Back to Journals » Patient Preference and Adherence » Volume 19
Medication Adherence Interventions Among People Living with Diabetes: A Systematic Review
Authors Wang M, Lee K, Thew HZ ![]() , Sowtali SN, Jiang Q, Cao Y, Lim PY
, Sowtali SN, Jiang Q, Cao Y, Lim PY ![]()
Received 3 June 2025
Accepted for publication 4 September 2025
Published 7 October 2025 Volume 2025:19 Pages 3095—3112
DOI https://doi.org/10.2147/PPA.S544443
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Meng Wang,1 Khuan Lee,1 Hui Zhu Thew,2 Siti Noorkhairina Sowtali,3 Qiuhuan Jiang,4 Yang Cao,1 Poh Ying Lim5
1Department of Nursing, Faculty of Medicine & Health Sciences, Universiti Putra Malaysia, Serdang, SGR, Malaysia; 2Department of Family Medicine, Faculty of Medicine & Health Sciences, Universiti Putra Malaysia, Serdang, SGR, Malaysia; 3Department of Professional Nursing Studies, International Islamic University, Kuala Lumper, SGR, Malaysia; 4Business Management Office, Henan Provincial People’s Hospital, Zhengzhou, Henan, People’s Republic of China; 5Department of Community Health, Faculty of Medicine & Health Sciences, Universiti Putra Malaysia, Serdang, SGR, Malaysia
Correspondence: Poh Ying Lim, Department of Community Health, Faculty of Medicine & Health Sciences, Universiti Putra Malaysia, UPM, Serdang, Selangor, 43400, Malaysia, Email [email protected]
Background: Medication adherence is a key factor in the management of Diabetes Mellitus (DM). Various interventions have been proposed to improve adherence.
Objective: The objective of this systematic review is to evaluate and summarize the effectiveness of different interventions aimed at improving medication adherence among people living with diabetes.
Methods: A comprehensive search was conducted across five databases (PubMed, Scopus, Embase, Cochrane Library, and ProQuest) to identify studies published between January 2015 and 1st April 2025. Studies were included if they focused on people living with diabetes and interventions targeting medication adherence, with an emphasis on randomized controlled trials (RCTs) published in English. Inclusion and exclusion criteria were independently reviewed for quality by three researchers.
Results: A total of 38 studies were included in this review, with 18 studies as low risk of bias, and the remaining studies exhibiting either some concerns risk of bias. Most studies were conducted in developing countries, with face-to-face education being the most commonly used intervention. Multi-component interventions were also frequently employed. The Morisky Medication Adherence Scale (MMAS) was the most widely used tool for measuring medication adherence. Additionally, eight studies incorporated theoretical models into their interventions.
Conclusion: Both traditional and modern interventions have demonstrated potential in improving medication adherence among people living with diabetes, with multi-component strategies showing the most promising results. Future research should focus on integrating appropriate theoretical models into intervention designs and assessing the long-term effectiveness of these interventions across different populations.
Keywords: diabetes mellitus, medication adherence, intervention, systematic review
Introduction
Diabetes mellitus (DM) is a chronic metabolic disease characterized by persistent hyperglycemia and has become a major global public health concern.1 It is estimated that in 2021, approximately 536.6 million individuals aged 20–79 years worldwide were living with diabetes and this number is projected to rise to 783.2 million by 2045.2 Without effective management, chronic hyperglycemia can lead to serious complications such as kidney disease,3 retinopathy4 and cardiovascular diseases,5 significantly compromising patients’ quality of life and life expectancy. Despite the availability of various effective pharmacological treatments, poor medication adherence remains a major barrier to achieving optimal glycemic control. Studies have reported that the prevalence of poor medication adherence among people living with diabetes ranges from 70% to 80%.6,7 Suboptimal adherence not only increases the risk of disease progression and the development of complications but also contributes to higher hospitalization rates and healthcare costs.8–10
In recent years, a variety of intervention strategies have been developed to improve medication adherence in people living with diabetes, including health education programs,11 blood glucose monitoring systems,12 and digital health technologies.13 However, existing systematic reviews have primarily focused on identifying influencing factors and evaluating measurement tools for medication adherence,14,15 rather than providing a comprehensive analysis of interventions themselves. Some reviews have categorized interventions based on behavior change techniques,16 yet they have not systematically summarized the specific characteristics and implementation methods of each intervention. Other reviews have narrowly focused on particular intervention types, such as pharmacist-led programs or smartphone applications,17,18 thereby limiting the generalizability of their findings. Additionally, many available reviews are based on studies conducted more than a decade ago,19,20 which may not adequately reflect recent advancements in medical technologies and healthcare delivery.
In light of these gaps, the present systematic review aims to comprehensively include studies published in the past decade, covering all types of DM patients. By systematically reviewing and synthesizing the latest evidence on medication adherence interventions, this study seeks to provide an updated, detailed and holistic overview of intervention strategies, implementation approaches and their effectiveness. The findings are expected to fill current gaps in the literature and offer practical insights for the development of more targeted and effective interventions in clinical practice, as well as guide future research directions.
Methods
This review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement21 and was prospectively registered in PROSPERO (International Prospective Register of Systematic Reviews, registration number CRD42024545467). The review includes studies published between 1st January 2015 and 1st April 2025. A total of five electronic databases were searched for relevant studies: PubMed, Scopus, Embase, Cochrane Library, and ProQuest.
Ethical Considerations
Since this study is a systematic review utilizing publicly available, non-identifiable secondary data from published studies, ethical approval was not necessary in accordance with institutional guidelines.
Search Strategy and Selection Criteria
The keywords used were “(diabetes mellitus OR diabetes OR diabetic OR type 1 DM OR type 2 DM OR T1DM OR T2DM OR glucose intolerance OR glucose metabolism disorders) AND (medication adherence OR medication compliance OR drug compliance OR drug adherence OR medication nonadherence OR nonadherence, medication OR noncompliance, medication OR medication non-adherence OR medication persistence) AND (intervention OR impact OR effect OR effectiveness)”. The inclusion criteria for studies are as follows: (1) study population must consist of individuals diagnosed with DM, (2) intervention must focus on medication adherence strategies, (3) study must be published in a peer-reviewed journal with an English language version, (4) study design must be a Randomized Controlled Trial (RCT) and (5) published between 2015 and 2025. The exclusion criteria are: (1) journals that are not published in peer-reviewed sources, such as conference proceedings, conference books, government reports, grey literature or short communications, (2) review journals or meta-analyses and (3) studies that are not available in full text.
Selection of Article (Screening and Eligibility)
This review excluded unpublished, duplicate, non-English, and irrelevant articles. To ensure objectivity, two researchers (MW and YC) independently screened titles, abstracts, and full texts based on the inclusion and exclusion criteria, cross-checking the extracted data. Disagreements were resolved by a third researcher (PYL). The screening process consisted of two phases: the first involved title and abstract review, followed by full-text assessment in the second phase to confirm relevance and adherence to the criteria.
Data Extraction
The data were extracted using a pre-designed form encompassing the following: (1) first author, publication date, (2) study population and sample size, (3) country, (4) study design, (5) measurement instrument and interventionist, (6) intervention on duration, delivery mode and time points, (7) intervention effect and statistical significance. Due to the high heterogeneity in study designs, interventions, measurement instruments and outcomes, a meta-analysis was not performed.
Risk of Bias Assessment
The quality of the Randomized Controlled Trials (RCTs) included in this review was assessed using the Cochrane Risk of Bias Tool 2 (RoB 2).22 This tool evaluated bias across five domains, ensuring that only studies with a low risk of bias contributed to the evidence on medication adherence interventions for people living with diabetes. Two researchers independently assessed the studies and discrepancies were resolved through discussion among all authors.
Results
Literature Search
Out of 11,711 potential articles, 3,923 duplicate records were removed using Endnote 21 software. Of the remaining 7,788 articles, 7,599 were excluded based on their titles, followed by 189 exclusions based on abstracts and keywords. Ultimately, 38 studies met all eligibility criteria for inclusion in this review. The selection process is illustrated in Figure 1.
 |
Figure 1 Flowchart of the systematic review selection process. |
Quality Assessment
Based on the RoB2 standard, the risk of bias for all 38 included RCTs was assessed. The overall risk of bias results showed that 20 studies as having some concerns and 18 studies as low risk of bias. Supplementary Figure 1 and Supplementary Figure 2 present the detailed evaluation of the included studies, covering aspects such as randomization, interventions, missing outcome data, outcome measurement and reporting of results.
Study Characteristics and Diversity
The 38 studies included in this review originated from various countries, with the highest number of studies coming from India, the United States and Iran. Among the 38 studies, 34 (89%) focused on T2DM (Type 2 Diabetes Mellitus) patients, 32 studies (84%) had participants aged ≥18 years, while 6 studies (16%) did not specify the age range. The largest study had a sample size of 63,012 participants, while the smallest included only 41 participants. The total sample size across all studies was 70,457 (excluding one community-based study that did not provide specific numbers). The duration of the studies varied widely, ranging from two weeks to 15 months. The measurement tools used across the included studies were primarily categorized into two forms: self-reported questionnaires and pill counts. The most commonly used adherence assessment instruments were the Morisky Medication Adherence Scale (MMAS), utilized in 14 studies (37%), and the Medication Adherence Report Scale (MARS), used in four studies (11%). Regarding intervention providers, 15 studies (40%) were pharmacist-led, while 19 studies (50%) did not specify the identity of the interventionist and were conducted by research staff. Additionally, three studies (8%) involved nurse-led interventions, and one study (3%) was led by a medical advisor or therapist. Further details are provided in Table 1.
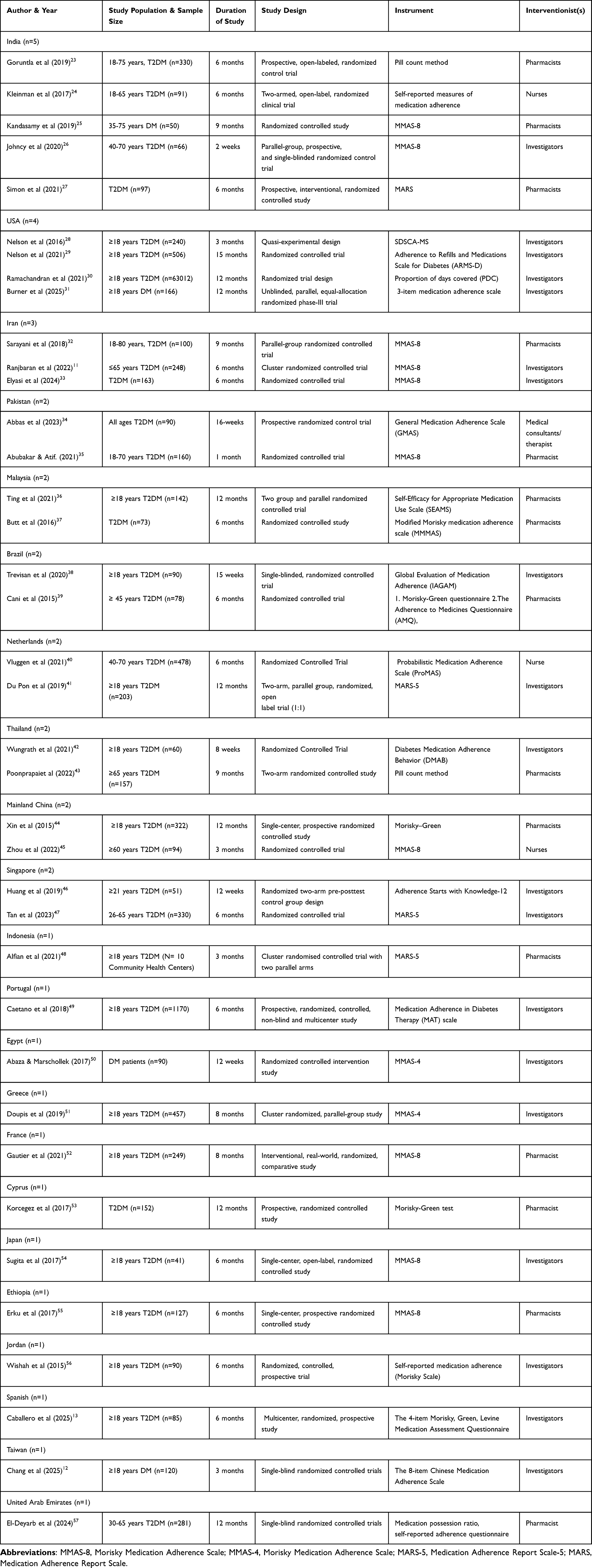 |
Table 1 Summary of the Selected Studies (N=38 Articles) |
Intervention Strategies and Theoretical Models for Medication Adherence in People Living with Diabetes
The 38 studies included in this review utilized a variety of interventions to improve medication adherence among people living with diabetes. 14 studies (37%) employed face-to-face interactions, including oral communication, meetings, educational courses and interviews. 11 studies (29%) utilized multiple combinations of methods. Additionally, five studies (13%) used text messages, three studies (8%) utilized internet-based interventions, two studies (5%) employed telephone interventions, two studies (5%) used mobile applications (apps) and one study (3%) involved fliers. Only eight studies (21%) incorporated theoretical models into their design. The most commonly used models were the theory of planned behavior, self-determination theory, information-motivation-behavioral skills model and the health belief model, with some studies combining multiple models. It is noteworthy that five studies (13%) showed no significant improvement in medication adherence (P > 0.05). Among these, one study used two different questionnaires to measure medication adherence: one questionnaire indicated a positive effect, while the other showed no effect. The remaining studies demonstrated a positive impact of the interventions on medication adherence among people living with diabetes. The detailed results are presented in Tables 2 and 3.
 |
Table 2 Intervention Associated with Medication Adherence Among DM Patients for Selected Studies (n=38) |
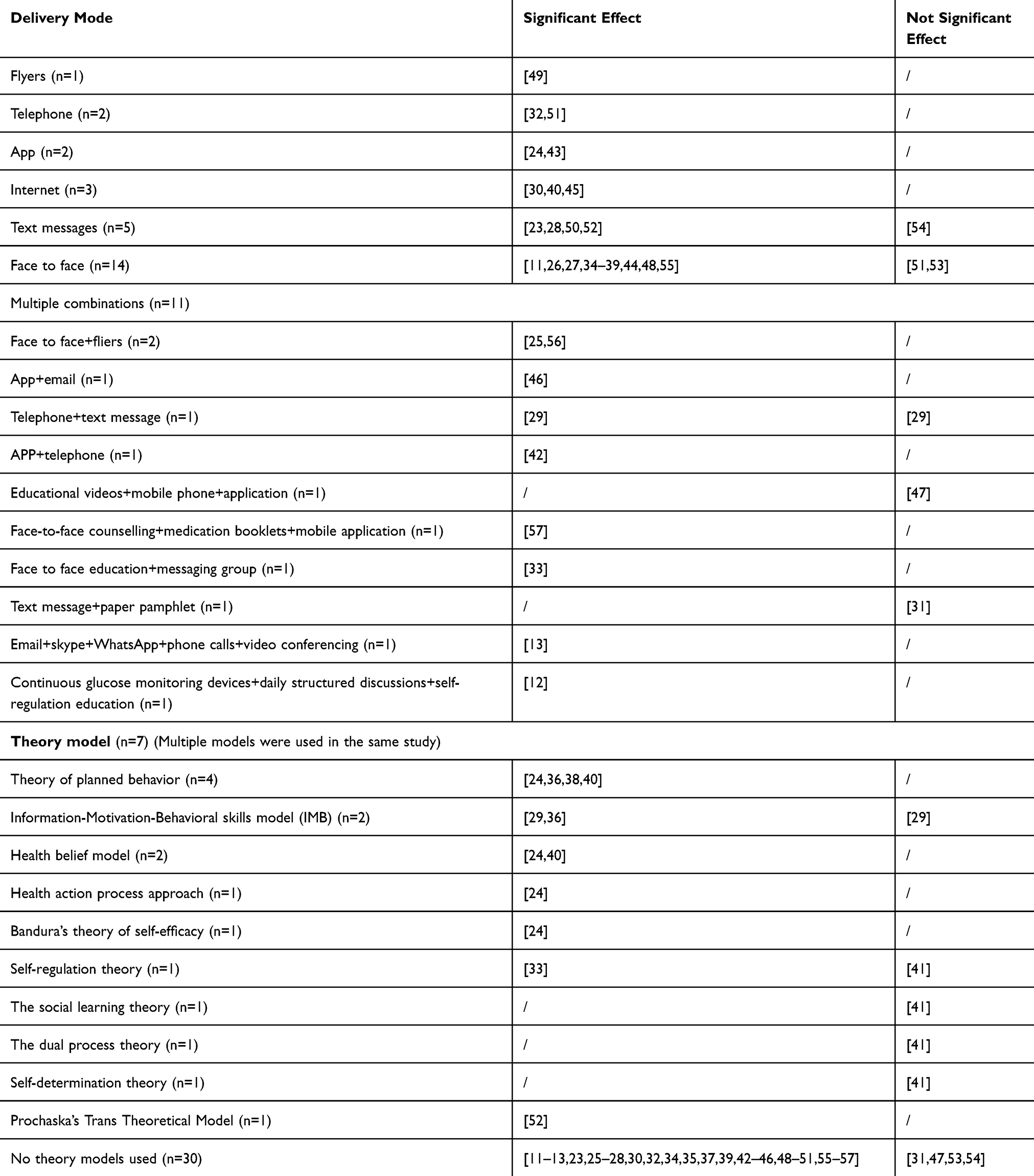 |
Table 3 Type of Theory Models and Delivery Mode Used in the Studies (n = 38 Articles) |
Discussion
This systematic review shows that over 90% of studies on medication adherence interventions focused on patients diagnosed with T2DM, likely because T2DM accounts for the largest proportion of all DM types, reaching 90–95% of cases.58,59 The majority of studies were conducted in developing countries, where medication adherence is generally lower, with over 50% of patients exhibiting poor adherence.60,61 Developing countries frequently encounter substantial constraints in healthcare resources and services, underscoring the importance of implementing cost-effective and efficient strategies, such as enhancing medication adherence. Targeted interventions can enhance adherence, thereby reducing the risks of ineffective treatment and acute complications associated with poor medication adherence.62,63
Questionnaires are the most commonly used tool for assessing medication adherence, with the MMAS being the most widely employed. This is supported by a systematic review conducted by Clifford et al (2014), which confirms the prevalence of this method.14 The widespread use of questionnaires may be attributed to their speed, simplicity, and cost-effectiveness, especially in large-scale studies. Compared to other objective measurement methods, questionnaires do not require expensive equipment or specialized personnel and can capture a range of information related to patients’ behaviors, attitudes, and perceptions about medication. They offer insights into patients’ cognitive, attitudinal, and emotional dimensions of medication adherence. In contrast, the pill count method and Proportion of Days Covered (PDC) are used less frequently. These methods, while providing more objective data, are often more complex and difficult to implement on a large scale, with challenges in data collection. Additionally, access to comprehensive medication records may be limited, especially in resource-constrained settings. A systematic review by Cramer (2004) highlighted that electronic monitoring systems can effectively improve medication adherence among people living with diabetes.64 However, since the studies included in this review were published before 2003 and were not limited to RCTs, this method was not incorporated into the current review. Future studies could explore the integration of these objective methods with more accessible tools like questionnaires to balance the accuracy of measurement with practical feasibility.
This systematic review included 14 studies that employed face-to-face interventions, primarily in the form of one-on-one education, health education sessions, lectures and workshops, and group discussions. Through direct interaction, patients and healthcare providers (such as physicians, nurses and pharmacists) were able to communicate more effectively, enabling patients to better understand and adhere to their medication regimens. A systematic review by Williams (2014) demonstrated that face-to-face education can significantly improve medication adherence among people living with diabetes, enhancing disease management and treatment outcomes.19 Although less commonly used, interventions such as text messaging, telephone calls, and printed materials (fliers) have also shown effectiveness in improving medication adherence. A systematic review by Presley (2019) found that these approaches can significantly enhance adherence, with digital materials and printed fliers demonstrating greater effectiveness than telephone-based interventions.17 With the advancement of technology, apps and internet-based interventions have emerged as promising tools. These technologies offer personalized medication reminders, health education and medication tracking features, thereby supporting patients in better managing their health. In this review, two studies using mobile apps and three using internet-based interventions reported positive outcomes, suggesting that modern digital approaches hold potential for improving medication adherence among patients with DM. A systematic review by Islam (2022), which examined the impact of smartphone applications on medication adherence in DM, emphasized the importance of rigorous evaluation and selection of such apps.18 The review noted that nearly half of publicly available, free apps failed to demonstrate moderate to high levels of effectiveness. Therefore, implementing only high-quality, evidence-based applications in clinical settings is essential to achieving meaningful health outcomes. However, a systematic review by Williams (2014) reported no significant improvements in adherence with internet-based interventions. This may be attributed to the fact that most of the included studies were conducted over a decade ago, at a time when internet technology was less developed and digital interventions were still in their early stages of implementation.
This systematic review included 11 studies that employed multi-component interventions to improve medication adherence among patients with DM. These interventions combined various strategies with the aim of enhancing patient engagement and adherence through multiple channels. Examples include face-to-face education combined with printed materials (fliers), mobile applications combined with email, educational videos combined with mobile phones and apps, and continuous glucose monitoring devices integrated with daily structured discussions and self-regulation education. Compared with single-mode interventions, multi-component approaches offer advantages in flexibility, personalization and sustainability. For instance, while traditional face-to-face interventions provide personalized education, they are often limited by fixed time and location, making them less adaptable to patients’ evolving needs. In contrast, digital tools such as mobile apps, SMS and emails can deliver support anytime and anywhere, enabling continuous patient engagement and improving adherence outcomes. However, the implementation of multi-component interventions also poses certain challenges. These include patients’ acceptance of new technologies, access to necessary devices and the effective integration of various components within a single intervention framework. Future research should further explore the feasibility and effectiveness of such interventions across diverse populations and settings and focus on optimizing their design to ensure maximum impact.
Notably, only a small number of studies incorporated theoretical models into interventions aimed at improving medication adherence among people living with diabetes. The most commonly used frameworks included the Theory of Planned Behavior (4 studies), the Health Belief Model (2 studies) and the Information-Motivation-Behavioral Skills Model (2 studies). With the exception of one study that applied four theoretical models simultaneously but did not yield significant results, all other theory-based interventions demonstrated improvements in adherence. Among the 30 studies that did not apply any theoretical framework, four reported no significant effects, while the rest showed positive outcomes. This suggests that the effectiveness of an intervention is not solely dependent on the presence of a theoretical model, but rather on the appropriateness of the model selected and the rigor of its application in both the design and implementation phases. The use of theoretical models is not about quantity, but fit. A well-matched theoretical framework can offer a structured understanding of health behaviors, clarify mechanisms of behavior change and guide the selection of targeted strategies and techniques. For example, the Theory of Planned Behavior emphasizes the roles of intention and perceived behavioral control, making it suitable for interventions that aim to enhance motivation and perceived ability to adhere to medication regimens.65 The Health Belief Model, on the other hand, focuses on perceived susceptibility, severity and benefits, and is useful in addressing beliefs about disease risk and treatment effectiveness.66 Therefore, future studies should prioritize the integration of relevant theoretical frameworks as a foundation for intervention design. Theory-driven approaches not only improve the precision and relevance of interventions, but also facilitate a better understanding of the underlying mechanisms contributing to behavior change. Ultimately, such approaches may lead to higher-quality and more sustainable improvements in medication adherence.
Limitations
Despite conducting an exhaustive search using five databases, this systematic review is not without its limitations. The search was confined to articles published between 1st January 2015 and 1st April 2025, exclusively including English articles, potentially influencing the study outcomes. The encompassed studies employed a diverse range of intervention measures, were carried out in various countries, and utilized a wide array of research tools, thereby rendering the conduction of a meta-analysis impractical.
Conclusion
This systematic review provides a comprehensive analysis of various interventions aimed at improving medication adherence among people living with diabetes. The findings suggest that face-to-face health education remains one of the most commonly used and effective intervention strategies, enhancing patient engagement and adherence. However, modern technological interventions, such as mobile applications and internet-based tools, also show great potential for improving adherence, particularly when used in combination with traditional methods. The integration of multi-component interventions, combining approaches like face-to-face interactions, digital tools and continuous monitoring devices, addresses the limitations of single-mode interventions by offering greater flexibility, personalization, and sustainability.
Despite the promising outcomes, challenges remain in ensuring the effective integration of these interventions and in improving patient acceptance of new technologies. Future studies should prioritize the selection of appropriate theoretical models to guide intervention design, as the effectiveness of these models hinges on their relevance to the specific behaviors and characteristics of the target population. The review emphasizes the importance of rigorously evaluating digital tools, with only high-quality validated applications being recommended for clinical use. While multi-component interventions and theoretical frameworks hold significant potential, further research is needed to assess their long-term effects and feasibility, in order to optimize intervention designs and achieve more sustainable improvements in medication adherence. This study provides valuable evidence and recommendations for improving medication adherence in people living with diabetes. Future intervention designs should focus more on comprehensiveness and personalization, providing stronger theoretical support and empirical data for diabetes medication adherence interventions.
Acknowledgments
The authors acknowledge Universiti Putra Malaysia for their support and contributions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors acknowledge Universiti Putra Malaysia for funding support for this article fees.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hossain MJ, Al-Mamun M, Islam MR. Diabetes mellitus, the fastest growing global public health concern: early detection should be focused. Health Sci Rep. 2024;7(3):e2004. doi:10.1002/hsr2.2004
2. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
3. Kumar M, Dev S, Khalid MU, et al. The bidirectional link between diabetes and kidney disease: mechanisms and management. Cureus. 2023;15(9):e45615. doi:10.7759/cureus.45615
4. Han JX, Wang H, Liang HH, Guo JX. Correlation of the retinopathy degree with the change of ocular surface and corneal nerve in patients with type 2 diabetes mellitus. Int J Ophthalmol. 2021;14(5):750–758. doi:10.18240/ijo.2021.05.17
5. Jyotsna F, Ahmed A, Kumar K, et al. Exploring the complex connection between diabetes and cardiovascular disease: analyzing approaches to mitigate cardiovascular risk in patients with diabetes. Cureus. 2023;15(8):e43882. doi:10.7759/cureus.43882
6. Heflin C, Hodges L, Ojinnaka CO, Arteaga I. Hypertension, diabetes and medication adherence among the older supplemental nutritional assistance program population. J Gerontol. 2022;41(3):780–787. doi:10.1177/07334648211022493
7. Ahmed S, Saif-Ur-Rahman KM, Dhungana RR, et al. Medication adherence and health-related quality of life among people with diabetes in Bangladesh: a cross-sectional study. Endocrinol Diabetes Metab. 2023;6(5):e444. doi:10.1002/edm2.444
8. Pallangyo P, Millinga J, Bhalia S, et al. Medication adherence and survival among hospitalized heart failure patients in a tertiary hospital in Tanzania: a prospective cohort study. BMC Res Notes. 2020;13(1):89. doi:10.1186/s13104-020-04959-w
9. Sendekie AK, Netere AK, Kasahun AE, Belachew EA. Medication adherence and its impact on glycemic control in type 2 diabetes mellitus patients with comorbidity: a multicenter cross-sectional study in Northwest Ethiopia. PLoS One. 2022;17(9):e0274971. doi:10.1371/journal.pone.0274971
10. Rasu RS, Xavier C, Rianon N. Dynamic changes in medication burden leading to fall and hospital readmissions in older adults: toward a strategy for improving risk and managing costs. J Manag Care Spec Pharm. 2025;31(1):96–100. doi:10.18553/jmcp.2025.31.1.96
11. Ranjbaran S, Shojaeizadeh D, Dehdari T, Yaseri M, Shakibazadeh EJD, Syndrome M. The effectiveness of an intervention designed based on health action process approach on diet and medication adherence among patients with type 2 diabetes: a randomized controlled trial. Diabetol Metab Syndr. 2022;14(1):1–10.
12. Chang HY, Yeh KC, Huang YY, Li JH. The impact of self-regulation education combined with Continuous Glucose Monitoring (CGM) on diabetes outcomes: a randomized controlled study. Nurs Rep. 2025;15(3):94. doi:10.3390/nursrep15030094
13. Caballero Mateos I, Morales Portillo C, Lainez López M, Vilches-Arenas Á. Efficacy of a digital educational intervention for patients with type 2 diabetes mellitus: multicenter, randomized, prospective, 6-month follow-up study. J Med Internet Res. 2025;27:e60758. doi:10.2196/60758
14. Clifford S, Perez-Nieves M, Skalicky AM, Reaney M, Coyne KS. A systematic literature review of methodologies used to assess medication adherence in patients with diabetes. Curr Med Res Opin. 2014;30(6):1071–1085. doi:10.1185/03007995.2014.884491
15. Gow K, Rashidi A, Whithead L. Factors influencing medication adherence among adults living with diabetes and comorbidities: a qualitative systematic review. Curr Diab Rep. 2024;24(2):19–25. doi:10.1007/s11892-023-01532-0
16. Teo V, Weinman J, Yap KZ. Systematic review examining the behavior change techniques in medication adherence intervention studies among people with type 2 diabetes. Ann Behav Med. 2024;58(4):229–241. doi:10.1093/abm/kaae001
17. Presley B, Groot W, Pavlova M. Pharmacy-led interventions to improve medication adherence among adults with diabetes: a systematic review and meta-analysis. Res Social Administrative Pharmacy. 2019;15(9):1057–1067. doi:10.1016/j.sapharm.2018.09.021
18. Islam SMS, Mishra V, Siddiqui MU, et al. Smartphone apps for diabetes medication adherence: systematic review. JMIR Diabetes. 2022;7(2):e33264. doi:10.2196/33264
19. Williams JL, Walker RJ, Smalls BL, Campbell JA, Egede LE. Effective interventions to improve medication adherence in type 2 diabetes: a systematic review. Diabetes Manag. 2014;4(1):29–48. doi:10.2217/dmt.13.62
20. Wang J, Mo Y, Biao R. Chinese version of the 8-item Morisky medication compliance questionnaire in elderly patients with type 2 diabetes application reliability and validity. Chin J Gerontol. 2015;35(21):6242–6244.
21. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
22. Sterne JAC, Savović J, Page MJ, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898. doi:10.1136/bmj.l4898
23. Goruntla N, Mallela V, Nayakanti D. Impact of pharmacist-directed counseling and message reminder services on medication adherence and clinical outcomes in type 2 diabetes mellitus. J Pharm Bioallied Sci. 2019;11(1):69–76. doi:10.4103/jpbs.JPBS_211_18
24. Kleinman NJ, Shah A, Shah S, Phatak S, Viswanathan V. Improved medication adherence and frequency of blood glucose self-testing using an m-health platform versus usual care in a multisite randomized clinical trial among people with type 2 diabetes in India. Telemedicine J e-Health. 2017;23(9):733–740. doi:10.1089/tmj.2016.0265
25. Kandasamy K, Rajagopal Shanmuga S. Impact of a pharmacist intervention on improving medication adherence and knowledge towards diabetes mellitus: a randomised controlled study. J Int J Pharmaceut Res. 2019;11(1):416–420.
26. Johncy K, Matthew J, Mathew A, Koshy G, Raj J. Efficacy of structured education in enhancing medication adherence in type-2 diabetic patients admitted to a rural tertiary care hospital - A randomized control trial. Natl J Physiol Pharm Pharmacol. 2020:1. doi:10.5455/njppp.2020.10.06158202028062020
27. Simon MA, Raja BY, Varughese PC, et al. Pharmacist led intervention towards management of type 2 diabetes mellitus and assessment of patient satisfaction of care - A prospective, randomized controlled study. Diab Metab Syndr. 2021;15(5):102208. doi:10.1016/j.dsx.2021.102208
28. Nelson LA, Mulvaney SA, Gebretsadik T, Johnson KB, Osborn CY. The MEssaging for Diabetes (MED) intervention improves short-term medication adherence among low-income adults with type 2 diabetes. J Behav Med. 2016;39(6):995–1000. doi:10.1007/s10865-016-9774-2
29. Nelson LA, Greevy RA, Spieker A, et al. Effects of a tailored text messaging intervention among diverse adults with type 2 diabetes: evidence from the 15-month REACH randomized controlled trial. Diabetes Care. 2021;44(1):26–34. doi:10.2337/dc20-0961
30. Ramachandran B, Trinacty CM, Wharam JF, et al. A randomized encouragement trial to increase mail order pharmacy use and medication adherence in patients with diabetes. J Gen Intern Med. 2021;36(1):154–161. doi:10.1007/s11606-020-06237-8
31. Burner E, Hazime D, Menchine M, et al. mHealth social support versus standard support for diabetes management in safety-net emergency department patients: randomized phase-III trial. JMIR Diabetes. 2025;10(e56934):e56934. doi:10.2196/56934
32. Sarayani A, Mashayekhi M, Nosrati M, et al. Efficacy of a telephone-based intervention among patients with type-2 diabetes; a randomized controlled trial in pharmacy practice. Int J Clin Pharm. 2018;40(2):345–353. doi:10.1007/s11096-018-0593-0
33. Elyasi Z, Ghiasi N, Khorshidi A, Bakhtiyari S, Jalilian M. The effect of a health education program on knowledge, medication adherence, and glycosylated hemoglobin in rural patients with type 2 diabetes. Current Diabetes Rev. 2024;21. doi:10.2174/0115733998332358240923112144
34. Abbas Q, Latif S, Ayaz Habib H, et al. Cognitive behavior therapy for diabetes distress, depression, health anxiety, quality of life and treatment adherence among patients with type-II diabetes mellitus: a randomized control trial. BMC Psychiatry. 2023;23(1):86. doi:10.1186/s12888-023-04546-w
35. Abubakar M, Atif M. Impact of pharmacist-led interventions on diabetes management at a community pharmacy in pakistan: a randomized controlled trial. Inquiry. 2021;58:469580211036283. doi:10.1177/00469580211036283
36. Ting CY, Ahmad Zaidi Adruce S, Lim CJ, et al. Effectiveness of a pharmacist-led structured group-based intervention in improving medication adherence and glycaemic control among type 2 diabetes mellitus patients: a randomized controlled trial. Res Social Administrative Pharmacy. 2021;17(2):344–355. doi:10.1016/j.sapharm.2020.03.026
37. Butt M, Mhd Ali A, Bakry MM, Mustafa N. Impact of a pharmacist led diabetes mellitus intervention on HbA1c, medication adherence and quality of life: a randomised controlled study. Saudi Pharmaceutical J. 2016;24(1):40–48. doi:10.1016/j.jsps.2015.02.023
38. Trevisan DD, São-João T, Cornélio M, et al. Effect of an ‘implementation intention’ intervention on adherence to oral anti-diabetic medication in Brazilians with type 2 diabetes. Patient Educ Couns. 2020;103(3):582–588. doi:10.1016/j.pec.2019.10.003
39. Cani CG, Lopes Lda S, Queiroz M, Nery M. Improvement in medication adherence and self-management of diabetes with a clinical pharmacy program: a randomized controlled trial in patients with type 2 diabetes undergoing insulin therapy at a teaching hospital. Clinics. 2015;70(2):102–106. doi:10.6061/clinics/2015(02)06
40. Vluggen S, Candel M, Hoving C, Schaper NC, de Vries H. A web-based computer-tailored program to improve treatment adherence in patients with type 2 diabetes: randomized controlled trial. J Med Internet Res. 2021;23(2):e18524. doi:10.2196/18524
41. du Pon E, El Azzati S, van Dooren A, Kleefstra N, Heerdink E, van Dulmen S. Effects of a proactive interdisciplinary self-management (PRISMA) program on medication adherence in patients with type 2 diabetes in primary care: a randomized controlled trial. Patient Preference Adherence. 2019;13:749–759. doi:10.2147/ppa.S188703
42. Wungrath J, Autorn N. Effectiveness of Line application and telephone-based counseling to improve medication adherence: a randomized control trial study among uncontrolled type 2 diabetes patients. Health Promotion Perspect. 2021;11(4):438–443. doi:10.34172/hpp.2021.55
43. Poonprapai P, Lerkiatbundit S, Saengcharoen W. Family support-based intervention using a mobile application provided by pharmacists for older adults with diabetes to improve glycaemic control: a randomised controlled trial. Int J Clin Pharm. 2022;44(3):680–688. doi:10.1007/s11096-022-01389-5
44. Xin C, Xia Z, Jiang C, Lin M, Li G. Effect of pharmaceutical care on medication adherence of patients newly prescribed insulin therapy: a randomized controlled study. Patient Preference Adherence. 2015;9:797–802. doi:10.2147/ppa.S84411
45. Zhou Q, Zhu H, Zhang ZJAo CP. Effects of internet+ intelligent-based 5A care model on blood glucose level, compliance, self-care abilities and quality of life in elderly patients with type 2 diabetes. Arch Clin Psychiatry. 2022;49(2).
46. Huang Z, Tan E, Lum E, Sloot P, Boehm BO, Car J. A smartphone app to improve medication adherence in patients with type 2 diabetes in Asia: feasibility randomized controlled trial. JMIR mHealth uHealth. 2019;7(9):e14914. doi:10.2196/14914
47. Tan NC, Tyagi S, Lee CS, et al. Effectiveness of an algorithm-driven home telemonitoring system on the metabolic control and self-care behaviour of Asian adults with type-2 diabetes mellitus: a randomised controlled trial. J Telemed Telecare. 2023:1357633x231203490. doi:10.1177/1357633x231203490
48. Alfian SD, van Boven JFM, Abdulah R, Sukandar H, Denig P, Hak E. Effectiveness of a targeted and tailored pharmacist-led intervention to improve adherence to antihypertensive drugs among patients with type 2 diabetes in Indonesia: a cluster randomised controlled trial. Br J Clin Pharmacol. 2021;87(4):2032–2042. doi:10.1111/bcp.14610
49. Caetano I, Santiago LM, Marques M. Impact of written information on control and adherence in type 2 diabetes. Revista da Associacao Medica Brasileira. 2018;64(2):140–147. doi:10.1590/1806-9282.64.02.140
50. Abaza H, Marschollek M. SMS education for the promotion of diabetes self-management in low & middle income countries: a pilot randomized controlled trial in Egypt. BMC Public Health. 2017;17(1):962. doi:10.1186/s12889-017-4973-5
51. Doupis J, Alexandrides T, Elisaf M, et al. Influence of supervised disease understanding and diabetes self-management on adherence to oral glucose-lowering treatment in patients with type 2 diabetes. Diabetes Ther. 2019;10(4):1407–1422. doi:10.1007/s13300-019-0648-9
52. Gautier JF, Boitard C, Michiels Y, Raymond G, Vergez G, Guedon G. Impact of personalized text messages from pharmacists on medication adherence in type 2 diabetes in France: a real-world, randomized, comparative study. Patient Educ Couns. 2021;104(9):2250–2258. doi:10.1016/j.pec.2021.02.022
53. Korcegez EI, Sancar M, Demirkan K. Effect of a pharmacist-led program on improving outcomes in patients with type 2 diabetes mellitus from northern cyprus: a randomized controlled trial. J Manag Care Spec Pharm. 2017;23(5):573–582. doi:10.18553/jmcp.2017.23.5.573
54. Sugita H, Shinohara R, Yokomichi H, Suzuki K, Yamagata Z. Effect of text messages to improve health literacy on medication adherence in patients with type 2 diabetes mellitus: a randomized controlled pilot trial. Nagoya J Med Sci. 2017;79(3):313–321. doi:10.18999/nagjms.79.3.313
55. Erku DA, Ayele AA, Mekuria AB, Belachew SA, Hailemeskel B, Tegegn HG. The impact of pharmacist-led medication therapy management on medication adherence in patients with type 2 diabetes mellitus: a randomized controlled study. Pharmacy Practice. 2017;15(3):1026. doi:10.18549/PharmPract.2017.03.1026
56. Wishah RA, Al-Khawaldeh OA, Albsoul AM. Impact of pharmaceutical care interventions on glycemic control and other health-related clinical outcomes in patients with type 2 diabetes: randomized controlled trial. Diab Metab Syndr. 2015;9(4):271–276. doi:10.1016/j.dsx.2014.09.001
57. El-Deyarbi M, Ahmed L, King J, et al. The effects of multifactorial pharmacist-led intervention protocol on medication optimisation and adherence among patients with type 2 diabetes: a randomised control trial. F1000Res. 2024;13:493. doi:10.12688/f1000research.146517.2
58. Bruno G, Runzo C, Cavallo-Perin P, et al. Incidence of type 1 and type 2 diabetes in adults aged 30-49 years: the population-based registry in the province of Turin, Italy. Diabetes Care. 2005;28(11):2613–2619. doi:10.2337/diacare.28.11.2613
59. Leslie RD, Evans-Molina C, Freund-Brown J, et al. Adult-onset type 1 diabetes: current understanding and challenges. Diabetes Care. 2021;44(11):2449–2456. doi:10.2337/dc21-0770
60. Chin SS, Lau SW, Lim PL, Wong CM, Ujang N. Medication adherence, its associated factors and implication on glycaemic control in patients with type 2 diabetes mellitus: a cross-sectional study in a Malaysian primary care clinic. Malays Fam Physician. 2023;18:14. doi:10.51866/oa.88
61. Li Wang J, Zhang H. Investigation and analysis of medication compliance of elderly patients with type 2 diabetes mellitus in community. Chin J Drug Abuse Prevention Treatment. 2024;30(2):252–263. doi:10.15900/j.cnki.zylf1995.2024.02.015
62. Basu S, Garg S, Sharma N, Singh MM. Improving the assessment of medication adherence: challenges and considerations with a focus on low-resource settings. Ci Ji Yi Xue Za Zhi. 2019;31(2):73–80. doi:10.4103/tcmj.tcmj_177_18
63. Kao CC, Hsieh HM, Lee DY, Hsieh KP, Sheu SJ. Importance of medication adherence in treatment needed diabetic retinopathy. Sci Rep. 2021;11(1):19100. doi:10.1038/s41598-021-98488-6
64. Cramer JA. A systematic review of adherence with medications for diabetes. Diabetes Care. 2004;27(5):1218–1224. doi:10.2337/diacare.27.5.1218
65. Ajzen I. The Theory of Planned Behavior. Organizational Behavior and Decision Processes. University of Massachusetts at Amherst. Academic Press. Inc Cambridge; 1991.
66. Rosenstock IM, Strecher VJ, Becker MH. Social learning theory and the health belief model. Health Educ Q. 1988;15(2):175–183. doi:10.1177/109019818801500203
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medication Adherence and Its Associated Factors Among Outpatients with Heart Failure
Jarab AS, Al-Qerem WA, Hamam HW, Alzoubi KH, Abu Heshmeh SR, Mukattash TL, Alefishat E
Patient Preference and Adherence 2023, 17:1209-1220
Published Date: 8 May 2023
Medication Adherence in People with Asthma: A Qualitative Systematic Review of Patient and Health Professional Perspectives
Zhang X, Ding R, Zhang Z, Chen M, Yin Y, Quint JK
Journal of Asthma and Allergy 2023, 16:515-527
Published Date: 9 May 2023
Utilizing Social Determinants of Health Model to Understand Barriers to Medication Adherence in Patients with Ischemic Stroke: A Systematic Review
Ruksakulpiwat S, Benjasirisan C, Ding K, Phianhasin L, Thorngthip S, Ajibade AD, Thampakkul J, Zhang AY, Voss JG
Patient Preference and Adherence 2023, 17:2161-2174
Published Date: 30 August 2023
Latent Profile Analysis of Medication Beliefs in Patients with Type 2 Diabetes in the Hospital-Home Transition and Comparison with Medication Adherence
Jiang S, Luo T, Zhu Z, Huang Y, Liu H, Li B, Feng S, Zeng K
Patient Preference and Adherence 2024, 18:839-853
Published Date: 16 April 2024
The Impact of Self-Management Interventions on Behavioral and Clinical Outcomes in Individuals with Systemic Lupus Erythematosus: A Systematic Review of Empirical Evidence From 2003-2024
Hanrop S, Narupan N, Praha N, Phianhasin L, Ruksakulpiwat S
Patient Preference and Adherence 2025, 19:1763-1779
Published Date: 17 June 2025