Back to Journals » Vascular Health and Risk Management » Volume 20
Arterial Stiffness and Aortic Aneurysmal Disease – A Narrative Review
Authors Moulakakis KG ![]() , Pitros CF
, Pitros CF ![]() , Theodosopoulos IT, Mylonas SN
, Theodosopoulos IT, Mylonas SN ![]() , Kakisis JD, Manopoulos C, Kadoglou NPE
, Kakisis JD, Manopoulos C, Kadoglou NPE
Received 3 August 2023
Accepted for publication 2 February 2024
Published 14 February 2024 Volume 2024:20 Pages 47—57
DOI https://doi.org/10.2147/VHRM.S410736
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 6
Editor who approved publication: Professor Roland Asmar
Konstantinos G Moulakakis,1,* Christos F Pitros,1,* Ioannis T Theodosopoulos,2 Spyridon N Mylonas,3 John D Kakisis,2 Christos Manopoulos,4 Nikolaos PE Kadoglou5
1Department of Vascular Surgery, Patras University Hospital, University of Patras, Patras, Greece; 2Department of Vascular Surgery, “Attikon” University Hospital, School of Medicine, National and Kapodistrian University of Athens, Athens, Greece; 3Department of Vascular and Endovascular Surgery, Faculty of Medicine and University Hospital of Cologne, University of Cologne, Cologne, 50937, Germany; 4Biofluid Mechanics and Biomedical Engineering Laboratory, Fluids Section, School of Mechanical Engineering, National Technical University of Athens, Athens, Greece; 5Medical School, University of Cyprus, Nicosia, Cyprus
*These authors contributed equally to this work
Correspondence: Konstantinos G Moulakakis, Associate Professor of Vascular Surgery, Vascular Surgery Department, Patras University Hospital, Patras, Greece, Tel +0030 6937357508, Email [email protected]
Abstract: It has been documented that large-artery stiffness is independently associated with increased cardiovascular risk and may potentially lead to heart and kidney failure and cerebrovascular disease. A systematic review of studies investigating changes in arterial stiffness in patients undergoing endovascular repair of aortic disease was conducted. In addition, a review of the available literature was performed, analyzing findings from studies using the cardio-ankle vascular index (CAVI) as a marker of arterial stiffness. Overall, 26 studies were included in the present analysis. Our research revealed a high heterogeneity of included studies regarding the techniques used to assess the aortic stiffness. Aortic stiffness was assessed by pulse wave velocity (PWV), elastic modulus (Ep), and augmentation index (AI). Currently a few studies exist investigating the role of CAVI in patients having an aortic aneurysm or undergoing endovascular aortic repair. The majority of studies showed that the treatment of an abdominal aortic aneurysm (AAA) either with open repair (OR) or endovascular aortic repair (EVAR) reduces aortic compliance significantly. Whether EVAR reconstruction might contribute a higher effect on arterial stiffness compared to OR needs further focused research. An increase of arterial stiffness was uniformly observed in studies investigating patients following thoracic endovascular aortic repair (TEVAR), and the effect was more pronounced in young patients. The effects of increased arterial stiffness after EVAR and TEVAR on the heart and the central hemodynamic, and an eventual effect on cardiac systolic function, need to be further investigated and evaluated in large studies and special groups of patients.
Keywords: arterial stiffness, pulse wave velocity, PWV, cardio-ankle vascular index, CAVI, augmentation index, AI, aortic aneurysm, endovascular aortic aneurysm repair, EVAR, thoracic endovascular aortic aneurysm repair, TEVAR
Introduction
It is well known and documented that large-artery stiffness increases with age, atherosclerosis, and in certain disease states, and is independently associated with increased cardiovascular risk.1,2 Large-artery stiffening plays a significant role in hemodynamic dysfunction characterized by excess pulsatility and may potentially lead to heart and kidney failure and cerebrovascular disease.1 Moreover, guidelines from the Japanese Society of Hypertension state that an increase of pulse wave velocity (PWV) is an indicator of organ damage and could be used for further evaluation of risk assessment.2
Several methods have been suggested to assess arterial stiffness, such as pressure-strain elastic modulus (Ep), stiffness parameter (β), pulse wave velocity (PWV), and vascular compliance (Cv). PWV is regarded as the simplest and most widely applied technique.3–7 Cardio-ankle vascular index (CAVI) is a technique used to assess the PWV, based on the stiffness parameter β. CAVI reflects the stiffness of the entire aorta and leg arteries (from the ascending segment to the tibial arteries) and has the advantage of being less affected by blood pressure at the time of measurement.8 However, it was recently suggested that CAVI is still intrinsically affected by blood pressure, leading to the introduction of CAVI0. It is believed to be effective as a CAVI enhancement in improving the pressure-independent evaluation of arterial stiffness.9
In recent decades, the endovascular repair for the treatment of thoracic (TEVAR) and abdominal aortic aneurysms (EVAR) has emerged as a competitive alternative to open surgery in both acute and elective settings, and is often the approach of choice for high-risk patients.10 The currently available stent-grafts used for aortic aneurysm exclusion consist of a metallic skeleton (stainless steel, nitinol) and a fabric cover (ePTFE, polyester). Clinical studies focusing on measuring and documenting the variations in arterial stiffness in patients with thoracic or abdominal aortic aneurysms, the impact of the treatment option, as well as the association with cardiovascular outcomes and events are scarce. The aim of the present study is a systematic presentation of the currently available literature focusing on: (1) Studies assessing arterial stiffness in patients with abdominal aortic aneurysm (AAA) and the impact of treatment option on its changes; and (2) Studies assessing arterial stiffness before and after thoracic endovascular aneurysm repair (TEVAR).
Materials and Methods
Search Strategy
Studies were identified by searching electronic databases and scanning bibliographic references of articles. The National Library of Medicine’s Medline database was searched using the PubMed interface and SCOPUS from 1992 to 2023. No language constraints were used. The last search was run on July 20, 2023. Keywords were selected using medical subject headings (MeSH) for PubMed and MeSH/Emtree for Scopus. The keywords “arterial stiffness”, “pulse wave velocity”, “PWV”, and “CAVI” “cardio-ankle vascular index” were combined with “AAA”, “TAAA”, “aortic aneurysm”, “EVAR”, and “TEVAR”. The databases were searched with an unrestricted search strategy, applying exploded MeSH and keywords combined with the Boolean operators AND or OR to retrieve relevant reports as reported in Table 1. A second-level search included a manual screen of the reference lists of the articles identified through the electronic search. Eligibility assessment was performed independently in an unblinded standardized manner by 2 reviewers; disagreements between reviewers were resolved by consensus.
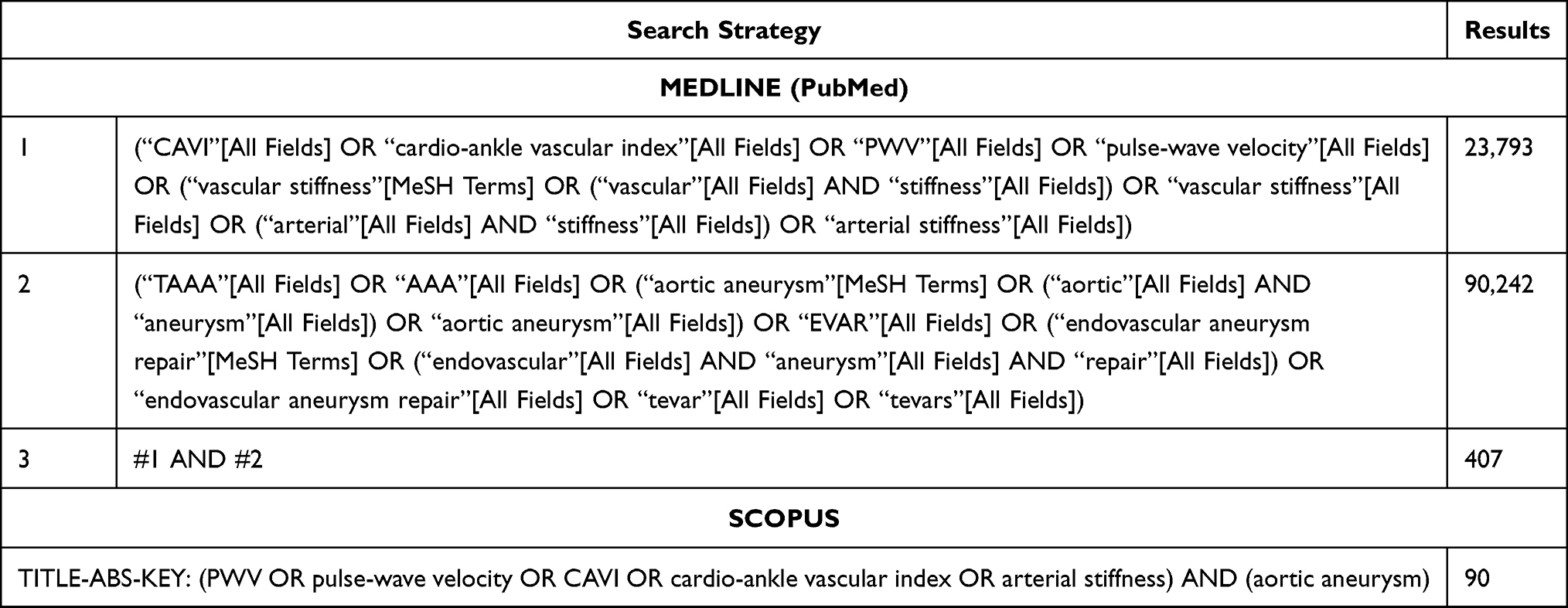 |
Table 1 Search Strategy and Medical Subject Headings (MeSH) Used for the Analysis |
Results
The search identified 431 records in total after application of the inclusion criteria and the control for duplicates. The literature search strategy is outlined in a study flow diagram (Figure 1). A total of 26 studies fulfilled the inclusion criteria. The selected studies were published between 2004 and 2023, reflecting study periods extending from 2002 to 2022.
 |
Figure 1 Study flow chart. |
Aortic stiffness was assessed by pulse wave velocity (PWV). The research revealed, however, heterogeneity among studies regarding the techniques used. Various levels of PWV measurement were used; between carotid and femoral (carotid-femoral), carotid and brachial (carotid-brachial), carotid and radial (carotid-radial), ankle and brachial (brachial-ankle), and heart central and carotid. CAVI was investigated in only a few studies in patients with an aortic aneurysm.
Studies Assessing Arterial Stiffness in Patients with AAA, Before and After Treatment
The review identified 16 studies (Table 2) reporting the influence of abdominal endografts, following EVAR, on arterial stiffness.5,11–25 Development of an aortic aneurysm could affect the arterial stiffness resulting in increased cardiovascular risk. Aykan et al investigated arterial stiffness by measuring the CAVI, in a cross-sectional study involving 59 subjects with abdominal aortic aneurysm (AAA) and 32 healthy subjects. The CAVI was significantly higher in AAA patients than in controls, positively correlated with AAA diameter, and negatively correlated with left ventricular ejection fraction.26 Moreover, in a recent original study CAVI values obtained from patients with AAA were found to be statistically higher than in control subjects (healthy adults, adjusted for age and gender).14
 |
Table 2 Studies Assessing Arterial Stiffness in Patients with AAA, Before and After Treatment |
Regarding the changes in arterial stiffness associated with AAA treatment, it has been described that EVAR is related to increased arterial stiffness as a result of the endograft implantation.5,21,22 When compared to healthy controls, patients undergoing EVAR seem to have higher measured levels of PWV5 and AI.21 Sekhri et al, in 2004, were the first to correlate endograft implantation for aortic aneurysm repair to aortic stiffness.11 In this pilot study, of a 38-patient cohort, it was shown that the treatment of the aortic aneurysm with open or endovascular technique reduces aortic compliance significantly. Also, EVAR appeared to cause significantly higher levels of elastic modulus (Ep) and aortic stiffness (β) compared to OR. Moreover, when EVAR was associated with the presence of endoleak a massive increase was reported in Ep and β, leading to the conclusion that sacs with endoleak were significantly less compliant. A few years later, in 2006, a study utilizing dynamic magnetic resonance angiography (MRA) for arterial stiffness measurement reported that the presence of an endoleak would not affect Ep or β.18 Nevertheless, these studies agreed that EVAR results in Ep and β increase at the level of the aneurysmal sac.
Increased aortic vascular stiffness after EVAR, as measured by PWV, was also reported in a 2014 study that additionally documented an induced left ventricular hypertrophy and impaired diastolic dysfunction.23 Holewijn et al highlighted the cardiovascular risk due to PWV increase after EVAR compared to baseline, which remained increased during the 1-year follow-up.15 Nevertheless, in this study, no differences in central pressure, augmentation index, or subendocardial viability ratio were reported. Furthermore, the type of the fabric cover has been found to play a role in the increase of arterial stiffness after EVAR. In a previous study at our center, polyester grafts were found to further increase PWV, when compared to PTFE grafts, and were associated to worse inflammatory response.22
Recently, PWV has been utilized to investigate its effect on sac behavior following EVAR.16,17,25 In a 2018 study of a 25-patient cohort, low preoperative PWV was associated to sac shrinkage after EVAR, whilst high postoperative PWV was an independent factor associated to sac enlargement.25 More recent studies with larger cohorts corroborate these findings, indicating that arterial stiffness is one of the key factors influencing sac behavior postoperatively16 and that PWV may be a useful tool for assessing the risk of future sac growth following EVAR.17
Another important question is whether the treatment strategy applied (EVAR vs OR) has an impact on arterial stiffness changes observed after AAA repair. In the attempt to provide an answer to this question, contradictory findings were revealed underlining the importance of the arterial stiffness measurement method applied. A recent study assessed the cardio-ankle vascular index (CAVI) before and after surgery in 110 patients undergoing EVAR and open repair. This study showed that at 48 hours postoperatively the CAVI values were increased in both groups (EVAR and OR) when compared to baseline values. At 6 months of follow-up the CAVI values returned to the baseline for the patients of the open repair group. However, in the endovascular group CAVI values remained higher when compared with the baseline values.14 Marketou et al found increased arterial stiffness (PWV) in both groups (EVAR and OR), and they also recorded a deterioration of left ventricular total longitudinal strain (GLS) which is an important diagnostic and prognostic marker of early systolic dysfunction.13 The authors concluded that AAA repair leads not only to an increase in aortic stiffness, measured by the increase in pulse wave velocity, but also to reduced cardiac systolic function.13
Further studies showed that the EVAR conferred a higher effect on arterial stiffness compared to OR. Sekhri et al found that elastic modulus (Ep) and stiffness beta were significantly higher in successful EVARs than in open repair, and sacs with endoleaks were significantly less compliant.11 Gray et al documented a significantly higher postoperative PWV measurement in EVAR patients compared to OR, posing the concern of the long-term effects on cardiovascular morbidity in patients undergoing endovascular repair.24 In addition, Lantelme et al found that the augmentation index increased after endograft implantation and decreased after graft prosthesis placement, concluding that stent-grafts (EVAR) increase reflected waves more than graft-prostheses (OR).19 Moloney et al showed in their study that, in both EVAR and OR, replacement of the aneurysmal aorta resulted in a decreased AI.20
In contrast, Valdivia et al did not find significant changes in carotid-radial pulse wave velocity (PWVCR) and central blood pressures for both EVAR and OR in the early term.12 However, they mentioned their concern regarding the use of PWVCR as a tool of arterial stiffness measuring post-AAA repair, since the site of repair was off this method’s route.
Studies Assessing Arterial Stiffness in Patients with TAA, Before and After Treatment
The review identified 10 studies (Table 3) reporting the influence of thoracic endografts, following TEVAR, on arterial stiffness.27–36 Most studies on TEVAR utilized PWV to measure arterial stiffness.27,28,30,33,35
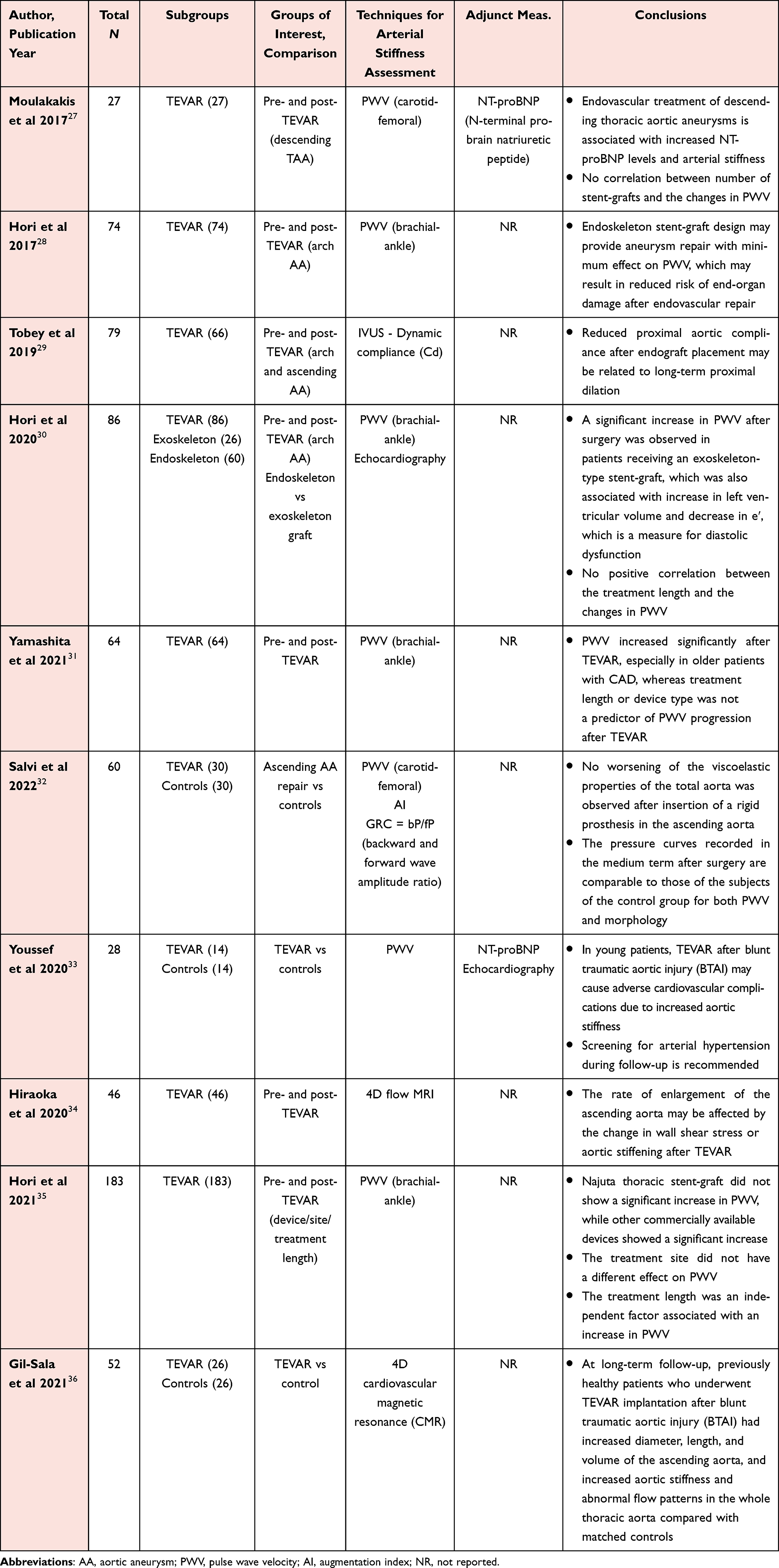 |
Table 3 Studies Assessing Aortic Stiffness in Patients with TAA, Before and After Treatment |
In 2017, PWV was used for measuring the arterial stiffness in patients following TEVAR for descending thoracic aorta disease, showing remarkable increase 6 months postoperatively.27 Hori et al suggest that endoskeleton (stents are mounted inside graft fabric) stent-graft design may allow for aneurysm repair with minimal impact on PWV, thereby reducing the risk of end-organ damage following endovascular repair.28 Adding to their suggestion, in 202030 they compared exoskeleton (metallic stents are mounted outside graft fabric) to endoskeleton endografts, highlighting that postoperatively exoskeleton endografts significantly increased PWV in patients undergoing TEVAR for aortic arch aneurysm, while patients who received an endoskeleton-type endograft experienced a significantly lower risk of cardiac and cerebrovascular events. This was also linked to changes of diastolic dysfunction markers. However, treatment length was not correlated to changes in PWV; this was found also in the Yamashita et al study.31 At this point, it should be stated that the method used by Yamashita et al was brachial-ankle PWV and thus the site of repair was off the route examined by this method. In contrast, a study has shown that, when the endograft is contained in the ascending aorta, there was no deterioration of the whole aorta’s viscoelastic characteristics.32 In addition, it was demonstrated more recently that treatment length was an independent factor related to PWV increase.35 The same study also showed that treatment site as a sole factor did not have a different effect on PWV.
Another useful tool that emerged recently is four-dimensional (4D) flow magnetic resonance imaging (MRI), utilized by two of the most recent studies on TEVAR once again proving the impact of endograft implantation on the hemodynamics of the ascending aorta.34,36 Gil-Sala et al, via their long-term follow-up (median 126 months), showed that, when compared to matched controls, previously healthy patients who received TEVAR implantation after blunt traumatic thoracic aortic injury exhibited increased ascending aortic diameter, length, and volume, as well as increased aortic stiffness and aberrant flow patterns throughout the whole thoracic aorta.36
In their study, Tobey et al pioneered the use of intravascular ultrasound (IVUS) for the measurement of aortic compliance of the ascending aorta and the aortic arch, following TEVAR, which is inextricably linked to the stiffening of the aorta. They demonstrated that thoracic aortic compliance can be properly evaluated by IVUS, and that decreased proximal aortic compliance following endograft implantation may be connected to long-term proximal dilatation.29
Since the thoracic aorta is more compliant in younger patients,29 studies speculate that young patients are more likely to be affected by the endograft implantation31 and, therefore, congestive cardiac failure and dilated cardiomyopathy post-TEVAR.37 In a recent study the role of aortic stiffening after TEVAR in young patients is pointed out and, therefore, screening for arterial hypertension during follow-up is suggested.32 Endograft placement has a known impact on heart remodeling increasing the stress that the left ventricle (LV) receives with each stroke.23,37 N-terminal pro-brain natriuretic peptide (NT-proBNP)27,33 and echocardiography23,30 are useful tools for assessing the impact of arterial stiffening on the heart.
Conclusions
Our review showed that the treatment of an abdominal aortic aneurysm either with open repair or endovascularly is associated with an increase of arterial stiffness. An increase of arterial stiffness was uniformly observed in studies investigating patients following thoracic endovascular aortic repair (TEVAR), and the effect was more pronounced in young patients. The effects of increased arterial stiffness after EVAR and TEVAR on the heart and the induced heart remodeling need to be further investigated and evaluated in large studies and special groups of patients. Assessing the association of aortic aneurysmal disease with arterial stiffness may help prevent future cardiovascular events in these patients.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Miyoshi T, Ito H. Arterial stiffness in health and disease: the role of cardio–ankle vascular index. J Cardiol. 2021;78(6):493–501. doi:10.1016/j.jjcc.2021.07.011
2. Umemura S, Arima H, Arima S, et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019). Hypertens Res. 2019;42(9):1235–1481. doi:10.1038/s41440-019-0284-9
3. O’Rourke MF, Staessen JA, Vlachopoulos C, Duprez D, Plante G. E. Clinical applications of arterial stiffness; definitions and reference values. Am J Hypertens. 2002;15(5):426–444. doi:10.1016/S0895-7061(01)02319-6
4. Tanaka H, Munakata M, Kawano Y, et al. Comparison between carotid-femoral and brachial-ankle pulse wave velocity as measures of arterial stiffness. J Hypertens. 2009;27(10):2022–2027. doi:10.1097/HJH.0b013e32832e94e7
5. Kadoglou NPE, Moulakakis KG, Papadakis I, et al. Changes in aortic pulse wave velocity of patients undergoing endovascular repair of abdominal aortic aneurysms. J Endovasc Ther. 2012;19(5):661–666. doi:10.1583/JEVT-12-3916MR.1
6. Xuereb RA, Magri CJ, Xuereb RG. Arterial Stiffness and its Impact on Cardiovascular Health. Curr Cardiol Rep. 2023;25(10):1337–1349. doi:10.1007/s11886-023-01951-1
7. Hayashi K, Yamamoto T, Takahara A, Shirai K. Clinical assessment of arterial stiffness with cardio-ankle vascular index. J Hypertens. 2015;33(9):1742–1757. doi:10.1097/HJH.0000000000000651
8. Saiki A, Sato Y, Watanabe R, et al. The role of a novel arterial stiffness parameter, cardio-ankle vascular index (CAVI), as a surrogate marker for cardiovascular diseases. J Atheroscler Thromb. 2016;23(2):155–168. doi:10.5551/jat.32797
9. Giudici A, Khir AW, Reesink KD, Delhaas T, Spronck B. Five years of cardio-ankle vascular index (CAVI) and CAVI0: how close are we to a pressure-independent index of arterial stiffness? J Hypertens. 2021;39(11):2128–2138. doi:10.1097/HJH.0000000000002928
10. Wanhainen A, Verzini F, Van Herzeele I, et al. Editor’s Choice – European Society for Vascular Surgery (ESVS) 2019 Clinical Practice Guidelines on the Management of Abdominal Aorto-iliac Artery Aneurysms. Eur J Vasc Endovasc Surg. 2019;57(1):8–93. doi:10.1016/j.ejvs.2018.09.020
11. Sekhri AR, Lees WR, Adiseshiah M. Measurement of aortic compliance in abdominal aortic aneurysms before and after open and endoluminal repair: preliminary results. J Endovasc Ther. 2004;11(4):472–482. doi:10.1583/04-1243.1
12. Valdivia AR, Fuente MF, Santos AD, et al. Impact of the Aortic Graft on Arterial Stiffness and Inflammatory Biomarkers after Endovascular Aortic Repair or Open Surgical Repair in Abdominal Aortic Aneurysm Disease. Ann Vasc Surg. 2019;59:84–90. doi:10.1016/j.avsg.2018.12.092
13. Marketou M, Papadopoulos G, Kontopodis N, et al. Early Left Ventricular Global Longitudinal Strain Deterioration After Aortic Aneurysm Repair: impact of Aortic Stiffness. J Endovasc Ther. 2021;28(2):352–359. doi:10.1177/1526602820976636
14. Mylonas SN, Moulakakis KG, Kadoglou N, et al. Arterial Stiffness Assessed by Cardio-Ankle Vascular Index in Patients With Abdominal Aortic Aneurysm and Its Alterations After Treatment. Vasc Endovascular Surg. 2021;55(8):804–810. doi:10.1177/15385744211023281
15. Holewijn S, Vermeulen JJM, van Helvert M, van de Velde L, Reijnen MMPJ. Changes in Noninvasive Arterial Stiffness and Central Blood Pressure After Endovascular Abdominal Aneurysm Repair. J Endovasc Ther. 2021;28(3):434–441. doi:10.1177/15266028211007460
16. Nishibe T, Kano M, Maekawa K, et al. Association of preoperative pulse wave velocity to aneurysm sac shrinkage after endovascular aneurysm repair. Int Angiol. 2021;40(5):409–415. doi:10.23736/S0392-9590.21.04691-5
17. Ugajin A, Iwakoshi S, Ichihashi S, et al. Prediction of Abdominal Aortic Aneurysm Growth After Endovascular Aortic Repair by Measuring Brachial-Ankle Pulse Wave Velocity. Ann Vasc Surg. 2022;81:163–170. doi:10.1016/j.avsg.2021.08.056
18. Van Herwaarden JA, Muhs BE, Vincken KL, et al. Aortic compliance following EVAR and the influence of different endografts: determination using dynamic MRA. J Endovasc Ther. 2006;13(3):406–414. doi:10.1583/06-1848.1
19. Lantelme P, Dzudie A, Milon H, et al. Effect of abdominal aortic grafts on aortic stiffness and central hemodynamics. J Hypertens. 2009;27(6):1268–1276. doi:10.1097/HJH.0b013e3283299b22
20. Moloney MA, McHugh S, O’Donnell DH, et al. Comparison of arterial stiffness and microcirculatory changes following abdominal aortic aneurysm grafting. Ir J Med Sci. 2011;180(2):375–378. doi:10.1007/s11845-010-0513-3
21. Lee CW, Sung SH, Chen CK, et al. Measures of carotid-femoral pulse wave velocity and augmentation index are not reliable in patients with abdominal aortic aneurysm. J Hypertens. 2013;31(9):1853–1860. doi:10.1097/HJH.0b013e328362360a
22. Kadoglou NPE, Moulakakis KG, Papadakis I, et al. Differential effects of Stent-graft fabrics on arterial stiffness in patients undergoing endovascular aneurysm repair. J Endovasc Ther. 2014;21(6):850–858. doi:10.1583/14-4772MR.1
23. Takeda Y, Sakata Y, Ohtani T, et al. Endovascular aortic repair increases vascular stiffness and alters cardiac structure and function. Circ J. 2014;78(2):322–328. doi:10.1253/circj.CJ-13-0877
24. Gray C, Goodman P, Badger SA, O’Malley MK, O’Donohoe MK, McDonnell CO. Endovascular aneurysm repair increases aortic arterial stiffness when compared to open repair of abdominal aortic aneurysms. Vasc Endovascular Surg. 2016;50(5):317–320. doi:10.1177/1538574416647503
25. Hori D, Nomura Y, Yamauchi T, et al. Perioperative factors associated with aneurysm sac size changes after endovascular aneurysm repair. Surg Today. 2019;49(2):130–136. doi:10.1007/s00595-018-1714-z
26. Aykan AÇ, Çetin M, Kalaycıoğlu E, Menteşe Ü. Assessment of cardio-ankle vascular index in patients with abdominal aortic aneurysm: an observational study. Vascular. 2021;29(2):190–195. doi:10.1177/1708538120946549
27. Moulakakis KG, Kadoglou NPE, Antonopoulos CN, et al. Changes in Arterial Stiffness and N-terminal pro-brain natriuretic peptide Levels after Endovascular Repair of Descending Thoracic Aorta. Ann Vasc Surg. 2017;38:220–226. doi:10.1016/j.avsg.2016.04.025
28. Hori D, Akiyoshi K, Yuri K, et al. Effect of endoskeleton stent graft design on pulse wave velocity in patients undergoing endovascular repair of the aortic arch. Gen Thorac Cardiovasc Surg. 2017;65(9):506–511. doi:10.1007/s11748-017-0787-8
29. Tobey DJ, Reynolds TS, Kopchok GE, Donayre CE, Khoynezhad A, White RA. In Vivo Assessment of Ascending and Arch Aortic Compliance. Ann Vasc Surg. 2019;57:22–28. doi:10.1016/j.avsg.2018.12.060
30. Hori D, Yuri K, Kusadokoro S, Shimizu T, Kimura N, Yamaguchi A. Effect of endoprostheses on pulse wave velocity and its long-term outcomes after thoracic endovascular aortic repair. Gen Thorac Cardiovasc Surg. 2020;68(10):1134–1141. doi:10.1007/s11748-020-01343-0
31. Yamashita Y, Oishi Y, Matsuyama S, et al. Determinants of Changes in Arterial Stiffness after Thoracic Endovascular Aortic Repair. Ann Vasc Surg. 2021;70:474–480. doi:10.1016/j.avsg.2020.06.062
32. Salvi L, Alfonsi J, Grillo A, et al. Postoperative and mid-term hemodynamic changes after replacement of the ascending aorta. J Thorac Cardiovasc Surg. 2022;163(4):1283–1292. doi:10.1016/j.jtcvs.2020.05.031
33. Youssef A, Kalaja I, Alkomi U, et al. Aortic stiffness and related complications after endovascular repair of blunt thoracic aortic injury in young patients. Vasa - Eur J Vasc Med. 2020;49(4):295–300. doi:10.1024/0301-1526/a000858
34. Hiraoka T, Komiya T, Shimamoto T. Enlargement Rate of the Ascending Aorta After Thoracic Endovascular Aortic Repair. Semin Thorac Cardiovasc Surg. 2020;32(2):211–217. doi:10.1053/j.semtcvs.2019.09.010
35. Hori D, Fujimori T, Kusadokoro S, Yamamoto T, Kimura N, Yamaguchi A. Treatment Site Does Not Affect Changes in Pulse Wave Velocity but Treatment Length and Device Selection Are Associated With Increased Pulse Wave Velocity After Thoracic Endovascular Aortic Repair. Front Physiol. 2021;12:1–11. doi:10.3389/fphys.2021.739185
36. Gil-Sala D, Guala A, Garcia Reyes ME, et al. Geometric, Biomechanic and Haemodynamic Aortic Abnormalities Assessed by 4D Flow Cardiovascular Magnetic Resonance in Patients Treated by TEVAR Following Blunt Traumatic Thoracic Aortic Injury. Eur J Vasc Endovasc Surg. 2021;62(5):797–807. doi:10.1016/j.ejvs.2021.07.016
37. Sultan S, Acharya Y, Soliman O, Parodi JC, Hynes N. TEVAR and EVAR, the unknown knowns of the cardiovascular hemodynamics; and the immediate and long-term consequences of fabric material on major adverse clinical outcome. Front Surg. 2022;9. doi:10.3389/fsurg.2022.940304
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparison of Predictive Ability of Arterial Stiffness Parameters Including Cardio-Ankle Vascular Index, Pulse Wave Velocity and Cardio-Ankle Vascular Index0
Nagayama D, Fujishiro K, Suzuki K, Shirai K
Vascular Health and Risk Management 2022, 18:735-745
Published Date: 12 September 2022