")
Back to Journals » Risk Management and Healthcare Policy » Volume 8
Barriers to health care for undocumented immigrants: a literature review
Authors Hacker K, Anies ME, Folb B, Zallman L
Received 8 August 2015
Accepted for publication 24 August 2015
Published 30 October 2015 Volume 2015:8 Pages 175—183
DOI https://doi.org/10.2147/RMHP.S70173
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Frank Papatheofanis
Karen Hacker,1,2 Maria Anies,2 Barbara L Folb,2,3 Leah Zallman4–6
1Allegheny County Health Department, Pittsburgh, PA, USA; 2Graduate School of Public Health, 3Health Sciences Library System, University of Pittsburgh, Pittsburgh, PA, USA; 4Institute for Community Health, Cambridge, MA, USA; 5Cambridge Health Alliance, Cambridge, MA, USA; 6Harvard School of Medicine, Boston, MA, USA
Abstract: With the unprecedented international migration seen in recent years, policies that limit health care access have become prevalent. Barriers to health care for undocumented immigrants go beyond policy and range from financial limitations, to discrimination and fear of deportation. This paper is aimed at reviewing the literature on barriers to health care for undocumented immigrants and identifying strategies that have or could be used to address these barriers. To address study questions, we conducted a literature review of published articles from the last 10 years in PubMed using three main concepts: immigrants, undocumented, and access to health care. The search yielded 341 articles of which 66 met study criteria. With regard to barriers, we identified barriers in the policy arena focused on issues related to law and policy including limitations to access and type of health care. These varied widely across countries but ultimately impacted the type and amount of health care any undocumented immigrant could receive. Within the health system, barriers included bureaucratic obstacles including paperwork and registration systems. The alternative care available (safety net) was generally limited and overwhelmed. Finally, there was evidence of widespread discriminatory practices within the health care system itself. The individual level focused on the immigrant’s fear of deportation, stigma, and lack of capital (both social and financial) to obtain services. Recommendations identified in the papers reviewed included advocating for policy change to increase access to health care for undocumented immigrants, providing novel insurance options, expanding safety net services, training providers to better care for immigrant populations, and educating undocumented immigrants on navigating the system. There are numerous barriers to health care for undocumented immigrants. These vary by country and frequently change. Despite concerns that access to health care attracts immigrants, data demonstrates that people generally do not migrate to obtain health care. Solutions are needed that provide for noncitizens’ health care.
Keywords: undocumented immigrants, health care, access, deportation, immigration and migration
Background
Over the last decade, international migration has continued to rise despite the efforts of many countries to tighten their borders.1 Factors such as conflict, discrimination, and the lack of employment opportunities in countries of origin contribute to migration patterns. Today, countries have used a variety of strategies to dissuade immigrants from crossing their borders ranging from border patrol to identity checks, detention, and deportation.2,3 With the unprecedented rates of migration, policies that disincentivize migration have spread to health care. Internationally, many countries, including the US, European nations, Scandinavia, Canada, and Costa Rica, have promulgated a range of policies that limit access to health services.4–8 In the US for example, the Affordable Care Act excludes undocumented immigrants from accessing health insurance.9 In the European Union, policies that limit undocumented immigrants’ access to health care are widespread and vary substantially. These policies range from denying all access to providing limited access to emergency and preventive care.4
Throughout the literature, undocumented immigrants/migrants, also referred to as illegal, irregular, and noncitizen, are seen as underutilizing the health care system.10–12 This underutilization not only puts their health at risk, as is the case with infectious diseases, but may also put the general public’s health at risk.13–15 Many papers examine the sequelae of undocumented immigrants’ limited access to health care.16,17 This includes the lack of follow-up for tuberculosis and HIV/AIDS, low immunization rates, and untreated mental health issues.14,15 A number of factors are presumed to exacerbate undocumented immigrants’ limited access to health care. These include their lack of knowledge, bureaucratic issues, confusion about rules and regulations, and discrimination.18 To date, however, we have not encountered a review focused specifically on the variety of barriers to health care beyond legal regulations that undocumented immigrants currently face. Nor have we found a review of strategies that have been used or might be used to alleviate these barriers. Therefore, this paper is aimed at reviewing the literature on barriers to health care for undocumented immigrants and identifying strategies that have or could be used to address these barriers.
Methods
To address our main study aim we conducted a literature review using a systematic approach to examine peer-reviewed literature related to barriers to health care faced by undocumented immigrants. We also identified recommended strategies for solutions within the literature reviewed.
Search strategy
Our literature search was conducted using PubMed by one author (BF) to capture our three main concepts: immigrants, undocumented, and access to health care. We limited our search to articles written in English over the last 10 years. Various terms for immigrants were used, including immigrants, foreigners, aliens, and migrants. In addition, a variety of search terms for undocumented were used, including undocumented, illegal, irregular, and noncitizen. The full search strategy is provided in the “PubMed search strategy” section of Supplementary materials. The search was designed to retrieve articles on a wide range of subtopics within the main topic but without being exhaustive, as would be required for a complete systematic review. By incorporating systematic review methods into the search, this study occupies a middle ground between traditional narrative reviews, which do not require documentation of search methods or defined criteria in their choice of articles for inclusion, and systematic reviews. We applied our search criteria on April 8, 2015 and identified 341 journal article records (Figure 1). All records were exported to an EndNote database for inclusion/exclusion evaluation.
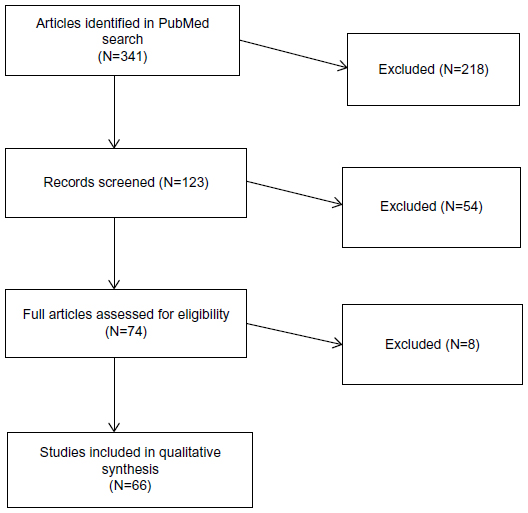 | Figure 1 Flow chart of review process. |
Article selection
We conducted a three-stage screening process starting with a title review followed by an abstract review and ending with a full-text article review. Articles were included if they addressed barriers to health care for undocumented immigrants and/or recommendations for strategies to solve problems of access. For the purposes of this search, editorials and opinion pieces were excluded.
In our title review stage, three authors (KH, MA, LZ) independently reviewed the journal article titles to determine whether they were relevant or irrelevant. Based on this title review, 123 articles were included for review and 218 were excluded. In our second stage, the authors independently screened the abstracts of the remaining 123 articles and determined that 74 initially met eligibility. Three reviewers examined full-text articles for eligibility. Seven articles were excluded as they were deemed to be opinion pieces and one article was deemed irrelevant. After excluding these articles, 66 articles were included in the qualitative analysis that followed (see Table S1; reviewed articles).
Abstraction
The reviewers then developed a data abstraction form and independently applied it to three eligible articles. They then reviewed their findings and developed an initial list of categories of barriers (eg, fear of deportation and insurance). They independently abstracted information from 10 to 12 articles each and met to review the tool, finalizing the list of categories of barriers. At this stage, one category was removed and four were added, yielding the finalized abstraction tool. Authors were instructed to highlight any themes that were not captured by the abstraction tool; however, no further key themes emerged. Once abstraction was complete, two authors (KH, LZ) met to review all of the data and consolidate the themes into categories for both barriers and recommendations.
Results
Barriers
The final categories for barriers identified from the literature represent the multiple levels where the barriers to health care for undocumented immigrants exist. These categories include barriers experienced in the policy arena, in the health care system, and at the individual level (Table 1). The policy arena focused on issues related to both law and policy including access to insurance for undocumented populations and limitations to the type of health care that they could utilize. The health care system focused on bureaucracy, capacity, and the discriminatory practices that were present. The individual level focused on the undocumented immigrants’ fears, stigma, and lack of capital (both social and financial) that, in turn, created barriers to health care.
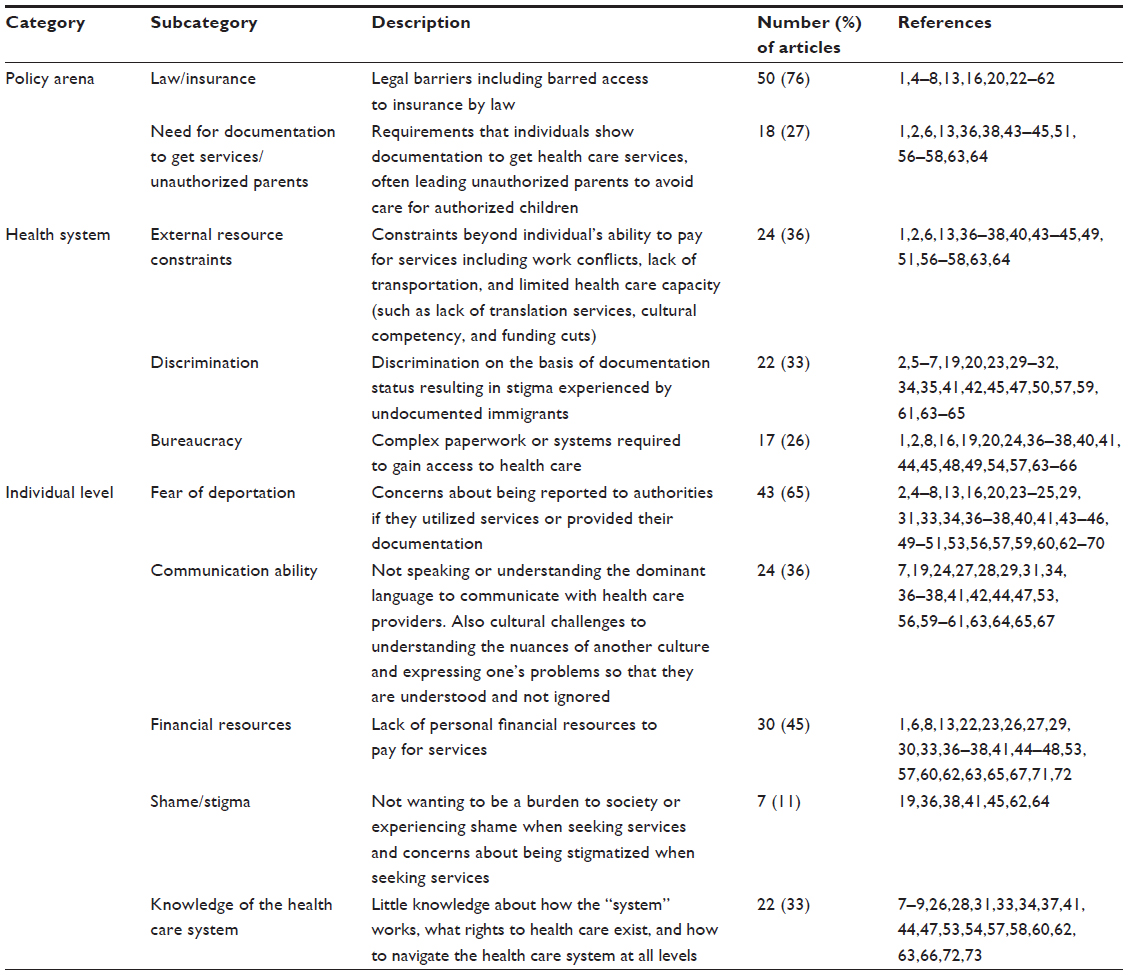 | Table 1 Barriers to health care experienced by undocumented immigrants |
Policy
National policies excluding undocumented immigrants from receiving health care were the most commonly cited barriers to health care. Three quarters of the articles described legal barriers including denying access to insurance. In some nations, active surveillance of providers led to the denial of care as providers feared losing their medical licenses or criminal procedures. A commonly cited mechanism for excluding undocumented immigrants from health care was laws limiting access to insurance. Because insurance was generally required for affordable care or required to receive services at all, these laws effectively barred access to care. The fact that medical repatriation was allowed in many countries – that is, repatriation of a sick individual to the country of origin against an individual’s will for the purposes of medical care (which is often insufficient in the country of origin) – led to avoidance of care. In addition, 27% of articles described requirements that individuals show documentation to get health care services as major barriers to care. Often, this need for documentation “spilled over” and affected authorized children of unauthorized parents, who did not seek care for their children because of the inability to provide documentation for themselves.
Health system
Health system barriers included external resource constraints, costs to the individual, discrimination, and high bureaucratic requirements. External resource constraints – or constraints such as work conflicts (eg, health care offered during work hours and fear of losing job due to time off seeking care), lack of transportation, and limited health care capacity (eg, lack of translation services, cultural competency, and funding cuts) – were identified in 36% of articles. One area where there was particularly limited capacity was in mental health care for undocumented immigrants. One third of articles discussed discrimination on the basis of nativity status; for some subpopulations, discrimination on the basis of nativity intersected with other forms of discrimination such as sexual discrimination, placing subpopulations at particularly high-risk of not receiving care. Finally, complicated bureaucracies created insurmountable barriers for not only undocumented immigrants but also providers wanting to provide care to immigrants; 26% of articles described this issue. Often bureaucratic regulations led to extensive paperwork requirements that were too complicated and costly to complete.
Individual
Individual barriers included fear of deportation, communication ability, financial resources, shame/stigma, and knowledge about the health care system. Fear of deportation, whether real or imagined, was identified as a barrier in 65% of articles. Undocumented immigrants reported avoiding health care and waiting until health issues were critical to seek services because of their concerns of being reported to authorities. This was seen in countries as diverse as France, the US, and Denmark. A second barrier – noted in 36% of articles – was communication, which not only included the inability to speak the language of the dominant culture but also included cultural discomfort with the way in which the dominant culture communicated. It was noted that undocumented immigrants were unable to communicate their health concerns to care providers or were misunderstood by those providers. For example, in one article, undocumented immigrants felt that the emergency room physicians did not fully believe their symptoms.19 Lack of financial resources was also a significant barrier, as noted in 45% of articles, and was particularly true in countries where undocumented immigrants were excluded from all health care services or had no access to insurance (the UK and Denmark). Eleven percent of papers reported the issue of shame and/or stigma as a barrier for accessing health care. Undocumented immigrants did not want to “be a burden on the system” or felt that they would be stigmatized if they sought services even in countries where services were available. Lastly, the final individual barrier that was identified was a lack of knowledge of the system itself. Undocumented immigrants often did not know what services were available to them nor what their rights to health care were. In addition, immigrants often did not know how to utilize the health care system, particularly when additional requirements were needed (ie, France’s requirement to obtain authorization prior to accessing services).20 This was identified as a barrier in 33% of the reviewed articles.
Recommendations
We identified five major categories of recommendations in the reviewed papers relevant to addressing barriers to health care for undocumented immigrants (Table 2). These categories are related to advocacy for policy change, insurance options, expansion of the safety net, training of providers to better care for immigrant populations, and education of undocumented immigrants on navigating the system.
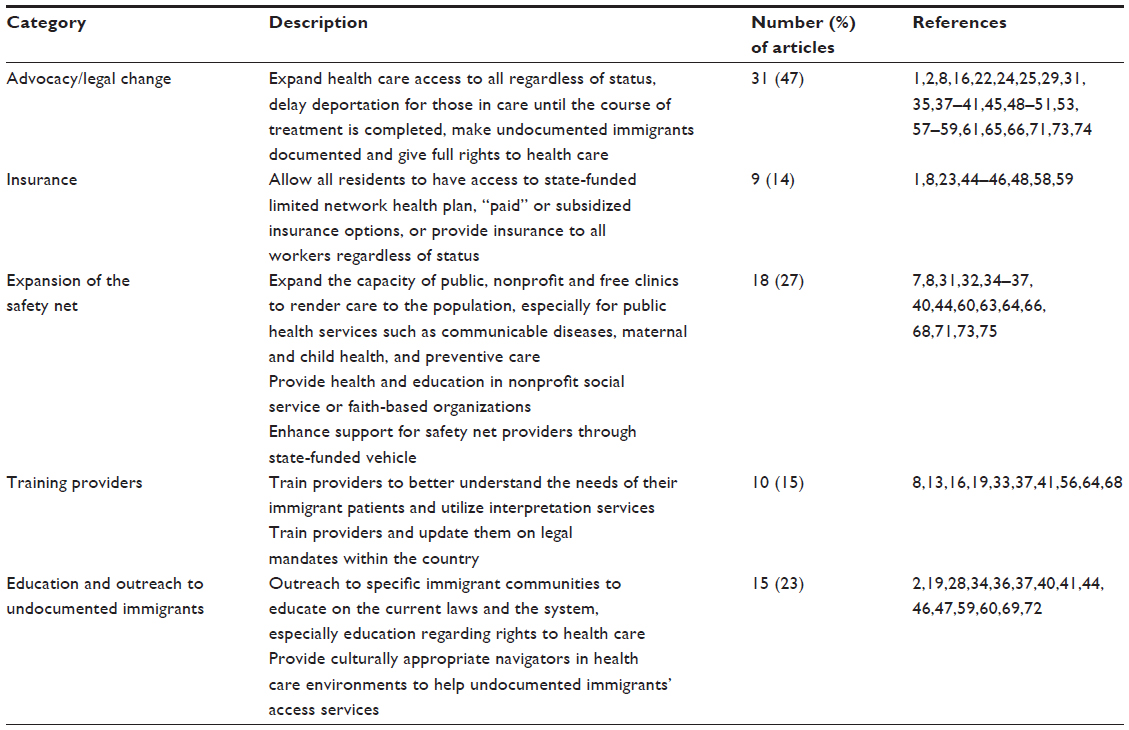 | Table 2 Recommendations for improving barriers |
Advocacy for policy change included a range of possible legislation to allow either full access to health care or varying levels of access such as public health services. Insurance options included special insurance programs through the state available to undocumented immigrants and/or full insurance benefits to employees regardless of their status. Expansion of the safety net focused on increasing the capacity of safety net providers (free clinics, state clinics, federally qualified health centers and public hospitals, and public health clinics) to service the population and receive reimbursement. In addition, strategies to employ sliding fee scales to accommodate low-income individuals and the use of voluntary organizations were mentioned. Training of providers included both training in the legal mandates of the individual country and training in cultural competency. Education for immigrants included providing specialized linguistically appropriate information on how to navigate the health care system and on what rights were afforded to undocumented immigrants. Authors also suggested using navigators to help undocumented immigrants maneuver through the health care system.
Advocacy/legal change
A variety of advocacy recommendations to change the existing laws were suggested in the majority of the papers reviewed (47%). These included not only changing laws to provide full access to care regardless of citizenship but also promoting legislation that would allow delayed deportation until treatment was completed. Others recommended major immigration reform that would grant legal status to undocumented immigrants after some period of time, thus making health care exclusion laws irrelevant.
Insurance options
Several papers suggested newly configured insurance options to support undocumented immigrants’ access to health care. These included a range of options from a state-funded insurance plan to a low-cost insurance plan with a limited network. Most of the insurance strategies recommended required undocumented immigrants to financially contribute at some level in order to access care. Fourteen percent of papers recommended changes in insurance options.
Expansion of the safety net
Twenty-seven percent of papers identified the need to expand the existing safety net to accommodate the needs of undocumented immigrants. This included expanding public and free clinics and hospitals, particularly for conditions that put the public’s health at risk (ie, tuberculosis [TB], and sexually transmitted diseases) or those related to maternal and child health (obstetrics and preventive care). They also noted that current voluntary organizations such as food banks could be important health care providers, particularly for prevention and health education. Many papers noted that the safety net system did not currently have capacity to take on this role and called for increased state support to do so.
Training of providers
A number of papers (15%) noted that providers themselves needed additional training to appropriately care for undocumented immigrants. A focus on cultural competency was needed to improve existing services as well as any new services. In some of the papers, it was also noted that providers did not adequately understand the current policies on access and might turn undocumented immigrants away based on false information. Therefore, a number of papers recommended additional training to keep providers up to date on changing legislation related to access.
Education and outreach
Lastly, a number of papers (23%) argued for education and specialized outreach to the undocumented immigrant community to facilitate their utilization of the health care system and their understanding of the policies relevant to them in the specific country. Several papers also recommended the use of navigators or cultural ambassadors to help undocumented immigrants maneuver through the bureaucracy and obtain needed care.
Discussion
In this literature review, we identified 66 peer-reviewed articles in the medical literature addressing barriers to health care among undocumented immigrants. These articles described multiple policy, health system, and individual barriers to care for this population. Policy-level barriers centered on legal barriers, particularly barred access to insurance, and the need to show documentation to get services. Health system barriers included external resource constraints (such as lack of transportation), discrimination within the health care system, and complex bureaucracies. Finally, individual-level barriers identified included fear of deportation, communication ability, lack of financial resources, and experience of shame or stigma.
The barriers to health care for undocumented immigrants are extensive and vary by country. Even in countries with more lenient health care access laws for undocumented immigrants, bureaucratic obstacles can be complex and have similar effects to limiting care. The literature suggests that the legal obstacles are not the only bureaucratic obstacles that undocumented immigrants face; undocumented immigrants deal with challenges that revolve around understanding the health care system, shame, and fear of deportation. Tying access to health care to deportation is perhaps the largest barrier to obtaining services even in countries that offer access. It is well known that immigrants overall and undocumented immigrants in particular are underutilizing the health care system. The ramifications of such obstacles might include a risk to the public’s health when communicable diseases are involved or a risk for more serious issues when health care is deferred.
Given the extent of immigration now and potentially in the future, countries will continue to grapple with developing strategies that serve the public’s health. Many of the recommendations that we identified in the reviewed articles have not been tested so it is difficult to ascertain whether or not they would be deemed successful. Recommendations mentioned frequently involved changing legislation to provide full health coverage regardless of status. Other recommendations suggested providing health care that was limited (by disease), only preventive in nature, or of low-cost. Many countries already have such systems in place.4,7,44
These secondary systems of health care for noncitizens have restricted access to care and require complex and costly bureaucracies to administer. Some of the recommendations we encountered suggested that a thoughtfully constructed (inclusive of preventive, acute, and secondary care) and controlled (limited networks), system might offer a low-cost alternative to full access.
Studies have documented that people migrate to flee violence or persecution or for economic opportunities rather than to obtain health care.21 It is therefore possible that despite concerns that access to health care attracts undocumented immigrants, integration of a noncitizens’ health care option into national systems may not increase immigration. However, more research is needed to better understand the impact of the various recommendations we identified on undocumented immigration, costs, and health outcomes.
Limitations
The literature search was limited to English language articles from the last 10 years and run using PubMed. It is likely that relevant articles are missing from this review that were published in other languages, and indexed in databases besides PubMed (such as PsycINFO and Embase, etc). Inclusion of those missing articles could have added more information on barriers and options for recommendations addressing undocumented immigrants’ access to health care.
In addition, this review was designed to answer a specific question about barriers to health care for undocumented immigrants. Recommendations examined were limited to those identified in the articles retrieved for our review of barriers. We did not carry out a separate review of strategies to address the provision of health care for undocumented immigrants, and a literature review focused on polices or strategies to address health care for this population might provide additional evidence not mentioned in this paper. Another review examining the impact of various health services for undocumented immigrants would be needed.
Because the review aimed to examine barriers in general rather than compare barriers by country, we are unable to present comparisons across countries. Further research would be needed to answer this question. Lastly, we were strictly focused on undocumented immigrants and are unable to comment on barriers to care for documented (legal) immigrants.
Conclusion
There are numerous and wide-ranging barriers to receipt of health care for undocumented immigrants. These barriers are not only legal in nature but also encompass challenges inherent in “undocumented” or illegal status. They include policy limitations, the fear of disclosure, and the lack of both social and financial assets. Given the current level of undocumented immigrants worldwide, these barriers will continue to impact human health. Additional research is needed to determine the effect of implemented health policies on undocumented immigrant health and decisions to immigrate.
Disclosure
The authors report no conflicts of interest in this work.
References
Grit K, den Otter JJ, Spreij A. Access to health care for undocumented migrants: a comparative policy analysis of England and the Netherlands. J Health Polit Policy Law. 2012;37(1):37–67. | |
Hacker K, Chu J, Leung C, et al. The impact of Immigration and Customs Enforcement on immigrant health: perceptions of immigrants in Everett, Massachusetts, USA. Soc Sci Med. 2011;73(4):586–594. | |
Rodriguez C, Chishti M, Capps R, St. John L. A Program in Flux: New Priorities and Implementation Challenges for 287 (g). Washington, DC: Migration Policy Institute; 2010. | |
Cuadra CB. Right of access to health care for undocumented migrants in EU: a comparative study of national policies. Eur J Public Health. 2012;22(2):267–271. | |
Hardy LJ, Getrich CM, Quezada JC, Guay A, Michalowski RJ, Henley E. A call for further research on the impact of state-level immigration policies on public health. Am J Public Health. 2012;102(7):1250–1254. | |
Magalhaes L, Carrasco C, Gastaldo D. Undocumented migrants in Canada: a scope literature review on health, access to services, and working conditions. J Immigr Minor Health. 2010;12(1):132–151. | |
Woodward A, Howard N, Wolffers I. Health and access to care for undocumented migrants living in the European Union: a scoping review. Health Policy Plan. 2014;29(7):818–830. | |
Biswas D, Toebes B, Hjern A, Ascher H, Norredam M. Access to health care for undocumented migrants from a human rights perspective: a comparative study of Denmark, Sweden, and the Netherlands. Health Hum Rights. 2012;14(2):49–60. | |
Edward J. Undocumented immigrants and access to health care: making a case for policy reform. Policy Politics Nurs Pract. 2014;15(1–2):5–14. | |
Stimpson JP, Wilson FA, Su D. Unauthorized immigrants spend less than other immigrants and US natives on health care. Health Aff. 2013; 32(7):1313–1318. | |
Stimpson JP, Wilson FA, Zallman L. ED visits and spending by unauthorized immigrants compared with legal immigrants and US natives. Am J Emerg Med. 2014;32(6):679–680. | |
Rodriguez MA, Bustamante AV, Ang A. Perceived quality of care, receipt of preventive care, and usual source of health care among undocumented and other Latinos. J Gen Intern Med. 2009;24(Suppl 3):508–513. | |
Hacker K, Chu J, Arsenault L, Marlin RP. Provider’s perspectives on the impact of Immigration and Customs Enforcement (ICE) activity on immigrant health. J Health Care Poor Underserved. 2012;23(2):651–665. | |
Asch S, Leake B, Anderson R, Gelberg L. Why do symptomatic patients delay obtaining care for tuberculosis? Am J Respir Crit Care Med. 1998; 157(4 Pt 1):1244–1248. | |
Asch S, Leake B, Gelberg L. Does fear of immigration authorities deter tuberculosis patients from seeking care? West J Med. 1994;161(4):373–376. | |
Martinez O, Wu E, Sandfort T, et al. Evaluating the impact of immigration policies on health status among undocumented immigrants: a systematic review. J Immigr Minor Public Health. 2013;17(3):947–970. | |
Zallman L, Himmelstein DH, Woolhandler S, et al. Undiagnosed and uncontrolled hypertension and hyperlipidemia among immigrants in the US. J Immigr Minor Public Health. 2013;15(5):858–865. | |
Karp RJ, Rhee D, Feldman D, Bouchkouj N. Outreach to immigrant communities: teaching pediatric residents about access to health care. J Health Care Poor Underserved. 2007;18(3):510–515. | |
Chandler JT, Malone RE, Thompson LM, Rehm RS. “No me ponian mucha importancia”: care-seeking experiences of undocumented Mexican immigrant women with chronic illness. ANS Adv Nurs Sci. 2012;35(2):E24–E36. | |
Larchanche S. Intangible obstacles: health implications of stigmatization, structural violence, and fear among undocumented immigrants in France. Soc Sci Med. 2012;74(6):858–863. | |
Mohanty SA, Woolhandler S, Himmelstein DU, Pati S, Carrasquillo O, Bor DH. Health care expenditures of immigrants in the United States: a nationally representative analysis. Am J Public Health. 2005;95(8):1431–1438. | |
Chernin G, Gal-Oz A, Schwartz IF, Shashar M, Schwartz D, Weinstein T. Care of undocumented-uninsured immigrants in a large urban dialysis unit. BMC Nephrol. 2012;13:112. | |
Wallace SP, Rodriguez M, Padilla-Frausto I, Arredondo A, Orozco E. Improving access to health care for undocumented immigrants in the United States. Salud Publica Mex. 2013;55(Suppl 4):S508–S514. | |
Biswas D, Kristiansen M, Krasnik A, Norredam M. Access to healthcare and alternative health-seeking strategies among undocumented migrants in Denmark. BMC Public Health. 2011;11:560. | |
Miklavcic A. Canada’s non-status immigrants: negotiating access to health care and citizenship. Med Anthropol. 2011;30(5):496–517. | |
Montealegre JR, Risser JM, Selwyn BJ, Sabin K, McCurdy SA. HIV testing behaviors among undocumented Central American immigrant women in Houston, Texas. J Immigr Minor Public Health. 2012;14(1):116–123. | |
Chavez LR. Undocumented immigrants and their use of medical services in Orange County, California. Soc Sci Med. 2012;74(6):887–893. | |
Dorn T, Ceelen M, Tang MJ, et al. Health care seeking among detained undocumented migrants: a cross-sectional study. BMC Public Health. 2011;11:190. | |
Jensen NK, Norredam M, Draebel T, Bogic M, Priebe S, Krasnik A. Providing medical care for undocumented migrants in Denmark: what are the challenges for health professionals? BMC Health Serv Res. 2011;11:154. | |
Korinek K, Smith KR. Prenatal care among immigrant and racial-ethnic minority women in a new immigrant destination: exploring the impact of immigrant legal status. Soc Sci Med. 2011;72(10):1695–1703. | |
Barnes N. Is health a labour, citizenship or human right? Mexican seasonal agricultural workers in Leamington, Canada. Glob Public Health. 2013;8(6):654–669. | |
Mylius M, Frewer A. Access to healthcare for undocumented migrants with communicable diseases in Germany: a quantitative study. Eur J Public Health. 2015;25(4):582–586. | |
Schoevers MA, van den Muijsenbergh ME, Lagro-Janssen AL. Illegal female immigrants in the Netherlands have unmet needs in sexual and reproductive health. J Psychosom Obstet Gynaecol. 2010;31(4):256–264. | |
Vargas Bustamante A, Fang H, Garza J, et al. Variations in healthcare access and utilization among Mexican immigrants: the role of documentation status. J Immigr Minor Public Health. 2012;14(1):146–155. | |
Committee on Health Care for Underserved Women. Committee opinion no 627: health care for unauthorized immigrants. Obstet Gynecol. 2015;125(3):755–759. | |
Carney MA. Eating and feeding at the margins of the state: barriers to health care for undocumented migrant women and the “Clinical” aspects of food assistance. Med Anthropol Q. 2015;29(2):196–215. | |
Poduval S, Howard N, Jones L, Murwill P, McKee M, Legido-Quigley H. Experiences among undocumented migrants accessing primary care in the United kingdom: a qualitative study. Int J Health Serv. 2015;45(2):320–333. | |
Hilfinger Messias DK, McEwen MM, Clark L. The impact and implications of undocumented immigration on individual and collective health in the United States. Nurs Outlook. 2015;63(1):86–94. | |
Hilfinger Messias DK, McEwen MM, Boyle JS. Undocumented migration in the United States: an overview of historical and current policy contexts. Nurs Outlook. 2015;63(1):60–67. | |
Rhodes SD, Mann L, Siman FM, et al. The impact of local immigration enforcement policies on the health of immigrant hispanics/latinos in the United States. Am J Public Health. 2015;105(2):329–337. | |
Teunissen E, Sherally J, van den Muijsenbergh M, et al. Mental health problems of undocumented migrants (UMs) in the Netherlands: a qualitative exploration of help-seeking behaviour and experiences with primary care. BMJ Open. 2014;4(11):e005738. | |
Jolivet A, Cadot E, Angenieux O, et al. Use of an emergency department in Saint-Laurent du Maroni, French guiana: does being undocumented make a difference? J Immigr MinorHealth. 2014;16(4):586–594. | |
Amuedo-Dorantes C, Puttitanun T, Martinez-Donate AP. How do tougher immigration measures affect unauthorized immigrants? Demography. 2013;50(3):1067–1091. | |
Gray BH, van Ginneken E. Health care for undocumented migrants: European approaches. Issue Brief (Commonw Fund). 2012;33:1–12. | |
Goldade K. “Health is hard here” or “health for all”? The politics of blame, gender, and health care for undocumented Nicaraguan migrants in Costa Rica. Med Anthropol Q. 2009;23(4):483–503. | |
Howell E, Trenholm C, Dubay L, Hughes D, Hill I. The impact of new health insurance coverage on undocumented and other low-income children: lessons from three California counties. J Health Care Poor Underserved. 2010;21(2 Suppl):109–124. | |
Sebo P, Jackson Y, Haller DM, Gaspoz JM, Wolff H. Sexual and reproductive health behaviors of undocumented migrants in Geneva: a cross sectional study. J Immigr Minor Health. 2011;13(3):510–517. | |
Committee on Health Care for Underserved Women. ACOG Committee Opinion No 425: health care for undocumented immigrants. Obstet Gynecol. 2009;113(1):251–254. | |
Castañeda H. Illegality as risk factor: a survey of unauthorized migrant patients in a Berlin clinic. Soc Sci Med. 2009;68(8):1552–1560. | |
Moynihan B, Gaboury MT, Onken KJ. Undocumented and unprotected immigrant women and children in harm’s way. J Forensic Nurs. 2008;4(3):123–129. | |
Heldal E, Kuyvenhoven JV, Wares F, et al. Diagnosis and treatment of tuberculosis in undocumented migrants in low- or intermediate-incidence countries. Int J Tuberc Lung Dis. 2008;12(8):878–888. | |
Rousseau C, ter Kuile S, Munoz M, et al. Health care access for refugees and immigrants with precarious status: public health and human right challenges. C J Public Health. 2008;99(4):290–292. | |
Stevens GD, West-Wright CN, Tsai KY. Health insurance and access to care for families with young children in California, 2001–2005: differences by immigration status. J Immigr Minor Health. 2010;12(3):273–281. | |
Nandi A, Galea S, Lopez G, Nandi V, Strongarone S, Ompad DC. Access to and use of health services among undocumented Mexican immigrants in a US urban area. Am J Public Health. 2008;98(11):2011–2020. | |
Ortega AN, Fang H, Perez VH, et al. Health care access, use of services, and experiences among undocumented Mexicans and other Latinos. Arch Intern Med. 2007;167(21):2354–2360. | |
Wolff H, Epiney M, Lourenco AP, et al. Undocumented migrants lack access to pregnancy care and prevention. BMC Public Health. 2008;8:93. | |
Simich L, Wu F, Nerad S. Status and health security: an exploratory study of irregular immigrants in Toronto. Can J Public Health. 2007;98(5):369–373. | |
Torres-Cantero AM, Miguel AG, Gallardo C, Ippolito S. Health care provision for illegal migrants: may health policy make a difference? Eur J Public Health. 2007;17(5):483–485. | |
Carr DD. Implications for case management: ensuring access and delivery of quality health care to undocumented immigrant populations. Lippincotts Case Manag. 2006;11(4):195–204; quiz 205–196. | |
Marshall KJ, Urrutia-Rojas X, Mas FS, Coggin C. Health status and access to health care of documented and undocumented immigrant Latino women. Health Care Women Int. 2005;26(10):916–936. | |
Staiti AB, Hurley RE, Katz A. Stretching the safety net to serve undocumented immigrants: community responses to health needs. Issue Brief Cent Stud Health Syst Change. 2006;104:1–4. | |
Whyte J, Whyte MD, Hires K. A study of HIV positive undocumented African migrants’ access to health services in the UK. AIDS Care. 2015;27(6):703–705. | |
Campbell RM, Klei AG, Hodges BD, Fisman D, Kitto S. A comparison of health access between permanent residents, undocumented immigrants and refugee claimants in Toronto, Canada. J Immigr Minor Health. 2014;16(1):165–176. | |
Dang BN, Giordano TP, Kim JH. Sociocultural and structural barriers to care among undocumented Latino immigrants with HIV infection. J Immigr Minor Health. 2012;14(1):124–131. | |
Suess A, Ruiz Perez I, Ruiz Azarola A, March Cerda JC. The right of access to health care for undocumented migrants: a revision of comparative analysis in the European context. Eur J Public Health. 2014;24(5):712–720. | |
Schoevers MA, Loeffen MJ, van den Muijsenbergh ME, Lagro-Janssen AL. Health care utilisation and problems in accessing health care of female undocumented immigrants in the Netherlands. Int J Public Health. 2010;55(5):421–428. | |
Goossens MC, Depoorter AM. Contacts between general practitioners and migrants without a residence permit and the use of “urgent” medical care. Scand J Public Health. 2011;39(6):649–655. | |
Lopez-Cevallos DF, Lee J, Donlan W. Fear of deportation is not associated with medical or dental care use among Mexican-origin farmworkers served by a federally-qualified health center-faith-based partnership: an exploratory study. J Immigr Minor Health. 2014;16(4):706–711. | |
Maldonado CZ, Rodriguez RM, Torres JR, Flores YS, Lovato LM. Fear of discovery among Latino immigrants presenting to the emergency department. Acad Emerg Med. 2013;20(2):155–161. | |
Wolff H, Stalder H, Epiney M, Walder A, Irion O, Morabia A. Health care and illegality: a survey of undocumented pregnant immigrants in Geneva. Soc Sci Med. 2005;60(9):2149–2154. | |
Zuber J. Healthcare for the undocumented: solving a public health crisis in the US. J Contemp Health Law Policy. 2012;28(2):350–380. | |
Devillanova C. Social networks, information and health care utilization: evidence from undocumented immigrants in Milan. J Health Econ. 2008;27(2):265–286. | |
Keygnaert I, Vettenburg N, Roelens K, Temmerman M. Sexual health is dead in my body: participatory assessment of sexual health determinants by refugees, asylum seekers and undocumented migrants in Belgium and the Netherlands. BMC Public Health. 2014;14:416. | |
Brindicci G, Trillo G, Santoro CR, Volpe A, Monno L, Angarano G. Access to health services for undocumented immigrants in Apulia. J Immigr Minor Health. 2015;17(2):618–623. | |
Schoevers MA, van den Muijsenbergh ME, Lagro-Janssen AL. Patient-held records for undocumented immigrants: a blind spot. A systematic review of patient-held records. Ethn Health. 2009;14(5):497–508. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.