Back to Journals » Research and Reports in Urology » Volume 15
A Diagnostic Test Combining Molecular Testing with Phenotypic Pooled Antibiotic Susceptibility Improved the Clinical Outcomes of Patients with Non-E. coli or Polymicrobial Complicated Urinary Tract Infections
Authors Korman HJ, Baunoch D, Luke N ![]() , Wang D
, Wang D ![]() , Zhao X, Levin M, Wenzler DL, Mathur M
, Zhao X, Levin M, Wenzler DL, Mathur M
Received 10 January 2023
Accepted for publication 13 April 2023
Published 1 May 2023 Volume 2023:15 Pages 141—147
DOI https://doi.org/10.2147/RRU.S404260
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Panagiotis J Vlachostergios
Howard J Korman,1 David Baunoch,2 Natalie Luke,2 Dakun Wang,3 Xihua Zhao,4 Michael Levin,1 David L Wenzler,1 Mohit Mathur5
1Comprehensive Urology Division, Michigan Healthcare Professionals, Royal Oak, MI, USA; 2Department of Research and Development, Pathnostics, Irvine, CA, USA; 3Department of Writing, Stat4Ward, Pittsburgh, PA, USA; 4Department of Statistical Analysis, Stat4Ward, Pittsburgh, PA, USA; 5Department of Medical Affairs, Pathnostics, Irvine, CA, USA
Correspondence: Mohit Mathur, Pathnostics, 15545 Sand Canyon Suite 100, Irvine, CA, 92618, USA, Email [email protected]
Purpose: Complicated UTIs (cUTIs) cause significant morbidity and healthcare resource utilization and cost. Standard urine culture has limitations in detecting polymicrobial and non-E. coli infections, resulting in the under-diagnosis and under-treatment of cUTIs. In this study, patient-reported outcomes were compared between treated and untreated patients when an advanced diagnostic test combining multiplex-polymerase chain reaction (M-PCR) with a pooled antibiotic susceptibility method (P-AST) was incorporated into the patients’ clinical management.
Methods: Patients who had symptoms typical of cUTI and positive M-PCR/P-AST test results were recruited from urology clinics. Symptom reduction and clinical cure rates were measured from day 0 through day 14 using the American English Acute Cystitis Symptom Score (ACSS) Questionnaire. Clinical cure was defined based on the sum of the scores of four US Food and Drug Administration (FDA) symptoms and the absence of visible blood in the urine.
Results: Of 264 patients with suspected cUTI, 146 (55.4%) had exclusively non-E. coli infections (115 treated and 31 untreated) and 190 (72%) had polymicrobial infections (162 treated and 28 untreated). Treated patients exhibited greater symptom reduction compared to untreated ones on day 14 for those with exclusively non-E. coli organisms (3.18 vs 1.64, p = 0.006) and polymicrobial infections (3.52 vs 1.41, p = 0.002), respectively. A higher percentage of treated patients than of untreated patients achieved clinical cure for polymicrobial infections on day 14 (58.7% vs 36.4%, p = 0.049).
Conclusion: Patients with cUTIs treated based on the M-PCR/P-AST diagnostic test had significantly improved symptom reduction and clinical cure rates compared to untreated patients among those with non-E. coli or polymicrobial infections.
Keywords: urinary tract infection, complicated urinary tract infection, antibiotic, clinical outcome, diagnostic testing, polymerase chain reaction
Background
Urinary tract infections (UTIs), the most common infections in the United States, account for 10.5 million physician office visits and three million emergency department (ED) visits annually, representing a major healthcare burden.1,2 In many cases, particularly complicated UTIs (cUTIs), patients require antimicrobials to treat the infection. When an individual has one or more risk factors that predispose to higher treatment failure and poor outcomes, such as persistence of UTI, increasing severity, or occurrence of complications such as urosepsis, recurrence, and perinephric abscess, the case is considered a cUTI.3–5
Currently, the accepted UTI diagnostic test, standard urine culture (SUC), has several inherent limitations that favor the detection of E. coli6–8 over non-E. coli Gram-negative uropathogens such as Pseudomonas aeruginosa and species of Proteus and Klebsiella, as well as Gram-positive bacteria such as E. faecalis, E. faecium, and S. aureus, which are well-established as causes of UTIs and can lead to sepsis.3,6,9–11 Khasriya (2013) demonstrated that culture of the shed urothelial cells in patients with chronic lower urinary tract symptoms found large numbers of bacteria that were undetected by SUC.12
SUC also often misses polymicrobial cases due to the general practice of reporting samples with more than two or three organisms as contaminated or mixed flora.13,14 These polymicrobial infections, which have been reported in up to 39% of suspected UTI cases in elderly populations,14,15 have been associated with poor outcomes.16
These limitations of SUC hinder the effective diagnosis and treatment of cUTIs, especially in polymicrobial or non-E. coli cases, which could be underdiagnosed, left untreated, or mistreated. Indeed, Price et al found that SUC missed 50% of uropathogens in patients with severe urinary tract symptoms, and 36% of the patients continued to have symptoms even after receiving SUC-directed treatment.17
This study focuses on an advanced diagnostic test that combines multiplexed polymerase chain reaction (M-PCR) to detect bacterial and yeast uropathogens and antibiotic resistance genes with pooled antibiotic susceptibility testing (P-AST). Prior studies have shown its superiority in bacterial identification, especially for non-E. coli and polymicrobial UTIs.18–20 Furthermore, an observational retrospective study of 66,381 UTI patients revealed a 13.7% decrease (3.27% vs 3.79%, p = 0.003) in ED visits and hospital admissions when using this test compared to patients diagnosed via SUC.21
This prospective study compares the effects of the M-PCR/P-AST test on clinical outcomes for treated vs untreated patients based on responses to a validated clinical symptom score questionnaire for patients with non-E. coli or polymicrobial cUTIs.
Materials and Methods
Study Design and Participants
A Western IRB review and approval was obtained in accordance with the Declaration of Helsinki (20214705). Trial registration: NCT05091931. Registered 25 October 2021, https://clinicaltrials.gov/ct2/show/NCT05091931. The IRB determined that the study protocol met all three requirements for a partial waiver of authorization: that the use of PHI involved no more than minimal risk to the study participants, the research could not be practicably conducted without access to PHI, and the research could not practicably be conducted without the waiver. All 369 subjects gave verbal informed consent prior to enrollment.
This is an interim analysis of an ongoing observational prospective study. We included male or female patients who presented to urology clinics with symptoms and clinical presentations highly suspicious of cUTI (see Supplemental Table 1 for full Inclusion and Exclusion Criteria). This analysis focused on the clinical impact of treatment decisions on polymicrobial or non-E. coli cases, which are less likely to be detected by SUC than by novel M-PCR/P-AST testing.
Physicians evaluated patients’ clinical presentations on their first office visit (day 0) and recorded their demographics, clinical information, and antimicrobial treatment information when applicable, and collected urine samples for the M-PCR/P-AST test.
Patients completed a baseline survey on day 0 and daily surveys from day 1 through day 14. The surveys include symptom severity and antimicrobial treatment information. The symptom portion of the survey used a validated American English Acute Cystitis Symptom Score (ACSS) Questionnaire, asking patients to evaluate six typical UTI symptoms: urinary frequency, urinary urgency, dysuria, incomplete bladder emptying, suprapubic pain, and visible blood in the urine, according to each one’s severity (scoring 0–3): no (0), mild (1), moderate (2), severe (3).22,23 Each patient’s treatment was at the discretion of the treating clinician. Treatment status (treated or untreated with antimicrobials, including antibiotic and anti-fungal drugs, between day 0 and day 14) was determined based on the clinical evaluation form completed by physicians, patients’ daily surveys, and medical records.
Clinical Outcomes
Clinical outcomes evaluated in this analysis included average symptom score reductions and clinical cure rates on day 7 and day 14 based on the results of the survey based on the ASCC Questionnaire. This questionnaire was designed for symptom severity evaluation for acute cystitis, which is the relevant set of symptoms for patients included in this study. The symptom scores were the sum of four typical symptom scores for UTI defined by the US Food and Drug Administration (FDA) (urinary frequency, urinary urgency, dysuria, and suprapubic pain).22–24 Clinical cure was defined as the four FDA symptom scores adding up to ≤ 4, none of the four symptom scores being > 1, and the absence of visible blood in the urine. To best investigate the clinical cure rate, only patients with a sum of the four symptom scores of > 4 or at least one of the four symptom scores > 1 on day 0 were included in the clinical outcome analysis.
M-PCR/P-AST Test (Guidance® UTI, Offered by Pathnostics, Irvine, CA)
As described previously,19,20,25 the first step of the test involves DNA extraction from the patient’s urine sample using the King Fisher/MagMAX™ automated DNA extraction instrument and the MagMAX™ DNA Multi-Sample Ultra Kit (Thermo Fisher, Carlsbad, CA) per the manufacturer’s instructions. Extracted DNA from subjects’ samples was mixed with a universal PCR master mix and amplified using TaqMan technology in a Life Technologies 12K Flex 112-format Open Array System (Thermo Fisher Scientific, Wilmington, NC). Probes and primers were used to detect 26 bacteria/bacterial groups, fastidious and non-fastidious, and four yeast species.19,20
As part of the M-PCR/P-AST test, 32 antibiotic-resistance genes were also tested as described previously.25 In addition, fluorescence-based P-AST was performed when at least one non-fastidious bacterium is identified by M-PCR in the first step.25 P-AST determines the pooled antibiotic susceptibility profile, which accounts for bacterial interactions, against 19 antibiotics that are commonly used for UTIs.18
Statistical Analysis
Patients’ demographics, including age, sex, day 0 symptom scores, and the prevalence of each baseline symptom, were summarized using the mean and standard deviation (SD) for continuous variables and frequency (proportion) for dichotomized variables. For patients with non-E. coli or polymicrobial infections, the symptom scores were summarized by treatment status on day 0, day 7, and day 14, respectively. In addition, the changes in the symptom scores from day 0 to day 7 and from day 0 to day 14 were also summarized. The Kruskal–Wallis test was used to compare the difference in symptom scores between treated and untreated patients.The chi-square test or Fisher’s exact test was used to test whether the clinical cure rates differed according to the treatment status. The analysis was performed using Statistical Analysis System (SAS) 9.4.
Results
Patients’ Demographic and Clinical Information
A total of 369 patients with positive M-PCR/P-AST results were enrolled between 03/28/2022 and 02/08/2022 from any one of the 22 urology clinics located in diverse geographic and socioeconomic cities and suburban areas in the state of Michigan. Among them, 264 patients (163 female and 101 male patients) started with either a sum of the four FDA typical symptom scores of > 4 or at least one of the four FDA symptom scores of > 1 on day 0, which was the criterion for inclusion in this analysis.
The average age of the 264 patients was 68.5 years, and the majority (180, 68.2%) of them were aged ≥ 65 years. The mean baseline symptom scores based on the four FDA symptoms on day 0 were 5.5. The most frequent baseline symptoms were frequent urination (242, 91.7%) and urgent urination (239, 90.5%) (Table 1). All but one of the urine samples were collected via the midstream clean catch.
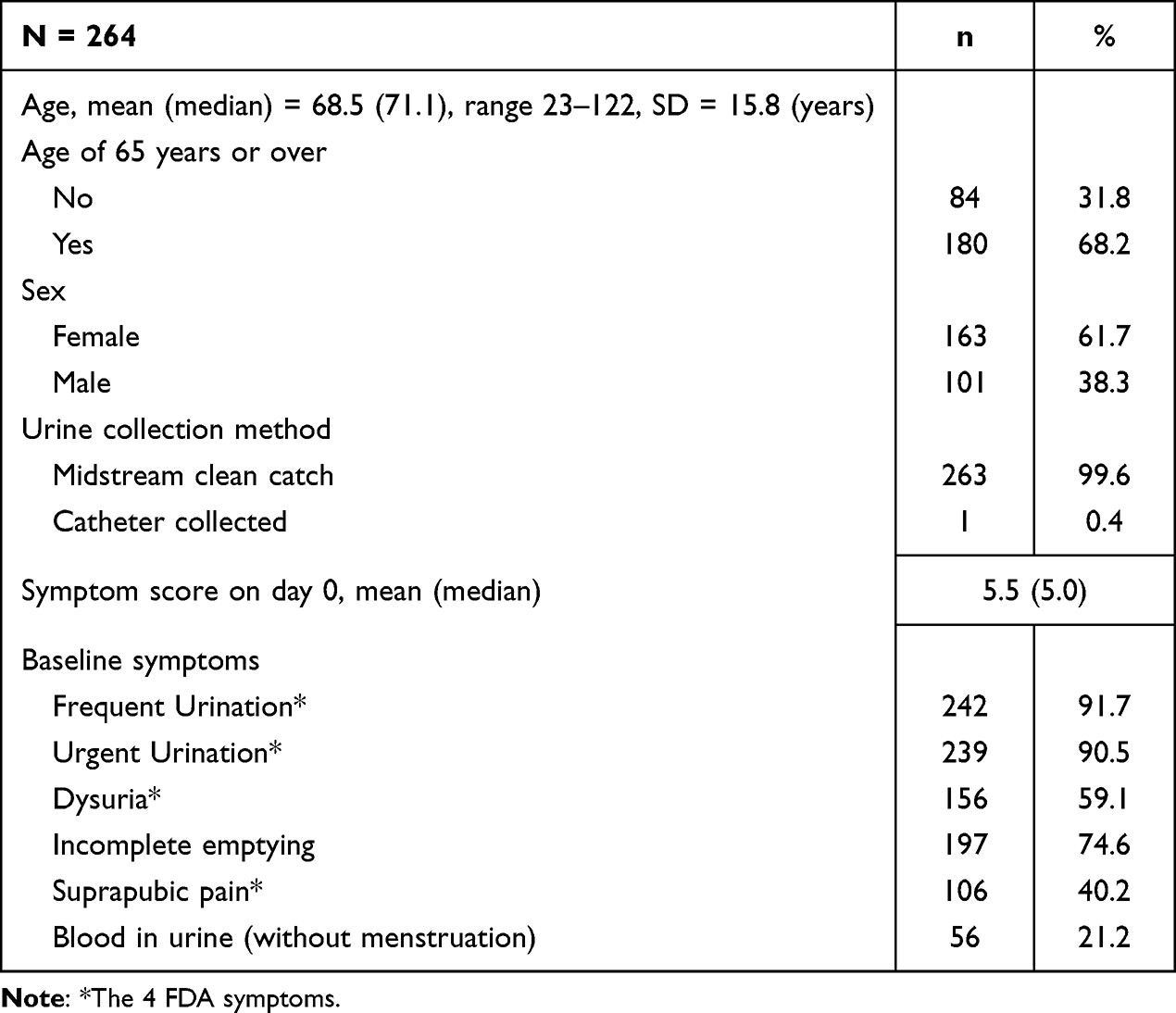 |
Table 1 Patients’ Demographic and Clinical Information |
Symptom Reduction and Clinical Cure Rates in Treated and Untreated Patients with Polymicrobial cUTIs
Polymicrobial UTIs, defined as the presence of two or more organisms, were detected in 190 (72.0%) patients, including 162 that received antimicrobial treatment and 28 that did not. There was no statistically significant difference in baseline symptom scores between the two groups of patients (5.70 vs 4.86, p = 0.054, Table 2). The mean symptom score reduction from day 0 was significantly greater in the treated than the untreated group on day 7 and day 14 (3.04 vs 1.48,p = 0.004 and 3.52 vs 1.41, p = 0.002, respectively; Table 2). A higher clinical cure rate was achieved in treated than in untreated patients on day 14 (58.7% vs 36.4%, p = 0.049, Table 3).
 |
Table 2 Mean Symptom Score Reduction on Day 7 and Day 14 in Treated and Untreated Patients |
 |
Table 3 Clinical Cure on Day 7 and Day 14 in Treated and Untreated Patients |
Symptom Reduction and Clinical Cure Rates in Treated and Untreated Patients with Non-E. coli cUTIs
We detected 146 (55.4%) patients with exclusively non-E. coli bacteria and yeast infections, including 115 that received treatment and 31 that did not. The baseline symptom scores between the two groups of patients did not differ significantly (5.59 vs 4.87, p = 0.083, Table 2). Among these patients, the mean symptom score reduction from day 0 was significantly greater in the treated than the untreated group on day 7 and day 14 (2.96 vs 1.57, p = 0.012 and 3.18 vs 1.64, p = 0.006, respectively; Table 2). Clinical cure rates in the treated and untreated group did not show a statistically significant difference on day 7 and day 14 (53.1% vs 37.9%, p = 0.15 and 55.6% vs 35.7%, p = 0.061, respectively; Table 3).
Discussion
For cases of non-E. coli or polymicrobial infections, where SUC has known shortcomings, it is important to consider alternative tests that can provide more accurate and rapid results. The M-PCR/P-AST diagnostic test reported here has been demonstrated in prior studies to be better at detecting non-E. coli and polymicrobial UTIs than SUC.19,20 There have been questions raised about the clinical value of identifying these types of organisms, and if they are associated with clinical manifestations of UTI or are incidental findings that do not cause disease. This study evaluated whether patients improved with treatment in cases where E. coli is absent or where there is a polymicrobial infection detected using an M-PCR/P-AST test that can identify 26 bacteria/bacterial groups and four yeast species. The P-AST component provides phenotypic results that account for bacterial interactions in polymicrobial infections.
The majority of the 264 symptomatic patients with presumed cUTI were diagnosed with non-E. coli (146/264, 55.4%) or polymicrobial (190/264, 72.0%) infections. These percentages are consistent with those in previous reports and further demonstrate the importance and prevalence of non-E. coli and polymicrobial UTIs. Due to the inherent limitations of SUC, many of these uropathogens would not have been detected, leading to under-treatment or inadequate antibiotic use, which elevates the risk of disease progression and antibiotic-resistance.
Here, both treated and untreated patients started with similar baseline symptom scores in cases with non-E. coli or polymicrobial infections. Mean symptom scores decreased faster on both day 7 and day 14 for non-E. coli and polymicrobial infection in the treated compared to the untreated group. In addition, a higher clinical cure rate was achieved in the treated than in the untreated group among patients with polymicrobial UTIs. There was a trend that more patients with non-E. coli infections achieved clinical cure in the treated than in the untreated group on day 14; however, the difference was not statistically significant.
One limitation of our study was that the 22 urology clinics were all located in Michigan as part of a single entity, Comprehensive Urology, which has extensive experience utilizing M-PCR/P-AST in the clinical diagnosis and management of UTIs. Further studies involving greater geographic distribution and an additional group to compare the M-PCR/P-AST test to SUC are warranted.
Conclusion
The lack of accurate and rapid directed treatment of cUTIs presents a significant healthcare problem, causing a higher risk of treatment failure, persistence, increasing severity, progression to acute pyelonephritis, recurrence and urosepsis.4,26 Increased ED and hospitalization visits, along with urosepsis (which is responsible for 25% of sepsis cases), causes increased healthcare cost and significant patient morbidity. These indicate a strong need for more accurate and rapid diagnosis and better-targeted therapy for these cases. The results of this study indicate the use of this M-PCR/P-AST test for polymicrobial or non-E. coli cUTI cases might be beneficial, showing an association with better symptom resolution and clinical cure rates.
Abbreviations
ASCC, Acute Cystitis Symptom Score; cUTIs, Complicated UTIs; ED, emergency department; M-PCR, multiplex-polymerase chain reaction; P-AST, pooled antibiotic susceptibility method; SD, standard deviation; SUC, standard urine culture; UTIs, Urinary tract infections.
Data Sharing Statement
All relevant data are present within the manuscript text and Tables.
Ethics Approval and Consent to Participate
All patients provided verbal informed consent (Western IRB 20214705) prior to enrollment.
Funding
Pathnostics and Thermo Fisher funded the study.
Disclosure
D.B., N.L., and M.M. are employees of Pathnostics, and D.W. and X.Z. are paid consultants of Pathnostics. Dr Howard J Korman is a Scientific Advisory Board member and Consultant for Pathnostics. Dr David Baunoch has a patent US 10,160,991 issued to PATHNOSTICS, a patent US 11,053,532 issued to PATHNOSTICS, a patent US 17/178,091 pending to PATHNOSTICS, a patent US 17/335,767 pending to PATHNOSTICS, a patent US 17/830,227 pending to PATHNOSTICS, a patent PCT/US22/16816 pending to PATHNOSTICS, a patent PCT/US22/77477 pending to PATHNOSTICS. The authors report no other conflicts of interest in this work.
References
1. Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nat Rev Microbiol. 2015;13(5):269–284. doi:10.1038/nrmicro3432
2. Simmering JE, Tang F, Cavanaugh JE, Polgreen LA, Polgreen PM. The increase in hospitalizations for urinary tract infections and the associated costs in the United States, 1998–2011. Open Forum Infect Dis. 2017;4(1):ofw281. doi:10.1093/ofid/ofw281
3. Wagenlehner FME, Johansen TEB, Cai T, et al. Epidemiology, definition and treatment of complicated urinary tract infections. Nat Rev Urol. 2020;17(10):586–600. doi:10.1038/s41585-020-0362-4
4. Leslie AS. Complicated urinary tract infections. StatPearls [Internet]; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK436013/.
5. Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women: a 2010 update by the infectious diseases society of America and the European Society for microbiology and infectious diseases. Clin Infect Dis. 2011;52(5):e103–e120. doi:10.1093/cid/ciq257
6. Sokhn ES, Salami A, Roz AE, Salloum L, Bahmad HF, Ghssein G. Antimicrobial susceptibilities and laboratory profiles of Escherichia coli, Klebsiella pneumoniae, and Proteus mirabilis isolates as agents of urinary tract infection in Lebanon: paving the way for better diagnostics. Med Sci. 2020;8(3):32. doi:10.3390/medsci8030032
7. Hooton TM. Uncomplicated urinary tract infection. N Engl J Med. 2012;366(11):1028–1037. doi:10.1056/nejmcp1104429
8. Foxman, B. Urinary tract infection syndromes occurrence, recurrence, bacteriology, risk factors, and disease burden.pdf. Infect Dis Clin N Am. 2014;28(1):1–13. doi:10.1016/j.idc.2013.09.003.
9. Ronald A. The etiology of urinary tract infection: traditional and emerging pathogens. Am J Med. 2002;113(1):14–19. doi:10.1016/S0002-9343(02)01055-0
10. Dreger NM, Degener S, Ahmad-Nejad P, Wöbker G, Roth S. Urosepsis—etiology, diagnosis, and treatment. Dtsch Arztebl Int. 2015;112(49):837–847;quiz 848. doi:10.3238/arztebl.2015.0837
11. Kline KA, Lewis AL, Mulvey MA, Stapleton AE, Klumpp DJ. Gram-positive uropathogens, polymicrobial urinary tract infection, and the emerging microbiota of the urinary tract. Microbiol Spectr. 2016;4(2):2. doi:10.1128/microbiolspec.uti-0012-2012
12. Khasriya R, Sathiananthamoorthy S, Ismail S, et al. Spectrum of bacterial colonization associated with urothelial cells from patients with chronic lower urinary tract symptoms. J Clin Microbiol. 2013;51(7):2054–2062. doi:10.1128/jcm.03314-12
13. Folaranmi T, Harley C, Jolly J, Kirby A. Clinical and microbiological investigation into mixed growth urine cultures. J Med Microbiol. 2022;71(5):5. doi:10.1099/jmm.0.001544
14. Price TK, Dune T, Hilt EE, et al. The clinical urine culture: enhanced techniques improve detection of clinically relevant microorganisms. J Clin Microbiol. 2016;54(5):1216–1222. doi:10.1128/jcm.00044-16
15. Hilt EE, McKinley K, Pearce MM, et al. Urine is not sterile: use of enhanced urine culture techniques to detect resident bacterial flora in the adult female bladder. J Clin Microbiol. 2013;52(3):871–876. doi:10.1128/jcm.02876-13
16. McCann E, Sung AH, Ye G, Vankeepuram L, Tabak YP. Contributing factors to the clinical and economic burden of patients with laboratory-confirmed carbapenem-nonsusceptible gram-negative urinary tract infections. Clin Outcomes Res Ceor. 2020;12:191–200. doi:10.2147/ceor.s234840
17. Price TK, Hilt EE, Dune TJ, Mueller ER, Wolfe AJ, Brubaker L. Urine trouble: should we think differently about UTI? Int Urogynecol J. 2018;29(2):205–210. doi:10.1007/s00192-017-3528-8
18. Vollstedt A, Baunoch D, Wolfe A, et al. Bacterial interactions as detected by Pooled Antibiotic Susceptibility Testing (P-AST) in polymicrobial urine specimens. J Surg Urol. 2020;2020:1.
19. Wojno KJ, Baunoch D, Luke N, et al. Multiplex PCR based Urinary Tract Infection (UTI) analysis compared to traditional urine culture in identifying significant pathogens in symptomatic patients. Urology. 2019;136:119–126. doi:10.1016/j.urology.2019.10.018
20. Vollstedt A, Baunoch D, Wojno K, et al. Multisite prospective comparison of multiplex polymerase chain reaction testing with urine culture for diagnosis of urinary tract infections in symptomatic patients. J Sur Urol. 2020;2020:JSU–102.
21. Daly A, Baunoch D, Rehling K, et al. Utilization of M-PCR and P-AST for diagnosis and management of urinary tract infections in home-based primary care. JOJ Uro Nephron. 2020;7(2):555707.
22. Alidjanov JF, Overesch A, Abramov-Sommariva D, et al. Acute cystitis symptom score questionnaire for measuring patient-reported outcomes in women with acute uncomplicated cystitis: clinical validation as part of a Phase III trial comparing antibiotic and nonantibiotic therapy. Investig Clin Urol. 2020;61(5):498–507. doi:10.4111/icu.20200060
23. Alidjanov JF, Abdufattaev UA, Makhsudov SA, et al. The acute cystitis symptom score for patient-reported outcome assessment. Urol Int. 2016;97(4):402–409. doi:10.1159/000448591
24. FDA. Uncomplicated urinary tract infections: developing drugs for treatment guidance for industry; 2019. Available from: https://www.fda.gov/media/129531/download.
25. Baunoch D, Luke N, Wang D, et al. Concordance between antibiotic resistance genes and susceptibility in symptomatic urinary tract infections. Infect Drug Resist. 2021;14:3275–3286. doi:10.2147/idr.s323095
26. Balasubramanian S, Wang X, Sahil S, Cheng A, Sutkin G, Shepherd JP. Risk factors for the development of acute pyelonephritis in women with a positive urine culture. Neurourol Urodyn. 2022. doi:10.1002/nau.25005
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Multiplex Polymerase Chain Reaction/Pooled Antibiotic Susceptibility Testing Was Not Associated with Increased Antibiotic Resistance in Management of Complicated Urinary Tract Infections
Korman HJ, Mathur M, Luke N, Wang D, Zhao X, Levin M, Wenzler DL, Baunoch D
Infection and Drug Resistance 2023, 16:2841-2848
Published Date: 9 May 2023
Pediatric Acute Lobar Nephronia: A Case Series and Literature Review
Lavi K, Klein A, Shtein N, Schichter Konfino V, Nir V
International Journal of Nephrology and Renovascular Disease 2024, 17:333-337
Published Date: 17 December 2024
The Use of Antibiotics for Uncomplicated Urinary Tract Infections in Adult Women: Qualitative Findings From the SCOUT Trial
Munné-Barellas B, Monfà R, Llor C, Garcia-Sangenís A, Miranda-Jiménez C, Morros R, Moragas A, Alvarez-Greciano P, Leiva A, Lozano-Del Hoyo ML, Sánchez-Calavera MA, Marín-Cañada J, Sánchez-Ruano R
Patient Preference and Adherence 2025, 19:2673-2685
Published Date: 31 August 2025