Back to Journals » Journal of Pain Research » Volume 16
Are We Any Closer to Understanding How Chronic Pain Develops? A Systematic Search and Critical Narrative Review of Existing Chronic Pain Vulnerability Models
Authors Delgado-Sanchez A, Brown C, Sivan M ![]() , Talmi D, Charalambous C, Jones AKP
, Talmi D, Charalambous C, Jones AKP ![]()
Received 15 March 2023
Accepted for publication 27 June 2023
Published 14 September 2023 Volume 2023:16 Pages 3145—3166
DOI https://doi.org/10.2147/JPR.S411628
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jonathan Greenberg
Ariane Delgado-Sanchez,1 Christopher Brown,2 Manoj Sivan,3 Deborah Talmi,4 Christiana Charalambous,5 Anthony KP Jones1
1Division of Human Communication, Development, and Hearing, University of Manchester, Manchester, UK; 2Institute of Population Health, University of Liverpool, Liverpool, UK; 3Leeds Institute of Rheumatic and Musculoskeletal Medicine, University of Leeds, Leeds, UK; 4Department of Psychology, University of Cambridge, Cambridge, UK; 5Department of Mathematics, University of Manchester, Manchester, UK
Correspondence: Ariane Delgado-Sanchez, Clinical Sciences Building, Salford Royal Foundation Trust, Salford, Greater Manchester, United Kingdom, Email [email protected]
Abstract: Identifying biopsychosocial factors underlying chronic pain vulnerability is essential for the design of preventative efforts. Multiple chronic pain vulnerability models exist, however, there is a lack of comprehensive evaluation of these models in the literature, potentially due to the lack of guidelines that specify the criteria by which these types of work should be assessed. In this work, we created evaluation criteria (based on the general goals of conceptual models), and we then used them to critically review the chronic pain vulnerability models available in the current peer-reviewed literature (identified through a systematic search). Particularly, we evaluated the models on the basis of conceptual clarity/specificity of measures, depth of description of aetiological and mechanistic factors, use of a whole system approach, and quality of the evidence associated with the models. We found nine conceptual models that have been explored in detail (eg, fear avoidance model, diathesis-stress model). These models excel at clarity and are supported mostly by self-report evidence of a psychological nature (anxiety sensitivity, pain catastrophizing, etc.), but provide little explanation of mechanistic and aetiological factors. In the future, models could be improved by complementing them with proposals from other models and exploring potential causal factors and mechanisms maintaining the condition. This task could be carried out through prospective cohort studies, and computational approaches, amongst others.
Plain Language Summary: Several theories explain why some people are more vulnerable to develop chronic pain; however, there is no previous work that compares these theories or evaluates their quality. After evaluating these theories, we concluded that they are very good at identifying what psychological characteristics make someone vulnerable to develop chronic pain. However, they lack an explanation regarding what makes people develop those characteristics or how they lead to pain. We propose ways in which the different theories could be complemented.
Keywords: vulnerability, evaluation, theory, conceptual model
Introduction
Chronic pain is defined as “persistent or recurrent pain lasting longer than 3 months”.1 The ICD-11 divides pain into two main categories: primary pain (chronic pain in which there is no identifiable underlying cause or in which symptoms are out of proportion to the identified cause) and secondary pain (pain is a consequence/symptom of another condition).2 Chronic pain is an important public health issue affecting between 35% and 51.3% of the UK population3 and 19% of the European population.4 Although still not fully understood, the factors influencing the development of vulnerability – the relative risk to develop chronic pain – are not completely unknown. Several conceptual models of chronic pain vulnerability have gathered supporting evidence.
We define conceptual models as “visual or written products that explain, either graphically or in narrative form, the main things to be studied—the key factors, concepts, or variables—and the presumed relationships between them”.5 Models or theories are key elements in the development of research and intervention. In fact, theoretical illiteracy has been pointed out as an important obstacle for the progress of scientific advancement.6 Nevertheless, although it is clearly important to have good theories, there are no specific guidelines to assess the quality of conceptual models. In this work, we used the literature regarding the use of conceptual models and the proposals made regarding what makes a good theory to develop evaluation criteria for conceptual models. We then used these criteria to assess the most prominent chronic pain vulnerability models.
Methods
The current review analysed and evaluated the current conceptual models of chronic pain vulnerability. To begin with, we explored the literature regarding the use of conceptual models to identify the criteria that should be used to evaluate this type of scientific work. We then used the outputs of this research to develop specific evaluation criteria for conceptual models. Note that the developed criteria are not exclusive to chronic pain and could be applicable to any conceptual model exploring a health condition or psychological concept. Nevertheless, in this specific work, we used them to evaluate the quality of conceptual models exploring chronic pain vulnerability.
Current chronic pain vulnerability models were identified by performing a systematic search on Web of Science, PubMed and PsycINFO for the terms “chronic pain” and “vulnerability” and (“model” or “theory” or “framework”). These searches lead to 270, 349 and 239 results, respectively, in each of the databases. The decision to include the three terms (model, theory and framework) was taken based on the interchangeable use that is given to these three concepts in the literature. Furthermore, models were also included based on knowledge of experts in the field.
In the literature search, after deleting duplicates, the titles and abstracts of the papers were analysed. Models were included in this work if they proposed (1) an explanation for the aetiology of primary pain (ie, pain is the main disorder)2 or (2) an explanation for inter-individual differences in chronic pain severity or pain intensity in secondary pain (ie, pain is a consequence of another disorder).2 Empirical studies and reviews that presented the following characteristics were excluded: articles in which chronic pain was used as the predictor and not the outcome; articles in which pain was not treated as the main symptom but just one of the symptoms in another condition that is being studied; articles in which the quality of life/pain intensity was assessed in population who had already developed chronic pain; and articles in which the model refers to a statistical model only as a methodology, animal models, treatment models or drug use control/trajectory models. Finally, papers that were not available in English or Spanish were also excluded. The remaining articles were inspected to identify the disease vulnerability models present in the literature.
Once the models were identified, a further search of the literature was performed with each one of them (by searching the model name in the three databases mentioned above) to gather further information on their proposal and associated evidence. We explored the titles and abstracts to identify the papers that explored the evidence associated with the models of interest and these were used to perform the subsequent evaluation. Since one of the goals of this work was to evaluate quality of the evidence associated with the models, we included papers from all different levels of evidence and then assessed them in the evidence section of the evaluation criteria (see Table 1). A flowchart of the methods can be found in Figure 1.
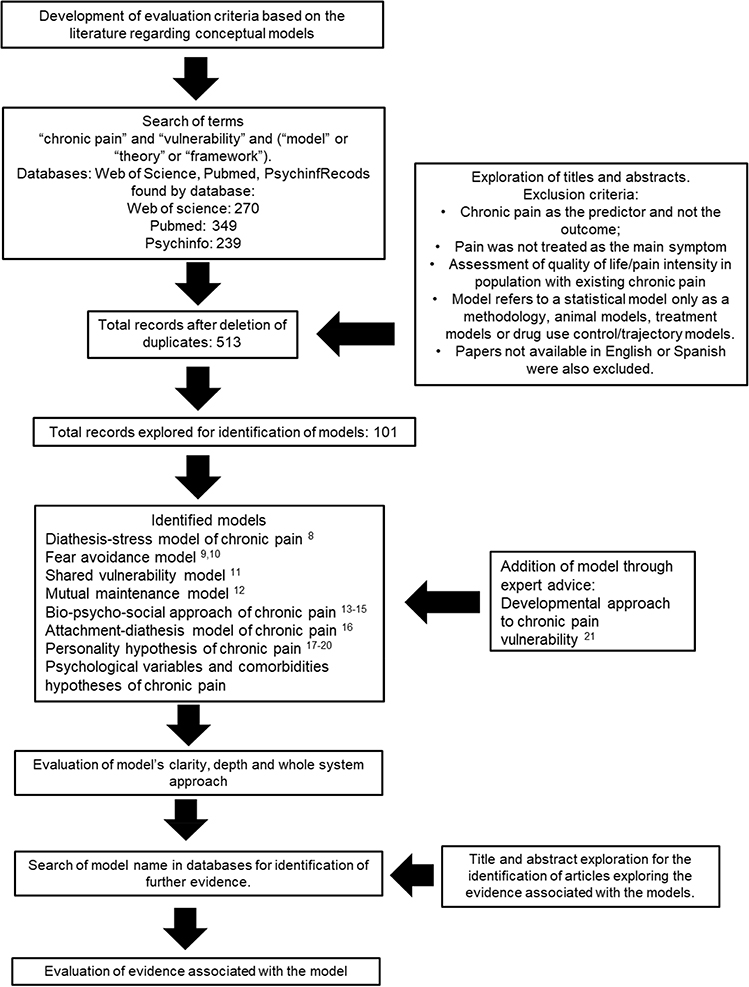 |
Figure 1 Flowchart of review process.8–21 |
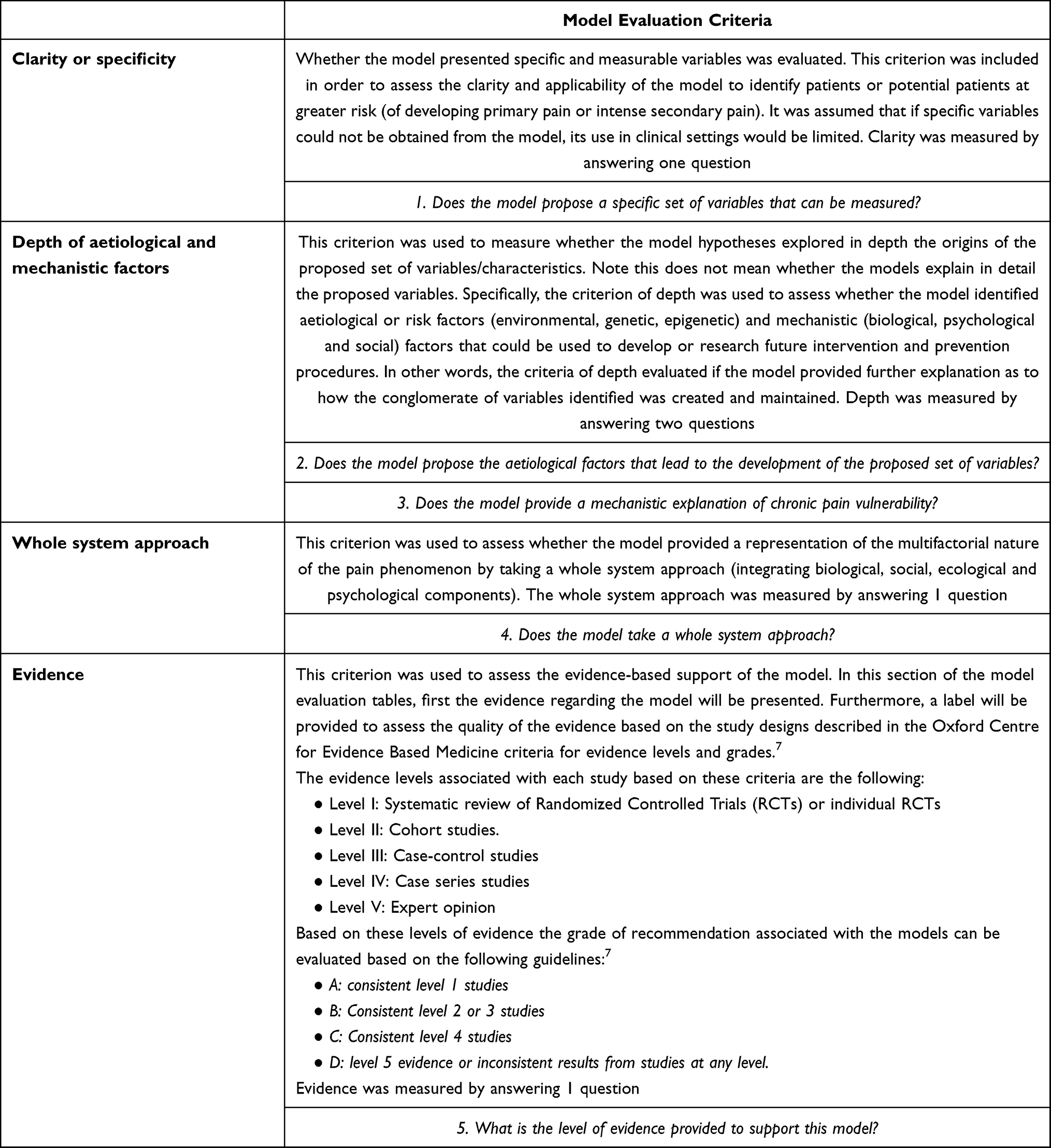 |
Table 1 Model Evaluation Criteria |
Results
Evaluation Criteria for Conceptual Models
Evaluation criteria to assess the quality of the models were developed based on the principles and objectives of conceptual models in general. Overall, different authors have proposed that conceptual models should be tools to guide practice and research.22,23 It has also been proposed that theories should provide an explanation for the causal and maintenance factors of a disease6 and that their best use is achieved when they integrate socio-ecological and biological components.23 Based on these proposals regarding the objectives of models and theories, we concluded that a model’s quality should be evaluated based on the following three principles: (1) its usefulness in practice, (2) its ability to direct research to the insight into causal and maintenance factors and (3) its use of a whole system approach (integration of biological, ecological, psychological and social components). Furthermore, based on the risk of dogmatic acceptance of existing theories pointed out in the literature6 we proposed a fourth principle, 4 - the empirical support associated with the model.
In this work, we developed evaluation criteria to assess conceptual models based on the key objectives associated with these types of theories. In order to evaluate the usefulness of a theory in practice (principle 1) we assessed whether specific measurable factors were proposed that could be of use for clinicians. To measure the ability to direct research into causal and maintenance factors (principle 2) we evaluated whether the model proposed any causal or risk factors linked to the development of the main variables and whether it presented a mechanistic explanation. It is worth clarifying that we understand mechanism both as a “complex arrangement of entities and activities, organised in such a way as to be regularly or predictably responsible for the phenomenon to be explained” and a “spatio-temporal pathway along which certain features are propagated from the starting point to the end point”.24 The whole system approach was evaluated by analysing whether the model integrated social, ecological, psychological and biological components. Finally, the evidence supporting the model was evaluated based on the Oxford Centre for Evidence-based Medicine Levels of Evidence (OCEBM).7 All of these points were formalised in the evaluation criteria presented in Table 1 and subsequently used to assess the identified models.
Current Models for Chronic Pain Vulnerability
The following models were identified through the review: the diathesis-stress model of chronic pain,8 the fear avoidance model,9,10 the shared vulnerability model,11 the mutual maintenance model,12 the bio-psycho-social approach of chronic pain13–15 the attachment-diathesis model of chronic pain,16 the personality hypothesis of chronic pain,17–20 and the psychological variables and comorbidities hypotheses of chronic pain. The following model was added as a consequence of experts’ review: the developmental approach to chronic pain vulnerability.21
Diathesis-Stress Model of Chronic Pain11
This model was created with the objective of explaining the development of disability and chronic pain after a traumatic experience, when there is no tissue damage that would explain the level of disability. Turk8 proposes that when faced with a traumatic event (stress), the likelihood of a patient developing chronic pain could be influenced by predisposing cognitive and behavioural factors (diathesis). Particularly, this model gives special attention to Anxiety Sensitivity (AS) as a predisposing factor. “As is the fear of arousal-related sensations, arising from beliefs that certain sensations have adverse consequences such as death, insanity, or social rejection”.25 Turk8 proposes that high levels of this construct will lead to an increased fear of pain, which in turn results in a higher anticipation of pain and higher pain perception. Furthermore, the fear of pain will make patients avoid behaviours that could cause an unpleasant sensory experience and, therefore, predispose them to more fear and disability.
Moreover, people with high AS will present hypervigilance towards their bodily sensations. In this way, when faced with a threatening event (such as a car accident), their attentional bias may make them interpret innocuous bodily sensations as abnormal or even painful, and establish a causal attribution with the threatening event. This interpretation of bodily sensations will in turn lead to higher fear and anticipation of pain.
High AS is linked with increased catastrophizing within the model. Catastrophizing has several definitions in the field of pain research.26,27 Turk8 clarifies that in their model catastrophizing is defined as a coping mechanism characterised by negative self-statements, and overly negative thoughts and ideas about the future.8 The model states that increased catastrophizing once again results in increased fear of pain.
Finally, the concepts of self-efficacy and operant conditioning are also included in the proposal. As previously stated, the final result of the psychological and cognitive diathesis is an increased avoidance of behaviours that are feared to cause pain. In this way, whilst operant conditioning feeds back the maladaptive cognitions and beliefs; higher self-efficacy leads to a lower avoidance of behaviours perceived as threatening.8
Little research has focused on empirically testing the model; nevertheless, the existing few attempts have had positive results.28 In general, most studies have found a correlation between most of the proposed variables with pain29,30. Nevertheless, although the different elements of the model seem to be related to pain, there is still an open debate regarding the hierarchy of importance of the different psychological factors. For instance, anxiety sensitivity, which is given a central role in this and other models, has failed to show an effect on pain when controlling for other variables.29 Future research should attempt to test the mediating factors and determine which variables are central for the development of chronic pain and which represent just a moderating or confounding effect.
Furthermore, although this model very clearly states the variables that should be measured to test vulnerability, it does not provide an explanation as to what leads to the development of this vulnerability. The model takes almost exclusively a psychological perspective, leaving out biological and social components. In order to improve the model and promote research in the area it would be prudent to expand the proposal to include both aetiological factors and bio-social correlates that could help present a clearer picture of the phenomenon.
A summary of the evaluation criteria results can be observed in Table 2, and the full application of the evaluation criteria on the model can be seen in Table 3.
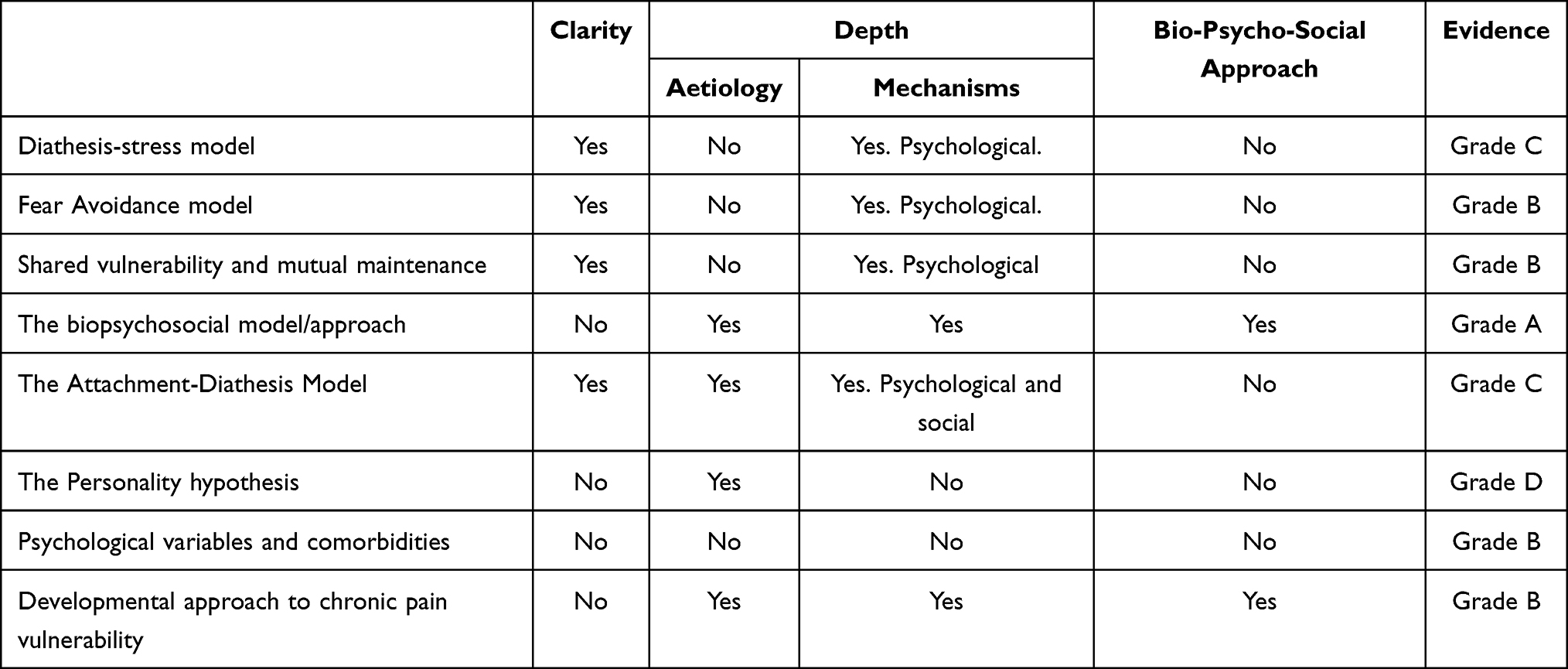 |
Table 2 Summary and Comparison Table of the Current Chronic Pain Vulnerability Models |
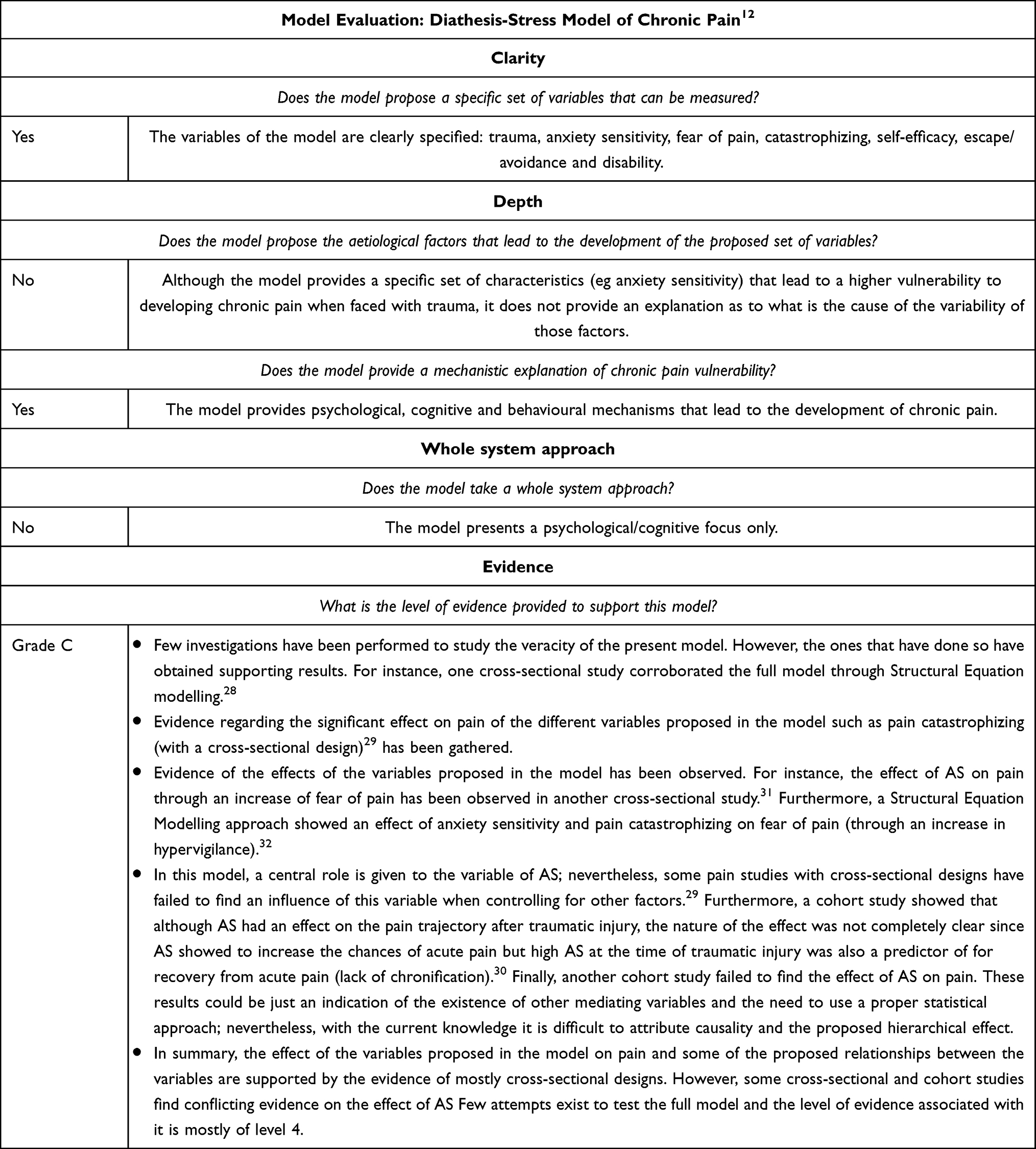 |
Table 3 Evaluation of the Diathesis-Stress Model of Chronic Pain12 |
Fear Avoidance Model9,13
This model was created to explain the “exaggerated pain perception” observed in some chronic low-back pain patients.9 It is one of the most researched models in chronic pain vulnerability and it delves into very similar concepts as the ones presented in the Diathesis-Stress model; however, the current model has a central focus on the concept of fear of pain. In the original proposal, Lethem et al9 postulated that when faced with a painful experience, individuals could take two approaches based on their fear levels: confrontation (more likely to occur with low fear) or avoidance (more likely to occur with high fear). These approaches would lead to opposite consequences. Confrontation would lead patients to mobilisation, calibration of the pain experience with the nociceptive input and effective rehabilitation. Meanwhile, avoidance would lead to reinforcement of the fear of pain and avoidant behaviour, physical consequences due to lack of movement and exaggerated pain perception. Furthermore, Lethem et al9 stated that fear of pain is mediated by the psychosocial context of each patient.
The general principle of the model stood the test of time (fear of pain leads to disability/chronicity) and subsequent proposals refined the originally proposed model. This way, some years later the model was applied to musculoskeletal pain.10 In this new postulation, authors included other elements that could be feeding into the fear of pain, such as pain catastrophizing and negative affect. Furthermore, they also included, as a consequence of fear of pain, the increase in hypervigilance to one’s bodily sensations.
These two versions of the fear avoidance model are not the only ones that have been postulated. Several researchers have proposed small alterations to this model, such as the inclusion of resilience as a protective factor influencing fear.33
This model is probably the most widespread model of chronic pain vulnerability and has proven useful for many researchers and clinicians. Particularly, its predictiveness of disability has been corroborated by the literature on multiple occasions.31,33–36 Nevertheless, although the general principle of the model seems to be solid, conceptual details and the specific effect of different variables have shown less clear results. For instance, some research has encountered a lack of effect of certain variables such as anxiety sensitivity;37 other investigations have found that the relationships between fear and pain are moderated by factors not included in the model,38,39 and finally, some researchers have encountered that adding new factors such as resilience to the model could improve its predictive accuracy.33 Taking all of this into account, it is important for future research to explore the exact mechanisms that could be leading the correlation between fear and pain in order to provide some clarity to the model’s proposals and better guide the design of interventions based on the principles defined by the model.
Furthermore, a higher focus on the aetiological factors that lead fear of pain would be beneficial. Some proposals have postulated the idea of prior experience with pain being a potential cause of the vulnerability;9 future research could explore this in more depth, as well as analysing other potential influencing factors. Finally, as with the diathesis-stress model, not much detail is provided regarding the bio-social correlates of the psychological variables proposed, which would be a good addition to the theory.
A summary of the evaluation criteria results can be observed in Table 2, and the full application of the evaluation criteria on the model can be seen in Table 4.
 |
Mutual Maintenance12 and Shared Vulnerability Models14
These models were built to explain the comorbidity found between Chronic Pain and Post Traumatic Stress Disorder (PTSD). The shared vulnerability model proposed that the high co-occurrence of this disorders could be due to the same factors leading the vulnerability to chronic pain and PTSD. Particularly, the authors consider that AS may have a central role in increasing the vulnerability to both pathologies; therefore, someone with high AS would be more likely to develop both chronic pain and PTSD explaining part of the comorbidity between these two.11 Furthermore, in the Mutual Maintenance Theory, the authors propose that the comorbidity between these two disorders is a consequence of a feedback between several common or interacting symptoms:12
- Attentional bias: both chronic pain and PTSD are proposed to be characterized by an increased attention to stimuli related to pain or the traumatic event respectively. Pain could be a reminder of the trauma in PTSD and therefore an increased attention to those stimuli may result in increased pain.
- Anxiety Sensitivity is proposed as a common symptom in both disorders that increases catastrophizing and consequently the likelihood of interpreting the arousal characteristic of PTSD as potentially threatening stimuli.
- Reminders of Trauma: As mentioned before, pain could be a reminder of the trauma which would increase arousal. Due to the proposed attentional bias in patients, the consequent increase in arousal and pain could result in an increase in fear and more avoidance.
- Avoidance: The avoidance of behaviours that are feared to cause pain or may be a reminder of symptoms is proposed to prevent the extinction of negative reactions, and in turn favour the maintenance of both disorders.
- Both disorders commonly co-occur with depression that will result in a decrease in activity that may serve to maintain both PTSD and chronic pain by giving way to avoidance of reminders of trauma and increasing disability respectively.
- High anxiety levels are thought to reduce pain thresholds and tolerance.
- Since dealing with the symptoms, such as catastrophic cognitions and intrusions, requires cognitive load, patients are thought to struggle to adopt cognitively active coping strategies to change these patterns.
In general, evidence exists to support the proposals of the models. The mutual maintenance model has received the most support,41–43 perhaps due to its higher level of detail that allows for its hypotheses to be studied in more depth. Nevertheless, it is important to mention that new research has found that the model could be improved by the inclusion of other variables such as sleep44 and mindfulness,45 indicating that the full phenomenon of the correlation between pain and PTSD is still a work in progress. It is important to consider that in the last decades since this model was proposed, research in the area of both PTSD and pain has grown exponentially, and therefore, an update of the model with the new knowledge from both fields would be beneficial. In order to improve the quality of the model, adding knowledge regarding bio-social factors would be particularly recommendable since, like in previously presented proposals, this model is mostly focused on psychological components.
When it comes to the shared vulnerability model, the results are not as solid. Once again, the model sets its focus on anxiety sensitivity, a variable that has shown some contradictory results in its association with pain.29,37 In order to improve the model, exploring other factors that lead to the vulnerability would be beneficial. Some investigations have already identified variables such as pre-injury health and social support,46 although more research is needed to corroborate these findings and identify further vulnerability factors. Furthermore, just like with the diathesis-stress and fear avoidance models, looking at the aetiological factors and mechanisms would be a beneficial addition to improve model quality.
A summary of the evaluation criteria results can be observed in Table 2, and the full application of the evaluation criteria on the model can be seen in Table 5.
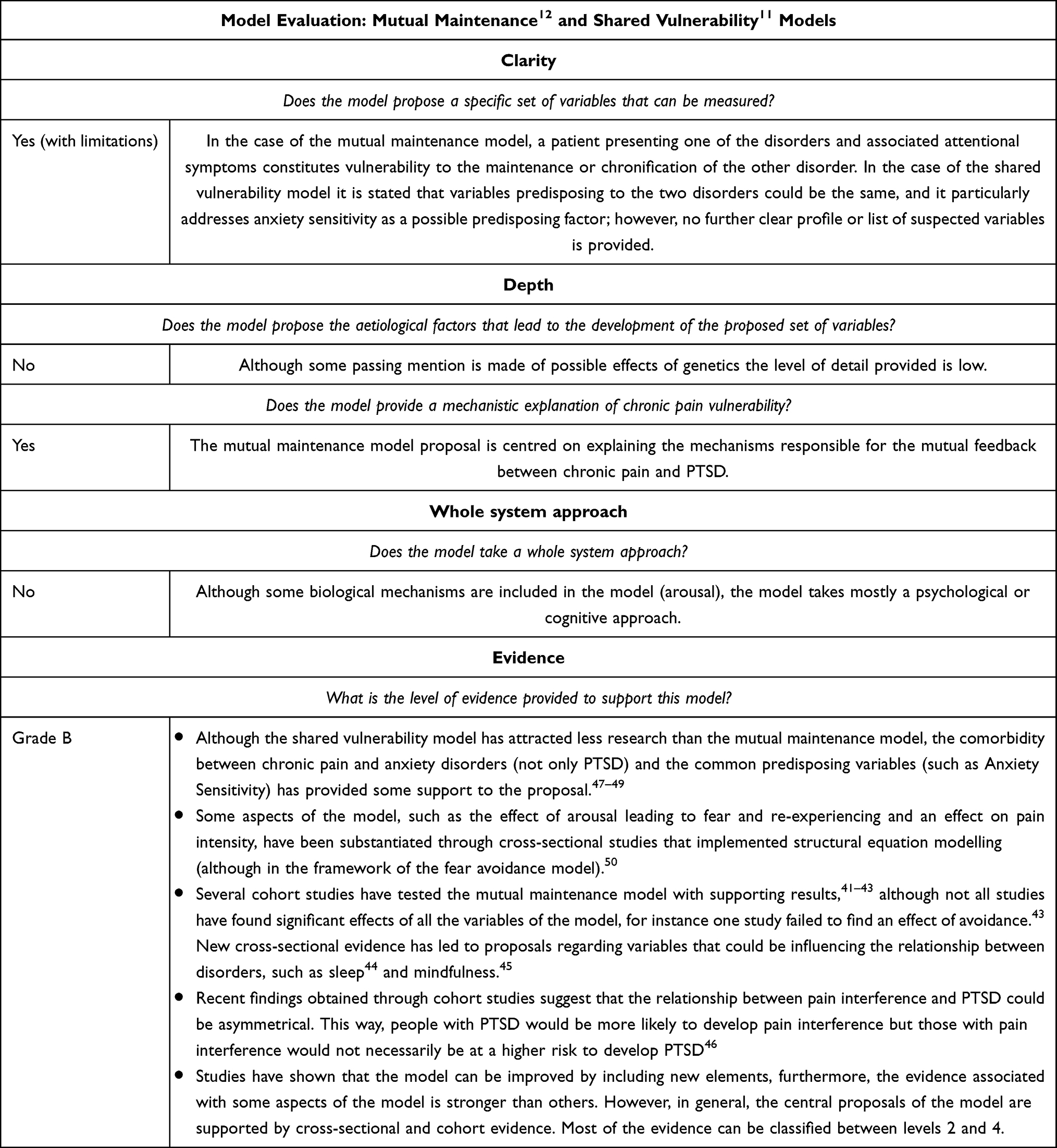 |
Table 5 Evaluation of the Mutual Maintenance12 and Shared Vulnerability11 Models |
The Biopsychosocial Model/Approach of Chronic Pain
This model, instead of a formal chronic vulnerability model (like the ones presented above), could be classified more accurately as the application of the biopsychosocial approach13 to understanding chronic pain vulnerability.51 Perhaps, this is the reason why the focus on validating component factors of this model is quite variable. Some proposals are more dominated by the biological component with elements such as genetic, immune and endocrine factors being included.14 Other proposals give more attention to psychosocial factors and in the biological component they include elements such as comorbidities, sex and age.15 Nevertheless, in general terms, the biopsychosocial approach or model for chronic pain can be defined as those models or approaches that envision pain as a multidimensional, dynamic interaction among physiological, psychological, and social factors that reciprocally influence one another, resulting in chronic and complex pain syndromes.52
Although not always presented under the concept of the biopsychosocial model of pain, ample research exists on the different biological correlates of chronic pain vulnerability and their potential links with psychological and social components. For instance, one area of research that has gained a lot of attention links stressful life events with chronic pain vulnerability. It has been proposed that stressful life events increase individuals’ allostatic load (accumulation of stress consequences in the body) which leads to psychological, neuroendocrine, immune and brain alterations.53 Evidence exists linking early life stress with neuroendocrine alterations54 and high levels of inflammatory biomarkers,55 as well as evidence linking high inflammatory markers and sensitivity to pain.56–58 The exact mechanisms through which these alterations take place are still in the hypothetical stage59 but research efforts are being conducted to understand them. Moreover, other factors aside from stress have also been linked to these biological alterations such as diet60 or exposure to pollutants.61 Regarding the social components involved in the mechanisms described, research has linked some social factors, such as Socio Economic Status, with the experience of stressful events,62 higher consumption of pro-inflammatory diets63 and exposure to pollutants.64 Furthermore, other social elements have also gained attention in their relation with pain vulnerability and the associated psychological components. For instance, social support is an important predictor of disability.65
In summary, a lot of research is being developed in the area of the bio-psycho-social model of pain with supporting results. This model presents strengths unlike other models presented in this paper, mostly in providing aetiological and mechanistic explanations for chronic pain vulnerability and taking a whole-system approach. Nevertheless, this theory scores lower in one area in which other models excel: providing clear variables to measure by clinicians. Chronic pain is a multifactorial phenomenon that with our current knowledge is hard to fully summarize in a few variables – perhaps the reason why the other models opted to focus on just a few factors/a small part of the full phenomenon. Nevertheless, for clinical applications, it is important to understand what the key variables are in the complex cycle of chronic pain. Therefore, it would be beneficial for this model to evolve to identify the most clinically relevant variables that would make its application more feasible. Perhaps, research in which multiple different variables are measured and a reduction in dimensionality is performed through factor analysis would be recommendable. Another option would be to identify the mechanism(s) that link the different factors and use those as diagnostic and treatment targets (currently, research on metabolic and immune factors seems to be promising for this purpose59). Moreover, it is also important to note that the evidence supporting the model, such as that presented above, is often based on studies focusing on different components of the model separately. This way, there is a great amount of evidence linking psychological and biological components, social and psychological components or social and biological components. Nevertheless, studies that link the three components at once are less common. Consequently, the evidence oftentimes linked to the bio-psycho-social model could only be considered as partial support for the model instead of a strong corroboration of the model’s proposals.
A summary of the evaluation criteria results can be observed in Table 2, and the full application of the evaluation criteria on the model can be seen in Table 6.
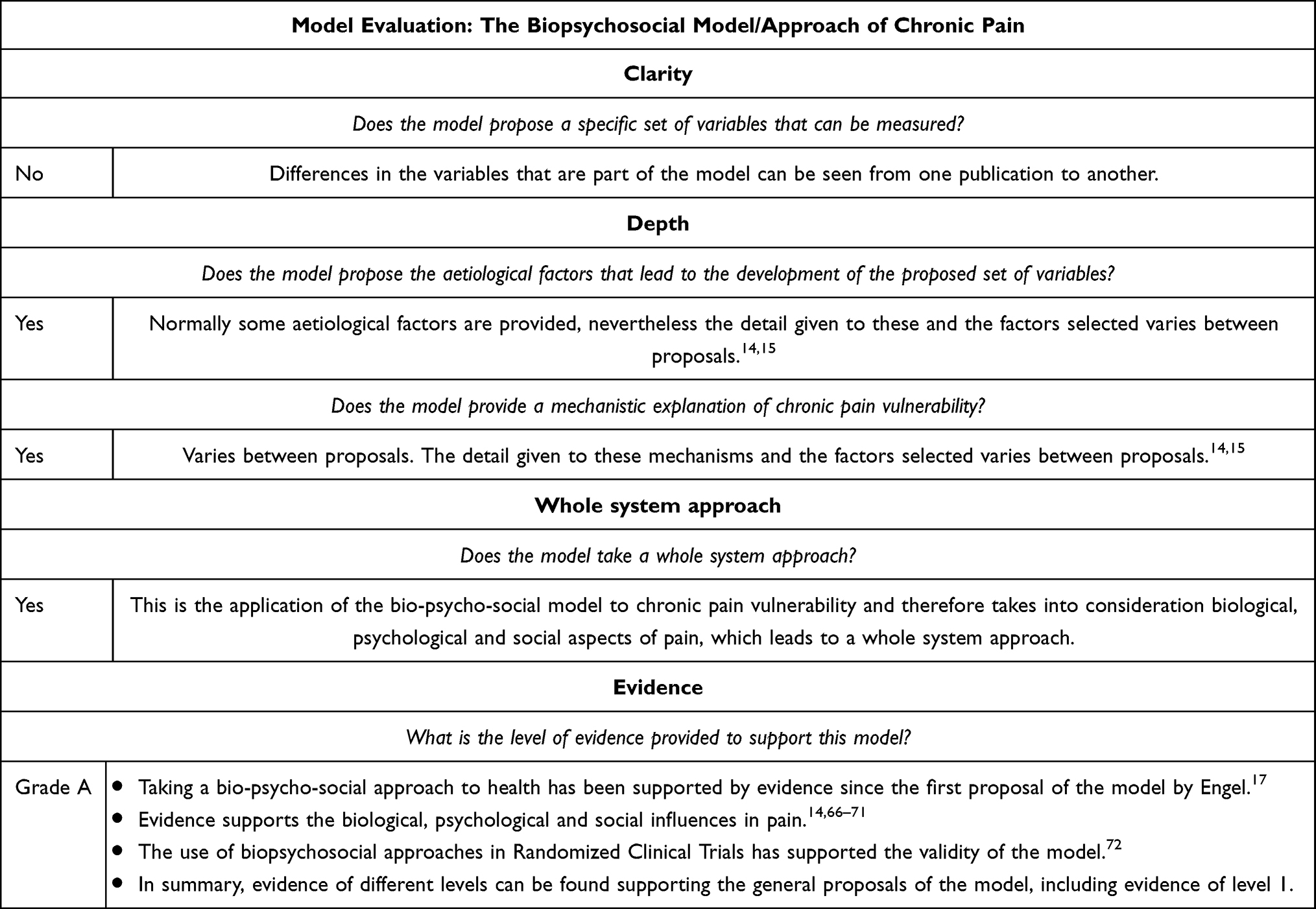 |
Table 6 Evaluation of the Biopsychosocial Model/Approach of Chronic Pain |
The Attachment-Diathesis Model of Chronic Pain19
Attachment theory is one of the most established and supported theories in psychology.73 This developmental theory states that an infant will develop an internal working model of relationships based on the early interactions they have with their primary caretaker. The internal working model is a mental representation or schema of oneself, others, and the world that will serve as a base for future appraisals, perceptions and behaviours. In general, individuals can be classified in three attachment styles: a secure attachment style, developed in those who encounter positive and sensitive interactions with their main caretaker; and two insecure attachment styles (insecure-avoidant and insecure-anxious ambivalent), for those who receive a less sensitive treatment from their caretakers.74
Since attachment style serves as the foundation of the appraisals and perceptions of an individual, the Attachment-Diathesis Model of Chronic Pain makes the following proposal: (1) When an individual is exposed to a painful stimulus the attachment style or internal working model is activated (diathesis). (2) The nature of the attachment style (secure, insecure-avoidant or insecure ambivalent) will then lead the appraisals made about the pain, one’s ability to manage it and other´s ability to provide support. (3) These appraisals will, in turn, determine the coping strategies, support-seeking behaviours and emotional states experienced. (4) Finally, these responses to the appraisals made will have an effect on each one’s experience and adjustment to pain.16
Meredith, Ownsworth and Strong16 specifically propose that those individuals with an insecure attachment will be more likely to develop chronic pain and less likely to manage it efficiently. This is due to the tendency individuals with insecure attachment have to present less adaptive appraisals (eg, higher catastrophizing, lower self-efficacy, etc.) and coping strategies (eg, emotion focused coping, denial coping, etc.).16
Different types of evidence have corroborated the proposals of this model.75–80 Overall, the theory is one of the best constructed ones, with explanations of aetiological factors and the different variables associated with them. However, although the theory is solid and supported by the evidence, the effect sizes are sometimes small81 and some contradictory findings have been encountered.82 Many potential explanations could be given for this. To begin with, we must consider that attachment is not an easy construct to measure and different methods may lead to different estimations.83 Furthermore, changes of attachment style could occur through the lifetime84 which presents numerous challenges for testing the model. The effects of attachment could be a consequence of the current attachment style or the attachment style on a critical developmental period, and if both do not match, identifying effects on chronic pain development could be challenging. To improve the quality of the model, future research could explore the temporal dynamics of the relationship between attachment and pain, perhaps through longitudinal studies. Another element that would increase the quality of the model would be the exploration of biological correlates of the proposal. Evidence already exists linking attachment with different neuroendocrine alterations.85,86 The inclusion of these elements in the model could be a way to complement the proposal and perhaps give way to the study of new methods of measurement and treatment.
Finally, we must consider that factors other than attachment will have an effect on chronic pain vulnerability. Consequently, to identify the relative importance of the proposals of the model, it would be interesting to compare them alongside other vulnerability factors. This would allow the identification of the relative weight attachment presents in comparison with other variables, and therefore, the value of their inclusion in clinical settings.
A summary of the evaluation criteria results can be observed in Table 2, and the full application of the evaluation criteria on the model can be seen in Table 7.
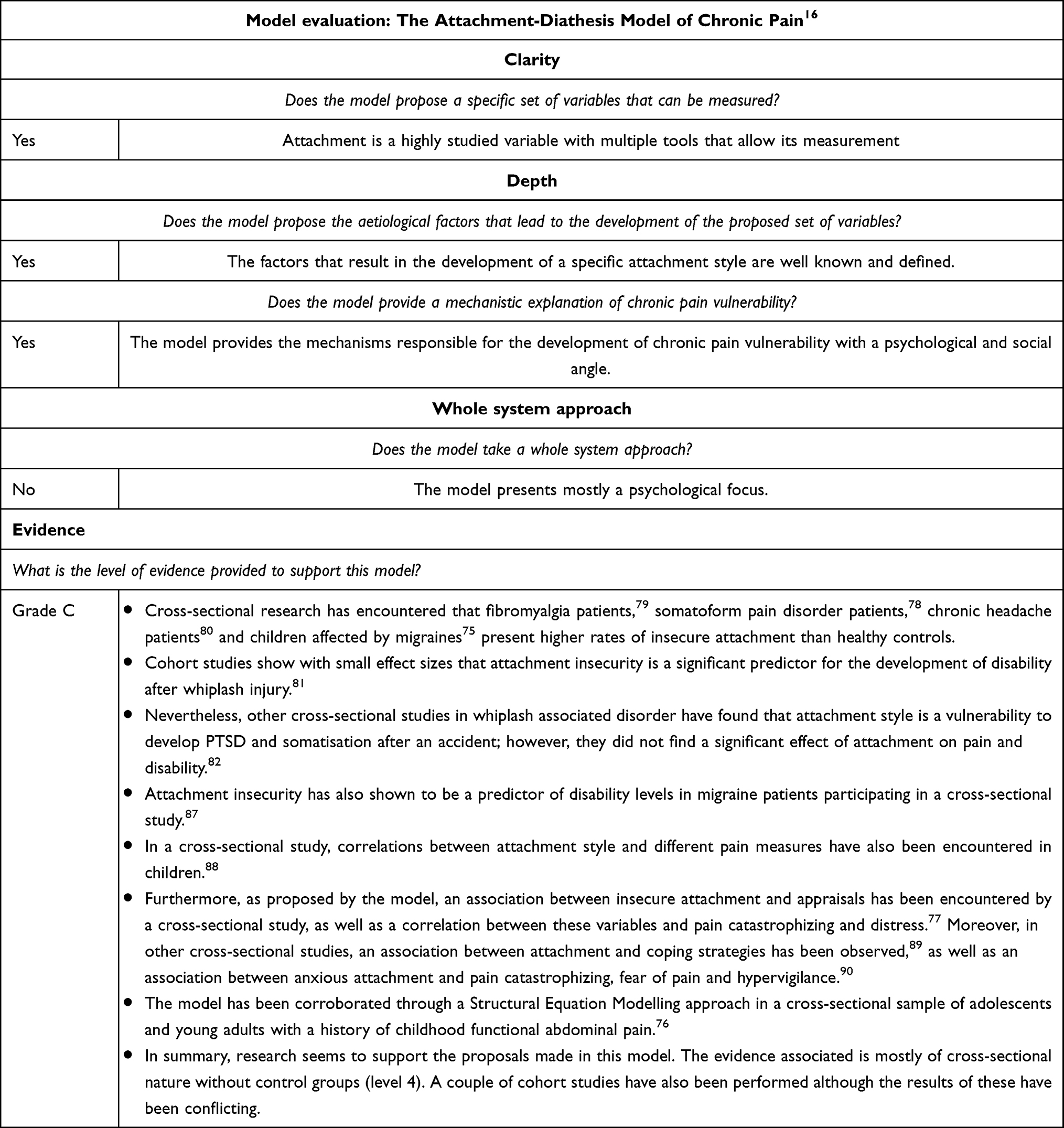 |
Table 7 Evaluation of the Attachment-Diathesis Model of Chronic Pain19 |
The Personality Hypothesis of Chronic Pain
The idea that a certain type of personality is more likely to experience chronic pain has been discussed in the pain literature for more than a century. Possibly, one of the first formal proposals of this link was made by psychoanalytic researchers and their theories surrounding the “hysteric” personality.17 Since then, research on different personality traits and chronic pain vulnerability has bloomed with variable results. The most common link is perhaps the association between neuroticism (a personality trait characterized by high emotional negativity) and the presence of clinical pain18,19 or neuroticism and psychological factors associated with pain, such as fear avoidance.91 Others have proposed that chronic pain vulnerability is driven by the presence of high harm avoidance (a temperament trait that is hypothesized to be dependent on biological traits) and low self-directedness (a character trait defined as the ability to self-adjust to achieve goals, that is hypothesized to be dependent on learning).20 In summary, certain personality traits that favour avoidance and/or catastrophizing could be a predisposing factor for chronic pain, although the effect sizes are small.18
In summary, evidence regarding the link between some personality factors18,19 and chronic pain vulnerability is present in the literature. However, some doubt has been cast into its validity with authors proposing that chronic pain might be what causes changes in personality92 and not the other way around. Evidence in this area is conflicted and characterized by small effect sizes.
Finally, social implications associated with the model call for a cautious analysis and application of this model in clinical practice. To begin with, we must consider that the ideas of the model have been around since the 19th century, which could increase the risk of dogmatic acceptance of the model. Furthermore, it is important to note that the initial ideas that inspired this model (hysteric personality) have been associated with the mistreatment of women in healthcare through history93 and seem to still have a discriminatory impact even in today’s medical settings.94
Consequently, although we cannot disregard the research that finds a link between some personality factors and pain, and it is important to point out that most research in the area has advanced from the Freudian view of chronic pain; social responsibility calls for a critical and cautious appraisal of the model, especially if we ever intend to bring it back to clinical practice. A summary of the evaluation criteria results can be observed in Table 2, and the full application of the evaluation criteria on the model can be seen in Table 8.
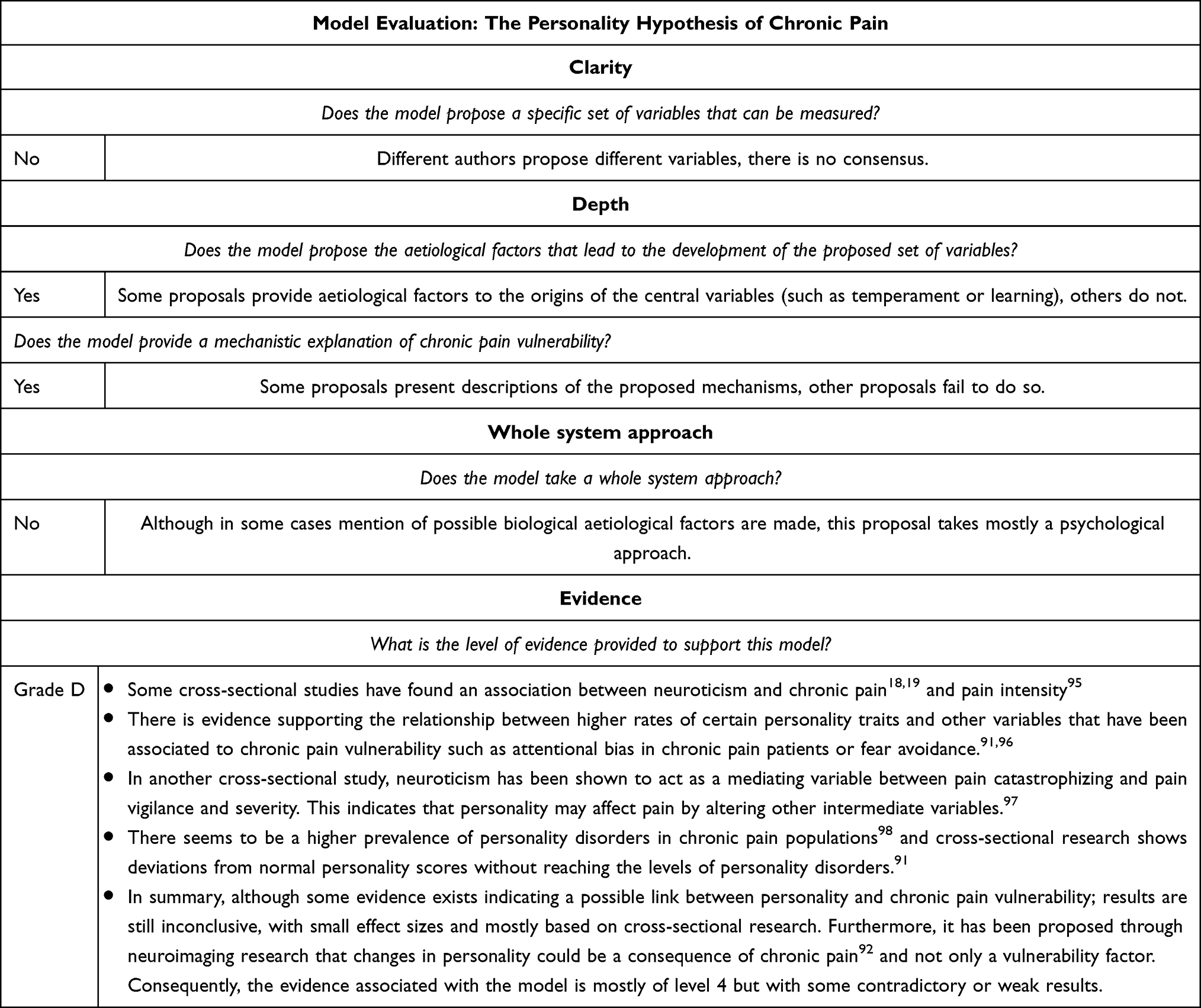 |
Table 8 Evaluation of the Personality Hypothesis of Chronic Pain |
Psychological Variables and Comorbidities
Finally, although they are not part of a model, plenty of research on chronic pain vulnerability is centred on the different psychological variables and comorbid disorders that may prompt, accelerate, exacerbate or accompany the development of a pain condition.99 Sometimes, these studies will be framed in the analysis of one of the previously presented models;33 other times, they will be part of an independent correlation study.100 On the other hand, when it comes to comorbid disorders, chronic pain has been associated with several mental health and physical health issues. Associations with depressive and anxiety disorders,101 sleep disorders,102 obesity103 and coronary disease104,105 have been encountered by many researchers. The associations proposed are mostly bidirectional and therefore, lead to the suspicion of common vulnerabilities.
It is difficult to assess the quality of these proposals since they are all framed independently and not under the same unifying theory, making it a challenge to guide investigations in the area. Consequently, the development of a synthesizing model in which the common vulnerabilities and aetiological factors for the different disorders are presented alongside the mechanisms that lead comorbidity would be a beneficial addition to the research field.
A summary of the evaluation criteria results can be observed in Table 2, and the full application of the evaluation criteria on the model can be seen in Table 9.
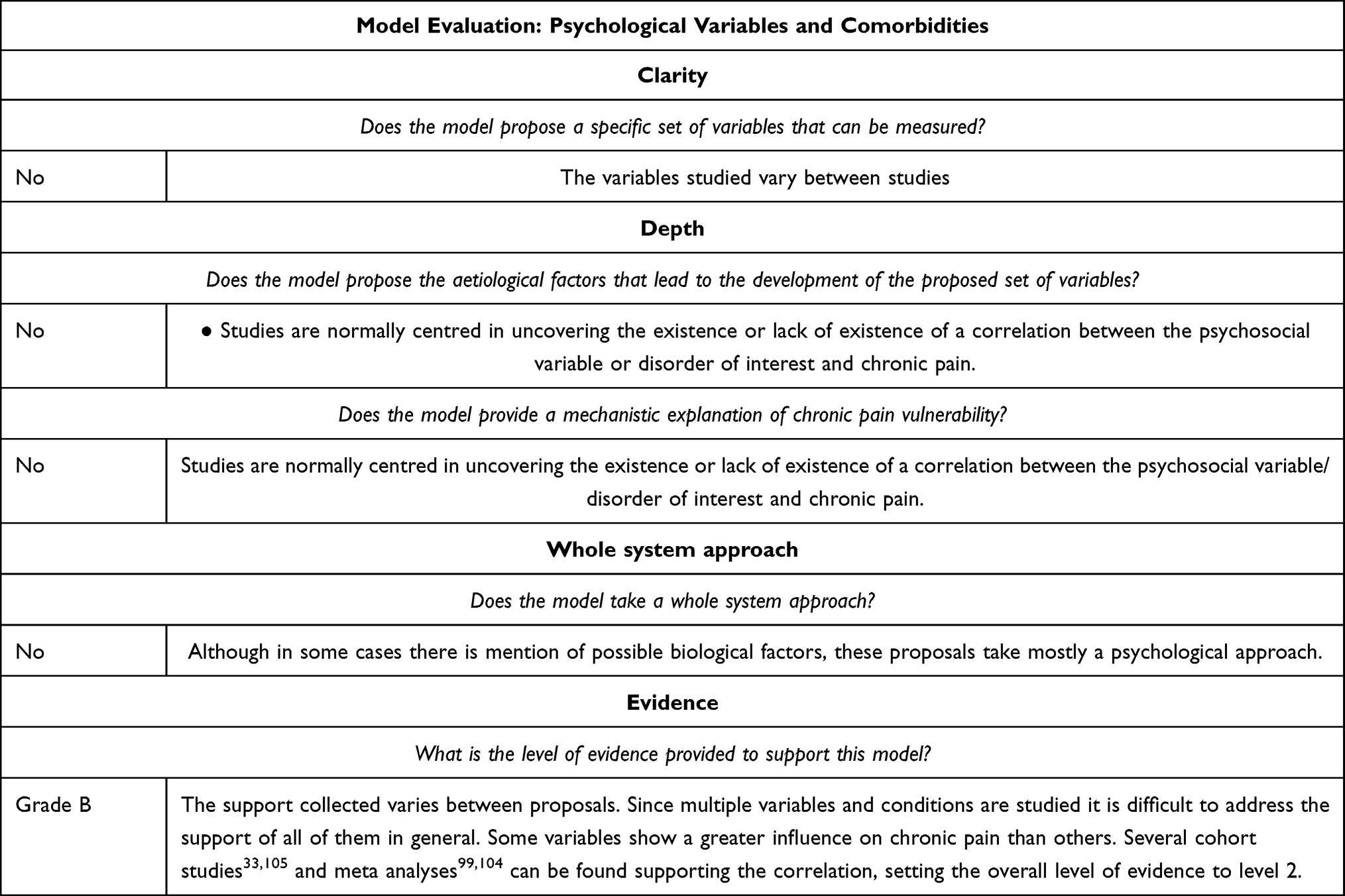 |
Table 9 Evaluation of Psychological Variables and Comorbidities Evidence |
The Developmental Approach to Chronic Pain Vulnerability24
This model proposes chronic pain as a consequence of alterations in healthy developmental processes, understanding vulnerability as a phenomenon that can be influenced by the different changes (biological, psychological and social) that occur through the lifespan. Particularly, the authors put the focus on the paediatric development of nociception and pain, long-term effects of paediatric pain and biological, psychological and socioenvironmental aging changes. It is proposed that if alterations occur in these processes, they could lead to chronic pain vulnerability.21
This idea shows good promise as a concept that could help understand the aetiology and mechanisms of chronic pain, and in fact, supporting evidence for these principles can be found in the literature. For instance, research has found that childhood pain is a predictor of adulthood pain106 and that neonatal care experiences alter the nociceptive system of children.107,108 Moreover, research has also pointed out at a potential developmental effect of parental chronic pain that influences the development of chronic pain through childhood.109 On the same line, the previously pointed out research regarding the attachment model75–80 and childhood trauma54,110,111 can also be interpreted under this model as a confirmation of the effects that developmental processes or disruptions to them can have on long-term chronic pain vulnerability. Finally, literature studying the changes in aging associated with chronic pain has also encountered supporting outcomes, with results indicating that aging is associated with changes in endogenous pain modulation.112
Although the evidence associated with the model is positive and the prospects of finding aetiological and mechanistic explanations through this approach are promising, the model still presents some limitations. These limitations are similar to the ones encountered by the bio-psycho-social model of chronic pain, namely the breath of the model impedes the identification of specific variables that could be measured in clinical settings. Consequently, future research could focus on identifying the key processes that lead vulnerability, in order to provide a more specific set of characteristics that could be used in practice to identify vulnerability.
A summary of the evaluation criteria results can be observed in Table 2, and the full application of the evaluation criteria on the model can be seen in Table 10.
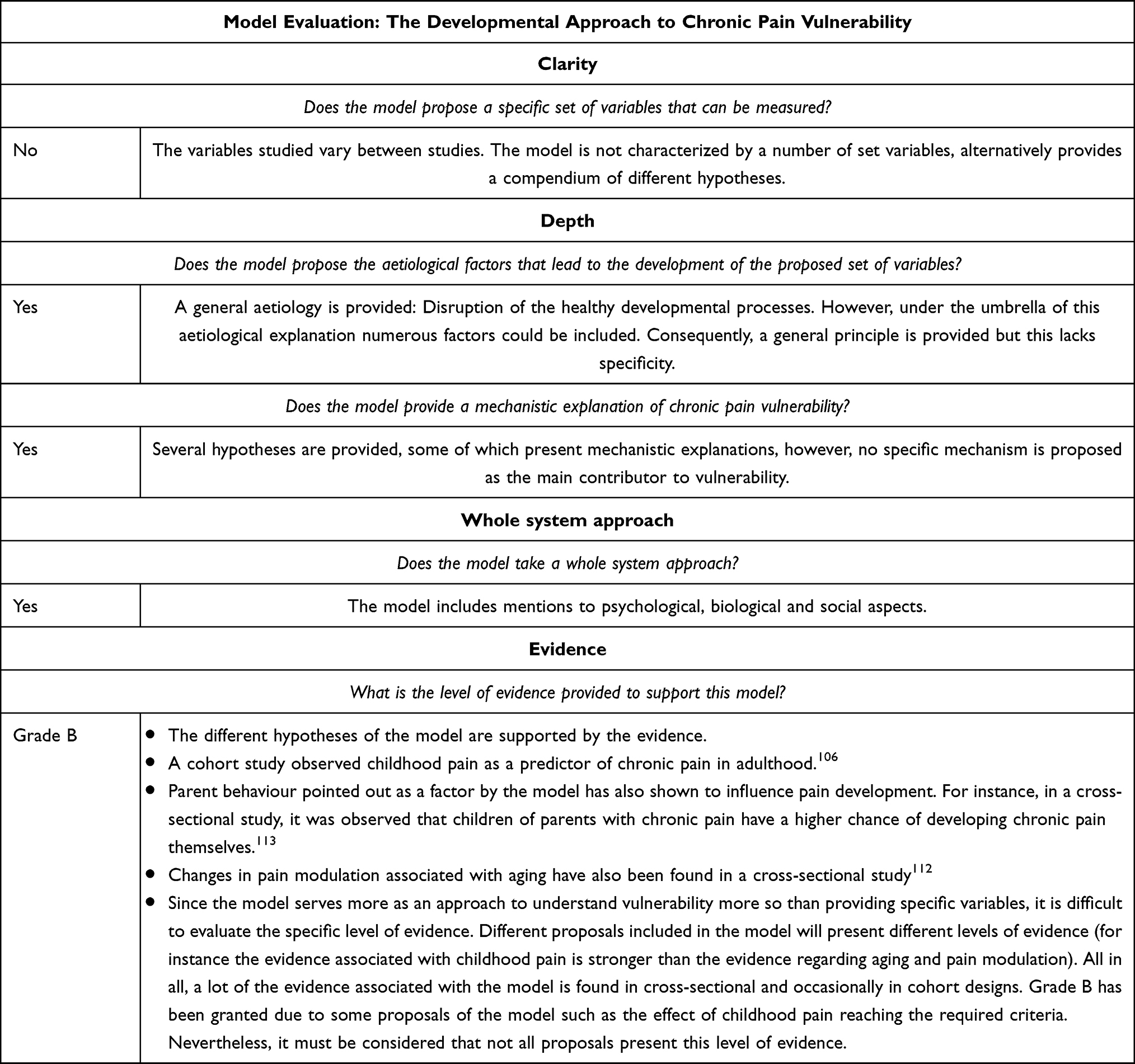 |
Table 10 Evaluation of the Developmental Approach to Chronic Pain Vulnerability Evidence24 |
Discussion
The models presented above are grounded in a large amount of research that identified variables that interact in the onset and maintenance of chronic pain. Table 2 provides a summary of the model evaluations. We found that most of the current models provided excellent specific measures and that most were also supported well by empirical evidence, indicating their validity to be used in practice. Particularly, the fear avoidance model,9,10 the diathesis-stress model,8 the shared vulnerability11 and mutual maintenance models,12 and the attachment diathesis model77 seem to be strongest on these points, whereas the personality hypothesis was the weakest. Nevertheless, all models present some limitations. Particularly, the focus of most of the models is not directed to study in-depth the aetiology of the vulnerability and the mechanisms that lead to it. Furthermore, most models take a psychological approach with little focus on biological and social factors and on the interactions between bio-psycho-social variables. In summary, the presented models do an excellent job of identifying the psychological profile for chronic pain vulnerability but do not delve into the causes of this profile or its biological correlates.
This is an understandable approach when considering the multifactorial nature of chronic pain and how difficult it can be to create an all-encompassing theory. In fact, the limitations of including multiple variables can be observed when evaluating the bio-psycho-social model of chronic pain. In this model, in contrast to the other models, a great focus is given to presenting a whole system approach and identifying aetiological and mechanistic factors. However, due to the breath in scope, the model falls short in giving specific variables that can be measured in a clinical setting to estimate individual risk.
Based on the results of this evaluation, it is clear that a middle ground between both approaches (whole-system vs specific factors) is hard to obtain. Nevertheless, certain steps can be taken based on our observations to increase the quality of the models and aid clinicians and researchers in the application and improvement of the current knowledge. To begin with, as we have mentioned throughout the text, some key variables in the more specific models (eg, anxiety sensitivity) have been questioned as to their real influence on chronic pain development. Therefore, a re-analysis of the relative importance of the different variables would be a beneficial step to take by researchers. Furthermore, another way to improve the quality of the more specific models might be to directly compare the models in terms of the predictive value of the variables that compose them. For instance, research could collect data on the main variables of the diathesis-stress model, fear avoidance model and the attachment-diathesis model, and then the predictive value of each one of the models could be compared to establish which would be the most useful for clinicians. Complementarily, a factor analysis could be performed with the variables from different models in order to identify overlapping or equivalent constructs between models, or even to establish which combination of variables offers the most information regarding vulnerability to chronic pain. Finally, another way to improve the quality of the models would be to tackle the lack of attention of each one of the models to aetiological and mechanistic factors. In this way, each one of the models could try to identify the most likely aetiological factors contributing to their key variables. For instance, the diathesis-stress model could explore the influence of traumatic life events or certain genetic predispositions on the variables of anxiety sensitivity and pain catastrophizing. It would be particularly interesting to study the mechanistic relationship between psychological and biological findings as this has been suggested to be a way to move forward in identifying the causal narrative of a disease.114
Furthermore, a mechanistic focus would encourage the use of experimental designs that go further than the observational level, to build evidence at a higher level than those currently related to the models. A way to explore the mechanistic and causal relationships may be through Randomized Controlled Trials (RCTs) in which the intervention modifies suspected causes and mechanisms in order to test whether chronic pain is prevented by specifically targeting those causes/mechanisms. For instance, an RCT in which attachment-based therapy vs other psychological treatment was delivered to a chronic pain sample would serve to whether insecure attachment is influencing pain. Nevertheless, since these may be costly and difficult to carry out, alternatives to this option exist. To begin with, instead of targeting the mechanisms of a disease through RCT, measures of a suspected mechanism could be included in RCTs exploring the effectivity of different treatments and their influence on treatment success could be explored this way. Furthermore, an alternative to RCTs has been proposed in the use of computational designs such as Bayesian predictive models.115 Particularly, in this type of design probabilistic models can be created that try to replicate the process of pain perception that the brain performs. By evaluating the ability of the models to predict real outcomes, some light can be shed into the processes that the organism is undergoing. For instance, to study the hypothesis that attachment could be influencing chronic pain vulnerability, the attachment score could be included in a Bayesian model as a prior of the weight placed on the influence of psychological states on pain perception within an experimental task or by using general pain rating scores of chronic pain. Then the predictive ability of this model could be compared to another without the inclusion of this informative prior.
Furthermore, it would also be valuable to perform prospective cohort studies to examine the prognostic factors associated with the development and maintenance of pain.
This is the first work that evaluates the quality of the different conceptual models proposed for chronic pain vulnerability. We consider this an important step to ensure both the avoidance of dogmatic acceptance of old theories and to identify the points that need further attention in future research. Nevertheless, it is also important to note that, although necessary, this work presents certain limitations. Particularly, it must be considered that the evaluation criteria have been developed based on what the literature has identified as the goals of conceptual models, but other important quality criteria could exist that have not been considered here.
Finally, it is important to mention the practical applications of the current models. As it can be seen through the evaluation, although the models show room for improvement, most of them already excel in their clarity, meaning that they provide specific factors that would be easy to measure in clinical settings. Considering this practicality and that the evidence gathered mostly supports the proposals of the models, it would already be feasible for the model variables to be used to identify those at a higher risk of developing chronic pain and therefore providing them with appropriate preventative help. These types of preventative efforts would be most suitable for patients that suffer a traumatic injury since a lot of the current evidence is based on pain chronification in this population. This way, clinical services could measure the vulnerability variables identified by the models and provide psychological help or advice to those who show high vulnerability. Regarding the specific model variables that should be used, perhaps the first option would be the ones presented by the fear avoidance model, since, of those models with good clarity, this one presents the highest quality and quantity of evidence.
In conclusion, current conceptual models for chronic pain vulnerability provide good descriptive evidence of the relationship between different psychological variables associated with chronic pain vulnerability. Nevertheless, in order to improve these models and gain more insight into what is leading the vulnerability, it would be important to explore in further detail the potential causal factors and mechanisms maintaining the condition and doing so from a bio-psycho-social approach.
Funding
Ariane Delgado-Sanchez is funded by an MRC DTP program (Award number: MR/N013751/1).
Disclosure
Ms Ariane Delgado-Sanchez reports grants from Medical Research Council (UKRI), during the conduct of the study; grants from Medical Research Council (UKRI), outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. IASP Task Force on Taxonomy. Part I: topics and Codes. Classification of Chronic Pain; IASP Press; 1994. 1.
2. Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. PAIN. 2015;156(6):1. doi:10.1097/j.pain.0000000000000160
3. Fayaz A, Croft P, Langford RM, Donaldson LJ, Jones GT. Prevalence of chronic pain in the UK: a systematic review and meta-analysis of population studies. BMJ Open. 2016;6(6):e010364. doi:10.1136/bmjopen-2015-010364
4. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287–333. doi:10.1016/j.ejpain.2005.06.009
5. Miles MB, Huberman MA. Qualitative Data Analysis: An Expanded Sourcebook. Sage publications, Inc; 1994.
6. Ward T. Why theory matters in correctional psychology. Aggress Violent Behav. 2019;48(August):36–45. doi:10.1016/j.avb.2019.08.015
7. Oxford Centre for Evidence-Based Medicine: levels of Evidence (March 2009) — centre for Evidence-Based Medicine (CEBM), University of Oxford. Available from: https://www.cebm.ox.ac.uk/resources/levels-of-evidence/oxford-centre-for-evidence-based-medicine-levels-of-evidence-march-2009.
8. Turk DC. A diathesis-stress model of chronic pain and disability following traumatic injury. Pain Res Manage. 2002;7(1):9–19. doi:10.1155/2002/252904
9. Lethem J, Slade PD, Troup JDG, Bentley G. Outline of a fear-avoidance model of exaggerated pain perception-I. Behav Res Ther. 1983;21(4):401–408. doi:10.1016/0005-7967(83)90009-8
10. Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–332. doi:10.1016/S0304-3959(99)00242-0
11. Asmundson GJG, Coons MJ, Taylor S, Katz J. PTSD and the experience of pain: research and clinical implications of shared vulnerability and mutual maintenance models. Canadian J Psychiatry. 2002;47(10):930–937. doi:10.1177/070674370204701004
12. Sharp TJ, Harvey AG. Chronic pain and posttraumatic stress disorder: mutual maintenance? Clin Psychol Rev. 2001;21(6):857–877. doi:10.1016/S0272-7358(00)00071-4
13. Engel GL. The need for a new medical model: a challenge for biomedicine. Science. 1977;196(4286):129–136. doi:10.1126/science.847460
14. Gatchel RJ, Peng YB, Peters ML, Fuchs PN, Turk DC. The biopsychosocial approach to chronic pain: scientific advances and future directions. Psychol Bull. 2007;133(4):581–624. doi:10.1037/0033-2909.133.4.581
15. Miaskowski C, Blyth F, Nicosia F, et al. A biopsychosocial model of chronic pain for older adults. Pain Med. 2019;1:1–13. doi:10.1093/pm/pnz329
16. Meredith P, Ownsworth T, Strong J. A review of the evidence linking adult attachment theory and chronic pain: presenting a conceptual model. Clin Psychol Rev. 2008;28(3):407–429. doi:10.1016/j.cpr.2007.07.009
17. Breuer J, Freud S. Studies on Hysteria. Basic Books; 1895.
18. Wranker LS, Rennemark M, Elmståhl S, Berglund J. The influence of personality traits on perception of pain in older adults - Findings from the Swedish National Study on Aging and Care - Blekinge study. Scandinavian J Pain. 2015;7:3–8. doi:10.1016/j.sjpain.2014.12.002
19. Strachan E, Poeschla B, Dansie E, Succop A, Chopko L, Afari N. Clinical and evoked pain, personality traits, and emotional states: can familial confounding explain the associations? J Psychosom Res. 2015;78(1):58–63. doi:10.1016/j.jpsychores.2014.09.019
20. Naylor B, Boag S, Gustin SM. New evidence for a pain personality? A critical review of the last 120 years of pain and personality. Scandinavian J Pain. 2017;17:58–67. doi:10.1016/j.sjpain.2017.07.011
21. Walco GA, Krane EJ, Schmader KE, Weiner DK. Applying a lifespan developmental perspective to chronic pain: pediatrics to geriatrics. J Pain. 2016;17(9):T108–T117. doi:10.1016/j.jpain.2015.11.003
22. Bigbee JL, Issel LM. Conceptual models for population-focused public health nursing interventions and outcomes: the state of the art. Public Health Nurs. 2012;29(4):370–379. doi:10.1111/j.1525-1446.2011.01006.x
23. Brady SS, Brubaker L, Fok CS, et al. Development of Conceptual Models to Guide Public Health Research, Practice, and Policy: synthesizing Traditional and Contemporary Paradigms. Health Promot Pract. 2020;21(4):510–524. doi:10.1177/1524839919890869
24. Parkkinen VP, Wallmann C, Wilde M, et al. An Introduction to Mechanisms. Evaluating Evidence of Mechanisms in Medicine: Principles and Procedures. Springer; 2018:11–21. doi:10.1007/978-3-319-94610-8_2
25. Taylor S, Zvolensky MJ, Cox BJ, et al. Robust dimensions of anxiety sensitivity: development and initial validation of the anxiety sensitivity index-3. Psychol Assess. 2007;19(2):176–188. doi:10.1037/1040-3590.19.2.176
26. Leung L. Pain Catastrophizing: an Updated Review. Indian J Psychol Med. 2012;34(3):204–217. doi:10.4103/0253-7176.106012
27. Quartana PJ, Campbell CM, Edwards RR. Pain catastrophizing: a critical review. Expert Rev Neurother. 2009;9(5):745–758. doi:10.1586/ern.09.34
28. Martin AL, Halket E, Asmundson GJG, Flora DB, Katz J. Posttraumatic stress symptoms and the diathesis-stress model of chronic pain and disability in patients undergoing major surgery. Clin J Pain. 2010;26(6):518–527. doi:10.1097/AJP.0b013e3181e15b98
29. Payne LA, Rapkin AJ, Lung KC, Seidman LC, Zeltzer LK, Tsao JCI. Pain Catastrophizing Predicts Menstrual Pain Ratings in Adolescent Girls with Chronic Pain. Pain Med. 2015;17(1):n/a–n/a. doi:10.1111/pme.12869
30. Rosenbloom BN, Katz J, Chin KYW, et al. Predicting pain outcomes after traumatic musculoskeletal injury. Pain. 2016;157(8):1733–1743. doi:10.1097/j.pain.0000000000000580
31. Cappucci S, Simons LE. Anxiety sensitivity and fear of pain in paediatric headache patients. Eur J Pain. 2015;19(2):246–252. doi:10.1002/ejp.542
32. Wong WS, Lam HM, Chow YF, et al. The effects of anxiety sensitivity, pain hypervigilance, and pain catastrophizing on quality of life outcomes of patients with chronic pain: a preliminary, cross-sectional analysis. Quality Res. 2014;23(8):2333–2341. doi:10.1007/s11136-014-0683-y
33. Slepian PM, Ankawi B, France CR. Longitudinal Analysis Supports a Fear-Avoidance Model That Incorporates Pain Resilience Alongside Pain Catastrophizing. Ann Behav Med. 2020;54(5):335–345. doi:10.1093/abm/kaz051
34. Zale EL, Ditre JW. Pain-related fear, disability, and the fear-avoidance model of chronic pain. Curr Opinion Psychol. 2015;5(5):24–30. doi:10.1016/j.copsyc.2015.03.014
35. Varallo G, Scarpina F, Giusti EM, et al. Does kinesiophobia mediate the relationship between pain intensity and disability in individuals with chronic low-back pain and obesity? Brain Sci. 2021;11(6):684. doi:10.3390/brainsci11060684
36. McGeary C, Nabity P, Reed D, et al. A test of the fear avoidance model to predict chronic pain outcomes in a polytrauma sample. NeuroRehabilitation. 2020;47(1):35–43. doi:10.3233/NRE-203084
37. Esteve R, Bendayan R, López-Martínez AE, Ramírez-Maestre C. Resilience and vulnerability factors when pain is acute as predictors of disability: findings from a two-year longitudinal study. Pain Med. 2017;18(11):2116–2125. doi:10.1093/pm/pnx053
38. Cushing CC, Kichline T, Friesen C, Schurman JV. Individual Differences in the Relationship Between Pain Fear, Avoidance, and Pain Severity in a Chronic Abdominal Pain Sample and the Moderating Effect of Child Age. Ann Behav Med. 2021;55(6):571–579. doi:10.1093/abm/kaaa096
39. Markfelder T, Pauli P. Fear of pain and pain intensity: meta-analysis and systematic review. Psychol Bull. 2020;146(5):411–450. doi:10.1037/bul0000228
40. Rogers AH, Farris SG. A meta-analysis of the associations of elements of the fear-avoidance model of chronic pain with negative affect, depression, anxiety, pain-related disability and pain intensity. Eur J Pain. 2022;26(8):1611–1635. doi:10.1002/ejp.1994
41. Jenewein J, Wittmann L, Moergeli H, Creutzig J, Schnyder U. Mutual influence of posttraumatic stress disorder symptoms and chronic pain among injured accident survivors: a longitudinal study. J Trauma Stress. 2009;20(3):n/a–n/a. doi:10.1002/jts.20453
42. Liedl A, O’Donnell M, Creamer M, et al. Support for the mutual maintenance of pain and post-traumatic stress disorder symptoms. Psychol Med. 2010;40(7):1215–1223. doi:10.1017/S0033291709991310
43. de Vries V, de Jong AEE, Hofland HWC, Van Loey NE. Pain and posttraumatic stress symptom clusters: a cross-lagged study. Front Psychol. 2021;12(May):1–8. doi:10.3389/fpsyg.2021.669231
44. Noel M, Vinall J, Tomfohr-Madsen L, Holley AL, Wilson AC, Palermo TM. Sleep Mediates the Association Between PTSD Symptoms and Chronic Pain in Youth. J Pain. 2018;19(1):67–75. doi:10.1016/j.jpain.2017.09.002
45. Lebeaut A, Zegel M, Healy NA, Rogers AH, Buser SJ, Vujanovic AA. PTSD symptom severity, pain intensity, and pain-related disability among trauma-exposed firefighters: the moderating role of mindfulness. Mindfulness. 2022;13(3):786–798. doi:10.1007/s12671-022-01836-4
46. Pozzato I, Craig A, Gopinath B, et al. Outcomes after traffic injury: mental health comorbidity and relationship with pain interference. BMC Psychiatry. 2020;20(1):1–13. doi:10.1186/s12888-020-02601-4
47. Asmundson GJG, Katz J. Understanding the co-occurrence of anxiety disorders and chronic pain: state-of-The-art. Depress Anxiety. 2009;26(10):888–901. doi:10.1002/da.20600
48. Jastrowski Mano KE, O’bryan EM, Gibler RC, Beckmann E. The co-occurrence of pediatric chronic pain and anxiety: a theoretical review of a developmentally informed shared vulnerability model. Clin J Pain. 2019;35(12):989–1002. doi:10.1097/AJP.0000000000000763
49. Unseld M, Zeilinger EL, Fellinger M, et al. Prevalence of pain and its association with symptoms of post‐traumatic stress disorder, depression, anxiety and distress in 846 cancer patients: a cross sectional study. Psycho-Oncology. 2021;30(4):504–510. doi:10.1002/pon.5595
50. López-Martínez AE, Ramírez-Maestre C, Esteve R. An examination of the structural link between post-traumatic stress symptoms and chronic pain in the framework of fear-avoidance models. Eur J Pain. 2014;18(8):1129–1138. doi:10.1002/j.1532-2149.2014.00459.x
51. Vail RE, Harridge SDR, Hodkinson PD, Green NDC, Pavlou M. A novel biopsychosocial approach to neck pain in military helicopter aircrew. Aerospace Med Human Performance. 2021;92(5):333–341. doi:10.3357/AMHP.5449.2021
52. Edwards RR, Dworkin RH, Sullivan MD, Turk DC, Wasan AD. The role of psychosocial processes in the development and maintenance of chronic pain. J Pain. 2016;17(9):T70–T92. doi:10.1016/j.jpain.2016.01.001
53. McEwen BS. Brain on stress: how the social environment gets under the skin. Proc Natl Acad Sci U S A. 2012;109(SUPPL.2):17180–17185. doi:10.1073/pnas.1121254109
54. Kumari M, Head J, Bartley M, Stansfeld S, Kivimaki M. Maternal separation in childhood and diurnal cortisol patterns in mid-life: findings from the Whitehall II study. Psychol Med. 2013;43(3):633–643. doi:10.1017/S0033291712001353
55. Slopen N, McLaughlin KA, Dunn EC, Koenen KC. Childhood adversity and cell-mediated immunity in young adulthood: does type and timing matter? Brain Behav Immun. 2013;28(1):63–71. doi:10.1016/j.bbi.2012.10.018
56. Iordanova Schistad E, Kong XY, Furberg AS, et al. A population-based study of inflammatory mechanisms and pain sensitivity. PAIN. 2019;161(2):1. doi:10.1097/j.pain.0000000000001731
57. Schistad EI, Stubhaug A, Furberg AS, Engdahl BL, Nielsen CS. C-reactive protein and cold-pressor tolerance in the general population. PAIN. 2017;158(7):1280–1288. doi:10.1097/j.pain.0000000000000912
58. Valdes AM, Ravipati S, Menni C, et al. Association of the resolvin precursor 17-HDHA, but not D-or E-series resolvins, with heat pain sensitivity and osteoarthritis pain in humans. Sci Rep. 2017;7(1):1–8. doi:10.1038/s41598-017-09516-3
59. Hannibal KE, Bishop MD. Chronic stress, cortisol dysfunction, and pain: a psychoneuroendocrine rationale for stress management in pain rehabilitation. Phys Ther. 2014;94(12):1816–1825. doi:10.2522/ptj.20130597
60. Dean E, Gormsen Hansen R. Prescribing optimal nutrition and physical activity as “first-line” interventions for best practice management of chronic low-grade inflammation associated with osteoarthritis: evidence synthesis. Arthritis. 2012;2012(2):1–28. doi:10.1155/2012/560634
61. Hajat A, Allison M, Diez-Roux AV, et al. Long-term exposure to air pollution and markers of inflammation, coagulation, and endothelial activation a repeat-measures analysis in the multi-ethnic study of atherosclerosis (Mesa). Epidemiology. 2015;26(3):310–320. doi:10.1097/eDe.0000000000000267
62. Reiss F, Meyrose AK, Otto C, Lampert T, Klasen F, Ravens-Sieberer U. Socioeconomic status, stressful life situations and mental health problems in children and adolescents: results of the German BELLA cohort-study. PLoS One. 2019;14(3):1–16. doi:10.1371/journal.pone.0213700
63. Lopez-Garcia E, Schulze MB, Fung TT, et al. Major dietary patterns are related to plasma concentrations of markers of inflammation and endothelial dysfunction. Am J Clin Nutr. 2004;80(4):1029–1035. doi:10.1093/ajcn/80.4.1029
64. Hajat A, Hsia C, O’Neill MS. Socioeconomic disparities and air pollution exposure: a global review. Curr Environ Health Rep. 2015;2(4):440–450. doi:10.1007/s40572-015-0069-5
65. Oraison HM, Kennedy GA. The effect of social support in chronic back pain: number of treatment sessions and reported level of disability. Disabil Rehabil. 2021;43(11):1526–1531. doi:10.1080/09638288.2019.1668969
66. Sweeney L, Moss-Morris R, Czuber-Dochan W, Murrells T, Norton C. Developing a better biopsychosocial understanding of pain in inflammatory bowel disease: a cross-sectional study. Eur J Gastroenterol Hepatol. 2020;32(3):335–344. doi:10.1097/MEG.0000000000001615
67. Rabbitts JA, Palermo TM, Lang EA. A conceptual model of biopsychosocial mechanisms of transition from acute to chronic postsurgical pain in children and adolescents. J Pain Res. 2020;13:3071–3080. doi:10.2147/JPR.S239320
68. Falasinnu T, Drenkard C, Bao G, Mackey S, Lim SS. The problem of pain in systemic lupus erythematosus: an explication of the role of biopsychosocial mechanisms. J Rheumatol. 2021;48(8):1279–1289. doi:10.3899/jrheum.200595
69. Schreiber KL, Zinboonyahgoon N, Flowers KM, et al. Prediction of persistent pain severity and impact 12 months after breast surgery using comprehensive preoperative assessment of biopsychosocial pain modulators. Ann Surg Oncol. 2021;28(9):5015–5038. doi:10.1245/s10434-020-09479-2
70. Martínez-Borba V, Ripoll-Server P, Yakobov E, Suso-Ribera C. Predicting the physical and mental health status of individuals with chronic musculoskeletal pain from a biopsychosocial perspective. Clin J Pain. 2021;37(3):211–218. doi:10.1097/AJP.0000000000000913
71. Murphy LK, Rights JD, Ricciuto A, Church PC, Ahola Kohut S. Biopsychosocial correlates of presence and intensity of pain in adolescents with inflammatory bowel disease. Front Pediatrics. 2020;8(September):1–9. doi:10.3389/fped.2020.00559
72. Kamper SJ, Apeldoorn AT, Chiarotto A, et al. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ. 2015;350:h444. doi:10.1136/bmj.h444
73. Sutton TE. Review of Attachment Theory: familial Predictors, Continuity and Change, and Intrapersonal and Relational Outcomes. Marriage Fam Rev. 2019;55(1):1–22. doi:10.1080/01494929.2018.1458001
74. Bowlby J. Attachment and Loss. Basic Books; 1969.
75. Esposito M, Parisi L, Gallai B, et al. Attachment styles in children affected by migraine without aura. Neuropsychiatr Dis Treat. 2013;9:1513–1519. doi:10.2147/NDT.S52716
76. Laird KT, Preacher KJ, Walker LS. Attachment and adjustment in adolescents and young adults with a history of pediatric functional abdominal pain. Clin J Pain. 2015;31(2):152–158. doi:10.1097/AJP.0000000000000090
77. Meredith PJ, Strong J, Feeney JA. Evidence of a relationship between adult attachment variables and appraisals of chronic pain. Pain Res Manage. 2005;10(4):191–200. doi:10.1155/2005/745650
78. Nacak Y, Morawa E, Tuffner D, Erim Y. Insecure attachment style and cumulative traumatic life events in patients with somatoform pain disorder: a cross-sectional study. J Psychosom Res. 2017;103(October):77–82. doi:10.1016/j.jpsychores.2017.10.003
79. Peñacoba C, Perez-Calvo S, Blanco S, Sanroman L. Attachment styles, pain intensity and emotional variables in women with fibromyalgia. Scand J Caring Sci. 2018;32(2):535–544. doi:10.1111/scs.12477
80. Savi L, Buccheri R, Tambornini A, De Martino P, Albasi C, Pinessi L. Attachment styles and headache. J Headache Pain. 2005;6(4):254–257. doi:10.1007/s10194-005-0200-3
81. Andersen TE, Sterling M, Maujean A, Meredith P. Attachment insecurity as a vulnerability factor in the development of chronic whiplash associated disorder – a prospective cohort study. J Psychosom Res. 2019;118(January):56–62. doi:10.1016/j.jpsychores.2019.01.008
82. Andersen TE, Elklit A, Vase L. The relationship between chronic whiplash-associated disorder and post-traumatic stress: attachment-anxiety may be a vulnerability factor. Eur J Psychotraumatol. 2011;2(1):5633. doi:10.3402/ejpt.v2i0.5633
83. Ravitz P, Maunder R, Hunter J, Sthankiya B, Lancee W. Adult attachment measures: a 25-year review. J Psychosom Res. 2010;69(4):419–432. doi:10.1016/j.jpsychores.2009.08.006
84. Thompson RA, Simpson JA, Berlin LJ. Taking perspective on attachment theory and research: nine fundamental questions. Attach Hum Dev. 2022;24(5):543–560. doi:10.1080/14616734.2022.2030132
85. Kidd T, Hamer M, Steptoe A. Examining the association between adult attachment style and cortisol responses to acute stress. Psychoneuroendocrinology. 2011;36(6):771–779. doi:10.1016/j.psyneuen.2010.10.014
86. Quirin M, Pruessner JC, Kuhl J. HPA system regulation and adult attachment anxiety: individual differences in reactive and awakening cortisol. Psychoneuroendocrinology. 2008;33(5):581–590. doi:10.1016/j.psyneuen.2008.01.013
87. Rossi P, Di Lorenzo G, Malpezzi MG, et al. Depressive Symptoms and Insecure Attachment as Predictors of Disability in a Clinical Population of Patients With Episodic and Chronic Migraine. J Head Face Pain. 2005;45(5):561–570. doi:10.1111/j.1526-4610.2005.05110.x
88. Failo A, Giannotti M, Venuti P. Associations between attachment and pain: from infant to adolescent. SAGE Open Med. 2019;7:205031211987777. doi:10.1177/2050312119877771
89. Andrews NE, Meredith PJ, Strong J, Donohue GF. Adult attachment and approaches to activity engagement in chronic pain. Pain Res Manage. 2014;19(6):317–327. doi:10.1155/2014/838954
90. Amini Fasakhoudi M, Abbasi Z, Bakhshipour A, Mazaheri M. Structural relationship of anxious attachment style with pain catastrophizing, fear of pain, and vigilance to pain in cases without clinical pain. Iranian J Psychiatry Behav Sci. 2022. doi:10.5812/ijpbs.111215
91. Ibrahim ME, Weber K, Courvoisier DS, Genevay S. Big five personality traits and disabling chronic low back pain: association with fear-avoidance, anxious and depressive moods. J Pain Res. 2020;13:745–754. doi:10.2147/JPR.S237522
92. Gustin SM, McKay JG, Petersen ET, Peck CC, Murray GM, Henderson LA. Subtle alterations in brain anatomy may change an individual’s personality in chronic pain. PLoS One. 2014;9(10):e109664. doi:10.1371/journal.pone.0109664
93. Tasca C, Rapetti M, Carta MG, Fadda B. Women and hysteria in the history of mental health. Clin Pract Epidemiol Ment Health. 2012;8:110–119. doi:10.2174/1745017901208010110
94. Samulowitz A, Gremyr I, Eriksson E, Hensing G. “Brave Men” and “Emotional Women”: a Theory-Guided Literature Review on Gender Bias in Health Care and Gendered Norms towards Patients with Chronic Pain. Pain Res Manag. 2018;2018:6358624. doi:10.1155/2018/6358624
95. Gharavi Roudsari E, Mousavi Nasab SMH, Ghavidel-Parsa B, Yazdi F, Khezri Moghadam N. Personality and pain intensity in rheumatoid arthritis patients: the mediating role of pain catastrophizing and cognitive emotion regulation strategies. Pers Individ Dif. 2022;186(PB):111390. doi:10.1016/j.paid.2021.111390
96. Franklin ZC, Holmes PS, Smith NC, Fowler NE. Personality type influences attentional bias in individuals with chronic back pain. PLoS One. 2016;11(1):1–12. doi:10.1371/journal.pone.0147035
97. Goubert L, Crombez G, Van Damme S. The role of neuroticism, pain catastrophizing and pain-related fear in vigilance to pain: a structural equations approach. Pain. 2004;107(3):234–241. doi:10.1016/j.pain.2003.11.005
98. Weisberg JN. Personality and personality disorders in chronic pain. Curr Rev Pain. 2000;4(1):60–70. doi:10.1007/s11916-000-0011-9
99. Martinez-Calderon J, Flores-Cortes M, Morales-Asencio JM, Luque-Suarez A. Which psychological factors are involved in the onset and/or persistence of musculoskeletal pain? An umbrella review of systematic reviews and meta-analyses of prospective cohort studies. Clin J Pain. 2020;36(8):626–637. doi:10.1097/AJP.0000000000000838
100. Khan RS, Ahmed K, Blakeway E, et al. Catastrophizing: a predictive factor for postoperative pain. Am J Surgery. 2011;201(1):122–131. doi:10.1016/j.amjsurg.2010.02.007
101. Yalcin I, Barrot M. The anxiodepressive comorbidity in chronic pain. Curr Opin Anaesthesiol. 2014;27(5):520–527. doi:10.1097/ACO.0000000000000116
102. Jank R, Gallee A, Boeckle M, Fiegl S, Pieh C. Chronic pain and sleep disorders in primary care. Pain Res Treat. 2017;2017:34–37. doi:10.1155/2017/9081802
103. Okifuji A, Hare BD. The association between chronic pain and obesity. J Pain Res. 2015;8:399–408. doi:10.2147/JPR.S55598
104. Fayaz A, Ayis S, Panesar SS, Langford RM, Donaldson LJ. Assessing the relationship between chronic pain and cardiovascular disease: a systematic review and meta-analysis. Scandinavian J Pain. 2016;13(October):76–90. doi:10.1016/j.sjpain.2016.06.005
105. McBeth J, Symmons DP, Silman AJ, et al. Musculoskeletal pain is associated with a long-term increased risk of cancer and cardiovascular-related mortality. Rheumatology. 2009;48(1):74–77. doi:10.1093/rheumatology/ken424
106. Walker LS, Dengler-Crish CM, Rippel S, Bruehl S. Functional abdominal pain in childhood and adolescence increases risk for chronic pain in adulthood. Pain. 2010;150(3):568–572. doi:10.1016/j.pain.2010.06.018
107. Hohmeister J, Demirakça S, Zohsel K, Flor H, Hermann C. Responses to pain in school-aged children with experience in a neonatal intensive care unit: cognitive aspects and maternal influences. Eur J Pain. 2009;13(1):94–101. doi:10.1016/j.ejpain.2008.03.004
108. Goffaux P, Lafrenaye S, Morin M, Patural H, Demers G, Marchand S. Preterm births: can neonatal pain alter the development of endogenous gating systems? Eur J Pain. 2008;12(7):945–951. doi:10.1016/j.ejpain.2008.01.003
109. Palermo TM, Valrie CR, Karlson CW. Family and parent influences on pediatric chronic pain: a developmental perspective. Am Psychol. 2014;69(2):142–152. doi:10.1037/a0035216
110. Davis DA, Luecken LJ, Zautra AJ. Are reports of childhood abuse related to the experience of chronic pain in adulthood? A meta-analytic review of the literature. Clin J Pain. 2005;21(5):398–405. doi:10.1097/01.ajp.0000149795.08746.31
111. Van Houdenhove B, Egle U, Luyten P. The role of life stress in fibromyalgia. Curr Rheumatol Rep. 2005;7(5):365–370. doi:10.1007/s11926-005-0021-z
112. Grashorn W, Sprenger C, Forkmann K, Wrobel N, Bingel U. Age-Dependent Decline of Endogenous Pain Control: exploring the Effect of Expectation and Depression. PLoS One. 2013;8(9):e75629. doi:10.1371/journal.pone.0075629
113. Hoftun GB, Romundstad PR, Rygg M. Association of Parental Chronic Pain With Chronic Pain in the Adolescent and Young Adult: family Linkage Data From the HUNT Study. JAMA Pediatr. 2013;167(1):61–69. doi:10.1001/jamapediatrics.2013.422
114. Thomas JG, Sharp PB. Mechanistic science: a new approach to comprehensive psychopathology research that relates psychological and biological phenomena. Clin Psychol Sci. 2019;7(2):196–215. doi:10.1177/2167702618810223
115. Jones AKP, Brown CA. Predictive mechanisms linking brain opioids to chronic pain vulnerability and resilience. Br J Pharmacol. 2018;175(14):2778–2790. doi:10.1111/bph.13840
 © 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.