Back to Journals » Cancer Management and Research » Volume 10
Aristolochic acid containing herbs induce gender-related oncological differences in upper tract urothelial carcinoma patients
Authors Xiong G ![]() , Yao L
, Yao L ![]() , Hong P
, Hong P ![]() , Yang L
, Yang L ![]() , Ci W
, Ci W ![]() , Liu L, He Q, Gong K, Li X, Zhou L
, Liu L, He Q, Gong K, Li X, Zhou L
Received 29 June 2018
Accepted for publication 24 September 2018
Published 4 December 2018 Volume 2018:10 Pages 6627—6639
DOI https://doi.org/10.2147/CMAR.S178554
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Antonella D'Anneo
Gengyan Xiong,1,* Lin Yao,1,* Peng Hong,1,* Li Yang,2 Weimin Ci,3 Libo Liu,1 Qun He,1 Kan Gong,1 Xuesong Li,1 Liqun Zhou1
1Department of Urology, Peking University First Hospital, Institute of Urology, Peking University, National Urological Cancer Center, Beijing, China; 2Department of Nephrology, Peking University First Hospital, Beijing, China; 3Key Laboratory of Genomic and Precision Medicine, Beijing Institute of Genomics, Chinese Academy of Sciences, Beijing, China
*These authors contributed equally to this work
Background: In China, upper tract urothelial carcinoma (UTUC) is less prevalent but more malignant in males. This study investigates the prognostic factors and causes of gender-based differences in Chinese populations.
Methods: Between 1999 and 2011, 687 UTUC patients who underwent surgery were utilized for this study. We evaluated the differences in oncological characteristics, epigenetic biomarkers, cancer-specific survival (CSS), bladder recurrence (BR) rate, and contralateral upper tract recurrence (CUTR) rate. Smoking history, benzene exposure history, and the history of using aristolochic acid (AA) containing herbs were analyzed in detail.
Results: Compared with male patients, female patients showed poorer renal function, lower proportions of tumor stage III/IV, and smaller tumor diameters. The CSS in male patients was lower than that in female patients. Significant gender-related differences were observed concerning various prognostic factors. In female patients, poorer survival rates were attributed to the primary tumor location in the ureter, large diameter primary tumors, severe chronic kidney disease, papillary tumor architecture, high tumor stages, positive N status, and methylated ABCC6 promoters. In male patients, older age, ipsilateral hydronephrosis, large tumor diameters, sessile tumor architecture, high tumor stages, and methylated TMEFF2 promoters were associated with higher cancer-specific mortality. AA might be the main cause of these gender-based differences. The AA-induced UTUC patients presented smaller tumor diameters, lower tumor stages, fewer positive N statuses, more multifocal tumors, lower methylation indices, and poorer renal function. Although AA-induced UTUC patients exhibited better survival rates, BR and CUTR rates were significantly worse.
Conclusion: In China, there exist significant AA-induced differences between male and female UTUC patients. The bladders and contralateral upper urinary tracts of AA-induced UTUC patients should be carefully monitored after surgery.
Keywords: upper tract urothelial carcinoma, aristolochic acid, gender difference, oncological outcomes, China
Background
Upper tract urothelial carcinoma (UTUC) is a malignant tumor differentiated from ureteral and renal pelvis urothelial epithelial tissue. UTUCs account for 5%–10% of all urothelial carcinomas and approximately 10% of renal tumors within the USA.1,2 However, it has been noted that UTUC has a lower incidence in females than in males. A higher proportion of female UTUC patients in Western populations have higher tumor stages, higher tumor grades, and lymph node metastasis (LNM) than males.3,4 The effect of gender on oncological outcomes of UTUC has long been disputed and is not considered as an independent prognostic factor that influences tumor-specific mortality in Western populations.3–5
However, in our previous studies, the incidence, oncological characteristics, chronic kidney disease (CKD) prevalence, epigenetic biomarkers, and outcomes of tumor were different in Chinese populations.6–10 Gender was a factor that indicated a significant difference. Unlike Western populations where the male-to-female ratio of UTUC patients is approximately 3:1, Chinese female UTUCs have a higher prevalence than males – though they are less likely to develop worse histology outcomes (at higher stages and LNM).5 Furthermore, being male is considered a significant prognostic factor for poorer survival.7
No study has investigated this gender phenomenon in Chinese vs Caucasian UTUC patients. We performed this study to assess the differences in oncological characteristics, epigenetic biomarkers, cancer-specific survival (CSS), and bladder recurrence (BR) predictors between Chinese men and women and further investigated the possible cause of gender differences in Chinese UTUC patients.
Methods
Patient population
In this study, we obtained data from patients (N=687) pathologically diagnosed with UTUC who underwent surgery at Peking University First Hospital (Beijing, China) between August 1, 1999, to December 31, 2011. The Institutional Ethics Committee of Peking University First Hospital approved the study. All patients had signed consent forms before discharge to authorize the future analysis of their medical records.
Procedure
Radical nephroureterectomy or partial ureterectomy (for solitary kidney patients or CKD stage IV–V patients) procedures were performed on all members of the study population. When radiographies were atypical, ureteroscopies with tumor biopsies were performed to determine appropriate treatment strategies. Ipsilateral hydronephroses were determined by urinary ultrasound, magnetic resonance imaging (MRI), or computed tomography (CT) before surgery. All blood samples were collected before surgery, and estimated glomerular filtration rate (eGFR) was calculated with a re-expressed Modification of Diet in Renal Disease formula for the Chinese population.11 Tumor stages were assessed according to the UICC TNM 2002 classification of malignant tumors.12 Tumor grades were assessed according to the 1973 classification from the WHO.13 Tumor structures were defined as papillary or sessile. Our previous study detected 10 genes (ABCC6, BRCA1, CDH1, GDF15, HSPA2, RASSF1A, SALL3, THBS1, TMEFF2, and VIM) and found that gene methylation status was related to the prognoses of UTUC patients.7 Our previous study also described the methylation status detection method of 10 gene promoters.7 These genes were also included within the present study. For the followed-up patients, routine urinalyses, ultrasonographies, MRI/CT, chest X-rays, urine cytologies (or urine fluorescence in situ hybridization), and cystoscopies were performed every 3 months in the first 2 years and once a year after 2 years. As for AA-containing herbs history, we made a list of AA-containing herbs and inquired whether these AA-containing herbs were taken one by one. AA-containing herbs included Long Dan Xie Gan mixture, Guan Xin Su mixture, Ba Zheng He mixture, Pai Shi mixture, Dao Chi mixture, Fu Ke Fen Qing mixture, and so on. Furthermore, we also inquired the time and frequency for using AA-containing herbs. We also asked patients about the types of traditional Chinese medicine (TCM) used for long periods of time and wrote down the name of the said TCM.
Statistical analysis
Patients were divided into two groups according to gender. Differences between the two groups were analyzed by the Mann–Whitney U test for nonstandard, normally distributed continuous variables and grade variables, as well as the chi-squared test for categorical variables. Univariable log-rank tests and multivariable Cox regressions were conducted to evaluate the prognostic significance of each variable with respect to CSS, BR, and contralateral upper tract recurrence (CUTR). A predictive model (nomogram) for CSS was built for each gender using statistical software R (The R Foundation for Statistical Computing, Bell Laboratories, NY, USA). Other statistical tests were performed using SPSS 21.0 software (IBM Corp., Armonk, NY, USA). A P-value <0.05 was considered significant.
Results
A total of 687 patients pathologically diagnosed with UTUC were enrolled in our study. The majority of patients were female (55.5%). When patients were grouped according to gender, several significant differences emerged (Table 1). There were fewer smokers (5% vs 34%, P<0.001) and more aristolochic acid (AA) herb users (14% vs 6%, P<0.001) within the female cohort. Moreover, in contrast to Western populations, the Chinese female UTUC patients showed a lower proportion of individuals with pT3/pT4 (27% vs 37%, P=0.006). Further, when compared with the male UTUC patients, the female cohort had smaller tumor diameters (3.2±0.1 vs 3.7±0.1 cm, P=0.005). The female group also had poorer renal function when juxtaposed to the male group (a relatively high severe CKD proportion was observed, 16% vs 8%, P=0.003). Finally, the percentages of methylation of the ABCC6 (17% vs 11%, P=0.034) and BRCA1 (21% vs 13%, P=0.008) gene promoters were higher in the female cohort.
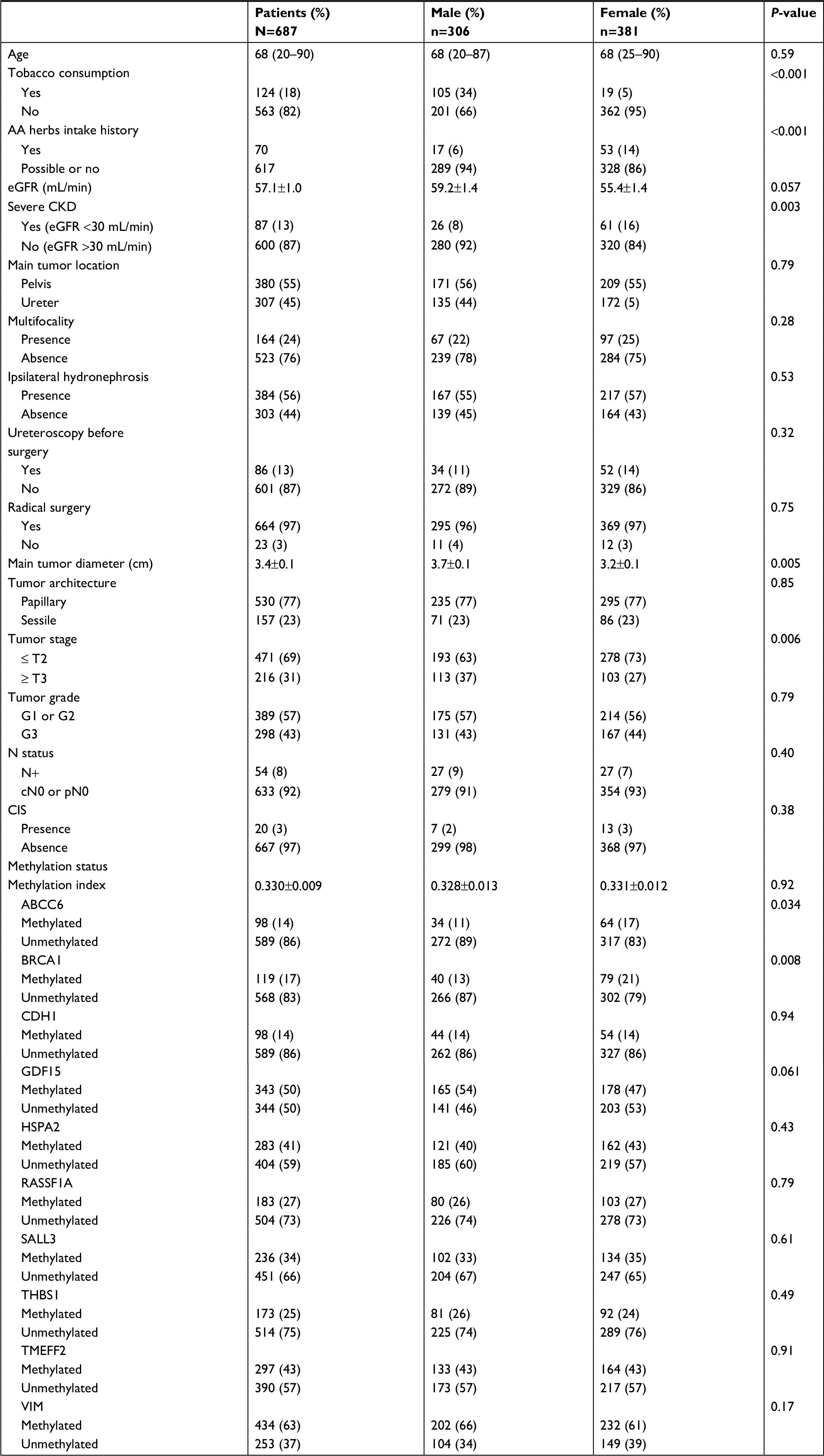 | Table 1 Patients characteristics Abbreviations: AA, aristolochic acid; CIS, carcinoma in situ; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate; cN0, clinical N0; pN0, pathological N0. |
There were significant gender differences observed in the oncological outcomes for our study population. For the female patients, 100 patients (26.2%) died from UTUC (the median follow-up time, 64 months, range: 3–150), and 123 patients (32.3%) developed BR after surgery (the median follow-up time, 52 months, range: 2–139). For the male patients, 125 patients (40.8%) died from UTUC (the median follow-up time, 66 months, range: 4–144), while 105 patients (34.3%) developed BR (the median follow-up time, 47 months, range: 2–144). Although no significant difference was observed in BR (P=0.27), the CSS in the male group was much poorer than that of the female group (HR=1.71, P<0.001) (Figure 1A).
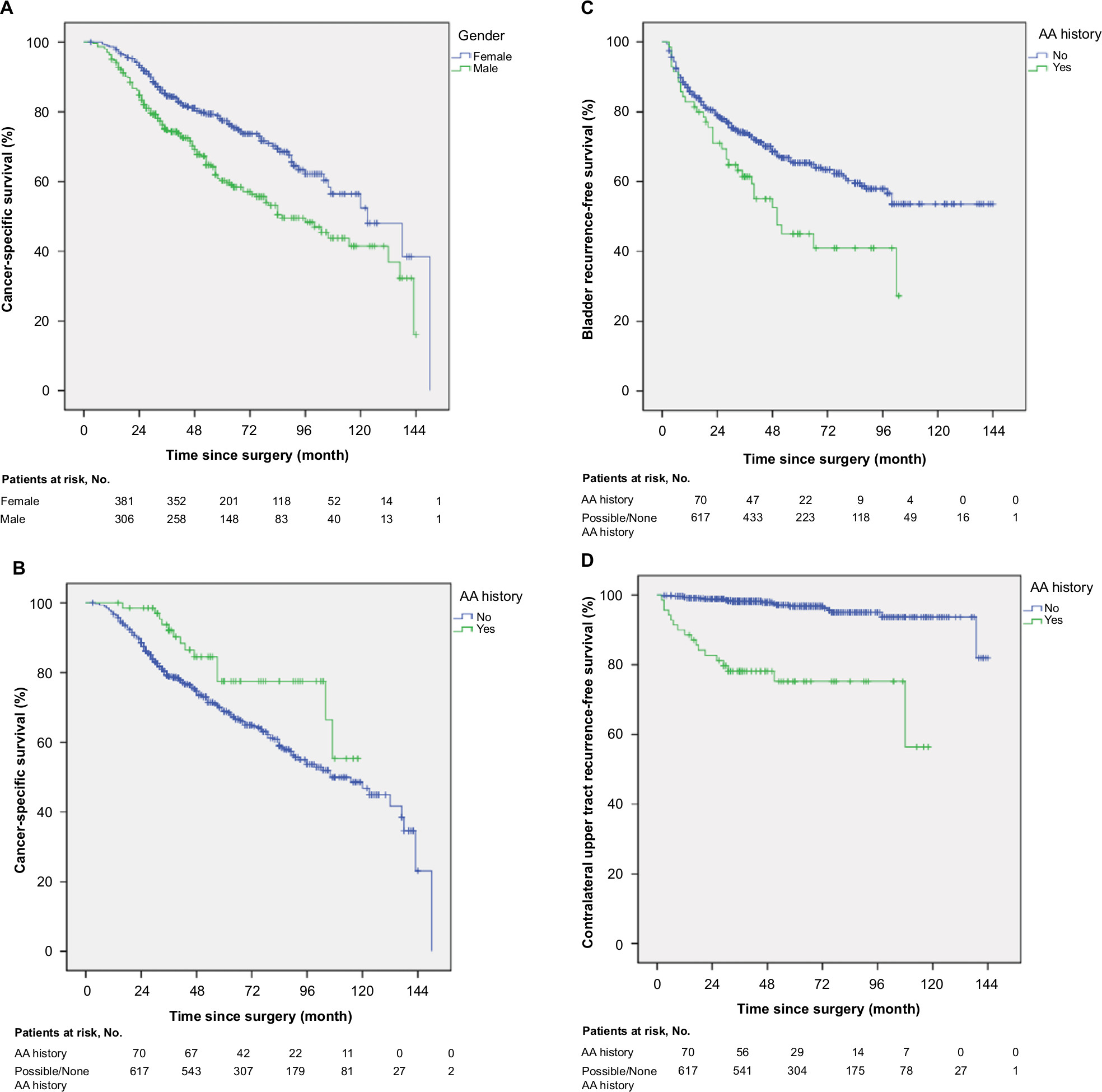 | Figure 1 (A) Estimated Kaplan–Meier curve representing cancer-specific survival stratified by gender (P<0.001). Estimated Kaplan–Meier curve representing (B) cancer-specific survival (P=0.023), (C) bladder recurrence-free survival (P=0.005), and (D) contralateral upper tract recurrence-free survival (P<0.001) stratified by AA history. Abbreviation: AA, aristolochic acid. |
In the female cohort, the following observations were associated with poorer survival (Table 2): main tumors located in the ureter (P<0.001), large main tumor diameters (>5 cm, P<0.001), severe CKD (P=0.017), papillary tumor architecture (P=0.023), higher tumor stages (P<0.001), positive N status (P=0.001), and methylated ABCC6 promoter (P=0.004). Patients with multifocal tumors (P=0.001), histories of ureteroscopy (P=0.004), and unmethylated RASSF1A promoters (P=0.017) had higher rates of BR after surgery (Table 3). In the male cohort, the following observations were associated with higher cancer-specific mortality (Table 2): older age (P=0.002), multifocal tumors (P=0.050), ipsilateral hydronephrosis (P=0.018), large tumor diameters (>5 cm, P=0.020), sessile tumor architectures (P=0.007), higher tumor stages (P=0.001), and methylated TMEFF2 promoters (P=0.012). Patients with histories of ureteroscopy (P=0.046) and unmethylated RASSF1A promoters (P=0.004) were associated with higher BR rates (Table 3). For further analysis, CSS predictive models were also built for both genders, respectively (Figure 2A–D).
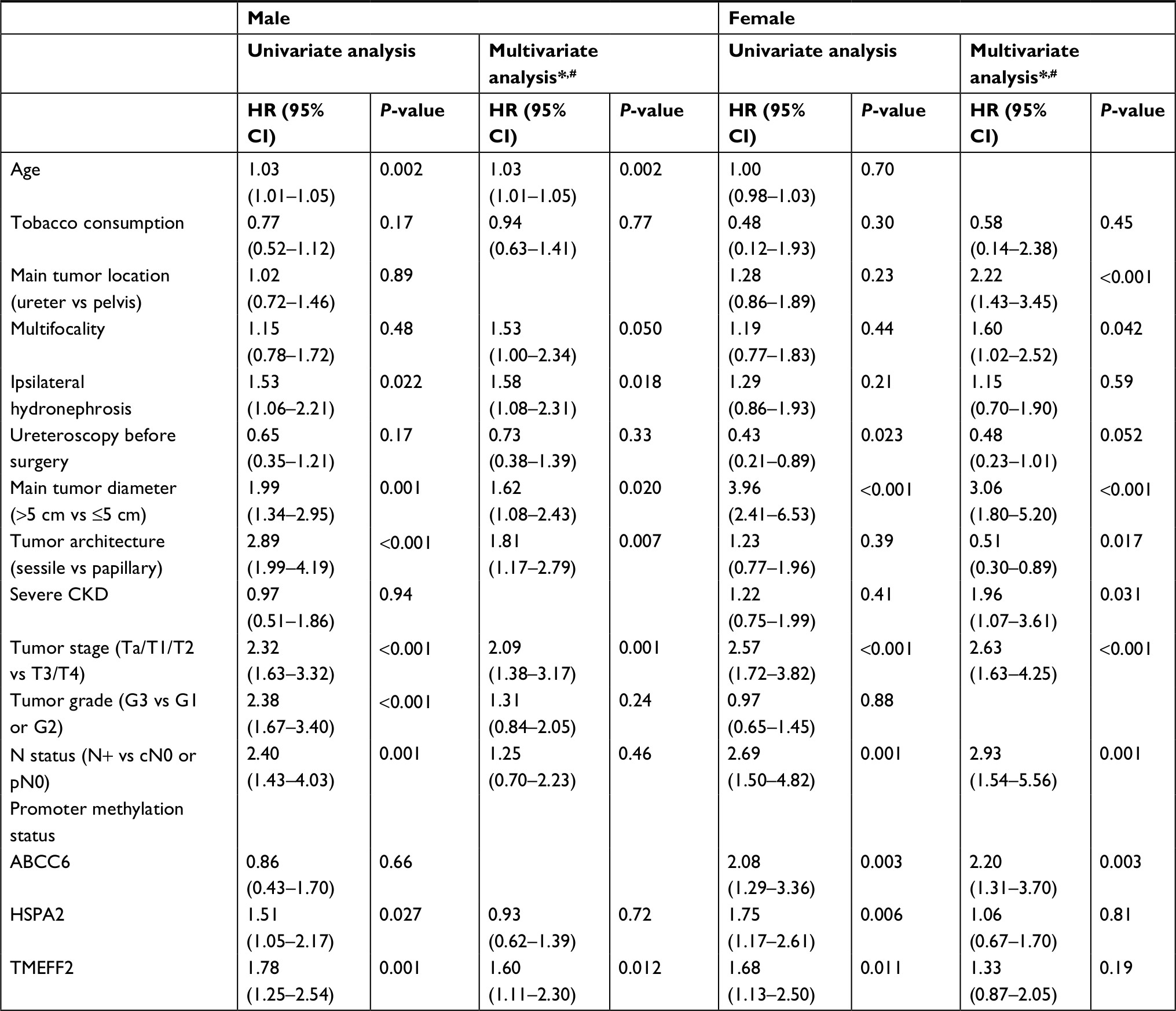 | Table 2 Prognostic factors for cancer-specific survival after surgery*,# Notes: *Variables with a P<0.5 (univariate analysis) were analyzed further in the multivariate Cox regression. #Variables with a P>0.05 (univariate analysis) (BRCA1, P=1.00 [male], P=0.30 [female]; CDH1, P=0.49 [male], P=0.32 [female]; GDF15, P=0.52 [male], P=0.26 [female]; RASSF1A, P=0.24 [male], P=0.19 [female]; SALL3, P=0.57 [male], P=0.28 [female]; THBS1, P=0.097 [male], P=0.80 [female]; VIM, P=0.20 [male], P=0.39 [female]) and variables with low proportion in the overall population (radical surgery, P=0.74 [male], P=0.33 [female]; Cis, P=0.15 [male], P=0.25 [female]) were not included in the multivariate Cox regression. Abbreviations: CKD, chronic kidney disease; cN0, clinical N0; pN0, pathological N0. |
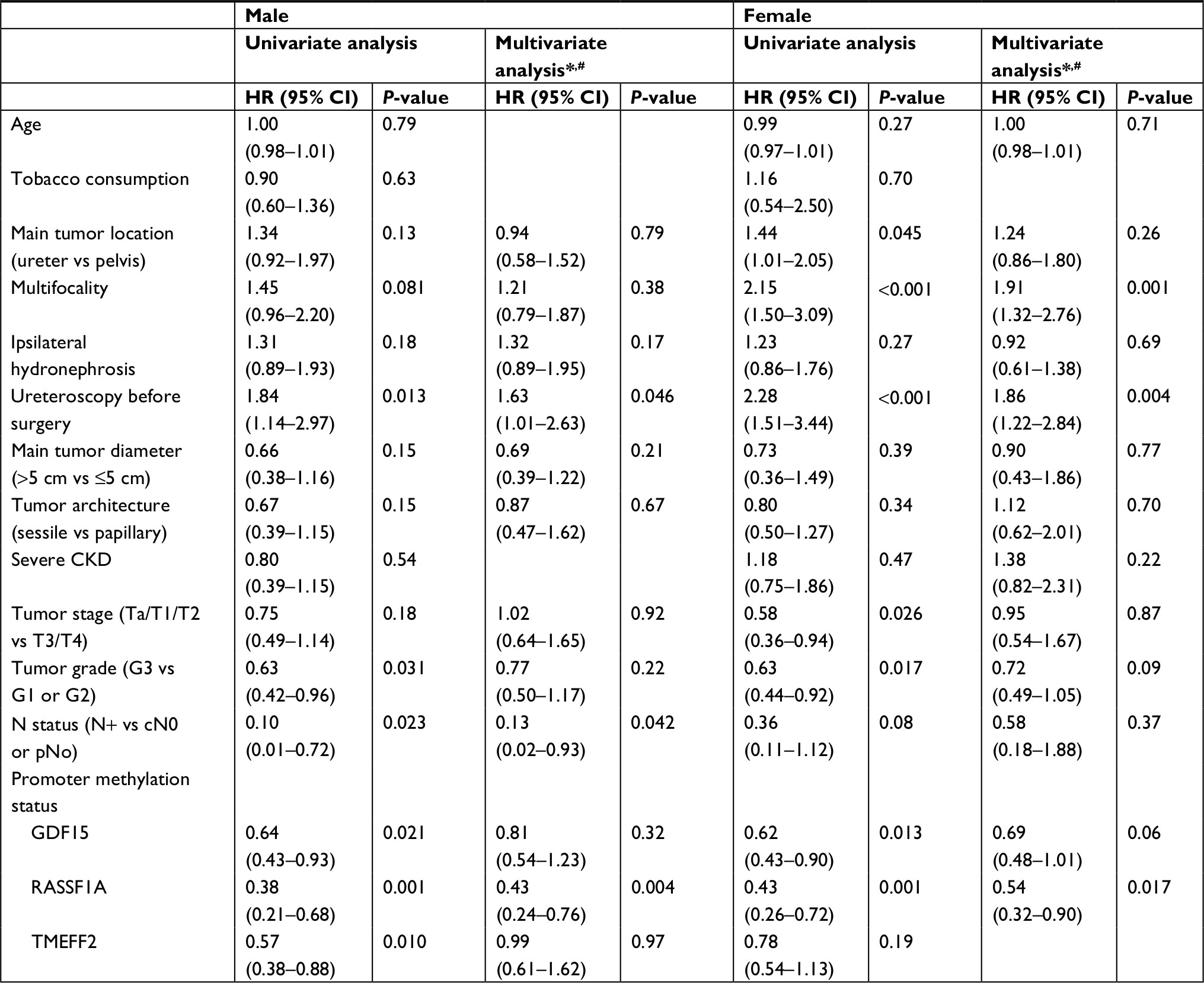 | Table 3 Prognostic factors for bladder recurrence after surgery*,# Notes: *Variables with a P<0.5 (univariate analysis) were analyzed further in the multivariate Cox regression. #Variables with a P>0.05 (univariate analysis) (ABCC6, P=0.28 [male], P=0.09 [female]; BRCA1, P=0.61 [male], P=0.96 [female]; CDH1, P=0.22 [male], P=0.27 [female]; HSPA2, P=0.12 [male], P=0.27 [female]; SALL3, P=0.28 [male], P=0.31 [female]; THBS1, P=0.15 [male], P=0.14 [female]; VIM, P=0.54 [male], P=0.24 [female]) and variables with low proportion in the overall population (radical surgery, P=0.52 [male], P=0.27 [female]; Cis, P=0.38 [male], P=0.88 [female]) were not included in the multivariate Cox regression. Abbreviations: CKD, chronic kidney disease; cN0, clinical N0; pN0, pathological N0. |
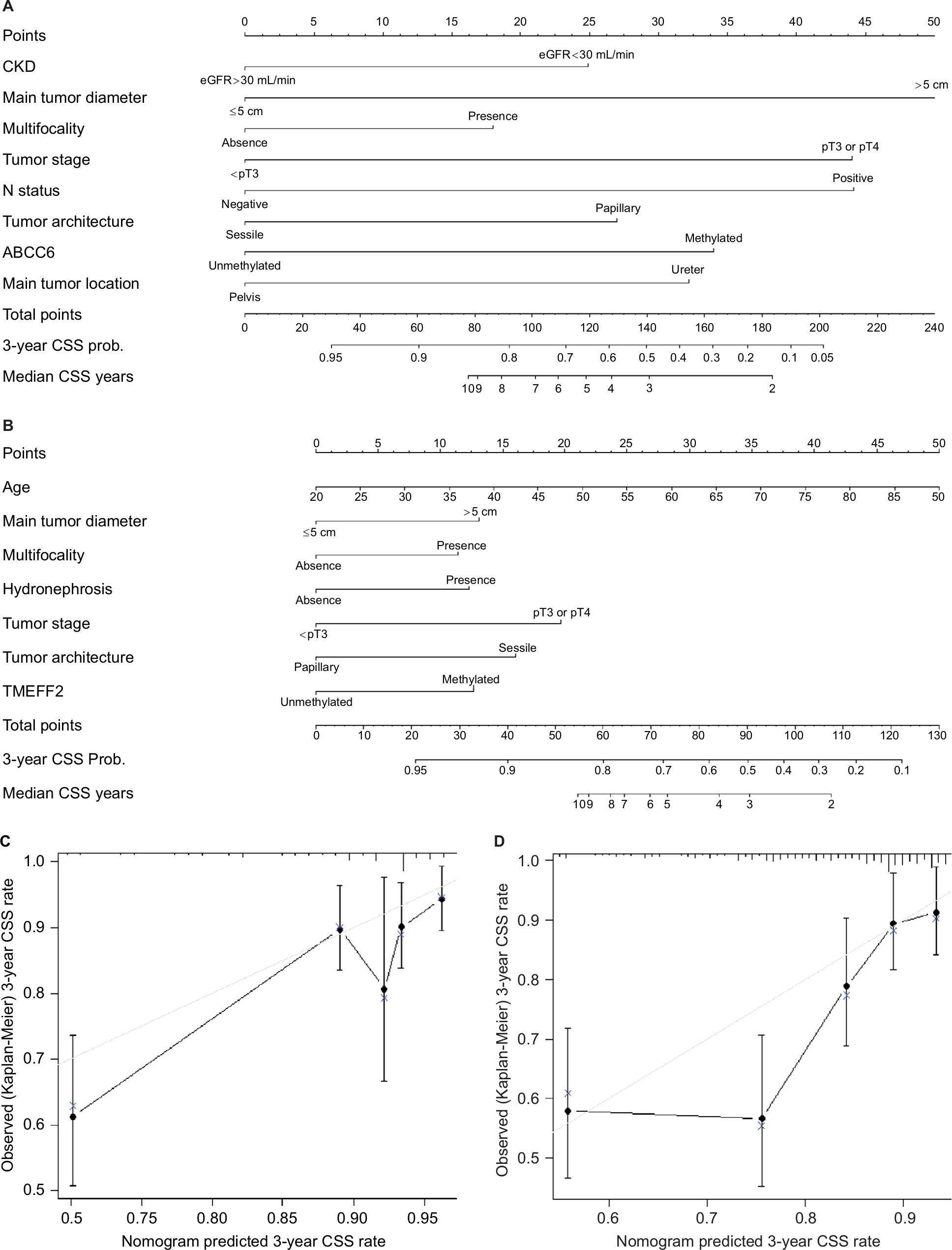 | Figure 2 Nomogram to predict 3-year CSS probability and median CSS time for (A) female and (B) male upper tract urothelial carcinoma patients. Calibration plot for predicted (gray straight line) and observed (patients were divided into five equal groups, vertical lines represent the 95% CI) 3-year CSS probability for (C) female and (D) male patients. Notes: Predictors are located on the left side, tailing with their respective scales on the right. Each scale position has corresponding points located on the “Points” scale. The sum of all points for each variable was used to calculate “Total Points.” Each “Total Points” represents the different 3-year CSS probability, and the corresponding position on the “Median CSS Years” represents median life expectancy for patients with identical characteristics. Abbreviation: CSS, cancer-specific survival. |
To explore the causes for the observed gender differences, we also investigated tobacco exposure and the intake history of AA herbs, this is owing to the fact that environmental factors could contribute to the development of UTUCs.14,15 Although the male smoking rate was significantly higher (P<0.001), the prevalence was lower than that of women. There was also no difference in tumor stage (P=0.52) and CSS (P=0.92) between smokers and nonsmokers. However, several interesting phenomena were revealed when we focused on the intake history of AA herbs (Table 4). A higher proportion of females (75.7%) reported a history of AA intake. Their renal function was much poorer (eGFR, 34.3 vs 59.7 mL/min, P<0.001), and they were less likely to develop worse histology outcomes. The patients with histories of taking AA herbs were less positive for LNM (1% vs 9%, P=0.035), had lower tumor stages (T3 or T4, 14% vs 33%, P=0.001), and had smaller tumor diameters (2.9 vs 3.5 cm, P=0.004). Multifocal tumors were also more common (40% vs 22%, P=0.001). Finally, the AA-associated patients presented better CSS (HR =0.53, P=0.023) (Figure 1B), higher BR rates (HR=1.67, P=0.005) (Figure 1C), and higher CUTR rates (HR=9.27, P<0.001) (Figure 1D) after surgery.
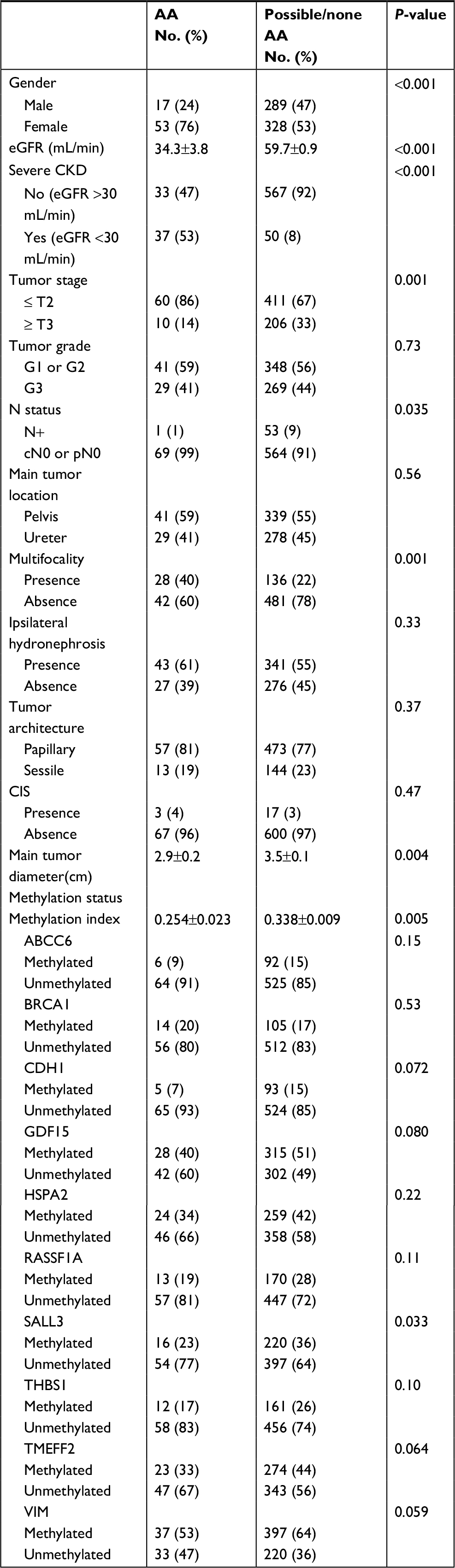 | Table 4 Characteristics of AA UTUCs compared with possible/none AA UTUCs Abbreviations: AA, aristolochic acid; CIS, carcinoma in situ; CKD, chronic kidney disease; eGFR, estimated glomerular filtration rate. |
Discussion
Unlike Western patients, our study showed that there were three typical gender-related oncological features for Chinese UTUC patients. First, the UTUC prevalence in women (55.5%) was higher than that in men. Second, with a higher prevalence of severe CKD (16% vs 8%, P=0.003), the female patients were less likely to develop higher tumor stages than male patients (HR=0.63, P=0.006). Finally, the CSS of the female patients (HR=0.59, P<0.001) was better than that of the male patients. However, it was observed that the predictors for CSS were different between the two gender cohorts.
According to typical epidemiology theories, many environmental factors contribute to the development of UTUCs. Tobacco exposure and occupation-based variables are the principal risk factors for UTUCs in Western populations.14–16 AA contains a set of highly toxic nitrophenolate derivatives that exhibit powerful mutagenic actions because of their ability to form covalent bonds with cell DNA. Therefore, AA is another important risk factor among Balkan endemic nephropathy patients and Chinese herbs consumers.17,18 In our study, <3% of the patients had a history of exposure to benzidine or β-naphthalene; thus, these factors were not likely to be the main causes of the gender-related differences. We further investigated the smoking history of the patients and found very significant differences. The proportion of males who smoked was much higher than that of females (34% vs 5%, P<0.001). However, this result was opposite to the gender distribution in our study cohort – the smoking history of the patients could not be the cause of the gender-related oncological differences.
The AA history of the patients was consistent with the oncological gender distribution. Female patients predominated the AA intake UTUC cohort (53/70, 76%). Due to the powerful covalent links of AA derivatives with cellular DNA, the carcinogenicity of AA has been carefully studied. After metabolic activation, AA binds covalently to DNA to form aristolactam (AL)-DNA adducts.19 These lesions could be the biomarker of exposure to AA and might exist in urothelial tissues.17 The AL-DNA adducts are associated with mutations in carcinogenesis genes, such as the TP53 tumor suppressor gene.20 Studies indicate that AA is the cause for this type of TP53 mutation.21 Preferential A:T-to-T:A transversions in the TP53 gene were detected in tumor samples from both Balkan and Taiwanese patients with AA-UTUC.17 Multiple mutations (KDM6A, LRRK2, etc) eventually induce malignant urothelial carcinomas.17,18,22–24 This could account for the gender distribution in our study. However, only 70 patients (11% of total patients) presented an exact AA intake history in our cohort. Therefore, this factor appears to only partially influence the observed gender-based differences. However, it is still believed that the exact AA intake history is the key cause for the observed gender-based differences for several reasons. First, the number of patients with AA exposure was likely underestimated owing to the high prevalence of TCM intake history. The compositions of TCM are very complex, with hundreds of types of herbs, minerals, and animal tissues – including AA – among the commonly used ingredients. Furthermore, TCM prescriptions vary among patients, even for the same disease; most patients do not know the exact ingredients of these medicines. When the UTUC patient histories were recorded, a majority of the patients could not accurately recount a credible history of AA intake because of the prevalent use of TCMs. In our study, we assigned patients who could recall long-term (>3 months) uses of exact AA-containing TCM in the AA cohort; other patients were classified into the possibly using or not using AA group. Therefore, the actual AA-induced UTUC patient proportion was likely much higher than reported. Second, the female patients were more likely to take AA-containing TCMs than the male patients. According to TCM theory, Caulis aristolochiae manshuriensis can be used to treat urinary tract infections (the prevalence of urinary tract infections is much higher in female populations than in male ones), regulate the menstrual cycle, increase breast milk production, and reduce the secretion of leucorrhea. Consequently, this TCM is widely used by Chinese women. Third, the female UTUC cohort shared a few similar characteristics with the AA-induced UTUC cohort. The severe CKD proportion was higher, the tumor stage was lower, the tumor diameter was smaller, and the CSS was higher.
In addition to the gender-based differences, the AA-induced UTUCs presented several unique characteristics. According to the typical pathology of AA diseases, UTUCs greatly decrease renal function and induce fibroses in the renal cortex.25,26 In our AA-induced UTUCs group, the average eGFR was only 34.3±3.8 mL/min, and the proportion of severe CKD (eGFR <30 mL/min) was 47%. More surprisingly, the AA-induced UTUCs presented lower tumor stages, smaller tumor diameters, a higher prevalence of multifocal tumors, lower methylation index, increased CSS rates, higher BR rates, and greater CUTR rates. In one retrospective study of UTUC in Balkan endemic nephropathy patients from 1957 to 1986, lower tumor stages predominated in the endemic settlements.27 Together with our results, this indicated that UTUCs caused by AA may have lower malignancies and better CSS rates. Tumor recurrence was the chief oncological risk for AA-induced UTUCs patients. In this cohort, 41 of the 70 patients (59%) exhibited BR or CUTR during the follow-up period. Moreover, 11 of the 41 patients (27%) presented both BR and CUTR. Unlike the seeding seeds recurrence theory, field metastases were likely the main causes of recurrence for the AA-induced UTUC patients. Our previous study indicated that TCMs are used nationwide and might contain nephrotoxic and carcinogenic toxins, inducing neoplasms of the entire urothelium.28 It also indicated that chronic renal insufficiency was independent risk factor for CUTR.28 In addition to inducing the primary carcinoma, AA may activate oncogenes or inactivate suppressor genes throughout the urothelium, thereby inducing the growth of new carcinomas in the bladder or the contralateral upper tract. This pathology could account for the observed higher multifocal proportion and recurrence rate. The characteristics of AA-UTUC to “FAME-PIC” have been summarized in Figure 3.29,30
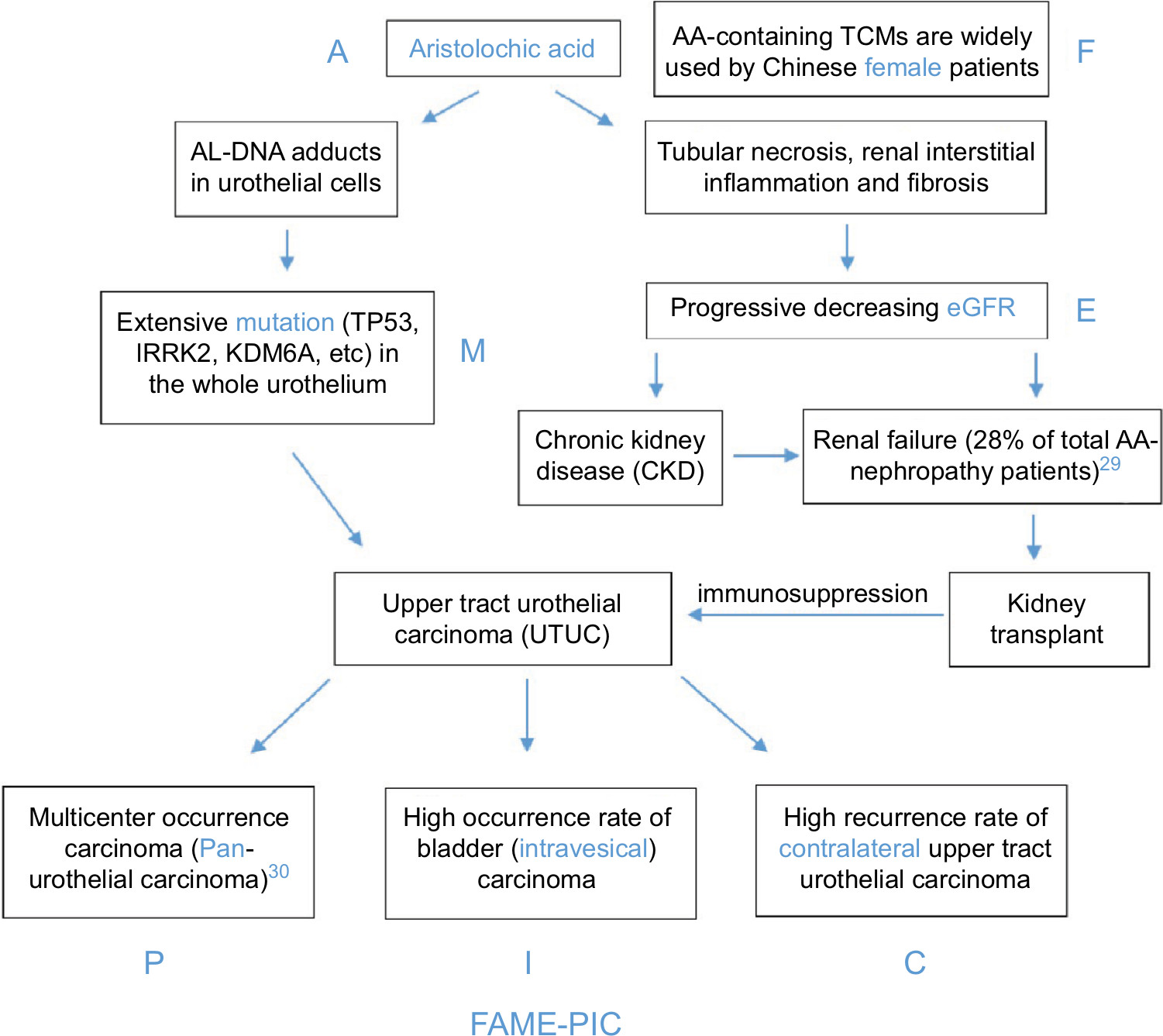 | Figure 3 Oncological characteristics of AA-induced upper tract urothelial carcinoma: FAME-PIC. Abbreviations: AA, aristolochic acid; TCM, traditional Chinese medicine; A, aristolochic acid; F, female; M, mutation; E, eGFR; P, pan-urothelial carcinoma; I, intravesical; C, contralateral upper tract; FAME-PIC, aristolochic acid- female-mutation-eGFR-pan-urothelial carcinoma-intravesical-contralateral upper tract. |
More than 12 years have passed since the Food and Drug Administration (FDA) of China forbade the use of Caulis aristolochiae manshuriensis. However, during nationwide epidemiological cross-section investigations, the issue with AA-induced UTUCs remained undetected because of the inaccurate AA intake histories. Even in our single-center study, the patients could only be divided into an AA-induced UTUC group and a possible/non-AA-induced UTUC group. Based on the several unique characteristics identified in the AA-induced UTUC group, we evaluated the prevalence of UTUC cases with AA use in patients treated from 1999 to 2011. If AA-containing herbs were regulated, the proportion of AA-induced UTUCs should decrease. Subsequently, in the overall UTUC population, the gender ratio, renal function, multifocal proportions, methylation index, tumor stages, and tumor diameters should also correspondingly change over time. We chronologically divided our study patients into five equal groups and analyzed the exact proportion of AA-induced UTUC patients based on these six factors (Figure 4).
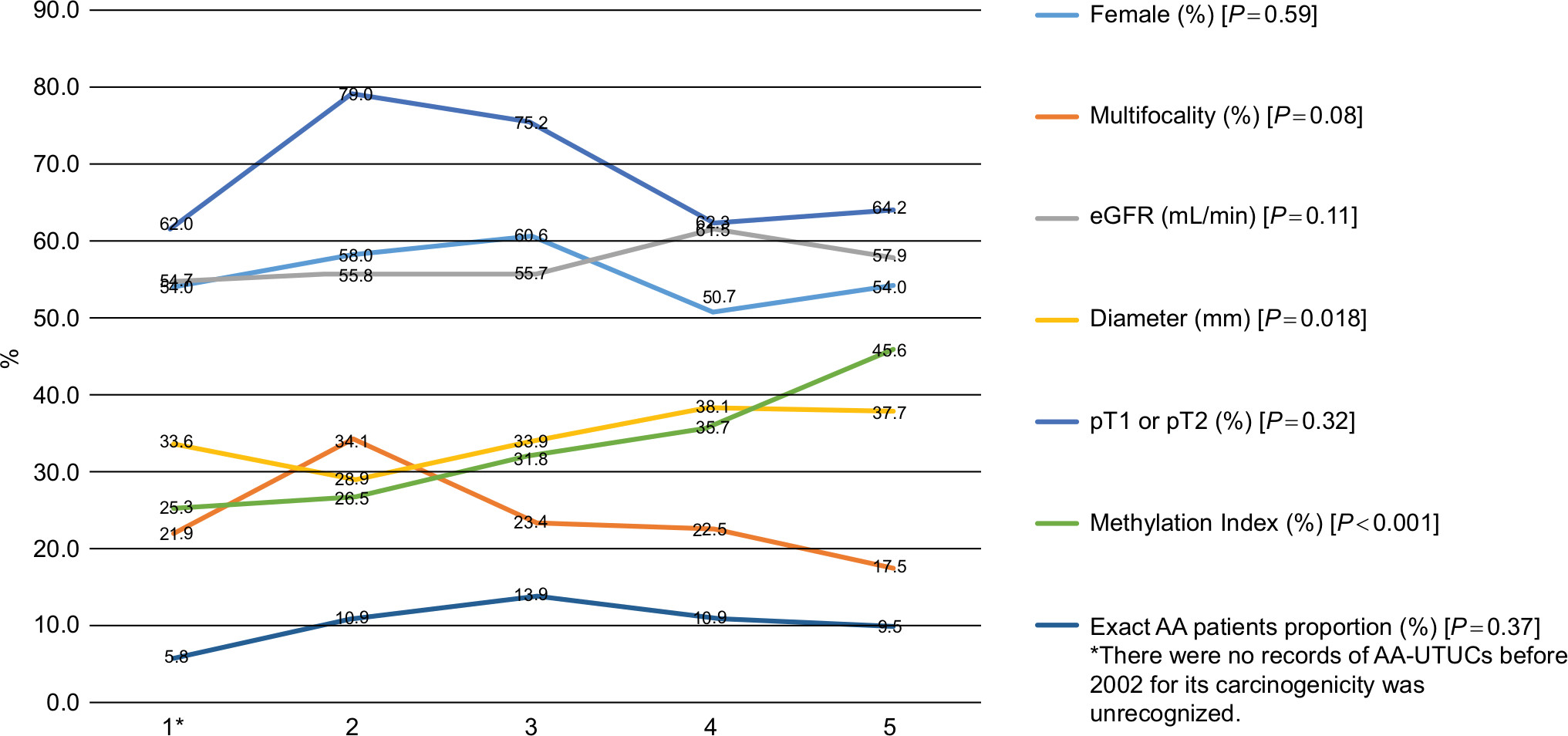 | Figure 4 The trends of oncological characteristics for AA-induced UTUC patients from 1999 to 2011 (patients were divided into five equal groups). Abbreviations: AA, aristolochic acid; eGFR, estimated glomerular filtration rate; UTUC, upper tract urothelial carcinoma. |
While the methylation index and tumor diameter showed increasing trends, the gender ratio, eGFR, multifocal proportion, pT1/pT2 percentage, and AA-induced UTUC proportion remained unchanged. These results suggest that cases of AA-induced UTUC may be declining in China. However, the proportion of cases with AA-induced UTUC was still substantial because the eGFR and exact AA-induced UTUC proportion did not change. As such, AA-induced UTUC remains to be a serious issue within China. There are approximately 20 types of AA-containing herbs that are widely used in China, and the Chinese FDA has only prohibited three of these herbs. Considering the 0.75 billion TCM clinical visits and the 6.5 billion US dollars spent on TCM herbs in 2012,31 the reporting of AA-containing TCM intake history for each UTUC patient should be accurately recorded. To protect renal function and reduce the prevalence of UTUC, official lists of prohibited TCM should be extended to all herbs containing AA. Furthermore, the bladders and contralateral upper tracts of these patients should be carefully monitored after surgery because of high recurrence rates. While these practices may not reduce the overall recurrence of UTUCs, the early detection and treatment of UTUCs will be beneficial in improving survival rates.
This study has certain limitations and constraints. First, the inaccurate AA intake history may have misclassified likely AA-UTUC patients into the possible/non-AA cohort. This may negatively affect the accuracy of this study. However, because all patients in the AA-UTUC cohort supplied an extremely reliable AA-containing herb intake history, the results for the AA-UTUC cohort are credible. Second, the analyzed data were based on a retrospective review of findings at a single center. Third, we evaluated the AA-induced UTUCs using an indirect method, potentially reducing the strength of this study.
Conclusion
In China, female UTUC patients have a higher prevalence than males and are more likely to have lower tumor stages and better survival rates. Furthermore, the oncological outcome predictors between the two genders are quite different. The main cause of these gender-based differences is attributed to TCMs containing AA. AA-induced UTUCs remain prevalent. While AA-induced UTUC patients exhibit lower tumor stages and better survival rates, their renal function, BR, and CUTR are worse than those of patients with other types of UTUCs.
Ethics approval and consent to participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of Peking University First Hospital ethics committee. And all patients consented to participate and for review their medical records. And our manuscript was accepted as poster session and discussed in the AUA2016 (MP27-13).
Availability of data and material
The datasets analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors thank Dong Fang, Yu Fan, Ding Peng, Yanqing Gong, Qi Tang, Lei Zhang, Cuijian Zhang, Lin Cai, Zheng Zhang, Zhisong He, Gang Wang, and Yinglu Guo for their contributions on this study. The authors thank Lian Zhang, Qianling Liu, Yun Cui, Min Zhang, and Feng Xie for their excellent experimental techniques. The authors thank the entire staff of the Department of Urology, Peking University First Hospital. This study was supported by The Capital Health Research and Development of Special (2016-1-4077) and The Clinical Features Research of Capital (No. Z151100004015173) and Clinical Medicine Plus X - Young Scholars Project, Peking University.
Disclosure
The authors report no conflicts of interest in this work.
References
Rouprêt M, Babjuk M, Compérat E, et al. European guidelines on upper tract urothelial carcinomas: 2013 update. Eur Urol. 2013;63(6):1059–1071. | ||
Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics. CA Cancer J Clin. 2014;2014(64):9–29. | ||
Shariat SF, Favaretto RL, Gupta A, et al. Gender differences in radical nephroureterectomy for upper tract urothelial carcinoma. World J Urol. 2011;29(4):481–486. | ||
Lughezzani G, Sun M, Perrotte P, et al. Gender-related differences in patients with stage I to III upper tract urothelial carcinoma: results from the Surveillance, Epidemiology, and End Results database. Urology. 2010;75(2):321–327. | ||
Fernández MI, Shariat SF, Margulis V, et al. Evidence-based sex-related outcomes after radical nephroureterectomy for upper tract urothelial carcinoma: results of large multicenter study. Urology. 2009;73(1):142–146. | ||
Xiong G, Chen X, Li X, et al. Prevalence and factors associated with baseline chronic kidney disease in China: a 10-year study of 785 upper urinary tract urothelial carcinoma patients. J Formos Med Assoc. 2014;113(8):521–526. | ||
Xiong G, Liu J, Tang Q, et al. Prognostic and predictive value of epigenetic biomarkers and clinical factors in upper tract urothelial carcinoma. Epigenomics. 2015;7(5):733–744. | ||
Chen XP, Xiong GY, Xs L, et al. Predictive factors for worse pathological outcomes of upper tract urothelial carcinoma: experience from a nationwide high-volume centre in China. BJU Int. 2013;112:917–924. | ||
Fang D, Xiong G, Li X, et al. Incidence, characteristics, treatment strategies, and oncologic outcomes of synchronous bilateral upper tract urothelial carcinoma in the Chinese population. Urol Oncol. 2015;33(2):66.e1–66.e11. | ||
Zhang L, Xiong G, Fang D, et al. Contralateral upper tract urothelial carcinoma after nephroureterectomy: the predictive role of DNA methylation. J Exp Clin Cancer Res. 2015;34(1):5. | ||
Yc M, Zuo L, Chen JH, Luo Q, Xq Y, Li Y. et at. Modified glomerular filtration rate estimating equation for chinese patients with chronic kidney disease. J Am Soc Nephrol. 2006;17:2937–2944. | ||
Sobin LH, Gospodarowicz MK, Wittekind C, editors. TNM Classification of Malignant Tumours. Hoboken, NJ: John Wiley & Sons; 2011. | ||
Mostofi FK, Sobin LH, Torloni H. Histological Typing of Urinary Bladder Tumors. Geneva, Switzerland: World Health Organization; 1973. | ||
Mclaughlin JK, Silverman DT, Hsing AW, et al. Cigarette smoking and cancers of the renal pelvis and ureter. Cancer Res. 1992;52:254–257. | ||
Colin P, Koenig P, Ouzzane A, et al. Environmental factors involved in carcinogenesis of urothelial cell carcinomas of the upper urinary tract. BJU Int. 2009;104(10):1436–1440. | ||
Shinka T, Miyai M, Sawada Y, Inagaki T, Okawa T. Factors affecting the occurrence of urothelial tumors in dye workers exposed to aromatic amines. Int J Urol. 1995;2(4):243–248. | ||
Grollman AP, Shibutani S, Moriya M, et al. Aristolochic acid and the etiology of endemic (Balkan) nephropathy. Proc Natl Acad Sci. 2007;104(29):12129–12134. | ||
Chen CH, Dickman KG, Moriya M, et al. Aristolochic acid-associated urothelial cancer in Taiwan. Proc Natl Acad Sci U S A. 2012;109(21):8241–8246. | ||
Arlt VM, Stiborova M, Schmeiser HH. Aristolochic acid as a probable human cancer hazard in herbal remedies: a review. Mutagenesis. 2002;17(4):265–277. | ||
Lord GM, Hollstein M, Arlt VM, et al. DNA adducts and p53 mutations in a patient with aristolochic acid-associated nephropathy. Am J Kidney Dis. 2004;43(4):e11–e17. | ||
Attaluri S, Bonala RR, Yang IY, et al. DNA adducts of aristolochic acid II: total synthesis and site-specific mutagenesis studies in mammalian cells. Nucleic Acids Res. 2010;38(1):339–352. | ||
Poon SL, Pang ST, Mcpherson JR, et al. Genome-wide mutational signatures of aristolochic acid and its application as a screening tool. Sci Transl Med. 2013;5:197:ra101. | ||
Hoang ML, Chen CH, Sidorenko VS, et al. Mutational signature of aristolochic acid exposure as revealed by whole-exome sequencing. Sci Transl Med. 2013;5(197):ra102. | ||
Nortier JL, Martinez MC, Schmeiser HH, et al. Urothelial carcinoma associated with the use of a Chinese herb (Aristolochia fangchi). N Engl J Med. 2000;342(23):1686–1692. | ||
Pozdzik AA, Berton A, Schmeiser HH, et al. Aristolochic acid nephropathy revisited: a place for innate and adaptive immunity? Histopathology. 2010;56(4):449–463. | ||
Yang L, Su T, Li XM, et al. Aristolochic acid nephropathy: variation in presentation and prognosis. Nephrol Dial Transplant. 2012;27(1):292–298. | ||
Cukuranovic R, Ignjatovic I, Visnjic M, et al. Characteristics of upper urothelial carcinoma in an area of Balkan endemic nephropathy in south Serbia. A fifty-year retrospective study. Tumori. 2010;96(5):674–679. | ||
Fang D, Zhang L, Li X, et al. Risk factors and treatment outcomes of new contralateral upper urinary urothelial carcinoma after nephroureterectomy: the experiences of a large Chinese center. J Cancer Res Clin Oncol. 2014;140(3):477–485. | ||
Yang L, Su T, Li XM, et al. Aristolochic acid nephropathy: variation in presentation and prognosis. Nephrol Dial Transplant. 2012;27(1):292–298. | ||
Fang D, Liu P, Li X, et al. Characteristics and treatment outcomes of pan-urothelial cell carcinoma: a descriptive analysis of 45 patients. Sci Rep. 2016;5(1):18014. | ||
China statistical yearbook of health and family planning, version; 2013. Available from: http://www.nhfpc.gov.cn/htmlfiles/zwgkzt/ptjnj/year2013/index2013.html. Accessed December 13, 2015. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.