Back to Journals » Clinical Ophthalmology » Volume 16
Evaluation of Refractive Accuracy of ORA and the Factors Impacting Residual Astigmatism in Patients Implanted with Trifocal IOLs During Cataract Surgery: A Retrospective Observational Study
Authors Watanabe K ![]()
Received 20 April 2022
Accepted for publication 26 July 2022
Published 10 August 2022 Volume 2022:16 Pages 2491—2503
DOI https://doi.org/10.2147/OPTH.S371555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Keizo Watanabe
Minami Osaka Eye Clinic, Osaka, Japan
Correspondence: Keizo Watanabe, Minami Osaka Eye Clinic, Osaka, Japan, Tel +81 072-453-1750, Email [email protected]
Purpose: To assess the refractive accuracy of the intraoperative aberrometer Optiwave Refractive Analysis (ORA) and evaluate factors impacting residual astigmatism in eyes implanted with PanOptix (TFNT) trifocal intraocular lenses (IOLs) during cataract surgery.
Patients and Methods: This retrospective study examined 180 eyes implanted with a toric or non-toric trifocal IOL during cataract surgery. The mean refractive prediction error (RPE), median absolute RPE, and percentage of eyes with an absolute RPE ≤ 0.25, ≤ 0.50, ≤ 0.75, and ≤ 1.00 diopter (D) were determined for ORA and each of the IOL power formulas (Sanders–Retzlaff–Kraft/Theoretical [SRK/T], Barrett Universal II, and Haigis). Correlation analysis of postoperative residual astigmatism and factors associated with it was performed using Pearson’s and Spearman correlations in eyes with non-toric trifocal IOLs.
Results: After optimization, the median absolute RPE was 0.19 D, 0.25 D, 0.20 D, and 0.26 D in eyes measured using ORA and the SRK/T, Barrett Universal II, and Haigis formulas, respectively. An absolute RPE ≤ 0.50 D after optimization was noted in 92.8%, 83.3%, 88.3%, and 81.1% of the eyes using ORA and the SRK/T (p=0.0093), Barrett Universal II (p=0.2071), and Haigis (p=0.0018) formulas, respectively, showing significant differences between ORA and the SRK/T and Haigis formulas. The mean±standard deviation subjective residual astigmatism in non-toric IOL eyes (N=76) was 0.46± 0.39 D and showed a strong positive correlation with preoperative objective refractive astigmatism (r=0.2925, p=0.0109), intraoperative ORA–measured astigmatism (r=0.5555, p< 0.0001), postoperative objective refractive astigmatism (r=0.8188, p< 0.0001), and postoperative total corneal astigmatism (TCA) (r=0.4051, p=0.0003) and a negative correlation with preoperative anterior corneal astigmatism (r=− 0.3541, p=0.0017).
Conclusion: ORA is a salient tool for improving the postoperative refractive accuracy of trifocal IOL power calculations and may help in determining the need for toric IOL use in astigmatic eyes with cataracts. Residual astigmatism correlated with objective refractive astigmatism, ORA-measured astigmatism, and postoperative TCA.
Keywords: cataract surgery, intraoperative aberrometry, residual astigmatism, refractive prediction error, trifocal IOL
Plain Language Summary
During cataract surgery, the cloudy natural lens causing blurry vision is replaced with a clear artificial lens called an intraocular lens (IOL), which may be monofocal or multifocal. Trifocal IOLs, such as the AcrySof IQ PanOptix Trifocal IOL, correct near vision loss by enhancing intermediate and near vision while maintaining desirable distance vision.
While planning for cataract removal, an accurate IOL power calculation is performed to provide an IOL that fits individual patients’ needs and improves refractive outcomes impacting vision. An eye surgeon determines the correct power for an IOL by measuring various features of the eye. The accuracy of these measurements before surgery (using power formulas) or during surgery (using intraoperative aberrometers such as Optiwave Refractive Analysis [ORA]) is often critical in obtaining greatly improved visual acuity and reduced spectacle dependence. ORA provides real-time guidance to surgeons during cataract surgery for power selection and positioning of the lens, as well as in detecting abnormal curvature of the eye (astigmatism). Our findings showed that ORA considerably improved the accuracy of these refractive measurements.
Astigmatism can cause eyes to produce distorted images and is corrected using toric IOLs. For many years, it was thought that residual astigmatism after cataract surgery mainly arises from the anterior corneal surface. We used ORA to detect residual astigmatism arising from several parts of the eye and lens parameters to understand the association between them. ORA could accurately measure residual astigmatism and detect changes in total corneal astigmatism resulting from incisions during surgery.
Introduction
Multifocal intraocular lenses (IOLs) have become widely popular in cataract surgery with the availability of bifocal, extended depth-of-focus, and trifocal lens types.1 AcrySof IQ PanOptix TNFT lenses (Alcon Vision LLC, Fort Worth, TX, USA) are trifocal non-toric/toric IOLs which have an intermediate focal point of 60 cm and provide good visual acuity at all ranges of vision, along with excellent rotational and axial stability.2 These features optimize visual outcomes after cataract surgery, thereby increasing patient satisfaction.1 However, in eyes implanted with multifocal IOLs, postoperative refractive error and subjective residual astigmatism can worsen uncorrected visual acuity (UCVA).1,3
Each diopter (D) rise in astigmatism can lower uncorrected distance visual acuity (UDVA) by 1.5 lines and significantly increase spectacle dependency after surgery.4,5 True spectacle independence can only be achieved if the cataract surgery leads to ≤0.50 D of astigmatism.6 These concerns can cause patient dissatisfaction and necessitate further improvements in the accuracy of the procedure.5 Corrective surgery for astigmatism includes corneal incisions, corneal refractive surgery, and toric IOL implantation.4 Moreover, improved visual outcomes have been reported with the use of toric IOLs than with other corrective surgeries for astigmatism, such as corneal incisions and corneal refractive surgery.4 Besides refractive accuracy of the postoperative spherical equivalent, reduced postoperative residual astigmatism (≤0.75 D) also plays a crucial role in improving UCVA with trifocal IOLs.3,7
Residual astigmatism is influenced by several ocular components, especially anterior corneal astigmatism (ACA) and posterior corneal astigmatism (PCA); however, keratometry measures only ACA, assuming a constant posterior/anterior corneal curvature ratio.8 Moreover, in cases where corneal ectatic diseases are present or changes in corneal curvature occur following refractive surgery, such objective total corneal astigmatism (TCA) measurements can be highly inaccurate.9 The selection of toric IOLs and the determination of cylinder have relied solely on ACA values; however, recent reports suggest that accounting for PCA as well could help achieve improved visual correction outcomes.10–12
The Optiwave Refractive Analysis (ORA) system (Alcon Vision LLC, Fort Worth, TX, USA), inspired by the Talbot–Moiré technique of interferometry, is a widely used wavefront aberration analyzer that allows surgeons to estimate refraction, improve cylinder and IOL power, and aid IOL alignment during cataract surgery.4,13 The consideration of aberrometry measurements obtained using the ORA system before finalizing the toric IOL power has been found to improve outcomes, even in patients who had undergone previous corneal refractive surgeries.13 A large retrospective database analysis including 32,189 eyes found that the percentage of absolute prediction error ≤0.5 D for the ORA system was significantly greater than that for the preoperative calculation formula in eyes with AcrySof IQ IOL, AcrySof IQ toric IOL, or AcrySof IQ Restor IOL (81.9% versus 75.9%; P<0.0001).14 In another study involving AcrySof IQ toric IOL implants, the percentage of eyes with astigmatism ≤0.5 D at 1 month was higher for the ORA system than for the preoperative calculation formula and toric calculator (89.2% versus 76.6%; p=0.006).15
Although further improvements in accuracy and satisfaction can be expected by using ORA, studies exploring the accuracy of refractive prediction estimated by ORA with AcrySof IQ PanOptix (TFNT), the first trifocal IOL to be approved by the Food and Drug Administration, are limited and need to be validated against conventional preoperative planning.16,17 While previous studies have reported astigmatic outcomes after the implantation of TFNT toric IOLs, per our knowledge, no study has investigated the relationship between postoperative residual astigmatism and each of the ocular components that contribute to it.5,18 Therefore, this study aimed to assess the accuracy of refractive prediction, determined by ORA, for trifocal IOL implantation in comparison with preoperative IOL power calculations, assess the correlation between residual astigmatism and ORA measurement, and determine the factors associated with residual astigmatism.
Materials and Methods
Study Design
This single-center, retrospective, observational study was conducted using electronic medical records of patients visiting the Minami Osaka Eye Clinic in Japan from July 2019 to December 2020 for cataract surgery. MINS Institutional Review Board, an independent ethics committee and a non-profit organization, reviewed and approved the clinical study protocol (approval number 200247) with a waiver of consent because of the retrospective nature of the study. All patient data were deidentified and an opt-out approach was adopted to allow patients the option of refusing participation in the study. The study was conducted in accordance with the Declaration of Helsinki and the Ethical Guidelines for Medical and Health Research Involving Human Subjects.
Inclusion and Exclusion Criteria
Electronic medical records of consecutively included patients meeting the following inclusion criteria were analyzed retrospectively: age ≥20 years; implanted with a TFNT IOL in the capsular bag and intraoperatively analyzed using the ORA between July 2019 and December 2020; followed up 1–3 months postoperatively; and having a postoperative best-corrected visual acuity (BCVA) of 0.0 logarithm of the minimum angle of resolution (logMAR) visual acuity or better.
The exclusion criteria included a history of ophthalmic surgeries within 3 months after cataract surgery; corneal lesions (opacity and scarring) that prevented or could prevent accurate intraoperative measurement using ORA; an incompletely fixed IOL in the lens capsule; a history of keratorefractive surgery; the use of drugs or the presence of diseases that could affect postoperative visual acuity or refraction; the presence of a ruptured Zinn’s zonule or posterior capsule, vitreous prolapse, or hyphema during surgery; or the presence of other systemic or ophthalmic disorders considered inappropriate for inclusion by the physician.
Preoperative, Intraoperative, and Postoperative Keratometry
Preoperative and postoperative examinations were performed using OA-2000 (Tomey Corporation, Nagoya, Japan) and Auto Ref/Keratometer (Nidek Co. Ltd, Gamagori, Aichi, Japan), along with anterior segment three-dimensional optical coherence tomography-CASIA2 (Tomey Corporation, Nagoya, Japan), which was used to measure the refractive power of the anterior and posterior corneal surfaces as well as the tilt and decentration of the preoperative crystalline lens and postoperative IOLs. Preoperative IOL power calculations using the Sanders–Retzlaff–Kraft/Theoretical (SRK/T), Barrett Universal II, and Haigis formulas were obtained using axial length, anterior chamber depth, and corneal power measured using OA-2000, with IOL constants of 119.1 for SRK/T; 1.94 for Barrett Universal II; and a0=1.39, a1=0.4, and a2=0.1 for Haigis, as suggested by the manufacturer, and surgically induced astigmatism (SIA) of 0.25 D.
Anterior capsulotomy and lens fragmentation were performed using a LenSx Femtosecond Laser (Alcon Vision LLC, Fort Worth, TX, USA), corneal incisions were made using a 2.4-mm scalpel from the superior side, and phacoemulsification was performed using a Centurion Vision System (Alcon Vision LLC, Fort Worth, TX, USA) by the same surgeon in all cases. Intraoperative wavefront measurement was obtained using the ORA system optimized with the global AnalyzOR database and did not include personal optimization. Intraoperative toric IOL alignment was conducted using a VERION Image Guided System (Alcon Vision LLC, Fort Worth, TX, USA) and the ORA System. AcrySof IQ PanOptix IOLs or AcrySof IQ PanOptix toric IOLs, such as TFNT00, TFNT30, TFNT40, TFNT50, or TFNT60 (Alcon Vision LLC, Fort Worth, TX, USA) were implanted. Spherical power and cylinder power were determined by the surgeon based on preoperative measurement values, preoperative IOL power calculation, and intraoperative measurement using ORA. Toric IOLs were used in eyes with against-the-rule (ATR) ACA ≥0.75 D and in eyes with with-the-rule (WTR) astigmatism ≥1.0 D.
Endpoints
The primary endpoints of this study were refractive prediction error (RPE); absolute RPE; percentage of eyes with an absolute RPE ≤0.25 D, ≤0.50 D, ≤0.75 D, ≤1.0 D; residual astigmatism and its correlation with related factors such as preoperative/postoperative refractive astigmatism, intraoperative ORA–measured astigmatism, preoperative/postoperative TCA, and preoperative/postoperative ACA.19
The RPE for each IOL power calculation and ORA was defined as the difference in the predicted refractive spherical equivalent determined preoperatively/intraoperatively and the actual spherical equivalent of the subjective refractive value determined 1–3 months postoperatively. In this analysis, the SRK/T, Barrett Universal II, and Haigis formulas were optimized specifically for the study population by adding the mean RPE for each formula to the predicted spherical equivalent for each eye, thereby driving the mean RPE to zero. 19
Secondary endpoints included monocular BCVA, UCVA, uncorrected intermediate visual acuity (UCIVA) at 60 cm, and uncorrected near visual acuity (UCNVA) at 40 cm. Spherical equivalent and cylinder were also noted.
Statistical Analyses
Statistical analysis was performed using JMP Pro 15 2.1 software (SAS Inc, Cary, NC, USA). A sample size of 180 eyes was targeted such that the power of the intergroup differences in absolute RPE for ORA and absolute RPE for preoperative IOL power calculation by OA-2000 exceeded 90% (paired t-test; two-sided significance level of 5%).
Data of patient characteristics were summarized using descriptive statistics. RPE, percentage of absolute RPE (≤0.25 D, ≤0.50 D, ≤0.75 D, ≤1.0 D) measured using ORA, and the respective IOL power calculation formulas (SRK/T, Barrett Universal II, and Haigis) are expressed as mean±standard deviation (SD) and percentages, respectively. Absolute RPE was expressed as median values. Paired t-test and Wilcoxon signed-rank test were used to compare the RPE and absolute RPE between the ORA and IOL power formula groups. Cochran’s Q test was used to compare the percentages of absolute RPE, and McNemar’s test was used to compare the percentages of absolute RPE between groups.
Of the 123 eyes implanted with non-toric IOLs, CASIA2 data were available for 76 eyes, which were analyzed to describe residual astigmatism and related factors, including axial length, ORA-measured astigmatism, and preoperative and postoperative values of refractive astigmatism, ACA, TCA, and lens tilt and decentration. This was followed by a correlation analysis using Pearson’s product-moment correlation (r) and Spearman’s rank correlation coefficient (ρ). A scatter plot matrix for residual astigmatism and select variables, such as ORA-measured astigmatism, preoperative ACA, and preoperative TCA, was also obtained.
Results
Patient Disposition, Demographics, and Baseline Characteristics
The study population included 180 eyes of 101 patients who had undergone cataract surgery and met the selection criteria (Figure 1). Patient demographics and preoperative baseline data are summarized in Table 1. The mean±SD age of the 69 female (68.3%) and 32 male (31.7%) patients enrolled in the study was 67.2±8.0 years.
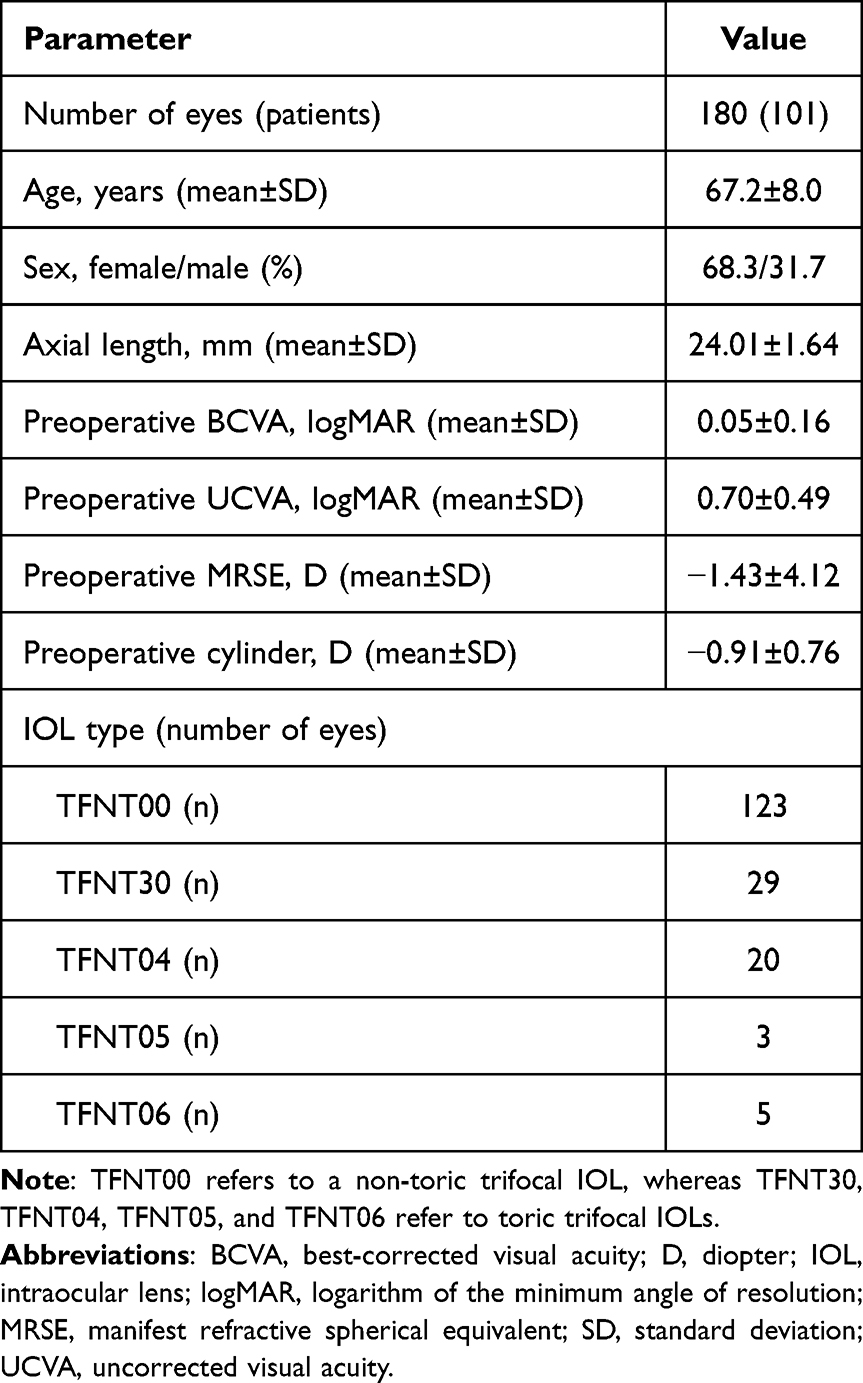 |
Table 1 Demographics and Baseline Characteristics of the Study Population |
 |
Figure 1 Patient disposition. Abbreviations: IOL, intraocular lens; logMAR, logarithm of the minimum angle of resolution. |
Overall, 123 (68.3%) eyes had indications for non-toric trifocal IOLs, whereas 57 (31.7%) eyes were considered suitable for toric trifocal IOLs. The mean±SD axial length of the eyes was 24.01±1.64 mm, whereas the preoperative spherical equivalent and cylinder were −1.43±4.12 D and −0.91±0.76 D, respectively.
Cases were selected retrospectively and consecutively from the date of approval by the Ethical Review Committee until a total of 180 eligible eyes was reached. Eight cases were excluded due to a postoperative BCVA <0.0 logMAR and one case each was excluded due to corneal opacity and a lack of follow-up data (Figure 1).
RPE and Absolute RPE
Before optimization, the mean±SD RPE using ORA was −0.06±0.30 D, which differed significantly (p<0.0001) from that calculated using the SRK/T (0.22±0.40 D), Barrett Universal II (0.22±0.32 D), and Haigis (−0.33±0.41 D) formulas. Significant differences in RPE were also noted between the SRK/T and Haigis formulas and between the Barrett Universal II and Haigis formulas (p<0.0001). After optimization, the mean±SD RPE using ORA was 0.00±0.30 D compared to 0.00±0.40 D, 0.00±0.32 D, and 0.01±0.41 D using the SRK/T, Barrett Universal II, and Haigis formulas, respectively (Figure 2A).
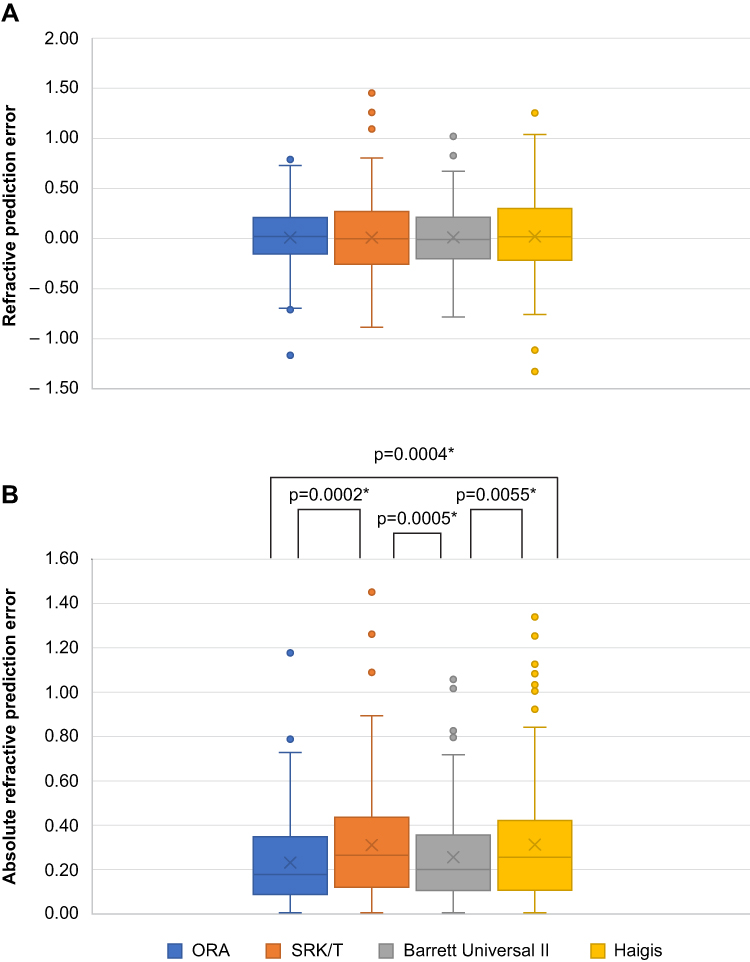 |
Figure 2 (A) Refractive prediction error and (B) absolute refractive prediction error. Abbreviations: ORA, Optiwave Refractive Analysis; SRK/T, Sanders–Retzlaff–Kraft/Theoretical formula. Notes: Figure 2A shows mean refractive prediction error expressed in diopters. Figure 2B shows median absolute refractive prediction error. *p<0.05 was considered significant. |
Before optimization, the median absolute RPE was 0.17 D, 0.28 D, 0.25 D, and 0.37 D in eyes measured using ORA and the SRK/T, Barrett Universal II, and Haigis formulas showing significant differences (ORA vs SRK/T [p<0.0001]; ORA vs Barrett Universal II [p=0.0039]; ORA vs Haigis [p <0.0001]) respectively. After optimization, the median absolute RPE was 0.19 D, 0.25 D, 0.20 D, and 0.26 D in eyes measured using ORA and the SRK/T, Barrett Universal II, and Haigis formulas respectively. As shown in Figure 2B, even after optimization significant differences were noted on comparing the median absolute RPE of ORA with the SRK/T (p=0.0002) and Haigis (p=0.0004) formulas and of the Barrett Universal II formula with the SRK/T (p=0.0005) and Haigis (p=0.0055) formulas.
Percentages of Absolute RPE
Before optimization, an absolute RPE of ≤0.50 D was noted in 87.8%, 73.3%, 78.9%, and 63.9% of the eyes using ORA and the SRK/T, Barrett Universal II, and Haigis formulas, respectively. After optimization, an absolute RPE of ≤0.50 D was noted in 92.8%, 83.3%, 88.3%, and 81.1% of the eyes using ORA and the SRK/T, Barrett Universal II, and Haigis formulas, respectively (Figure 3). Percentages of absolute RPE were significantly higher with ORA than with the SRK/T (p=0.0093) and Haigis (p=0.0018) formulas but was not significantly different from the Barrett Universal II formula (p=0.2071).
 |
Figure 3 Percentage of eyes with absolute refractive prediction error. Abbreviations: D, diopter; ORA, Optiwave Refractive Analysis; SRK/T, Sanders–Retzlaff–Kraft/Theoretical formula. Note: *p<0.05 was considered significant. |
Residual Astigmatism in Eyes with Non-Toric Trifocal IOLs and Associated Factors
Preoperative WTR corneal astigmatism was observed in 75.0% (57 of 76) of eyes implanted with non-toric IOLs. The mean±SD residual astigmatism in non-toric IOL eyes (N=76) was 0.46±0.39 D, and the centroid value±SD was 0.29 D@0±0.53 D. The mean±SD preoperative ACA, TCA, and intraoperative ORA–measured astigmatism were 0.60±0.40 D, 0.51±0.27 D, and 0.65±0.35 D, respectively, with a centroid value±SD of 0.41 D@88±0.60 D, 0.09 D@96±0.57 D, and 0.37 D@10±0.64 D, respectively (Table 2).
 |
Table 2 Residual Astigmatism and Individual Components of Astigmatism in Eyes with Non-Toric Trifocal IOLs (n=76) |
The mean±SD postoperative ACA (0.63±0.37 D, centroid value±SD: 0.21 D@84±0.70 D) and TCA (0.57±0.28 D, centroid value±SD: 0.13 D@173±0.62 D) were not significantly different compared with the preoperative values (p=0.48 and p=0.12, respectively). Preoperatively, the mean±SD objective refractive astigmatism, subjective astigmatism, and irregular astigmatism (higher-order aberrations) were 0.95±0.57 D, 0.65±0.50 D, and 0.25±0.05 D, respectively. However, a significant decrease in objective refractive astigmatism to 0.74±0.37 D (p=0.003) and subjective residual astigmatism to 0.46±0.39 D (p=0.002) was observed postoperatively (Table 2).
Compared with the preoperative tilt of the crystalline lens (4.40±1.30°), the postoperative tilt of the IOL was higher (4.66±1.53°, p=0.088), while the decentration decreased (0.71±4.58° preoperative to 0.21±0.12° postoperative, p=0.175); however, these differences were not significant.
Residual astigmatism positively correlated with preoperative objective refractive astigmatism (r=0.2925, p=0.0109), intraoperative ORA–measured astigmatism (r=0.5555, p<0.0001), postoperative objective refractive astigmatism (r=0.8188, p<0.0001), and postoperative TCA (r=0.4051, p=0.0003) and negatively correlated with preoperative ACA (r=−0.3541, p=0.0017; Table 3; Figure 4).
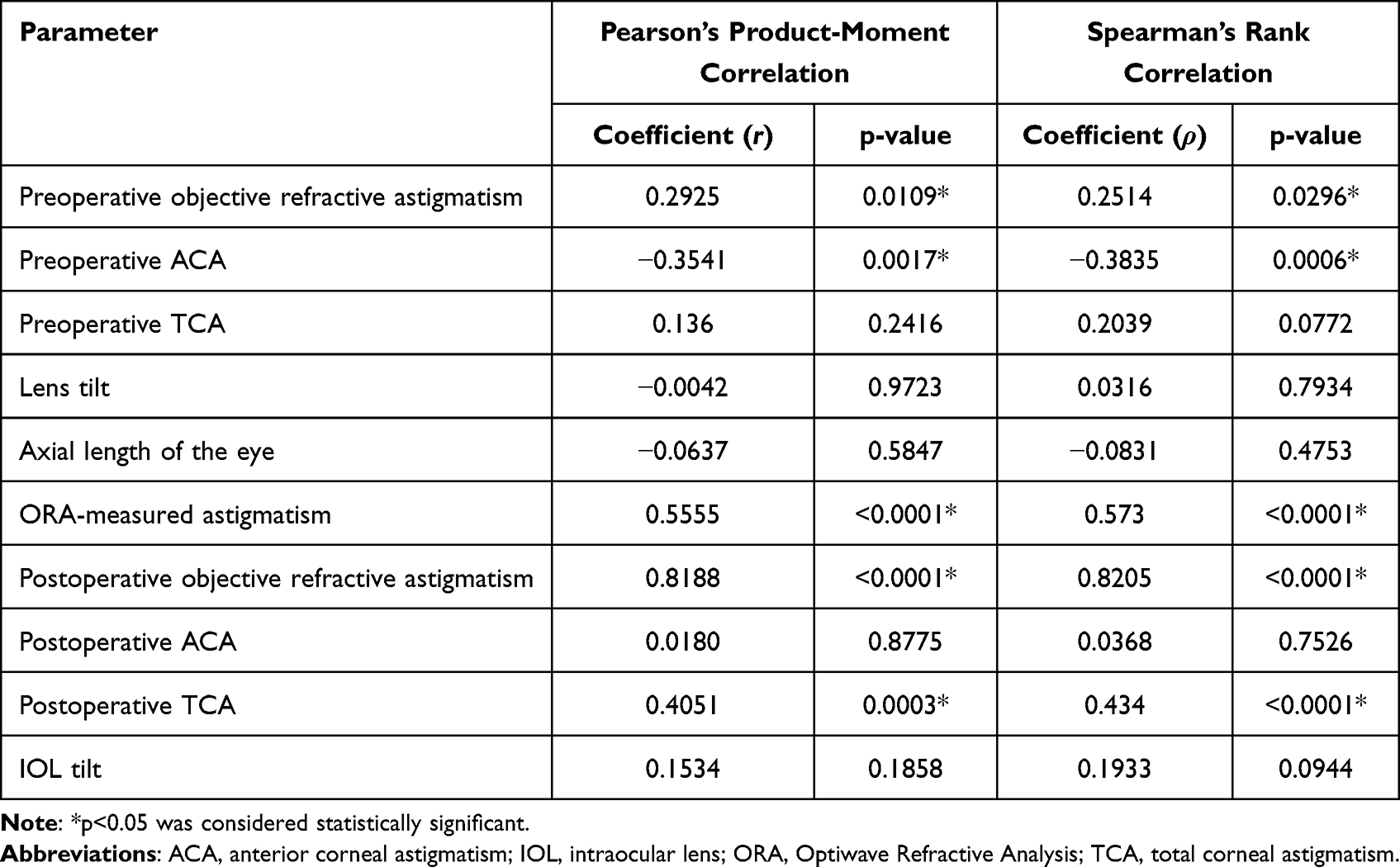 |
Table 3 Correlation Coefficients for Residual Astigmatism and Individual Astigmatic Components in Eyes with Non-Toric Trifocal IOLs (n=76) |
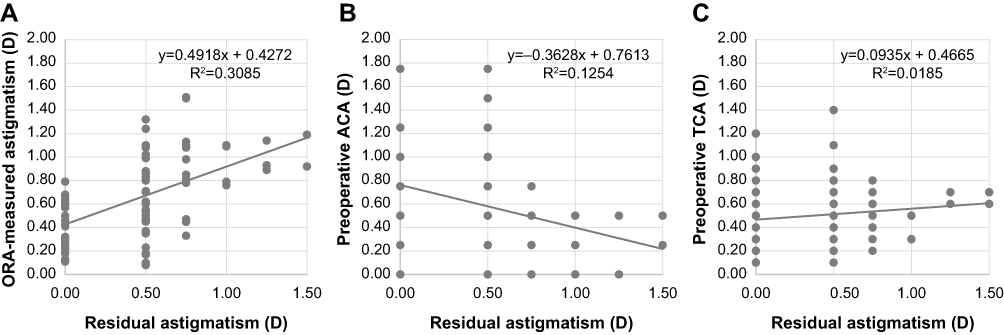 |
Figure 4 Scatter plot showing correlation of residual astigmatism with (A) ORA-measured astigmatism, (B) preoperative ACA, and (C) preoperative TCA in eyes with non-toric trifocal IOLs. Abbreviations: ACA, anterior corneal astigmatism; D, diopter; IOL, intraocular lens; ORA, Optiwave Refractive Analysis; TCA, total corneal astigmatism. |
Visual Acuity
Table 4 summarizes the mean±SD postoperative outcomes of the cohort. Postoperative BCVA (−0.12±0.06 logMAR) and UCVA (−0.04±0.10 logMAR) showed an improvement compared with preoperative values (BCVA: 0.05±0.16 logMAR; UCVA: 0.70±0.49 logMAR). All eyes achieved a postoperative BCVA that was equivalent or improved compared with the preoperative status. Postoperatively, UCIVA was 0.02±0.09 logMAR and UCNVA was 0.03±0.08 logMAR.
 |
Table 4 Postoperative Outcomes |
Discussion
Real-world data comparing the accuracy of refractive prediction determined using ORA with that using IOL power calculation formulas in eyes implanted with trifocal IOL along with quantification of residual astigmatism and its correlating factors have not been adequately explored; hence, this retrospective, observational study was conducted. In this study, the ability of ORA to predict the refractive accuracy of IOLs was superior to that of the SRK/T and Haigis formulas, and postoperative residual astigmatism was shown to correlate positively with multiple parameters and negatively with preoperative ACA.
It has been previously reported that among power calculation formulas, the Barrett Universal II formula performed the best for TFNT IOLs in the overall study population, except for eyes with a short axial length, particularly when they had higher astigmatism, wider white-to-white corneal diameter, and shorter axial length.20 Another study reported that RPE tended to be within ±0.25 D for most eyes analyzed using the Haigis formula and within ±0.50 D for all eyes analyzed using the Barrett Universal II formula among eyes with an axial length between 22.0 mm and 24.5 mm.21
In this study, we estimated the preoperative RPE for 180 eyes using three well-known IOL power formulas, including the third-generation SRK/T formula and the fourth-generation Barrett Universal II and Haigis formulas, and compared them with the intraoperative prediction of ORA to determine the most suitable method for IOL power selection in eyes with TFNT lenses.22 Although the accuracy of the IOL power formulas improved with optimization, the accuracy of refractive prediction for TFNT IOLs was the highest with ORA compared with that calculated using the SRK/T, Barrett Universal II, and Haigis formulas even after optimization of the IOL power formulas. This is congruent to the findings of Blaylock et al, wherein 83.9% and 95.6% of ORA-measured eyes had an absolute predicted error as low as 0.25 D and 0.50 D, respectively, and residual astigmatism of 0.25 D and 0.50 D was detected in 90.5% and 97.8% of 137 eyes, respectively, outperforming the back calculations derived using preoperative planned power.4 ORA allows real-time power calculation during the aphakic measurement phase, as well as cylinder power and axis positioning for toric IOLs during the pseudophakic phase.15
The outcome of refractive and cataract surgeries depends upon insight into the distribution of different astigmatic components, their relationship, and the counteractive or superimposed effect between ACA and ocular residual astigmatism based on the type of astigmatism, ie, ATR or WTR.23,24 Interestingly, a negative correlation between residual astigmatism and preoperative ACA was observed in this study, congruent to the findings of Lin J who found that ACA was offset by ocular residual astigmatism in 84.8% (140) of eyes.24 This can be due to the greater appearance of the posterior cornea’s ATR astigmatic component in cases of low WTR astigmatism of the anterior cornea as a consequence of steep meridian incision from the superior side.25 Steep meridian incision on the anterior corneal surface can induce off-steep meridian changes, leading to a torsional effect on TCA.26
Changes in the posterior corneal surface have been shown to correlate with residual astigmatism as the posterior corneal surface usually possesses an ATR astigmatism with a mean of 0.37 D.27–29 Furthermore, relying solely on ACA may overestimate true postoperative refractive astigmatism in WTR and underestimate it in ATR, leading to cylindrical inaccuracy after cataract surgery.8,11 In the present study, residual astigmatism positively correlated with postoperative TCA and not with postoperative ACA. This is consistent with previous reports, suggesting that the posterior corneal surface contributes to residual astigmatism.8,11,12
Despite indications for non-toric IOLs during preoperative planning, cases with postoperative residual astigmatism ≥0.75 D were identified. Apart from the anterior corneal surface effect, residual astigmatism can be influenced by several factors, such as posterior corneal surface effect, IOL tilt or decentration, and refractive changes in the anterior and posterior corneal surfaces from cataract incisions.30 In the present study, ORA-measured astigmatism showed a significant positive correlation with residual astigmatism, although preoperative ACA and preoperative TCA did not. This lack of significance between preoperative TCA and residual astigmatism could be attributed to refractive changes in the anterior and posterior corneal surfaces from cataract incisions.30,31 However, the ORA device confers surgeons the added advantage of measuring intraoperative aphakic astigmatism following changes in corneal shape due to corneal incisions, irrespective of lenticular astigmatism.4,32 Therefore, the accurate measurement of total refractive astigmatism in the eye plays an important role in predicting residual astigmatism. In addition to the correlation, centroid values of ORA-measured astigmatism and postoperative residual astigmatism were similar and contrasted with those of preoperative and postoperative ACA and preoperative TCA in this study. These findings suggest that while deliberating between the need for toric or non-toric lenses, toric lenses may be considered in eyes depending on the results of intraoperative measurements by ORA to reduce postoperative residual astigmatism. Some studies have estimated residual astigmatism using ORA versus preoperative planning using keratometry. Woodcock et al reported that compared with preoperative planning with preoperative biometry measurements, intraoperative aberrometry improved the postoperative astigmatism of eyes to ≤0.50 D (76.6% versus 89.2%, respectively) and reduced the mean postoperative refractive astigmatism (0.36±0.35 D versus 0.29±0.28 D, respectively) in one month.15 Blaylock et al reported that the proportion of eyes with postoperative refractive astigmatism ≤0.50 D and mean postoperative refractive astigmatism in TFNT was significantly lower using ORA (97.8%, mean±SD: 0.07 D±0.19 D) versus the back calculation with preoperative biometry measurements (80.3%, 0.31±0.33 D).4 Spekreijse et al have described double-angle vector plots, which show that astigmatism difference (SIA) between postoperative manifest refraction and intraoperative ORA was not significant (centroid: 0.06@115°±0.59), while showing a considerable difference between postoperative manifest refraction and preoperative keratometric astigmatism (centroid: 0.63@14°±0.50).32
To our knowledge, this is the first study to assess residual astigmatism in non-toric trifocal IOL eyes arising from different ocular components using an ORA system, in addition to comparing the accuracy of refractive prediction determined using ORA with established IOL power formulas. However, this single-center study design being applicable only in eyes with non-toric IOLs limits the generalizability of the results. The open-label, uncontrolled, retrospective aspects of this study do not rule out potential bias. Furthermore, the nonhomogeneity resulting from the analysis of a single eye in some patients and both eyes in other patients as well as the lack of a correlation analysis between both eye samples may also have impacted the strength of the study outcomes. Future studies can consider using an intra-class coefficient so that the correlation between both eyes of the same patient, if any, can be adjusted for in the analysis.
Conclusion
ORA is useful for improving postoperative refractive accuracy by providing real-time intraoperative guidance to surgeons and may help in determining the need for trifocal toric lens use in astigmatic eyes with cataracts. Residual astigmatism positively correlated with preoperative astigmatism, intraoperative ORA–measured astigmatism, postoperative astigmatism, and postoperative TCA and negatively correlated with preoperative ACA volume in eyes with non-toric trifocal IOLs. Desirable refractive outcomes and improved visual acuity were observed in patients postoperatively.
Abbreviations
ACA, anterior corneal astigmatism; ATR, against-the-rule; BCVA, best-corrected visual acuity; D, diopter; IOL, intraocular lens; logMAR, logarithm of the minimum angle of resolution; ORA, Optiwave Refractive Analysis; PCA, posterior corneal astigmatism; RPE, refractive prediction error; SD, standard deviation; SIA, surgically induced astigmatism; SRK/T, Sanders–Retzlaff–Kraft/Theoretical; TCA, total corneal astigmatism; UCIVA, uncorrected intermediate visual acuity; UCNVA, uncorrected near visual acuity; UCVA, uncorrected visual acuity; WTR, with-the-rule.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, K.W., upon reasonable request.
Acknowledgments
Medical writing support was provided by Nidhi Kona, MSc, of Cactus Life Sciences (part of Cactus Communications) and funded by Alcon Japan Ltd.
Funding
The study was supported with an investigator-initiated study grant (IIT#63631365) from Alcon Japan Ltd.
Disclosure
Dr Keizo Watanabe reports grants from Alcon Japan Ltd., during the conduct of the study; personal fees from Alcon Japan Ltd., outside the submitted work. The author declares that he has no other competing interests.
References
1. Zvorničanin J, Zvorničanin E. Premium intraocular lenses: the past, present and future. J Curr Ophthalmol. 2018;30(4):287–296. doi:10.1016/j.joco.2018.04.003
2. Alcon. Alcon AcrySof IQ PanOptix trifocal intraocular lens shows superior visual performance in head-to-head trial post-cataract surgery [media release]; 2018. Available from: https://www.alcon.com/media-release/alcon-acrysofr-iq-panoptixr-trifocal-intraocular-lens-shows-superior-visual.
3. Hayashi K, Yoshida M, Igarashi C, Hirata A. Effect of refractive astigmatism on all-distance visual acuity in eyes with a trifocal intraocular lens. Am J Ophthalmol. 2021;221:279–286. doi:10.1016/j.ajo.2020.07.051
4. Blaylock JF, Hall B. Astigmatic results of a diffractive trifocal toric IOL following intraoperative aberrometry guidance. Clin Ophthalmol. 2020;14:4373–4378. doi:10.2147/OPTH.S285711
5. Day AC, Dhariwal M, Keith MS, et al. Distribution of preoperative and postoperative astigmatism in a large population of patients undergoing cataract surgery in the UK. Br J Ophthalmol. 2019;103(7):993–1000. doi:10.1136/bjophthalmol-2018-312025
6. Rubenstein JB, Raciti M. Approaches to corneal astigmatism in cataract surgery. Curr Opin Ophthalmol. 2013;24(1):30–34. doi:10.1097/ICU.0b013e32835ac853
7. Abulafia A, Koch DD, Holladay JT, Wang L, Hill W. Pursuing perfection in intraocular lens calculations: IV. Rethinking astigmatism analysis for intraocular lens-based surgery: suggested terminology, analysis, and standards for outcome reports. J Cataract Refract Surg. 2018;44(10):1169–1174. doi:10.1016/j.jcrs.2018.07.027
8. Sano M, Hiraoka T, Ueno Y, Itagaki H, Ogami T, Oshika T. Influence of posterior corneal astigmatism on postoperative refractive astigmatism in pseudophakic eyes after cataract surgery. BMC Ophthalmol. 2016;16(1):212. doi:10.1186/s12886-016-0391-1
9. Llorens-Quintana C, Pavlatos E, Thaware O, et al. Accuracy of OCT-derived net corneal astigmatism measurement. J Cataract Refract Surg. 2022;48(3):267–274. doi:10.1097/j.jcrs.0000000000000766
10. Reitblat O, Levy A, Kleinmann G, Abulafia A, Assia EI. Effect of posterior corneal astigmatism on power calculation and alignment of toric intraocular lenses: comparison of methodologies. J Cataract Refract Surg. 2016;42(2):217–225. doi:10.1016/j.jcrs.2015.11.036
11. Savini G, Næser K. An analysis of the factors influencing the residual refractive astigmatism after cataract surgery with toric intraocular lenses. Invest Ophthalmol Vis Sci. 2015;56(2):827–835. doi:10.1167/iovs.14-15903
12. Koch DD, Ali SF, Weikert MP, Shirayama M, Jenkins R, Wang L. Contribution of posterior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg. 2012;38(12):2080–2087. doi:10.1016/j.jcrs.2012.08.036
13. Davison JA, Potvin R. Preoperative measurement vs intraoperative aberrometry for the selection of intraocular lens sphere power in normal eyes. Clin Ophthalmol. 2017;11:923–929. doi:10.2147/OPTH.S135659
14. Cionni RJ, Dimalanta R, Breen M, Hamilton C. A large retrospective database analysis comparing outcomes of intraoperative aberrometry with conventional preoperative planning. J Cataract Refract Surg. 2018;44(10):1230–1235. doi:10.1016/j.jcrs.2018.07.016
15. Woodcock MG, Lehmann R, Cionni RJ, Breen M, Scott MC. Intraoperative aberrometry versus standard preoperative biometry and a toric IOL calculator for bilateral toric IOL implantation with a femtosecond laser: one month results. J Cataract Refract Surg. 2016;42(6):817–825. doi:10.1016/j.jcrs.2016.02.048
16. Bissen-Miyajima H, Ota Y, Hayashi K, Igarashi C, Sasaki N. Results of a clinical evaluation of a trifocal intraocular lens in Japan. Jpn J Ophthalmol. 2020;64(2):140–149. doi:10.1007/s10384-019-00712-4
17. Alcon. Alcon introduces AcrySof IQ PanOptix Trifocal IOL in the U.S., the first and only FDA-approved trifocal lens [media release];2019. Avalaible from: https://www.alcon.com/media-release/alcon-introduces-acrysof-iq-panoptix-trifocal-iol-us-first-and-only-fda-approved.
18. Hovanesian JA. Comparison of preoperative measurements with intraoperative aberrometry in predicting need for correction in eyes with low astigmatism undergoing cataract surgery. Clin Ophthalmol. 2021;15:2189–2196. doi:10.2147/OPTH.S314618
19. Wang L, Koch DD, Hill W, Abulafia A. Pursuing perfection in intraocular lens calculations: III. Criteria for analyzing outcomes. J Cataract Refract Surg. 2017;43(8):999–1002.20. doi:10.1016/j.jcrs.2017.08.003
20. Choi A, Kwon H, Jeon S. Accuracy of theoretical IOL formulas for Panoptix intraocular lens according to axial length. Sci Rep. 2021;11(1):7346. doi:10.1038/s41598-021-86604-5
21. Mălăescu M, Stanca HT, Tăbăcaru B, Stănilă A, Stanca S, Danielescu C. Accuracy of five intraocular lens formulas in eyes with trifocal lens implant. Exp Ther Med. 2020;20(3):2536–2543. doi:10.3892/etm.2020.8891
22. Xia T, Martinez CE, Tsai LM. Update on intraocular lens formulas and calculations. Asia Pac J Ophthalmol. 2020;9(3):186–193. doi:10.1097/APO.0000000000000293
23. Gab-Alla AA. Contributions of anterior corneal and ocular residual astigmatism to autorefraction astigmatism in a myopic adult sample. Clin Ophthalmol. 2020;14:2125–2134. doi:10.2147/OPTH.S262167
24. Lin J. The contribution of ocular residual astigmatism to anterior corneal astigmatism in refractive astigmatism eyes. Sci Rep. 2021;11(1):1018. doi:10.1038/s41598-020-80106-6
25. Mohammadi SF, Khorrami-Nejad M, Hamidirad M. Posterior corneal astigmatism: a review article. Clin Optom. 2019;11:85–96. doi:10.2147/OPTO.S210721
26. Park Y, Kim HS. Torsional and flattening effect on corneal astigmatism after cataract surgery: a retrospective analysis. BMC Ophthalmol. 2017;17(1):10. doi:10.1186/s12886-017-0399-1
27. Miyake T, Shimizu K, Kamiya K, Pan C-W. Distribution of posterior corneal astigmatism according to axis orientation of anterior corneal astigmatism. PLoS One. 2015;10(1):e0117194. doi:10.1371/journal.pone.0117194
28. Nemeth G, Berta A, Lipecz A, Hassan Z, Szalai E, Modis LJ. Evaluation of posterior astigmatism measured with scheimpflug imaging. Cornea. 2014;33(11):1214–1218. doi:10.1097/ICO.0000000000000238
29. Tutchenko L, Patel S, Voytsekhivskyy O, Skovron M, Horak O. The impact of changes in corneal back surface astigmatism on the residual astigmatic refractive error following routine uncomplicated phacoemulsification. J Ophthalmol. 2020;2020:7395081. doi:10.1155/2020/7395081
30. Holladay JT, Pettit G. Improving toric intraocular lens calculations using total surgically induced astigmatism for a 2.5 mm temporal incision. J Cataract Refract Surg. 2019;45(3):272–283. doi:10.1016/j.jcrs.2018.09.028
31. Hirnschall N, Hoffmann PC, Draschl P, Maedel S, Findl O. Evaluation of factors influencing the remaining astigmatism after toric intraocular lens implantation. J Refract Surg. 2014;30(6):394–400. doi:10.3928/1081597X-20140429-01
32. Spekreijse LS, Bauer NJC, van den Biggelaar FJ, et al. Predictive accuracy of an intraoperative aberrometry device for a new monofocal intraocular lens. J Cataract Refract Surg. 2022;48(5):542–548. doi:10.1097/j.jcrs.0000000000000791
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effects of Angle Kappa on Clinical Results and Patient-Reported Outcomes After Implantation of a Trifocal Intraocular Lens
Sandoval HP, Potvin R, Solomon KD
Clinical Ophthalmology 2022, 16:1321-1329
Published Date: 27 April 2022
Refractive Outcomes Following Trifocal Intraocular Lens Implantation in Post-Myopic LASIK and PRK Eyes
Blaylock JF, Hall BJ
Clinical Ophthalmology 2022, 16:2129-2136
Published Date: 1 July 2022
Visual Function After Implantation of Trifocal and Trifocal Toric Intraocular Lenses Using Intraoperative Aberrometry
Brissette A, Cole B, Hall B
Clinical Ophthalmology 2024, 18:1547-1554
Published Date: 30 May 2024
Accuracy of Intraoperative Aberrometry-Based Prediction of Postoperative Refraction and Astigmatism After Novel Toric Intraocular Lens Implantation
Otani A
Clinical Ophthalmology 2025, 19:2681-2689
Published Date: 11 August 2025