Back to Journals » Clinical Ophthalmology » Volume 19
Accuracy of Intraoperative Aberrometry-Based Prediction of Postoperative Refraction and Astigmatism After Novel Toric Intraocular Lens Implantation
Authors Otani A
Received 18 April 2025
Accepted for publication 23 July 2025
Published 11 August 2025 Volume 2025:19 Pages 2681—2689
DOI https://doi.org/10.2147/OPTH.S534932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Atsushi Otani
Otani Eye Clinic, Iwade, Wakayama, Japan
Correspondence: Atsushi Otani, Otani Eye Clinic, 264-1 Nakabusa, Iwade-shi, Wakayama, 649‑6215, Japan, Tel +81 736 67 7012, Email [email protected]
Purpose: This study prospectively assessed the refractive and astigmatism prediction accuracy of intraoperative aberrometry, Optiwave Refractive Analysis (ORA), in eyes implanted with Clareon toric intraocular lenses (IOLs).
Patients and Methods: Patients with age-related cataracts who underwent phacoemulsification and toric IOL implantation using ORA were prospectively included in this single-center study. The absolute refractive prediction error (RPE) and rate of RPE for ORA, Sanders–Retzlaff–Kraft/Theoretical (SRK/T), and Barrett Universal II were evaluated 3 months after surgery. Uncorrected visual acuity (UCVA), residual astigmatism, refractive astigmatism prediction error, and the difference between the preoperatively planned axis and actual inserted axis recommended by ORA were assessed.
Results: Eighty eyes (80 patients, mean age: 75.0 ± 8.8 years) were included in this study. Mean ± standard deviation (SD) of preoperative corneal astigmatism was 1.91 ± 1.03 D. The median absolute RPE values for ORA, SRK/T, and Barrett Universal II were 0.17, 0.14, and 0.14 D, respectively. At the 3-month follow-up after surgery, the mean ± SD of UCVA and residual astigmatism were 0.06 ± 0.16 logarithm of the minimum angle of resolution and 0.43 ± 0.48 D, respectively. The refractive astigmatism prediction errors were 0.11 D in the centroid for both ORA and the Barrett toric formula, at 67° and 63°, respectively. The mean absolute values were 0.38 D for ORA and 0.41 D for the Barrett toric formula. The median absolute value of the axis difference between the planned and actual inserted axes based on ORA was 4.00°.
Conclusion: The accuracy of ORA in the prediction of spherical refraction and astigmatism was comparable to that of the preoperative IOL calculation formula in eyes with Clareon toric IOLs. ORA is a useful tool for determining IOL power and improving preoperative corneal astigmatism.
Keywords: astigmatism, intraoperative aberrometry, refractive prediction error, toric intraocular lenses
Introduction
Cataract surgery is one of the most common surgeries performed worldwide. Preoperative accurate refractive prediction is important for ensuring postoperative patient satisfaction. Furthermore, reducing residual astigmatism is important for patient satisfaction and visual outcomes after cataract surgery.1 The persistence of low-level residual astigmatism, such as 0.5–0.75 D after cataract surgery affects visual performance.1
Toric intraocular lenses (IOLs) reduce residual astigmatism after cataract surgery. The correction of astigmatism with toric IOLs provides better outcomes than that with other procedures, such as the corneal relaxing incision method,2 and, therefore, toric IOL constitutes the most popular solution for the correction of preoperative corneal astigmatism. However, the effect of astigmatism correction with a toric IOL is diminished by toric misalignment from the target axis or rotation following toric IOL implantation. Every degree of misalignment from the target axis reduces the effect of astigmatism correction by approximately 3.3%.3–6 Furthermore, toric IOL-based correction of astigmatism is influenced by preoperative corneal measurements of both the anterior and posterior surfaces. If only the measurements from the anterior surface of the cornea are used for cylindrical power calculations, the predicted residual astigmatism will be overestimated and underestimated in patients having with-the-rule and against-the-rule astigmatism, respectively.7,8 Therefore, it is preferable to use an IOL calculation formula that incorporates details of posterior corneal astigmatism in the preoperative IOL calculation formula.
The Optiwave Refractive Analysis (ORA) system (Alcon Vision LLC, Fort Worth, TX, USA) is an intraoperative wavefront-aberration analyzer system that enables surgeons to measure the whole-eye refraction, including the anterior and posterior cornea, and determine cylindrical and spherical IOL powers in the aphakic eye.9,10 In addition, ORA can indicate an axis position for the toric IOL that maintains residual astigmatism within 0.5 D in the pseudophakic eye. Although some studies have reported that ORA conferred better refractive and astigmatism outcomes compared with those predicted using preoperative IOL power calculation formulas, other studies have reported that ORA is equal to or inferior to the preoperative IOL power calculation formulas in terms of refractive outcomes.9–11 Sometimes, the IOL power and toric axis recommended by ORA differ from the preoperatively planned IOL power and toric axis. This creates uncertainty or doubt in the IOL power determination and access by the surgeon.
To date, only limited data are available regarding the evaluation of refractive and astigmatism outcomes for ORA in eyes implanted with Clareon material toric IOLs.12 Therefore, this study evaluated the refractive prediction and refractive astigmatism prediction errors for ORA and compared them with those derived from the preoperative IOL calculation formulas in eyes implanted with Clareon toric IOLs.
Material and Methods
Study Design
This was a prospective observational single-site study and included patients who underwent cataract surgery and toric IOL implantation. The study protocol was reviewed and approved by the MINS institutional review board of an independent and nonprofit organization in Tokyo, Japan (approval number: 220220) and performed in accordance with the Ethical Guidelines for Medical and Biological Research Involving Human Subjects in Japan and the tenets of the Declaration of Helsinki. Written informed consent was obtained from all patients involved in this study. The included patients aged ≥50 years with cataract for whom cataract surgery with implantation of Clareon toric IOL (model: CNW0Tx, Alcon Vision LLC) or Clareon PanOptix toric IOL (model: CNWTTx, Alcon Vision LLC) was planned, and intraoperative aberrometry with ORA was conducted. The exclusion criteria were having underwent additional surgery between cataract surgery and 3 months postoperatively, a history of corneal transplantation and corneal refractive surgery, presence of corneal disease that affected or prevented accurate ORA measurements, presence of any ocular pathology, use of medications that affected visual acuity, or ciliary zonule. One eye from each patient was included in this study. In the case of patients who with both eyes eligible for inclusion, the first operated eye was selected for analysis to minimize selection bias and ensure consistency.
Surgery
Swept Source OCT biometer ARGOS® (ARGOS, Alcon Vision LLC) was used for preoperative ocular measurement and IOL power calculations with Sanders–Retzlaff–Kraft/Theoretical (SRK/T) and Barrett Universal II formulas. The cylindrical power was calculated using Barrett toric formula with the measurement values by the ARGOS and the surgically induced astigmatism (SIA) of 0.4 D. In this study, we used an arched knife, which is a slit knife with a curved blade creating a 2.9 mm arc-shaped incision (Mani, Inc. Tochigi, Japan). When converted to a standard incision size, this corresponds approximately to a 2.7-mm horizontal width. The incision was made along the steep meridian on the anterior surface of the cornea. The SIA value was selected based on our clinical experience optimized with the arched knife. The Barrett toric formula can account for posterior corneal curvature, either by incorporating predicted values or by using actual measurements obtained from devices such as the Pentacam. In our study, we used the Barrett toric formula with predicted posterior corneal astigmatism values. Cataract surgery with phacoemulsification and IOL implantation were performed by only one experienced surgeon (A.O). After removing the crystalline lens with the phacoemulsification using the Centurion® Vision System (Alcon Vision LLC), intraoperative wavefront measurements were performed using the ORA system. CNW0T or CNWTT0 toric IOLs were implanted into the capsule bag and the axis of the toric IOL was aligned according to the recommendations of ORA. Spherical power calculated using the Barrett Universal II formula and cylindrical power calculated using the Barrett toric formula, both based on measurements from the ARGOS biometer, were used as a reference preoperatively. However, in all cases, the final decision regarding both spherical and cylindrical IOL power was made based on recommendations provided by the ORA system, with the goal of targeting emmetropia or slight myopia.
Endpoints and Postoperative Examination
The primary endpoint of this study was the absolute refractive error (RPE). Additional endpoints were rate of eyes with an absolute RPE ≤0.25, ≤0.50, ≤0.75, ≤1.0 D, monocular best corrected visual acuity (BCVA), monocular uncorrected visual acuity (UCVA), residual astigmatism, refractive astigmatism prediction error, axis difference between preoperative planning axis and actual inserted axis based on ORA recommendation, and toric IOL rotation after the surgery was completed.
The RPE was defined as the difference between the predicted spherical equivalent (SE) and the actual subjective SE at 3 months after surgery. Visual acuity and subjective refraction were examined at a distance of 5 m. Monocular BCVA, monocular UCVA, and subjective refraction were evaluated at 1 week and 3 months postoperatively.
Statistical Analysis
Statistical analysis was conducted with JMP® Pro 18 software (SAS Inc, Cary, NC, USA). The sample size for the mean absolute RPE with a confidence level of 95% and confidence width of 0.10 D was 68 eyes, when the standard deviation (SD) of the RPE was 0.41 D.13 Considering a dropout rate of 20%, the final sample size was estimated as 82 eyes.
Data on patient demographics, visual acuity, refraction, and RPE for ORA, SRK/T, and Barrett Universal II formulas were summarized using the descriptive statistics of the mean, SD, and median. The mean RPE was adjusted to zero for ORA and each IOL calculation formula to eliminate systematic errors from the chosen IOL constant based on reported method.14 The rate of eyes with absolute RPE (≤0.25, ≤0.50, ≤0.75, and ≤1.0 D) was described as percentages. The Friedman test was used for comparison of absolute RPE in the group. Monocular BCVA and UCVA were converted into logarithm of the minimum angle of resolution (logMAR) visual acuity. Cumulative histogram of the preoperative corneal and postoperative refractive subjective (residual) astigmatism was described with astigmatism ≤0.25, ≤0.5, ≤0.75, ≤1.0, ≤1.5, and ≤2.0 D. Vectors of the preoperative corneal astigmatism measured by the ARGOS and residual astigmatisms were plotted on double-angle plots. The vector of the refractive astigmatism prediction error for the Barrett toric formula and ORA was plotted on double angle plots. Wilcoxon signed-rank test was used for comparison of the refractive astigmatism prediction error between the Barrett toric formula and ORA.
Results
Patient Demographics
Table 1 shows the patient demographics. In total, 80 eyes of 80 participants who completed the 3-month postoperative follow-up were included from among 86 patients who were initially enrolled in this study. Overall, 6 patients were excluded because they lacked data for the 3-month follow-up visit. Of the 80 eyes, 9 had mild glaucoma and 1 an epiretinal membrane. No intra-or postoperative complications were observed. In total, 36 right eyes and 44 left eyes were selected for analysis. Among the 80 eyes included in the study, 62 received CNW0Tx and 18 received CNWTTx. A subgroup analysis showed no significant differences in any of the evaluated endpoints between the two groups. (p > 0.05 for all comparisons) ORA led to changes in the final IOL selection compared with the recommendation by preoperative Barrett formula. Specifically, the spherical power was modified in 54 eyes (68%) and the cylindrical power was adjusted in 59 eyes (74%) based on intraoperative ORA measurements.
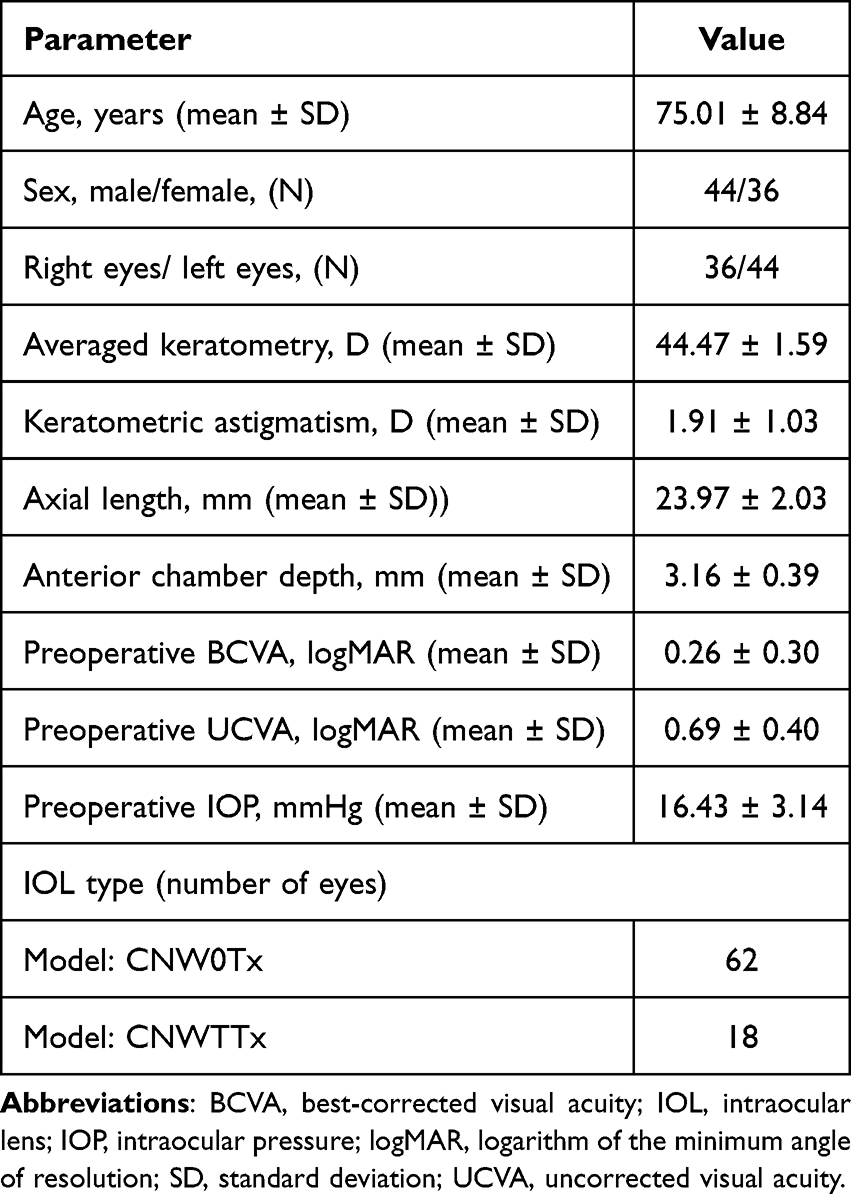 |
Table 1 Demographic Data of the Study Participants |
Refractive Prediction Error
The mean absolute RPE for ORA was 0.25 D (SD: 0.28, 95% confidence interval [CI]: 0.19–0.31). The median absolute RPE for ORA, SRK/T, and Barrett Universal II was 0.17, 0.14, and 0.14 D, respectively (p=0.8682, Friedman test) (Table 2). The rates of the absolute RPE within 0.25 D for ORA, SRK/T, and Barrett Universal II were 68.6%, 70.0%, and 68.4%, and those within 0.5 D were 83.8%, 90.0%, and 83.5%, respectively (Table 2).
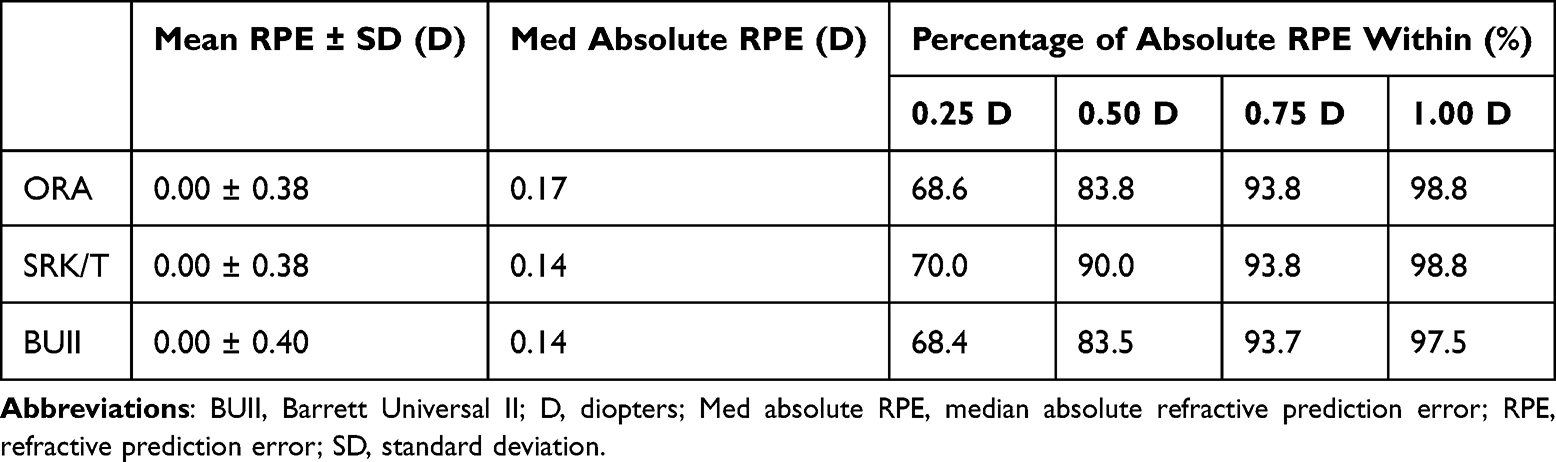 |
Table 2 Refractive Outcomes in All Eyes |
Visual Acuities
Table 3 summarizes the postoperative visual acuity and refractive outcomes 1 week and 3 months postoperatively. The monocular UCVA at 1 week after surgery was 0.09 ± 0.18 logMAR (median: 0.05 [−0.18–0.70]) and that at 3 months after surgery was 0.06 ± 0.16 logMAR (median: 0.02 [−0.18–0.82]). The monocular BCVA at 3 months was −0.03 ± 0.12 logMAR (median: −0.08 [−0.18–0.30]).
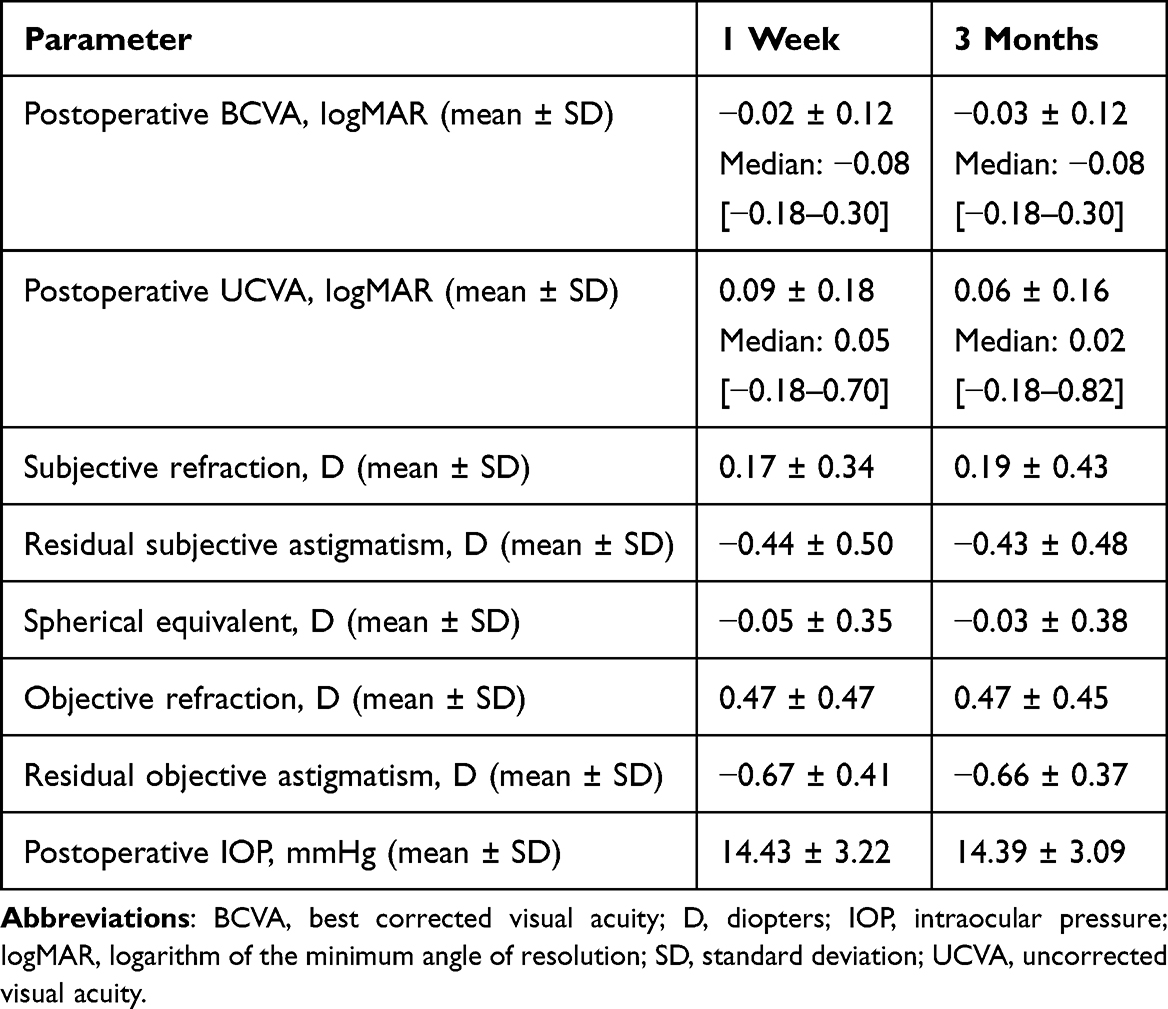 |
Table 3 Postoperative Visual and Refractive Outcomes |
Astigmatism
Figure 1A shows a cumulative histogram of the magnitude of preoperative corneal and postoperative residual astigmatism. The preoperative corneal astigmatism and residual astigmatism at 3 months were 1.91 ± 1.03 and 0.43 ± 0.48 D, respectively. The centroid of preoperative corneal astigmatism was 1.04 D at 183° and that of residual astigmatism was 0.04 D at 83° (Figure 1B and C, respectively). Double-angle vector plots for preoperative corneal and residual astigmatism are shown in Figure 1B and C, respectively. The postoperative refractive astigmatism prediction error for the Barrett toric formula was 0.11 D at 63° in centroid and 0.41 D in mean absolute value, whereas the postoperative refractive astigmatism prediction error for ORA was 0.11 D at 67° in centroid and 0.38 D in mean absolute value (x axis; p=0.8685, y axis; p=0.9357, paired t test) (Figure 2A and B, respectively).
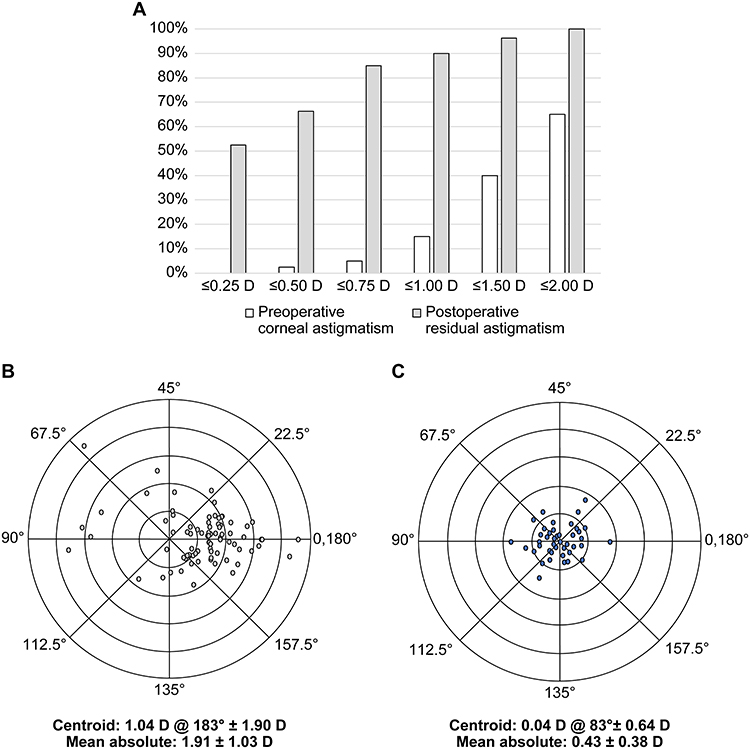 |
Figure 1 (A) Cumulative histogram of the magnitude of preoperative corneal and postoperative residual astigmatism; (B) double-angle plots of preoperative corneal astigmatism; and (C) double-angle plots of postoperative residual astigmatism. |
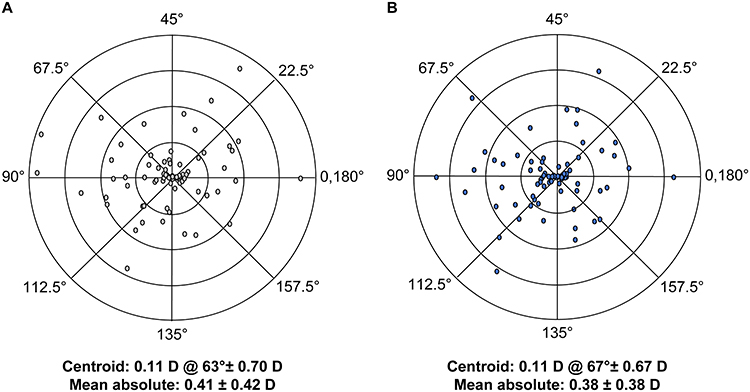 |
Figure 2 Double-angle plots of prediction errors regarding postoperative refractive astigmatism. (A) Barrett toric formula; and (B) Optiwave Refractive Analysis. |
Axis Difference
The difference between the preoperatively planned axis using the Barrett toric formula and the actual inserted axis based on ORA recommendation was calculated for 76 eyes, as shown in Figure 3A. The difference was 0.09 ± 7.79°, and the median absolute value of the difference was 4.00°. The maximum difference was observed at 21°; approximately 63.2% of the eyes were within 5.0° and 80.3% were within 10.0°. The toric IOL rotation from the end of the surgery was assessed in 53 eyes (Figure 3B). The median absolute value of rotation was 2.00°.
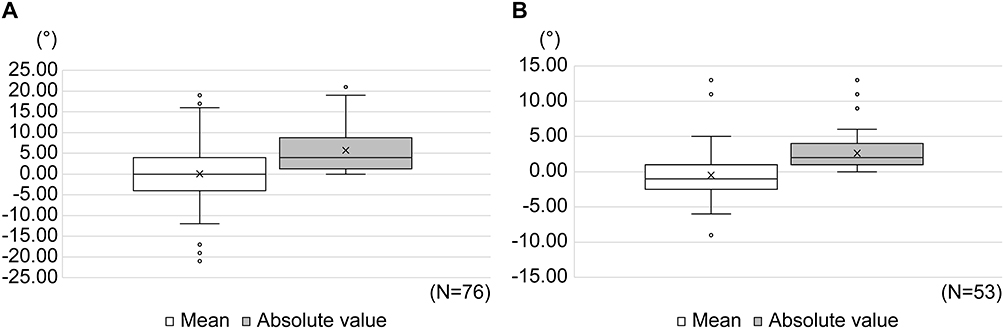 |
Figure 3 Distributions of mean (left) and absolute value (right). (A) The difference between the preoperative planning axis ascertained by the Barrett toric formula and the actual inserted axis based on the Optiwave Refractive Analysis recommendation; and (B) the toric IOL rotation from the end of surgery. |
Discussion
To achieve high postoperative patient satisfaction, it is important to meet the targeted refraction and reduce residual astigmatism by accurately measuring ocular components and predicting postoperative refraction and astigmatism. In the current study, the refractive and astigmatism accuracies of ORA predictions in eyes with Clareon toric IOLs were compared with those of preoperative IOL calculation formulas. The results showed that ORA provided accurate refractive and astigmatism predictions in eyes with Clareon toric IOLs.
In this study, the rate of the eyes with absolute RPE ≤0.5 D at 3 months after surgery was 83.8% for ORA, consistent with the 84% rate for ORA after the optimization in eyes implanted with Clareon monofocal IOL- reported by Spekreijse et al.15 In addition, Melendez et al reported that the rate of the eyes with absolute RPE ≤0.5 D for ORA when using ARGOS and femtosecond laser was 75% in eyes with Clareon PanOptix toric IOL.12 The refractive prediction for preoperative IOL calculation formulas using ARGOS in eyes with Clareon IOLs was accurate and the rates of the eyes with absolute RPE ≤0. 5D ranged from 69.7% to 86.3%.13,16 The results of refractive prediction for the SRK/T and Barrett Universal II formulas using the ARGOS were accurate, with 83.5% and 90.0% rates, respectively, for the eyes in the present study.
Several studies have used ORA to evaluate residual astigmatism after cataract surgery with toric IOL implantation. The rate of eyes with residual astigmatism ≤0.5 D in eyes implanted with AcrySof IQ toric IOL using ORA were 75.4%–89.4%.17–26 Furthermore, the rate of eyes with residual astigmatism ≤0.5 D in eyes implanted with Clareon PanOptix toric IOL using ORA, digital image tracking, and femtosecond laser was 80%.14 In the present study, the rate was 63%, which was lower than that reported in the previous study.14 Although most previous studies used a femtosecond laser for cataract surgery and only one type of toric IOL, in the current study, we did not use a femtosecond laser, we included two types of Clareon toric IOLs, and we used a specific arched knife to create a corneal incision at the steep median. All these factors could have led to the differences between the results of the previous studies and that of the present study.
ORA can measure whole-eye refraction and astigmatism, including posterior corneal astigmatism in aphakic eyes, and intraoperatively recommends the axis and cylindrical power for toric IOL implantation. In contrast, the Barrett toric formula can estimate posterior corneal astigmatism with an as yet unpublished algorithm and preoperatively recommends the axis and cylindrical power for toric IOL implantation. The results of the present study showed that both ORA and the Barrett toric formula accurately predicted astigmatism. In addition, the distribution of the double-angle vector plot of ORA in the refractive astigmatism prediction error is very similar to that of the Barrett toric formula. Despite the slight difference between the planning axis using the Barrett toric formula and the actual ORA-recommended inserted axis in this study, the difference in the axis did not affect the refractive astigmatism prediction error. Felipe et al reported that toric IOL rotation <10° changed the eye’s refraction by <0.5 D.6 The rate of the eyes with <10.0° axis difference was 80.3% in this study, which resulted in no effect on the refractive astigmatism prediction error.
In some cases, ORA had better prediction accuracy, whereas, in other cases, preoperative calculation formulas demonstrated better prediction accuracy.17,20 For instance, although ORA showed no clear advantage in eyes with post-radial keratotomy or short axial lengths, it was particularly effective in eyes with axial myopia, especially in reducing hyperopic surprises, compared with Barrett Universal II formulas.21–23 Furthermore, some reports indicated similar or slightly higher astigmatism prediction accuracy using predicted posterior corneal astigmatism than using the actual measured posterior corneal astigmatism.24–26 For the reasons stated above and the results from the current study, it may be better for determining IOL power to consider comprehensive calculated results including the modern preoperative IOL power calculation formula, such as the Barrett formula, as well as ORA, rather than making all decisions based on ORA. Future studies with larger sample size and predefined subgroup analyses are warranted to better guide the effective use of ORA in IOL power selection.
This study has some limitations. The number of included patients was relatively small for evaluating refractive accuracy. However, although most of the previous studies that evaluated refractive accuracy had a retrospective design, this study had a prospective design, and only one of the eyes from each patient was used for evaluation. These differences constitute the strengths of this study. Two types of Clareon IOLs were used in the study, which may increase the variation in the results. Future studies with only one type of IOL should be considered to confirm the refractive accuracy of ORA. Finally, we acknowledge that future studies may consider performing astigmatism analysis using objective refraction data as well, to provide a more comprehensive understanding of astigmatism prediction accuracy.
Conclusion
ORA can effectively predict visual and refractive outcomes in eyes with Clareon toric IOL implantation. The accuracy of ORA in the prediction of the postoperative refractive index and astigmatism was equivalent to that of the ARGOS-based preoperative IOL calculation formula. ORA is a useful tool for determining IOL power and improving preoperative corneal astigmatism.
Abbreviations
ORA, Optiwave Refractive Analysis; IOL, intraocular lens; RPE, refractive prediction error; SRK/T, Sanders–Retzlaff–Kraft/Theoretical; UCVA, uncorrected visual acuity; SD, standard deviation; BCVA, best corrected visual acuity; SE, spherical equivalent; logMAR, logarithm of the minimum angle of resolution.
Data Sharing Statement
Data that support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Informed Consent
The study protocol was approved by the MINS institutional review board of an independent and nonprofit organization (Tokyo, Japan, Approval number: 220220), and was performed in accordance with the tenets of the Declaration of Helsinki and the Ethical Guidelines for Medical and Biological Research Involving Human Subjects in Japan. Written informed consent for study participation was obtained from all participants.
Acknowledgments
The author would like to thank Apex LLC. for their editorial assistance in manuscript preparation, which was funded by Alcon Japan Ltd.
Funding
This study was supported by an investigator-initiated study grant (IIT#73582245) from Alcon Vision LLC. The funder had no role in the study design, collection, analysis, or interpretation of data; writing of the report; or decision to submit the article for publication.
Disclosure
Otani has received grants from Alcon Vision LLC.
References
1. Lehmann RP, Houtman DM. Visual performance in cataract patients with low levels of postoperative astigmatism: full correction versus spherical equivalent correction. Clin Ophthalmol. 2012;6:333–338. doi:10.2147/OPTH.S28241
2. Kessel L, Andresen J, Tendal B, Erngaard D, Flesner P, Hjortdal J. Toric intraocular lenses in the correction of astigmatism during cataract surgery: a systematic review and meta-analysis. Ophthalmology. 2016;123(2):275–286. doi:10.1016/j.ophtha.2015.10.002
3. Shimizu K, Misawa A, Suzuki Y. Toric intraocular lenses: correcting astigmatism while controlling axis shift. J Cataract Refract Surg. 1994;20(5):523–526. doi:10.1016/s0886-3350(13)80232-5
4. Novis C. Astigmatism and toric intraocular lenses. Curr Opin Ophthalmol. 2000;11(1):47–50. doi:10.1097/00055735-200002000-00007
5. Jjk M, Tseng SS. Simple method for accurate alignment in toric phakic and aphakic intraocular lens implantation. J Cataract Refract Surg. 2008;34(10):1631–1636. doi:10.1016/j.jcrs.2008.04.041
6. Felipe A, Artigas JM, Díez-Ajenjo A, García-Domene C, Alcocer P. Residual astigmatism produced by toric intraocular lens rotation. J Cataract Refract Surg. 2011;37(10):1895–1901. doi:10.1016/j.jcrs.2011.04.036
7. Sano M, Hiraoka T, Ueno Y, Itagaki H, Ogami T, Oshika T. Influence of posterior corneal astigmatism on postoperative refractive astigmatism in pseudophakic eyes after cataract surgery. BMC Ophthalmol. 2016;16(1):212. doi:10.1186/s12886-016-0391-1
8. Savini G, Næser K. An analysis of the factors influencing the residual refractive astigmatism after cataract surgery with toric intraocular lenses. Invest Ophthalmol Vis Sci. 2015;56(2):827–835. doi:10.1167/iovs.14-15903
9. Blaylock JF, Hall B. Astigmatic results of a diffractive trifocal toric IOL following intraoperative aberrometry guidance. Clin Ophthalmol. 2020;14:4373–4378. doi:10.2147/OPTH.S285711
10. Davison JA, Potvin R. Preoperative measurement vs intraoperative aberrometry for the selection of intraocular lens sphere power in normal eyes. Clin Ophthalmol. 2017;11:923–929. doi:10.2147/OPTH.S135659
11. Soifer M, Passi SF, Wisely CE, et al. Refractive outcomes using intraoperative aberrometry for highly myopic, highly hyperopic, and post-refractive eyes. J Refract Surg. 2021;37(9):609–615. doi:10.3928/1081597X-20210609-03
12. Melendez RF, Nguyen TH, Solis AI, Ortiz D, Moezzi C, Hall B. Outcomes after implantation of a trifocal toric intraocular lens using intraoperative aberrometry, digital image tracking, and femtosecond laser. Clin Ophthalmol. 2024;18:2033–2039. doi:10.2147/OPTH.S460060
13. Watanabe K. Accuracy of predicted refraction using two swept-source optical coherence biometers and an intraoperative aberrometer. J Cataract Refract Surg. 2025;43:999–1002. doi:10.1097/j.jcrs.0000000000001628
14. Wang L, Koch DD, Hill W, Abulafia A. Pursuing perfection in intraocular lens calculations: III. Criteria for analyzing outcomes. J Cataract Refract Surg. 2017;43(8):999–1002. doi:10.1016/j.jcrs.2017.08.003
15. Spekreijse LS, Bauer NJC, van den Biggelaar FJHM, et al. Predictive accuracy of an intraoperative aberrometry device for a new monofocal intraocular lens. J Cataract Refract Surg. 2022;48(5):542–548. doi:10.1097/j.jcrs.0000000000000791
16. Matsumoto Y, Karasawa Y, Azuma Y, Suzuki N. Implantation of hydrophobic acrylic toric intraocular lens with high-water contents using swept-source optical coherence tomography biometer integrated with a surgical guiding system. Clin Ophthalmol. 2024;18:1117–1124. doi:10.2147/OPTH.S456609
17. Davison JA, Makari S, Potvin R. Clinically relevant differences in the selection of toric intraocular lens power in normal eyes: preoperative measurement vs intraoperative aberrometry. Clin Ophthalmol. 2019;13:913–920. doi:10.2147/OPTH.S205352
18. Woodcock MG, Lehmann R, Cionni RJ, Breen M, Scott MC. Intraoperative aberrometry versus standard preoperative biometry and a toric IOL calculator for bilateral toric IOL implantation with a femtosecond laser: one-month results. J Cataract Refract Surg. 2016;42(6):817–825. doi:10.1016/j.jcrs.2016.02.048
19. Blaylock JF, Hall BJ. Clinical outcomes of monofocal toric IOLs using digital tracking and intraoperative aberrometry. Clin Ophthalmol. 2021;15:3593–3600. doi:10.2147/OPTH.S322523
20. Solomon KD, Sandoval HP, Potvin R. Evaluating the relative value of intraoperative aberrometry versus current formulas for toric IOL sphere, cylinder, and orientation planning. J Cataract Refract Surg. 2019;45(10):1430–1435. doi:10.1016/j.jcrs.2019.05.023
21. Hill DC, Sudhakar S, Hill CS, et al. Intraoperative aberrometry versus preoperative biometry for intraocular lens power selection in axial myopia. J Cataract Refract Surg. 2017;43:505–510.
22. Sudhakar S, Hill DC, King TS, et al. Intraoperative aberrometry versus preoperative biometry for intraocular lens power selection in short eyes. J Cataract Refract Surg. 2019;45:719–724.
23. Curado SX, Hida WT, Vilar CMC, Ordones VL, Chaves MAP, Tzelikis PF. Intraoperative aberrometry versus preoperative biometry for IOL power selection after radial keratotomy: a prospective study. J Refract Surg. 2019;35(10):656–661. doi:10.3928/1081597X-20190913-01
24. Shammas HJ, Yu F, Shammas MC, Jivrajka R, Hakimeh C. Predicted vs measured posterior corneal astigmatism for toric intraocular lens calculations. J Cataract Refract Surg. 2022;48(6):690–696. doi:10.1097/j.jcrs.0000000000000819
25. Yang S, Byun YS, Kim HS, Chung SH. Comparative accuracy of Barrett toric calculator with and without posterior corneal astigmatism measurements and the Kane toric formula. Am J Ophthalmol. 2021;231:48–57. doi:10.1016/j.ajo.2021.05.028
26. Yang Z, Zhou Y, Jin T, Li J. An evaluation of the accuracy of toric intraocular lens power calculation based on measured total corneal refractive power. Indian J Ophthalmol. 2023;71(2):541–546. doi:10.4103/ijo.IJO_1539_22
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of Refractive Accuracy of ORA and the Factors Impacting Residual Astigmatism in Patients Implanted with Trifocal IOLs During Cataract Surgery: A Retrospective Observational Study
Watanabe K
Clinical Ophthalmology 2022, 16:2491-2503
Published Date: 10 August 2022
Evaluation of the Accuracy of Modern Toric Intraocular Lens Formulas Based on Anterior Corneal Measurements
Matsumoto Y
Clinical Ophthalmology 2026, 20:590881
Published Date: 23 March 2026
Refractive Outcomes of a Low-Addition Refractive, Rotationally Asymmetric Bifocal IOL and Its Toric Version: A Comparative Cohort Study of 316 Eyes
Lognon A, Matagrin B, Agard E, El Chehab H, Verrecchia S, Levron A, Chudzinski R, Billant J, Goissaud-Mignard A, Fenniri I, Dot C
Clinical Ophthalmology 2026, 20:583057
Published Date: 1 May 2026