Back to Journals » Journal of Inflammation Research » Volume 18
Temporal Relationship Between Visceral Fat and Inflammation, and Their Joint Effect on Cardiometabolic Diseases: Evidence from the China Health and Retirement Longitudinal Study (CHARLS)
Authors Lin M ![]() , Zhou Y, Wu R, Li S, Ni X, Xiao J, Han S, Tang H, Huang J, Wen J
, Zhou Y, Wu R, Li S, Ni X, Xiao J, Han S, Tang H, Huang J, Wen J ![]() , Jiang L, Tan X
, Jiang L, Tan X ![]() , Chen Y
, Chen Y
Received 11 May 2025
Accepted for publication 2 October 2025
Published 27 October 2025 Volume 2025:18 Pages 14913—14926
DOI https://doi.org/10.2147/JIR.S539644
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Qing Lin
Mengyue Lin,1– 3,* Yilian Zhou,4,* Ruijie Wu,1,5 Shaobin Li,1,2 Xiaobin Ni,1 Jiaxin Xiao,1 Sirui Han,1,5 Haoxian Tang,1,2 Jieshan Huang,1,5 Jiasheng Wen,1,2 Liwen Jiang,1,2 Xuerui Tan,1– 3,6 Yequn Chen1,3,6
1Department of Cardiology, First Affiliated Hospital of Shantou University Medical College, Shantou, People’s Republic of China; 2Department of Clinical Medicine, Shantou University Medical College, Shantou, People’s Republic of China; 3Clinical Research Center, First Affiliated Hospital of Shantou University Medical College, Shantou, People’s Republic of China; 4Second Ward of Intensive Care Unit, First Affiliated Hospital of Shantou University Medical College, Shantou, People’s Republic of China; 5Department of Preventive Medicine, Shantou University Medical College, Shantou, People’s Republic of China; 6Human Phenome Institute of Shantou University Medical College, Guangdong Engineering Research Center of Human Phenome, Chemistry and Chemical Engineering Guangdong Laboratory, Shantou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xuerui Tan, Email [email protected] Yequn Chen, Email [email protected]
Background: Both visceral fat accumulation and inflammation are commonly observed in cardiometabolic diseases (CMD). We aimed to evaluate their joint effects on CMD risk, and assessed their temporal relationship and biological interactions.
Methods: The study comprised 9559 individuals from the China Health and Retirement Longitudinal Study (CHARLS), a nationally representative cohort initiated in 2011 and completed follow-up through 2020. Visceral fat was measured by the Chinese visceral adiposity index (CVAI), and inflammation was indicated by high-sensitivity C-reactive protein (hs-CRP). Multivariate regression analyses were applied to evaluate the joint effects of CVAI and hs-CRP on CMD, including hypertension, diabetes, heart diseases, and stroke. A cross-lagged panel model was used to examine the temporal relationship. Multiplicative and additive interactions were also assessed.
Results: The mean age of the study population was 59.3 ± 9.6 years, and 5164 (54.0%) were women. Both cross-sectional and longitudinal analyses yielded consistent results that visceral fat and inflammation were individually and jointly associated with CMD. When evaluating the effect of co-exposure, the highest CMD risks were observed for individuals with high CVAI and hs-CRP levels. Compared with people with low CVAI (< 93.32 [median]) and hs-CRP (< 1 mg/L), those concurrently with high CVAI (≥ 93.32) and hs-CRP (≥ 1 mg/L) had double the increased risk of diabetes and stroke, and 40% increased risk of hypertension and heart diseases. A unidirectional temporal relationship from baseline CVAI to follow-up hs-CRP was observed, with a standardized correlation coefficient of 0.130 (P < 0.001). There was significantly biological interaction between CVAI and hs-CRP, and the attributable proportion due to interaction was 19% for hypertension and 14% for diabetes.
Conclusion: The concurrent visceral fat accumulation and elevated inflammation synergistically lead to highest risks of CMD. The combined assessment of both factors may improve risk stratification and primary prevention of cardiometabolic diseases.
Keywords: visceral fat, inflammation, cardiometabolic diseases, additive interaction, temporal relationship
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Zhang has been published for this article.
Introduction
Cardiometabolic diseases (CMD), mainly involving hypertension, diabetes, obesity, dyslipidemia, coronary heart disease (CHD) and stroke, contribute more to morbidity and mortality than any other disorders.1,2 Globally, CMD is one of the greatest challenges to the public health burden, resulting in huge financial costs.3 In China, cardiovascular disease (CVD) was estimated in 2019 to affect about 330 million patients, in which 245 million with hypertension, 11.39 million with CHD, and 13 million with stroke, and more than 40% of deaths were attributable to CVD.4 The prevalence of diabetes was 12.8%, with an estimated 129.8 million adults affected in China.5 Along with the population aging and steady rise in the prevalence of metabolic risk factors, CMD has been and is rapidly increasing, and the burden will continue to expand. Although the mortality and disability rates are high, CMD is largely preventable and controllable. Given the impact on quality of life and financial implications, the opinion that prevention is always better than cure is desirable. In this perspective, early identification of high-risk individuals for primary prevention would be highly beneficial. However, although many factors have been proven to be predictive for CMD, approximately one third of individuals who experience a first-time cardiovascular event are misclassified as being low risk on the basis of traditional risk factors.6 Identifying entirely novel biomarkers that can significantly improve risk prediction is arduous. In reality, the complex process of CMD indicates that studying such diseases from the perspective of a single factor is inherently one-sided and limited.
Both visceral fat accumulation and chronic systemic inflammation are closely associated with CMD.7–9 As a phenotype of obesity, visceral adiposity has been demonstrated to outperform the general obesity phenotype in predicting CMD, and the Chinese visceral adiposity index (CVAI) is considered the optimal non-invasive indicator for measuring visceral fat.10–12 Moreover, its association with CMD has been robustly demonstrated in several recent studies.13–15 A proinflammatory milieu usually exists in patients with hypertension, obesity, diabetes, or other cardiovascular disorders.16 Mechanically, visceral adipose tissue (VAT) can promote the production and release of inflammatory cytokines directly or indirectly, which amplifies inflammatory response.17 These VAT-related pro-inflammatory cytokines, such as tumor necrosis factor-α and interleukin-6, contributes to abnormal metabolism by inducing insulin resistance, promoting endothelial dysfunction, fostering oxidative stress, and altering lipid metabolism.18,19 A genetic study reported a polygenic overlap between C-reactive protein (CRP) and plasma lipids, indicating the need to consider the role of both inflammation and lipid metabolism in evaluating risk of related diseases.20 Evidence has accumulated supporting the use of high-sensitivity C-reactive protein (hs-CRP) as a clinical measure of inflammation.21 In recent years, several studies found that some indicators related to obesity or lipid profile have different effects on CMD at different CRP levels, and some of them have synergistic effects with CRP.22–24 However, few studies have focused on the temporal relationship and the combined effect between CVAI and CRP.
Understanding the joint effects on diseases and the potential causal relationship can provide new insights into the mechanisms of disease occurrence and development. It would be beneficial for prevention strategies by translating the biological interweaving into epidemiological practice. Therefore, we conducted the present study using a nationally representative cohort to evaluate the combined effects of visceral fat (measured by CVAI) and inflammation (measured by hs-CRP) on the risk of CMD, including hypertension, diabetes, heart diseases, and stroke. We also assessed the temporal relationship between CVAI and hs-CRP, and explored their biological interactions.
Materials and Methods
Study Design and Population
The study population was from the China Health and Retirement Longitudinal Study (CHARLS), which is an ongoing nationally representative survey that aims to evaluate the social, economic, and health circumstances of Chinese community residents. The study procedure and the cohort profile were detailed previously.25 Briefly, a total of 17,708 individuals from 150 counties or districts and 450 villages within 28 provinces of China participated in the baseline survey between June 2011 and March 2012. Four subsequent follow-ups were performed in 2013–2014 (wave 2), 2015–2016 (wave 3), 2017–2018 (wave 4), and 2020 (wave 5), with blood samples collected in wave 1 and wave 3. The CHARLS received approval from the institutional review board of Peking University, and all participants provided written informed consent. The present study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee at the First Affiliated Hospital of Shantou University Medical College.
Study design and population selection were illustrated in Figure 1. Firstly, we excluded those without data of blood and physical examination, diagnosed malignant tumor, and with missing data. Accordingly, 9559 individuals out of 17,708 participants were included in the cross-sectional analysis. Secondly, among the 9559 individuals with complete baseline information, we further excluded those with history of cardiometabolic diseases and who were without any available follow-up data. The remaining subjects were followed up until 2020 and were included in the longitudinal analyses. Thirdly, those with complete blood examination in both wave 1 and wave 3 were included in the cross-lagged path analysis to evaluate the temporal relationship between visceral fat and inflammation.
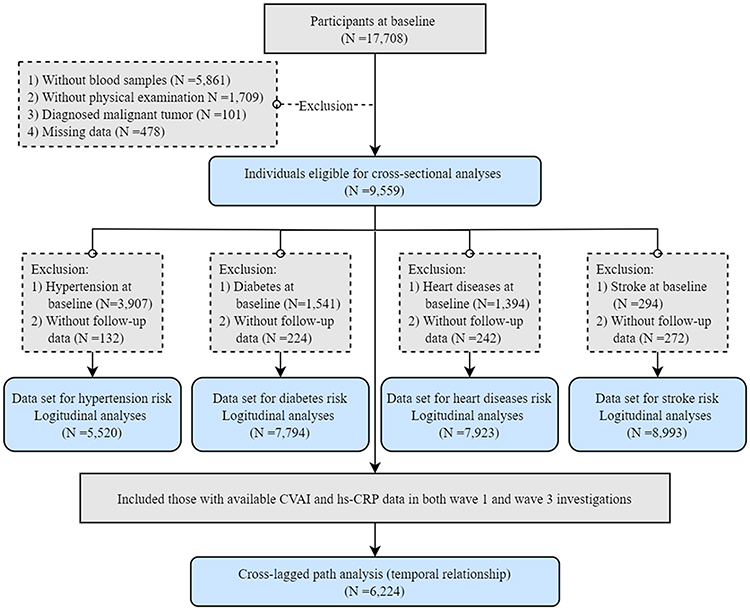 |
Figure 1 Flow chart of sample selection. |
Data Collection and Definition of Diseases
Details of data collection and the row data are available on the CHARLS website (http://charls.pku.edu.cn/en). A standardized questionnaire was applied for collecting information on demographic, socioeconomic and health-related data through face-to-face computer-assisted personal interviews at baseline survey and at each follow-up wave. Physical examinations were conducted by trained staff members, and venous blood samples were collected and tested using uniform assay methods.26 Variables extracted for the present study included age, sex, height, weight, waist circumference (WC), smoking status (ever/current or never), alcohol consumption (ever/current or never), educational levels (primary and below, middle school, or high school and above), systolic blood pressure (SBP), diastolic blood pressure (DBP), fasting plasma glucose (FPG), total cholesterol (TC), triglycerides (TG), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), serum creatinine (Scr), uric acid (UA), high-sensitivity C-reactive protein (hs-CRP), and disease status (including hypertension, diabetes, heart diseases, and stroke). Body mass index (BMI) was calculated by dividing weight by height-squared. The mean value of three measurements of blood pressure (BP) was used for analysis. Abdominal obesity was defined as a WC ≥90 cm for men and ≥85 cm for women.
Exposure and Outcome
Primary exposure was the joint effect of visceral fat and inflammation, which was assessed by CVAI and hs-CRP, respectively. The combined effect was defined according to baseline CVAI median (<93.32 or ≥93.32) and hs-CRP threshold (<1 mg/L or ≥1 mg/L). Therefore, four groups were generated as follows: group 1 served as reference and included those with CVAI <93.32 and hs-CRP <1; group 2 included those with CVAI <93.32 and hs-CRP ≥1; group 3 included those with CVAI ≥93.32 and hs-CRP <1; and group 4 included those with CVAI ≥93.32 and hs-CRP ≥1. The calculation formula of CVAI is as follows:27


The study outcome was cardiometabolic diseases, which included hypertension, diabetes, heart diseases, and stroke. The information of such diseases was collected by self-reported physician’s diagnosis, with the question of “Have you been told by a doctor that you have been diagnosed with hypertension/diabetes/heart diseases/stroke?” In addition, individuals who reported no history of hypertension or diabetes, but had a BP ≥140/90 mmHg or FPG ≥7.0 mmol/L, were classified as diagnosed with hypertension or diabetes, respectively. Heart diseases included heart attack, CHD, angina, and congestive heart failure. In the longitudinal analyses, participants contributed their follow-up time until the occurrence of the disease or the last available follow-up visit.
Statistical Analyses
Baseline information was summarized across the four co-exposure groups. Data are presented as mean ± standard deviation (SD), median (interquartile range), or number (percentage) where appropriate. Analysis of variance and chi-square tests were used for comparison of continuous and categorical variables, respectively. Kruskal–Wallis H-test was used for comparison of variable with skewed distribution.
The prevalences and person-year incidences of cardiometabolic diseases were calculated in the cross-sectional and longitudinal analyses, respectively. Logistic and Cox regression analyses were applied to explore the effect of CVAI and hs-CRP separately and their joint effect on each of the diseases. Three multivariable models were constructed for evaluating the independent association. Model 1 adjusted for demographic factors, including age, sex, smoking status, alcohol consumption and educational level. Model 2 further considered physical and laboratory examinations, including SBP, FPG, TC, LDL-C, Scr, and UA. Model 3 adjusted for variables in model 2 plus the cardiometabolic diseases (for the other disease analyses). The effect coefficients and the 95% confidence intervals (CIs) were calculated for binary CVAI and hs-CRP separately, each SD increase, and co-exposure (4 groups). Several sensitivity analyses were performed to evaluate the robustness of the main results. Firstly, given that no clear threshold for hs-CRP currently exists, we repeated the above analyses using another suggested clinical cutoff (<1, 1 to 3, ≥3 mg/L)28,29 to re-define the co-exposure. Secondly, for addressing the potential reverse causation, we performed repeated analyses by excluding those with endpoints occurring within the first follow-up visit. Thirdly, those with kidney diseases or hs-CRP ≥10 mg/L were excluded, considering potential confounding effects. To evaluate heterogeneity of the association, stratified analyses with multiplicative interaction terms were conducted according to different subgroups of age (<60 or ≥60 years), sex (female or male), BMI (<24 or ≥24 kg/m2), abdominal obesity (yes or no), smoking status (ever/current or never), and drinking status (ever/current or never).
The longitudinal design and repeated measurements of CVAI and hs-CRP at two time points (in both wave 1 and wave 3) was typically a cross-lagged panel design,30 which was applied in the present study to assess the temporal relationship between CVAI and hs-CRP. As a form of path analysis, the cross-lagged panel analysis simultaneously examined reciprocal and longitudinal relationships among a set of intercorrelated variables.23 One of two paths was designed to describe the effect of baseline CVAI (T1_CVAI) on follow-up hs-CRP (T2_hs-CRP), and another path indicated the effect of baseline hs-CRP (T1_hs-CRP) on follow-up CVAI (T2_CVAI). Prior to path analysis, the baseline and follow-up values of log-transformed CVAI and log-transformed hs-CRP were adjusted for age, sex, smoking and drinking status, educational levels, SBP, FPG, TC, LDL-C, Scr, UA, and history of cardiometabolic diseases by regression residual analyses, and then standardized by Z-transformation (mean =0, SD =1). The cross-lagged path coefficients were estimated simultaneously based on the correlation matrix using the maximum likelihood method. A significant coefficient would suggest directionality of the relationship. Based on the significant temporal relationships in path analysis, we further evaluated the joint effect of T1_CVAI and T2_hs-CRP on the disease, by using the above analysis strategies.
We also assessed biological interactions between visceral fat and inflammation by calculating parameters of additive interaction,31 including relative excess risk due to interaction (RERI), attributable proportion due to interaction (AP), and synergy index (SI).32,33 Specifically, when the 95% CI did not contain 0 for RERI and AP, and did not contain 1 for SI, it would indicate a significant interaction between the two variables. When RERI >0, AP >0, and SI >1, it would suggest that the combined effect of CVAI and hs-CRP on the cardiometabolic disease exceeded the sum of their individual effects, indicating a synergistic effect. Statistical analyses were conducted using SPSS 23.0 and R version 4.0.3 for Windows. A two-sided P <0.05 was considered statistically significant, except for interaction testing, in which P <0.1 was considered significant given the reduced statistical power for detecting interaction effects and the exploratory nature of the analyses.
Results
Baseline Characteristics of the Study Population
A total of 9559 participants were finally included (Figure 1), with mean age 59.3 ± 9.6 years, and 54.0% (n =5164) were female. The mean BP and FPG were 131/76 mmHg and 6.1 mmol/L, respectively. The proportions of cardiometabolic diseases at baseline were 40.9% (n =3907) for hypertension, 16.1% (n =1541) for diabetes, 14.6% (n =1394) for heart diseases, and 3.1% (n =294) for stroke. Details of baseline characteristics across the CVAI and hs-CRP groups are shown in Table 1. Participants with higher CVAI and hs-CRP had higher BMI, BP, FPG, TC, LDL-C, and UA levels, and also higher prevalence of cardiometabolic diseases (P for trend <0.001). Significant differences were observed in the prevalences between group 1 (low CVAI & low hs-CRP) and group 4 (high CVAI & high hs-CRP), which including 26.3% vs 57.7% for hypertension, 8.8% vs 24.5% for diabetes, 10.9% vs 19.0% for heart diseases, and 1.9% vs 4.5% for stroke (all P <0.001).
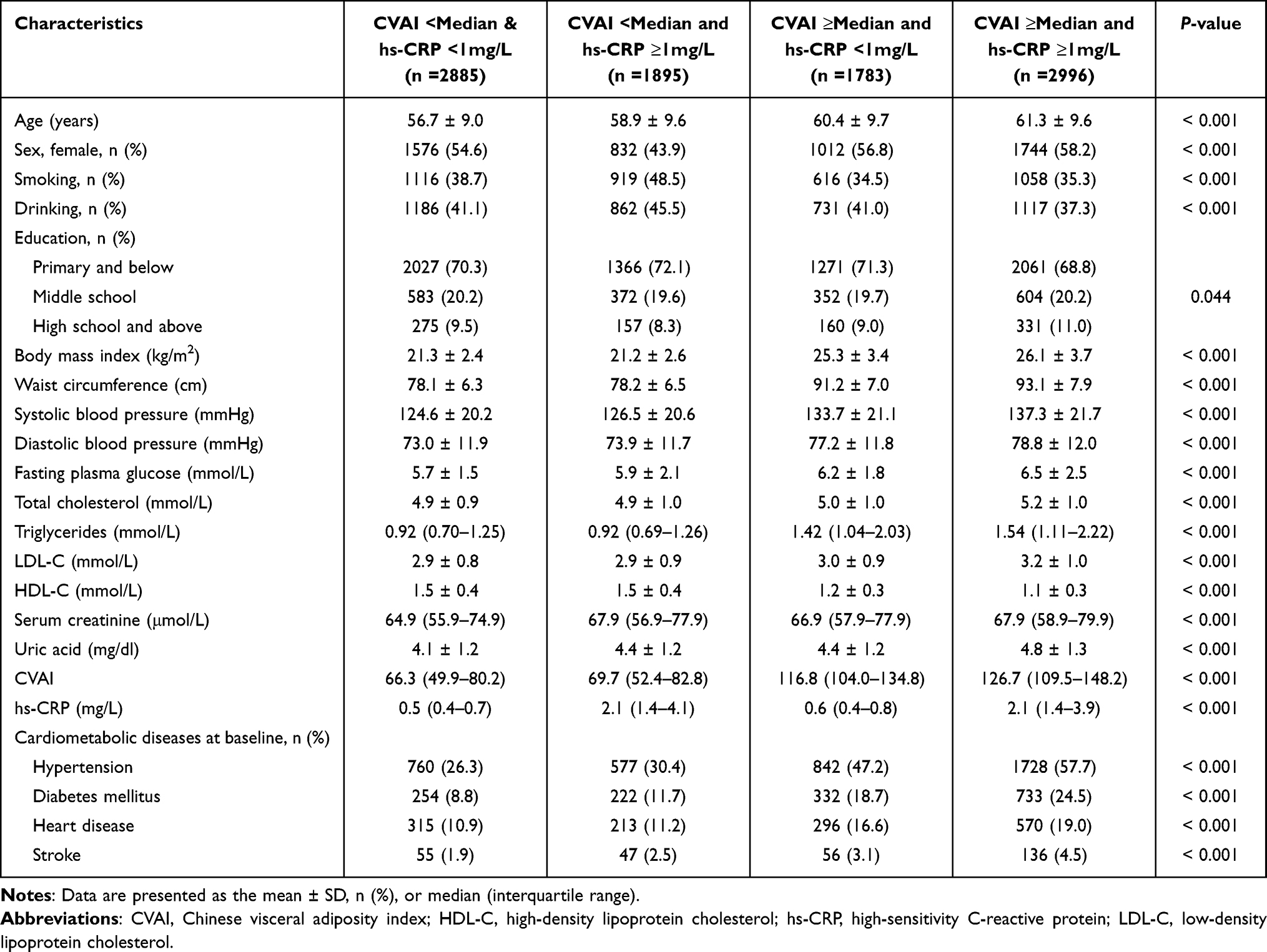 |
Table 1 Baseline Characteristics of the Study Population |
Joint Effects of Visceral Fat and Inflammation on Cardiometabolic Diseases (Cross-Sectional Analyses)
CVAI was independently associated with all of the four cardiometabolic diseases in both dichotomous and continuous variables (Table S1). The fully adjusted model, which considered demographic factors, biochemical indicators and health status, showed that those with higher CVAI (compared with CVAI <median) had more than double the odds for diabetes, and increases of 81% for hypertension, 35% for heart diseases, and 32% for stroke (Table S1, model 3). Similarly, hs-CRP was independently associated with hypertension and diabetes, and was marginally associated with stroke (P =0.079, Table S2). In addition, the association between hs-CRP and heart disease was attenuated after further considering for the combination of other diseases (Table S2, model 3). We further evaluated the association between CVAI and cardiometabolic diseases in different CRP strata (Table S3). Consistent results were observed for hypertension, diabetes and heart disease regardless of CRP level, whereas increase of CVAI-associated stroke odds were found only in those with higher hs-CRP.
The prevalence of each disease across groups defined by CVAI combined with hs-CRP are shown in Figure S1. As expected, those with high CVAI and high hs-CRP had highest prevalences for all cardiometabolic diseases. Compared with group 1 (low CVAI and low hs-CRP), the crude odds for individuals with high CVAI and high hs-CRP (group 4) were more than 3-fold for hypertension and diabetes, more than 2-fold for stroke, and nearly 2-fold for heart disease (Table 2). After adjustment for age, sex, smoking and drinking status, educational level, BP, FPG, TC, LDL-C, Scr, UA and disease status, group 4 carried highest odds for prevalent cardiometabolic diseases. The ORs of group 4 were 2.06 (95% CI: 1.74–2.43) for hypertension, 2.88 (95% CI: 2.45–3.40) for diabetes, 1.37 (95% CI: 1.16–1.61) for heart disease, and 1.51 (95% CI: 1.07–2.13) for stroke.
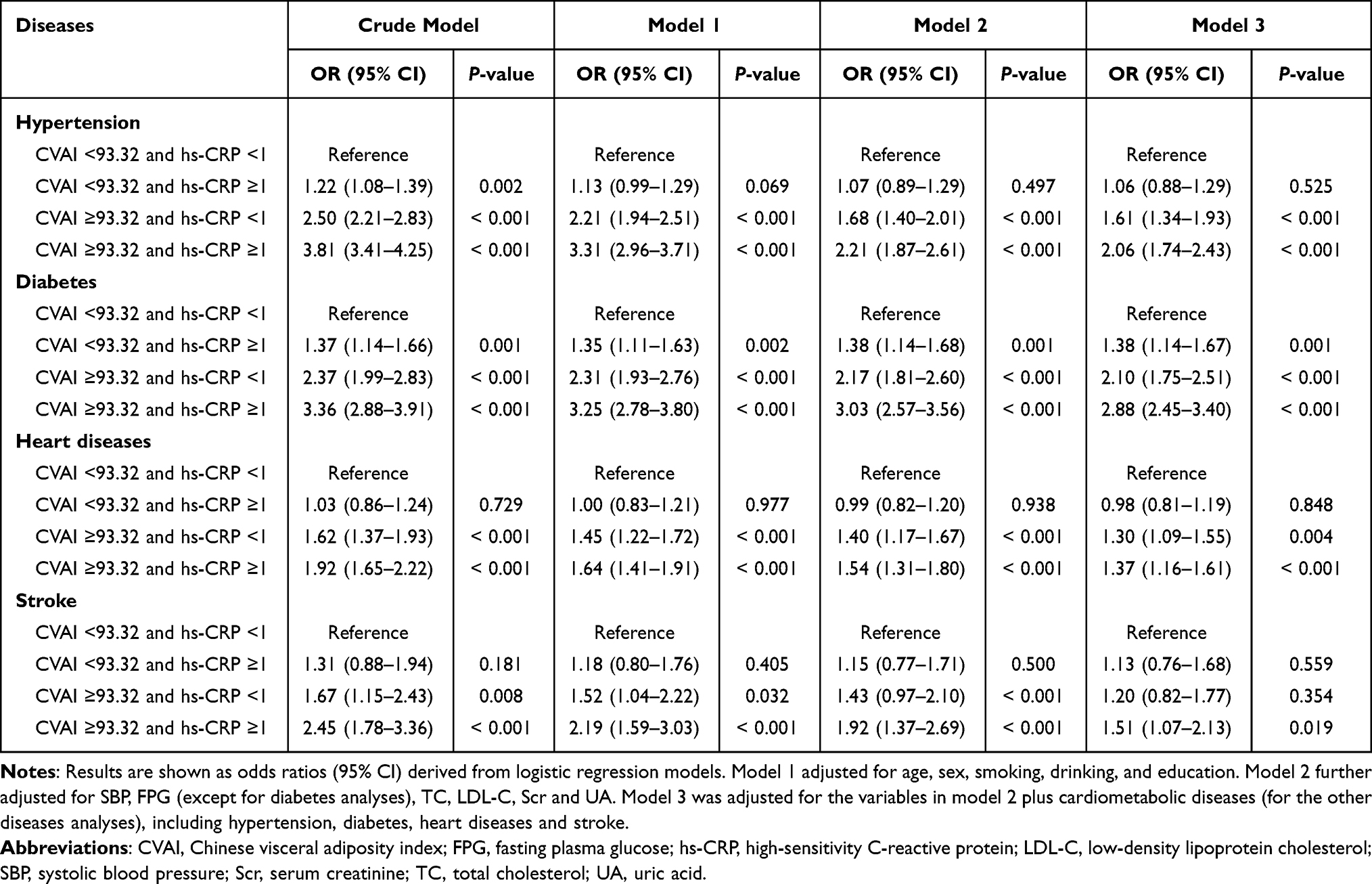 |
Table 2 Joint Effect of CVAI and Hs-CRP on Cardiometabolic Diseases (Cross-Sectional Association) |
Joint Effects of Visceral Fat and Inflammation on the Risk of Cardiometabolic Disease (Longitudinal Analyses)
Details of data sets for longitudinal analyses are shown in Table S4. The follow-up period was 9 years. Consistent with results in cross-sectional analyses, CVAI was independently associated with all of the four cardiometabolic diseases, in both its dichotomous and continuous forms (Table S5). After considering all potential confounders, each SD increase in CVAI corresponded to an increased risk of 25% increased risk for hypertension, 39% for diabetes, 20% for heart diseases, and 26% for stroke (all P <0.001). Similarly, hs-CRP was associated to varying degrees with the risk of cardiometabolic diseases, except for hypertension risk, which was significant only in the demographic-adjusted model (Table S6). The significant association between CVAI and risk of cardiometabolic disease was observed in both the low and high CRP strata (Table S7). It is noteworthy that the association appears to be stronger in those with high hs-CRP levels.
Among the four groups, the highest person-year incidences of the four diseases were observed in those with concurrently high CVAI and hs-CRP (Figure 2). Findings in the joint effects of CVAI and CRP on cardiometabolic diseases from the cross-sectional analyses were confirmed in the longitudinal analyses, in which the highest risks of disease were observed for individuals with high CVAI and CRP levels (Table 3). Crude Cox regression analyses showed that the HRs for the diseases for those in group 4 ranged from 1.72 to 2.83 (all P <0.001). After adjusting for demographic factors and biochemical indicators (Table 3, model 2), individuals with high CVAI and CRP were associated with more than a 2-fold increased risk of diabetes and stroke, and 47% increased risk of hypertension and heart diseases. Further consideration of the patient disease history did not substantially change the results (Table 3, model 3).
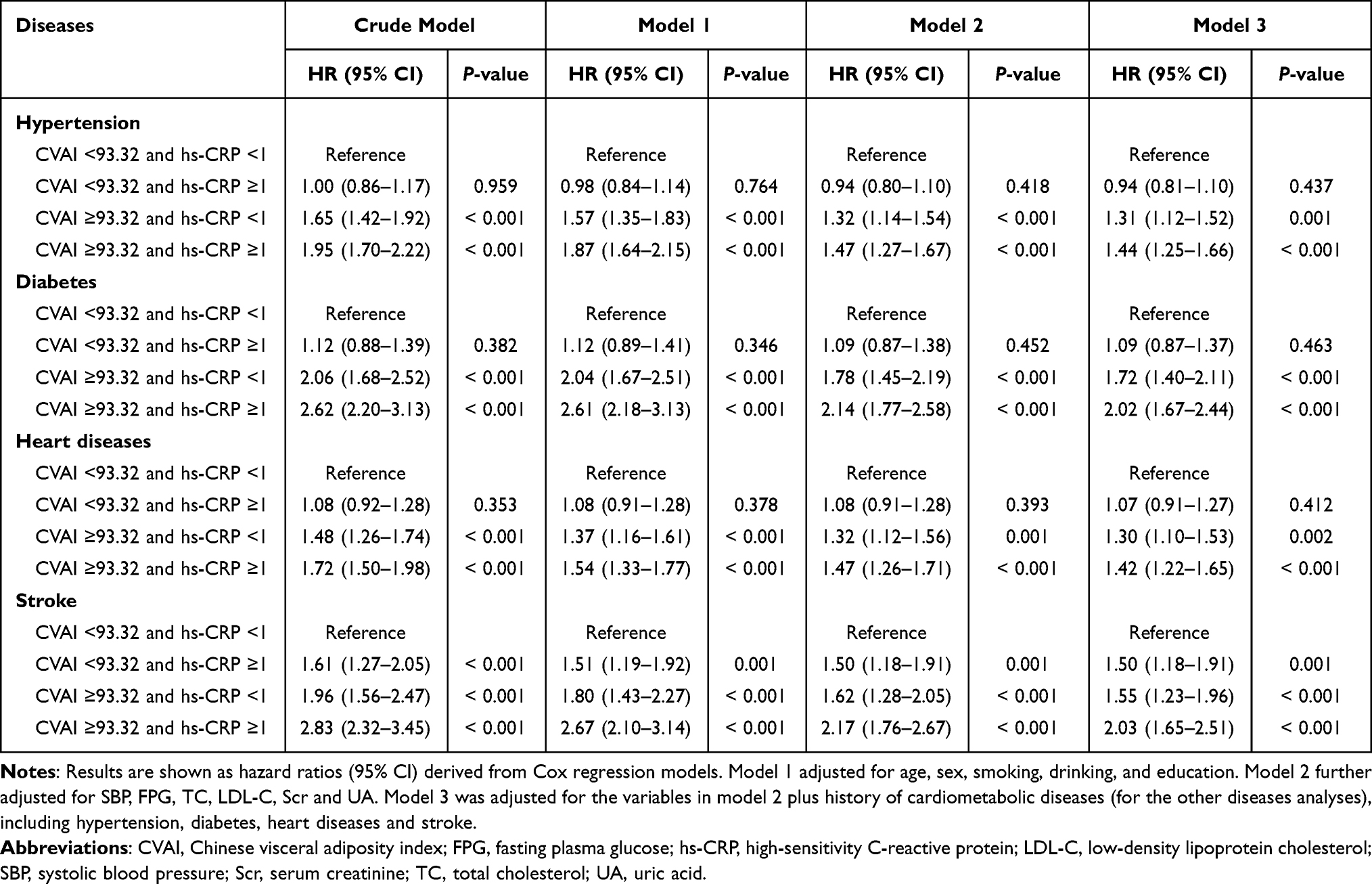 |
Table 3 Joint Effect of CVAI and Hs-CRP on the Risk of Cardiometabolic Diseases (Longitudinal Association) |
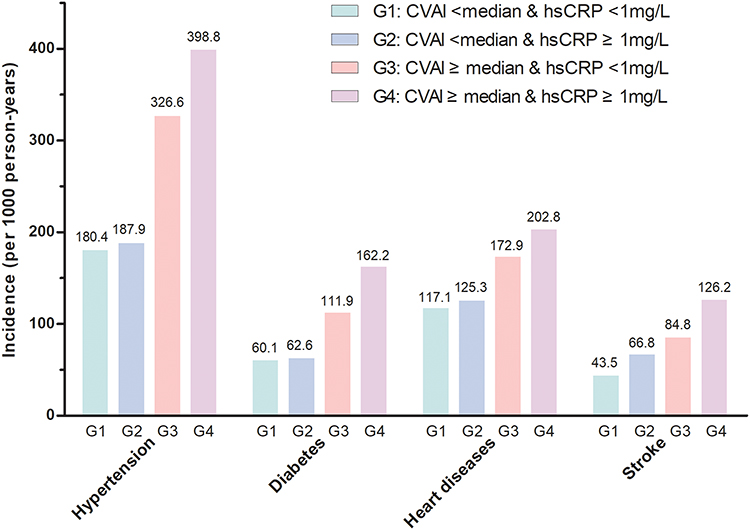 |
Figure 2 Incidence rates of chronic diseases across groups. Abbreviations: CVAI, Chinese visceral adiposity index; hs-CRP, high-sensitivity C-reactive protein. |
Sensitivity analyses by re-defined co-exposure stratified by hs-CRP thresholds (1 and 3 mg/L), and excluding those with endpoints occurring within the first follow-up visit, those with kidney disease at baseline, and those with hs-CRP ≥10 mg/L, confirmed the robustness of the main results (Table S8 to S11). Consistently, individuals with concurrently high CVAI and CRP had the highest risk for developed cardiometabolic diseases in all sensitivity analyses. Subgroup analyses by age, sex, obesity (general obesity defined by BMI and abdominal obesity defined by WC), and smoking and drinking status roughly confirmed the consistency of the results, with slight heterogeneity found in some subgroups (Table S12 to S17). The effects of co-exposure were found to be stronger on the risk of heart diseases and stroke in those <60 years old, men, those with BMI ≥24 kg/m2, and ever/current smokers or drinkers (P for interaction <0.1). It was stronger on hypertension risk in those with BMI <24 kg/m2 and in never drinkers (P for interaction <0.1), and stronger on diabetes risk in those with abdominal obesity, and on stroke risk in the aged (P for interaction <0.1).
Temporal Relationship Between Visceral Fat and Inflammation
The model design and results of the temporal analysis of CVAI and hs-CRP are displayed in Figure 3. A unidirectional temporal relationship between CVAI and hs-CRP was observed. In the fully adjusted model, the standardized correlation coefficient for T1_CVAI to T2_hs-CRP was 0.130 (P <0.001), indicating that for per standard deviation increase in CVAI at baseline, there is an average increase of 0.13 standard deviation in hs-CRP levels at the follow-up assessment. We then re-defined the exposure used baseline CVAI and follow-up hs-CRP, and further evaluated the joint effects on CMD risk (Table S18). Similarly, individuals with high baseline CVAI and follow-up hs-CRP carried the highest risk for cardiometabolic disease, with HRs of 1.77 for hypertension risk, 2.31 for diabetes risk, 1.38 for heart disease risk, and 1.72 for stroke risk. It is noteworthy that, in a low level of follow-up CRP, the hypertension risk for individuals with high CVAI was comparable to those with low CVAI.
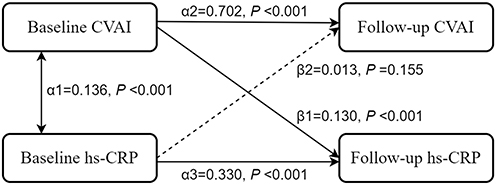 |
Figure 3 Cross-lagged path analysis for CVAI and hs-CRP. The cross-lagged model was adjusted for age, sex, smoking status, drinking status, education, SBP, FPG, TC, LDL-C, Scr, UA, history of hypertension, diabetes, heart disease, and stroke. Abbreviations: CVAI, Chinese visceral adiposity index; FPG, fasting plasma glucose; hs-CRP, high-sensitivity C-reactive protein; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; Scr, serum creatinine; TC, total cholesterol; UA, uric acid. |
Multiplicative and Additive Interaction of Visceral Fat and Inflammation on Cardiometabolic Diseases
No significant multiplicative interaction was found. We additionally evaluated the biological interaction by assessing additive interactions (Table 4). There were significant additive interactions between visceral fat and inflammation on hypertension (RERI: 1.09, 95% CI: 0.71–1.47; AP: 0.28, 95% CI: 0.20–0.37). After considering all potential confounders, the additive interactions were attenuated but remained significant, with 19% attributable to the joint effect of their interaction. Similar interaction was observed in diabetes. In the fully adjusted model, the attributable proportion of the joint effect was 14% for the interaction between CVAI and hs-CRP. There were no addictive interactions were found for heart disease and stroke. The results were confirmed in longitudinal analyses (Table S19).
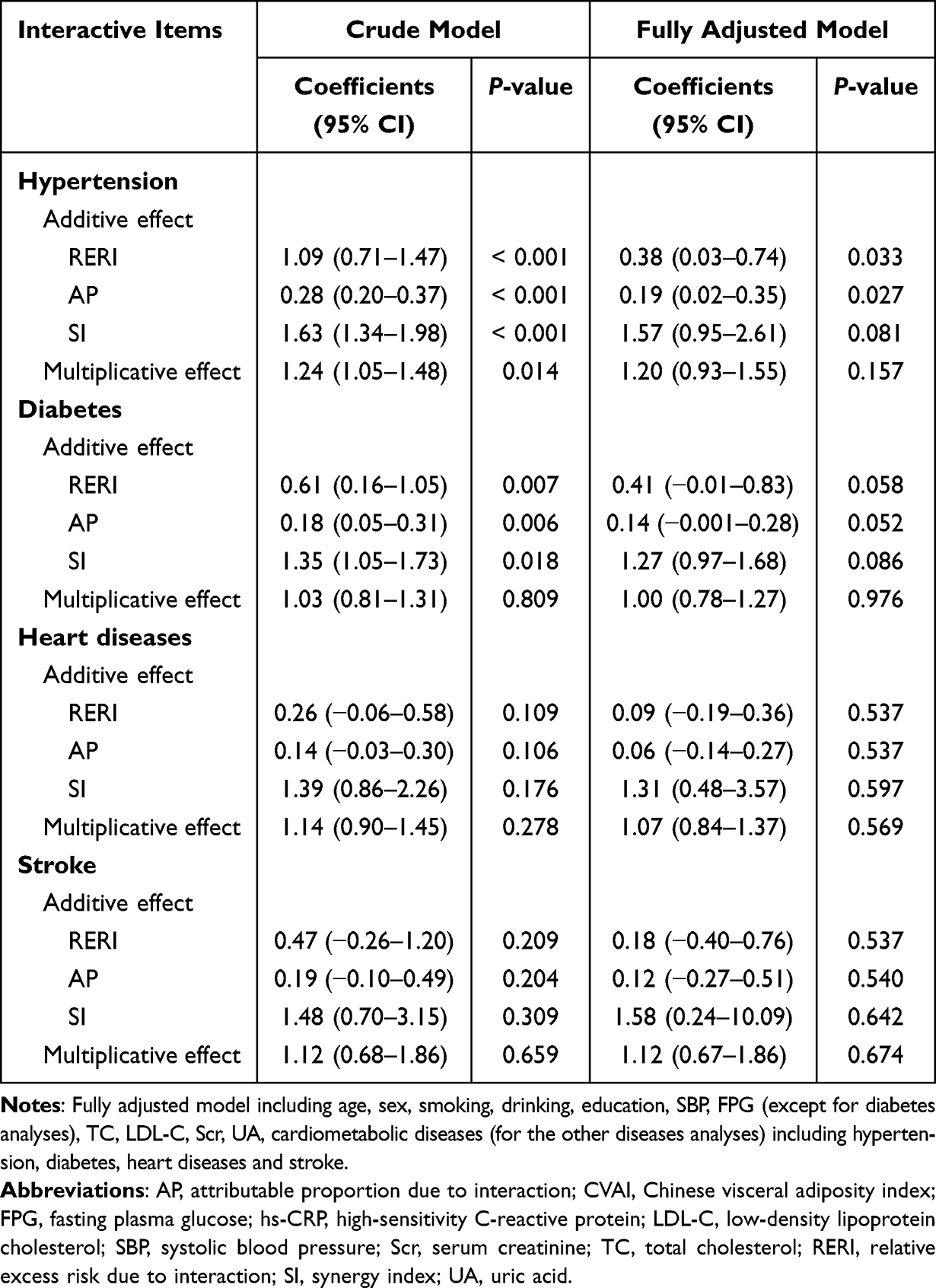 |
Table 4 Interactive Effects of CVAI and Hs-CRP on Cardiometabolic Diseases |
Discussion
The present study, based on a nationally representative population, involving 9559 participants followed up for 9 years, comprehensively evaluated the individual and joint effects, statistical and biological interactions, and temporal relationship of visceral fat and inflammation on CMD risk. Moreover, a series of sensitivity and subgroup analyses were conducted to confirm the consistency and stability of the principal results. Primarily, visceral fat and inflammation are individually and jointly associated with CMD risk, and individuals with both high visceral fat accumulation and elevated inflammation have the highest risk of developing hypertension, diabetes, heart diseases, and stroke, independent of a cluster of potential confounders, including age, sex, smoking and drinking status, educational level, SBP, FPG, TC, LDL-C, Scr, UA, and disease situation. Among them, a significant biological interaction between CVAI and hs-CRP was observed, with the attributable proportion due to interaction being 19% for hypertension and 14% for diabetes. There was a unidirectional temporal relationship from baseline CVAI to follow-up hs-CRP. Sensitivity and subgroup analyses roughly confirmed the main results. These findings suggest that the combined assessment of both visceral fat and inflammation may improve risk stratification and primary prevention of cardiometabolic diseases.
Obesity and inflammation are two well-known independent risk factors of CMD. Visceral adiposity has been demonstrated to be the most damaging to target organs compared to other phenotypes of obesity.34,35 Among several common indicators, CVAI is the optimal for predicting diabetes in non-general obese patients, and for predicting renal damage in patients with hypertension and diabetes,7,36 and it is also associated with other cardiovascular and metabolic factors.37–39 Most of the previous studies mainly focused on the association of CVAI with diabetes. The present study yielded similar results, which confirmed the findings and extended the association to the common CMD. We found higher CVAI is independently associated with increased risk of hypertension, diabetes, heart disease, and stroke. Elevated inflammation is similarly associated with increased risk of diabetes, heart disease and stroke, which is consistent with previous studies.40–42 However, the association between hs-CRP and hypertension risk disappeared after adjusting for confounders. This finding is supported by several previous studies.43,44 Inflammation is generally considered a secondary change involving hypertension-related factors, such as obesity, dyslipidemia and abnormal glucose metabolism. The impact of these factors on hypertension may far exceed the influence of the inflammatory response, which could partly explain the results. In addition, differences among populations and study design may also lead to varying observations.45,46
Based on the nationally representative cohort, our study provides epidemiological evidence on the combined effects between visceral fat and inflammation on CMD risk. Although there was a slight difference in the individual effect of hs-CRP on diseases, consistent results were observed for the joint effects of CVAI and hs-CRP on the risk of the four CMDs, which has rarely been focused in previous studies. A recent study reported that adiposity, measured by BMI, WC, and fatty liver, has a joint effect with inflammation on diabetes, with 11.5% to 15.7% attributable to their interaction.47 The present study found that visceral fat accumulation, as measured by CVAI, increases diabetes risk by interacting biologically with elevated hs-CRP, with the attributable proportion due to interaction being 14%. Moreover, for the first time, a significant interaction between the two was observed on hypertension risk, with 19% of the effects attributable to the interaction. Additionally, it is noteworthy that the highest risk for heart diseases and stroke is also observed in individuals with both high CVAI and CRP levels, although not statistically significant in interaction. These findings expand the understanding of the links between adiposity, inflammation, and CMD, providing insight into the mechanisms of related diseases. In clinical practice, more attention is paid to the role of a single factor in the occurrence and development of diseases, while the combined effect of multiple factors is ignoring, which may contribute to the unsatisfactory prevention and control rates of CMD. A comprehensive analysis of the combined effects of potentially related factors and their biological interactions may fill this gap. According to our findings, approaches that simultaneously target adiposity and inflammation should yield greater benefits than targeting each individual risk factor. Moreover, future studies focus on the incremental utility of CVAI and hs-CRP in risk prediction models would be valuable.
Although adiposity concomitant with elevated inflammation has long been observed,48,49 the temporal relationship between visceral fat accumulation and inflammation remains to be explored. Recently, a bidirectional relationship between CRP and atherogenic index of plasma (AIP) was reported, with an interesting negative association for baseline AIP to future CRP.24 Liu et al reported in temporal analyses that inflammation had a greater impact on metabolic disorders than vice versa.50 Our study shows a unidirectional temporal relationship between CVAI and hs-CRP, where the accumulation of visceral fat occurs before the elevation in inflammation, which seems to suggest a potential mediating effect of CRP. However, the significant association between CVAI and disease risk persisted even in individuals with low CRP level, which may imply the presence of alternative pathways. It is noteworthy that, in a recent study regarding dementia, the effect of adiposity was mainly driven directly by factors associated with body fat distribution, with no evidence of mediation through inflammation.51 Studies have shown that inflammation can affect lipid metabolism.52 However, there is insufficient evidence demonstrating an effect of inflammation on visceral fat accumulation. A recent experimental study reported that macrophages are involve in the process of adipose tissue biology by regulating adipocyte stem cell differentiation via the TGFβ1 signaling pathway.53 Adipose tissue macrophage-derived miR-690, an anti-inflammatory molecule, modulates adipocyte precursor cell maintenance and adipogenesis.54 The lipid overload leads to endoplasmic reticulum stress, increased expression of the inflammation regulator NF-κB and the production of inflammation-inducing signals such as IL-6.55,56 Other molecules/signaling pathways, including extracellular signal-regulated kinase, TNF-α and inositol-requiring protein 1, are also involving into this complex process.57,58 In brief, the accumulation of visceral fat directly or indirectly leads to inflammation, and the effects of both are superimposed, ultimately contributing to the increased risk of CMD. Drugs that target inflammation have been shown to be potentially effective in improving glucose metabolism and reducing cardiovascular events.59–61 Colchicine has been shown to reduce cardiovascular events in patients with established coronary artery disease.62,63 Similarly, canakinumab, a monoclonal antibody targeting interleukin-1β, has demonstrated efficacy in reducing cardiovascular risk in secondary prevention.61,64 Anti-inflammatory treatments may reduce CMD risk by reducing the damage of visceral fat. Clinical trials targeting inflammatory pathways for its treatment are warranted.
This study has several strengths. First, the study is based on a nationally representative cohort conducted by an excellent research team with well-established design, ensuring data quality and reliability. Second, the longitudinal design and analysis for temporal relationships provide evidence supporting the causal hypothesis. The consistency and stability of the main results were confirmed by a series of sensitivity and subgroup analyses. Third, comprehensive insight for understanding the association and potential mechanisms between visceral fat, inflammation and CMD was obtained by cross-sectional and longitudinal analyses, temporal relationships, and statistical and biological interactions analyses. There are also certain limitations that should be discussed. Firstly, given the number of groups and sample size, we used a CRP cutoff of 1 mg/L in the primary analyses, which is different from the cutoffs (2 or 3 mg/L) used in some previous studies. The lower value may have attenuated the effect of inflammation, although significant results were observed in most analyses. Nonetheless, sensitivity analysis using 1 or 3 as the threshold for CRP yielded similar results. Notably, the present study suggests that even a low-grade inflammation could increase CMD risk by interacting with CVAI. Secondly, a post hoc power calculation indicated moderate power (approximately 60–68%) to detect the observed interaction at α=0.1, which is a common challenge in observational studies due to the high sample size requirements for interaction tests. Thirdly, the status of visceral fat accumulation was defined by median CVAI (93.32), which was not entirely consistent with previous studies. Future researches with specialized design are needed for assessing the diagnostic threshold of CVAI for visceral adiposity. Fourthly, the lack of details on subtypes of heart diseases and stroke limited further evaluation. Fifthly, our findings require verification in populations from other regions or ethnic backgrounds, as well as in younger individuals. Additionally, residual confounding from unmeasured factors, such as cultural and dietary patterns, cannot be ruled out, which may have influenced the estimation of effect sizes.
In conclusion, this study provides comprehensive insight for understanding the association between visceral fat and inflammation and their effects on CMD risk, involving individual and joint effects, statistical and biological interactions, and the temporal relationship between the two factors. Elevations in both visceral fat and inflammation have joint effects, that increased the risk of hypertension, diabetes, heart disease, and stroke, in a manner greater than the sum of the two separate effects. Dual assessment of both visceral fat and inflammation is important for the primary prevention and management of cardiometabolic diseases. Specifically, early monitoring of CRP levels is recommended for individuals with high CVAI. Furthermore, future randomized controlled trials are warranted to evaluate the efficacy of anti-inflammatory therapies in reducing CMD risk for in this high-risk population.
Data Sharing Statement
Data of the China Health and Retirement Longitudinal Study are available at its website (http://charls.pku.edu.cn/). Other materials are available from the corresponding author (Yequn Chen and Xuerui Tan) upon reasonable request.
Ethics Approval and Consent to Participate
The CHARLS project received approval from the institutional review board of Peking University, and all participants provided written informed consent. The present study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee at the First Affiliated Hospital of Shantou University Medical College.
Acknowledgments
The China Health and Retirement Longitudinal Study was developed by a team of researchers from Peking University. We sincerely thank who participated in the data collection and management.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Key Disciplinary Project of Clinical Medicine under the High-level University Development Program, Guangdong, China (2020); National Natural Science Foundation of China (No. 82073659); Guangdong Province Science and Technology Special Fund (2022-124-6); Guangdong Provincial Innovation Team (2024KCXTD019).
Disclosure
The authors declare that they have no competing interests.
References
1. O’Sullivan JW, Ashley EA, Elliott PM. Polygenic risk scores for the prediction of cardiometabolic disease. Eur Heart J. 2023;44(2):89–99. doi:10.1093/eurheartj/ehac648
2. Valenzuela PL, Carrera-Bastos P, Castillo-García A, Lieberman DE, Santos-Lozano A, Lucia A. Obesity and the risk of cardiometabolic diseases. Nat Rev Cardiol. 2023;20(7):475–494. doi:10.1038/s41569-023-00847-5
3. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990-2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
4. The Writing Committee Of The Report On Cardiovascular Health And Diseases in China, and Hu S.-S. Report on cardiovascular health and diseases in china 2021: an updated summary. J Geriatr Cardiol. 2023;20(6):399–430. doi:10.26599/1671-5411.2023.06.001
5. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ. 2020;369:m997. doi:10.1136/bmj.m997
6. Naghavi M, Libby P, Falk E, et al. From vulnerable plaque to vulnerable patient: a call for new definitions and risk assessment strategies: part II. Circulation. 2003;108(15):1772–1778. doi:10.1161/01.CIR.0000087481.55887.C9
7. Lin M, Xie Y, Hong L, et al. Abnormal adiposity indices are associated with an increased risk of diabetes in a non-obese Asian population. Public Health. 2024;226:144–151. doi:10.1016/j.puhe.2023.11.012
8. Koenen M, Hill MA, Cohen P, Sowers JR. Obesity, adipose tissue and vascular dysfunction. Circ Res. 2021;128(7):951–968. doi:10.1161/CIRCRESAHA.121.318093
9. Rolver MG, Emanuelsson F, Nordestgaard BG, Benn M. Contributions of elevated CRP, hyperglycaemia, and type 2 diabetes to cardiovascular risk in the general population: observational and Mendelian randomization studies. Cardiovasc Diabetol. 2024;23(1):165. doi:10.1186/s12933-024-02207-0
10. Bi H, Zhang Y, Qin P, et al. Association of Chinese visceral adiposity index and its dynamic change with risk of carotid plaque in a large cohort in China. J Am Heart Assoc. 2022;11(1):e022633. doi:10.1161/JAHA.121.022633
11. Lin M, Wu S, Deng X, Chen Y, Tan X. Visceral fat and its dynamic change are associated with renal damage: evidence from two cohorts. Clin Exp Hypertens. 2023;45(1):2271187. doi:10.1080/10641963.2023.2271187
12. Li B, Wang J, Zhou X, et al. Chinese visceral adiposity index is more closely associated with hypertension and prehypertension than traditional adiposity indices in chinese population: results from the REACTION study. Front Endocrinol. 2022;13:921997. doi:10.3389/fendo.2022.921997
13. Niu ZJ, Cui Y, Wei T, et al. The effect of insulin resistance in the association between obesity and hypertension incidence among Chinese middle-aged and older adults: data from China health and retirement longitudinal study (CHARLS). Front Public Health. 2024;12:1320918. doi:10.3389/fpubh.2024.1320918
14. Wen S, Huang X, Huang Z, et al. The association of changes in the Chinese visceral adiposity index and cardiometabolic diseases: a cohort study. Diabetol Metab Syndr. 2024;16(1):228. doi:10.1186/s13098-024-01460-3
15. Ye X, Zhang G, Han C, Wang P, Lu J, Zhang M. The association between Chinese visceral adiposity index and cardiometabolic multimorbidity among Chinese middle-aged and older adults: a national cohort study. Front Endocrinol. 2024;15:1381949. doi:10.3389/fendo.2024.1381949
16. Awan Z, Genest J. Inflammation modulation and cardiovascular disease prevention. Eur J Prev Cardiol. 2015;22(6):719–733. doi:10.1177/2047487314529350
17. Esser N, Legrand-Poels S, Piette J, Scheen AJ, Paquot N. Inflammation as a link between obesity, metabolic syndrome and type 2 diabetes. Diabet Res Clin Pract. 2014;105(2):141–150. doi:10.1016/j.diabres.2014.04.006
18. Kolb H. Obese visceral fat tissue inflammation: from protective to detrimental? BMC Med. 2022;20(1):494. doi:10.1186/s12916-022-02672-y
19. Tchernof A, Després JP. Pathophysiology of human visceral obesity: an update. Physiol Rev. 2013;93(1):359–404. doi:10.1152/physrev.00033.2011
20. Desikan RS, Schork AJ, Wang Y, et al. Polygenic overlap between C-reactive protein, plasma lipids, and alzheimer disease. Circulation. 2015;131(23):2061–2069. doi:10.1161/CIRCULATIONAHA.115.015489
21. Lawler PR, Bhatt DL, Godoy LC, et al. Targeting cardiovascular inflammation: next steps in clinical translation. Eur Heart J. 2021;42(1):113–131. doi:10.1093/eurheartj/ehaa099
22. Eltoft A, Arntzen KA, Wilsgaard T, Hansen JB, Mathiesen EB, Johnsen SH. Joint effect of carotid plaque and c-reactive protein on first-ever ischemic stroke and myocardial infarction? J Am Heart Assoc. 2018;7(11). doi:10.1161/JAHA.118.008951
23. Yan Y, Liu Y, Li S, et al. Temporal relationship between inflammation and insulin resistance and their joint effect on hyperglycemia: the Bogalusa heart study. Cardiovasc Diabetol. 2019;18(1):109. doi:10.1186/s12933-019-0913-2
24. Lan Y, Chen G, Wu D, et al. Temporal relationship between atherogenic dyslipidemia and inflammation and their joint cumulative effect on type 2 diabetes onset: a longitudinal cohort study. BMC Med. 2023;21(1):31. doi:10.1186/s12916-023-02729-6
25. Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol. 2014;43(1):61–68. doi:10.1093/ije/dys203
26. Chen X, Crimmins E, Hu PP, et al. Venous blood-based biomarkers in the China health and retirement longitudinal study: rationale, design, and results from the 2015 wave. Am J Epidemiol. 2019;188(11):1871–1877. doi:10.1093/aje/kwz170
27. Xia MF, Chen Y, Lin HD, et al. A indicator of visceral adipose dysfunction to evaluate metabolic health in adult Chinese. Sci Rep. 2016;6:38214. doi:10.1038/srep38214
28. Ridker PM. A test in context: high-sensitivity C-reactive protein. J Am Coll Cardiol. 2016;67(6):712–723. doi:10.1016/j.jacc.2015.11.037
29. DeGoma EM, French B, Dunbar RL, Allison MA, Mohler ER 3rd, Budoff MJ. Intraindividual variability of C-reactive protein: the multi-ethnic study of atherosclerosis. Atherosclerosis. 2012;224(1):274–279. doi:10.1016/j.atherosclerosis.2012.07.017
30. Kivimäki M, Feldt T, Vahtera J, Nurmi JE. Sense of coherence and health: evidence from two cross-lagged longitudinal samples. Soc Sci Med. 2000;50(4):583–597. doi:10.1016/S0277-9536(99)00326-3
31. Knol MJ, VanderWeele TJ. Recommendations for presenting analyses of effect modification and interaction. Int J Epidemiol. 2012;41(2):514–520. doi:10.1093/ije/dyr218
32. Andersson T, Alfredsson L, Källberg H, Zdravkovic S, Ahlbom A. Calculating measures of biological interaction. Eur J Epidemiol. 2005;20(7):575–579. doi:10.1007/s10654-005-7835-x
33. Källberg H, Ahlbom A, Alfredsson L. Calculating measures of biological interaction using R. Eur J Epidemiol. 2006;21(8):571–573. doi:10.1007/s10654-006-9037-6
34. Piché ME, Tchernof A, Després JP. Obesity phenotypes, diabetes, and cardiovascular diseases. Circ Res. 2020;126(11):1477–1500. doi:10.1161/CIRCRESAHA.120.316101
35. Neeland IJ, Ross R, Després JP, et al. Visceral and ectopic fat, atherosclerosis, and cardiometabolic disease: a position statement. Lancet Diabetes Endocrinol. 2019;7(9):715–725. doi:10.1016/S2213-8587(19)30084-1
36. Lin M, Li N, Heizhati M, et al. Chinese visceral adiposity index is associated with incident renal damage in patients with hypertension and abnormal glucose metabolism: a longitudinal study. Front Endocrinol. 2022;13:910329. doi:10.3389/fendo.2022.910329
37. Zhang Z, Zhao L, Lu Y, Meng X, Zhou X. Association between Chinese visceral adiposity index and risk of stroke incidence in middle-aged and elderly Chinese population: evidence from a large national cohort study. J Transl Med. 2023;21(1):518. doi:10.1186/s12967-023-04309-x
38. Wan H, Wang Y, Xiang Q, et al. Associations between abdominal obesity indices and diabetic complications: chinese visceral adiposity index and neck circumference. Cardiovasc Diabetol. 2020;19(1):118. doi:10.1186/s12933-020-01095-4
39. Wu Z, Yu S, Kang X, et al. Association of visceral adiposity index with incident nephropathy and retinopathy: a cohort study in the diabetic population. Cardiovasc Diabetol. 2022;21(1):32. doi:10.1186/s12933-022-01464-1
40. Yang X, Tao S, Peng J, et al. High-sensitivity C-reactive protein and risk of type 2 diabetes: a nationwide cohort study and updated meta-analysis. Diabetes Metab Res Rev. 2021;37(8):e3446. doi:10.1002/dmrr.3446
41. Kitagawa K, Hosomi N, Nagai Y, et al. Cumulative effects of LDL cholesterol and CRP levels on recurrent stroke and TIA. J Atheroscler Thromb. 2019;26(5):432–441. doi:10.5551/jat.45989
42. Zhou Y, Han W, Gong D, Man C, Fan Y. Hs-CRP in stroke: a meta-analysis. Clin Chim Acta. 2016;453:21–27. doi:10.1016/j.cca.2015.11.027
43. Bisaria S, Terrigno V, Hunter K, Roy S. Association of elevated levels of inflammatory marker high-sensitivity C-reactive protein and hypertension. J Prim Care Community Health. 2020;11:2150132720984426. doi:10.1177/2150132720984426
44. Ebong IA, Schreiner P, Lewis CE, Appiah D, Ghelani A, Wellons M. The association between high-sensitivity C-reactive protein and hypertension in women of the CARDIA study. Menopause. 2016;23(6):662–668. doi:10.1097/GME.0000000000000609
45. Lakoski SG, Herrington DM, Siscovick DM, Hulley SB. C-reactive protein concentration and incident hypertension in young adults: the CARDIA study. Arch Intern Med. 2006;166(3):345–349. doi:10.1001/archinte.166.3.345
46. Jae SY, Kurl S, Laukkanen JA, et al. Relation of C-reactive protein, fibrinogen, and cardiorespiratory fitness to risk of systemic hypertension in men. Am J Cardiol. 2015;115(12):1714–1719. doi:10.1016/j.amjcard.2015.03.016
47. Wu D, Lan Y, Chen S, et al. Combined effect of adiposity and elevated inflammation on incident type 2 diabetes: a prospective cohort study. Cardiovasc Diabetol. 2023;22(1):351. doi:10.1186/s12933-023-02067-0
48. Fernández-Sánchez A, Madrigal-Santillán E, Bautista M, et al. Inflammation, oxidative stress, and obesity. Int J Mol Sci. 2011;12(5):3117–3132. doi:10.3390/ijms12053117
49. Kawai T, Autieri MV, Scalia R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am J Physiol Cell Physiol. 2021;320(3):C375–c391. doi:10.1152/ajpcell.00379.2020
50. Liu C, Liu T, Zhang Q, et al. Temporal relationship between inflammation and metabolic disorders and their impact on cancer risk. J Glob Health. 2024;14:04041. doi:10.7189/jogh.14.04041
51. Karlsson IK, Zhan Y, Wang Y, et al. Adiposity and the risk of dementia: mediating effects from inflammation and lipid levels. Eur J Epidemiol. 2022;37(12):1261–1271. doi:10.1007/s10654-022-00918-w
52. McGillicuddy FC, de la Llera Moya M, Hinkle CC, et al. Inflammation impairs reverse cholesterol transport in vivo. Circulation. 2009;119(8):1135–1145. doi:10.1161/CIRCULATIONAHA.108.810721
53. Yu X, Hu Y, Lim HY, et al. Septal LYVE1(+) macrophages control adipocyte stem cell adipogenic potential. Science. 2025;389(6763):eadg1128. doi:10.1126/science.adg1128
54. Cunha ERK, Tan B, Kempf J, et al. Adipose tissue macrophage-derived miR-690 modulates adipocyte precursor cell maintenance and adipogenesis. Mol Metab;2025. 102246. doi:10.1016/j.molmet.2025.102246
55. Stenkula KG, Erlanson-Albertsson C. Adipose cell size: importance in health and disease. Am J Physiol Regul Integr Comp Physiol. 2018;315(2):R284–r295. doi:10.1152/ajpregu.00257.2017
56. Lemmer IL, Willemsen N, Hilal N, Bartelt A. A guide to understanding endoplasmic reticulum stress in metabolic disorders. Mol Metab. 2021;47:101169. doi:10.1016/j.molmet.2021.101169
57. Hong S, Song W, Zushin PH, et al. Phosphorylation of Beta-3 adrenergic receptor at serine 247 by ERK MAP kinase drives lipolysis in obese adipocytes. Mol Metab. 2018;12:25–38. doi:10.1016/j.molmet.2018.03.012
58. Foley KP, Chen Y, Barra NG, et al. Inflammation promotes adipocyte lipolysis via IRE1 kinase. J Biol Chem. 2021;296:100440. doi:10.1016/j.jbc.2021.100440
59. Rissanen A, Howard CP, Botha J, Thuren T. Effect of anti-IL-1β antibody (canakinumab) on insulin secretion rates in impaired glucose tolerance or type 2 diabetes: results of a randomized, placebo-controlled trial. Diabetes Obes Metab. 2012;14(12):1088–1096. doi:10.1111/j.1463-1326.2012.01637.x
60. Ridker PM, Howard CP, Walter V, et al. Effects of interleukin-1β inhibition with canakinumab on hemoglobin A1c, lipids, C-reactive protein, interleukin-6, and fibrinogen: a phase IIb randomized, placebo-controlled trial. Circulation. 2012;126(23):2739–2748. doi:10.1161/CIRCULATIONAHA.112.122556
61. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. N Engl J Med. 2017;377(12):1119–1131. doi:10.1056/NEJMoa1707914
62. Nidorf SM, Fiolet ATL, Mosterd A, et al. Colchicine in patients with chronic coronary disease. N Engl J Med. 2020;383(19):1838–1847. doi:10.1056/NEJMoa2021372
63. Tardif JC, Kouz S, Waters DD, et al. Efficacy and safety of low-dose colchicine after myocardial infarction. N Engl J Med. 2019;381(26):2497–2505. doi:10.1056/NEJMoa1912388
64. Everett BM, MacFadyen JG, Thuren T, Libby P, Glynn RJ, Ridker PM. Inhibition of interleukin-1β and reduction in atherothrombotic cardiovascular events in the CANTOS trial. J Am Coll Cardiol. 2020;76(14):1660–1670. doi:10.1016/j.jacc.2020.08.011
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.