Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
The Cost-Effectiveness and Budget Impact Analysis of Upadacitinib for Moderate-to-Severe Atopic Dermatitis in Saudi Arabia
Authors Abu-Shraie N, Al-Sheikh A, Alharbi I, Alanizy L, Alshraim M, Khoshhal SI, AlSalman SA, Alrumaih A, Fasseeh AN, Elezbawy B, Abaza N, Semida A, George M, Amin S, Binamer Y
Received 27 February 2026
Accepted for publication 1 June 2026
Published 11 June 2026 Volume 2026:18 604093
DOI https://doi.org/10.2147/CEOR.S604093
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Samer Hamidi
Nada Abu-Shraie,1 Afaf Al-Sheikh,1 Ibtisam Alharbi,2 Layla Alanizy,3 Mohammed Alshraim,1 Sahal I Khoshhal,4 Sarah A AlSalman,1 Ali Alrumaih,5 Ahmad Nader Fasseeh,6,7 Baher Elezbawy,6,8 Nada Abaza,6 Amr Semida,9 Marina George,10 Shireen Amin,9 Yousef Binamer11
1Ministry of National Guard-Health Affairs (MNGHA), King Abdul Aziz Medical City (KAMC), Riyadh, Saudi Arabia; 2Medical Services for Armed Forces, Ministry of Defence, Jeddah, Saudi Arabia; 3Department of Clinical Pharmacy, King Saud University, Riyadh, Saudi Arabia; 4Pharmaceutical Care Services, International Medical Center, Jeddah, Saudi Arabia; 5Medical Services for Armed Forces, Ministry of Defence, Riyadh, Saudi Arabia; 6Syreon Middle East, Alexandria, Egypt; 7Faculty of Pharmacy, Alexandria University, Alexandria, Egypt; 8Doctoral School of Pharmaceutical Sciences, Semmelweis University, Budapest, Hungary; 9Abbvie, Riyadh, Saudi Arabia; 10Abbvie, Berkshire, UK; 11Department of Dermatology, King Faisal Specialist Hospital and Research Centre, Riyadh, Saudi Arabia
Correspondence: Baher Elezbawy, Syreon Middle East, Alexandria, Egypt, Tel +201227608160, Email [email protected]
Objective: Atopic dermatitis (AD) is a prevalent dermatological disease in Saudi Arabia. This study aimed to estimate the cost-effectiveness and budget impact of upadacitinib in adults and adolescents with moderate-to-severe AD in Saudi Arabia.
Methods: A 1-year decision tree model followed by a lifetime Markov model was developed to estimate the cost-effectiveness of upadacitinib compared to dupilumab and other novel AD treatments in moderate-to-severe AD patients aged ≥ 12 years in Saudi Arabia from the public payer perspective. In addition, we developed a 5-year budget impact model to estimate the financial consequences of increasing the market share of upadacitinib. Probabilistic and deterministic sensitivity analyses were conducted to test the model’s robustness.
Results: Over a lifetime horizon, upadacitinib 15 mg was associated with 0.21 additional quality-adjusted life years (QALYs) and lower costs by 148,068 SAR (39,484 USD) compared with dupilumab 300 mg. The net monetary benefit of upadacitinib 15 mg versus dupilumab 300 mg was 158,656 SAR (42,308 USD). For the budget impact, increasing the market share of upadacitinib over 5 years was associated with estimated savings of 1.5 billion SAR (412 million USD). Sensitivity analyses results supported the direction of the base-case findings.
Conclusion: Upadacitinib may be a cost-effective treatment for moderate-to-severe AD in Saudi Arabia. Increasing its market share could be considered for the target population and may reduce public healthcare costs over 5 years. However, these model-based estimates should be interpreted with uncertainty due to input assumptions and local data limitations.
Keywords: upadacitinib, cost-effectiveness, budget impact, Saudi Arabia, atopic dermatitis, eczema
Introduction
Atopic dermatitis (AD), or eczema, is a chronic and relapsing inflammatory dermatological disorder.1 It presents with itchiness, redness, and the formation of dry, scaly skin patches.1 AD can affect individuals of all ages; however, it is frequently diagnosed in childhood and may persist into adulthood.2 The disease is highly prevalent with estimates indicating prevalence as high as 30% among children and 10% in adults in certain countries.2 Moderate-to-severe AD in adults is characterized by persistent and widespread skin lesions, severe itching, and a significant negative impact on quality of life (QoL).3 Its treatment often requires a comprehensive approach.1 AD can be treated by topical corticosteroids, immunomodulators, and systemic therapies.4 The treatment plan is usually personalized according to each patient’s needs, disease severity, comorbidities, and preferences.4
For most patients, topical management is the foundation of AD care, including emollients, topical corticosteroids (TCS), topical calcineurin inhibitors, and other anti-inflammatory agents. These treatments aim to control symptoms, reduce flares, and support maintenance therapy. However, patients with moderate-to-severe AD who are inadequately controlled with topical therapy, or require repeated or prolonged topical treatment, may require escalation to phototherapy or systemic therapy.5 Current international guidelines recognize several systemic options, including oral Janus-kinase (JAK) inhibitors such as upadacitinib, abrocitinib, and baricitinib, as well as targeted immunomodulators (TIMs), including interleukin inhibitors such as dupilumab, lebrikizumab, and tralokinumab. These therapies offer a targeted therapeutic approach for patients with an inadequate response, intolerant, or contraindicated to systemic immunosuppressants.5,6
Treatment has a crucial role in enhancing disease control and improving QoL.7 Several factors contribute to the substantial burden of AD, including its high prevalence, considerable indirect costs, and the cost of continuous medical care, especially in moderate-to-severe stages.8 In the Kingdom of Saudi Arabia (KSA), AD is highly prevalent affecting a substantial proportion of the population across different age groups.9 Among adults and adolescents, AD contributes to an annual burden of approximately 373 million Saudi Riyals (SAR) (USD 100 million) in direct healthcare costs and 1.4 billion SAR (USD 373 million) in indirect costs.9,10
Currently, there is a growing emphasis on the importance of economic evaluations to guide decision-makers in optimizing resource allocation and improving the cost-effectiveness of medical interventions in alignment with the goals of KSA Vision 2030.11 Saudi experts recently published their national guidelines for economic evaluations to standardize and improve the quality of health economic studies in the country,12 representing a formal step toward integrating health economics into policymaking in KSA, ensuring more efficient and effective healthcare delivery.
Several published cost-effectiveness analyses demonstrated that JAK inhibitors and TIMs for moderate-to-severe AD are cost-effective compared with conventional systemic treatments across different healthcare settings.13,14 Although these treatments are associated with higher acquisition costs, they showed gains in quality-adjusted life years (QALYs), resulting in favorable cost effectiveness outcomes. Budget impact analyses further suggest that the overall financial impact of introducing these therapies may be associated with cost savings.15
Despite the significant burden of AD, recent evidence on the cost-effectiveness or budget impact of these novel therapies in the KSA context remains scarce.
The objective of this study was to assess the cost-effectiveness and net monetary benefit (NMB) of upadacitinib compared to other novel systemic treatments for moderate-to-severe adult and adolescent AD patients in KSA from the public payer perspective. Additionally, we aimed to assess the budget impact of increasing the market share of upadacitinib in KSA. Conducting this study was essential to ensure choosing cost-effective interventions which could help to mitigate the burden of AD and effectively utilize the resources towards better health outcomes for the population.
Methods
We conducted a cost-effectiveness and budget impact analysis of upadacitinib for moderate-to-severe AD in adults and adolescents from the Saudi public payer perspective, with dupilumab, abrocitinib, baricitinib, tralokinumab, and best supportive care (BSC), as comparators, each assessed with or without TCS. Detailed dosing regimens for all comparators is provided in Supplementary Table 1. BSC included a combination of emollients, TCS, phototherapy sessions, and treatment of flares costs, as defined by National Institute for Health and Care Excellence (NICE) technology appraisal report.16
The target population was patients aged ≥12 years with moderate-to-severe AD. The model design was based on a previous model developed by Edwards et al to evaluate AD treatments in a similar target population.17 We validated the model structure and assumptions in line with the validation framework and validation steps described by Nagy et al,18 and we adapted key components to reflect treatment pathways, resource utilization, unit costs, relevant to the healthcare system in KSA. Additionally, we incorporated a budget impact model to estimate the financial consequences of increasing the market share of upadacitinib for the target population.
The model’s base-case scenario compares upadacitinib 15 mg with dupilumab 300 mg. Dupilumab was selected as the base-case comparator as it is the most currently used treatment modality for moderate-to-severe adult and adolescent AD patients in KSA, according to expert opinion. Additional systemic comparators were selected because they represent approved or near-approval targeted treatment options for moderate-to-severe AD and are relevant to the evolving treatment landscape in KSA, while TCS was included to reflect its continued role as background topical therapy. Base-case results are reported in the main text, while results for other comparators, with and without TCS, are presented in the supplementary tables.
Key model outcomes include incremental costs, incremental health benefits, incremental cost-effectiveness (ICER) results, NMB, and budget impact. The study was reported in accordance with the Consolidated Health Economic Evaluation Reporting Standards (CHEERS) reporting checklist.19
Cost-Effectiveness Analysis (CEA) Model
The cost-effectiveness model comprises an initial 1-year decision tree followed by a lifetime Markov model to capture patient transitions across health states over time. During the first year, patients transition within the decision tree model, then at week 52, they are assigned to the Markov model’s health states based on their final health state in the decision tree (See Figures 1 and 2 for model structure).
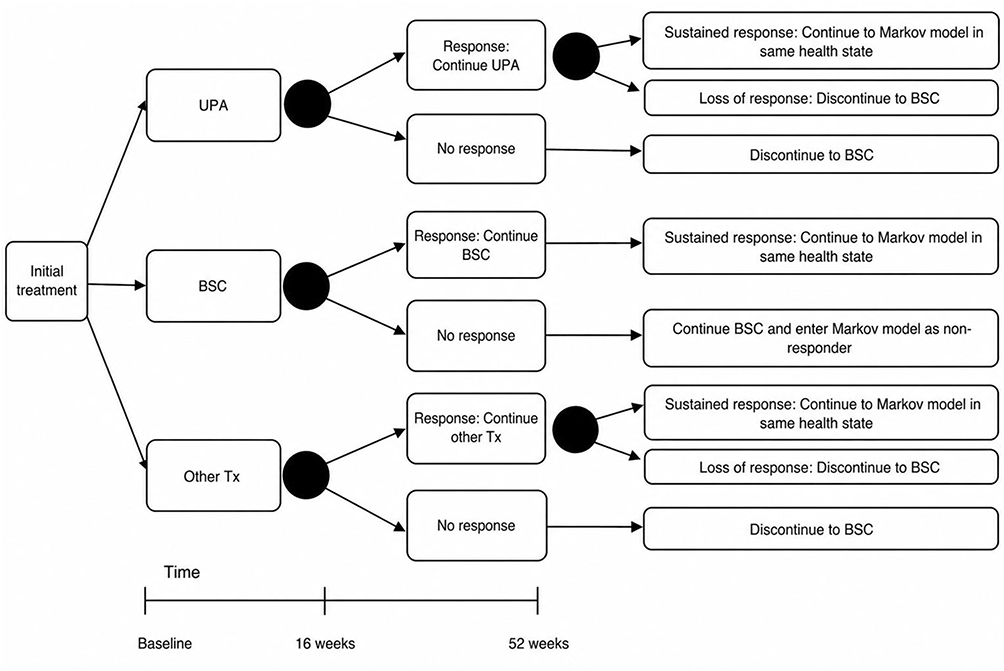 |
Figure 1 Schematic representation of 1 year decision tree model. Abbreviations: BSC, Best supportive care; Tx, Treatment; Other Tx include, dupilumab, abrocitinib, baricitinib, and tralokinumab; UPA, Upadacitinib. Note: Details of response health states incorporate 3 sub-health states (EASI-50, EASI-75, and EASI-90) but are not shown in the figure for simplicity. |
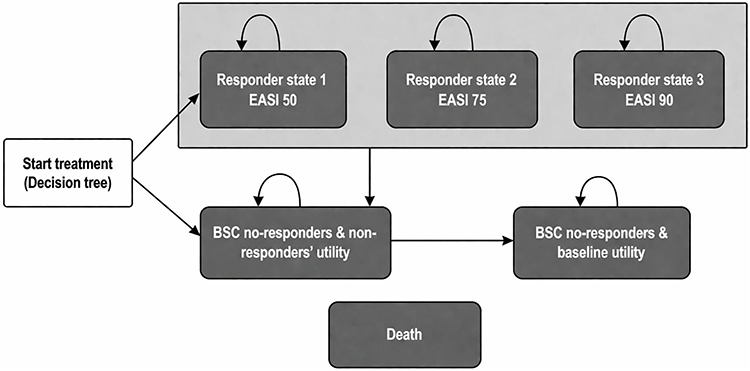 |
Figure 2 Schematic representation of lifetime Markov model. Abbreviations: BSC, Best supportive care; EASI, Eczema Area Severity Index. |
Patients start treatment at baseline and receive one of the following: BSC, upadacitinib 15 mg (base case) or 30 mg oral tablets, dupilumab 300 mg subcutaneous injection (base case comparator), abrocitinib 100 mg or 200 mg oral tablets, baricitinib 2 mg or 4 mg oral tablets, or tralokinumab 300 mg subcutaneous injection. Each of these treatments was evaluated with and without TCS.
Treatment response was evaluated using the Eczema Area Severity Index (EASI), a validated tool for assessing disease severity in AD.20 Alive patients were categorized into four health states: non-responders, EASI-50, EASI-75, and EASI-90, corresponding to the following reductions from baseline EASI score: <50%; 50% to <75%, 75% to <90%; and ≥90%, respectively. In both the decision tree and the Markov model, patients could be in one of these health states or death.
A monthly background mortality rate is applied in the model according to age- and sex- specific KSA life tables.21 A cost-effectiveness threshold (CET) of 50,000 SAR per QALY was adopted, aligning with the lower limit of CET in KSA economic evaluations guidelines.22
Decision Tree Model (Year 1)
The decision tree model was selected to reflect the clinical trials’ evaluation frameworks, where patient response is evaluated at two key time points: week 16 and week 52 (1 year),23,24 based on the percentage reduction in EASI score. In line with the clinical trials’ assessment schedule, responders are assumed to remain in their respective health states until the next assessment at week 52. Non-responders discontinue treatment and transition to receive BSC. At the 52-week reassessment, patients may remain in their responder health state or may lose response and transition to the non-responder health state.
The decision tree is structured in weekly cycles by incorporating time-dependent calculations before transitioning to the Markov model. While transitions between responder and non-responder health states occur only in weeks 16 and 52, patient-level inputs including general mortality, costs, probabilities of flares, and adverse events are updated on a weekly basis.The decision tree model structure is illustrated in Figure 1.
Markov Model (from Year 2 Onwards)
Patients start the Markov model based on the health states from the 52-week assessment, distributed over the five health states. Patients are evaluated at the end of each cycle to determine whether they remain responders, discontinue treatment (based on treatment compliance rates), or die. Response and treatment compliance rates are informed by the treatments’ clinical trials.23,25 Patients who discontinue treatment are categorized as non-responders and are assumed to receive BSC.
Patients who start the Markov model on BSC are assigned baseline utility and non-responder cost profile. While patients starting on upadacitinib or other novel treatments who are initial responders are assumed not to be able to transition between the EASI responder categories, but they can transition to non-responders’ health state. Non-responders are assumed to discontinue treatment and are then classified as non-responders receiving the non-responder health state corresponding utilities. For patients who lose response, tunnel health states are used in the model to capture the gradual waning of treatment effect over a specified duration, after which patients transition to the collective non-responder health state, and return to the baseline utility. Waning is defined as patients losing QoL benefit of the treatment received. The structural framework of this Markov model is illustrated in Figure 2.
The Markov model is conducted over a lifetime time horizon (up to a maximum age of 100 years), with a cycle length of one year. Survival was constrained by background population mortality. After the initial year, where patients are in the decision tree model, a discount rate of 4% is applied to both costs and health outcomes, in accordance with KSA guidelines.12 Discounting was implemented in the Markov model to reflect the lower present valuation of costs and health outcomes expected in the future.
Model Inputs
Efficacy Inputs
Treatment efficacy inputs were derived from a published network meta-analysis (NMA) and its subsequent update by Silverberg et al, which compared the efficacy of systemic therapies for moderate-to-severe AD.26,27 These NMAs synthesized comparative evidence from clinical trials of several treatment regimens and were used to inform transition probabilities within the model.
Cost Inputs
The model incorporated direct medical costs, including medications, visits, diagnostics, flare treatments, phototherapy, psychology sessions, and costs of managing adverse events. Average local costs, resource utilization patterns, and estimated market shares were derived from a tailored questionnaire distributed among Saudi healthcare experts to reflect the healthcare payer perspective. Supplementary Tables 2–4 show the questionnaires used to collect expert inputs. Cost data were subgrouped into non-responders, responders at year 1 with treatment, and responders at year 2 or more with treatment, since the resource utilization largely differs after the first year of treatment based on the experts’ opinions. A summary of the annual direct medical costs based on resource utilization and local unit costs is provided in Table 1. These cost estimates exclude the costs of novel AD treatments, which were applied for each arm separately.
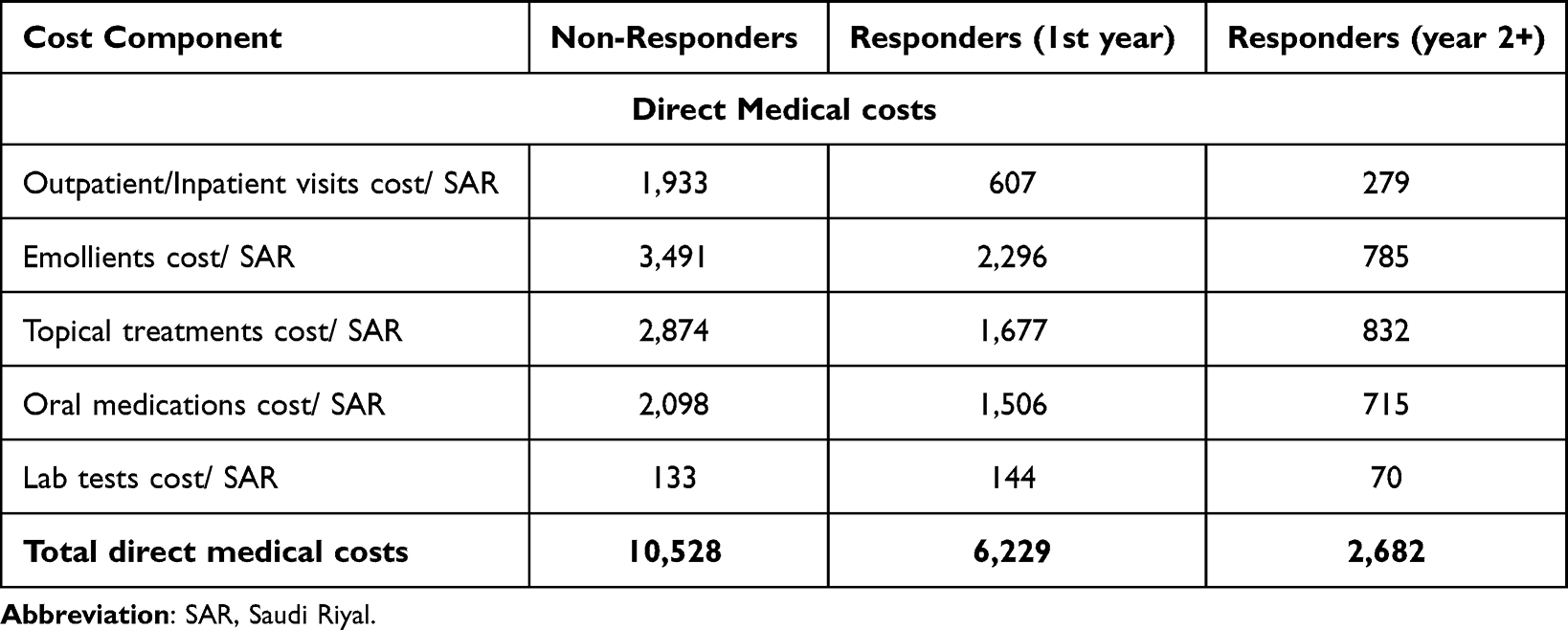 |
Table 1 Average Annual Direct Medical Cost per Patient in SAR |
Drug costs were abstracted from the Saudi National Unified Procurement Company (NUPCO) tender prices (Tender code: NPT0066/22).28 All costs are expressed in SAR and reported in 2025 values. Indirect costs and out-of-pocket payments were excluded from the analysis in line with the public payer perspective adopted in this model.
Utility Inputs
The base-case utilities were derived from the MEASURE UP-1, MEASURE UP-2,23 and AD UP trials,29 with EQ-5D-5L values converted to EQ-5D-3L using van Hout et al’s methodology.30 The model assigned utility values to health states using regression-derived coefficients and baseline patient characteristics. Due to the lack of local data on utilities of the model’s specific health states, we used the global patient utility data provided by the trials shown in Table 2. These trials were conducted in multiple countries, so we assumed utility in KSA would follow the global average used in the trials. This assumption was tested for validity through sensitivity analysis.
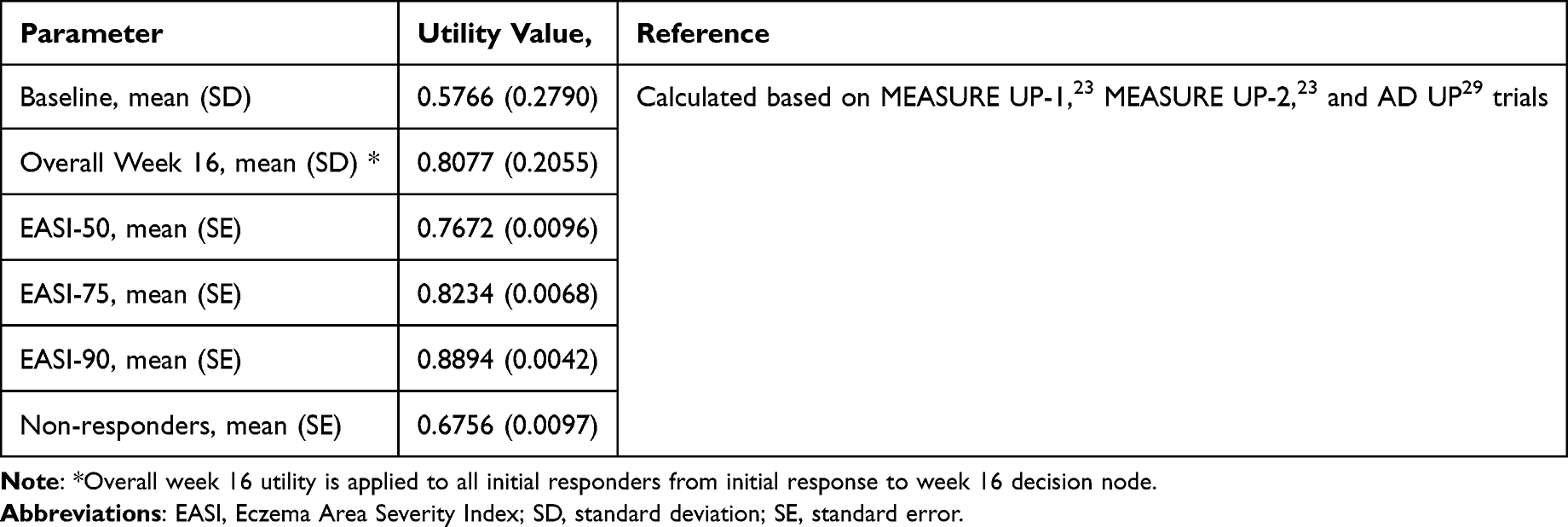 |
Table 2 Summary of Utility Values Used in the Model Base Case |
The model applies an age-related decline in health-related QoL (HRQoL) using age-specific decrements derived from the Ara and Brazier regression equation.31 The model also assumes that utility benefit from treatment does not persist, particularly for those on BSC, where a rapid return to baseline utility is expected at the next cycle. This assumption is supported by empirical evidence from van der Schaft et al32 For patients receiving novel treatments, the model assumes a more stable response, but with a gradual loss of utility over time, based on data published by NICE technology appraisal report for dupilumab,16 and was applied consistently across all novel treatments (waning effect).
Budget Impact Analysis (BIA) Model
A 5-year BIA model was developed by comparing a current market shares scenario to a projected scenario in which upadacitinib adoption increases over time for the target population. Budget impact was calculated as the total cost under the increased-upadacitinib scenario minus the total cost under the current-market-share scenario. The BIA model was informed by the CEA, including patient pathways, costs, adverse events, and mortality, and included approved or near-approval all systemic therapies (upadacitinib, dupilumab, abrocitinib, baricitinib, and tralokinumab)27 based on their market shares in KSA.
Costs per patient were derived from the CEA model based on patients’ distribution over the first 5 years. Estimated number of patients was calculated based on local data and caclualtions33–37 as detailed in Table 3. The estimated total number of new upadacitinib-eligible patients for each year is shown in Supplementary Table 5. The baseline eligible population in 2024 was estimated as:
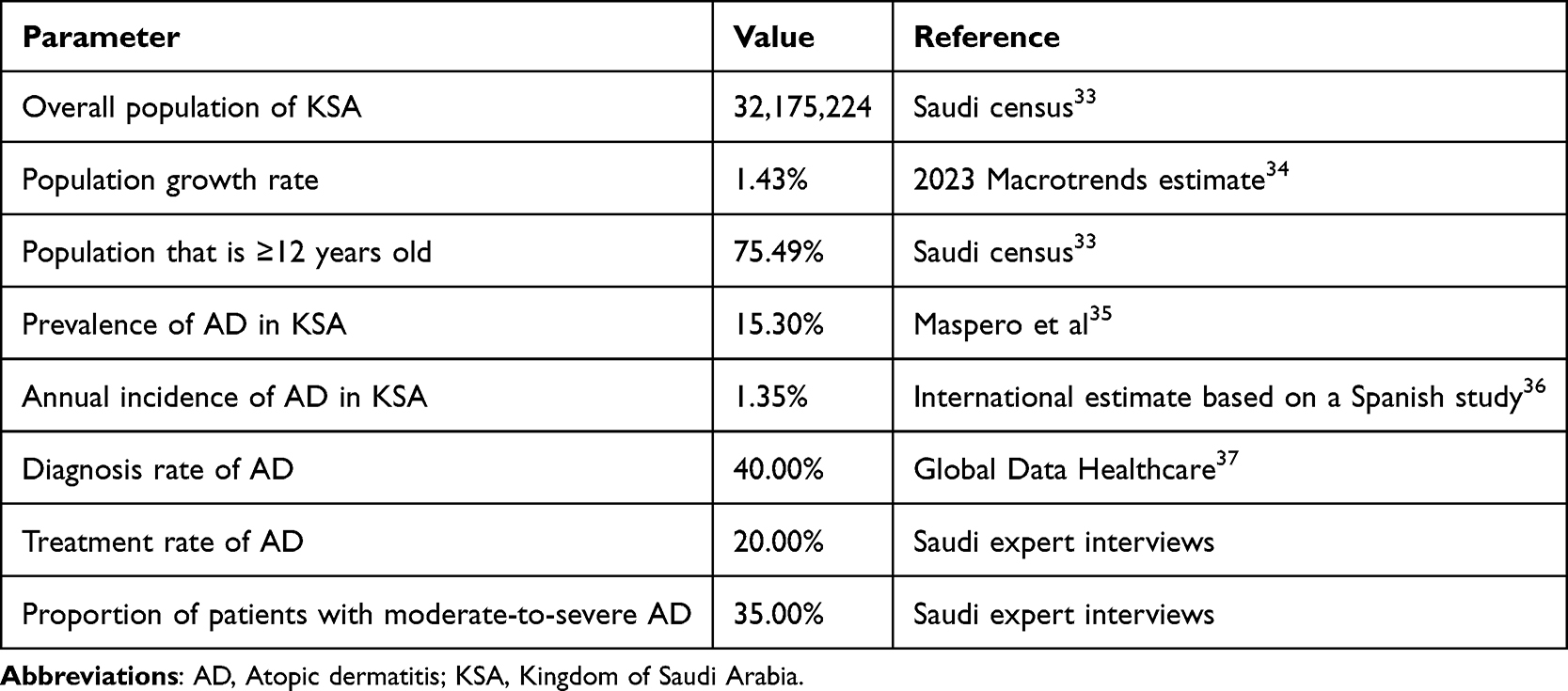 |
Table 3 Estimated Number of Moderate-to-Severe Adult and Adolescent AD Patients in 2024 |

For subsequent years, new eligible patients were estimated using annual AD incidence and estimated population growth, while the model carried forward previously eligible patients and applied cycle-level mortality and treatment pathways.
Market shares were based on historical data, IQVIA projections,38 and local expert input, reflecting current use (Scenario 1) and projected uptake (Scenario 2). Experts confirmed that abrocitinib, and tralokinumab are not currently used in the KSA public sector, so they were assigned no market share. Upadacitinib 15 mg accounted for 6.51% in Scenario 1 and was projected to increase gradually from 8.33% in year 1 to 12.67% in year 5 in Scenario 2. Detailed annual market shares are presented in Supplementary Table 6.
Sensitivity Analyses
We conducted sensitivity analyses to assess parameter uncertainty. In the CEA, deterministic sensitivity analysis (DSA) and probabilistic sensitivity analysis (PSA) were conducted for upadacitinib 15 mg versus dupilumab, with and without TCS. DSA results were presented as tornado diagrams based on NMB, while PSA results were presented using cost-effectiveness scatter plots. For the BIA, uncertainty was assessed using DSA and presented as tornado diagrams.
In the DSA, parameters were varied using 95% confidence intervals or predefined minimum and maximum values when available. Otherwise, parameters were varied by ±10%, except costs, which were varied by ±50% to reflect greater uncertainty. The PSA used 1,000 Monte Carlo simulations, with beta distributions for probabilities, event rates, and utilities; gamma distributions for costs; normal distributions for age and treatment-related disutilities; and log-normal distributions for relative treatment effects, following standard health economic modelling guidance. A list of model inputs and their corresponding sensitivity analysis values is provided in Supplementary Table 7.
Model Assumptions
Key assumptions were defined a priori based on the clinical pathway, previous AD economic models, local expert validation, and available Saudi data. Where local data were unavailable, international evidence was used for parameters expected to be less setting-specific, such as relative treatment effects and health-state utilities. Setting-dependent inputs, including unit costs, resource use, market shares, and background mortality, were informed by Saudi sources. Parameter uncertainty was assessed through DSA and PSA, and scenarios were conducted for different comparators and using TCS with treatments. A list of model assumptions, including the rationale for each assumption, is provided in Supplementary Table 8.
Data Analysis and Validation
The decision-analytic model and all analyses were implemented in Microsoft Excel (Microsoft Corporation, Redmond, WA, USA). Heterogeneity across patient subgroups was not explicitly explored, as the model aimed to inform cost-effectiveness and budget impact for moderate-to-severe patients in KSA overall rather for specific subgroups. The final models were validated using the framework by Nagy et al18 covering face validity (model structure and inputs), internal validity (technical and calculations validity), cross-validity (compared to other models), and external validity (compared to published evidence).
Results
CEA Model Results
In the base-case analysis, upadacitinib 15 mg was associated with lower total costs (−148,068 SAR) and higher QALYs (+0.21) compared with dupilumab over the model time horizon, resulting in a positive NMB of 158,656 SAR (Table 4).
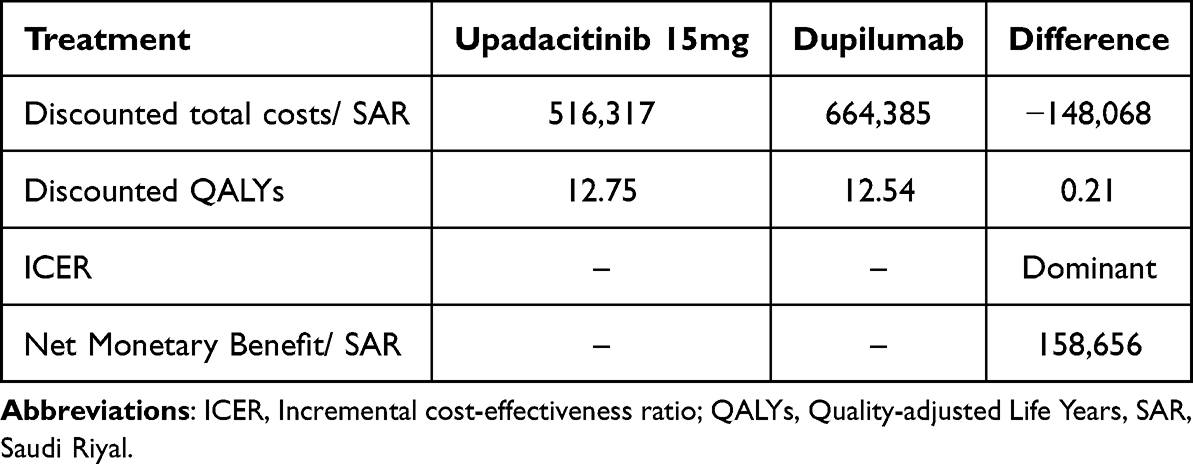 |
Table 4 UPA 15 mg vs Dupilumab Base-Case Cost-Effectiveness Model results |
In the scenario including TCS, upadacitinib 15 mg plus TCS was associated with lower costs (−205,679 SAR) and slightly lower QALYs (12.98 vs 13.01; difference: −0.035 QALYs) compared with dupilumab plus TCS. At a willingness-to-pay threshold of 50,000 SAR/QALY, this resulted in a positive NMB of 203,914 SAR. Results of this scenario are presented in Supplementary Table 9.
CEA Sensitivity Analyses
Base case DSA for upadacitinib 15 mg versus dupilumab indicates that the model’s three most sensitive inputs were dupilumab efficacy response at week 16, dupilumab compliance rates after year 2, and discount rate. The NMB remained positive across the tested upper and lower bounds for these parameters. Figure 3 presents the 20 inputs with the greatest impact on NMB.
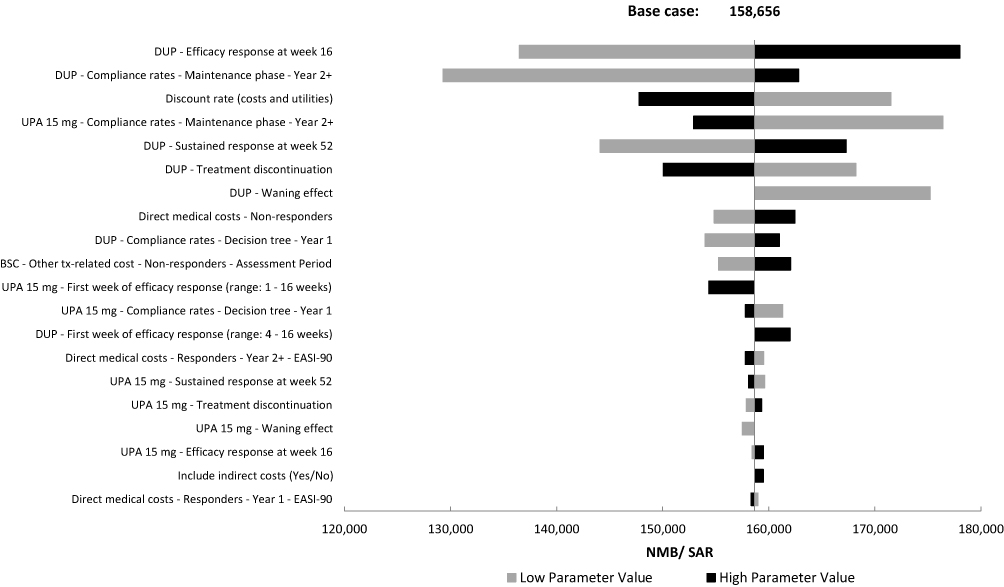 |
Figure 3 Deterministic sensitivity analysis (DSA) tornado diagram of upadacitinib 15 mg vs dupilumab illustrating the 20 most influential input parameters affecting the net monetary benefit. Abbreviations: BSC, Best supportive care; DUP, Dupilumab; EASI, Eczema Area Severity Index; NMB, Net monetary benefit, SAR, Saudi Riyal; UPA, Upadacitinib. |
For the upadacitinib 15 mg plus TCS versus dupilumab plus TCS, the DSA results reveal that the model is most sensitive to dupilumab plus TCS compliance rates after the first year, discount rate, and dupilumab plus TCS efficacy response at week 16 (Supplementary Figure 1).
The PSA simulated results for upadacitinib 15 mg versus dupilumab were predominantly below the cost-effectiveness threshold. Most simulations (94.9%) showed lower costs and higher QALYs, while 5.1% showed lower costs and lower QALYs compared with dupilumab (Figure 4).
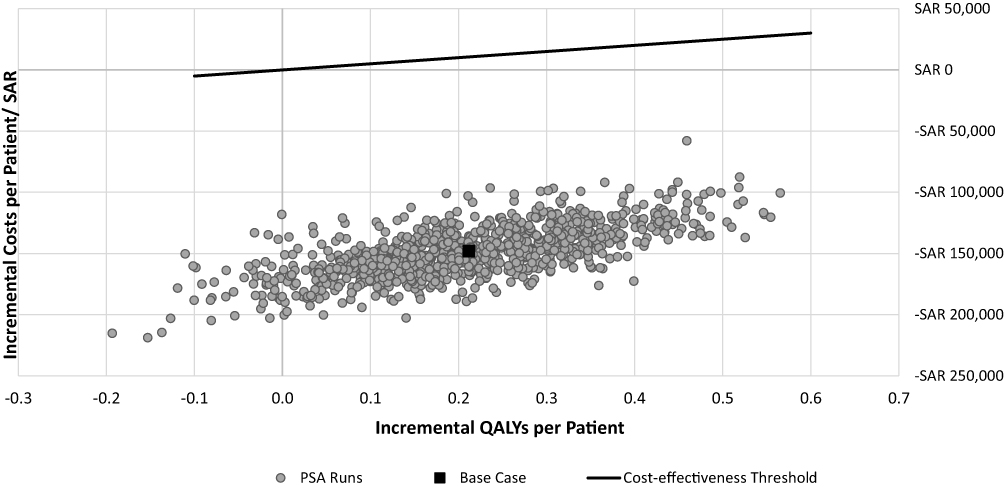 |
Figure 4 Probabilistic sensitivity analysis (PSA) scatter plot showing the results of base-case scenario and an additional 1,000 iterations. Abbreviations: PSA, Probabilistic Sensitivity Analysis; QALYs, Quality-adjusted life years. |
For the TCS scenario, PSA for upadacitinib 15 mg plus TCS versus dupilumab plus TCS showed consistently lower incremental costs, while incremental QALYs varied around zero, indicating higher or lower QALYs across simulations. All simulations remained below the cost-effectiveness threshold, reflecting lower costs with limited differences in QALYs between the two treatment options (Supplementary Figure 2).
BIA Model Results
The projected market share scenario was associated with lower estimated costs than the current market share scenario over five years. Cumulative costs were reduced from 28.13 billion to 26.58 billion SAR, corresponding to a total budget savings of 1.54 billion SAR. Annual differences ranged from −174 million SAR in year 1 to −429 million SAR in year 5. Annual cost details are presented in Table 5, and trends across both scenarios are shown in Figure 5.
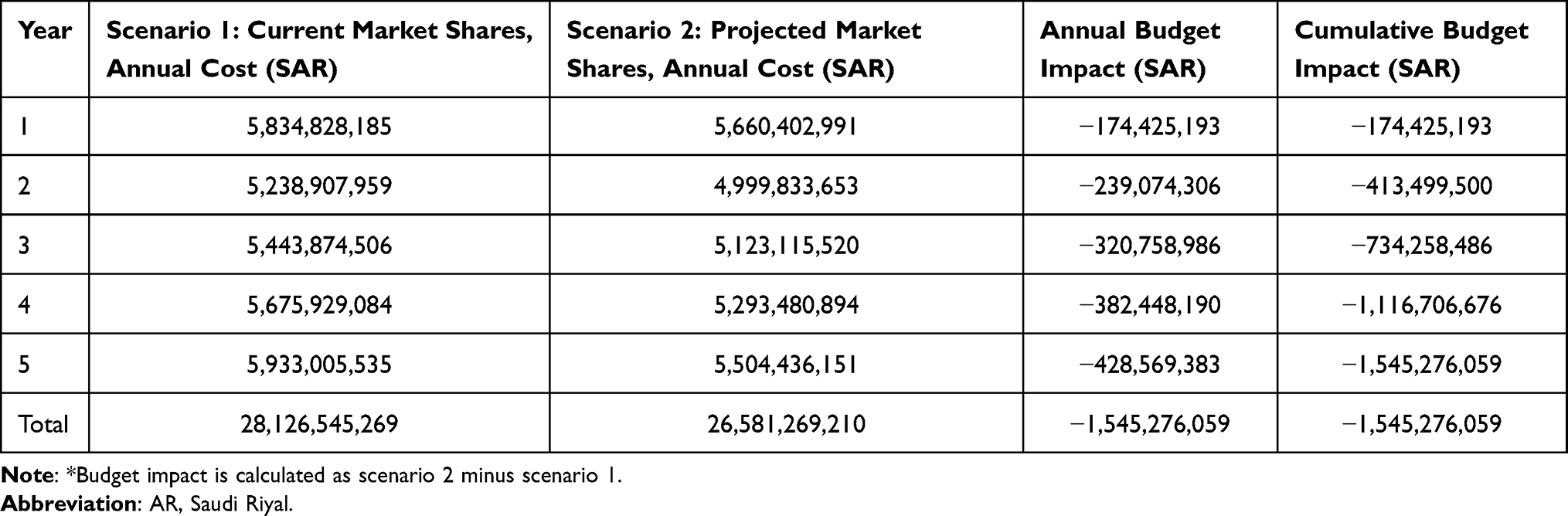 |
Table 5 Projected Annual Budget Impact of Increasing Upadacitinib Market Shares Over the Next 5 Years* |
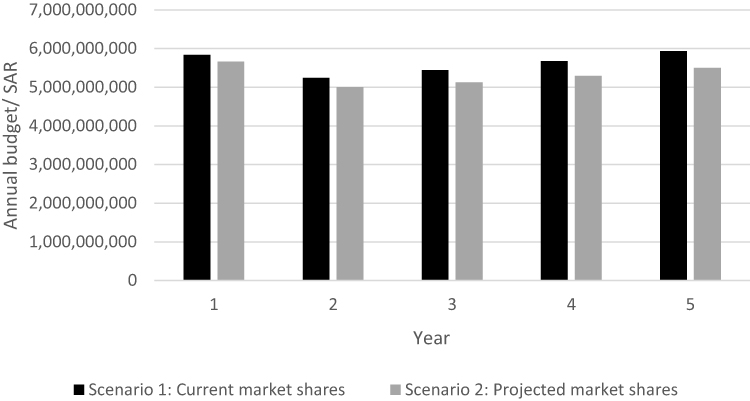 |
Figure 5 Advanced therapies budget for moderate-to-severe AD in KSA. Abbreviations: AD, Atopic dermatitis; SAR, Saudi Riyal; UPA, Upadacitinib. |
BIA Sensitivity Analysis
The one-way DSA for the BIA model showed that the model is most sensitive to the diagnosis rate, treatment rate, share of prevalent patients, and proportion of patients aged ≥12 years. Across tested parameter ranges, the projected market share scenario remained associated with budget savings compared to the current market share scenario (Supplementary Figure 3).
Incremental Analysis
In the incremental analysis, all interventions were compared to BSC. In the scenario without TCS, patients receiving BSC accrued 416,856 SAR in costs and gained 11.22 QALYs over the model time horizon. Upadacitinib 30 mg provided the largest incremental QALY gain versus BSC, followed by abrocitinib 200 mg and upadacitinib 15 mg. BSC, tralokinumab, upadacitinib 15 mg, and upadacitinib 30 mg formed the cost-effectiveness frontier, while the other interventions were dominated.
In the scenario with TCS, patients receiving BSC accrued 424,903 SAR and gained 11.26 QALYs over the model time horizon. Upadacitinib 30 mg plus TCS provided the largest incremental QALY gain versus BSC, followed by dupilumab, and upadacitinib 15 mg. BSC, tralokinumab + TCS, upadacitinib 15 mg + TCS, and upadacitinib 30 mg + TCS formed the cost-effectiveness frontier, while the remaining interventions were dominated.
Details of the incremental analysis are presented in Supplementary Tables 10 and 11 and illustrated in Supplementary Figures 4 and 5.
Discussion
This study presents a comprehensive economic evaluation of upadacitinib for moderate-to-severe AD in KSA from the public payer perspective, assessing its cost-effectiveness and budget impact. In the base-case analysis, upadacitinib 15 mg was associated with lower costs and higher QALYs compared with dupilumab, resulting in a positive NMB at the applied CET. Sensitivity analyses showed that the results remained below the CET when key inputs were varied, although the findings should be interpreted as model-based estimates that depend on input assumptions, data quality, and forecasts.
In the scenario with TCS, upadacitinib 15 mg plus TCS was associated with lower costs and slightly lower QALYs compared with dupilumab plus TCS. This placed some simulations of the PSA in the southwest quadrant of the cost-effectiveness plane, reflecting lower costs with lower effectiveness. However, the QALY difference was minor, resulting in an overall positive NMB at the selected threshold. PSA results showed uncertainty around the incremental QALYs, with simulations distributed around zero, while incremental costs remained consistently lower than the comparator.
The model incorporated local evidence where available, including unit costs, resource use, market shares, and background mortality. International data were used when local estimates were unavailable and when parameters were less likely to differ substantially by setting. To address this uncertainty in input parameters, deterministic sensitivity analyses varied model inputs, including wider ranges for cost parameters, and probabilistic analyses assessed joint parameter uncertainty. These analyses supported the overall direction of the findings, but they do not remove the inherent uncertainty associated with economic modelling.
The BIA suggested that increasing the projected market share of upadacitinib could reduce public healthcare costs over 5 years compared with current market shares. Estimated cumulative budget savings reached 1.54 billion SAR with annual savings increasing over time. The BIA DSA findings showed consistent budget savings across all tested scenarios, indicating that even with the uncertainty in input parameters, the projected market shares are expected to generate savings.
Overall, upadacitinib may be considered among treatment options for the target population in KSA, while decisions should account for clinical appropriateness, patient characteristics, affordability, and uncertainty in long-term model assumptions.
Our CEA results are consistent with previously published economic evaluations in the same disease area and among comparable target populations.13,39,40 In Spain, a study aiming to assess the cost-effectiveness of abrocitinib against other systemic treatments for severe AD in adults showed consistency with our results. Similar to our model, the Spanish study results also shows that upadacitinib 15 mg provides lower costs (€166,073 vs €177,407) and higher QALYs (5.88 vs 5.84) compared to dupilumab.13 While another study conducted in Singapore comparing dupilumab, abrocitinib, baricitinib, and upadacitinib in adults showed that dupilumab plus TCS present higher costs (S$59,416 vs S$47,547) and slightly higher QALYs (3.4946 vs 3.4875) compared to upadacitinib 15 mg plus TCS, which is also matching our results.39 The budget impact model results were also consistent with another study conducted in Argentina assessing the budget impact of upadacitinib for moderate-to-severe atopic dermatitis in adults and adolescents, with both analyses demonstrating cost savings. In the Argentine study, the model estimated savings of 7.3% from the social security perspective.40
The budget savings could help alleviate the financial burden of the disease on the healthcare system. Moreover, these freed-up resources could be strategically reallocated towards treating more patients, or towards other valuable interventions, potentially yielding even greater QALYs for the population. Considering the substantial prevalence of AD in KSA, these findings underscore the critical importance of strategic resource allocation in addressing this disease area. Effective resource allocation can yield significant benefits not only for the healthcare system, but also for the entire population by improving patient outcomes and QoL.
The study findings may be broadly applicable to the KSA public healthcare setting, as the inputs considered were representing data reflecting the overall public healthcare structure in KSA rather than a single institution. The timeliness of these study results is particularly noteworthy, as they coincide with KSA’s ongoing shift towards integrating health economics into policymaking and prioritizing resource allocation to enhance the overall health of its citizens. The findings of this model may support local policymakers in decision-making regarding resource allocation and healthcare budget planning in KSA.
Several limitations should be considered. First, some inputs, including utility values, treatment efficacy inputs, and age-specific incidence estimates, were not available from local sources. Global data were therefore used for these parameters, as they were expected to be less setting-specific than costs, resource use, market shares, and background mortality, which were informed by local sources. Nevertheless, we acknowledge that using non-local inputs may introduce uncertainty, although sensitivity analyses showed that the overall direction of the findings was maintained across the tested assumptions.
Second, indirect costs were not included because the analysis was conducted from the healthcare payer perspective. This is a conservative approach, as it may underestimate the broader economic burden of AD, including productivity losses due to absenteeism and presenteeism; results may therefore slightly differ if a societal perspective is adopted.
Third, variation across healthcare sectors in KSA may affect local inputs, including treatment patterns, patient characteristics, and market shares. This was partially addressed by using aggregated estimates from multiple experts and validating assumptions with additional local experts.
Fourth, heterogeneity was not explored among patient groups due to limitations in local patient population data.
Fifth, the base-case scenario used on an older NMA because the most recent NMA did not report EASI-50 data. This might have slightly affected the precision of treatment effect estimates; however, sensitivity analyses using alternative NMAs did not change the direction of the findings.
Finally, half-cycle correction was not applied, which may introduce minor approximation error in the annual Markov phase. However, this was expected to have a limited impact because the first year was modelled using weekly cycles, while long-term outcomes were driven by annual health-state distributions over a lifetime horizon extending up to 100 years, diluting the effect of half cycle correction adjustment.41
Conclusions
This study suggests that upadacitinib may represent a cost-effective treatment option for moderate-to-severe atopic dermatitis in KSA. In the CEA, upadacitinib 15 mg was associated with lower costs and higher QALYs compared with dupilumab, while upadacitinib 15 mg plus TCS had lower costs and slightly lower QALYs compared with dupilumab plus TCS, resulting in a positive NMB at the selected willingness-to-pay threshold. The BIA showed that increasing the projected market share of upadacitinib was associated with lower estimated healthcare costs over 5 years compared with current market shares. These findings suggest that upadacitinib could support both clinical and economic decision-making in KSA by offering an efficient treatment option while contributing to more sustainable allocation of healthcare resources.
Data Sharing Statement
All data are included in this article. Further inquiries can be directed to the corresponding author.
Ethics/Ethical Approval
This study was based on previously published studies, model-based economic evaluation, and aggregated expert input, and did not involve new interventional research with human participants or animals. Therefore, IRB approval was not required.
Acknowledgments
The authors would like to thank all contributors for their commitment and dedication in developing this model. The authors would like to acknowledge the writing assistance provided by Syreon Middle East and statistical analysis support provided by Syreon Middle East which were funded by AbbVie. Syreon Middle East was a contractual partner of Abbvie Saudi Arabia. The authors are fully responsible for all content and editorial decisions, were involved at all stages of abstract development, and have approved the final version.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by AbbVie GmbH, Kingdom of Saudi Arabia. AbbVie contributed to the design, analysis, and interpretation of data; in reviewing and approval of final version based on the authors’ input and direction. No honoraria or payments were made for authorship. AbbVie sponsored the analysis and interpretation of data.
Disclosure
BE, NAba, and ANF are employees at Syreon and may hold company shares. AS, MG, and ShAm are employees at Abbvie and may hold company shares. All other co-authors have not received any funding and report no conflicts of interest in this work.
References
1. Frazier W, Bhardwaj N. Atopic dermatitis: diagnosis and treatment. Am Fam Physician. 2020;101(10):590–14.
2. Kolb L, Ferrer-Bruker S. Atopic Dermatitis. StatPearls [Internet] Treasure Island (FL): statPearls Publishing. 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448071/.
3. Kleyn CE, Barbarot S, Reed C, et al. Burden of moderate to severe atopic dermatitis in adults from France, Italy, and the UK: patient-reported outcomes and treatment patterns. Dermatol Ther. 2022;12(8):1947–1965. doi:10.1007/s13555-022-00777-z
4. Taylor K, Swan DJ, Affleck A, Flohr C, Reynolds NJ. Treatment of moderate‐to‐severe atopic eczema in adults within the UK: results of a national survey of dermatologists. Br J Dermatol. 2017;176(6):1617–1623. doi:10.1111/bjd.15235
5. Chu DK, Schneider L, Asiniwasis RN, et al. Atopic dermatitis (eczema) guidelines: 2023 American Academy of Allergy, Asthma and Immunology/American College of Allergy, Asthma and Immunology joint task force on practice parameters GRADE–and institute of medicine–based recommendations. Ann Allergy Asthma Immunol. 2024;132(3):274–312. doi:10.1016/j.anai.2023.11.009
6. Royeck S. Biologics in the treatment of atopic dermatitis: approved active substances and monoclonal antibodies in advanced clinical trials. Allergo J Int. 2025;34(6):159–166. doi:10.1007/s40629-025-00340-0
7. Fomina DS, Mukhina OA, Mikhailova VI, et al. Treatment of atopic dermatitis with upadacitinib: adcare single center experience. Front Med. 2024;11:1385720. doi:10.3389/fmed.2024.1385720
8. Fasseeh AN, Elezbawy B, Korra N, et al. Burden of atopic dermatitis in adults and adolescents: a systematic literature review. Dermatol Ther. 2022;12(12):2653–2668. doi:10.1007/s13555-022-00819-6
9. Elezbawy B, Fasseeh AN, Fouly E, et al. The humanistic and economic burden of atopic dermatitis among adults and adolescents in Saudi Arabia. J Med Econ. 2022;25(1):1231–1239. doi:10.1080/13696998.2022.2152234
10. Elezbawy B, Fasseeh AN, Fouly E, et al. Humanistic and economic burden of atopic dermatitis for adults and adolescents in the middle east and africa region. Dermatol Ther. 2023;13(1):131–146. doi:10.1007/s13555-022-00857-0
11. Maraiki F, Bazarbashi S, Scuffham P, Tuffaha H. Methodological approaches to cost-effectiveness analysis in Saudi Arabia: what can we learn? A systematic review. MDM Policy Pract. 2022;7(1):23814683221086869. doi:10.1177/23814683221086869
12. Saudi Food and Drug Authority. Economic Evaluation Studies Guideline. 2024. Available from: https://sfda.gov.sa/sites/default/files/2024-07/EconomicEvaluationStudies.pdf.
13. Romero Jiménez RM, Herranz Pinto P, Domínguez C, et al. Cost-effectiveness analysis of abrocitinib compared with other systemic treatments for severe atopic dermatitis in Spain. Pharmacoecon Open. 2024;8(2):291–302. doi:10.1007/s41669-023-00459-2
14. Zimmermann M, Rind D, Chapman R, Kumar V, Kahn S, Carlson J. Economic evaluation of dupilumab for moderate-to-severe atopic dermatitis: a cost-utility analysis. J Drugs Dermatol. 2018;17(7):750–756.
15. Espinola N, Rodríguez Cairoli F, Rojas-Roque C, et al. Budget impact and cost per responder analysis of upadacitinib for the treatment of moderate to severe atopic dermatitis from the perspective of the social security and the private sector in Argentina. Expert Rev. Pharmacoeconomics Outcomes Res. 2025;25(1):101–111. doi:10.1080/14737167.2024.2394124
16. NICE. Single technology appraisal dupilumab for treating moderate to severe atopic dermatitis after topical treatments Available from: https://www.nice.org.uk/guidance/ta534/documents/committee-papers.
17. Edwards SJ, Karner C, Jhita T, et al. Abrocitinib, tralokinumab and upadacitinib for treating moderate-to-severe atopic dermatitis. Health Technol Assess. 2024;28(4):1–113. doi:10.3310/lexb9006
18. Nagy B, Szilberhorn L, Molnár A. Validation of decision models. In: Nagy B, Campbell JD, Kaló Z. editors. The Role of Modelling in Economic Evaluations in Health Care. 2019. https://www.eltereader.hu/media/2019/07/Nagy_Balazs_NT_WEB.pdf.
19. Husereau D, Drummond M, Augustovski F, et al. Consolidated Health Economic Evaluation Reporting Standards 2022 (CHEERS2022) Statement: updated Reporting Guidance for Health Economic Evaluations. MDM Policy Pract. 2022;7(1):23814683211061097. doi:10.1016/j.jval.2021.11.1351
20. Hanifin JM, Baghoomian W, Grinich E, Leshem YA, Jacobson M, Simpson EL. The Eczema Area and Severity Index—A Practical Guide. Dermatitis. 2022;33(3):187–192. doi:10.1097/DER.0000000000000895
21. UNdata. Population by age, sex and urban/rural residence; 2018. Available from: http://data.un.org/Data.aspx?d=POP&f=tableCode%3A22.
22. Al-Jedai AH, Lomas J, Almudaiheem HY, et al. Informing a cost-effectiveness threshold for Saudi Arabia. J Med Econ. 2023;26(1):128–138. doi:10.1080/13696998.2022.2157141
23. Guttman-Yassky E, Teixeira HD, Simpson EL, et al. Once-daily upadacitinib versus placebo in adolescents and adults with moderate-to-severe atopic dermatitis (Measure Up 1 and Measure Up 2): results from two replicate double-blind, randomised controlled Phase 3 trials. Lancet. 2021;397(10290):2151–2168. doi:10.1016/s0140-6736(21)00588-2
24. Silverberg JI, Gooderham MJ, Paller AS, et al. Early and sustained improvements in symptoms and quality of life with upadacitinib in adults and adolescents with moderate-to-severe atopic dermatitis: 52-week results from two Phase III randomized clinical trials (Measure Up 1 and Measure Up 2). Am J Clin Dermatol. 2024;25(3):485–496. doi:10.1007/s40257-024-00853-4
25. Simpson EL, Bieber T, Guttman-Yassky E, et al. Two phase 3 trials of dupilumab versus placebo in atopic dermatitis. N Engl J Med. 2016;375(24):2335–2348. doi:10.1056/NEJMoa1610020
26. Silverberg JI, Thyssen JP, Fahrbach K, et al. Comparative efficacy and safety of systemic therapies used in moderate‐to‐severe atopic dermatitis: a systematic literature review and network meta‐analysis. J Eur Acad Dermatol Venereol. 2021;35(9):1797–1810. doi:10.1111/jdv.17351
27. Silverberg JI, Hong HC, Calimlim BM, et al. Comparative efficacy of targeted systemic therapies for moderate-to-severe atopic dermatitis without topical corticosteroids: an updated network meta-analysis. Dermatol Ther. 2023;13(10):2247–2264. doi:10.1007/s13555-023-01000-3
28. NUPCO tenders. 2023. Available from: https://www.nupco.com/en/tenders/.
29. Reich K, Teixeira HD, de Bruin-Weller M, et al. Safety and efficacy of upadacitinib in combination with topical corticosteroids in adolescents and adults with moderate-to-severe atopic dermatitis (AD Up): results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2021;397(10290):2169–2181. doi:10.1016/S0140-6736(21)00589-4
30. van Hout B, Janssen MF, Feng Y-S, et al. Interim scoring for the EQ-5D-5L: mapping the EQ-5D-5L to EQ-5D-3L value sets. Value Health. 2012;15(5):708–715. doi:10.1016/j.jval.2012.02.008
31. Ara R, Brazier JE. Populating an economic model with health state utility values: moving toward better practice. Value Health. 2010;13(5):509–518. doi:10.1111/j.1524-4733.2010.00700.x
32. van der Schaft J, Politiek K, van den Reek JM, et al. Drug survival for ciclosporin A in a long‐term daily practice cohort of adult patients with atopic dermatitis. Br J Dermatol. 2015;172(6):1621–1627. doi:10.1111/bjd.13730
33. General Authority for Statistics. Saudi Census. 2024. Available from: https://portal.saudicensus.sa/portal/public/1/15/100646?type=TABLE.
34. Macrotrends. Saudi Arabia Population Growth Rate 1950-2024; 2024. Available from: https://www.macrotrends.net/global-metrics/countries/SAU/saudi-arabia/population-growth-rate.
35. Maspero J, Rubini ND, Zhang J, et al. Epidemiology of adult patients with atopic dermatitis in AWARE 1: a second international survey. World Allergy Organ J. 2023;16(3):100724. doi:10.1016/j.waojou.2022.100724
36. Arnedo-Pena A, Puig-Barberà J, Artero-Civera A, et al. Atopic dermatitis incidence and risk factors in young adults in Castellon (Spain): a prospective cohort study. Allergol Immunopathol. 2020;48(6):694–700. doi:10.1016/j.aller.2020.01.004
37. Clinical Trials Arena. Over 50% of all atopic dermatitis cases go undiagnosed in key pharmaceutical markets; 2022. Available from: https://www.clinicaltrialsarena.com/analyst-comment/atopic-dermatitis-cases-undiagnosed/#:~:text=These%20forecast%20data%20demonstrate%20that,primarily%20by%20misdiagnosis%20and%20underdiagnosis.
38. Prognosis IM. 2023. Available from: https://secure.constellation.iqvia.com/MarketPrognosisGlobal.
39. Ong C, Briones J, Lim ZZ, et al. Cost-effectiveness of dupilumab and oral janus kinase inhibitors for the treatment of moderate-to-severe atopic dermatitis in Singapore. Pharmacoecon Open. 2024;8(6):809–822. doi:10.1007/s41669-024-00507-5
40. Espinola N, Rodriguez Cairoli F, Rojas-Roque C, et al. Budget impact analysis of upadacitinib for moderate-to-severe atopic dermatitis for social security and private third-party payers in Available from: https://www.ispor.org/docs/default-source/intl2023/2021unbrandedpostertemplatevertispor-usa-priemr-borradoriecs-003-pdf.pdf?sfvrsn=edcf7dd4_0.
41. Nemeth B, Vincziczki Á. The role of half-cycle correction in the models used for health technology assessment. Value Health. 2013;16(7):A592–3. doi:10.1016/j.jval.2013.08.1654
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Managing Atopic Dermatitis with Lebrikizumab – The Evidence to Date
Labib A, Ju T, Yosipovitch G
Clinical, Cosmetic and Investigational Dermatology 2022, 15:1065-1072
Published Date: 8 June 2022
Management of Atopic Dermatitis: Clinical Utility of Ruxolitinib
Owji S, Caldas SA, Ungar B
Journal of Asthma and Allergy 2022, 15:1527-1537
Published Date: 25 October 2022
Alternative Psychotherapeutic Approaches to the Treatment of Eczema
Oska C, Nakamura M
Clinical, Cosmetic and Investigational Dermatology 2022, 15:2721-2735
Published Date: 14 December 2022
Improving Psychological Health Outcomes in Children with Atopic Dermatitis
Mostafa N, Smith SD
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2821-2827
Published Date: 10 October 2023
Cost-Effectiveness and Budget Impact Analyses of Selective Internal Radiation Therapy versus Atezolizumab Plus Bevacizumab from a German Statutory Health Insurance Perspective
Schwander B, Klesper K, Rossol S, Herrmann K, Zoellner YF
ClinicoEconomics and Outcomes Research 2024, 16:483-492
Published Date: 6 June 2024