Back to Journals » Journal of Inflammation Research » Volume 18
Association of Recreational Physical Activity with Gut Microbiota Diversity and Composition, and Symptom Burden in Crohn’s Disease: A Cross-Sectional Study
Authors Sun S ![]() , Chen Y, Zheng M
, Chen Y, Zheng M ![]() , Zhou M, Weng C, Fan Y, Lv B
, Zhou M, Weng C, Fan Y, Lv B
Received 17 March 2025
Accepted for publication 25 July 2025
Published 31 July 2025 Volume 2025:18 Pages 10295—10310
DOI https://doi.org/10.2147/JIR.S528820
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Nadia Andrea Andreani
Shaopeng Sun,* Yifei Chen,* Mingxu Zheng, Mi Zhou, Chunyan Weng, Yihong Fan, Bin Lv
Department of Gastroenterology, The First Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bin Lv, Department of Gastroenterology, The First Affiliated Hospital of Zhejiang Chinese Medical University, No. 54, Youdian Road, Shangcheng District, Hangzhou, Zhejiang Province, 310003, People’s Republic of China, Email [email protected]
Objective: This study aimed to investigate the potential benefits of physical activity (PA) on patient-reported outcomes (PROs) in individuals with Crohn’s disease (CD) and to examine whether these benefits are associated with gut microbiota.
Methods: This cross-sectional study included 251 patients with CD from two inflammatory bowel disease centers in China. Participants with CD provided information on their health background, PA, and PROs using the Global Physical Activity Questionnaire (GPAQ) and the Patient-reported Outcome Measurement Information System (PROMIS). Part of participants also provided a single fecal sample for analysis. Latent profile analysis (LPA) was conducted to categorize individuals with CD into classes based on PROs. Metagenomic sequencing was then performed, followed by bioinformatics assessment of taxonomy and diversity metrics.
Results: LPA identified two PRO patterns: low and high symptoms. Univariate and multivariate analyses indicated that disease activity and sedentary behavior were risk factors for symptom severity, whereas recreational PA, rather than work-and travel-related PA, and income served as protective factors (all p< 0.05). After controlling for age, gender, disease activity level, and other covariates, recreational PA explained microbiome diversity in patients with CD (p=0.016). The gut microbiota diversity (alpha or beta) significantly varied between patients with CD and low and high levels of recreational PA (all p< 0.05). A total of 29 dominant gut microbial taxa, including Oscillospiraceae, Ruminococcus, and Eubacterium rectale, have been identified as associated with recreational PA and primarily function in the butyric acid metabolism pathway.
Conclusion: Promoting the incorporation of recreational PA as an indicator of healthy lifestyle management for CD may improve patients’ subjective psychological and mental well-being, while also preserving intestinal microbial diversity. Recreational PA is associated with favorable patient-reported outcomes and increased diversity of gut microbiota in CD, supporting its inclusion in lifestyle management strategies.
Keywords: physical activity, exercise, Crohn’s disease, patient-reported outcomes, global physical activity questionnaire
Introduction
Crohn’s disease (CD) is a form of inflammatory bowel disease (IBD) characterized by persistent inflammation that can result in serious complications, such as fibrosis, intestinal fistulas, arthritis, and intestinal tumors.1–3 Although the incidence of CD has stabilized or declined in Western countries,4 it is increasing in Asia, particularly in China.5 A survey using urban medical insurance data in China reported an IBD incidence rate of 10.04 per 100,000, which was between newly industrialized and Western countries.6 CD is characterized by alternating periods of activity and remission. As there is currently no cure for CD, lifelong medication is required to manage symptoms and slow disease progression, posing significant physical and psychological challenges for patients.7 The precise etiology of CD remain unclear, but it is widely considered to be influenced by a combination of genetic, immune, microbial, and environmental factors.8 Although the introduction of biologics has ushered CD into the era of targeted therapy,9 clinical efficacy remains limited by factors such as variable drug responses, the high cost of biologics, and associated medication risks.10
Given that genetic factors contribute less than 10% of the pathogenesis of IBD, environmental factors are increasingly recognized as key determinants of disease onset and prognosis.11 Although medication remains the foundation of treatment, there is growing interest in the potential benefits of nonpharmacological interventions for patients with IBD.12 For instance, a Western diet increases the risk of developing CD.13 In addition, various lifestyle factors, such as sleep, stress, physical activity (PA), smoking, and alcohol consumption, are closely associated with the risk of CD.14 Consequently, lifestyle modifications play a crucial role in the clinical management of CD,15,16 with PA being a cost-effective approach for preventing various diseases.17
Several large-scale cohort studies have indicated that insufficient PA may increase the risk of CD.18,19 Similarly, a meta-analysis of seven studies supported this finding, revealing that individuals with higher PA levels have a lower risk of developing CD (RR = 0.63, 95% CI: 0.50–0.79).20 Thus, some researchers have designed exercise intervention programs for patients with CD to investigate the potential benefits of PA. Robinson et al21 were the first to implement a low-impact exercise program focused on core flooring for patients with CD, demonstrating that progressive low-impact exercise can enhance bone density and lower the risk of osteoporotic fractures. Souza Tajiri GJ et al22 developed an 8-week progressive resistance training program targeting the quadriceps to help alleviate muscle weakness in patients with CD. A controlled before-after study23 was conducted on patients with CD who had a predominantly sedentary lifestyle and who implemented a 12-week walking program. This intervention led to significant improvements in several indicators, including the inflammatory bowel disease stress index, inflammatory bowel disease quality of life index, and Harvey and Bradshaw simple index of Crohn’s Disease activity. Cronin et al24 conducted a randomized crossover study involving an 8-week combined aerobic and resistance training program. After trial completion, the exercise group exhibited significant improvements in body composition, cardiorespiratory fitness, and gut microbiota, with no reported adverse effects. Emerging evidence suggests that the gut microbiota mediates the impact of PA on CD. A previous population-based study involving 8416 healthy participants confirmed a correlation between PA and gut microbiota abundance of specific microbial taxa.25 A narrative review summarized that exercise can alter and reverse the microbiota dysbiosis associated with colon cancer.26 CD is characterized by significant dysbiosis, including reduced short-chain fatty acid-producing bacteria. Although few PA intervention studies conducted in CD populations have used gut microbiota as an outcome measure, evidence from animals with colitis revealed that PA intervention significantly increased gut microbiota diversity and the abundance of butyrate-producing bacteria, while fecal propionate and butyrate content also increased.27
This growing body of evidence supports the idea that PA can improve the outcomes of patients with CD. However, recent studies have suggested that the health benefits of PA may vary depending on the domain in which it is performed.28,29 For instance, research on cardiovascular disease indicates that recreational PA lowers the risk of onset and mortality,30,31 whereas high levels of work PA are associated with an increased risk of adverse health outcomes.32,33 This potential contrasting health effect between recreational and work PA is known as the “PA paradox”,34 highlighting the distinct characteristics of physical activities performed during leisure time and work. However, no studies have yet examined the different effects of recreational PA and work-related PA on the outcomes of patients with CD.
This study used the Patient-reported Outcome Measurement Information System (PROMIS) for symptom profiling and the Global Physical Activity Questionnaire (GPAQ) for PA quantification. Patients with CD were classified into two patient-reported outcomes (PROs)-based groups: low-symptom and high-symptom groups. Stratification by PROMIS domains may help identify subgroups who would benefit most from tailored lifestyle interventions. The relationship between the three types of PA (work, travel, and recreation) and these PRO classes was further examined. Notably, distinguishing PA domains is particularly relevant in Chinese contexts, where work PA often dominates daily energy expenditure, whereas recreational PA remains under-prioritized. A microbial-dependent mechanism was proposed to explain the potential benefits of recreational PA. As an observational cross-sectional study, these findings provide preliminary evidence for future mechanistic research.
Methods
Study Design and Setting
This prospective cross-sectional study was conducted at two Chinese IBD centers: Zhejiang Provincial Hospital of Traditional Chinese Medicine and the Second Affiliated Hospital of Zhejiang University School of Medicine. The recruitment and study period spanned from January 6, 2024, to March 8, 2024. All eligible patients with CD were invited to complete a questionnaire and provide stool samples.
Using the collected questionnaire responses and metagenomic sequencing data, two datasets were developed: the PA questionnaire and PA metagenomics datasets. A detailed description of these datasets is provided in the following section. This study was conducted in accordance with the guidelines of the Strengthening the Reporting of Observational Studies in Epidemiology statement. This study complies with the Declaration of Helsinki. Figure 1 shows the study flowchart.
 |
Figure 1 Flowchart of the study. |
Physical Activity Questionnaire Dataset (PAQD)
The PAQD included demographic details (age, gender, BMI, education, marital status, and income), personal lifestyle factors (smoking and alcohol consumption), disease-related data (disease duration, medication use, and surgical history), PA levels over the past week (work, travel, and recreation), and patient-reported outcomes. The complete PAQD can be found in Supplementary Table 1. The inclusion criteria were as follows: patients aged > 18 years with a confirmed diagnosis of CD based on endoscopic and histological findings. The exclusion criteria included the inability to provide informed consent or communicate in Chinese. A total of 251 valid questionnaires were collected to assess the association between PA levels and PROs.
Physical Activity Metagenomics Dataset (PAMD)
The PAMD contains fecal metagenomic data from 52 patients with CD who met the inclusion and exclusion criteria, along with 38 healthy control (HC) populations. Questionnaire data from 52 patients with CD were used to analyze the microbiota-dependent effects of PA. Considering the influence of diet, and antibiotic use on the gut microbiota, two exclusion criteria were applied during fecal sample collection: 1) antibiotic use within the past week, and 2) declining hospital-provided meals on the day of fecal sample collection. A total of 38 volunteers have been recruited. At the time of sample collection, they were not on any medication and ate the standardized hospital-provided meals. The raw sequencing data were submitted to the Sequence Read Archive (SRA) database (PRJNA1184213).
Assessment of PA
This study used the Chinese version of the GPAQ (version 2) available at https://www.who.int/zh/publications/m/item/global-physical-activity-questionnaire. The GPAQ comprises 16 questions, including one on sedentary behavior, to evaluate participants’ typical PA levels over the past week across three domains: work, travel-related, and recreational activities. PA levels were quantified using metabolic equivalent tasks (METs). Work- and recreation-related activities of moderate and vigorous intensity were assigned MET values of 4 and 8, respectively, while travel-related activities were scored at 4 METs. The total moderate-to-vigorous PA (MVPA) was then assessed. Participants were categorized into low-level and high-level PA groups according to their work, travel, and recreational PA levels. Based on the approach of Lo et al,18 individuals with high PA levels were defined as those in the top 50% of the cohort with nonzero values. This classification helps assess the influence of different types of PA on patient outcomes.
Patient-Reported Outcome Measurement
The patient-reported outcome measurement Information System (PROMIS-57) is a comprehensive 57-item multidimensional questionnaire used to evaluate various symptoms, including physical functioning, anxiety, depression, fatigue, sleep disturbances, pain interference, pain intensity, and social role participation.35 Pain intensity was evaluated using one item with 11 response options (ranging from 0 to 10), while the remaining domains were evaluated using eight items that were scored on a five-point Likert scale. Thus, the total scores for each domain ranged from 8 to 40.36 The raw scores were converted to T-scores (mean = 50, standard deviation (SD) = 10). Higher T-scores indicate improved functioning or increased symptom severity. The Cronbach α coefficient for this sample was excellent (0.96). The Chinese version of the PROMIS-57 was translated by the PROMIS National Center (PNC)-China (https://pnc-china.fudan.edu.cn), and permission to use the PROMIS instrument was obtained from PNC-China.
Latent Profile Analysis (LPA)
LPA is a statistical method used to identify unobserved (latent) subgroups within a population based on continuous variables, enabling the assessment of potential heterogeneity.37 The optimal number of LPA profiles was determined using several criteria, including Akaike’s information criterion (AIC), Bayesian information criterion (BIC), Lo–Mendell–Rubin test (LMR), bootstrapped likelihood-ratio test (BLRT), and entropy. Lower AIC and BIC values indicate better model fit, while higher entropy values suggest greater classification accuracy. LMR and BLRT were employed to compare the K-1 and K profile models. A P-value greater than 0.05 indicated that the K model was more suitable.38 The entropy was calculated to evaluate the accuracy of the profile classification, with higher values indicating clearer distinctions between profiles. When selecting the optimal number of profiles, it is also essential to consider model interpretability based on human judgment and experience.39 In summary, LPA was performed to obtain categorical latent variables that classify individuals into distinct groups based on their PROMIS-57 domain scores.
Fecal Sample Processing and Metagenomics Bioinformatics Analysis
Fecal samples were primarily collected for metagenomic sequencing to assess the gut microbiota status of patients. Immediately after collection, each sample was placed in a liquid nitrogen bottle. Microbiome analysis was conducted by Lianchuan Biotechnology Co., Ltd. (Hangzhou, China). Bacterial genomic DNA was extracted using Magnetic Beads Fecal Genome Extraction Kit (DP712, TIANGEN, China) from frozen colon contents based on the manufacturer’s instructions. Paired-end libraries were prepared using TruSeq Nano DNA LT Library Preparation Kit (Illumina, San Diego, CA, USA), with fragmentation, end-repair, adapter ligation, and PCR amplification steps performed according to the manufacturer’s protocol. After passing the quality assessment, high-throughput sequencing was conducted on the NovaSeq 6000 in PE150 sequencing mode. The raw sequencing data undergo de-splicing, processing of low-quality sequence data, and removal of host sequences to ensure that subsequent assembly and analysis focus solely on microbial sequences, leading to more accurate species identification and functional annotation. De novo assembly was performed on each sample, followed by coding sequence (CDS) prediction and the removal of short contigs. The nonredundant unigenes sets were then generated through sequence clustering. The unigenes were compared with the NR_sta library to classify species across various taxonomic levels. Alpha and Beta diversity analyses were conducted using annotated species-level statistical data. The raw sequencing data were submitted to the NCBI Sequence Read Archive (http://www.ncbi.nlm.nih.gov/bioproject/1184213).
The microbiome data were normalized by the CPM (Counts Per Million) method. Microbial diversity was assessed using α-diversity and β-diversity indices. α-diversity indices (Chao1, observed_species, Shannon index, and Simpson index) were calculated using R package “vegan”. β-diversity was evaluated using principal coordinate analysis (PCoA) to visualize the similarities and differences in community composition among samples. The Bray–Curtis distance was calculated based on microbial abundance information, and a permutational multivariate analysis of variance (PERMANOVA) test was performed using the R package “vegan”. Differential analysis was performed using the Wilcoxon rank-sum test. The screening threshold for differential species was p<0.05 and | log2 (fold_change) |>1. Differentially abundant gut microbiota (species level) were classified as “increased in abundance” when log2FC > 1 and “decreased in abundance” when log2FC < −1. P-values were adjusted using a false discovery rate (FDR) threshold of 0.05.
Statistical Analyses
LPA was performed using Mplus version 8.0, whereas logistic regression and Metagenomics bioinformatics analyses were performed using R Version 4.1.0. Continuous variables are presented as mean and standard deviation (SD). Categorical variables were summarized using frequency and proportion. Comparisons between the two groups were performed using Student’s t-test. To examine the association between demographic characteristics and LPA classification, univariate and multiple logistic regression analyses were conducted using the “epiDisplay” package in R. The multivariate association with linear models algorithm (MaAsLin2) was used to assess and control for potential confounding factors, enabling multivariate association analysis between recreational PA and microbial taxonomy in a clinical cohort. All statistical tests were two-sided, with significance set at a P value of less than 0.05. Differential metagenomics data were considered significant only if the adjusted P-value<0.05 and log2FC > 1 or log2FC < −1.
Results
Two Classes of Symptom Patterns Identified Through CD Patient-Reported Outcomes
A total of 251 individuals with CD completed the questionnaire and were included in the analysis. Among them, 82.9% (208/251) reported being in remission, whereas 17.1% (43/251) were in an active disease state. The overall male-to-female ratio was 2.3 (175/76), with an average participant age of 30.43 years (30.43±8.76).
All participants who completed the questionnaire (n = 251) were included in the LPA model. Table 1 lists the model fit indices for the one- to five-class models. As the number of classes increased, the AIC and BIC values decreased, and all models exhibited high entropy. Although the BLRT P-values were significant across all models, only the two-class model exhibited a significant LMR P-value. Thus, the two-class model demonstrated the best goodness-of-fit index and was selected as the optimal classification solution. Figure 2 illustrates the two latent profile subgroups. Class 1 (84%, n = 211) exhibited lower PROMIS scores and was identified as the low-symptom group. In contrast, Class 2 (16%, n = 40) exhibited higher PROMIS scores and was labeled as the high-symptom group. Table 2 presents the T–scores for the core symptoms of each class.
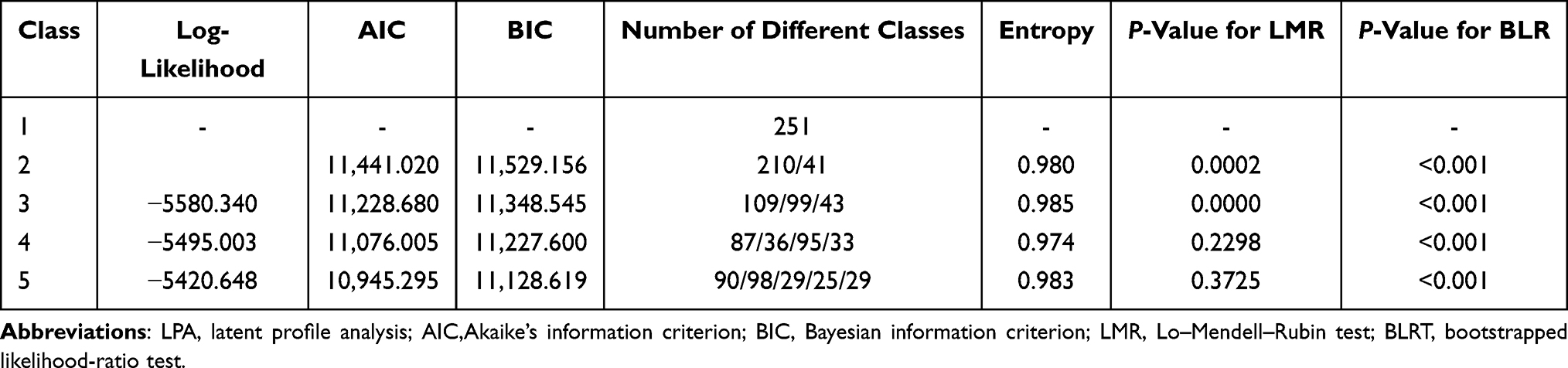 |
Table 1 Comparison of the LPA Model Fit Indices |
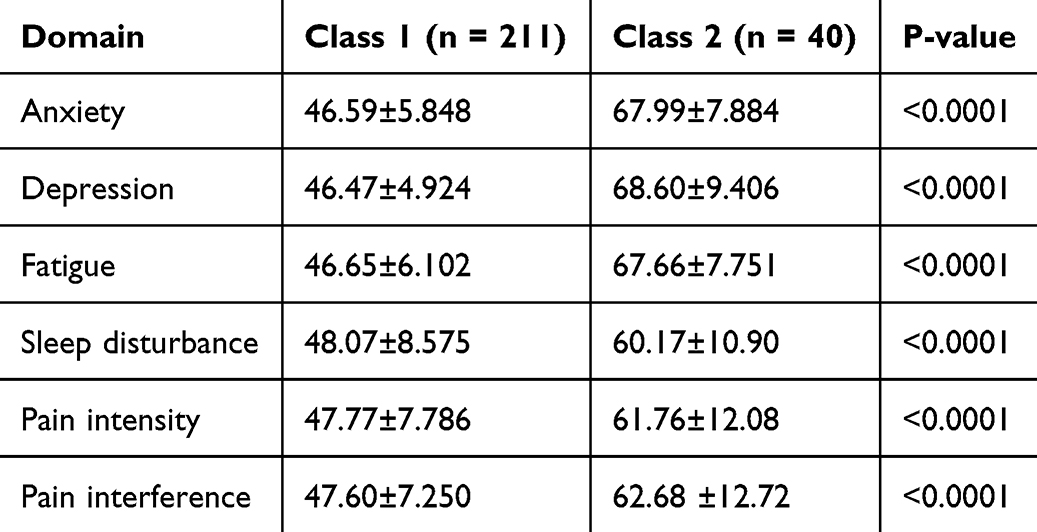 |
Table 2 T-Scores for Core Symptoms in Each Class, M (SD) |
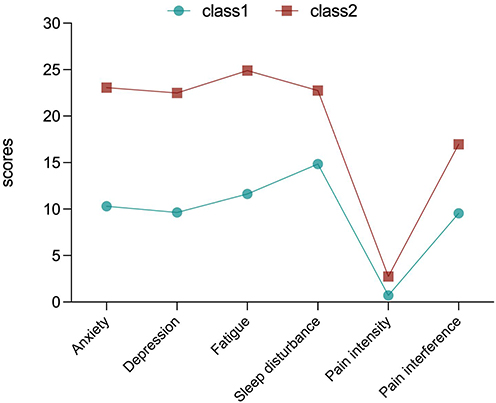 |
Figure 2 Two latent profiles with PROMIS items. |
Differences in Clinical Characteristics and PA Among the Latent Classes
Demographic variables were analyzed using univariate and multinomial logistic regression analyses to examine differences between the two subgroups. The low-symptom group (Class 1, n=211) was selected as the control. As presented in Table 3, univariate logistic regression analysis revealed significant differences between the high-symptom group (Class 2) and the control group, particularly in disease activity level, recreational PA, and sedentary time (all p<0.05). No significant differences were observed between the two groups in terms of age, gender, BMI, disease course, smoking, alcohol consumption, income, marital status, residence, current medications, or surgical history (all p>0.05).
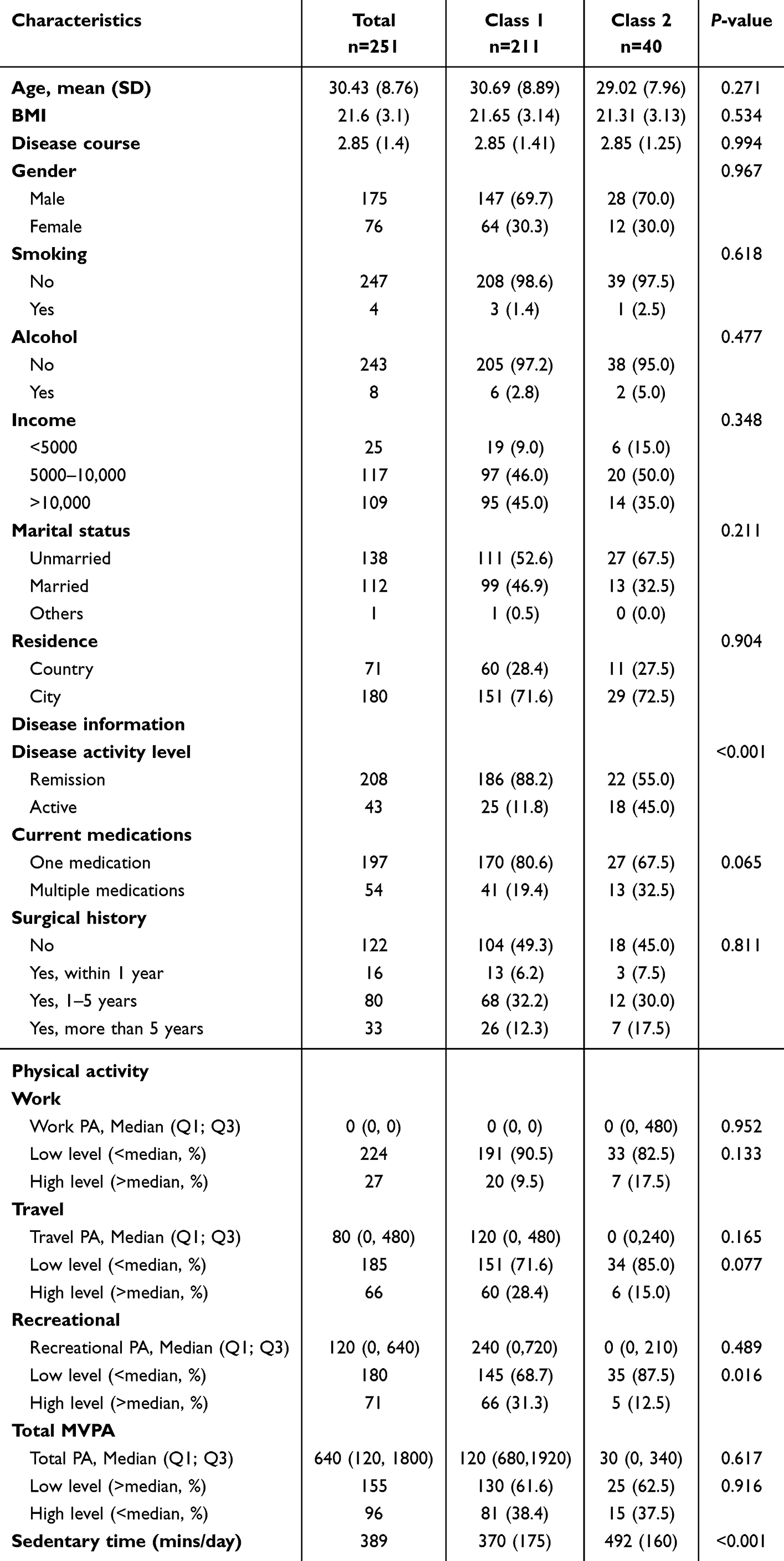 |
Table 3 Differences in Demographic Characteristics Between the Latent Classes |
This study primarily examined the impact of various types of PA on patient-reported outcomes. Statistical analysis revealed no significant differences in work-related or transportation-related PA between the two groups. However, recreational PA (p=0.016) and sedentary time (p<0.001) were identified as distinguishing factors (Table 3).
Clinical and PA-related variables were incorporated into the multinomial logistic regression model. Class 1, representing the “low-symptom group”, served as the reference for comparison. Male, no smoking and alcohol, unmarried, country, one medication, remission status, low levels of work, travel, recreation PA, and low-level total MVPA were used as reference categories. The age, disease course, BMI, sedentary time were treated as a continuous variable. As illustrated in Figure 3, patients in the active disease stage (odds ratio [OR] = 8.84, p<0.001), those with lower levels of recreational PA (OR = 0.24, p=0.037) and income (OR=0.19, p=0.029), and those with prolonged sedentary time (OR = 1.005, p<0.001) were more likely to be classified into Class 2. These findings indicate that active disease status and extended sedentary time are independent risk factors for patient-reported outcomes, whereas participation in recreational PA and high income are independent protective factors.
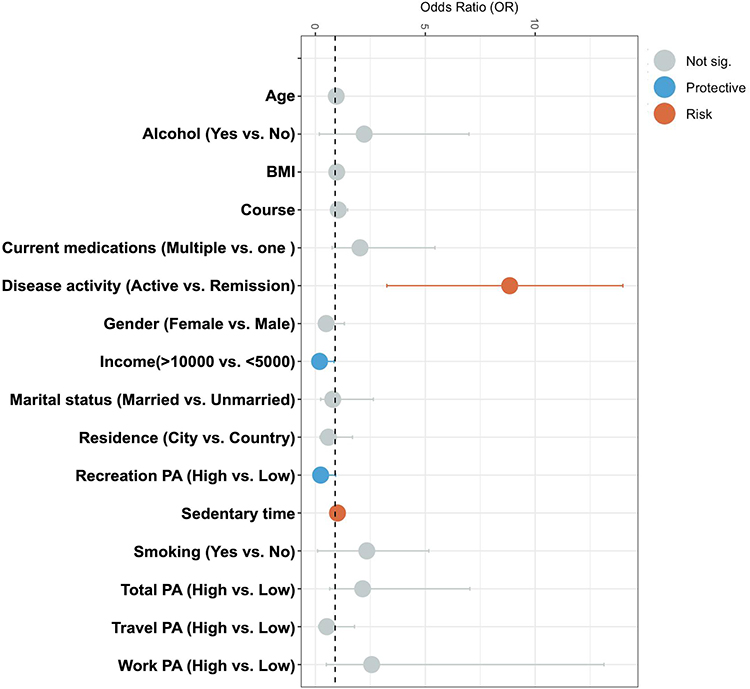 |
Figure 3 Forest plot of variables characteristics between latent profile subgroups. |
In addition, we further examined the association between sedentary time and disease status (remission or active) among all participants (n=251) and found no significant difference (p>0.05) in sedentary time among patients in the active stage compared with those in the remission stage (Supplementary Figure 1 and Supplementary Table 2).
Microbiome Diversity of CD Explained by Recreational PA
The findings of the aforementioned research, particularly the protective effects of recreational PA in patients with CD, have significantly piqued our interest. Research on the general population indicates that the protective effects of PA may be associated with gut microbiota; however, it remains unclear whether this protective effect persists in patients with CD. In this study, of the 251 participants who completed the questionnaire, 52 individuals provided additional fecal samples, including 40 (76.9%) in remission, and 12 (23.1%) with active disease. Among the 52 participants, those in the top 50% of the nonzero cohort, based on the GPAQ questionnaire results, were classified as having high recreational PA. In total, 32 participants were classified as having high recreational PA, and 20 as low-level participants (Figure 4A).
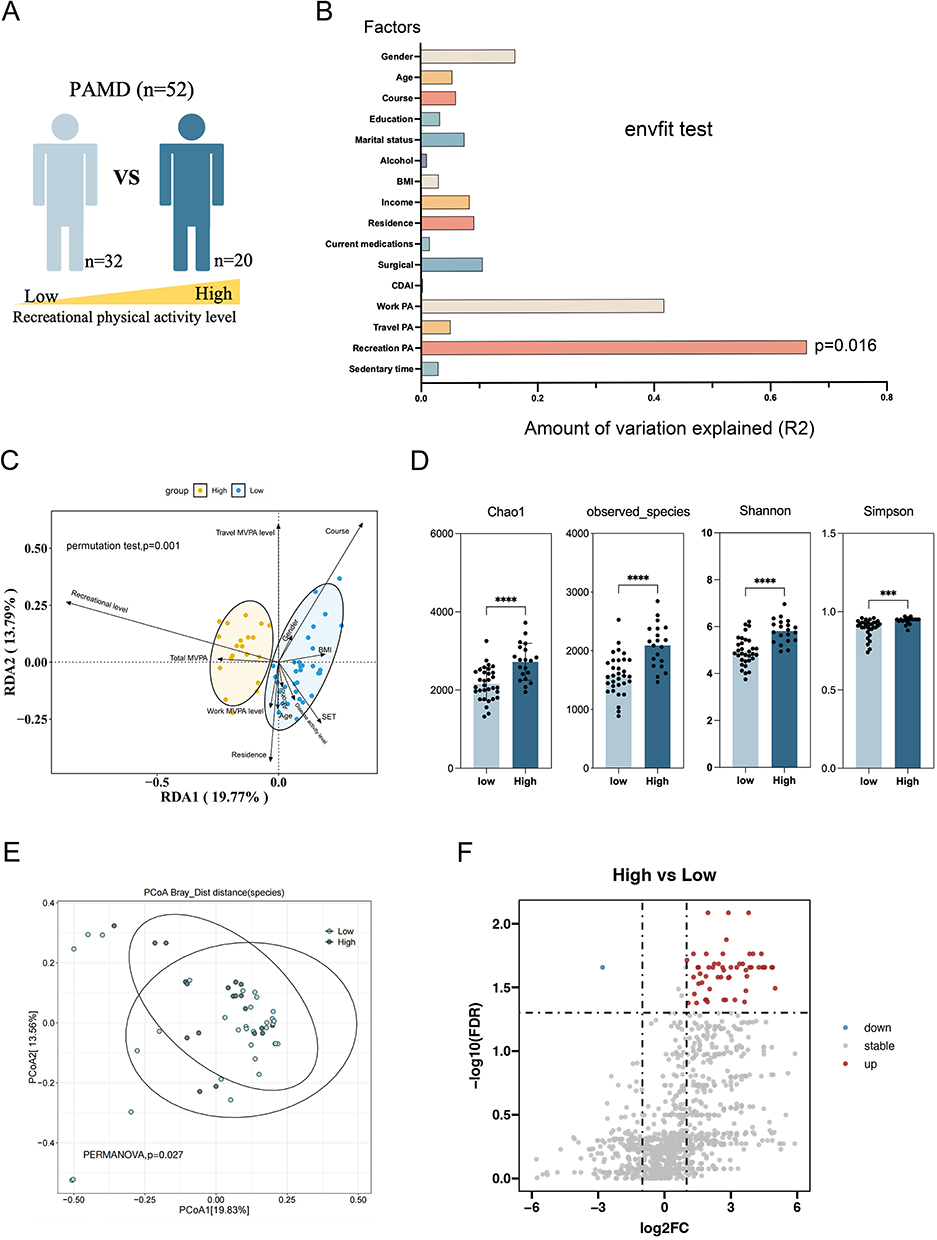 |
Figure 4 Recreational PA describes CD-related microbiome changes. (A) schematic; (B) Microbiome diversity of patients with CD explained by various factors using the envfit test. R2 represents the coefficient of determination for covariates influencing microbiome distribution. (C) Redundancy Discriminant Analysis of the effects of recreational sports activities on the figcomposition of two distinct microbial communities.; (D) Alpha diversity of gut microbiota in low and high recreation PA participants with CD; (E) Beta diversity of gut microbiota in low and high recreation PA participants with CD; (F) Volcano plot showing differential gut microbiota between low and high groups. ***P < 0.001; ****P < 0.0001. |
The individual gut microbiota varies greatly and is influenced by various clinical and environmental factors, such as disease factors, lifestyle habits, gender, dietary habits, and so on. In this study, envfit test was used to effectively determine the correlation between clinical variables and community structure. No significant microbiome differences were observed in terms of demographic characteristics (age, gender, BMI, education, marital status, and income), lifestyle factors (alcohol consumption), or disease-related factors (disease duration, medication use, and surgical history). Interestingly, gut microbiota variation was only significantly associated with recreational PA (R2 = 0.63, p = 0.016), whereas no significant associations were found with work PA, travel PA, and sedentary time (Figure 4B). This result indicated that from microbiological perspective, recreational PA had a significant effect in gut microbiome diversity.We conducted an additional analysis to examine the relationship between these clinical variables and two distinct microbial communities using Redundancy Analysis (RDA). The results of the permutation test indicated that, after adjusting for all included variables, the level of recreational PA exerted a statistically significant influence on the microbiota composition in low and high-level groups (p = 0.01) (Figure 4C).
The microbial differences among patients with CD who have different levels of recreational PA are of particular interest. The analysis of microbial diversity revealed that compared with the low-level group (n = 32), the high-level group (n = 20) exhibited a significant increase in all four alpha diversity (Figure 4D) and beta diversity (Figure 4E) metrics (all p<0.05). The volcano plot (Figure 4F) indicate that engaging in high-level recreational PA enhances microbiota diversity in patients with CD, notably by upregulating 55 bacterial species (Log2FC>1, FDR<0.05) and downregulating one bacterial species (Log2FC> −1, FDR<0.05) (Figure 4F).
Characteristics of Dominant Gut Microbiota Associated with Levels of Recreational PA
A total of 38 healthy volunteers were recruited to provide fecal samples as a control group (Figure 5A). The gut microbiota community was initially analyzed by comparing the CD and control groups. Alpha diversity (Figure 5B) was utilized to evaluate gut microbiota richness and diversity. Although the Simpson index showed no significant difference between the control and CD groups (P>0.05), the Chao1 (p<0.0001), observed_species (p<0.0001), and Shannon (p<0.001) indices were notably higher in the control group compared with the CD group. In addition, PCoA of beta diversity (Figure 5C) revealed significant differences in gut microbiota community composition between the two groups. These findings (Figure 5D) illustrates the differences in bacterial strains between the CD and control groups, with a total of 231 different bacteria (species level), including 51 increased abundance (Log2FC>1 and FDR<0.05) and 180 decreased abundance (Log2FC> −1 and FDR<0.05). These differences in bacterial strains indicate a potential association with disease.
 |
Figure 5 Microbiota-dependent effects of recreation PA on CD. (A) schematic; (B) Alpha diversity of gut microbiota in CD and control groups; (C) Beta diversity of gut microbiota in CD and control groups; (D) Volcano plot showing differential gut microbiota between CD and control groups; (E) Venn diagram comparing disease-associated microbiota with recreation PA-associated microbiota; (F) Heatmaps of 29 specific bacterial strains between low and high recreation PA participants in CD; (G) Bacteria at the species level associated with recreation PA after adjusting for other confounding factors using MaAsLin2; (H) Importance ranking of 29 bacterial strains based on random forest analysis. **P < 0.01; ****P < 0.0001. Abbreviation: ns, not significant. |
The Venn diagram (Figure 5E) shows the overlap between disease-associated and recreation PA-related bacterial strains (11.2%), with 29 strains exhibiting decreased abundance in the CD group (compared with the control group) but increased abundance in the high-level group (compared with the low-level group). This finding indicates that recreational PA may help mitigate the adverse effects of CD on the gut microbiota. The heatmap (Figure 5F) illustrates notable differences in the abundance of 29 specific bacterial strains between CD participants with low and high levels of recreational PA. A literature review revealed that most of these bacterial communities are associated with butyrate production. MaAsLin2 analysis was used to adjust for the impact of potential confounding factors on microbial abundance and confirm taxonomic differences between the low- and high-level recreational PA groups. After adjusting for demographic information of participants (age, gender, BMI, education, marital status, and income), personal lifestyle factors (alcohol consumption), disease-related variables (disease duration, medication, and surgical history), other types of PA (work and travel), and sedentary time, the effects of these 29 bacterial strains on recreational PA remained significant. Figure 5G shows the effect values of the 29 bacterial strains with significant correlations at p < 0.05 (FDR corrected). Random forests were further applied to rank the importance of the 29 bacterial strains associated with recreational PA (Figure 5H). The results indicated that according to the MeanDecreaseAccuracy algorithm, the top three bacterial strains were: Oscillospiraceae_unclassified, uncultured_Ruminococcus_sp., and Oscillospiraceae_bacterium. Using the MeanDecreaseGini algorithm, the top three bacterial strains were Oscillospiraceae_unclassified, Oscillospiraceae_bacterium, and Roseburia_intestinalis. The results of the two random forest algorithms have strong consistency, among which Oscillospiraceae was identified as the most important feature strain.
Discussion
PA is an affordable method for preventing various diseases. Most existing research on PA has been conducted with Western populations, and there is a lack of studies focusing on exercise interventions for Chinese patients with CD. Due to environmental and cultural differences, variations in preferred exercise types and the level of acceptance between Eastern and Western populations may exist. Therefore, the perspectives of Chinese patients with CD on exercise were explored in our two previous studies using social media, followed by the recruitment of patients with CD for in-depth interviews.40,41 This cross-sectional survey further quantified the correlation between PA and patient-reported outcomes, revealing an interesting finding: recreational PA, rather than work- or travel-related activity, proved beneficial for patients with CD. This indicates that recreational PA should be recommended to promote mental health.
PROMIS has evolved into a globally recognized system for measuring and reliably collecting self-reported physiological, psychological, and social health outcomes from patients.36 This study collected physical health symptoms (fatigue, sleep, pain intensity, and pain interference) and mental health symptoms (anxiety and depression) of patients with CD using PROMIS, providing a comprehensive assessment of the patient’s health status. LPA offers a classification approach based on the multiple symptoms experienced by patients. Ultimately, two categories were identified based on PROs, with approximately 84% of patients classified as the low-symptom group (class 1) and 16% as the high-symptom group (class 2). To the best of our knowledge, this is the first study to apply the LPA method to explore symptomatic heterogeneity in patients with CD. This multimorbid symptom profile (class 2) may require integrated lifestyle interventions targeting both physical and psychological domains, whereas the low-symptom group (Class 1) might benefit more from focused, single-component approaches. For instance, dietary modifications (eg, low-FODMAP diets) in CD patients with a high symptom burden may need to be combined with stress-reduction techniques (eg, mindfulness) to address pain-fatigue-anxiety interactions. Our LPA-derived classes could serve as a preliminary framework for stratifying patients in lifestyle intervention trials. Future studies should empirically test whether LPA-based subgroups influence intervention efficacy, potentially through randomized trials comparing homogeneous vs heterogeneous symptom groups in response to standardized lifestyle protocols.
The potential factors affecting heterogeneity were further explored by incorporating clinical variables based on existing literature and prior clinical experience. The possible effects of the three types of PA on PROs were examined. These findings indicate that recreational activities, rather than work and transportation, are more likely to bring beneficial changes in patients. A 10-year follow-up study42 in Denmark demonstrated that recreational PA can significantly lower the risk of major cardiovascular events, including heart attacks, strokes, and coronary heart disease mortality, as well as overall mortality rates. However, increased PA during work, such as walking, carrying, and heavy physical activities, is associated with a higher risk of major cardiovascular events and all-cause mortality. The “Physical activity paradox” is believed to arise from the fact that recreational sports typically involve dynamic exercises with varying intensity, which are effective for improving health in a short time while allowing adequate recovery. In contrast, work often involves static loads, repetitive and uncomfortable postures, and prolonged periods of non-regulated activities, with insufficient time for recovery.43 This phenomenon has also been observed in several animal models of colitis in exercise intervention studies.44,45 After 6 weeks of forced treadmill exercise, mice showed a reduced ability to resist colitis, whereas their resistance substantially improved after engaging in voluntary wheel running.44 Forced treadmill exercise is typically considered a forced and unpleasant activity, whereas voluntary wheel running is considered a form of recreational PA.
Although moderate exercise is commonly recommended to patients by healthcare providers, the exact mechanisms through which exercise affects the intestine remain unclear, making it impossible for this recommendation to evolve into an “exercise prescription.” Several omics studies investigating the mechanisms of exercise have indicated that gut microbiota may be a primary target for the effects of exercise.46 Previous PA intervention studies in patients with CD have mostly focused on outcome indicators such as body composition, disease activity, skeletal muscle changes, quality of life, and safety, with less attention paid to changes in gut microbiota.47 Our study explains the benefits of PA from a unique perspective of microorganisms. The effects of recreational PA on the symptoms of patients with CD warrant further exploration of its potential influence on the microbial community. Recreational PA was classified into two categories, and differential microbial communities at the species level, which can be considered associated with recreational PA, were explored. This conclusion remains valid even after excluding other potential confounding factors, such as age, gender, work PA, and SET. A total of 29 core bacterial strains were identified and compared with strains showing disease-related differences (patients with CD vs healthy individuals), all of which were butyrate-producing bacteria. This finding is consistent with previous evidence on exercise mechanisms. Numerous studies have suggested that exercise and the gut microbiome are interrelated, influencing metabolism and internal balance, regardless of diet.48 Animal studies and human research have demonstrated that exercise can increase the relative abundance of butyrate-producing microorganisms, increasing butyrate production.49–51 These microbiota must be verified through functional experiments, such as in vitro culture and animal models. The differences between mouse models and human CD models (such as immune mechanisms and gut microbiota composition) have not been explained, and caution should be exercised when extrapolating to clinical settings.
Beyond the direct effects of PA on the gut microbiota, psychological factors such as anxiety and depression may significantly modulate this relationship. Anxiety and depression are known to have a distinctive dysbiosis, characterized by reduced microbial diversity and depletion of butyrate-producing bacteria52—a pattern that overlaps with our observations in patients with CD. Given the high prevalence of anxiety and depression in CD (22.8–32.8%),53 it is plausible that psychological status influences both PA engagement and microbiota composition. For instance, depressive symptoms may reduce motivation for recreational PA while exacerbating stress-related physiological responses during occupational activities, potentially contributing to the observed “PA paradox”. Furthermore, the gut-brain axis could mediate bidirectional effects: recreational PA may improve mental health via butyrate-mediated anti-inflammatory mechanisms, whereas sustained PA participation may promote better mental health. Future studies should incorporate standardized psychological assessments to clarify whether the microbiota changes associated with PA are independent of or influenced by underlying anxiety or depression.
This study has several limitations. First, given its cross-sectional design, this study cannot establish a causal relationship between PA levels and patient-reported outcomes. Consequently, future longitudinal studies are needed to address this gap. Second, PA was measured using a questionnaire, which may introduce recall bias. Wearable device-based accelerometers can provide more accurate and objective measurements of PA. Third, the microbiota associated with recreational PA identified in this study still requires experimental confirmation. Fourth, the intensity and duration of other types of exercise may affect recreational PA. Therefore, based on time use epidemiology, individual 24-hour activity behavior (PA, sedentary behavior, and sleep) may be a different perspective to explain the relationship between exercise patterns and outcomes. Fifth, despite controlling for factors such as disease activity, antibiotic use, and diet when selecting participants in the microbial investigation of recreational PA, limitations such as small sample size and potential confounding factors remain. Further longitudinal and interventional studies with objective activity tracking and larger microbial datasets are warranted to substantiate and expand upon these preliminary findings.
Conclusion
In conclusion, this study provides new insights into the benefits of PA for patients with CD, particularly highlighting the significant potential of recreational PA. In addition, microbiological explanations are provided for the positive effects of recreational PA, laying the foundation for the development of “exercise prescriptions” for patients with CD.
Data Sharing Statement
All data is provided in the supplementary documents and NCBI database.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board of the First Affiliated Hospital of Zhejiang Chinese Medical University (No. 2024-KL-016-02).
Acknowledgments
The researchers would like to express their gratitude to the participants for their involvement. We also thank all developers of the R programming packages and software. We also thank the PNC China Center for authorizing the use of PRMIS-57. ©2008-2022 PROMIS Health Organization (PHO). This material can be reproduced without permission by clinicians for use with their patients. Any other use, including electronic use, requires written permission of the PHO.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the 2024 General Scientific Research Project of the Zhejiang Provincial Department of Education-Special Project for Reform of Professional Degree Graduate Training Mode (No. Y202456174).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. Crohn’s disease. Lancet. 2017;389(10080):1741–1755. doi:10.1016/s0140-6736(16)31711-1
2. Hedin CRH, Vavricka SR, Stagg AJ, et al. The Pathogenesis of Extraintestinal Manifestations: implications for IBD Research, Diagnosis, and Therapy. J Crohns Colitis. 2019;13(5):541–554. doi:10.1093/ecco-jcc/jjy191
3. Cabuk B, Gokten DB, Solakoglu TM, et al. A single-center experience: enteropathic arthritis in inflammatory bowel diseases. Egypt Rheumatologist. 2024;46(4):171–174. doi:10.1016/j.ejr.2024.07.001
4. Larsen L, Karachalia Sandri A, Fallingborg J, et al. Has the Incidence of Inflammatory Bowel Disease Peaked? Evidence From the Population-Based NorDIBD Cohort 1978-2020. Am J Gastroenterol. 2023;118(3):501–510. doi:10.14309/ajg.0000000000002187
5. Ng SC, Leung WK, Shi HY, et al. Epidemiology of Inflammatory Bowel Disease from 1981 to 2014: results from a Territory-Wide Population-Based Registry in Hong Kong. Inflamm Bowel Dis. 2016;22(8):1954–1960. doi:10.1097/mib.0000000000000846
6. Xu L, He B, Sun Y, et al. Incidence of Inflammatory Bowel Disease in Urban China: a Nationwide Population-based Study. Clin Gastroenterol Hepatol. 2023;21(13):3379–3386.e29. doi:10.1016/j.cgh.2023.08.013
7. Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2017;390(10114):2769–2778. doi:10.1016/s0140-6736(17)32448-0
8. Ananthakrishnan AN. Epidemiology and risk factors for IBD. Nat Rev Gastroenterol Hepatol. 2015;12(4):205–217. doi:10.1038/nrgastro.2015.34
9. Ma C, Jairath V, Feagan BG, et al. Interpreting modern randomized controlled trials of medical therapy in inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. 2024;21(11):792–808. doi:10.1038/s41575-024-00989-y
10. Jeong DY, Kim S, Son MJ, et al. Induction and maintenance treatment of inflammatory bowel disease: a comprehensive review. Autoimmun Rev. 2019;18(5):439–454. doi:10.1016/j.autrev.2019.03.002
11. Estevinho MM, Midya V, Cohen-Mekelburg S, et al. Emerging role of environmental pollutants in inflammatory bowel disease risk, outcomes and underlying mechanisms. Gut. 2025;74(3):477–486. doi:10.1136/gutjnl-2024-332523
12. Ananthakrishnan AN, Bernstein CN, Iliopoulos D, et al. Environmental triggers in IBD: a review of progress and evidence. Nat Rev Gastroenterol Hepatol. 2018;15(1):39–49. doi:10.1038/nrgastro.2017.136
13. Fitzpatrick JA, Melton SL, Yao CK, Gibson PR, Halmos EP. Dietary management of adults with IBD - the emerging role of dietary therapy. Nat Rev Gastroenterol Hepatol. 2022;19(10):652–669. doi:10.1038/s41575-022-00619-5
14. Lopes EW, Chan SSM, Song M, et al. Lifestyle factors for the prevention of inflammatory bowel disease. Gut. 2022. doi:10.1136/gutjnl-2022-328174
15. García-Mateo S, Martínez-Domínguez SJ, Gargallo-Puyuelo CJ, et al. Healthy Lifestyle Is a Protective Factor from Moderate and Severe Relapses and Steroid Use in Inflammatory Bowel Disease: a Prospective Cohort Study. Inflamm Bowel Dis. 2025;31(1):95–104. doi:10.1093/ibd/izae062
16. Ananthakrishnan AN, Kaplan GG, Bernstein CN, et al. Lifestyle, behaviour, and environmental modification for the management of patients with inflammatory bowel diseases: an International Organization for Study of Inflammatory Bowel Diseases consensus. Lancet Gastroenterol Hepatol. 2022;7(7):666–678. doi:10.1016/s2468-1253(22)00021-8
17. Chen J, Sun S. Unlocking the Power of Physical Activity in Inflammatory Bowel Disease: a Comprehensive Review. Gastroenterol Res Pract. 2024;2024:7138811. doi:10.1155/grp/7138811
18. Lo CH, Khalili H, Song M, et al. Healthy Lifestyle Is Associated With Reduced Mortality in Patients With Inflammatory Bowel Diseases. Clin Gastroenterol Hepatol. 2021;19(1):87–95.e4. doi:10.1016/j.cgh.2020.02.047
19. Khalili H, Ananthakrishnan AN, Konijeti GG, et al. Physical activity and risk of inflammatory bowel disease: prospective study from the Nurses’ Health Study cohorts. BMJ. 2013;347:f6633. doi:10.1136/bmj.f6633.
20. Wang Q, Xu KQ, Qin XR, Wen L, Yan L, Wang XY. Association between physical activity and inflammatory bowel disease risk: a meta-analysis. Dig Liver Dis. 2016;48(12):1425–1431. doi:10.1016/j.dld.2016.08.129
21. Robinson RJ, Krzywicki T, Almond L, et al. Effect of a low-impact exercise program on bone mineral density in Crohn’s disease: a randomized controlled trial. Gastroenterology. 1998;115(1):36–41. doi:10.1016/s0016-5085(98)70362-2
22. de Souza Tajiri GJ, de Castro CL, Zaltman C. Progressive resistance training improves muscle strength in women with inflammatory bowel disease and quadriceps weakness. J Crohns Colitis. 2014;8(12):1749–1750. doi:10.1016/j.crohns.2014.09.001
23. Loudon CP, Corroll V, Butcher J, Rawsthorne P, Bernstein CN. The effects of physical exercise on patients with Crohn’s disease. Am J Gastroenterol. 1999;94(3):697–703. doi:10.1111/j.1572-0241.1999.00939.x
24. Cronin O, Barton W, Moran C, et al. Moderate-intensity aerobic and resistance exercise is safe and favorably influences body composition in patients with quiescent Inflammatory Bowel Disease: a randomized controlled cross-over trial. BMC Gastroenterol. 2019;19(1):29. doi:10.1186/s12876-019-0952-x
25. Baldanzi G, Sayols-Baixeras S, Ekblom-Bak E, et al. Accelerometer-based physical activity is associated with the gut microbiota in 8416 individuals in SCAPIS. EBioMedicine. 2024;100:104989. doi:10.1016/j.ebiom.2024.104989
26. Boytar AN, Nitert MD, Morrision M, Skinner TL, Jenkins DG. Exercise-induced changes to the human gut microbiota and implications for colorectal cancer: a narrative review. J Physiol. 2022;600(24):5189–5201. doi:10.1113/jp283702
27. Maillard F, Vazeille E, Sauvanet P, et al. Preventive Effect of Spontaneous Physical Activity on the Gut-Adipose Tissue in a Mouse Model That Mimics Crohn’s Disease Susceptibility. Cells. 2019;8(1):33. doi:10.3390/cells8010033
28. Allesøe K, Holtermann A, Aadahl M, Thomsen JF, Hundrup YA, Søgaard K. High occupational physical activity and risk of ischaemic heart disease in women: the interplay with physical activity during leisure time. Eur J Prev Cardiol. 2015;22(12):1601–1608. doi:10.1177/2047487314554866
29. Hall C, Heck JE, Sandler DP, Ritz B, Chen H, Krause N. Occupational and leisure-time physical activity differentially predict 6-year incidence of stroke and transient ischemic attack in women. Scand J Work Environ Health. 2019;45(3):267–279. doi:10.5271/sjweh.3787
30. Piercy KL, Troiano RP, Ballard RM, et al. The Physical Activity Guidelines for Americans. JAMA. 2018;320(19):2020–2028. doi:10.1001/jama.2018.14854
31. WHO Guidelines Approved by the Guidelines Review Committee. WHO Guidelines on Physical Activity and Sedentary Behaviour. World Health Organization; 2020.
32. Harari G, Green MS, Zelber-Sagi S. Combined association of occupational and leisure-time physical activity with all-cause and coronary heart disease mortality among a cohort of men followed-up for 22 years. Occup Environ Med. 2015;72(9):617–624. doi:10.1136/oemed-2014-102613
33. Clays E, Lidegaard M, De Bacquer D, et al. The combined relationship of occupational and leisure-time physical activity with all-cause mortality among men, accounting for physical fitness. Am J Epidemiol. 2014;179(5):559–566. doi:10.1093/aje/kwt294
34. Holtermann A, Hansen JV, Burr H, Søgaard K, Sjøgaard G. The health paradox of occupational and leisure-time physical activity. Br J Sports Med. 2012;46(4):291–295. doi:10.1136/bjsm.2010.079582
35. Cella D, Choi SW, Condon DM, et al. PROMIS(®) Adult Health Profiles: efficient Short-Form Measures of Seven Health Domains. Value Health. 2019;22(5):537–544. doi:10.1016/j.jval.2019.02.004
36. Cella D, Riley W, Stone A, et al. The Patient-Reported Outcomes Measurement Information System (PROMIS) developed and tested its first wave of adult self-reported health outcome item banks: 2005-2008. J Clin Epidemiol. 2010;63(11):1179–1194. doi:10.1016/j.jclinepi.2010.04.011
37. Oberski D. Mixture Models: Latent Profile and Latent Class Analysis. Springer International Publishing; 2016.
38. Meredith W, Jacob A, Nicholas T. Personality traits are associated with the types of social support/strain: a latent profile analysis. Innovation Aging. 2024;8(Supplement_1):746.
39. Lim K, Smucny J, Barch DM, Lam M, Lee J. Cognitive Subtyping in Schizophrenia: a Latent Profile Analysis. Schizophrenia Bulletin. 2020;46(3). doi:10.1093/schbul/sbz091
40. Sun S, Chen J, Zheng M, et al. Impact of exercise on outcomes among Chinese patients with Crohn’s disease: a mixed methods study based on social media and the real world. BMC Gastroenterol. 2024;24(1):441. doi:10.1186/s12876-024-03533-z
41. Sun S, Hu Y, Li H, et al. Patients’ perspectives on, experience with and concerns about crohn’s disease: insights from Chinese social media. BMC Gastroenterol. 2023;23(1):105. doi:10.1186/s12876-023-02747-x
42. Holtermann A, Schnohr P, Nordestgaard BG, Marott JL. The physical activity paradox in cardiovascular disease and all-cause mortality: the contemporary Copenhagen General Population Study with 104 046 adults. Eur Heart J. 2021;42(15):1499–1511. doi:10.1093/eurheartj/ehab087
43. Holtermann A, Krause N, van der Beek AJ, Straker L. The physical activity paradox: six reasons why occupational physical activity (OPA) does not confer the cardiovascular health benefits that leisure time physical activity does. Br J Sports Med. 2018;52(3):149–150. doi:10.1136/bjsports-2017-097965
44. Cook MD, Martin SA, Williams C, et al. Forced treadmill exercise training exacerbates inflammation and causes mortality while voluntary wheel training is protective in a mouse model of colitis. Brain Behav Immun. 2013;33:46–56. doi:10.1016/j.bbi.2013.05.005
45. Bilski J, Mazur-Bialy AI, Brzozowski B, et al. Moderate exercise training attenuates the severity of experimental rodent colitis: the importance of crosstalk between adipose tissue and skeletal muscles. Mediators Inflamm. 2015;2015(1):605071. doi:10.1155/2015/605071
46. Dohnalová L, Lundgren P, Carty JRE, et al. A microbiome-dependent gut-brain pathway regulates motivation for exercise. Nature. 2022;612(7941):739–747. doi:10.1038/s41586-022-05525-z
47. Jones K, Kimble R, Baker K, Tew GA. Effects of structured exercise programmes on physiological and psychological outcomes in adults with inflammatory bowel disease (IBD): a systematic review and meta-analysis. PLoS One. 2022;17(12):e0278480. doi:10.1371/journal.pone.0278480
48. Mailing LJ, Allen JM, Buford TW, Fields CJ, Woods JA. Exercise and the Gut Microbiome: a Review of the Evidence, Potential Mechanisms, and Implications for Human Health. Exerc Sport Sci Rev. 2019;47(2):75–85. doi:10.1249/jes.0000000000000183
49. Vijay A, Kouraki A, Gohir S, et al. The anti-inflammatory effect of bacterial short chain fatty acids is partially mediated by endocannabinoids. Gut Microbes. 2021;13(1):1997559. doi:10.1080/19490976.2021.1997559
50. Kang SS, Jeraldo PR, Kurti A, et al. Diet and exercise orthogonally alter the gut microbiome and reveal independent associations with anxiety and cognition. Mol Neurodegener. 2014;9(1):36. doi:10.1186/1750-1326-9-36
51. Matsumoto M, Inoue R, Tsukahara T, et al. Voluntary running exercise alters microbiota composition and increases n-butyrate concentration in the rat cecum. Biosci Biotechnol Biochem. 2008;72(2):572–576. doi:10.1271/bbb.70474
52. Chin Fatt CR, Asbury S, Jha MK, et al. Leveraging the microbiome to understand clinical heterogeneity in depression: findings from the T-RAD study. Transl Psychiatry. 2023;13(1):139. doi:10.1038/s41398-023-02416-3
53. Luo K, Zhang M, Tu Q, et al. From gut inflammation to psychiatric comorbidity: mechanisms and therapies for anxiety and depression in inflammatory bowel disease. J Neuroinflam. 2025;22(1):149. doi:10.1186/s12974-025-03476-6
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Is It Important to Increase Physical Activity Among University Students During the Second-Wave COVID-19 Pandemic in Asian Countries? A Cross-Sectional Study of the Knowledge, Attitudes, and Practices in Asian Countries

Sari DK, Mani S, Fadli M, Ihksan R, Machrina Y, Arrasyid NK, Siregar KB, Sunarno A
Journal of Multidisciplinary Healthcare 2022, 15:1559-1571
Published Date: 21 July 2022
Influence of Coaching on Effectiveness, Participation, and Safety of an Exercise Program for Postmenopausal Women with Osteoporosis: A Randomized Trial
Bragonzoni L, Barone G, Benvenuti F, Ripamonti C, Lisi L, Benedetti MG, Marini S, Dallolio L, Maietta Latessa P, Zinno R, Audino G, Kemmler W, Pinelli E
Clinical Interventions in Aging 2023, 18:143-155
Published Date: 5 February 2023
An Effectiveness Trial of an Exercise Physiologist Service to Improve Quality of Life in Adults with Severe Mental Illness: Protocol for the MOVEMENT Study
Chapman JJ, Siskind D, Yung AR, Lee YY, Arnautovska U, Scott JG, Burke K, Malacova E, Korman N, Wyder M, Doohan MA, Keating SE, Parker S, Walker ME, Hu D, O’Brien J, Lau G, Pratt GF, Rosenbaum S, Curtis J, Chatterton ML, Simmons L, Wheeler AJ
Neuropsychiatric Disease and Treatment 2025, 21:1399-1408
Published Date: 11 July 2025
Exercise Attitudes Mediate the Impact of Mental Health on Physical Activity Practices Among Chinese College Students: A Cross-Sectional Study in Chongqing
Wang W, Yang H, Chen X, Ma W, Li Y, Zhang K, Yang J, Chang Q
Journal of Multidisciplinary Healthcare 2026, 19:588577
Published Date: 3 June 2026