Back to Journals » Orthopedic Research and Reviews » Volume 13
Arthroscopic Management of Meniscal Cysts: A Systematic Review
Authors Haratian A ![]() , Bolia IK
, Bolia IK ![]() , Hasan LK
, Hasan LK ![]() , Fathi A, Solaru S, Homere A, Petrigliano FA
, Fathi A, Solaru S, Homere A, Petrigliano FA ![]() , Weber AE
, Weber AE
Received 16 July 2021
Accepted for publication 6 September 2021
Published 17 September 2021 Volume 2021:13 Pages 123—139
DOI https://doi.org/10.2147/ORR.S321893
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Aryan Haratian, Ioanna K Bolia, Laith K Hasan, Amir Fathi, Samantha Solaru, Andrew Homere, Frank A Petrigliano, Alexander E Weber
USC Epstein Family Center for Sports Medicine at Keck Medicine of USC, Los Angeles, CA, USA
Correspondence: Alexander E Weber
USC Epstein Family Center for Sports Medicine at Keck Medicine of USC, 1520 San Pablo Street, Suite 2000, Los Angeles, CA, 90033, USA
Email [email protected]
Purpose: The purpose of this study was to systematically review the outcomes of arthroscopic management of meniscal cysts and to compare the results across the reported surgical techniques.
Methods: Following the PRISMA methodology, 3 databases (PubMed, Scopus and Web of Science) were searched from inception to June 2021 for randomized controlled trials (RCTs) and observational studies reporting outcomes on patients with meniscal cysts who underwent arthroscopic surgery. The Mixed Methods Appraisal Tool (MMAT) was used to evaluate the study quality.
Results: Eighteen studies examining 753 patients (761 meniscal cysts; 92.5% in the lateral meniscus) were included. Overall, 486/736 (66.0%) patients underwent purely arthroscopic decompression, 174/736 (23.6%) received arthroscopic excision, 58/736 (7.9%) received arthroscopy assisted percutaneous drainage, and 18/736 (2.4%) received a combined procedure. The recurrence rate for meniscal cysts was 7.1% across all arthroscopic procedures; 8.3%, 3.4%, and 0% for arthroscopic decompression, arthroscopic excision, and arthroscopy assisted percutaneous drainage, respectively. A total of 79.3% of patients returned to the same level of sport and 85.7% had resolution or minimal knee symptoms after arthroscopic surgery for meniscal cysts. Patient perception of surgical outcomes after any type of arthroscopic surgery for meniscal cysts was reported by 5 studies, with 189/203 (93.1%) reporting satisfaction with their surgical procedure.
Conclusion: Based on current evidence, arthroscopic management of meniscal cysts yields satisfactory patient outcomes, low cyst recurrence rates and high return to sport rates regardless of the surgical technique. Rates of cyst recurrence were relatively higher with arthroscopic decompression versus excision and percutaneous drainage; however, prospective studies using modern surgical techniques are necessary to better evaluate the surgical outcomes and to compare those with nonoperative modalities, given that a significant proportion of the included articles in this review were relatively outdated.
Level of Evidence: Systematic review of level II and IV studies.
Keywords: systematic review, meniscal cyst, arthroscopic surgery, outcomes
Introduction
Meniscal cysts, also known as parameniscal cysts, are a relatively uncommon knee pathology; the prevalence has been reported to range between 1% and 8%, with most cases diagnosed at an average age of 30–40 years.1–6 Previous history of trauma has been implicated as a potential risk factor in the development of meniscal cysts.7–9 Meniscal cysts are often asymptomatic and found incidentally on imaging but may also be associated with dull joint-line tenderness and swelling in symptomatic patients.10–12 While meniscal cysts are typically asymptomatic and may be detected as an incidental finding on imaging, they have been implicated in causing activity-related knee pain, swelling, knee locking and popping, and/or instability. Serious complications related to meniscal cysts have been reported including peroneal nerve palsy, erosion of the tibial plateau, and promotion of inappropriate osteogenesis of the lower extremity.9,11,13–22
In addition to considering presenting symptoms, physicians can often palpate meniscal cysts on exam, especially those originating in the lateral meniscus.3,4 The physical exam maneuver to differentiate meniscal cysts from other knee masses was first described by Pisani and involves the visualization of the mass, while the knee is locked in extension, with disappearance of the mass in flexion.23 While MRI remains the gold standard for diagnosis, meniscal cysts may also be diagnosed clinically when palpable or with the use of in-clinic musculoskeletal ultrasound in cases where MRI is not readily available or contraindicated.24–28
Meniscal cysts can either be treated conservatively (aspiration of the cyst through a large bore needle followed by a corticosteroid injection; ultrasound assisted percutaneous needle decompression) or with surgical excision or decompression.29–31 Open drainage with total meniscectomy was historically the preferred surgical technique for the treatment of meniscal cysts; however, this procedure has fallen out of favor with the advent of arthroscopic surgery and increased interest in meniscus preservation.12,32 Various techniques have been described in the literature for arthroscopic decompression.1,33,34 Early arthroscopic procedures primarily focused on simple evacuation of cyst contents into the joint cavity, with newer techniques exploring arthroscopic marsupialization of the cyst through creation of a channel, and incorporation of supplementary debridement of cyst cavity following evacuation.1,33,34 Percutaneous decompression using a low gauge needle is now often attempted with arthroscopic visualization, and comprises an additional method of surgical management for meniscal cysts.14,35
The purpose of this study was to systematically review the outcomes of arthroscopic management of meniscal cysts and to compare the results across the reported surgical techniques. We hypothesized that all currently used arthroscopic techniques in the management of meniscal cysts would yield relatively comparable clinical outcomes.
Methods
Search Strategy
This systematic review was performed using the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) statement as a guide.36 Medline, Scopus, and Web of Science were queried for eligible studies using the following search terms used in various combinations including: Knee meniscus cyst management; knee joint cyst arthroscopy; meniscus cyst arthroscopic surgery; meniscus cyst surgical management patient outcomes; knee joint meniscal cyst arthroscopic management outcomes; meniscal cyst arthroscopic surgical techniques; management; treatment; procedure; meniscal cyst arthroscopy, meniscal cyst patient outcomes; meniscal cyst outcomes; meniscal cyst arthroscopy pain; meniscal cyst surgery pain scores; meniscal cyst arthroscopy recurrence; meniscal cyst randomized controlled trial; meniscal cyst RCT; meniscal cyst retrospective study; meniscal cyst case series; meniscal cyst prospective study. Eligible studies consisted of peer-reviewed articles including randomized controlled trials, prospective studies, and retrospective studies. Studies not published in the English language were included only when an available copy in English was accessible. Excluded were case reports, case series with <8 participants, review articles, non-human or cadaveric studies, and non-peer reviewed articles. There was no exclusion of studies based on publication year.
Study Selection and Data Aggregation
Articles were screened by title, abstract, and full-text sequentially by two authors (IB, AH) independently according to the inclusion-exclusion criteria specified a priori. Any discrepancies in the screening process were resolved by a third co-author (AEW). The reference lists of included articles were screened by hand to ensure that no relevant article was missed during the aggregation and screening process.
Data was collected from studies included in the review into Microsoft Excel 2017 (Microsoft Corporation). The variables aggregated included study type, Level of Evidence, patient demographics (age and gender), surgical technique utilized, localization of the meniscal cysts, presence of coexisting meniscal tears and their morphologies, patient clinical outcomes, such as Lysholm scores, subjective outcome ratings, return to sport, and rates of cyst recurrence.
Quality Assessment
Two co-authors (AH and LH) independently conducted an additional quality assessment using the 2018 version of the Mixed Method Appraisal Tool (MMAT) to evaluate the appropriateness of study aim, methodology, design, data collection and analysis, and presentation of findings.37 The level of evidence included was based on the previously accepted guidelines of the American Academy of Orthopedic Surgeons (AAOS).38
Statistical Analysis
Weighted means were calculated for age and Lysholm scores when available. For all other variables including rate of cyst recurrence, frequency of meniscal tears and morphologies, subjective patient outcomes, and others, proportions were calculated using aggregated data across all studies when available for each unique variable. A meta-analysis comparing different arthroscopic techniques was attempted but was precluded due to the type and number of studies, as well as the variabilities in surgical technique observed between available studies in this review.
Results
Search Results and Quality Assessment
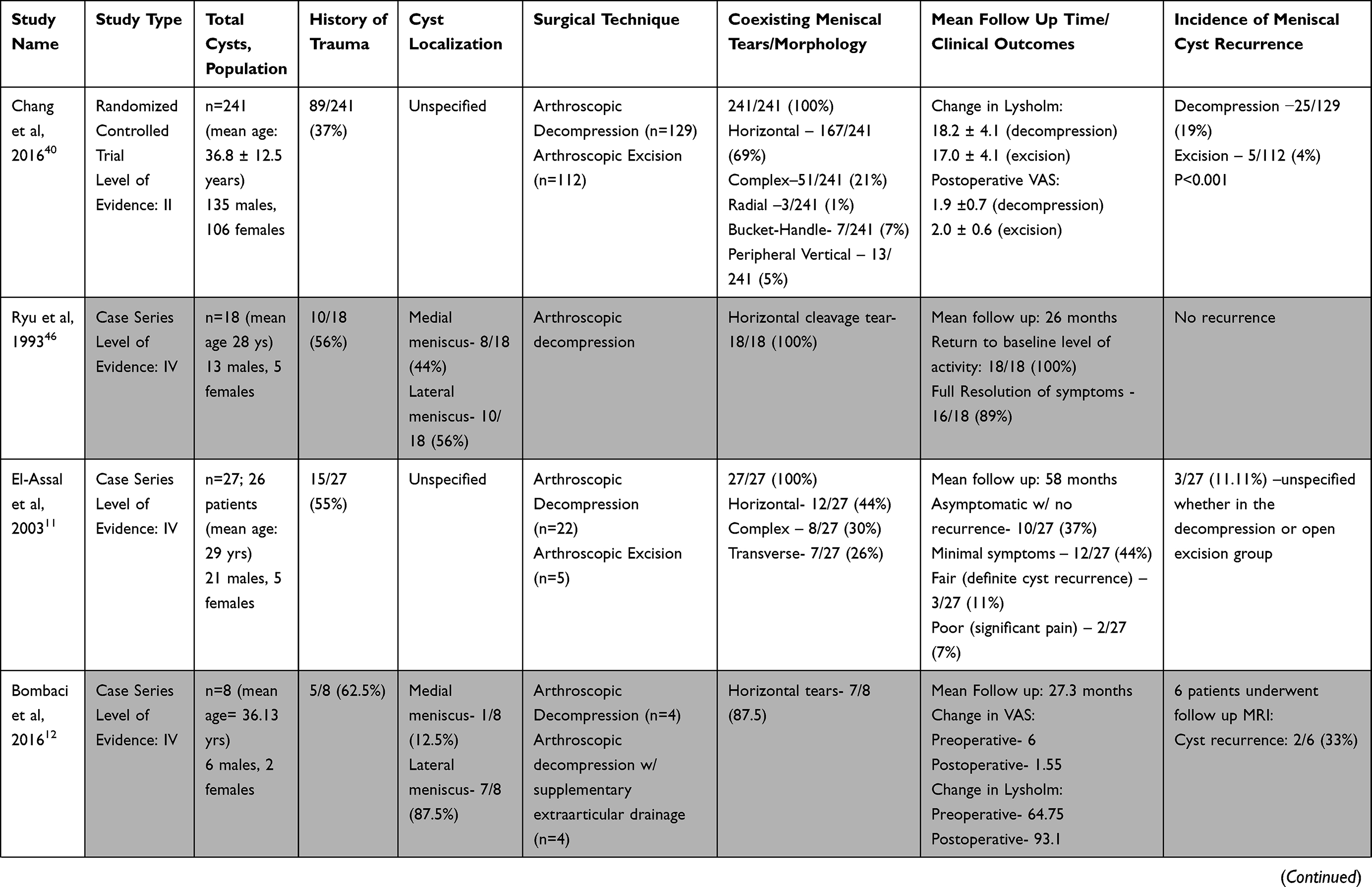
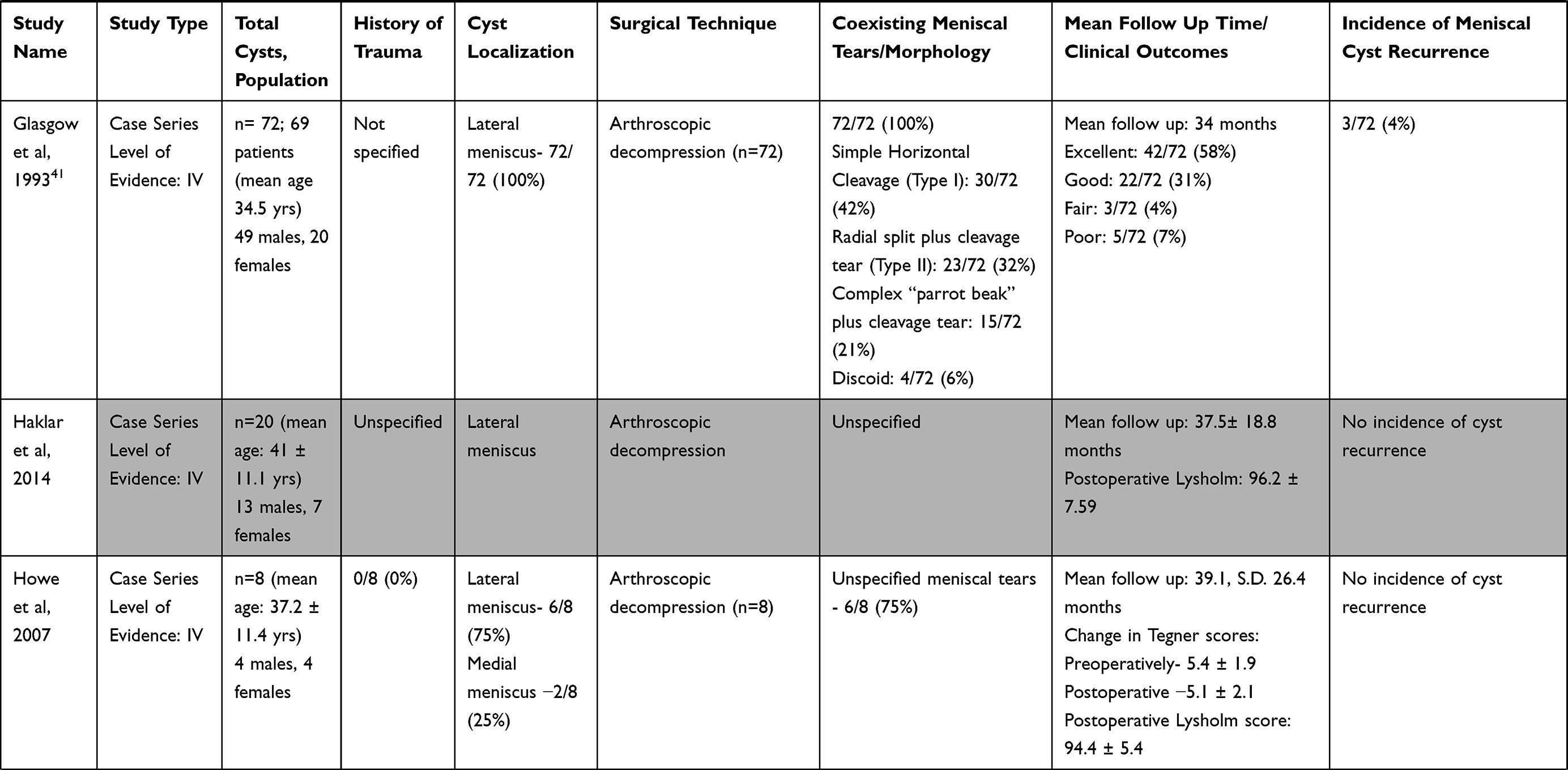
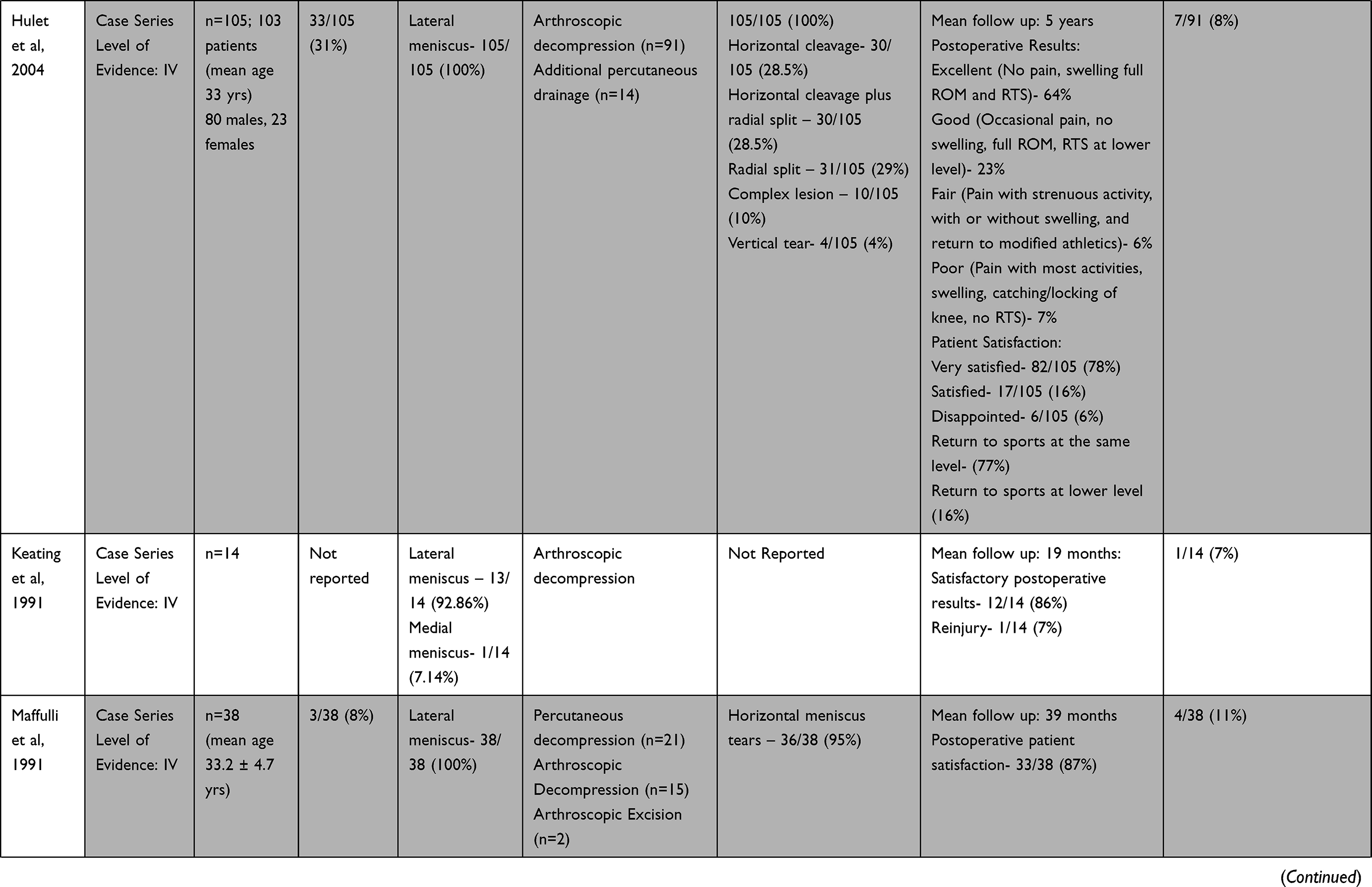
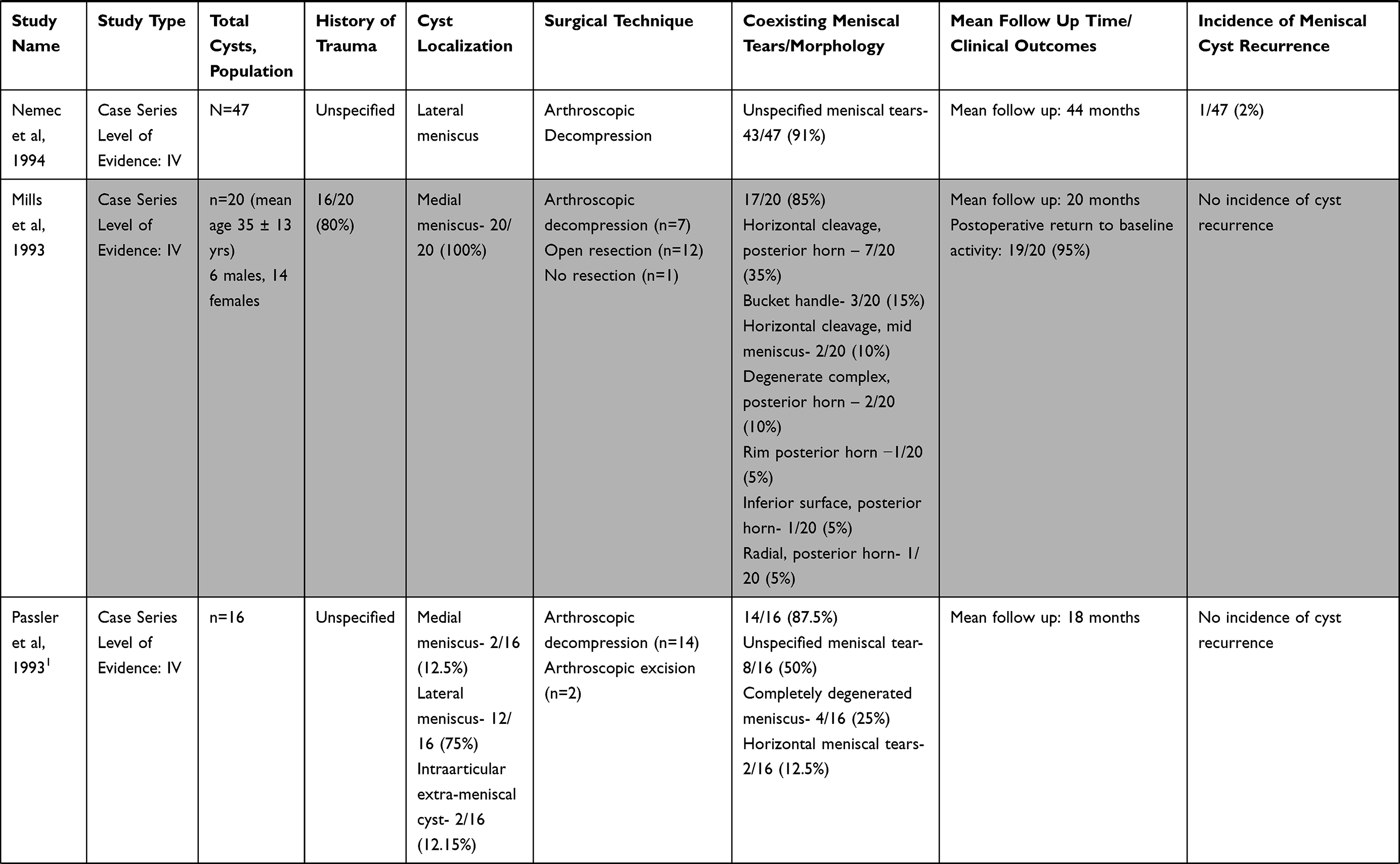
A total of 2390 potentially relevant studies were queried from the described search strategy. After the removal of duplicates, this list was consolidated into 377 reports that were then screened by title, which were consolidated into 107 abstracts, and 31 full texts that were selected for further review. Of these, a total of 18 studies met the inclusion criteria and were ultimately included in the systematic review, with 17/18 being case series and 1/18 being a randomized controlled trial (RCT). A summary of the search results and screening is provided in Figure 1. Regarding operative technique, 13/18 of the studies included utilized primarily arthroscopic decompression, 2/18 reported primarily on arthroscopic excision, 1/18 reported on both arthroscopic decompression and excision, and 2/18 reported on arthroscopy assisted percutaneous decompression. Furthermore, the meniscus was repaired and/or debrided in all the studies. The studies included are summarized in Table 1. The quality of the included studies was critically evaluated using the MMAT with calculated scores summarized in Appendix A.
 |
 |
 |
 |
 |
 |
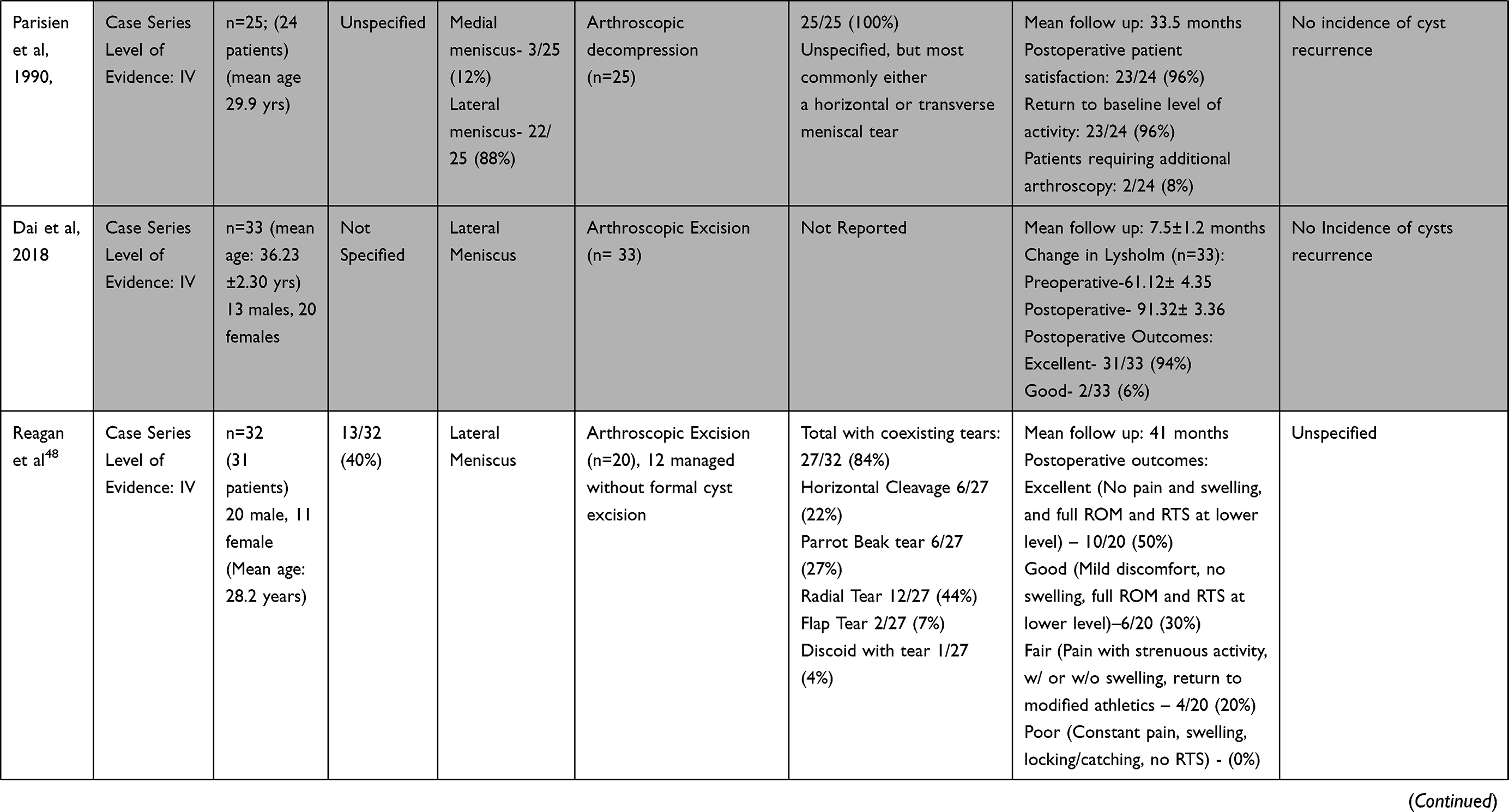
Table 1 Summary of Studies Included in Systematic Review |
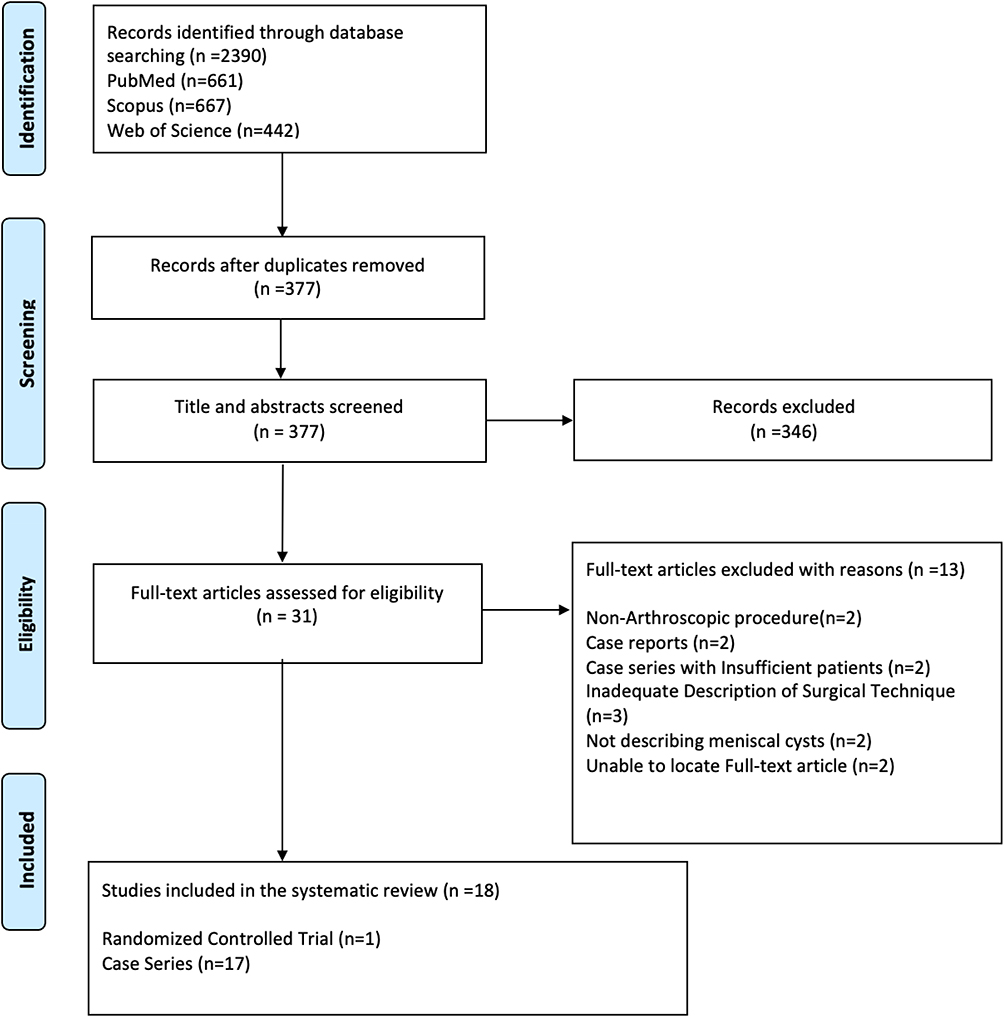 |
Figure 1 Preferred reporting items for systematic reviews and meta-analyses (PRISMA) diagram.Notes: PRISMA figure adapted from Moher D, Liberati A, Altman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Journal of clinical epidemiology. 2009;62(10). Creative Commons.36 |
Study Population, Demographics, Arthroscopic Surgical Techniques
Between the 18 studies included in this systematic review, we aggregated data on 753 patients with a total of 761 meniscal cysts collectively. Of these, 736 meniscal cysts were managed through some form of arthroscopic procedure. A total of 486/736 (66.0%) underwent purely arthroscopic decompression, 174/736 (23.6%) received arthroscopic excision, 58/736 (7.9%) received arthroscopy assisted percutaneous drainage, and 18/736 (2.4%) received a combined procedure involving arthroscopic decompression and either additional percutaneous or extraarticular drainage. In regard to demographics, the average age of patients was made available by 15/18 studies, with a calculated mean weighted age of 34.6 years, and 13/18 studies provided information regarding patient gender with 383/614 (62.4%) males and 231/614 (37.6%) females. Of the studies included, 11/18 provided data on the history of trauma to the affected knee with over a third of patients with meniscal cysts 200/534 (37.5%) having an identifiable history of trauma.
Cyst Localization and Co-Existing Meniscal Tears and Morphology
In this systematic review, a total of 16/18 studies provided the localization of the meniscal cyst with 454/491 (92.5%) occurring in the lateral meniscus and 37/491 (7.5%) occurring in the medial meniscus (Table 2). Additionally, 15/18 studies provided data as to how often meniscal tears were found to be present in patients with meniscal cysts. Between these fifteen studies, 675/694 (97.3%) meniscal cysts were accompanied with a concurrently occurring meniscal tear.Eleven studies provided additional details as to the specific morphology of the meniscal tear present, with 327/574 (57.0%) horizontal tears, 49/574 (8.5%) radial tears, 53/574 (9.2%) combinations of horizontal and radial tears, 96/574 (16.7%) complex or “parrot beak” tears, 10/574 (1.7%) “bucket-handle” tears, 7/574 (1.2%) discoid tears, and 32/574 (5.6%) that were classified as “other” for the purposes of this analysis (Figure 2). Further clarification on specific tear patterns described as “other” can be found in Table 3.
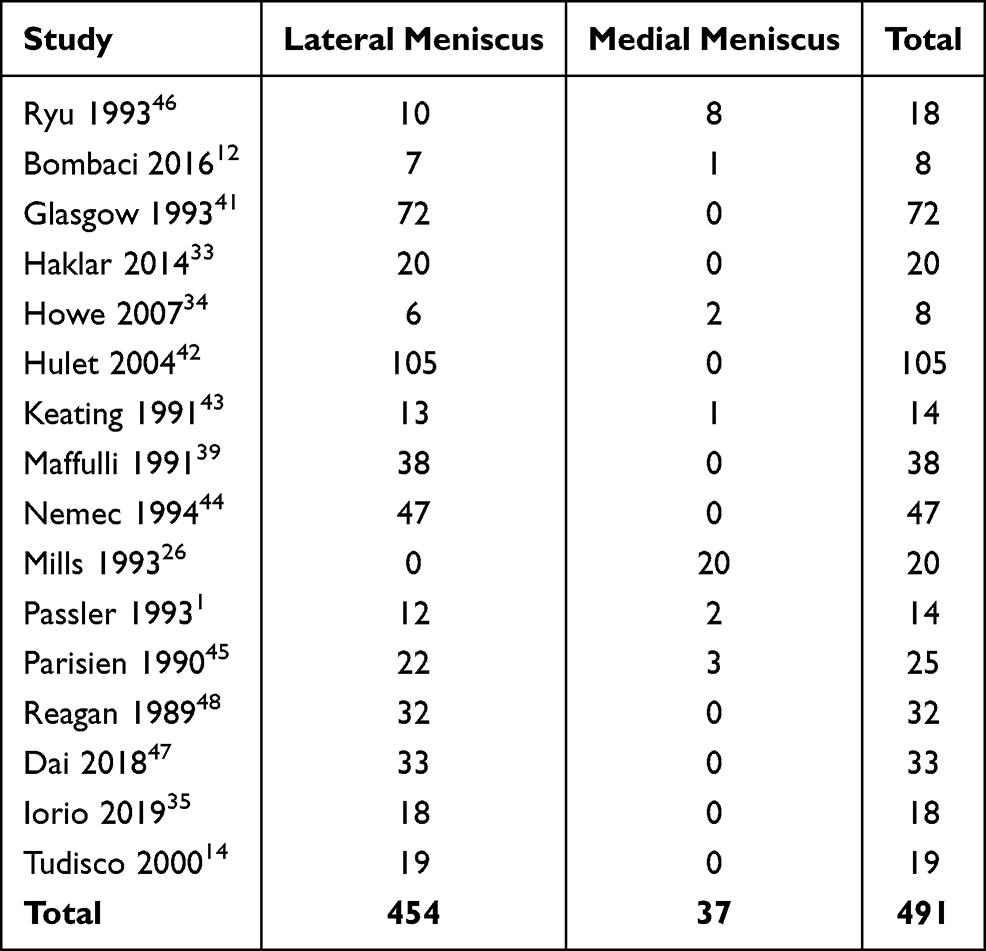 |
Table 2 Meniscal Cyst Localization |
 |
Table 3 Summary of Arthroscopic Techniques for Treatment of Meniscal Cysts |
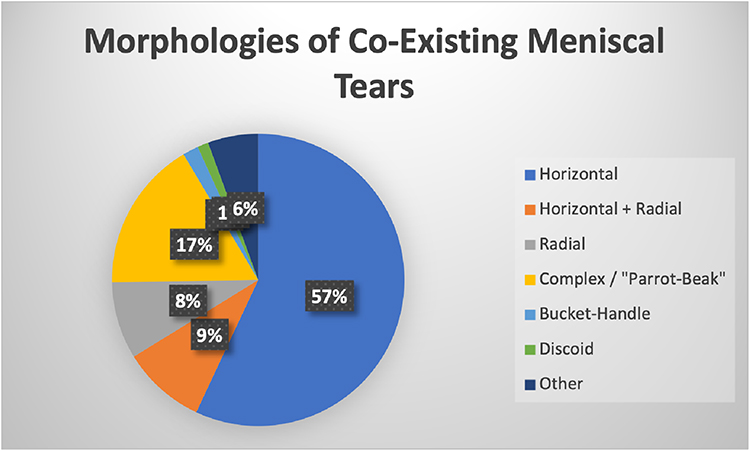 |
Figure 2 A visual representation of the distribution of morphologies of co-existing meniscal tears in patients with meniscal cysts. Horizontal tears were the most commonly seen morphology on arthroscopy, followed by Complex/“Parrot-Beak”, horizontal + radial, and radial tears. |
Rates of Cyst Recurrence
Seventeen studies reported the incidence of meniscal cyst recurrence postoperatively with a collective rate of 51/716 (7.1%) recurrences after arthroscopic management. Three studies were excluded from a sub-analysis of cyst recurrence across specific surgical technique due to the use of multiple techniques with inadequate detail regarding the rates of cyst recurrence between each of the techniques described.11,12,39 Eleven studies reported data on the rate of cyst recurrence after pure arthroscopic decompression, which was calculated to be 37/445 (8.3%) (Table 4).1,26,33,34,40–46 Similarly, 3 studies were used to calculate a recurrence rate of 5/147 (3.4%) for arthroscopic excision (Table 4).1,40,47 Only 2 studies provided insight on the rates of recurrence after arthroscopy assisted percutaneous decompression, which was calculated to be 0/37 (0%) (Table 4).14,15
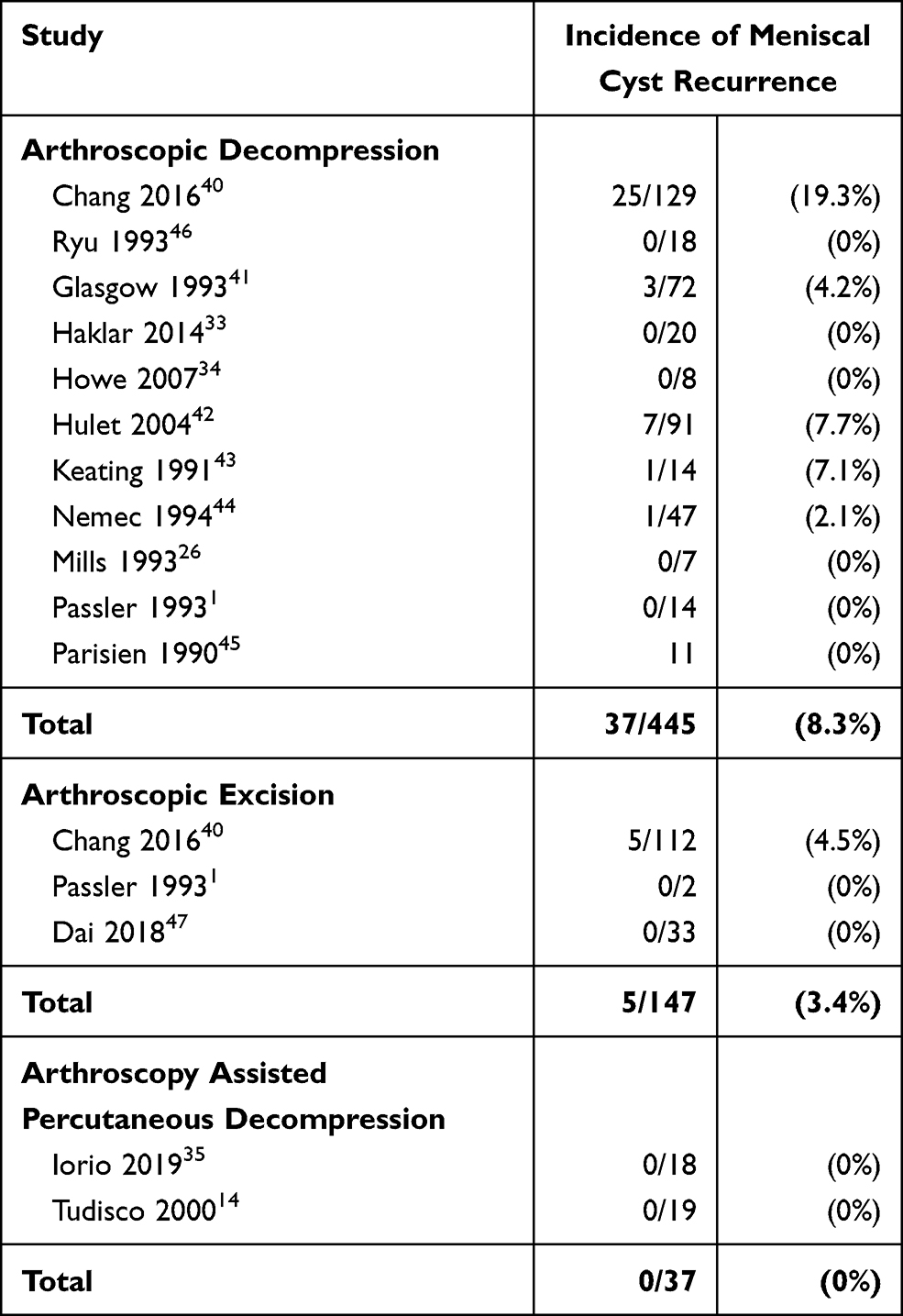 |
Table 4 Incidence of Meniscal Cyst Recurrence Across Surgical Techniques |
Patient Outcomes
A total of 5 studies reported Lysholm scores to reflect patient knee functionality postoperatively.15,33,34,40,47 Among these studies, 2/5 reported Lysholm scores for patients undergoing only arthroscopic decompression, 1/5 on those undergoing solely arthroscopic excision, 1/5 on patients undergoing arthroscopy assisted percutaneous, and 1/5 on both patients undergoing arthroscopic decompression and excision. The calculated weighted mean Lysholm score across all studies was 77.7 with mean weighted Lysholm scores for each individual technique calculated to be 76.5, 77.9, and 85 for patients undergoing arthroscopic decompression, arthroscopic excision and arthroscopy assisted percutaneous drainage, respectively. Only a single study, by Chang et al, reported a specific change in pain visual analog scale (VAS) values from preoperatively to postoperatively.40 This mean change in VAS was reported as −3.3 ± 0.7 for both patients undergoing arthroscopic decompression and those undergoing arthroscopic excision (p > 0.05).
Six studies provided subjective ratings on patient outcomes after undergoing an arthroscopic procedure.11,14,41,42,47,48 A total of 167/274 (60.9%) patients were characterized as having “excellent” results, 75/274 (27.4%) as having “good” results, 18/274 (6.6%) as having “fair” results, and 14/274 (5.1%) as having “poor” results (Figure 3A). Further stratification of subjective outcomes by surgical technique was possible in 4 studies that solely reported on a single procedure, among these, 1/4 on arthroscopic decompression, 2/4 on arthroscopic excision, and 1/4 on arthroscopy assisted percutaneous decompression. Of those undergoing purely arthroscopic decompression, 42/72 (58.3%) were classified as having “excellent outcomes, 22/72 (30.6%) with “good” outcomes, 3/72 (4.2%) with “fair outcomes, and 5/72 (6.9%) with “poor” outcomes (Figure 3B). In regard to arthroscopic excision, 41/53 (77.4%) were classified as having “excellent” outcomes, 8/53 (15.1%) with “good” outcomes, 4/53 (7.4%) with “fair outcomes, and no recorded “poor” outcomes (Figure 3B). For arthroscopy assisted percutaneous decompression, a single study reported 8/19 (42.1%) patients with “excellent” outcomes, 9/19 (47.4%) with “good” outcomes, 2/19 (10.5%) with “fair outcomes, and no reported “poor” outcomes (Figure 3B).
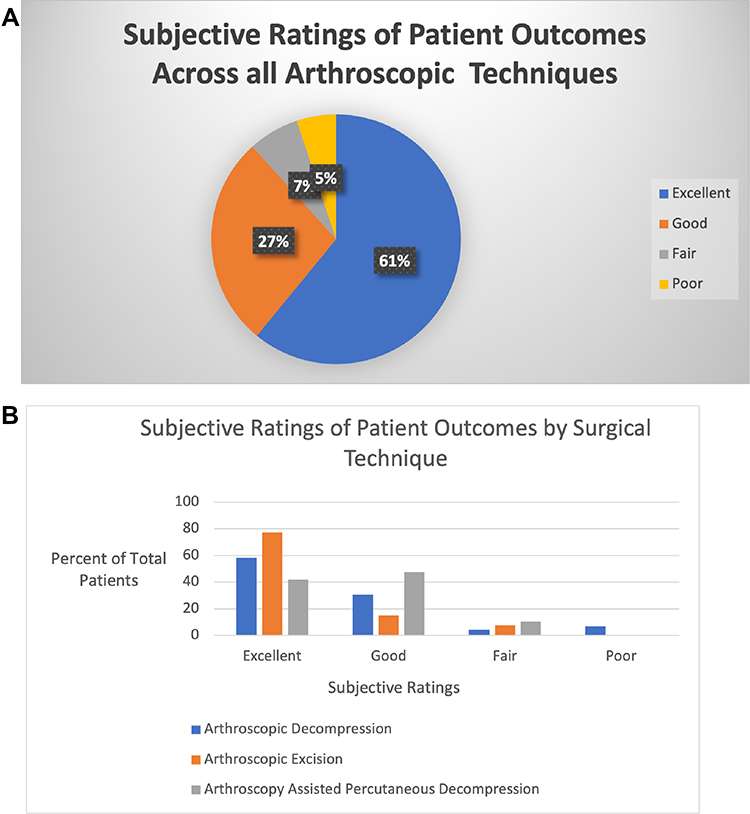 |
Figure 3 (A) Visual representation of subjective postoperative patient outcomes across all techniques in arthroscopic management of meniscal cysts. Overall, 88% of patients undergoing arthroscopic management of meniscal cysts had either “excellent” or “good” subjective results postoperatively. (B) Graphical representation of subjective postoperative patient outcomes by surgical technique after arthroscopic management of meniscal cysts reported as percent of total patients for whom subjective scores were available for each technique. |
Patient perception of surgical outcomes after any type of arthroscopic surgery for meniscal cysts was reported by 5 studies, with an average calculated satisfaction rate (patients who self-reported being either very satisfied or satisfied) of 189/203 (93.1%) across these studies.11,14,35,42,45 Extrapolation of satisfaction rate by specific procedure type was precluded in two studies where more than one surgical technique was utilized without adequate distinction of outcomes for each group.11,42 Using data from the other 3 studies, satisfaction rates for arthroscopic decompression and arthroscopy assisted percutaneous drainage were noted to be 23/24 (95.8%) and 43/48 (89.6%), respectively.
In the case of 5 studies encompassing all 3 types of arthroscopic procedures for the management of meniscal cysts, we were able to further extrapolate the data and calculated that 146/184 (79.3%) of patients were able to return to sport postoperatively at the same level as before.14,45,46,48,49 Additionally, through an analysis of 4 studies, it was calculated that 144/168 (85.7%) of patients undergoing some form of arthroscopic surgery for meniscal cysts had either resolution of or minimal knee symptoms postoperative.11,46,48,49 While some additional studies did report a return to sport rate and prevalence of postoperative knee symptoms, they were excluded if data was included on patients undergoing non-arthroscopic management of meniscal cysts without adequate distinction between the outcomes.
Discussion
The results of this systematic review demonstrated that meniscal cysts can be successfully managed arthroscopically with cyst decompression, excision, and/or percutaneous decompression with arthroscopic visualization. Overall, cyst recurrence rates among all procedures were less than 10%. Among all 3 procedures, the majority of patients (88%) subjectively had either “excellent” or “good” clinical outcomes, resolution or minor symptoms (85.7%), and were able to successfully return to sport postoperatively at the same level (79.3%). While these results are promising, it is important to note that our systematic review is limited by the relatively outdated articles and surgical methodologies, and therefore results must be taken with caution.
Various theories for the recurrence of meniscal cysts even after arthroscopic surgery have been provided including inadequate debridement, poor disruption of the “check-valve mechanism”, as well as a concomitant large meniscal tear that may hinder a surgeon’s ability to adequately debride the cyst and the connecting tract, all of which are potential pitfalls to a greater degree with arthroscopic decompression rather than excision.40,42,46,48,50 In this review, the rate of meniscal cyst recurrence was estimated to be 7.1% across all 3 arthroscopic procedures. Sub-group analysis by procedure type revealed a relatively higher rate of recurrence in those receiving arthroscopic decompression (8.3%) vs those receiving arthroscopic excision (3.4%), although it is important to note that this analysis was greatly limited by the number of studies available. Thus, the higher rates of recurrence in the arthroscopic decompression group can potentially be explained by the relatively technical difficulty involved in debridement and disruption of the “check-valve” mechanisms, whereas in arthroscopic excision the entirety of the cyst is removed without consideration of these factors. That said, this can further be influenced by the degree of surgeon expertise, and therefore explain the variations in rates of meniscal cyst recurrence observed across the studies employing arthroscopic decompression. However, without larger randomized controlled trials comparing the surgical techniques directly, it can be difficult to deduce which arthroscopic procedure is superior in preventing cyst recurrence.
More recently, a relatively small study by Kumar et al suggested promising clinical outcomes in patients receiving partial meniscectomy without overt decompression or excision of the meniscal cyst, with a mean postoperative Lysholm scores of 93.7 and 85.6 for patients with medial and lateral meniscal cysts, respectively, at final follow-up.51 In this review, the mean weighted Lysholm scores across all arthroscopic procedures were 77.7 with nearly all included data from cysts of the lateral meniscus. The greatest weight for this review’s calculated mean weighted Lysholm scores was from a single study by Chang et al, which reported Lysholm scores of 72.4 and 74 for arthroscopic decompression and excision, respectively.40 All other incorporated studies in this review had Lysholm scores of 85 or higher at the final follow-up.15,33,34,47 Thus, it is possible that patients in the included study by Chang et al had functionally lower scores preoperatively than those described by Kumar et al who received partial meniscectomy without formal decompression or removal of the cyst.40,51 This consideration could potentially explain why the mean Lysholm scores for patients undergoing arthroscopic management of meniscal cysts were lower than those purely receiving a partial meniscectomy, although whether formal management of the meniscal cyst after partial meniscectomy is necessary or not remains a topic for future studies.
In the literature, lateral meniscal cysts are much more common than those of the medial meniscus, and nearly all cysts are associated with a coexisting meniscal tear.4,5,16,50 This is consistent with the results from this systematic review with 92.5% of meniscal cysts localized to the lateral meniscus, and 7.5% were localized to the medial meniscus. Furthermore, 97.3% of meniscal cysts in this study were associated with a coexisting meniscal tear. Horizontal tears have been identified in studies as the most common morphology seen in those with meniscal cysts followed by complex and radial tears, which is in line with the results from this systematic review.3,5,52,53 Whether certain meniscal tear morphologies create a greater propensity for cyst development is still unknown and presents avenues for further research with larger and longitudinal studies that can better identify if such an association exists.
Trauma, whether induced surgically or through activity, is thought to induce both tears and degenerative changes that promote meniscal cyst formation in younger patients, while generalized meniscal degeneration over time is indicated as the likely mechanism for promoting cyst formation in the older population.7–9 This theory agrees with the results from this study, with 37.4% of patients having a history of trauma to the affected knee indicating that trauma is likely a significant risk factor for the development of meniscal cysts. There is debate as to the exact mechanism of cyst formation, with current theories suggesting either tears in the meniscus promote the influx and collection of synovial fluid or a history of repetitive trauma induces hemorrhage and degeneration, which promotes further tearing in the meniscus and creates a predisposition to cyst formation.46,48,54 While trauma was seen in a relatively large subset of patients, the majority of those with meniscal cysts included in this systematic review had no history of trauma, thus indicating that there must be other, less understood risk factors and mechanisms for the development of meniscal cysts.
Less commonly, meniscal repair has been implicated as a potential risk factor for meniscal cysts formation.55–61 Studies have correlated a higher incidence of meniscal cysts in patients, particularly in those treated with the all-inside (AI) suture technique for symptomatic meniscal tears, with prevalence as high as 29.5%; however, in these cases, the meniscal cysts that formed were often asymptomatic.6,55 None of the included studies in this review suggested previous meniscal repair. As nearly all patients included in this analysis were symptomatic, this would be consistent with the current understanding that most cysts forming after meniscal repair are asymptomatic. The relatively poor understanding of contributory factors to meniscal cyst formation suggests room for ongoing studies to better elucidate additional risk factors and alternative mechanisms for the development of meniscal cysts.
Limitations
Despite a comprehensive and systematic search of multiple databases, our study does have a few limitations worth considering. While every attempt was made to include all studies reporting on outcomes in arthroscopic management of meniscal cysts, there is a possibility that not all studies meeting this criterion were included. Additionally, nearly all the studies included in the systematic review were case series, which is not ideal. Without an adequate comparison group, it can be difficult to draw definitive conclusions on which type of arthroscopic procedure provides the most optimal patient outcomes. This, combined with the variabilities in surgical technique in each included study, precluded our ability to conduct a meta-analysis, which limits our ability to draw definitive conclusions.
Additionally, among the studies reporting on arthroscopic decompression, it is important to note that slight variations in surgical technique made it difficult to assess whether these variations in technique contributed to differences in observed outcomes between the studies. Furthermore, the majority of the patients in this review came from only a few studies, and therefore our reported analysis was, to a great extent, heavily weighted on these studies. Some of the studies included reported on more than one surgical technique and failed to distinguish between the specific procedures when reporting outcomes leading to their exclusion during our analysis of outcomes, thereby reducing this number further and thus limiting our analysis.
The majority of studies included in this systematic review were conducted over 10 years ago highlighting the need for more recent investigations. As such, a combination of older and newer operative techniques were included which created a degree of heterogeneity between the studies included in the analysis. Given that meniscal cysts are generally uncommon occurrences, especially those that are symptomatic to a degree to warrant surgical management, studies on this topic are relatively scarce. While our analysis is limited by the age of studies currently available in the literature, this study emphasizes the need for larger investigations, especially those of a comparative nature, employing current arthroscopic practices. Such studies can serve to better guide surgeons on the most optimal surgical approach that can maximize patient outcomes and reduce the risk of cyst recurrence.
Conclusion
Based on current evidence, arthroscopic management of meniscal cysts yields satisfactory patient outcomes, low cyst recurrence rates and high return to sport rates regardless of the surgical technique. Rates of cyst recurrence were relatively high with arthroscopic decompression versus excision and percutaneous drainage; however, prospective studies using modern surgical techniques are necessary to better evaluate the surgical outcomes and to compare those with nonoperative modalities, given that a significant proportion of the included articles in this review were relatively outdated.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Passler JM, Hofer HP, Peicha G, Wildburger R. Arthroscopic treatment of meniscal cysts. J Bone Joint Surg Br. 1993;75(2):303–304. doi:10.1302/0301-620X.75B2.8444954
2. Schuldt DR, Wolfe RD. Clinical and arthrographic findings in meniscal cysts. Radiology. 1980;134(1):49–52. doi:10.1148/radiology.134.1.7350634
3. De Smet AA, Graf BK, Del Rio AM. Association of parameniscal cysts with underlying meniscal tears as identified on MRI and arthroscopy. AJR Am J Roentgenol. 2011;196(2):W180–186. doi:10.2214/AJR.10.4754
4. Campbell SE, Sanders TG, Morrison WB. MR imaging of meniscal cysts: incidence, location, and clinical significance. AJR Am J Roentgenol. 2001;177(2):409–413. doi:10.2214/ajr.177.2.1770409
5. Anderson JJ, Connor GF, Helms CA. New observations on meniscal cysts. Skeletal Radiol. 2010;39(12):1187–1191. doi:10.1007/s00256-010-0993-2
6. Terai S, Hashimoto Y, Yamasaki S, Takahashi S, Shimada N, Nakamura H. Prevalence, development, and factors associated with cyst formation after meniscal repair with the all-inside suture device. Arch Orthop Trauma Surg. 2019;139(9):1261–1268. doi:10.1007/s00402-019-03176-w
7. Raine GE, Gonet LC. Cysts of the menisci of the knee. Postgrad Med J. 1972;48(555):49–51. doi:10.1136/pgmj.48.555.49
8. Decker MJ, Thorpe MS, Pavlov H, Soila K. Atypical clinical and magnetic resonance imaging manifestations of meniscal cysts. A report of two cases and review of the literature. Am J Sports Med. 1999;27(2):230–234. doi:10.1177/03635465990270021901
9. Thompson SM, Cross TM, Cross MJ, Wood DG. Medial meniscal cyst as a cause of painful erosion of the tibial plateau. Knee Surg Sports Traumatol Arthrosc. 2016;24(5):1544–1546. doi:10.1007/s00167-015-3596-6
10. Crowell MS, Westrick RB, Fogarty BT. Cysts of the lateral meniscus. Int J Sports Phys Ther. 2013;8(3):340–348.
11. El-Assal M, Mostafa M, Abdel-Aal A, El-Shafee M. Arthroscopy alone or in association with open cystectomy: in treatment of lateral meniscal cysts. Knee Surg Sports Traumatol Arthrosc. 2003;11(1):30–32. doi:10.1007/s00167-002-0321-z
12. Bombaci H, Kuyumcu M, Coskun T, Kaya E. When should the external approach be resorted to in the arthroscopic treatment of perimeniscal cyst? SICOT J. 2016;2:19. doi:10.1051/sicotj/2015046
13. Thompson AT, Gallacher PD, Rees R. Lateral meniscal cyst causing irreversible peroneal nerve palsy. J Foot Ankle Surg. 2013;52(4):505–507. doi:10.1053/j.jfas.2013.03.016
14. Tudisco C, Meo A, Blasucci C, Ippolito E. Arthroscopic treatment of lateral meniscal cysts using an outside-in technique. Am J Sports Med. 2000;28(5):683–686. doi:10.1177/03635465000280051101
15. Iorio R, Mazza D, Drogo P, et al. Lateral meniscal cysts: long-term clinical and radiological results of a partial meniscectomy and percutaneous decompressive needling. Int Orthop. 2020;44:487–493. doi:10.1007/s00264-019-04446-3
16. Herode P, Shroff A, Mandlewala V, Chaudhary A. Post-traumatic medial meniscal cyst in young: a case report. J Orthop Case Rep. 2016;6(3):7–9.
17. Niceforo A, Di Giunta AC, Caminiti S, Tirrò S. Case Report A rare case of a large lateral meniscal cyst of the knee. Arthroscopy. 1998;14(7):759–761. doi:10.1016/S0749-8063(98)70106-9
18. Enis JE, Ghandur-Mnaymneh L. Cyst of the lateral meniscus causing erosion of the tibial plateau. A case report. J Bone Joint Surg Am. 1979;61(3):441–442. doi:10.2106/00004623-197961030-00025
19. Jowett AJL, Johnston JFA, Gaillard F, Anderson SE. Lateral meniscal cyst causing common peroneal palsy. Skeletal Radiol. 2008;37(4):351–355. doi:10.1007/s00256-007-0430-3
20. Edwards MS, Hirigoyen M, Burge PD, Compression of the common peroneal nerve by a cyst of the lateral meniscus. A case report. Clin Orthop Relat Res. 1995;316:131–133. doi:10.1097/00003086-199507000-00018
21. Al-Khateeb H, Ruiz A. Lateral meniscal cyst producing lesion of the tibial plateau and literature review. Int J Surg. 2008;6(5):412–414. doi:10.1016/j.ijsu.2006.05.004
22. Mason RJ, Friedman SJ, Frassica FJ. Medial meniscal cyst of the knee simulating a solitary bone lesion. A case report and review of the literature. Clin Orthop Relat Res. 1994;304:190–194.
23. Pisani AJ. Pathognomonic sign for cyst of the knee cartilage. Arch Surg. 1947;54(2):188–190. doi:10.1001/archsurg.1947.01230070193007
24. Choi EH, Huang J, Bryk D, Bryk E. Giant medial parameniscal cyst in an osteoarthritic knee. Orthopedics. 2009;32(10):770.
25. Chen H. Diagnosis and treatment of a lateral meniscal cyst with musculoskeletal ultrasound. Case Rep Orthop. 2015;2015:432187.
26. Mills CA, Henderson IJ. Cysts of the medial meniscus. Arthroscopic diagnosis and management. J Bone Joint Surg Br. 1993;75(2):293–298. doi:10.1302/0301-620X.75B2.8444952
27. Bhatti A, Iqbal MJ. Pericruciate intra-articular lateral meniscal cyst without meniscal tear. Knee Surg Sports Traumatol Arthrosc. 2006;14(9):869–871. doi:10.1007/s00167-006-0041-x
28. Chang A. Imaging-guided treatment of meniscal cysts. HSSJ. 2009;5:58–60. doi:10.1007/s11420-008-9098-z
29. Muddu BN, Barrie JL, Morris MA. Aspiration and injection for meniscal cysts. J Bone Joint Surg Br. 1992;74(4):627–628. doi:10.1302/0301-620X.74B4.1624532
30. Macmahon PJ, Brennan DD, Duke D, Forde S, Eustace SJ. Ultrasound-guided percutaneous drainage of meniscal cysts: preliminary clinical experience. Clin Radiol. 2007;62(7):683–687. doi:10.1016/j.crad.2007.02.007
31. Mortada M, Ezzeldin N, Hammad M. AB0761 efficacy of per-cutaneous ultrasound guided drainage of degenerative meniscal cysts in knee osteoarthritis patients. Ann Rheum Dis. 2016;75:1165. doi:10.1136/annrheumdis-2016-eular.1868
32. Mazas F, de la Caffinière JY, Martin E. Cysts of the external meniscus. Rev Chir Orthop Reparatrice Appar Mot. 1976;62(7):721–729.
33. Haklar U, Ayhan E, Ustundag S, Canbora K. A new arthroscopic technique for lateral parameniscal cyst decompression. Knee. 2014;21(1):126–128. doi:10.1016/j.knee.2013.04.019
34. Howe TS, Koh JSB. Arthroscopic internal marsupialization of meniscal cysts. Knee. 2007;14(5):408–410. doi:10.1016/j.knee.2007.05.005
35. Iorio R, Mazza D, Drogo P, et al. Lateral meniscal cysts: long-term clinical and radiological results of a partial meniscectomy and percutaneous decompressive needling. Int Orthop. 2019;44:487–493. doi:10.1007/s00264-00019-04446-00263
36. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535. doi:10.1136/bmj.b2535
37. Hong QN, Gonzalez‐Reyes A, Pluye P. Improving the usefulness of a tool for appraising the quality of qualitative, quantitative and mixed methods studies, the mixed methods appraisal tool (MMAT). J Eval Clin Pract. 2018;24(3):459–467. doi:10.1111/jep.12884
38. Schmidt AH, Zhao G, Turkelson C. Levels of evidence at the AAOS meeting: can authors rate their own submissions, and do other raters agree? J Bone Joint Surg Am. 2009;91(4):867–873. doi:10.2106/JBJS.G.01233
39. Maffulli N, Petricciuolo F, Pintore E. Lateral meniscal cyst: arthroscopic management. Med Sci Sports Exerc. 1991;23(7):779–782. doi:10.1249/00005768-199107000-00002
40. Chang -J-J, Li Y-H, Lin G-M, Wu -C-C, Shen H-C, Pan R-Y. Comparison of the recurrence risk of parameniscal cysts between patients treated with arthroscopic excision and arthroscopic decompression techniques. Knee Surg Sports Traumatol Arthrosc. 2016;24(5):1547–1554. doi:10.1007/s00167-016-3998-0
41. Glasgow MM, Allen PW, Blakeway C. Arthroscopic treatment of cysts of the lateral meniscus. J Bone Joint Surg Br. 1993;75(2):299–302. doi:10.1302/0301-620X.75B2.8444953
42. Hulet C, Souquet D, Alexandre P, Locker B, Beguin J, Vielpeau C. Arthroscopic treatment of 105 lateral meniscal cysts with 5-year average follow-up. Arthroscopy. 2004;20(8):831–836. doi:10.1016/S0749-8063(04)00599-7
43. Keating JF, Muirhead A, MacMillan J, Scott PD. Arthroscopic decompression of meniscal cysts: report of 14 cases. J R Coll Surg Edinb. 1991;36(2):137–138.
44. Nemec B, Michelić R, Matovinović D, Vengust V, Kozić S. Arthroscopic treatment of lateral meniscal cyst by intraarticular dekompression. Acta Chir Orthop Traumatol Cech. 1994;61(4):205–207.
45. Parisien JS. Arthroscopic treatment of cysts of the menisci. A preliminary report. Clin Orthop Relat Res. 1990;257:154–158.
46. Ryu RK, Ting AJ. Arthroscopic treatment of meniscal cysts. Arthroscopy. 1993;9(5):591–595. doi:10.1016/S0749-8063(05)80411-6
47. Dai P-Y, Tan H-L, Yuan Y-H, Li X-Y. Arthroscopic cyst removal and wire-guided suture for the treatment of lateral meniscal cyst of knee joint. Zhongguo Gu Shang. 2018;31(10):944–948.
48. Reagan WD, McConkey JP, Loomer RL, Davidson RG. Cysts of the lateral meniscus: arthroscopy versus arthroscopy plus open cystectomy. Arthroscopy. 1989;5(4):274–281. doi:10.1016/0749-8063(89)90141-2
49. Hulet C, Schiltz D, Locker B, Beguin J, Vielpeau C. Lateral meniscal cyst. Retrospective study of 105 cysts treated with arthroscopy with 5 year follow-up. Rev Chir Orthop Reparatrice Appar Mot. 1998;84(6):531–538.
50. Seger BM, Woods GW. Arthroscopic management of lateral meniscal cysts. Am J Sports Med. 1986;14(2):105–108. doi:10.1177/036354658601400201
51. Kumar NS, Jakoi AM, Swanson CE, Tom JA. Is formal decompression necessary for parameniscal cysts associated with meniscal tears? Knee. 2014;21(2):501–503. doi:10.1016/j.knee.2013.11.015
52. Lui TH. Endoscopic resection of medial extra-articular cysts of the knee. Arthrosc Tech. 2017;6(2):e461–e466. doi:10.1016/j.eats.2016.11.001
53. Ferrer-Roca O, Vilalta C. Lesions of the meniscus. Part II: horizontal cleavages and lateral cysts. Clin Orthop Relat Res. 1980;146):301–307.
54. Lu K-H. Arthroscopic meniscal repair and needle aspiration for meniscal tear with meniscal cyst. Arthroscopy. 2006;22(12):
55. Nishino K, Hashimoto Y, Nishida Y, et al. Incidence and risk factors for meniscal cyst after meniscal repair. Arthroscopy. 2019;35(4):1222–1229. doi:10.1016/j.arthro.2018.11.039
56. Choi N-H, Kim S-J. Meniscal cyst formation after inside-out meniscal repair. Arthroscopy. 2004;20(1):E1–E3. doi:10.1016/j.arthro.2003.11.020
57. Yoo JH, Yoon J-R, Lee S-J. Parameniscal cyst formation after arthroscopic meniscal repair with biodegradable meniscal arrow: a case report. Knee Surg Sports Traumatol Arthrosc. 2008;16(9):815–817. doi:10.1007/s00167-008-0553-7
58. Kulkarni V, Mulford J. Cyst following meniscal repair. Knee Surg Sports Traumatol Arthrosc. 2012;20(11):2197–2199. doi:10.1007/s00167-011-1803-7
59. Lombardo S, Eberly V. Meniscal cyst formation after all-inside meniscal repair. Am J Sports Med. 1999;27(5):666–667. doi:10.1177/03635465990270052001
60. Nagura I, Yagi M, Kokubu T, Yoshiya S, Kurosaka M. Generation of meniscal cyst after arthroscopic meniscal repair. Arthroscopy. 2004;20(8):869–871. doi:10.1016/S0749-8063(04)00801-1
61. Kimura M, Hagiwara A, Hasegawa A. Cyst of the medial meniscus after arthroscopic meniscal repair. Am J Sports Med. 1993;21(5):755–757. doi:10.1177/036354659302100524
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.