Back to Journals » Advances in Medical Education and Practice » Volume 10
Simulation-based education workshop: perceptions of participants
Authors Piryani RM ![]() , Piryani S
, Piryani S ![]() , Shrestha U, Acharya A, Kanskar S, Shahi M, Kayastha J, Chaulagain A, Agarwal JP, Bajracharya SR
, Shrestha U, Acharya A, Kanskar S, Shahi M, Kayastha J, Chaulagain A, Agarwal JP, Bajracharya SR ![]()
Received 11 February 2019
Accepted for publication 17 June 2019
Published 23 July 2019 Volume 2019:10 Pages 547—554
DOI https://doi.org/10.2147/AMEP.S204816
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Rano Mal Piryani,1 Suneel Piryani,2 Unisha Shrestha,3 Asmita Acharya,3 Srijana Kanskar,3 Mandira Shahi,4 Jeny Kayastha,5 Amrita Chaulagain,6 Jagdish Prasad Agarwal,7 Sangha Ratna Bajracharya8
1Health Professions Training Committee, Universal College of Medical Sciences, Bhairahawa, Nepal; 2Department of Community Health Sciences, Aga Khan University, Karachi, Pakistan; 3Simulation Based Education Training, Laerdal Global Health Nepal, Kathmandu, Nepal; 4Maharajganj Nursing Campus and National Centre for Health Professions Education (NCHPE), Institute of Medicine Nepal, Kathmandu, Nepal; 5Orthopaedic Department, St Vincent’s Private Hospital Northside, Brisbane, QLD, Australia; 6Research, Jeebanta Advanced Kathmandu Imaging Private Limited, Kathmandu, Nepal; 7Neurology and Medical Education Training, Tribhuvan University Institute of Medicine, Kathmandu, Nepal; 8Pharmacology and Medical Education, Tribhuvan University Institute of Medicine, Kathmandu, Nepal
Background: Simulation-based education (SBE) is increasingly endorsed as an educational strategy. It allows health-care professionals to practice clinical skills within a safe learning environment, and requires devices for simulation or simulated patients, trained teachers, and an appropriate environment. The objective of this study was to evaluate perceptions of participants on SBE and an SBE workshop.
Methods: A 1-day SBE workshop was conducted on September 4, 2018, in collaboration with Laerdal Global Health Nepal and the National Centre for Health Professions Education (NCHPE), Institute of Medicine, Kathmandu, Nepal. Semistructured pretest and posttest questionnaires were used to evaluate the perceptions of participants regarding SBE and the effectiveness of the workshop. Data were analyzed using SPSS 21.
Results: The mean difference in participant perceptions of SBE before and after participation in the workshop was significant (P<0.05) on seven statements: enhances communication skills (pretest 4.53±0.72, posttest 4.84±0.75; P=0.03), helps in seeing and managing even rarest of cases (pretest 3.59±1.00, posttest 4.21±0.92; P=0.02), overcomes the problem of uncooperative patients (pretest 3.12±0.93, posttest 3.95±1.22; P=0.004), increases confidence of students in dealing with real patients (pretest 4.29±0.77, posttest 4.79±0.42; P=0.041), enables preparation of rating scales for skills and attitude evaluation (pretest 3.76±0.83, posttest 4.11±0.76; P=0.049), provides immediate feedback during simulation (pretest 4.06±0.9, posttest 4.58±0.51; P=0.016), and keeps materials/equipment ready before simulation (pretest 4.29±0.68, posttest 4.79±0.53; P=0.007). Mean scores for participant feedback on the workshop using a Likert scale of 1–5 (5= strongly agree, 1= strongly disagree) were notable: objective of workshop fulfilled (4.16±0.688), session very interesting (4.37±0.597), session useful for future job (4.47±0.513), scenario relevant to subject (4.21±0.787), what I learnt will be useful in practice (4.05±0.78), resource persons/facilitators were helpful and effective (4.37±0.597), professional (4.42±0.507), and answered all questions (4.32±0.478), and course content was presented clearly (4.26±0.452). Almost all participants found the workshop useful and well presented, and suggested conducting such workshops frequently.
Conclusion: The SBE workshop produced substantial differences in perceptions of participants. Participants found the workshop effective in improving knowledge and understanding of SBE.
Keywords: evaluation, faculty, perception, simulation education, workshop
Introduction
The modern era of medical simulation started in the 1960s, with the use of mannequins for cardiopulmonary resuscitation designed by Peter Safar and Ausmund Laerdal.1 Simulation-based education (SBE), a relatively new approach, is used to teach, educate, train, and coach health-care professionals with simulated patients or simulative aids. This educational strategy is used to achieve adequate command in learning on preselected real-life or near-real-life clinical scenarios, avoiding undesirable features encountered or confronted in learning with real patients and undue stress to real patients.1–3
Simulation is one of the educational strategies based on mock components and features of patient care, executed with simulated and standardized patients, mannequins, virtual-reality computer-generated simulation or combinations of these. This strategy replicates substantive aspects of real-life experiences. With this strategy, novice health-care professionals acquire all three domains of learning (knowledge, skills, and attitudes) in a quite safe and risk-free environment.1–3,6 Use of simulation benefits patients, students, medical educators, and practicing health-care providers. This strategy enhances clinical learning, thereby improving the quality of care, preventing and minimizing medical errors, and decreasing the risk of harm to a patient.1–3,5–7
The modalities for simulation are generally categorized into five main groups: low technology (low-cost models or mannequins), screen based computer simulators (use of software), standardized patients (trained simulated patients or actors), complex-task trainers (high-fidelity computer-based simulators), and realistic patient simulators (high-fidelity computer-based mannequins).1–3 Largely, there are four delivery methods/models/settings of SBE: in-situ simulators (brought to actual workplace for demos), mobile-based (loaded in vehicle), simulation centers with a control room, and computer-based or online.1,2,6
Simulation-based learning is explained as experiential learning, usually dealing with adult learners in health-care professions. The essential feature of simulation is continuous feedback, and a more significant component of simulation sessions is debriefing.1,4,8 SBE training must be integrated at all levels of health-care professions education. Teachers, educators, instructors, facilitators, and faculty members need to be cognizant of SBE, its importance and issues, uses, modalities and delivery methods, process of delivery, and assessment. They must be trained in these aspects of SBE and motivated and rewarded for their implementation.3,7 In collaboration with Laerdal Global Health Nepal, a 1-day SBE workshop was organized by the National Center for Health Professions Education (NCHPE), Tribhuvan University (TU), Institute of Medicine (IOM) for faculty members to sensitize them about SBE and its importance, utility, and benefits. Similarly, the objective of this study was to evaluate the perception of participants of SBE and the SBE workshop.
Methods
In collaboration with Laerdal Global Health Nepal, the NCHPE, TU-IOM organized a 1-day SBE workshop for September 4, 2018. The overall goal of the workshop was to sensitize educators (faculty members) about the importance of SBE. The objectives of the workshop were to brief educators about the utility and benefits of SBE and enhance their confidence to use simulation as an educational tool to increase the efficiency of leaners. The schedule was divided into three sessions:
- Session I (tutorial with brainstorming): SBE and its importance as a teaching and learning method, assessment in SBE, the mission, vision, and goals of Laerdal in promoting SBE, implementation of SBE, and brainstorming on the structure of a simulation scenario
- Session II (medical simulation): demonstration of two preselected scenarios (cardiac arrest and shoulder presentation abnormal delivery) on low-fidelity mannequins with debriefing
- Session III (hands-on practice): visit to Skills Lab and hands-on practice on mannequins
Two resource persons and four facilitators conducted the workshop. Twenty faculty members participated in the workshop: eleven from Maharajgunj Medical Campus and nine from Maharajgunj Nursing Campus. Heads of the respective departments nominated the faculty member on the directive of the executive director of the NCHPE. Of the 20, 17 agreed to participate in pretest and posttest evaluation and consented to publish the findings. The executive director approved the study protocol.
The objective of this study was to evaluate the perception of participants of SBE and the SBE workshop. Evaluation of the workshop was done with pretest and posttest using semi-structured questionnaires. These had been piloted by Laerdal Global Health Nepal in a previous workshop and validated. Questionnaires had four parts:
- Characteristics: individual and organizational characteristics of participants (age, sex, years of working experience, degree obtained, and specialty) and organizational characteristics of the participants (designation, department, and institute) were gathered during pretest.
- Statements on perception: structured parts of both pretest and posttest questionnaires contained 26 statements on the same topics to be responded to by participants on a 5 points Likert scale (strongly disagree = 1, disagree = 2, agree to some extent = 3, agree = 4, strongly agree = 5).
- Statements on feedback: Another structured part of the posttest questionnaire contained 15 items on assessment of the workshop to be responded to by participants on the 5 point Likert scale 1–5.
- Suggestions: The last part of the posttest questionnaire contained three open-ended questions on suggestions for the workshop, suggestions for integration of SBE into the curriculum, and possible areas for integration.
The collected data were checked for completeness, accuracy, and consistency and entered in IBM SPSS 21 for analysis. Descriptive analysis was done for frequency and means ± SD, and paired t-tests were used for pretest and posttest comparison of responses.
Results
The findings include descriptive information on individual and organizational characteristics, perception of participants of SBE and feedback on the workshop, and analysis of mean differences in perception and the open-ended questions regarding suggestions for the session, integration of SBE, and possible areas for integration of SBE into medical education.
Descriptive analysis
Individual and organizational characteristics
Of 20 participants at the workshop, 17 consented to fill the questionnaire. Among these, 41.2% were aged 35–40 years, 41.2% >40–45 years, 11.8% >45–55 years and 5.9% >55–60 years. There were more female participants (64.7%) than males (35.3%). Regarding experience of the participants, 41.2% had 5–10 years, 17.6% 10–15 years, 17.6% 15–20 years, and 23.6% 20–25 years. Nine (53%) participants were nursing faculty who had 2 years master’s degrees in nursing (two in adult health, three in child health, two in midwifery, and two in women's health, while 47% (n=8) were medical faculty. Among these, three had the 3-year postgraduate degree of Doctor of Medicine (one in internal medicine and two in pediatrics), two had the 3-year postgraduate degree of Master of Surgery (one each in anesthesia and obstetrics and gynecology), two possessed the advanced degree of Doctorate in Medicine (one each in emergency medicine and neurology) and one possessed the advanced surgery degree of Magister Chirurgiae (in cardiothoracic and vascular surgery).
Perceptions of participants of SBE
Table 1 depicts mean scores for pretest and posttest responses of participants to statements on perception of SBE on the Likert scale.
 |
Table 1 Perception of participants regarding the simulation-based education (SBE) workshop (n=17) |
Feedback on SBE workshop from participants
Table 2 shows feedback from participants on the SBE workshop (Likert scale).
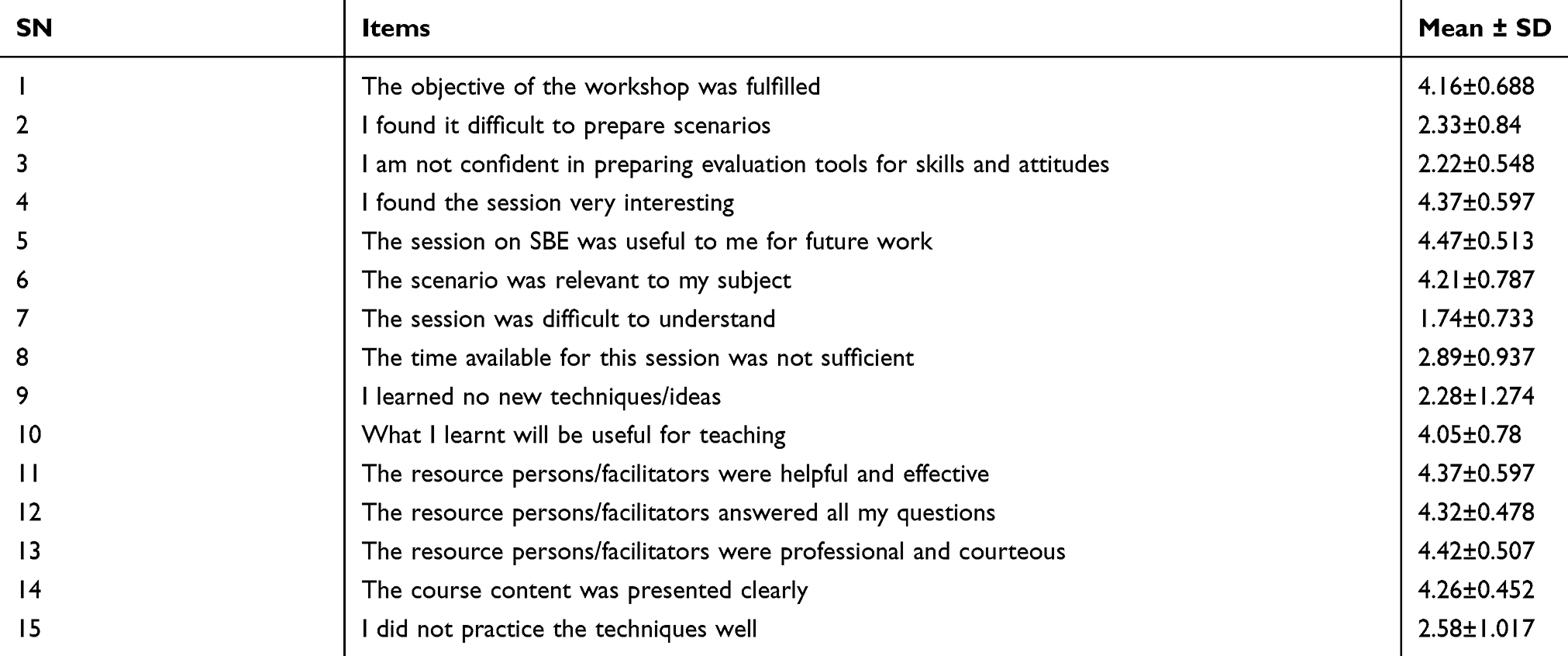 |
Table 2 Feedback for the simulation-based education (SBE) workshop from participants (n=17) |
Analysis of mean differences in perceptions of SBE
Table 3 reports mean differences in perceptions of participants before and after the workshop, calculated by paired t-tests with 95% CI and 16 degrees of freedom. P<0.05 was taken as statistically significant. Seven out of 26 statements were found to be statistically significant.
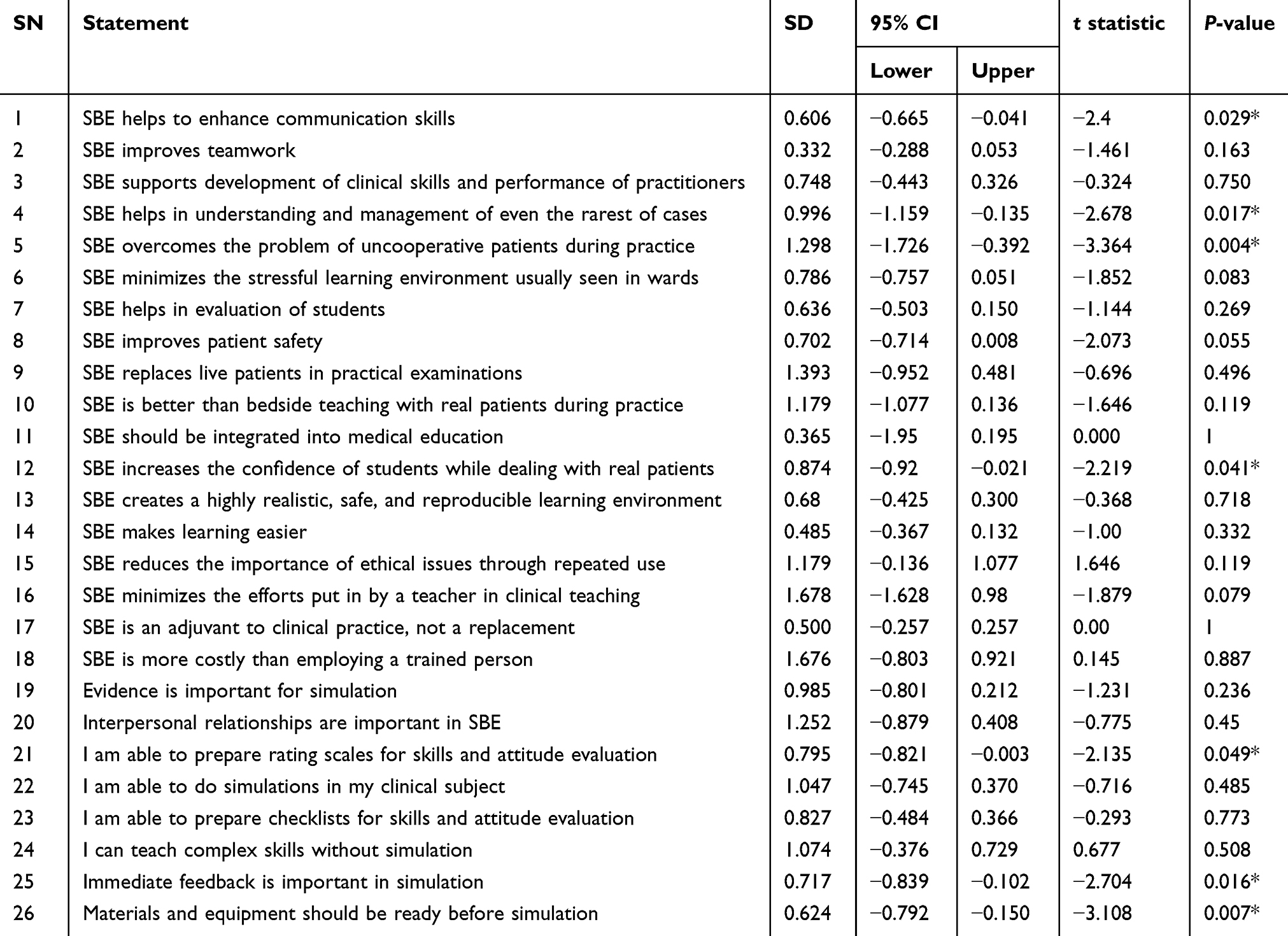 |
Table 3 Mean differences in perception of the participants of simulation-based education (SBE) before and after participation in the SBE workshop (n=17) |
Findings from open-ended questions
Suggestions regarding the workshop
Almost all participants found the workshop interesting, useful, and well demonstrated. Participants believed such workshops should be conducted frequently, their duration increased, and used to train grass root–level health-care professionals. One participant mentioned, “Today’s session was interesting but short, so needs to have expanded time”. Another added, “Good and interactive session. Further details on the various types of simulation would have been useful. One day might not be sufficient”. Similarly, another participant stated, “Very well demonstrated and interesting, and it’s useful for our day-to-day activity, so it should be continued periodically”. Another mentioned, “Needs more simulation of cases of disaster and trauma”, while another added, “It was a good session; however, it could have been better if the participants were given chance to perform independently without the help of the facilitators”.
Suggestions for integration of SBE
All participants mentioned that integration of SBE was important to build up one’s professional capacity, resulting in better quality of medical care through better learning opportunities. One participant mentioned, “The curriculum for the entire group should include SBE with proper system. The campus has to coordinate with all the departments and make a schedule”. Another participant mentioned “provision of appropriate model for practicing and conducive environment”. Similarly, another participant added, “Better to have proper monitoring and supervision to help make it possible”.
Possible areas in medical education for integration of simulation and areas most requiring SBE
Participants had varied responses regarding where integration of SBE has to be done. Areas mentioned were surgery, emergency/trauma medicine, midwifery/obstetrics, medical/surgical nursing, critical care, neonatal care, operatiing theater, and fundamentals of nursing. One participant added, “It can be applied in almost all areas, specially the ones that require our psychomotor skills”. Another participant mentioned, “Basic life support, advanced life support, management of normal delivery and shoulder presentation, emergency medicine”. Similarly, another participant mentioned, “SBE needed in nursing education, also in public health education, but most need is for MBBS education, as there are lots of practical procedure[s] in medicine, but not applying any format or checklists for doing any kind of procedures”. Another participant added, “We are midwifery educators, we apply SBE into the teaching methodology; however, periodic refresher training and orientation to new concepts is crucial to us”.
Discussion
Simulation-based health-profession education has been shown to be beneficial for learners, educators, and patients, and overall for the health-care system to improve performance of care providers, care process, and patient outcomes.3,9–11 Simulation-based learning is not a substitute for learning with real patients in real clinical contexts, but it is an accepted technique for educating and training health-care professionals in both technical and nontechnical skills prior to working with real patients.3,10,12 As learning with this method happens in a controlled environment prior to exposure to real patients, it improves patient safety and quality of care, prevents or limits errors, minimizes harm to patients, and helps in developing safe, competent health-care professionals.1–3,7 The simulation-based teaching/learning strategy must be incorporated and integrated into undergraduate and postgraduate health-profession education.12–16 Educators must be trained in how to use simulation-based teaching/learning strategies for teaching students or training trainees through faculty development programs.3,15,17
With these facts in mind, the NCHPE, TU-IOM, Kathmandu, Nepal organized the 1-day SBE workshop to sensitize medical and nursing faculty members about SBE and its importance, utility, and benefits. Feedback from participants was taken on their perceptions of SBE and the training workshop, as perceptions of health-professional educators matter simplicity in SBE implementation.18 The limitations of the study were purposive sample, small sample, and being conducted in one institution, so the findings cannot be generalized. The study assessed only reactions and perceptions of the participants, not long-term impact.
This study presents an insight on perceptions of participants about SBE and the workshop. From the pretest and posttest mean scores of 26 statements, it is obvious that perception improved appreciably on 19 statements and significantly on seven. The 19 statements were: SBE improves teamwork; supports development of clinical skills and performance of practitioners; minimizes the stressful learning environment usually seen in wards; helps in evaluation of students; improves patient safety; replaces live patients in practical examinations; is better than bedside teaching; should be integrated into medical education; creates a highly realistic, safe, reproducible learning environment; makes learning easier; reduces the importance of ethical issues through repeated use; minimizes efforts put in by a teacher in clinical teaching; is an adjuvant for clinical practice, not a replacement; and more costly than employing a trained person; that evidence is important for simulation; interpersonal relationships bare important in SBE; ability to do simulations in my clinical subject; able to prepare checklists for skills and attitude evaluation; and can teach complex skills without simulation.
Weller et al emphasized that SBE contributes to the learning of health care–profession students and clinicians in areas of clinical decision-making, interprofessional communication, communication with patients, teamwork, and clinical and procedural skills.14 They elucidated that learning experience with a real patient is fundamental for acquiring clinical expertise, but simulation provides an opportunity for practice in minimizing chances of error. They further clarified that SBE ensures a high degree of confidence and competence among students before they are exposed to real patients. SBE requires curriculum integration, adequate infrastructure, and trained faculty clearly explaining it.14 Ahmed et al found positive perceptions and attitudes of health-professional educators toward integration of SBE into an undergraduate curriculum.18 Sørensen et al said that simulation is going to be increasingly used for assessment.6
Cheng et al stated that simulation has increasingly been used as a tool, device, and/or environment that imitates a facet of clinical care to improve performance of health-care professionals, health-care processes, and outcomes of real patients care.9 Salam et al stated that SBE provides an opportunity for trainees/students to practice within a safe learning environment without subjecting patients to avoidable harm and thereby improve patient safety.19 AlHarbi stated that SBE creates a safe, risk-free environment for novice health-care professionals to acquire knowledge, skills, and attitudes.2 SBE is increasingly advocated as an educational strategy for improving patient safety.20
In the course content of SBE, latest evidence-based practices need to be incorporated for training of novice health-care professionals.21 SBE offers options to candidates for practicing rarely seen invasive procedures, helping to alleviate ethical dilemmas.1Al Kuwari revealed that cost-effectiveness is an issue in SBE implementation, but that it can be initiated with low cost and low-fidelity equipment that is found to be beneficial to novice health-care students.7 Pai explained that low-cost solutions for SBE implementation are readily available in the existing literature.15
The mean scores clearly show that perception of participants had significantly(p-value <0.05) improved on seven assertions: helping to enhance communication skills (P=0.029), helps in identification and management of even the rarest cases (P=0.017), overcomes the problem of uncooperative patients (P=0.004), increases the confidence of students while dealing with patients (P=0.041), helps in ability to prepare rating scales for skills and attitude evaluation (P=0.049), that immediate feedback is important in simulation (P=0.016), and that materials and equipment should be ready before simulations (P=0.007).
Jones et al mentioned that SBE provides a safe and controlled environment for both teaching and assessing technical and nontechnical skills like communication skills, teamwork skills, and leadership skills.1 Weller et al mentioned that SBE helps health-care professionals to learn and practice communication skills, leadership skills, coordination, and cooperation with other health-care professionals.14 In their study using a “simulation-enhanced interprofessional education strategy to improve attitudes toward teamwork and communication”, Wong et al found significant improvement in attitudes of staff toward teamwork and effective communication.22
SBE offers options to candidates for practicing rarely seen invasive procedures, helping to alleviate ethical dilemmas.1 Weller et al explained that simulations infuse a high degree of confidence among students before practicing on real patients.14 It appears that simulation-based assessments can be used effectively, as stated by Ryall et al in their systematic review on simulation-based assessments in health-professional education23 In their systematic review, Brydges et al concluded that simulation-based tools likely substituted work-based assessment of selected procedural skills.24
Feedback is critical for effective learning in SBE and has a direct impact on learning. It must be guided as per the learning needs of the individual or team.10,19,25 It is clearly mentioned by Purva et al that testing of all simulation equipment must be done before and after every session of SBE to ensure that they are in good working condition.26 Mean feedback scores were >4 on nine statements of 15: objective of the workshop was fulfilled (4.16±0.688), the session was very interesting (4.37±0.597), the session was useful to me for future jobs (4.47±0.513), the scenario was relevant to my subject (4.21±0.787), what I learnt will be useful for teaching practices (4.05±0.78), the resource persons/facilitators were helpful and effective (4.37±0.597), the resource persons/facilitators answered all my questions (4.32±0.478), the resource persons/facilitators were professional and courteous (4.42±0.507), and the course content was presented clearly and Power Point slides were good (4.26±0.452).
Overall, participants believed the training workshop achieved its objective. Participants acknowledged the usefulness of the workshop and mentioned that it was stimulating and fascinating. Participants perceived clinical scenarios as a relevant and suitable method for SBE teaching, and that resource persons and facilitators were adequately prepared and focused. Perceptions of tutors were similar after participating in a training workshop on SBE (“train the trainer”) at Universiti Kebangsaan Malaysia Medical Centre in 2014.19
The mean feedback score on six items was around 2: felt difficulty in preparing scenarios (2.33±0.84), not confident in preparing evaluation tools for skills and attitudes (2.22±0.548), the session was difficult to understand (1.74±0.733), the time available for this session was not sufficient (2.89±0.937), learnt no new techniques/ideas (2.28±1.274), and did not perform the technique well (2.58±1.017). This indicates that the time for the workshop was not sufficient for participants to understand the subject, prepare scenarios and evaluation tools for skills and attitudes, and practice. Their perspectives seem valid.
Conclusion
SBE is an established strategy for health care–profession education. It is increasingly being used for teaching, learning, and training of health-care professionals and assessment. SBE alleviates the anxiety of health-care professionals by developing and updating their knowledge, skills, and attitudes, while safeguarding patients from unwarranted risk. To increase the efficiency of learners, teachers must be trained in SBE. This workshop for SBE has created a significant difference in perceptions of participant faculty members. Participants found the workshop very effective in improving knowledge and understanding of SBE.
Acknowledgments
We would like to thank the University Grant Commission Nepal for providing funds for conducting the workshop on SBE. We acknowledge Professor Doctor JP Agrawal, dean, Tribhuvan University, Institute of Medicine, for granting permission to conduct the workshop. We appreciate Dr Asmita Acharya, Laerdal representative in Nepal, Centre for Medical Simulation and her team for their support and express our heartfelt thanks to Professor Doctor Rano Mal Piryani for conducting the workshop. We express our gratitude to Associate Professor Doctor Sangha Ratna Bajrachara for his support in organizing this workshop. We are indebted to the executive director of NCHPE for granting approval to conduct this study. We recognize the participants for their active involvement in this workshop and participation in this study. We would like to express our heartfelt thanks to all staff of NCHPE for their cooperation and assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jones F. Passos-Neto CE,Braguiroli OFM. Simulation in medical education: brief history and methodology. PPCR. 2015;1(2):56–63.
2. AlHarbi WM. Simulation-based medical education: theory and practice. Int J Scientific & Eng Res. 2016;7(5):249–253.
3. Chacko TV. Simulation‐based medical education: using best practices and curriculum mapping to maximize educational benefits in the context of shift toward competency‐based medical education. Arch Med Health Sci. 2017;5:
4. Fanning RM, Gaba DM. The role of debriefing in simulation-based learning. Simul Healthcare. 2007 Summer;2(2):115–125. doi:10.1097/SIH.0b013e3180315539
5. Phrampus PE. Simulation and integration into patient safety systems. Simul Healthcare. 2018;13(4):225–226. doi:10.1097/SIH.0000000000000332
6. Sørensen JL, Østergaard D, LeBlanc V, et al. Design of simulation-based medical education and advantages and disadvantages of in situ simulation versus off-site simulation. BMC Med Educ. 2017;17:20. doi:10.1186/s12909-016-0838-3
7. Al Kuwari KM. Simulation-based medical education. Bahrain Med Bulletin. 2018;40(1):9–10. doi:10.12816/0047451
8. Burns CL. Using debriefing and feedback in simulation to improve participant performance: an educator’s perspective. Int J Med Edu. 2015;6:118–120. doi:10.5116/ijme.55fb.3d3a
9. Cheng A, Kessler D, Mackinnon R, et al. Reporting guidelines for health care simulation research: extension to the CONSORT and STROBE statements. SimulHealthc. 2016;11(4):238–248.
10. Motola I, Devine LA, Chung HS, Sullivan JE, Issenberg SB. Simulation in healthcare education: a best evidence practical guide. AMEE Guide No. 82. Med Teach. 2013;35(10):e1511–30. doi:10.3109/0142159X.2013.818632
11. Riley RH, Grauze AM, Chinnery C, Horely RA, Trewhella NH. Three years of CASMS: the world’s busiest medical simulation centre. Med J Aust. 2003;179(11–12):626–630.
12. Lawson S, Reid J, Morrow M, Gardiner K. Simulation-based education and human factors training in postgraduate medical education: a Northern Ireland perspective. Ulster Med J. 2018;87(3):163–167.
13. Nuzhat A, Salem RO, Al Shehri FN, Al Hamdan N. Role and challenges of simulation in undergraduate curriculum. Med Teach. 2014;36(Suppl 1):S69–S73. doi:10.3109/0142159X.2014.886017
14. Weller JM, Nestel D, Marshall SD, Brooks PM, Conn JJ. Simulation in clinical teaching and learning. Med J Aust. 2012;196(9):594. doi:10.5694/mja10.11474
15. Pai D. Use of simulation for undergraduate medical education. Int J Adv Med Health Res. 2018;5(1):
16. Ayres-De-Campos D. Simulation-based training in obstetrics and gynecology. Fvv in Obgyn. 2012;Monograph:28–32.
17. McGaghie WC, Issenberg SB, Petrusa ER, Scalese RJ. A critical review of simulation‐based medical education research: 2003‐2009. Med Educ. 2010;44(1):
18. Ahmed S, Al-Mously N, Al-Senani F, Zafar M, Ahmed M. Medical teachers’ perception towards simulation-based medical education: a multicenter study in Saudi Arabia. Med Teach. 2016;38(Suppl1):S37–S44. doi:10.3109/0142159X.2016.1142513
19. Salam A, Saiboon IM, Jaafar MJ, et al. Tutors perception on a training workshop on simulation based medical education. Bangladesh J Med Sci. 2016;15(2):195–200. doi:10.3329/bjms.v15i2.28653
20. Sollid SJM, Dieckman P, Aase K, Søreide E, Ringsted C, Østergaard D. Five topics health care simulation can address to improve patient safety: results from a consensus process. J Patient Saf. 2016. doi:10.1097/PTS.0000000000000254
21. Royal College of Pediatrics and Child Health. Quality Assurance and Standards Guidelines for Simulation and Technology Enhanced Learning. Lichfield: The Association for Simulated Practice in Healthcare (ASPiH); 2014.
22. Wong AHW, Gang M, Szyld D, Mahoney H. Making an “attitude adjustment”- using a simulation-enhanced inter-professional education strategy to improve attitude toward teamwork and communication. Sim Healthcare. 2016;11(2):117–125. doi:10.1097/SIH.0000000000000133
23. Ryall T, Judd BK, Gordon CJ. Simulation-based assessments in health professional education: a systematic review. J Multidiscip Healthc. 2016;9:69–82. doi:10.2147/JMDH.S94676
24. Brydges R, Hatala R, Zendejas B, Erwin PJ, Cook DA. Linking simulation- based educational assessments and patient-related outcomes: a systematic review and meta-analysis. Acad Med. 2015;90:246–256. doi:10.1097/ACM.0000000000000549
25. Burton R, Hope A. Simulation based education and expansive learning in health professional education: a discussion. J Appl Learn Teach. 2018;1(1):25–34.
26. Purva M, Nicklin J. ASPiH standards for simulation-based education: process of consultation, design and implementation. BMJ Simul Technol Enhanc Learn. 2018;4(Suppl 2):A86-A94.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.