Back to Journals » Journal of Inflammation Research » Volume 18
Comments on “Temporal Relationship Between Visceral Fat and Inflammation, and Their Joint Effect on Cardiometabolic Diseases: Evidence from the China Health and Retirement Longitudinal Study (CHARLS)” [Response to Letter]
Mengyue Lin,1–4 Xuerui Tan,1–4 Yequn Chen1,3,4
1Department of Cardiology, First Affiliated Hospital of Shantou University Medical College, Shantou, People’s Republic of China; 2Shantou University Medical College, Shantou, People’s Republic of China; 3Clinical Research Center, First Affiliated Hospital of Shantou University Medical College, Shantou, People’s Republic of China; 4Human Phenome Institute of Shantou University Medical College, Guangdong Engineering Research Center of Human Phenome, Chemistry and Chemical Engineering Guangdong Laboratory, Shantou, People’s Republic of China
Correspondence: Xuerui Tan; Yequn Chen, Email [email protected]; [email protected]
View the original paper by Dr Lin and colleagues
This is in response to the Letter to the Editor
Dear editor
We appreciate the interest and insightful comments from Dr. Zhang regarding our study entitled “Temporal Relationship Between Visceral Fat and Inflammation, and Their Joint Effect on Cardiometabolic Diseases: Evidence from the China Health and Retirement Longitudinal Study. (CHARLS)”.1 In our study, a total of 9559 participants, followed up to 9 years, were included. We found that visceral fat accumulation and inflammation were individually and jointly associated with cardiometabolic disease (CMD) risk. Individuals with concomitant high visceral fat accumulation and elevated inflammation have highest risk of hypertension, diabetes, heart disease, and stroke. There was a biological interaction between visceral fat and inflammation on the incident hypertension and diabetes. In addition, a unidirectional temporal relationship from baseline visceral fat to follow-up inflammation levels was observed. These indicated that combined assessment of both visceral fat and inflammation may improve risk stratification and primary prevention of CMD. We would like to address the valuable points raised by Zhang.2
Based on potential mechanisms linking visceral fat and inflammation, this study was conducted to verify one of our hypotheses that there might be a bidirectional relationship between the two factors. A cross-lagged path analysis was performed to evaluate the bidirectional relationship between Chinese visceral adiposity index (CVAI) and high-sensitivity C-reactive protein (hs-CRP), including both directions (visceral fat → inflammation, and inflammation → visceral fat). As shown in Figure 3 (in the original paper), there were temporal relationships from baseline CVAI to follow-up hs-CRP, but not from baseline hs-CRP to follow-up CVAI, indicating a unidirectional relationship. Despite the theoretical possibility that inflammation influences visceral fat accumulation, our study found no statistical evidence for this reverse causal pathway. However, future research should account for potential variations in results due to heterogeneity in populations, disease types, and analytical models. We agree with Dr. Zhang’s opinion that other statistical methods can be used to further verify the causal relationship.
As described in the limitation section, we used a hs-CRP threshold of 1mg/L in the primary analyses given the number of groups and sample size, which was lower than that in some previous studies. It is noteworthy that even a low-grade inflammation could increase CMD risk by interacting with visceral fat accumulation. Moreover, the stability of the main results was verified in sensitivity analyses using 1 or 3 as the threshold for hs-CRP, in which similar results were observed (Table S8 in the original paper).
While both multiplicative and additive interaction analyses evaluate effect modification between exposures, they operate on different scales (ratio or difference), and thus address distinct research questions. Consequently, the results from these two approaches may not always be consistent. As far as we know, additive interaction is more sensitive for assessing biological interactions,3 and it has more values in public health and clinical decision-making, as it provided quantitative measurement of additional absolute risks.4 We agree with Dr. Zhang that the effect of visceral fat accumulation and inflammation may not be completely synergistic, which needs to be further explored through more statistical analyses and basic experimental research. Nonetheless, the combined assessment of both visceral fat and inflammation could be used to identify individuals early who are at high risk of hypertension and diabetes.
As mentioned in the original paper, our findings require verification in population from other regions or ethnic backgrounds, as well as in younger individuals, because the included population was composed of middle-aged and elderly people from China. It is noteworthy that similar results regarding the individual effects of visceral adiposity and inflammation on cardiovascular diseases were reported from different populations.5–9 Future studies from other regions or populations are warranted to explore the combined and interaction effects of visceral fat and inflammation on cardiovascular diseases. In response to Zhang’s comments, we have provided the baseline characteristics of the exclusion population and compared them with the inclusion population, based on available data (Table 1). Characteristics of BMI, drinking status, blood pressure, serum creatinine, and hs-CRP were statistically comparable between the two groups of population (P > 0.05). The other baseline characteristics showed significant but slight difference, which may mainly due to the relatively large sample size. For instance, there was statistical difference in age between the two groups (P < 0.001), but the difference in mean value was only 0.5 years. Similarly, for the fasting plasma glucose, the difference was only 0.1 mmol/L, whereas the P value was 0.004. Although there was higher proportion of cardiometabolic diseases in the inclusion group, the prevalences of hypertension and diabetes of the inclusion population (mainly composed of middle-aged and elderly people) were similar to reports of other nationwide surveys in China.10,11 In addition, missing data may have contributed to the underestimation of the prevalences in the excluded population. We agree with Dr. Zhang that the generalizability of the results should be verified in other populations.
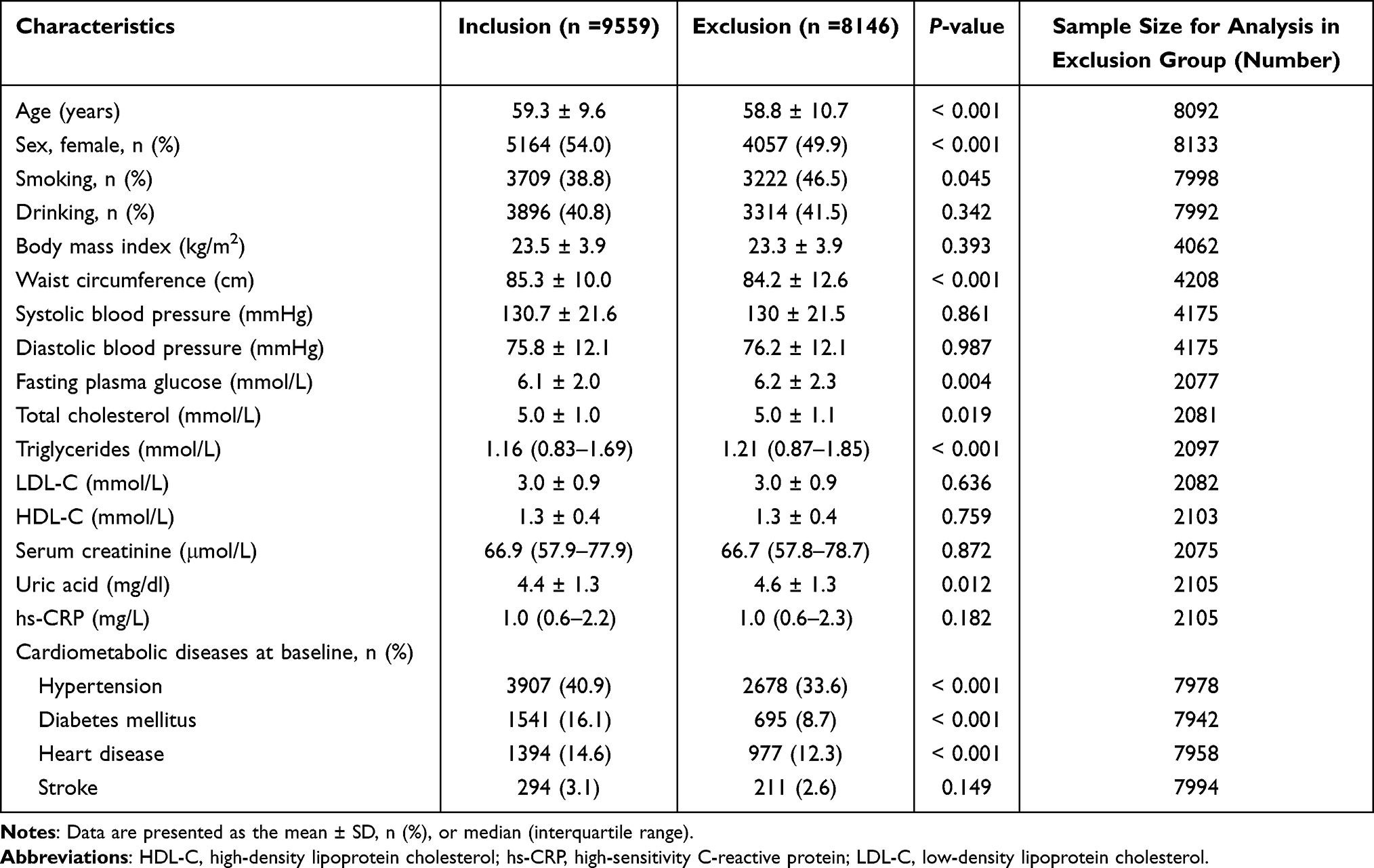 |
Table 1 Comparison in Baseline Characteristics Between Inclusion and Exclusion Populations |
In summary, Dr. Zhang’s comments, which focused on the stability and generalizability of our findings, are valuable for improving the current study and instructive for future research. We believe that our study provides a comprehensive insight for understanding the association and potential mechanisms between visceral fat accumulation, inflammation and cardiometabolic diseases. Approaches that simultaneously target adiposity and inflammation should yield greater benefits than targeting each individual risk factor. In addition, future studies focus on the incremental value of CVAI and hs-CRP in risk prediction models would be valuable.
Data Sharing Statement
No new data has been generated for this communication.
Author Contributions
Mengyue Lin – Conceptualization, Formal analysis, Writing – original draft, Writing – Review & Editing; Xuerui Tan – Conceptualization, Data curation, Validation, Writing – Review & Editing; Yequn Chen – Conceptualization, Data curation, Validation, Writing – Review & Editing. All authors agreed to the journal where this communication was submitted, agreed to the final version submitted for publication and agree to be accountable for the contents of this communication.
Funding
This communication did not receive any funding.
Disclosure
The authors declare that they have no competing interests.
References
1. Lin M, Zhou Y, Wu R. et al. Temporal relationship between visceral fat and inflammation, and their joint effect on cardiometabolic diseases: evidence from the China Health and Retirement Longitudinal Study (CHARLS). J Inflamm Res. 2025;18:14913–14926. doi:10.2147/JIR.S539644
2. Zhang Z. Comments on “Temporal relationship between visceral fat and inflammation, and their joint effect on cardiometabolic diseases: evidence from the China Health and Retirement Longitudinal Study (CHARLS)” [Letter]. J Inflamm Res. 2025;18:16063–16064. doi:10.2147/JIR.S580342
3. Ahlbom A, Alfredsson L. Interaction: a word with two meanings creates confusion. Eur J Epidemiol. 2005;20(7):563–564. doi:10.1007/s10654-005-4410-4
4. Andersson T, Alfredsson L, Källberg H, Zdravkovic S, Ahlbom A. Calculating measures of biological interaction. Eur J Epidemiol. 2005;20(7):575–579. doi:10.1007/s10654-005-7835-x
5. Amato MC, Giordano C, Galia M, et al. Visceral adiposity index: a reliable indicator of visceral fat function associated with cardiometabolic risk. Diabetes Care. 2010;33(4):920–922. doi:10.2337/dc09-1825
6. Zhang Z, Zhao L, Lu Y, Meng X, Zhou X. Association between Chinese visceral adiposity index and risk of stroke incidence in middle-aged and elderly Chinese population: evidence from a large national cohort study. J Transl Med. 2023;21(1):518. doi:10.1186/s12967-023-04309-x
7. Nusrianto R, Tahapary DL, Soewondo P. Visceral adiposity index as a predictor for type 2 diabetes mellitus in Asian population: a systematic review. Diabetes Metab Syndr. 2019;13(2):1231–1235. doi:10.1016/j.dsx.2019.01.056
8. Lin M, Li N, Heizhati M, et al. Chinese visceral adiposity index is associated with incident renal damage in patients with hypertension and abnormal glucose metabolism: a longitudinal study. Front Endocrinol. 2022;13:910329. doi:10.3389/fendo.2022.910329
9. Hamirani YS, Pandey S, Rivera JJ, et al. Markers of inflammation and coronary artery calcification: a systematic review. Atherosclerosis. 2008;201(1):1–7. doi:10.1016/j.atherosclerosis.2008.04.045
10. Wang Z, Chen Z, Zhang L, et al. Status of hypertension in China: results from the China hypertension survey, 2012–2015. Circulation. 2018;137(22):2344–2356. doi:10.1161/CIRCULATIONAHA.117.032380
11. Wang L, Peng W, Zhao Z, et al. Prevalence and treatment of diabetes in China, 2013–2018. JAMA. 2021;326(24):2498–2506. doi:10.1001/jama.2021.22208
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.