, Kedrion, NovoNordisk, Pfizer, Sanofi, Takeda, and uniQure; and is on the board of directors of the Foundation of Women and Girls with Blood Disorders, Partners in Bleeding Disorders, and the Thrombosis and Hemostasis Societies of North America. The authors report no other conflicts of interest in this work.
References
1. Benson G, Auerswald G, Dolan G, et al. Diagnosis and care of patients with mild haemophilia: practical recommendations for clinical management. Blood Transfus. 2018;16(6):535–544. doi:10.2450/2017.0150-17
2. Srivastava A, Santagostino E, Dougall A, et al. WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia. 2020;26(Suppl 6):1–158. doi:10.1111/hae.14046
3. Soucie JM, Miller CH, Dupervil B, Le B, Buckner TW. Occurrence rates of haemophilia among males in the United States based on surveillance conducted in specialized haemophilia treatment centres. Haemophilia. 2020;26(3):487–493. doi:10.1111/hae.13998
4. National Bleeding Disorders Foundation. Hemophilia A. Available from: https://www.hemophilia.org/bleeding-disorders-a-z/types/hemophilia-a.
5. Zanon E, Pasca S. Intracranial haemorrhage in children and adults with haemophilia A and B: a literature review of the last 20 years. Blood Transfus. 2019;17(5):378–384. doi:10.2450/2019.0253-18
6. Witmer C, Presley R, Kulkarni R, et al. Associations between intracranial haemorrhage and prescribed prophylaxis in a large cohort of haemophilia patients in the United States. Br J Haematol. 2011;152(2):211–216. doi:10.1111/j.1365-2141.2010.08469.x
7. Bray G. Inhibitor questions: plasma-derived factor VIII and recombinant factor VIII. Ann Hematol. 1994;68(Suppl 3):S29–S34. doi:10.1007/BF01774527
8. Wight J, Paisley S. The epidemiology of inhibitors in haemophilia A: a systematic review. Haemophilia. 2003;9(4):418–435. doi:10.1046/j.1365-2516.2003.00780.x
9. Gomez K, Klamroth R, Mahlangu J, et al. Key issues in inhibitor management in patients with haemophilia. Blood Transfus. 2014;12(Suppl 1):s319–s329. doi:10.2450/2013.0246-12
10. Zanon E, Iorio A, Rocino A, et al. Intracranial haemorrhage in the Italian population of haemophilia patients with and without inhibitors. Haemophilia. 2012;18(1):39–45. doi:10.1111/j.1365-2516.2011.02611.x
11. von Drygalski A, Kolaitis NA, Bettencourt R, et al. Prevalence and risk factors for hypertension in hemophilia. Hypertension. 2013;62(1):209–215. doi:10.1161/HYPERTENSIONAHA.113.01174
12. Pierre-Louis YS, Perla KMR, Perez GM, et al. The insurance coverage paradox - characterizing outcomes among dual-eligible hemorrhagic stroke patients. J Clin Neurosci. 2022;97:99–105 doi:10.1016/j.jocn.2021.12.023.
13. Andersson NG, Auerswald G, Barnes C, et al. Intracranial haemorrhage in children and adolescents with severe haemophilia A or B - the impact of prophylactic treatment. Br J Haematol. 2017;179(2):298–307. doi:10.1111/bjh.14844
14. Zwagemaker AF, Gouw SC, Jansen JS, et al. Incidence and mortality rates of intracranial hemorrhage in hemophilia: a systematic review and meta-analysis. Blood. 2021;138(26):2853–2873. doi:10.1182/blood.2021011849
15. Zappa S, McDaniel M, Marandola J, Allen G. Treatment trends for haemophilia A and haemophilia B in the United States: results from the 2010 practice patterns survey. Haemophilia. 2012;18(3):e140–e153. doi:10.1111/j.1365-2516.2012.02770.x
16. Arpey NC, Gaglioti AH, Rosenbaum ME. How socioeconomic status affects patient perceptions of health care: a qualitative study. J Prim Care Community Health. 2017;8(3):169–175. doi:10.1177/2150131917697439
17. Becker G, Newsom E. Socioeconomic status and dissatisfaction with health care among chronically ill African Americans. Am J Public Health. 2003;93(5):742–748. doi:10.2105/AJPH.93.5.742
18. National Academies of Sciences. Engineering, and Medicine. In: Baciu A, Negussie Y, Geller A, Weinstein JN, editors. Communities in Action: Pathways to Health Equity. Washington (DC): The National Academies Press; 2017.
19. Brackmann HH, White GC 2nd, Berntorp E, Andersen T, Escuriola-Ettingshausen C. Immune tolerance induction: what have we learned over time? Haemophilia. 2018;24(S3):3–14. doi:10.1111/hae.13445
20. Nakar C, Shapiro A. Hemophilia A with inhibitor: immune tolerance induction (ITI) in the mirror of time. Transfus Apher Sci. 2019;58(5):578–589. doi:10.1016/j.transci.2019.08.008
21. Gelbenegger G, Schoergenhofer C, Knoebl P, Jilma B. Bridging the missing link with emicizumab: a bispecific antibody for treatment of hemophilia A. Thromb Haemost. 2020;120(10):1357–1370. doi:10.1055/s-0040-1714279
22. Soucie JM, Evatt B, Jackson D. Occurrence of hemophilia in the United States. the hemophilia surveillance system project investigators. Am J Hematol. 1998;59(4):288–294. doi:10.1002/(SICI)1096-8652(199812)59:4<288::AID-AJH4>3.0.CO;2-I
23. Stieltjes N, Calvez T, Demiguel V, et al. Intracranial haemorrhages in French haemophilia patients (1991–2001): clinical presentation, management and prognosis factors for death. Haemophilia. 2005;11(5):452–458. doi:10.1111/j.1365-2516.2005.01090.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effect of Some Risk Factors on Over-Anticoagulation Disorders and Bleeding in Patients Receiving Anticoagulant Therapy with Overdosage of Vitamin K Antagonist
Dung Chu S, Thi Tran M
Vascular Health and Risk Management 2023, 19:663-672
Published Date: 18 October 2023