")
Back to Journals » Infection and Drug Resistance » Volume 13
The Existence of High Bacterial Resistance to Some Reserved Antibiotics in Tertiary Hospitals in Tanzania: A Call to Revisit Their Use
Authors Mikomangwa WP , Bwire GM , Kilonzi M , Mlyuka H , Mutagonda RF , Kibanga W, Marealle AI, Minzi O, Mwambete KD
Received 17 February 2020
Accepted for publication 3 June 2020
Published 17 June 2020 Volume 2020:13 Pages 1831—1838
DOI https://doi.org/10.2147/IDR.S250158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Wigilya P Mikomangwa,1,* George M Bwire,2,* Manase Kilonzi,1,* Hamu Mlyuka,1 Ritah F Mutagonda,1 Wema Kibanga,1 Alphonce Ignace Marealle,1 Omary Minzi,1 Kennedy D Mwambete2
1Department of Clinical Pharmacy and Pharmacology, Muhimbili University of Health and Allied Sciences, Dar-es-Salaam, Tanzania; 2Department of Pharmaceutical Microbiology, Muhimbili University of Health and Allied Sciences, Dar-es-Salaam, Tanzania
*These authors contributed equally to this work
Correspondence: Wigilya P Mikomangwa Email [email protected]
Background: Antibiotic resistance poses burden to the community and health-care services. Efforts are being made at local, national and global level to combat the rise of antibiotic resistance including antibiotic stewardship. Surveillance to antibiotic resistance is of importance to aid in planning and implementing infection prevention and control measures. The study was conducted to assess the resistance pattern to cefepime, clindamycin and meropenem, which are reserved antibiotics for use at tertiary hospitals in Tanzania.
Methods: A hospital-based antibiotic resistance surveillance was conducted between July and November 2019 at Muhimbili National Hospital and Bugando Medical Center, Tanzania. All organisms isolated were identified based on colony morphology, Gram staining and relevant biochemical tests. Antibiotic susceptibility testing was performed on Muller-Hinton agar using Kirby-Bauer disc diffusion method. Antibiotic susceptibility was performed according to the protocol by National Committee for Clinical Laboratory Standards.
Results: A total of 201 clinical samples were tested in this study. Urine (39.8%, n=80) and blood (35.3%, n=71) accounted for most of the collected samples followed by pus (16.9%, n=34). The bacterial resistance to clindamycin, cefepime and meropenem was 68.9%, 73.2% and 8.5%, respectively. About 68.4% Staphylococcus aureus isolates were resistant to clindamycin whereby 56.3%, 75.6%, 93.8% and 100% of the tested Escherichia coli, Klebsiella spp, Pseudomonas aeruginosa and Enterobacter cloacae, respectively, were cefepime resistant. About 8.5% of isolated Klebsiella spp were resistant and 6.4% had intermediate susceptibility to meropenem. Also, Pseudomonas aeruginosa was resistant by 31.2% and 25% had intermediate susceptibility to meropenem.
Conclusion: The bacterial resistance to clindamycin and cefepime is high and low in meropenem. Henceforth, culture and susceptibility results should be used to guide the use of these antibiotics. Antibiotics with low resistance rate should be introduced to the reserve category and continuous antibiotic surveillance is warranted.
Keywords: antibiotic resistance, clindamycin, cefepime, meropenem, reserved antibiotics, bacteria, susceptibility pattern
Background
Antibiotic resistance is rising to a dangerous level and is a global concern; bacteria are adapting new resistance mechanisms and spreading them across the species and geographical location, thus threatening over-decade achievement to treat common infectious diseases.1,2 Antibiotic resistance is associated with prolonged length of hospital stay, increased treatment cost, morbidity and mortality.1,3,4 Recent data shows that, worldwide, more than 700,000 people die annually because of resistant superbugs and the trend is expected to reach 10 million deaths per annum in 2050.5 In the USA, more than 2.8 million people were infected by severe antibiotic resistant infections, and more than 35,000 die from these infections every year.6 The problem is even worse in developing countries. For instance, in 2012, approximately 19,400 and 56,500 neonates in Nigeria and India respectively died from severe antibiotic-resistant pathogens.3 Also, antibiotics resistance has immense negative effect on the economy. It is estimated that by 2030 if it is left unaddressed the world will incur annual cost of about 1 trillion US$.7
In 2017, the World Health Organization (WHO) published the list of most evolving bacteria which are the leading cause of health-care facility acquired infection worldwide and pose great threat to the public health in general; Enterococcus spp., Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Escherichia coli, collectively termed ESKAPE.3
A growing list of infections such as urinary tract infections, pneumonia, bloodstream infections, reproductive tract infections, and foodborne diseases are becoming harder, and sometimes impossible to treat as antibiotics become less effective.1,2,8 In places, where antibiotics can be bought for human or animal use without prescription, the emergence and spread of resistance is made worse.3,9 Similarly, in countries without standard treatment guidelines, antibiotics are often overprescribed by health workers and veterinarians and over-used by the public. In addition, over prescription of antibiotics has been mentioned to be the significant contributor of antibiotic resistance.10
In 2019 the WHO established a model list of essential medicines in which antibiotics are included.11 The categories establish the antibiotics to be prescribed at different levels of health-care facilities; access group (dispensaries, health centers), watch group (council hospitals) and reserved group (tertiary hospitals such as national, zonal, and specialized hospitals).11 The reserved antibiotics play as the last weapon when all other antibiotics have failed. Grouping of antibiotics in respective categories is country specific. The Tanzanian Ministry responsible for health implemented the recommendations through the National Essential Medicine List (NEMLIT).12 The Ministry has created the reserve group that consists of cefepime, clindamycin and meropenem.
Several studies have reported the failure of clindamycin, cefepime and meropenem in different parts of the world.3,4,13 For example, in Africa 70% of E. coli and 77% of K. pneumonia from clinical isolates were resistant to third-generation cephalosporin. Invasive isolate from Europe indicated about 8% of K. pneumonia, 19% of P. aeroginosa and 56% of A. baumannii isolated from blood and cerebral spinal fluid were resistant to carbapenem. In 2009, Mshana et al, reported inducible resistance to occur in MRSA isolated at Bugando Medical Center (BMC), Tanzania; about 61% (16/26) of MRSA exhibited inducible clindamycin resistance.14 Tanzania has also reported resistance to meropenem from clinical isolates particularly Pseudomonas spp.15 Since categorizing of clindamycin, cefepime and meropenem in 2017 to reserve group, information on the susceptibility profile is scarce. Therefore, regular surveillance on the resistance profile of antibiotics is required to plan and implement infection prevention and control measures. Also, regular surveillance is also needed to evaluate the effectiveness of antimicrobial stewardship measures that have been implemented (like antibiotic restriction policies).
Methods
The Aim, Design and Setting of the Study
The study was conducted between July and November 2019. The study described the susceptibility pattern of antibiotics reserved for use at tertiary hospitals in Tanzania. The antibiotics were meropenem, cefepime and clindamycin. Two tertiary hospitals were involved in this study; the national and zonal hospital. The two tertiary teaching hospitals were Muhimbili National Hospital (MNH) and Bugando Medical Center (BMC) located at Dar es Salaam and Mwanza regions in Tanzania. MNH is a National Referral Hospital and University Teaching Hospital with 1500-bed facility, attending 1000 to 1200 outpatients per week, admitting 1000 to 1200 inpatients per week. The diagnostic laboratory department at MNH is the leading diagnostic laboratory in Tanzania. Bugando Medical Centre (BMC) representing Zonal hospital has 950-bed capacity, serves a population of about 16 million people and attends around 300,000 patients each year. Both MNH and BMC clinical microbiology laboratories are accredited with the international standard ISO 15189:2007.
Sample Size and Participant’s Characteristics
The overall size of sample was obtained using statistical formula for sample size calculation of cross-section studies.36 The prevalence of carbapenems resistance of 5.3%,15 with clinical differences of 4% and Z-score of 1.96, assuming 10% of inappropriately collected samples (duplicated isolates or contaminated with normal flora). A minimum of 201 clinical isolates were statistically powered to describe the susceptibility pattern in the selected study sites. The entry point was the microbiology laboratories in the study sites. The microbiology request forms were reviewed and the socio-demographic and clinical information on the microbiological request form were documented on the case report form (CRF).
Laboratory Procedures
Gram Stain, Culture and Identification
This was performed at the respective hospital (MNH & BMC) where organism from the clinical samples was isolated, cultured and identified according to their laboratory protocol. Direct Gram stain films were performed to examine the presence of microorganisms in the sample. Depending on the nature of the sample (throat swab, urine, stool, blood, pus or sputum) microbiological culture was performed using appropriate culture media and conditions as per microbiology laboratory protocol. All organisms isolated were identified based on colony morphology, Gram staining and relevant biochemical tests.37,38
Antibiotic Susceptibility Testing
Antibiotic susceptibility testing was performed on Muller-Hinton agar using Kirby-Bauer disc diffusion method at BMC and MNH clinical microbiology laboratory. Antibiotic susceptibility on the selected antibiotic discs; cefepime (30µg), clindamycin (2µg) and meropenem (10µg), was performed according to the protocol by Clinical and Laboratory Standards (CLSI).39
Interpretation and Reporting of the Results
Using the published CLSI guidelines, the susceptibility or resistance of the organism to each drug tested were determined.39 For each drug, the zone size was indicated on the recording sheet as susceptible (S), intermediate (I), or resistant (R) based on the interpretation chart.37
Quality Control
The American Type Culture Collection (ATCC) standard bacteria corresponding to each clinical isolate was used as control microorganisms for instance.39
Data Analysis
The collected microbiological information, socio-demographic and clinical data were extracted from the CRF to Microsoft excel, coded and analyzed using Statistical Package for Social Sciences (SPSS) version 23. The frequency distribution and proportion of identified bacteria per type of sample collected were summarized. The proportion of resistant bacteria per antibiotic (clindamycin, cefepime and meropenem) was determined. Enterococci are intrinsically resistant to cephalosporin such as cefepime and clindamycin, therefore such data were excluded in the final analysis. Patients’ age (in years) was categorized as ≤12 (children) and >12 (adult) as per MNH and BMC admission criteria. The differences in proportion of categorical variables were compared by Fisher’s exact or Pearson’s Chi-Square test. The two-tailed p-value of less than 0.05 was considered statistically significant.
Results
Socio-Demographic Characteristics and Type of Samples Collected
A total of 201 clinical samples were collected and met the criteria for inclusion in the study and final analysis. Male patients were majority of participants (51.4%) with age above 12years old (57.9%) (Table 1). Urine (39.8%, n=80) and blood (35.3%, n=71) accounted for most of the collected samples followed by pus (16.9%, n=34). Most of the blood samples were collected from children (46.8%) than adults (27.4%) (p-value<0.001). High proportion of pus (22.6%) and sputum (9.4%) samples were collected from adults while 48.1% of urine samples were collected from children (p-value<0.001). The one throat swab sample was collected from a child.
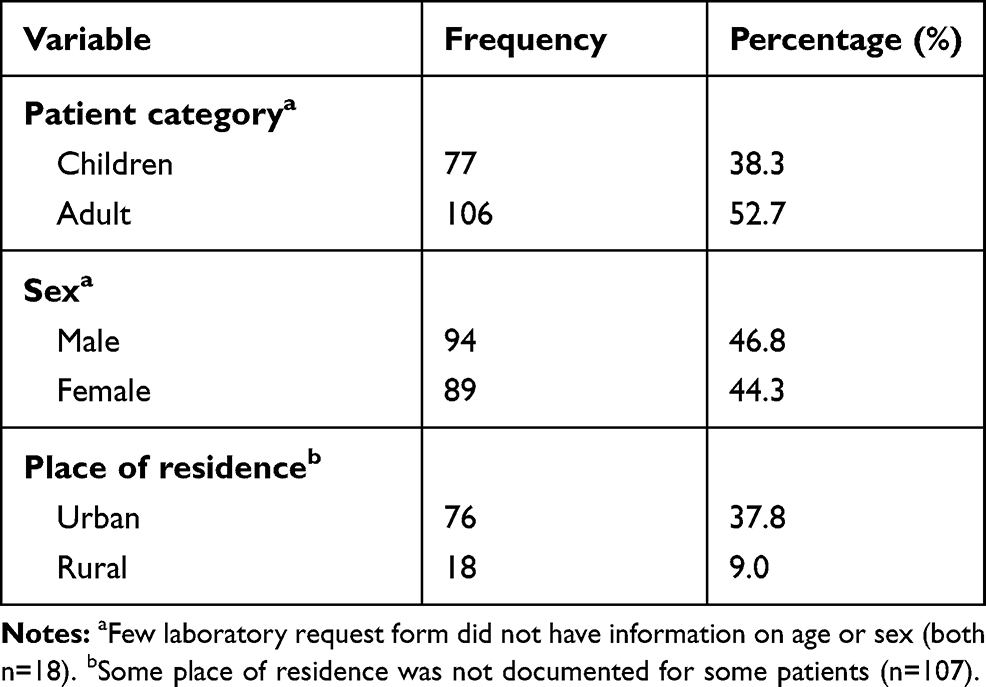 |
Table 1 Socio-Demographic Characteristics of Patients from Which the Samples Were Collected |
Culture results
Most (64.2%) of clinical isolates were found to be Gram negative strains. The distribution of type of strain (Gram negative or positive) did not differ by age groups (p-value=0.88). The most identified bacteria were S. aureus (28.4%), Klebsiella spp (23.4%), followed by Escherichia coli (17.9%). Staphylococcus aureus (56.3%) was the leading bacteria isolated from blood followed by Klebsiella spp (22.5%) while E. coli was highly (32.5%) found in urine samples. The highest proportion (38.5%) of Pseudomonas aeruginosa was found in sputum samples (Table 2).
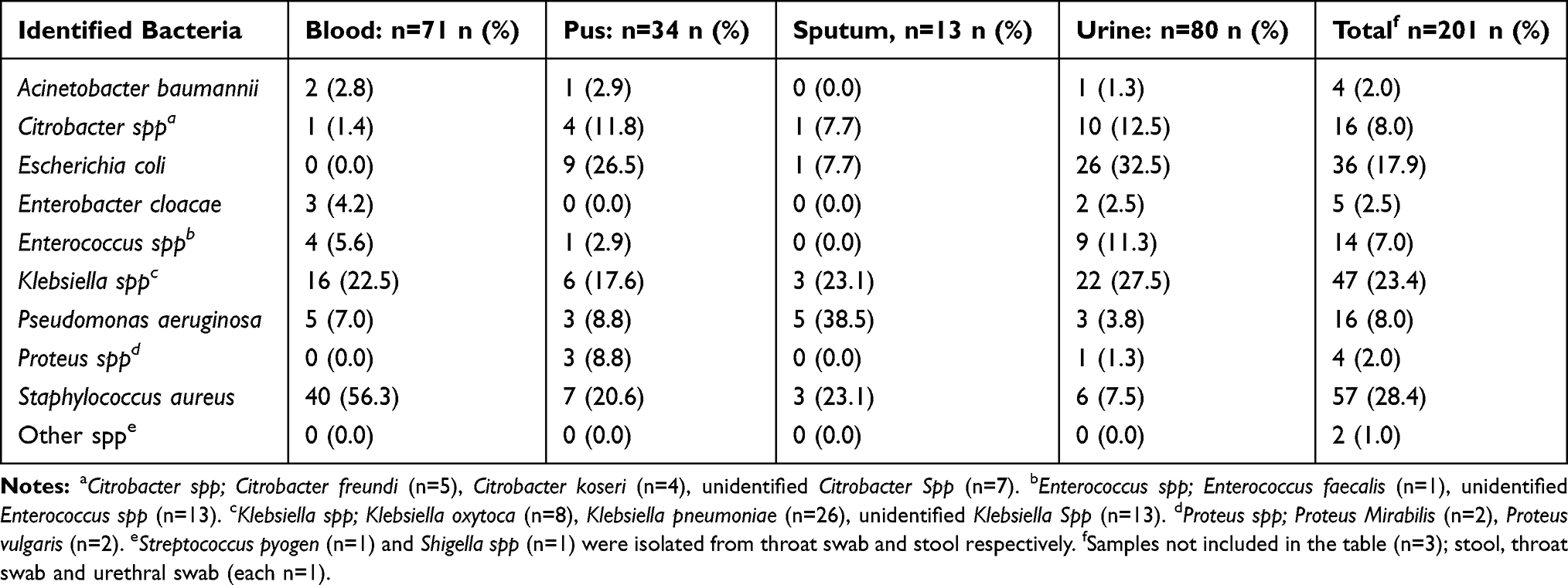 |
Table 2 Bacterial Isolates Distribution by Specimens |
Resistance Patterns of the Tested Bacteria
Resistance to Clindamycin
The Gram positive pathogens tested for susceptibility were S. aureus and Streptococcus pyogen. The overall proportion Gram positive pathogens resistant to clindamycin was 68.9%. Whereby 68.4% (n=57) of S. aureus were resistant to clindamycin.
Resistance to Cefepime
A total of 127 bacterial isolates were subjected to susceptibility test against cefepime. The overall proportion of Gram negative bacteria resistant to cefepime was 73.2%. Only 15.0% of isolates were susceptible to cefepime. Of 45 Klebsiella spp tested for susceptibility to cefepime, 75.6% were resistant and only 11.1% were susceptible. Whereas 32 isolates of E. coli tested for susceptibility to cefepime; 56.3% were resistant and 21.9% were susceptible. Also, sixteen (16) P. aeruginosa isolated were tested for susceptibility to cefepime of which 93.8% were found to be resistant (Table 3).
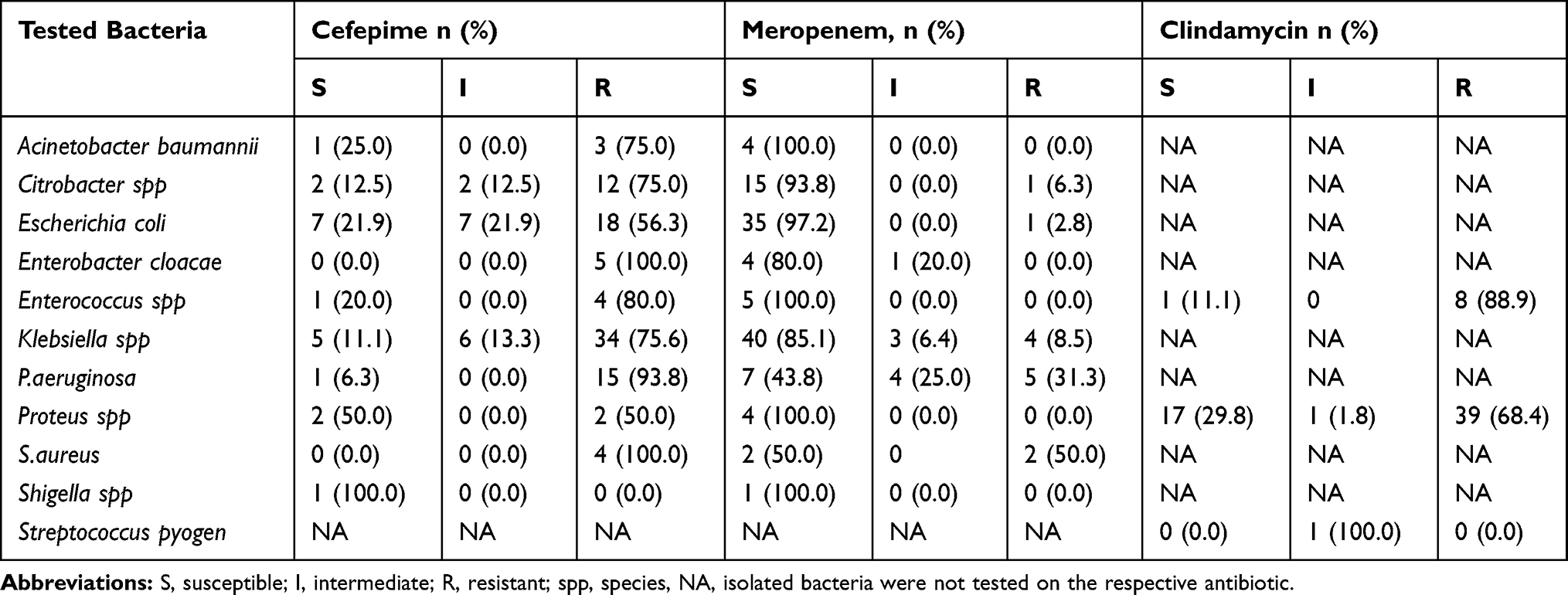 |
Table 3 Susceptibility Pattern of Tested Bacteria to Cefepime, Meropenem and Clindamycin |
Resistance to Meropenem
Furthermore, the Gram negative bacteria (n=128) isolated from clinical samples were tested for susceptibility against meropenem. Most of the pathogens were meropenem susceptible (85.3%), however, 8.5% of pathogens were found resistant. The isolated Klebsiella spp (n=47) was tested for susceptibility to meropenem, of which 8.5% were resistant and 6.4% had intermediate susceptibility; one K.oxytoca and two K.pneumonia were resistant. Of P. aeruginosa (n=16) isolated, 31.2% were resistant and 25% had intermediate susceptibility. All A.baumannii and Proteus spp (both 100.0%, n=4) were susceptible to meropenem (Table 3)
Discussion
This study described the resistance profile of clindamycin (lincosamide), cefepime (fourth-generation cephalosporin) and meropenem (carbapenem). In 2017 these antibiotics were reserved for use at tertiary hospitals following the WHO recommendation as a key focus to antibiotic stewardship.12,16 The study found the overall resistance to clindamycin, cefepime and meropenem to be 68.9%, 73.2% and 8.5% respectively, which was higher than previous studies conducted in Tanzania.14,15,17
The study also found resistant pathogenic bacteria in the collected samples as previously reported by Moremi et al, who did the study at BMC.17 Sadly, most of the blood samples collected in this study had resistant S. aureus which was suggestive of bloodstream infection. It has been documented that S.aureus was the leading cause of blood stream infection acquired in hospital settings.18–20 S.aureus get access to blood through intravascular devices such as central venous catheters, peripheral intravenous catheters, arterial catheters and urinary catheter.18,19,21 Thus presence of such microorganisms that are introduced through invasive procedures such as incision, intubation, puncture, and drug injections could greatly contribute to long hospital stays as results of bacteremia.18 Bloodstream infection has been reported to be more common among children similar to our study.19,20
Our study found 68.4% of tested S.aureus were resistant similar to Mshana et al, study in 2009 that found 61% of MRSA were resistant to clindamycin.14 Clindamycin is one of the potential alternative in high prevalent MRSA infections.22 The observed increased proportion of resistance could suggest extensive use of the antibiotic that leads to increase in resistance with time.23 In this study, Enterococcus spp isolates were found in urine and blood samples thus posing risk for development of urinary tract and bloodstream infections respectively similar to what has been reported previously.17 Most (88.9%) of the Enterococcus spp were resistant to clindamycin similar to the study by Sattari-Maraji et al who found the 96% resistance to clindamycin in Iran.24 It has been documented that the Enterococci is intrinsically resistant to clindamycin, which could explain the observed resistant pattern.8,25 Also, the previous use of clindamycin as additive drug to quinine for treatment of uncomplicated malaria in pregnant could have accelerated the resistance of this antibiotic.28
Most of the Gram negative pathogens in this study were resistant to cefepime which is the fourth cephalosporin generation antibiotic for instance, 75.6% Klebsiella Spp, 93.8% P. aeruginosa, 75.0% A.baumannii, and 56.3% E.coli were resistant. This pattern of resistance is comparable to the previous study that was conducted at BMC, the proportion of resistant Gram negative bacteria was 80.6%, 87.5% and 63.2% in the order of Klebsiella spp, P.aeruginosa, 56.3% E.coli.17 The slight observed difference in proportion could be attributed to the difference in generations of cephalosporin used. Their study assessed the susceptibility of Gram negative bacteria using third-generation cephalosporin (ceftriaxone/cefotaxime),17 contrary to our study in which we used fourth-generation cephalosporin (cefepime). Indeed, the observed high proportion of resistant bacteria was almost similar to the overall proportion of resistant Gram negative bacteria to third-generation cephalosporin in Africa.3 These bacteria are among the most mutating bacteria with high risk to human health.1,29 The high proportion of resistant Gram negative bacteria to fourth-generation cephalosporin (cefepime) could be suggestive of bacteria adaptive mechanisms by cross-resistance between generations of the same antibiotic class.29 The overuse and irrational use of antibiotics especially third-generation cephalosporin (ceftriaxone) could contribute to failure of subsequent cephalosporin generations.26,27,30
Pseudomonas aeruginosa and Klebsiella spp were isolated in all samples, this could have contributed to bloodstream infection, wound infection, urinary tract and respiratory tract infections as previously described. About 31.2% of the tested P. aeruginosa isolates were meropenem resistant contrary to the previous study which reported 8.9% of resistant Pseudomonas aeruginosa. The study was conducted between 2010 and 2011, more than eight years ago. The trend of increasing resistant P.aeruginosa was noted in a study that evaluated clinical isolated at BMC from 2007 to 2012 that found the prevalence of resistant P.aeruginosa to be 19.5%.15 A systematic review on antibiotic resistance in Africa found P.aeruginosa to be one of the bacteria resistant to carbapenem.31 The trend of increasing bacteria strains resistant to meropenem is threatening since this drug serve as the last weapon for most of Gram negative bacteria resistant to the commonly used antibiotics.
Furthermore, we found meropenem resistant Klebsiella spp to be 8.5% which was higher than the previous study by Mushi et al (1.5%) who conducted the study at BMC.15 The increase in proportion of resistant P. aeruginosa and Klebsiella spp could indicate heightening of antibiotic resistance with time necessitating questioning the effectiveness of the control measures in place. High susceptibility observed to some of pathogenic bacteria such as A.baumannii and Proteus spp could indicate good performance in some bacteria though the increasing resistance to some highly mutating bacteria is warranting strict control measures. Carbapenems are considered the treatment of choice and last option for the common nosocomial infection caused by P. aeruginosa resistant to other β-lactam antibiotics.32 Inappropriate use of antibiotics such as carbapenems especially in private health facilities could increase the prevalence of resistant bacteria to carbapenems; pressure from pharmaceutical companies and intending to make profit could be contributing factors33–35.
Limitations
This study is one of few studies conducted in East Africa that assessed the resistance pattern of clindamycin, cefepime and meropenem, however, most of the previous studies did not include cefepime which is the fourth generation cephalosporin and clindamycin,31,32 hence the current susceptibility pattern of these antibiotics has limited index comparator. Our study aimed at evaluating the current status of antibiotic resistance burden in our settings after the implementation of WHO stewardship program of reserving some antibiotics to be used as last resort when multidrug resistant infection is encountered. Therefore, we focused only to survey the resistant pattern of clindamycin, cefepime and meropenem. Being a cross-sectional design, the clinical outcomes of patients from which the resistant bacteria were isolated were not documented, therefore these findings should be interpreted with cautions because they do not equate to clinical outcomes and the number of clinical isolates was small. Furthermore, whether the infection was community or hospital acquired was not evaluated. In addition, this study was conducted at two tertiary teaching hospitals excluding other tertiary hospitals in the country hence should be generalized with high precaution.
Conclusion
High resistance to clindamycin and cefepime was revealed in this study. Meropenem resistant to P. aeruginosa and Klebsiella Spp was also observed. In addition, the pathogenic bacteria of high priority (ESKAPE) were resistant to all studied antibiotics at variable proportion. We recommend routine culture and susceptibility testing for proper use of these antibiotics as well as searching for new antibiotics. The Ministry responsible for Health should reconsider classifying clindamycin and cefepime as reserve antibiotics. A large study that will explore the countrywide susceptibility test is recommended. Taking into account that the resistance to antibiotics can assume uneven geographical distribution; either a national or zonal antibiotic resistance surveillance center should be established. The studied center (s) may serve as reference for monitoring the trend of antibiotic resistance as receive patients from different parts of the country and thus aid in planning and implementing control measures that may be stratified region.
Abbreviations
ESKAPE, Enterococcus spp., Staphylococcus aureus, Klebsiella pneumoniae, Acinetobacter baumannii, Pseudomonas aeruginosa, and Escherichia coli; NEMLT, National Essential Medicine List; MRSA, methicillin resistant Staphylococcus aureus; BMC, Bugando Medical Center; MNH, Muhimbili National Hospital.
Data Sharing Statement
The dataset generated and/or analyzed during this study is available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Approval to conduct this study was sought from the Ethical Committee of Muhimbili University of Health and Allied Sciences. In addition, permission was requested from the appropriate authorities of MNH and BMC to conduct the study at their facilities.
Acknowledgments
We highly appreciate the contribution from Nyanda Shango and his colleagues at BMC microbiology laboratory together with James Kalabashanga from MNH for their technical expertise during the phase of data collection.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Levy SB, Marshall B. Antibacterial resistance worldwide: causes, challenges and responses. Nat Med. 2004;10(12):S122–S129. doi:10.1038/nm1145
2. Wormser GP, Bergman MM. The antibiotic paradox: how the misuse of antibiotics destroys their curative powers, 2nd Edition By Stuart B. Levy Cambridge, Massachusetts: perseus Publishing, 2002. 376 pp., illustrated. $17.50 (paper). Clin Infect Dis. 2003;36(2):238. doi:10.1086/344957
3. Geneva. Prioritization of Pathogens to Guide Discovery, Research and Development of New Antibiotics for Drug-Resistant Bacterial Infections, Including Tuberculosis. World Health Organization; 2017:12.
4. Hawkey PM, Warren RE, Livermore DM, et al. Treatment of infections caused by multidrug-resistant gram-negative bacteria: report of the British society for antimicrobial chemotherapy/healthcare infection society/british infection association joint working party. J Antimicrobial Chemother. 2018;73(2015):iii2–iii78. doi:10.1093/jac/dky027
5. Roope LSJ, Smith RD, Pouwels KB, et al. The challenge of antimicrobial resistance: what economics can contribute. Science. 2019;364:eaau4679. doi:10.1126/science.aau4679
6. Frieden T. Antibiotic resistance threats in the United States. Centers Dis Control Prev. 2013;114. doi:CS239559-B.
7. Berthe F, Jean C, Wadsworth J, Thiebaud A, Marquez PV, Baris E. Pulling together to beat superbugs knowledge and implementation gaps in addressing antimicrobial resistance. In: HNP/Agriculture Global Antimicrobial Resistance Initiative. Washington, DC: World Bank Group; 2019.15:16:04
8. Cardoso T, Ribeiro O, Aragão IC, Costa-Pereira A, Sarmento AE. Additional risk factors for infection by multidrug-resistant pathogens in healthcare-associated infection: A large cohort study. BMC Infect Dis. 2012;12(1). doi:10.1186/1471-2334-12-375
9. Laxminarayan R, Matsoso P, Pant S, et al. Access to effective antimicrobials: a worldwide challenge. Lancet. 2016;387(10014):168–175. doi:10.1016/S0140-6736(15)00474-2
10. Payne LE, Gagnon DJ, Riker RR, et al. Cefepime-induced neurotoxicity: a systematic review. Crit Care. 2017;21(1):276. doi:10.1186/s13054-017-1856-1
11. WHO. World health organization model list of essential medicines. Mental and Holistic Health: Some International Perspectives; 2019:119–134.
12. Ministry of Health and Social Welfare. Standard Treatment Guidelines & National Essential Medicines List, Tanzania Mainland; 2017.
13. Lambert ML, Suetens C, Savey A, et al. Clinical outcomes of health-care-associated infections and antimicrobial resistance in patients admitted to European intensive-care units: A cohort study. Lancet Infect Dis. 2011;11(1):30–38. doi:10.1016/S1473-3099(10)70258-9
14. Mshana SE, Kamugisha E, Mirambo M, Chalya P, Rambau P, Mahalu W. Prevalence of clindamycin inducible resistance among methicillin-resistant Staphylococcus aureus at Bugando Medical Centre, Mwanza, Tanzania. Tanzania J Health Res. 2009;11(2):59–64.
15. Mushi MF, Mshana SE, Imirzalioglu C, Bwanga F. Carbapenemase Genes among Multidrug Resistant Gram Negative Clinical Isolates from a Tertiary Hospital in Mwanza, Tanzania. BioMed Res Int. 2014;2014.
16. Organization WH. WHO model list of essential medicines. World Health Organization; October, 2013:1–43. Available from: https://www.who.int/medicines/publications/essentialmedicines/en/.
17. Moremi N, Claus H, Mshana SE. Antimicrobial resistance pattern: a report of microbiological cultures at a tertiary hospital in Tanzania. BMC Infect Dis. 2016;1–7. doi:10.1186/s12879-016-2082-1
18. Bartlett JG. Nosocomial bloodstream infections in US hospitals: analysis of 24,179 cases from a prospective nationwide surveillance study. Infect Dis Clin Pract. 2004;12(6):376. doi:10.1097/01.idc.0000144912.27311.19
19. Bai Y, Zheng Z, Du M, Yao H, Liu Y, Suo J. Bloodstream Infection and its clinical characteristics and relevant factors associated with interventional therapy in a large tertiary hospital: a six years surveillance study. Biomed Res Int. 2019;2019:1–7. doi:10.1155/2019/8190475
20. Mhada TV, Fredrick F, Matee MI, Massawe A. Neonatal sepsis at Muhimbili National Hospital, Dar es Salaam, Tanzania; aetiology, antimicrobial sensitivity pattern and clinical outcome. BMC Public Health. 2012;12(1):904. doi:10.1186/1471-2458-12-904
21. Karchmer AW. Nosocomial bloodstream infections: organisms, risk factors, and implications. Clin Infect Dis. 2000;31(Supplement_4):S139–S143. doi:10.1086/314078
22. Fokas S, Fokas S, Tsironi M, Kalkani M, Dionysopouloy M. Prevalence of inducible clindamycin resistance in macrolide-resistant Staphylococcus spp. Clin Microbiol Infect. 2005;11(4):337–340. doi:10.1111/j.1469-0691.2005.01101.x
23. Odsbu I, Khedkar S, Lind F, et al. Trends in resistance to extended-spectrum cephalosporins and carbapenems among Escherichia coli and Klebsiella spp. Isolates in a district in Western India during 2004–2014. Int J Environ Res Public Health. 2018;15(1):1–15. doi:10.3390/ijerph15010155
24. Sattari-Maraji A, Jabalameli F, Node Farahani N, Beigverdi R, Emaneini M. Antimicrobial resistance pattern, virulence determinants and molecular analysis of Enterococcus faecium isolated from children infections in Iran. BMC Microbiol. 2019;19(1):156. doi:10.1186/s12866-019-1539-y
25. Kristich CJ, Rice LB, Arias CA. Enterococcal infection — treatment and antibiotic resistance molecular mechanisms of antibiotic resistance in enterococci. 2014;1–31.
26. Sonda TB, Horumpende PG, Kumburu HH, et al. Ceftriaxone use in a tertiary care hospital in Kilimanjaro, Tanzania: a need for a hospital antibiotic stewardship programme. PLoS One. 2019;14(8):1–11. doi:10.1371/journal.pone.0220261
27. Mboya EA, Sanga LA, Ngocho JS. Irrational use of antibiotics in the moshi municipality Northern Tanzania: a cross sectional study. Pan Afr Med J. 2018;31:1–10. doi:10.11604/pamj.2018.31.165.15991
28. Edition TUR of TSTG and EMLM of H and SWF. The United Republic of Tanzania Standard Treatment Guidelines and Essential Medicines List Ministry of Health and Social Welfare Fourth Edition; 2013.
29. Santajit S, Indrawattana N. Mechanisms of antimicrobial resistance in ESKAPE pathogens. Biomed Res Int. 2016;2016:1–8. doi:10.1155/2016/2475067
30. Wangai FK, Masika MM, Lule GN, et al. Bridging antimicrobial resistance knowledge gaps: the East African perspective on a global problem. PLoS One. 2019;14(2):1–12. doi:10.1371/journal.pone.0212131
31. Tadesse BT, Ashley EA, Ongarello S, et al. Antimicrobial resistance in Africa: a systematic review. BMC Infect Dis. 2017;17(1):1–17. doi:10.1186/s12879-017-2713-1
32. Ssekatawa K, Byarugaba DK, Wampande E, Ejobi F. A systematic review: the current status of carbapenem resistance in East Africa. BMC Res Notes. 2018;11(1):1–9. doi:10.1186/s13104-018-3738-2
33. Yan K, Xue M, Ye D, et al. Antibiotic prescribing practices in secondary and tertiary hospitals in Shaanxi province, western China, 2013–2015. PLoS One. 2018;13(12):2013–2015. doi:10.1371/journal.pone.0207229
34. Sharma M, Eriksson B, Marrone G, Dhaneria S, Lundborg CS. Antibiotic prescribing in two private sector hospitals; one teaching and one non-teaching: A cross-sectional study in Ujjain, India. BMC Infect Dis. 2012;12(1). doi:10.1186/1471-2334-12-155
35. Landstedt K, Sharma A, Johansson F, Stålsby Lundborg C, Sharma M. Antibiotic prescriptions for inpatients having non-bacterial diagnosis at medicine departments of two private sector hospitals in Madhya Pradesh, India: a cross-sectional study. BMJ Open. 2017;7(4):e012974. doi:10.1136/bmjopen-2016-012974
36. Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;35(2):121–126. doi:10.4103/0253-7176.116232
37. Collee JG, Miles RS, Watt B. (1996) Tests for the identification of bacteria. In: Collee JG, Marmion BP, Fraser AG, Simmons A, editors. Mackie & McCartney Practical Medical Microbiology, 14th Edition, Churchill Livingstone, New York, 131–151.
38. Şimşek S, Yurtseven N, Gerçekogalu H, et al. Ventilator-associated pneumonias in a cardiothoracic surgery centre postoperative intensive care unit. J Hosp Infect. 2001;47(4):321–324. doi:10.1053/jhin.2000.0932
39. CLSI. Performance Standards for Antimicrobial Disk Susceptibility Tests; Approved Standard—Twelfth Edition. CLSI document M02-A12. Wayne, PA: Clinical and Laboratory Standards Institute; 2015.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.