Back to Journals » Nature and Science of Sleep » Volume 11
Are sleep patterns influenced by race/ethnicity – a marker of relative advantage or disadvantage? Evidence to date
Authors Johnson DA, Jackson CL ![]() , Williams NJ, Alcántara C
, Williams NJ, Alcántara C
Received 4 January 2019
Accepted for publication 9 May 2019
Published 23 July 2019 Volume 2019:11 Pages 79—95
DOI https://doi.org/10.2147/NSS.S169312
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sutapa Mukherjee
Dayna A Johnson,1,2 Chandra L Jackson,3,4 Natasha J Williams,5 Carmela Alcántara6
1Department of Epidemiology, Rollins School of Public Health, Emory University, Atlanta, GA, USA; 2Division of Sleep and Circadian Disorders, Brigham and Women’s Hospital, Boston, MA, USA; 3Department of Health and Human Services, Epidemiology Branch, National Institute on Environmental Health Sciences, National Institutes of Health, Research Triangle Park, NC, USA; 4Department of Health and Human Services, Intramural Program, National Institute of Minority Health and Health Disparities, Bethesda, MD, USA; 5Department of Population Health, New York University School of Medicine, Center for Healthful Behavior Change, New York, NY, USA; 6School of Social Work, Columbia University, New York, NY, USA
Abstract: Sleep is a fundamental necessity of life. However, sleep health and sleep disorders are not equitably distributed across racial/ethnic groups. In fact, growing research consistently demonstrates that racial/ethnic minorities are more likely to experience, for instance, shorter sleep durations, less deep sleep, inconsistent sleep timing, and lower sleep continuity in comparison to Whites. However, racial/ethnic disparities in reports of sleepiness and sleep complaints are inconsistent. Racial/ethnic groups have significant heterogeneity, yet within-group analyses are limited. Among the few published within-group analyses, there are differences in sleep between non-US-born and US-born racial/ethnic groups, but the group with the more favorable sleep profile is consistent for non-US-born Latinos compared to US-born Latinos and Whites but unclear for other racial/ethnic minority groups. These sleep health disparities are a significant public health problem that should garner support for more observational, experimental, intervention, and policy/implementation research. In this review, we 1) summarize current evidence related to racial/ethnic disparities in sleep health and within-group differences, focusing on the sleep of the following racial/ethnic minority categories that are defined by the United States Office of Management and Budget as: American Indian/Alaska Native, Asian, African American/Black, Hispanic/Latino, and Native Hawaiian/Pacific Islander; 2) discuss measurement challenges related to investigating sleep health disparities; 3) discuss potential contributors to sleep health disparities; 4) present promising interventions to address sleep health disparities; and 5) discuss future research directions on intersectionality and sleep health.
Keywords: sleep, disparities, race/ethnicity, minority, measurement
Introduction
Sleep, a modifiable health behavior that is partially nonvolitional, is integral to optimal health and quality of life. However, health disparate populations such as racial and ethnic minorities are less likely than Whites to experience optimal sleep. More specifically, “sleep health” which includes multiple dimensions of sleep, namely sufficient sleep duration, sleep continuity or efficiency, sleep timing, alertness/sleepiness and satisfaction/quality that should occur on a consistent basis,1 varies by race/ethnicity. Adverse sleep health is associated with suboptimal performance and safety as well as a host of negative mental and physical health outcomes, including accidents (eg, occupational and drowsy driving), negative mood, impaired cognition, overweight/obesity, hypertension, type 2 diabetes, stroke, cardiovascular disease (CVD), and premature mortality.2–4 For example, sleep restriction (ie, shorter sleep duration <7 hours) has been linked to an increased risk of obesity – a strong risk factor for many poor health conditions – by dysregulating hormones like leptin and ghrelin that act in concert to increase weight gain and eventually obesity through overeating.5,6 Sleep restriction may also activate reward areas of the brain that lead to hedonistic behavior or a greater propensity to overeat.7,8 Overall, these health outcomes are disproportionately more prevalent among racial/ethnic minorities, who also experience worse sleep health than Whites. Therefore, it is plausible that sleep health disparities may contribute to health disparities in general health and cardiovascular health disparities, in particular.9 For example, growing evidence suggests that disparities in sleep duration contribute to racial/ethnic disparities in blood pressure10 and cardiometabolic risk.11 Thus, racial/ethnic disparities in sleep represent a significant public health problem that deserves immediate attention including more observational, experimental, intervention, and policy as well as translational/implementation research.
In this review, we present the current scientific evidence on racial/ethnic disparities in various dimensions of sleep health, with an emphasis on sleep duration. We also briefly present some evidence regarding differences (versus disparities) in sleep. This is an important distinction as disparities relate to inequities between groups (eg, race, ethnicity) that are preventable and unfair/unjust.12 As recently defined by Duran et al,13 “a health disparity is a health difference that adversely affects defined disadvantaged populations, based on one or more health outcomes”.13 While focusing on racial/ethnic disparities in sleep health, we define race as a social (and not genetic) construct with biological consequences that result from social (including economic) and environmental determinants that are differentially experienced across racial/ethnic groups due to historical and contemporary forms of discriminatory practices and policies on the basis of race/ethnicity.14 We specifically discuss the sleep of adult racial/ethnic minority groups, including individuals who – based on the United States Office of Management and Budget categories – self-identify as American Indian/Alaska Native, Asian, African American (henceforth referred to as Black), Hispanic/Latino, and Native Hawaiian/Pacific Islander in comparison to non-Hispanic Whites (henceforth referred to as White). In addition, whenever possible, we describe the results of studies on intersecting social identities (eg, race/ethnicity and sex), which may or may not have used an intersectionality framework in their design, analyses or interpretation. Herein, we define intersectionality as a theoretical framework to understand how multiple social identities (eg, race, ethnicity, gender, sexual orientation, ability, age, socioeconomic status [SES]) interact in ways that structure and reflect interconnected systems of power, privilege, and oppression, which in turn shape social inequalities that produce health disparities.15–17 In these studies, intersectionality is often tested analytically with effect modification through explicit stratification and interactions (eg, race-sex sleep disparities).
Several prior review articles have summarized the state of the literature on racial/ethnic sleep health disparities.18–21 Our review updates and expands on these prior review articles by summarizing within-racial/ethnic group data as opposed to only discussing data between groups. We also expand beyond the more frequently studied racial/ethnic minority groups (ie, Black and Hispanic/Latino) to include data on American Indian/Alaska Native, Asian, and Native Hawaiian/Pacific Islander populations. In particular, we 1) summarize the literature on racial/ethnic disparities in sleep health or on the sleep of racial/ethnic minorities and subgroups within these populations (eg, heritage); 2) discuss measurement challenges for investigating sleep health disparities; 3) discuss potential contributors to sleep health disparities; and 4) provide future directions for the field of sleep health disparities, including a discussion of intersectionality as well as non-exhaustive current and promising interventions.
Review approach
We conducted a PubMed review of articles that pertained either to racial/ethnic disparities in sleep or to the sleep of racial/ethnic minority populations (without regard to disparities or comparisons). The following search terms were used to identify articles published in peer-reviewed journals without study design restriction: sleep disparities, racial/ethnic disparities in sleep, sleep patterns, sleep health, and American Indian/Alaska Native, Asian, African American/Black, Hispanic/Latino or Native Hawaiian/Pacific Islander and sleep. While no restrictions were placed on date of studies published, the majority of studies were not published until the early 2000s.
Racial/ethnic disparities in multiple sleep dimensions
Although sleep health disparities are understudied (compared to other health disparities), a number of articles have explicitly examined racial/ethnic disparities in sleep health.22–44 These studies varied from small community samples to large nationally-representative or population-based studies that included a range of sleep assessments, such as questionnaires for self-report, wrist actigraphy, and polysomnography (PSG). In general, racial/ethnic minorities had objectively-measured and self-reported worse sleep duration and quality than Whites (Table 1). For example, Chen et al22 reported racial/ethnic disparities in sleep using data from the Multi-Ethnic Study of Atherosclerosis (MESA), which is one of the few large-scale epidemiological studies to have in-home PSG (one night), 7-day actigraphy, and validated sleep questionnaires among a large racially/ethnically diverse (White, Black, Hispanic/Latino, Asian – of predominately Chinese descent) population from six cities across the US.22 Black, Hispanic/Latino, and Chinese participants had a shorter actigraphy-measured sleep duration and higher prevalence of short sleep (<6 hours) than Whites, [average sleep duration: 6.05 (standard deviation=1.41), 6.56 (1.37), and 6.35 (1.34) vs 6.85 (1.22), and prevalence of <6 hours of sleep: 43.4%, 31.5% and 37.1% vs 19.4%, respectively].22 Additionally, Hispanic/Latino and Chinese participants had a higher prevalence of habitual snoring than Whites (49.4% and 43.1% vs 36.0%, respectively). Black, Hispanic/Latino, and Chinese participants were more likely to report poor sleep quality than Whites (8.3%, 6.7% and 6.6% vs 5.0%).22 Similarly, among a smaller diverse sample of Asian, Black, Hispanic/Latino and White adults in the Chicago Area Sleep Study (CASS) who underwent 7-day actigraphy, sleep duration was shorter among Black (399.5 minutes), followed by Asian (409.6 minutes) and Hispanic/Latino (411.7 minutes) participants in comparison to Whites (447.4 minutes).26 However, sleep duration was longer across all racial/ethnic groups in this study than the sleep duration estimates in the MESA study. This may be attributable to the age difference between the samples – MESA participants were older than CASS participants.
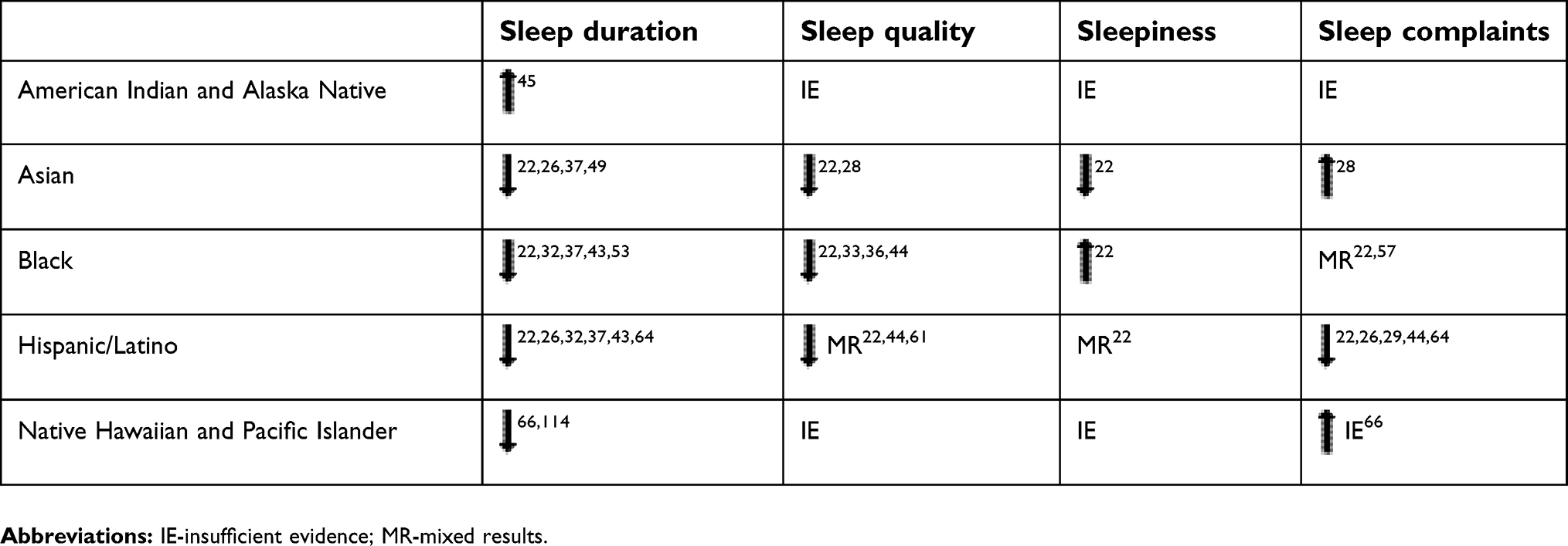 |
Table 1 Racial/ethnic disparities in selected sleep dimensions compared to non-Hispanic White adults |
In general, the most frequently assessed sleep health dimension is sleep duration, perhaps due to the ease of self-report measurement compared to sleep quality measures and sleep disorders. Inclusion of a single-item sleep duration measure is commonly utilized, particularly among US-based national datasets, such as the National Health Interview Survey (NHIS), National Health and Nutrition Examination Study (NHANES), and Behavioral Risk Factors Surveillance Study (BRFSS). The data from these national datasets provide our best population-level estimates of self-reported sleep duration. One of the earliest studies related to sleep disparities was conducted by Krueger et al32 in which pooled data from the 2004–2007 NHIS of 110,441 non-institutionalized Americans were analyzed. The authors found that Mexican American ethnicity was associated with longer self-reported sleep duration and non-Hispanic Black race/ethnicity was associated with increased odds of both short and long sleep duration relative to non-Hispanic Whites.32 These results were consistent with data from an earlier wave of NHIS.43 Using data from the 1990 supplement of the NHIS, Hale et al43 reported that both Black and Hispanic (excluding Mexican) had an increased risk of short sleep (≤6 hours/night); and Blacks had the highest risk.43 Similarly, using data from NHANES (2007–2008), Whinnery et al37 found that Blacks and Asians were more likely than Whites to report very short sleep (<5 hours).37 Contrary to the report from Krueger et al,32 Mexican Americans were less likely to report long sleep.37 These inconsistent results are further explained in the Sleep of Hispanic/Latino adultssection of this review, and highlight potentially important racial/ethnic within-group (eg, heritage or nativity, SES, sex, etc.) differences.
Although sleep duration is most commonly reported, similar patterns exist for racial/ethnic disparities in sleep quality.18 In a large racial/ethnically diverse study, Black and Hispanic/Latino vs non-Hispanic White participants had increased odds of self-reported poor sleep quality based on an overall rating of the quality of your sleep from restless to restful.44 Data from MESA also support disparities in measures of sleep quality, such as actigraphy-measured sleep efficiency, wake after sleep onset, and sleepiness between Blacks, Hispanics/Latinos, Asians, and Whites.22
In the following section, we provide a more detailed review of the sleep of racial/ethnic minority groups with a particular focus on studies that provide within-group comparisons.
Sleep of American Indian and Alaska Native adults
Few studies have investigated the sleep of American Indians and Alaska Natives. Results from the 2014 BRFSS showed that American Indians/Alaska Natives had a lower age-adjusted prevalence of healthy sleep (40.4%) compared with non-Hispanic Whites, Hispanics/Latinos, and Asians.45 A separate analysis of BRFSS data (2009–2010) showed that American Indians/Alaska Natives had a higher prevalence of insufficient sleep, defined as ≥14 days/past 30 days of not enough rest or sleep, compared to non-Hispanic Whites, 34.2% (95% confidence interval: 32.1–35.4) and 27.4% (27.1–27.6), respectively.46 This disparity was attenuated after adjustment for demographics, SES, obesity, and lifestyle factors, but was no longer statistically significant after adjustment for mental distress.
Ehlers et al47 investigated determinants of poor sleep in a community sample of 386 American Indian adults. The authors reported that short sleep (<6 hours) was more common among American Indians that were older and among those with a high degree of American Indian ancestry but not cultural identity (one's identification with his/her culture).47 Similar findings were reported for sleep quality.47 Based on the three studies that were reviewed, American Indians/Alaska Natives have a higher prevalence of poor sleep than Whites, but more studies are needed to evaluate the sleep of this population particularly with regard to sleepiness, sleep complaints, and sleep disorders. Importantly, none of the identified studies examined within-group differences in American Indians/Alaska Natives sleep health by tribal grouping, language, or setting (urban vs reservation). This is a significant scientific gap given the vast heterogeneity within the American Indian/Alaskan Native population, reflected in the existence of 567 federally recognized tribes speaking over 200 indigenous languages with various dialects who live on reservations and in urban settings.48
Sleep of Asian adults
While there are limited sleep studies with sufficient quantity of racial/ethnic minorities for explicit investigations, it is important to note that Asians are included in sleep research far less than Blacks and Hispanics/Latinos, but not less than American Indians/Alaska Natives or Native Hawaiians/Pacific Islanders. Few studies have also highlighted the specific country of origin (eg, China, Japan, India, Philippines); thus, most of the findings are limited and do not capture the full heterogeneity of this group. MESA however, enrolled a small number of Chinese adults (N=262) who underwent 7-day actigraphy and one night of in-home PSG. Chen et al22 reported that Chinese participants had a higher odds of actigraphy-measured short sleep duration (<6 hours) compared to Whites after adjustment for age, sex, and study site.22 In CASS, Carnethon et al26 assessed the sleep (using 7-day actigraphy) of Asian adults (N=109) and other racial/ethnic minority groups. In the prior study, the authors found that Asian participants had a shorter mean sleep duration (409.6 minutes) compared to White participants (447.4 minutes).26 It is important to note that, while Asians had shorter sleep durations than Whites, the sleep durations are longer than those for Black participants, but less than Hispanic/Latino participants.26
Results of the NHANES were briefly mentioned in the overview section of this review on Racial/ethnic disparities in multiple sleep dimensions, but given this is one of the largest studies to assess self-reported sleep of Asians in the US, we present more details in this section. Whinnery et al's37 analysis included almost 300 Asian adults, and found that Asians had a 2–3 fold higher odds of very short sleep (<5 hours) compared to Whites.37 Among a large robust sample of 125,610 adults, with 8,390 being Asian, Jackson et al49 found that Asian adults were more likely to report short sleep (<7 hours) than White adults, 33% compared to 28%.49 In fact, among professional and support-service occupations, the prevalence of short sleep was higher among Asian adults but no difference was observed among laborers. These results underscore the importance of exploring the social determinants of sleep.
One of the few studies that conducted within-group analyses of sleep health among an Asian population, included Malay and Indian adults who attended one of two public primary care clinics. In this study, Tan et al34 found a high prevalence of self-reported inadequate sleep (44%) defined as <7 hours of sleep on weekdays and a lower estimate on weekends (26%) among the entire sample.34 In studying ethnic differences, the authors reported that participants with Chinese ethnicity were more likely to obtain adequate sleep (≥7 hours) than Malay and Indian ethnicities during weekdays and weekends. This study is also important in that it is one of the few studies to make the distinction between insufficient sleep on weekdays and weekends, which is critical to identifying inconsistent sleep timing. Inconsistent sleep timing has been demonstrated to impact social jetlag (the discrepancy between social and biological time or between work and leisure days).68
There are also race-sex differences in the sleep quality of Asian adults. For example, Chen et al22 reported that Chinese men had a higher odds of daytime sleepiness compared to White men.22 Hale et al28 analyzed data from the Study of Women’s Health Across the Nation (SWAN), a diverse cohort of women, and compared the sleep of immigrants to their first-generation ethnic counterparts.28 The authors concluded that Chinese and Japanese immigrants were more likely to report sleep complaints (eg, difficulty falling asleep, awakenings at night, difficulty returning to sleep, and restless sleep quality) in comparison to their first-generation counterparts. This finding is inconsistent with other racial minority groups, such as Black immigrants who are less likely to report sleep complaints (discussed in further detail below).
Sleep of Black adults
Black adults are included in sleep studies more frequently and generally with larger sample sizes than other racial/ethnic minorities. As described previously, most studies report that Blacks have the highest risk and prevalence of poor sleep patterns across various dimensions of sleep health than any other racial/ethnic group.22,37 However, associations do vary based on sleep measurement and cohort demographics. This is an important distinction given the evidence demonstrating different effect estimates and more specifically differences in under/over reporting of sleep duration based on race.30,31 One of the most comprehensive studies involving a large sample of Black adults is MESA. Black participants in MESA had an approximately 5-fold higher odds of actigraphy-measured short sleep (<6 hours), and were 57% more likely to have poor sleep quality and 89% more likely to have a high Epworth Sleepiness Scale score in comparison to Whites after adjustment for demographics, SES and study site.22 In the Coronary Artery Risk Development in Young Adults (CARDIA) study of Black and White adults with wrist actigraphy, Black participants had a lower mean sleep duration in comparison to Whites.31 Similarly, in a small study of 187 adults, Mezick et al33 reported that Blacks had a shorter sleep duration and lower sleep efficiency, based on actigraphy and PSG.33 The same study also reported differences in sleep architecture such that Blacks had less time proportionately in slow wave sleep, stages 3–4 than Whites.33 These findings were consistent with two other studies of Black adults compared to White adults and adults from other racial groups.35,50 Investigators have also used sleep diaries to identify disparities. Thomas et al38 found that Blacks spent significantly more time in bed without sleeping than Whites,38 which underscores the importance of a multidimensional perspective on sleep health.
Jackson et al24 investigated Black-White disparities among 175,244 NHIS adults from 2004 to 2011 and reported that self-reported short sleep duration (<7 hours) was more prevalent in Blacks than Whites across occupation classes within many industries of employment.24 Of particular interest, short sleep duration increased with professional responsibility for Blacks but the reverse was found for Whites,24 suggesting a different sleep-SES gradient for Blacks and Whites. The authors hypothesized that the association was due to John Henryism, a unique stressor whereby marginalized populations may develop a strong work ethic as an attempt to combat/overcome negative stereotypes applied to their social identity group (eg, race).51 This coping strategy may become a stressor if their ambition is not supported by resources (eg, financial and/or emotional support). This hypothesis was corroborated with findings from the Jackson Heart Study (JHS), a large sample of Black adults in Jackson Mississippi. Johnson et al52 found that the association between stress and short sleep duration was more pronounced among those of higher (and not lower) educational attainment.52 In contrast, based on a study of 943 Black and White adults, the authors concluded that self-reported sleep quality was poorer among Black adults and those with fewer (and not more) years of educational attainment.36
BRFSS also provides population-level estimates of insufficient sleep among Blacks. Williams et al53 analyzed BRFSS data, which included 31,059 Black and White adults. Similar to the findings from NHIS, the authors found that Black participants had a 37% higher prevalence of self-reported insufficient sleep (<7 hours) in comparison to Whites.53 This estimate is much smaller than observed in the largest comprehensive study of objectively-measured sleep among Black adults, the JHS sleep study. Johnson et al54 reported that Black adults in the JHS sleep study had a 61.5% prevalence of actigraphy-measured short sleep duration (<7 hours).54 However, the BRFSS sample is a representative sample across the US, and the JHS sleep study is conducted among Black adults in Jackson, Mississippi who have a high prevalence of chronic conditions including hypertension and have higher levels of educational attainment than the general Black population.54
There are a few studies that have found no evidence of sleep disparities between Black and White adults.27 For example, among a sample of Black and White adults, there was no racial difference in sleep duration when these groups lived in similar residential environments; however, Black participants reported shorter sleep durations with increasing inflammation levels and White participants were more likely than Blacks to report shorter sleep with increasing stress and education levels.27 The lack of a Black/White sleep disparity when residing in similar environments is supported by evidence from NHIS, where Johnson et al55 reported no significant differences in sleep duration among Black and White men residing in trailers or mobile homes.55 Indeed, Black adults who lived in higher SES environments (homes or apartments) had a lower prevalence of sleep difficulties and were more likely to report waking feeling rested compared to White adults.55 Black women in lower SES environments (mobile home or trailer) had a lower prevalence of sleep difficulties than White women.55 The prior estimates were adjusted for demographics, SES, self-reported health status and region of residence. Similar findings were reported by Gaston et al56 who showed no difference in sleep duration among Black and White government-assisted renters (or public housing residents), which can serve as a proxy for low SES.56 The sleep disparities observed among higher SES groups are likely attributable to wealth disparities.
The findings regarding disparities in insomnia (eg, difficulty initiating or maintaining sleep, and early morning awakening) between Black and White adults are largely inconsistent. In the MESA study, Black adults reported insomnia more than White adults.22 Among participants of a community-based study in New York, White women had a higher prevalence of insomnia symptoms than Black women.57 In that study, insomnia complaints were defined as any report of either difficulty initiating sleep, maintaining sleep or early morning awakening. The authors suggest that the ethnicity-insomnia relationship is dependent on the degree of coping, but to our knowledge, there are no studies on coping as a protective factor for insomnia symptoms among Black adults. Given the above, it is also logical to speculate that these differences are related to measurement factors (see section on Cognitive Behavioral Therapy for Insomnia [CBT-I]).
Similar to other racial/ethnic groups, Blacks are a heterogeneous group, and it is important to investigate within-group ethnic differences in sleep, which are underexplored. The few studies that have studied within-group ethnic differences in sleep, found differences in the sleep of US born Blacks vs non-US born Blacks.41,58 Jackson et al58 reported that US and non-US-born Blacks in the NHIS (2004–2011) had a generally higher prevalence of self-reported short sleep (<7 hours) compared to other racial/ethnic groups. The authors also found that short sleep was highest among non-US-born Blacks not US-born Blacks.58 However, Jean Louis et al41 found that Caribbean Americans reported fewer sleep complaints than US-born African Americans.41 Although there are within-group ethnic differences in sleep, more research is needed to understand the sleep of the different subgroups of Blacks.
In addition to racial/ethnic disparities in sleep, there are also race-sex disparities in sleep. Researchers from CARDIA, reported race-sex disparities in sleep, such that Black men – the group with the lowest sleep duration – slept on average 82 minutes less per night than White women the group with the highest sleep duration, measured by actigraphy.31 A within-group analysis of Black adults, using data from the JHS found that Black men had a shorter average sleep duration but rated their sleep quality higher than Black women.52 Of note, emerging research suggests race-sex and sexual-orientation disparities in sleep duration. Using data from the NHIS, Trinh et al59 found that Black sexual minority women had a 52% higher prevalence of short sleep duration (<7 hours of sleep) compared to White heterosexual women after adjustment for demographics, SES, region, self-rated health, marital status, and immigrant status.59 There was no evidence of a disparity in the prevalence of short sleep duration between Black sexual minority men and heterosexual White men. Further research is needed to understand race and sexual-orientation disparities in sleep.
Sleep of Hispanic/Latino adults
Like Asian and Black racial/ethnic groups, Hispanics/Latinos are a heterogenous group, which is important to note because many studies include a general “Hispanic or Latino” racial/ethnic category without specifying the country of origin or heritage, providing disaggregated estimates. While most studies provide data on Latino-White, or Mexican-White between-group differences in sleep health dimensions, the proportion of studies on Latina/o within-group differences in sleep health outnumber those for the other racial/ethnic groups included in this review.
Using data from MESA, Chen et al22 found that Hispanics, in the aggregate, had 2–3 fold higher odds of actigraphy-measured short sleep duration (<6 hours) compared to non-Hispanic Whites in models adjusted for age, sex, and study site.22 This association was not observed when a short sleep duration category of 6–7 hours was used and compared to 7–8 hours. The odds for short sleep duration (<6 hours) were strongest among Hispanics who were younger, namely 54–64 years of age compared to their White and older aged counterparts.22 Importantly, Chen et al22 2015 did not find statistically significant differences in total sleep time between Hispanics and Whites. In contrast, using data from CASS, Carnethon et al,26 2016 found that Hispanics slept, on average, 35.7 minutes less than non-Hispanic Whites (based on actigraphy).26
Findings on Hispanic/Latino-White disparities in self-reported sleep duration are mixed and dependent on the specific Hispanic/Latino ethnic heritage group included in the sample. Specifically, while some studies have found that Other Hispanic/Latinos (those with non-Mexican ethnicity) had a 24–63% higher odds of self-reported shorter sleep duration (≤6 hours) compared to Whites,32,37,43 other studies did not document disparities in self-reported short sleep duration or mean total sleep duration between Mexican and Whites.32,43,60 Of note, when sleep duration included a very short sleep category (≤5 hours), Mexicans reported nearly a 3-fold increase in the odds of very short sleep compared to Whites.37 Much less work has focused on understanding Hispanic/Latino−White between-group differences in long sleep duration. Importantly, Chen et al22 found that in the aggregate, there were no statistically significant differences between Hispanics/Latinos and Whites in long sleep ≥8 hours measured using actigraphy.22 However, studies of self-reported long sleep have found both higher odds of self-reported long sleep (≥8 or 9 hours),32,43 and reduced odds of long sleep for Mexican Americans (and not Other Hispanics) compared to Whites.37
Overall, most studies did not find statistically significant Hispanic/Latino-White disparities on actigraphic indicators of sleep efficiency, and sleep continuity (eg, wake after sleep onset, sleep fragmentation) or self-reported sleepiness.22,26,60 For example, using PSG-based measures of sleep from the Sleep Heart Health Study, Redline et al61 found that Hispanic/Latinos did not significantly differ from Whites on indicators of sleep architecture, namely the proportion of stage 1, stage 2, stages 3–4, and sleep efficiency.61 Similarly, several studies did not find consistent statistically significant Hispanic/Latino-White between-group differences in subjectively-assessed sleep quality or insomnia symptoms, particularly after adjustment for sociodemographics and health risk behaviors.22,26,29,44 However, important disparities in sleep quality by interactions between race/ethnicity and age as well as race/ethnicity and SES have emerged. For example, Chen et al22 found evidence of greater odds of poor sleep quality only among Latinos aged 75–93 years of age compared to their ethnic and age counterparts; this was not observed for the other age groups.22 Patel et al44 also found that only Latinos below the poverty line (and not those above) had 2.57 higher odds of poor sleep quality when compared to Whites above the poverty line, though this association was no longer statistically significant after further adjustment for sociodemographics and health risk behaviors.44
Data from the largest probability-based study of Latino health, the Hispanic Community Health Study/Study of Latinos (HCHS/SOL), and the HCHS/SOL Sueño Ancillary study support differences in every dimension of sleep health by Hispanic/Latino ancestry or heritage group.62 Overall, those with Puerto Rican ancestry appear to have worse overall sleep health compared to those with Mexican ancestry. Specifically, Patel et al63 found that those with Puerto Rican and Other or Mixed Latino ancestry had 63–107% higher odds of self-reported short sleep duration (<7 hours) compared to those with Mexican ancestry.63 Puerto Rican and South Americans also had the highest prevalence of excessive daytime sleepiness at 20.6% and 22.9%, respectively.63 Relatedly, compared to those with Mexican heritage, those with Puerto Rican, Central American, and South American heritage had, on average, 12, 13, and 19 minutes shorter sleep durations based on actigraphy, respectively, even in models adjusted for demographics, behavioral, clinical, and SES factors.62 Moreover, Dudley et al62 found that those with Puerto Rican heritage had 3.4% greater actigraphy-measured mean sleep fragmentation index, 2.0% less sleep efficiency, and lower inter-daily consistency scores than those of Mexican heritage in adjusted models.62 To our knowledge only Dudley et al62 examined within Latino group variation in sleep timing on actigraphy, finding that the sleep midpoint for those with Puerto Rican heritage in Chicago was 29 minutes later than those of Mexican Heritage and 35 minutes later than those of Central American heritage in Chicago in multivariable-adjusted models.62
Study findings on the non-US-born vs US-born differences in sleep duration among Latinos are consistent and suggestive of an immigrant health advantage. Specifically, in a seminal article, Seicean et al,64 found that Mexican immigrants had 30% lower odds of short habitual sleep (<7 hours) than US-born Whites or US-born Mexican Americans in models controlling for demographics, health risk behaviors, SES, and depressive symptoms.64 Similarly, using NHIS data, Hale et al65 found that 20% of Mexican immigrants residing in the US had self-reported short sleep duration (<6.5 hours sleep/night) compared to 25.9% of US-born Mexicans. However, these differences were no longer statistically significant after further adjustment for health risk behaviors.65 Nativity status was not statistically related to short sleep duration (<7 hours) in HCHS/SOL; however, non-US-born status or immigrant status regardless of duration in US resulted in 22−29% lower odds of long-sleep (>9 hours) compared to US-born Hispanic/Latino counterparts.63
Study findings on nativity status differences in self-reported sleep quality among Hispanics/Latinos have been mixed. Hale et al28 found no statistically significant differences between Hispanic immigrants and their US-born counterparts in insomnia-based sleep complaints in the SWAN study. However, higher levels of linguistic acculturation (ie, increased English proficiency) in SWAN was associated with a 9% increase in sleep complaints among Hispanic women in race/ethnicity stratified analyses.28 Similarly, Mexican immigrants had 60–70% reduced odds of mild/moderate-to-severe insomnia symptoms compared to US-born Whites and US-born Mexican Americans.64
The interactions between race/ethnicity and sex on Hispanic/Latino sleep have been disproportionately understudied. Using data from NHANES, Seicean et al64 2011 found evidence of an immigrant health advantage in sleep duration for Mexican immigrant males and not females.64 Specifically, Mexican immigrant males had 40% lower odds of short habitual sleep (<7 hours) than US-born Whites or US-born Mexican Americans in models controlling for demographics, health risk behaviors, SES, and depressive symptoms.64 In contrast, in the same analysis, Seicean et al64 2011 found that Mexican immigrant males and females had 50–80% reduced odds of mild/moderate-to-severe insomnia symptoms compared to US-born Whites and US-born Mexican Americans in adjusted models.64 Additional sex-stratified analyses of the Mexican sample did not find evidence of an immigrant sleep health advantage after a final adjustment for language use at home.64 Jackson et al58 also examined race-sex disparities in the prevalence of short sleep duration by occupational class among Hispanics/Latinos and Whites.58 Similar to the results observed among Blacks, among the US-born, the prevalence of short sleep duration increased with increasing occupational class, with the highest prevalence observed among US-born Hispanics/Latinos working in professional management, followed by support services, and laborers compared to their US-born White counterparts in models adjusted for sociodemographics, SES, and health conditions. The sex-stratified analyses suggest that among the US-born, this work-sleep pattern is driven by US-born Hispanic/Latino women and not men. However, the Hispanic/Latino-White disparities in the work-sleep pattern was less consistent among the non-US born sample. Importantly, in one of the first studies to document race-sex and sexual-orientation disparities in sleep duration, Trinh et al found that Hispanic/Latina women sexual minorities and Hispanic/Latino men sexual minorities had 33–51% increased prevalence ratio of short sleep duration (<7 hours of sleep) compared to non-Hispanic/Latino White heterosexuals in models adjusted for demographics, SES, region, self-rated health, marital status, and immigrant status.59
Sleep of Native Hawaiian and Pacific Islander adults
As previously described, there is limited research on the sleep of racial/ethnic minorities, and the sleep of Native Hawaiians and Pacific Islanders (NHPI) is even more understudied. Researchers who have included NHPI’s in their sleep-related studies, often have too small of a sample size to make robust/stable comparisons. For example, a study by Hicken et al29 included an “Hispanic other” race category (eg, American Indians, Asians, and Pacific Islanders), which accounted for 4% of the study’s 3,094 participants. Therefore, the sample size precluded the authors ability to provide firm conclusions, in addition to the inclusion of multiple races and ethnicities into this one category making the interpretation/usefulness of results difficult.29
However, a limited number of studies have provided insight on the sleep of NHPIs. Using data from the NHPI NHIS’ ancillary study specific to NHPIs, researchers found a high prevalence (40%) of self-reported short (<7 hours) sleep duration and a low prevalence (4%) of long (>9 hours) sleep duration.66 In this study, 47.5% also reported trouble falling or staying asleep in the last week and 16.7% reported never waking up feeling well rested.66 A separate study using data from the 2009 Hawaii BRFSS, researchers reported that the prevalence of insufficient sleep was highest among Native Hawaiians compared to other racial/ethnic groups in the state.67 More studies are needed to provide additional insight (eg, potential sex differences, determinants of poor sleep) into the sleep of this particular population.
Measurement challenges for sleep duration and its potential impact on sleep disparities research
One of the major methodological challenges in the field of sleep health concerns the measurement of sleep duration. Although self-reported sleep duration is most commonly used in epidemiological studies and is used to infer population differences or disparities in sleep, a few prior research studies have determined the level of agreement between self-reported and objectively-measured sleep duration. Previous concordance studies were conducted mainly among White adults and generally found moderate correlations ranging from 0.31 to 0.47.69–71 Racial and ethnic differences in measurement error for self-reported compared to actigraphy- or PSG-measured sleep duration were investigated in several population-based epidemiological studies, including CARDIA and recently the MESA as well as the HCHS/SOL sleep ancillary studies.
Among 647 CARDIA study participants with a mean age of 42.9±3.6 years for which 58% were women and 44% Black, there was a correlation of 0.45 (0.26 for Blacks; 0.54 Whites) and a mean difference of 1.2 hours between actigraphy-measured sleep duration and sleep duration measured using the question “How many hours of sleep do you usually get at night (or when you usually sleep)?”.31 In HCHS/SOL Sueño ancillary study, there was a 1 hour and 12 minute difference between actigraphy and self-report, and a correlation of 0.43 among 2,086 Hispanics/Latinos with a mean age of 47.1±11.5 years. The self-reported data were based on bed and wake times.72 Using MESA data, Jackson et al30 found that self-reported sleep duration, as also estimated by the difference between bed and wake times on weekdays (or work/school days), only moderately correlated [ρ =0.38 overall, with correlations significantly lower only among Blacks compared with Whites (ρ =0.45 for Whites, ρ =0.28 Blacks, ρ =0.38 Hispanics/Latinos, and ρ =0.35 Chinese)] with multi-day actigraphy-measured assessments. Actigraphy-measured sleep explained only 14% of the variance in self-reported sleep duration.30 Self-reported sleep correlated even less to sleep measured by single night PSG (ρ =0.20). Furthermore, self-reported sleep duration overestimated sleep duration by an average of 64 minutes in comparison to actigraphy-measured total sleep time, 49 minutes for 5-day actigraphy-measured time in bed, and 64 minutes for sleep time based on PSG. Sleep duration was overestimated by all racial/ethnic groups when comparing self-report to both wrist actigraphy and PSG, and there was only slight-to-fair agreement (based on κ statistics) across all comparisons. Among PSG and questionnaire comparisons, racial differences in systematic bias for sleep duration were observed such that Whites were more likely to overestimate their sleep duration compared to Blacks and Chinese participants. However, Whites had significantly higher correlations for subjectively- and objectively-measured sleep duration in addition to better calibration (for some measures) compared with Blacks, which suggests greater potential for random misclassification of sleep in Blacks compared with Whites. Furthermore, the rarely investigated comparison between actigraphy and PSG revealed that data from self-report corresponded only weakly to PSG-measured sleep duration. This finding underscores the need to cautiously extrapolate findings from studies using certain measurement instruments and applying them to other studies with different instruments. Another recent study investigated agreement between in-home PSG over 2 nights, wrist actigraphy over 9 days, and prospective sleep diaries among Black, White, and Asian participants (N=223) who were of middle-to-older age. Sleep duration estimates significantly differed across all measures, and PSG was less concordant with prospective diary estimates among Blacks.73
Potential modifiers of the relationship between subjective and objective sleep duration investigated across studies include sociodemographic (eg, age, sex, race/ethnicity, educational attainment, household income, primary language spoken), health (eg, obesity, depression, self-rated health) and sleep (eg, insomnia, sleep apnea, sleepiness, sleep efficiency, sleep variability) characteristics. Based on CARDIA data, Lauderdale et al31 found that bias was closer to 0 for participants who were Black, obese, had high depression scores, high risk for sleep apnea which made the greatest difference in measurement error, high levels of sleepiness, and among participants with high sleep efficiency.31 According to MESA data, Jackson et al30 found no significant differences in measurement error for insomnia, depression, or educational attainment for each racial/ethnic group.30 Participants who spoke Chinese vs. English as the primary language overestimated their sleep time. This finding, as well as data from the Sueño study published by Cespedes et al,72 suggests there is a potential influence of culture or language on self-reported sleep duration. Matthews et al72 also found that hostility, depressive symptoms, and poor health perceptions influenced the magnitude of concordance.73
Ultimately, the main findings, which were largely consistent across studies, inform future health disparities studies seeking to determine the impact of sleep among various racial/ethnic groups. There may be an overestimation of racial differences in sleep duration based on self-reported data if Whites overestimate more than Blacks, and misclassification among racial/ethnic minorities may lead to the underestimation of racial disparities in the true association of health outcomes. Future research should both determine the necessity of including objective measures of sleep and evaluate the psychometric properties of various widely-used sleep instruments across racial/ethnic groups as self-reported sleep (eg, getting the sleep needed to feel your best) may remain important independent of objective measures. Agreement studies for other sleep measures beyond sleep duration and methodologies like sleep diaries should also be investigated among diverse populations. A recent study investigating agreement between the consensus sleep diary and a wrist-worn device Fitbit Alta among 10 healthy young adults found significant differences in recording sleep and, nonetheless, concluded that the devices could be interchangeably used with the exception of when recording wakes during the night.74 Of note, there are likely measurement error differences across diaries, characteristics like race/ethnicity and disorders like insomnia for which actigraphy is not recommended may modify the level of agreement, and the Fitbit Alta algorithms are proprietary. Ultimately, more research is warranted.
Determinants and consequences of sleep health disparities
Racial/ethnic minorities are more likely to experience social disadvantage due to historical and contemporary forms of race-based institutional and interpersonal discriminatory policies and practices. Such practices likely manifest into health disparities because of disadvantaged groups having less access to health promoting goods and services and greater exposure to health-damaging physical and social environments. More specific to sleep health disparities, there is evidence (albeit limited) that suggests psychosocial stressors, neighborhood context (physical and social), urban/inner city living, SES, access to and utilization of health care, and acculturation contribute to poor sleep health among racial/ethnic minorities as well as to racial/ethnic disparities in a host of health outcomes.18,28,65,75–81 Indeed, in race-stratified models, the associations between the neighborhood environment and short sleep (eg, <7 hours) are evident among only Black adults,78,80 illustrating the importance of the environment to sleep in this population. The aforementioned social and environmental factors also independently influence health outcomes. Sleep may modify or mediate these associations and may, therefore, be a point of intervention to improve/maintain health and address health disparities.9
Some of the general sleep health disparities observed may be partially due to time in bed and difficulty falling or staying asleep. The latter is related to insomnia-related symptoms, which are understudied among racial/ethnic minorities. It is likely that certain stressors are more strongly associated with increased insomnia-related symptoms. For example, Hicken et al29 suggested that racism-related vigilance – the anticipation of experiencing racism – may be a unique source of chronic stress that contributes to the higher prevalence of sleep difficulty among Blacks.29 Similarly, in related work with Hispanics/Latinos, Alcantara et al80 2019 found that acculturation stress – the distress associated with integrating and adapting to the US mainland culture – was a unique contributor to insomnia symptoms beyond chronic stress, sociodemographic factors, and health risk behaviors.81 However, as previously discussed, self-reported sleep difficulties are often underreported among racial/ethnic minorities. A study conducted by Jean Louis et al41 reported that Black and Caribbean Americans were less likely to report sleep difficulties, despite having more measurable sleep difficulties.41 The authors suggest that Blacks may under-report sleep complaints, which may result from perceptions regarding the undertone of how questions are phrased as judgmental (eg, complaints).18 Regarding the health consequences of these potential upstream determinants, emerging data identifies suboptimal sleep as a potential link between race and poor health outcomes, such as CVD. In a study using data from a US-based cohort study, the authors demonstrated that sleep duration accounted for the racial differences in cardiometabolic risk.11 Identifying the fundamental causes or determinants of poor sleep among racial/ethnic minority groups may reveal upstream intervention targets that could help reduce health disparities.
Approaches to mitigate sleep disparities
In addition to the importance of documenting disparities in sleep health dimensions, it is important to document the extent to which existing behavioral sleep interventions are generalizable to racial/ethnic minorities along with what approaches (if any) have been implemented in racial/ethnic minority communities. In this next section, we briefly review the major evidence-based behavioral health sleep interventions conducted, to date, and their implications for racial/ethnic minority populations discussed in this review. Of note, the vast majority of the interventions below address proximal (eg, individual factors) rather than distal or upstream factors (eg, institutional polices). Thus, described below are non-exhaustive proximal interventions that do not necessarily address the root causes (eg, social and environmental determinants caused by discriminatory practices and policies) of sleep disparities, but may help mitigate the commonly observed disparities.
Cognitive behavioral therapy for insomnia (CBT-I)
The most common behavioral intervention for insomnia is Cognitive Behavioral Therapy for Insomnia (CBT-I). CBT-I is a multicomponent treatment package that includes sleep restriction, sleep hygiene education, cognitive restructuring, stimulus control, and relaxation techniques.82 Several well-designed meta-analyses have been conducted to establish the efficacy of CBT-I and have found that it reduces sleep latency, reduces wake after sleep onset, increases sleep quality, and reduces insomnia symptoms based on the Insomnia Severity Index.83,84 Indeed, the American College of Physicians and the American Academy of Sleep Medicine recommend CBT-I as first-line therapy.85 Moreover, CBT-I improves the prognosis for co-morbid conditions including depression,86 anxiety,87 pain,87 post-traumatic stress disorder,87,88 and breast cancer.88 However, the criteria for inclusion in CBT-I trials are overly rigid89 because as many as 50% of adults experience insomnia symptoms90 but may not meet the Diagnostic and Statistical Manual V criteria for chronic insomnia disorder, which includes symptoms for at least 3 months and daytime distress or impairment.91 Therefore, a large segment of the population may not receive treatment. For racial/ethnic minority populations, this is especially important because some studies (as previously described) suggest that depending on the criteria used, racial/ethnic minorities may experience greater sleep disturbance than their White counterparts. Also important, endorsement of sleep disturbance or traditional insomnia questions, may depend on questionnaire wording. For example, Grandner et al91 found that Black adults did not report differences in “difficulty falling asleep” when compared to their White counterparts.92 However, when asked about the amount of time it takes to fall asleep, Blacks reported a longer time (indicative of longer sleep latency) than Whites.92 In other words, epidemiologic studies may underestimate this particular insomnia symptom in minorities. Additionally, there is an unsettled issue of generalizability with respect to CBT-I, because the majority of CBT-I trials were conducted among primarily White highly-educated females.93 As important, of those trials that report enrollment of racial/ethnic minorities, the sample sizes are often too small for any meaningful analyses to be conducted explicitly among these populations. As a result, we are limited in our understanding of the effectiveness of CBT-I among racial/ethnic groups. On the other hand, borrowing from CBT interventions more broadly than its use for treating insomnia, which are well-characterized therapeutic treatments, it has been argued that culturally-adapting CBT for racial/ethnic minority populations and underserved populations is necessary. For example, although the evidence is sparse, culturally adapted CBT to address mental health issues, including depression and anxiety, and smoking has produced positive results.94 These might include both surface-level and deep-level adaptations such as the incorporation of linguistic strategies, using real life individuals or role models that reflect the target community for content delivery, or incorporating cultural values into the treatment content.95 Surprisingly, to the best of our knowledge, we know of no CBT-I culturally adapted interventions in the US.
Sleep hygiene
When other sleep disorders are ruled out (ie Chronic Insomnia Disorder, Sleep Disordered Breathing), sleep hygiene education may be effective to address insufficient sleep duration (eg, sleeping too little). Notably, one factor related to insufficient sleep among racial/ethnic minority populations is limited sleep hygiene awareness and practices.96 Similarly, rigidly held beliefs about sleep can also contribute to poor sleep quality. In a study using the dysfunctional beliefs about sleep scale (DBAS-16) short form,97 the mean score reported was 4.27, (scores on the DBAS-16 range from 0 to 16 with higher scores indicating unrealistic beliefs about sleep).98 This is important because, in a study conducted by Grandner et al, Black women endorsed practices that have been shown to exacerbate sleep difficulties including “stay in bed and…read…and watch television” as well as “drink alcohol”.99 Although sleep hygiene is not recommended as a standalone intervention,100 these studies suggest that a sleep hygiene education intervention could improve sleep quality among racial/ethnic minorities without a sleep disorder. Additional research would be necessary to test an intervention of sleep hygiene and demonstrate whether culturally tailoring sleep hygiene education would be beneficial, which has been shown in other studies.94,101
Other approaches
Other types of behavioral health treatments to address sleep disturbance could include complementary and alternative approaches. In 2012, the NHIS reported 33.2% of adults used some type of complementary and alternative approach to improving well-being with yoga being the most widely used (80%).102 Yoga has been found to reduce oxidative stress,103,104 and improve psychological well-being,105 and sleep.105,106 Mindfulness is another type of complementary and alternative treatment that encourages the individual to be present in the moment, purposeful, and non-judgmental.107 Mindfulness Based Stress Reduction (MBSR) is the most common form of mindfulness used in the US.108 It includes yoga and deep breathing. MBSR therapy has garnered substantial interest in recent years and has shown promising results in improving sleep quality. One meta-analysis reported increased sleep efficiency and decreased wake after sleep onset, but it should be noted that most studies were among patients with medical morbidity.108 It appears that these complementary approaches would be a feasible and an affordable option for sleep problems amongst racial/ethnic minority populations.
A particularly important question is to what extent do these interventions need to be culturally adapted to be effective for racial/ethnic minority populations. As important, is whether or not there should be comparative studies of culturally adapted interventions vs standard interventions. While culturally adapting interventions is a time-intensive process, using data from previous trials to explore differences in treatment for minorities and non-minorities while controlling for important factors such as SES, education, relationship status in the meanwhile, will be essential for determining how minorities fare with respect to established treatment guidelines. There is at least one meta-analysis of cultural adaptations of psychological interventions which found a large (g =0.67, p<0.001) overall effect size for adapted psychological interventions compared to no intervention or other interventions, and a medium effect size (g =0.52) for the adapted versus unadapted version of the same intervention.109 Notably, none of the adapted psychological interventions targeted sleep health. Ultimately, more studies are needed to understand the effectiveness of culturally adapted sleep health interventions.
Public health and policy implications
From a public health perspective, the importance of adding sleep objectives to Healthy People 2020, the nation’s public health agenda, is an important milestone. Healthy People provides a 10-year framework for health promotion and disease prevention. Moreover, such objectives encourage community-based and health-related organizations and federal agencies to direct funds towards achieving these goals. Lamentably, the mid-year review for meeting sleep objectives includes minimum change. At present, 67.6% of adults report sufficient sleep, which is lower than the target of 70.8% for 2020.110 Strengthening the surveillance of the population’s sleep duration at local and national levels could increase the level of awareness about sleep health. Screening for sleep disorders is perhaps the most important policy implication for sleep disorders, especially in primary-care settings. It has been reported that as many as 75% of patients presenting in a non-sleep health care facility report sleep complaints.111 As is likely, there will be individuals who will be screened for sleep disorders that have, for instance, undiagnosed and therefore untreated sleep apnea. Importantly, one study found that in an urban hospital, patients who were screened for sleep apnea were more obese and had a higher apnea hypopnea index, indicating severe sleep apnea.112 Of note, racial/ethnic minorities have a high rate of undiagnosed and therefore untreated sleep apnea.22,54 Absent from the literature is the use of community-based principles in improving screening or treatment for sleep disorders. Principles of community-based approaches have a rich history in improving the uptake and adherence to important medical guidelines,113,114 and only when these trials are completed,109 will we be able to better assess to what extent can community-based approaches impact sleep health. Given that planning for Healthy People 2030 is underway, now more than ever, is it crucial to include these objectives with a particular focus on racial/ethnic minorities and from a social determinants of health perspective.
Conclusion
In conclusion, we reviewed the current state of the scientific evidence and identified important scientific gaps in the literature on the sleep of racial/ethnic minority groups. We found that the most consistent racial/ethnic disparities exist for sleep duration, which is likely attributable to sleep duration being the most studied sleep health dimension, perhaps, due to its ease of measurement. Across all the racial/ethnic minority groups studied, we found the evidence to be more consistent for short sleep duration, but less consistent findings were observed with respect to long sleep duration. Furthermore, we included a few studies that were focused on measures of sleep quality; but, among those included, we found that racial/ethnic minorities have the worst sleep quality. Although there were mixed results observed for measures of sleep quality; overall racial/ethnic minority groups, particularly Blacks, were less likely than Whites to report sleep complaints despite overall poorer sleep based on objective measures of sleep. Importantly, we found that sleep timing or circadian disruptions are disproportionately understudied among racial/ethnic minorities. Emerging evidence indicates that circadian disruptions, independent of sleep, contribute to disparities in cardiovascular outcomes;115 thus, more studies are warranted.
While few studies generally investigated within-ethnic group disparities, there was substantial evidence of within-ethnic group disparities in sleep health patterns among Asians and Hispanics/Latinos, as well as some evidence of important subgroup disparities among Black adults. Overall, for Hispanic/Latino adults, there was evidence of an immigrant health advantage for sleep duration and sleep quality (including insomnia). There were consistent disparities in sleep patterns by Latino heritage or ancestry, with evidence that those of Puerto Rican heritage/ancestry experience worse sleep profiles than those with Mexican ancestry. For Black adults the two studies reviewed found mixed results regarding an immigrant health advantage for sleep.
Equally important to advancing the field of sleep science is the need to better differentiate between a sleep health difference and a sleep health disparity in published articles.12,18 While our review has attempted to highlight racial/ethnic disparities in sleep health rather than differences, this distinction was often unclear in the literature. Future work outlining how the Institute of Medicine definition of health disparities and the recent National Institute on Minority Health and Health Disparities definition could be applied to sleep health research is warranted.12,13 As discussed in the introduction, a major trend and contribution of research on racial/ethnic minorities’ sleep health has been the analysis of sleep patterns among intersecting social identities related to age and ethnicity, gender and ethnicity, SES and ethnicity, sexual orientation and ethnicity, or nativity status and ethnicity. Of note, none of the studied reviewed overtly applied an intersectionality framework at the design stage of the research process. Future sleep health disparities research that tests intersecting social identities should apply an intersectionality framework at each stage of the research process, for example, beginning with the generation of hypotheses, sampling, operationalization, analysis, and interpretation of findings.15–17 The application of an intersectionality approach to the design, analysis, and interpretation of research on sleep health disparities not only has the potential to uncover subpopulations among marginalized populations at greatest risk for poor sleep, but to examine how these social identities are interconnected with institutional power and contribute to the root causes of sleep disparities. This type of nuanced understanding may help in the design of population-level and policy-level interventions that address root causes of sleep disparities as well as individual-level interventions that target sleep health for racial/ethnic groups.
Ultimately, there are clearly racial/ethnic disparities in sleep health that persist after adjustment for demographic, behavioral, clinical, and SES factors. The literature is strongest for sleep duration given it is the most studied dimension, which supports the need to investigate other dimensions of sleep health that may be even more directly linked in terms of biological mechanisms to particular health outcomes. Based on the evidence presented in this review, we offer the following suggestions for future research related to racial/ethnic disparities in sleep health: 1) conduct more within-group studies to identify drivers of poor sleep as subgroups are not monolithic; 2) refine measurement tools and our understanding of their utility to better and more comprehensively assess all sleep health dimensions among large, diverse populations; 3) investigate the contribution of sleep disparities to health disparities; 4) determine the potential contributions of applying an intersectionality framework to the study of sleep health; and 5) develop intervention strategies to address poor sleep among racial/ethnic minorities.
Acknowledgments
This work was, in part, supported by National Heart, Lung, and Blood Institute, K01HL138211, K23HL125939, and K23HL125748 as well as the Intramural Program at the NIH, National Institute of Environmental Health Sciences (Z1A ES103325-01).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Buysse DJ. Sleep health: can we define it? Does it matter? Sleep. 2014;37:9–17.
2. Newman AB, Spiekerman CF, Enright P, et al; The Cardiovascular Health Study Research Group. Daytime sleepiness predicts mortality and cardiovascular disease in older adults. J Am Geriatr Soc. 2000;48:115–123.
3. Altevogt BM, Colten HR, editors. Sleep Disorders and Sleep Deprivation: An Unmet Public Health Problem. National Academies Press; 2006.
4. Cai H, Shu XO, Xiang YB, et al. Sleep duration and mortality: a prospective study of 113,138 middle-aged and elderly Chinese men and women. Sleep. 2015;38:529–536. doi:10.5665/sleep.4564
5. Buxton OM, Cain SW, O’Connor SP, et al. Adverse metabolic consequences in humans of prolonged sleep restriction combined with circadian disruption. Sci Transl Med. 2012;4:129ra43.
6. Buxton OM, Pavlova M, Reid EW, Wang W, Simonson DC, Adler GK. Sleep restriction for 1 week reduces insulin sensitivity in healthy men. Diabetes. 2010;59:2126–2133. doi:10.2337/db09-0699
7. St-Onge MP, McReynolds A, Trivedi ZB, Roberts AL, Sy M, Hirsch J. Sleep restriction leads to increased activation of brain regions sensitive to food stimuli. Am J Clin Nutr. 2012;95:818–824. doi:10.3945/ajcn.111.027383
8. Chaput JP, St-Onge MP. Increased food intake by insufficient sleep in humans: are we jumping the gun on the hormonal explanation? Front Endocrinol (Lausanne). 2014;5:116. doi:10.3389/fendo.2014.00116
9. Jackson CL, Redline S, Emmons KM. Sleep as a potential fundamental contributor to disparities in cardiovascular health. Annu Rev Public Health. 2015;36:417–440. doi:10.1146/annurev-publhealth-031914-122838
10. Knutson KL, Van Cauter E, Rathouz PJ, et al. Association between sleep and blood pressure in midlife: the CARDIA sleep study. Arch Intern Med. 2009;169:1055–1061. doi:10.1001/archinternmed.2009.119
11. Curtis DS, Fuller-Rowell TE, El-Sheikh M, Carnethon MR, Ryff CD. Habitual sleep as a contributor to racial differences in cardiometabolic risk. Proc Natl Acad Sci U S A. 2017;114:8889–8894. doi:10.1073/pnas.1618167114
12. McGuire TG, Alegria M, Cook BL, Wells KB, Zaslavsky AM. Implementing the Institute of Medicine definition of disparities: an application to mental health care. Health Serv Res. 2006;41:1979–2005. doi:10.1111/hesr.2006.41.issue-5
13. Duran DG, Perez-Stable EJ. Novel approaches to advance minority health and health disparities research. Am J Public Health. 2019;109:S8–S10. doi:10.2105/AJPH.2018.304931
14. Smedley A, Smedley BD, Smedley A, Smedley BD. Race as biology is fiction, racism as a social problem is real: anthropological and historical perspectives on the social construction of race. Am Psychol. 2005;60:16–26.
15. Cole ER. Intersectionality and research in psychology. Am Psychol. 2009;64:170–180. doi:10.1037/a0014564
16. Bowleg L. The problem with the phrase women and minorities: intersectionality – an important theoretical framework for public health. Am J Public Health. 2012;102:1267–1273. doi:10.2105/AJPH.2012.300750
17. Collins PH. Intersectionality’s definitional dilemmas. Annu Rev Sociol. 2015;41:1–20. doi:10.1146/annurev-soc-073014-112142
18. Grandner MA, Williams NJ, Knutson KL, Roberts D, Jean-Louis G. Sleep disparity, race/ethnicity, and socioeconomic position. Sleep Med. 2016;18:7–18. doi:10.1016/j.sleep.2015.01.020
19. Jean-Louis G, Grandner M. Importance of recognizing sleep health disparities and implementing innovative interventions to reduce these disparities. Sleep Med. 2016;18(1–2).
20. Petrov ME, Lichstein KL. Differences in sleep between black and white adults: an update and future directions. Sleep Med. 2016;18:74–81. doi:10.1016/j.sleep.2015.01.011
21. Williams NJ, Grandne MA, Snipes A, et al. Racial/ethnic disparities in sleep health and health care: importance of the sociocultural context. Sleep Health. 2015;1:28–35. doi:10.1016/j.sleh.2014.12.004
22. Chen X, Wang R, Zee P, et al. Racial/ethnic differences in sleep disturbances: the Multi-Ethnic Study of Atherosclerosis (MESA). Sleep. 2015;38:877–888.
23. Matthews EE, Li C, Long CR, Narcisse MR, Martin BC, McElfish PA. Sleep deficiency among Native Hawaiian/Pacific Islander, Black, and White Americans and the association with cardiometabolic diseases: analysis of the National Health Interview Survey Data. Sleep Health. 2018;4:273–283. doi:10.1016/j.sleh.2018.01.004
24. Jackson CL, Redline S, Kawachi I, Williams MA, Hu FB. Racial disparities in short sleep duration by occupation and industry. Am J Epidemiol. 2013;178:1442–1451. doi:10.1093/aje/kwt028
25. Bertisch SM, Sillau S, de Boer IH, Szklo M, Redline S. 25-hydroxyvitamin D concentration and sleep duration and continuity: multi-ethnic study of atherosclerosis. Sleep. 2015;38:1305–1311. doi:10.5665/sleep.4914
26. Carnethon MR, De Chavez PJ, Zee PC, et al. Disparities in sleep characteristics by race/ethnicity in a population-based sample: Chicago Area Sleep Study. Sleep Med. 2016;18:50–55. doi:10.1016/j.sleep.2015.07.005
27. Gamaldo AA, McNeely JM, Shah MT, Evans MK, Zonderman AB. Racial differences in self-reports of short sleep duration in an urban-dwelling environment. J Gerontol B Psychol Sci Social Sci. 2015;70:568–575. doi:10.1093/geronb/gbt117
28. Hale L, Troxel WM, Kravitz HM, Hall MH, Matthews KA. Acculturation and sleep among a multiethnic sample of women: the Study of Women’s Health Across the Nation (SWAN). Sleep. 2014;37:309–317. doi:10.5665/sleep.3404
29. Hicken MT, Lee H, Ailshire J, Burgard SA, Williams DR. “Every shut eye, ain’t sleep”: the role of racism-related vigilance in racial/ethnic disparities in sleep difficulty. Race Soc Probl. 2013;5:100–112. doi:10.1007/s12552-013-9095-9
30. Jackson CL, Patel SR, Jackson WB
31. Lauderdale DS, Knutson KL, Yan LL, Liu K, Rathouz PJ. Self-reported and measured sleep duration: how similar are they? Epidemiology. 2008;19:838–845.
32. Krueger PM, Friedman EM. Sleep duration in the United States: a cross-sectional population-based study. Am J Epidemiol. 2009;169:1052–1063. doi:10.1093/aje/kwn409
33. Mezick EJ, Matthews KA, Hall M, et al. Influence of race and socioeconomic status on sleep: Pittsburgh SleepSCORE project. Psychosom Med. 2008;70:410–416. doi:10.1097/PSY.0b013e31816fdf21
34. Tan NC, Tan MS, Hwang SW, et al. Sleep time and pattern of adult individuals in primary care in an Asian urbanized community: a cross-sectional study. Medicine (Baltimore). 2016;95:e4749. doi:10.1097/MD.0000000000004864
35. Thomas KS, Bardwell WA, Ancoli-Israel S, Dimsdale JE. The toll of ethnic discrimination on sleep architecture and fatigue. Health Psychol. 2006;25:635–642. doi:10.1037/0278-6133.25.5.635
36. Turner AN, Maierhofer C, Funderburg NT, et al. High levels of self-reported prescription opioid use by HIV-positive individuals. AIDS Care. 2016;28:1559–1565. doi:10.1080/09540121.2016.1198746
37. Whinnery J, Jackson N, Rattanaumpawan P, Grandner MA. Short and long sleep duration associated with race/ethnicity, sociodemographics, and socioeconomic position. Sleep. 2014;37:601–611. doi:10.5665/sleep.3508
38. Thomas SJ, Lichstein KL, Taylor DJ, Riedel BW, Bush AJ. Epidemiology of bedtime, arising time, and time in bed: analysis of age, gender, and ethnicity. Behav Sleep Med. 2014;12:169–182. doi:10.1080/15402002.2013.778202
39. Rao U, Poland RE, Lutchmansingh P, Ott GE, McCracken JT, Lin KM. Relationship between ethnicity and sleep patterns in normal controls: implications for psychopathology and treatment. J Psychiatr Res. 1999;33:419–426. doi:10.1016/S0022-3956(99)00019-9
40. Grandner MA, Buxton OM, Jackson N, Sands-Lincoln M, Pandey A, Jean-Louis G. Extreme sleep durations and increased C-reactive protein: effects of sex and ethnoracial group. Sleep. 2013;36:769E–779E.
41. Jean-Louis G, Magai CM, Cohen CI, et al. Ethnic differences in self-reported sleep problems in older adults. Sleep. 2001;24:926–933. doi:10.1093/sleep/24.8.926
42. Hall MH, Matthews KA, Kravitz HM, et al. Race and financial strain are independent correlates of sleep in midlife women: the SWAN sleep study. Sleep. 2009;32:73–82.
43. Hale L, Do DP. Racial differences in self-reports of sleep duration in a population-based study. Sleep. 2007;30:1096–1103.
44. Patel NP, Grandner MA, Xie D, Branas CC, Gooneratne N. “Sleep disparity” in the population: poor sleep quality is strongly associated with poverty and ethnicity. BMC Public Health. 2010;10:475. doi:10.1186/1471-2458-10-475
45. Liu Y, Wheaton AG, Chapman DP, Cunningham TJ, Lu H, Croft JB. Prevalence of healthy sleep duration among adults – United States, 2014. MMWR Morb Mortal Wkly Rep. 2016;65:137–141. doi:10.15585/mmwr.mm6506a1
46. Chapman DP, Croft JB, Liu Y, Perry GS, Presley-Cantrell LR, Ford ES. Excess frequent insufficient sleep in American Indians/Alaska natives. J Environ Public Health. 2013;2013:259645. doi:10.1155/2013/259645
47. Ehlers CL, Wills DN, Lau P, Gilder DA. Sleep quality in an adult American Indian community sample. J Clin Sleep Med. 2017;13:385–391. doi:10.5664/jcsm.6486
48. Norris T, Vines PL, Hoeffel EM. The American Indian and Alaska Native Population: 2010. Washington, DC: US Department of Commerce, Economics and Statistics Administration, US Census Bureau; 2012.
49. Jackson CL, Kawachi I, Redline S, Juon HS, Hu FB. Asian-White disparities in short sleep duration by industry of employment and occupation in the US: a cross-sectional study. BMC Public Health. 2014;14:552. doi:10.1186/1471-2458-14-552
50. Tomfohr L, Pung MA, Edwards KM, Dimsdale JE. Racial differences in sleep architecture: the role of ethnic discrimination. Biol Psychol. 2012;89:34–38. doi:10.1016/j.biopsycho.2011.09.002
51. James SA, LaCroix AZ, Kleinbaum DG, Strogatz DS. John Henryism and blood pressure differences among black men. II. The role of occupational stressors. J Behav Med. 1984;7:259–275.
52. Johnson DA, Lisabeth L, Lewis TT, et al. The contribution of psychosocial stressors to sleep among African Americans in the Jackson Heart Study. Sleep. 2016;39:1411–1419. doi:10.5665/sleep.5974
53. Williams NJ, Grandner MA, Wallace DM, et al. Social and behavioral predictors of insufficient sleep among African Americans and Caucasians. Sleep Med. 2016;18:103–107. doi:10.1016/j.sleep.2015.02.533
54. Johnson DA, Guo N, Rueschman M, Wang R, Wilson JG, Redline S. Prevalence and correlates of obstructive sleep apnea among African Americans: the Jackson Heart Sleep Study. Sleep. 2018;41. doi:10.1093/sleep/zsy024
55. Johnson DA, Thorpe RJ, McGrath JA, Jackson WB, Jackson CL. Black-white differences in housing type and sleep duration as well as sleep difficulties in the United States. Int J Environ Res Public Health. 2018;15. doi:10.3390/ijerph15061188
56. Gaston SA, Jackson WB
57. Jean-Louis G, Magai C, Consedine NS, et al. Insomnia symptoms and repressive coping in a sample of older Black and White women. BMC Womens Health. 2007;7:1. doi:10.1186/1472-6874-7-1
58. Jackson CL, Hu FB, Redline S, Williams DR, Mattei J, Kawachi I. Racial/ethnic disparities in short sleep duration by occupation: the contribution of immigrant status. Soc Sci Med. 2014;118:71–79. doi:10.1016/j.socscimed.2014.07.059
59. Trinh MH, Agenor M, Austin SB, Jackson CL. Health and healthcare disparities among U.S. women and men at the intersection of sexual orientation and race/ethnicity: a nationally representative cross-sectional study. BMC Public Health. 2017;17:964. doi:10.1186/s12889-017-4937-9
60. Johnson DA, Brown DL, Morgenstern LB, Meurer WJ, Lisabeth LD. The association of neighborhood characteristics with sleep duration and daytime sleepiness. Sleep Health. 2015;1:148–155. doi:10.1016/j.sleh.2015.06.002
61. Redline S, Kirchner HL, Quan SF, Gottlieb DJ, Kapur V, Newman A. The effects of age, sex, ethnicity, and sleep-disordered breathing on sleep architecture. Arch Intern Med. 2004;164:406–418. doi:10.1001/archinte.164.4.406
62. Simonelli G, Dudley KA, Weng J, et al. Neighborhood factors as predictors of poor sleep in the sueno ancillary study of the hispanic community health study/study of Latinos. Sleep. 2017;40. doi:10.1093/sleep/zsw025
63. Patel SR, Sotres-Alvarez D, Castaneda SF, et al. Social and health correlates of sleep duration in a US hispanic population: results from the hispanic community health study/study of Latinos. Sleep. 2015;38:1515–1522. doi:10.5665/sleep.5036
64. Seicean S, Neuhauser D, Strohl K, Redline S. An exploration of differences in sleep characteristics between Mexico-born US immigrants and other Americans to address the Hispanic Paradox. Sleep. 2011;34:1021–1031. doi:10.5665/SLEEP.1154
65. Hale L, Rivero-Fuentes E. Negative acculturation in sleep duration among Mexican immigrants and Mexican Americans. J Immigr Minor Health. 2011;13:402–407. doi:10.1007/s10903-009-9284-1
66. Young MC, Gerber MW, Ash T, Horan CM, Taveras EM. Neighborhood social cohesion and sleep outcomes in the Native Hawaiian and Pacific Islander National Health Interview Survey. Sleep. 2018;41. doi:10.1093/sleep/zsy024
67. Reyes-Salvail F, Liang S, McKnight-Eily L. Sleep related prevalence and associations with selected health indicators. Hawaii State, Department of Health Special Report. 2010. Publication by the Hawaii State Department of Health. Available from: https://health.hawaii.gov/brfss/files/2013/11/Sleep_related.pdf
68. Wittmann M, Dinich J, Merrow M, Roenneberg T. Social jetlag: Misalignment of biological and social time. Chronobiology international. 2006 Jan 1;23 (1–2):497-509. doi:10.1080/07420520500545979
69. Goodwin JL, Silva GE, Kaemingk KL, Sherrill DL, Morgan WJ, Quan SF. Comparison between reported and recorded total sleep time and sleep latency in 6- to 11-year-old children: the Tucson Children’s Assessment of Sleep Apnea Study (TuCASA). Sleep Breath. 2007;11:85–92. doi:10.1007/s11325-006-0086-6
70. Girschik J, Fritschi L, Heyworth J, Waters F. Validation of self-reported sleep against actigraphy. J Epidemiol. 2012;22:462–468.
71. Van Den Berg JF, Van Rooij FJ, Vos H, et al. Disagreement between subjective and actigraphic measures of sleep duration in a population-based study of elderly persons. J Sleep Res. 2008;17:295–302. doi:10.1111/j.1365-2869.2008.00638.x
72. Cespedes EM, Hu FB, Redline S, et al. Comparison of self-reported sleep duration with actigraphy: results from the Hispanic Community Health Study/Study of Latinos Sueno Ancillary Study. Am J Epidemiol. 2016;183:561–573. doi:10.1093/aje/kwv251
73. Matthews KA, Patel SR, Pantesco EJ, et al. Similarities and differences in estimates of sleep duration by polysomnography, actigraphy, diary, and self-reported habitual sleep in a community sample. Sleep Health. 2018;4:96–103. doi:10.1016/j.sleh.2017.10.011
74. Liu J, Wong WT, Zwetsloot IM, Hsu YC, Tsui KL. Preliminary agreement on tracking sleep between a wrist-worn device fitbit alta and consensus sleep diary. Telemed J E Health. 2019. doi:10.1089/tmj.2018.0202
75. Kingsbury JH, Buxton OM, Emmons KM. Sleep and its relationship to racial and ethnic disparities in cardiovascular disease. Curr Cardiovasc Risk Rep. 2013;7. doi:10.1007/s12170-013-0330-0
76. Alcantara C, Patel SR, Carnethon M, et al. Stress and sleep: results from the Hispanic Community Health Study/Study of Latinos Sociocultural Ancillary Study. SSM Popul Health. 2017;3:713–721. doi:10.1016/j.ssmph.2017.08.004
77. Slopen N, Lewis TT, Williams DR. Discrimination and sleep: a systematic review. Sleep Med. 2016;18:88–95. doi:10.1016/j.sleep.2015.01.012
78. Owens SL, Hunte HER, Sterkel A, Johnson DA, Johnson-Lawrence V. Association between discrimination and objective and subjective sleep measures in the midlife in the United States Study Adult Sample. Psychosom Med. 2017;79:469–478. doi:10.1097/PSY.0000000000000428
79. Simonelli G, Dudley KA, Weng J, et al. Neighborhood factors as predictors of poor sleep in the sueno ancillary study of the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Sleep. 2016;40(1):zsw025.
80. Johnson DA, Hirsch JA, Moore KA, Redline S, Diez Roux AV. Associations between the built environment and objective measures of sleep: the Multi-Ethnic Study of Atherosclerosis. Am J Epidemiol. 2018;187:941–950. doi:10.1093/aje/kwx302
81. Alcantara C, Gallo LC, Wen J, et al. Employment status and the association of sociocultural stress with sleep in the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Sleep. 2019;42. doi:10.1093/sleep/zsz002
82. Murtagh DR, Greenwood KM. Identifying effective psychological treatments for insomnia: a meta-analysis. J Consult Clin Psychol. 1995;63:79–89.
83. Morin CM, Culbert JP, Schwartz SM. Nonpharmacological interventions for insomnia: a meta-analysis of treatment efficacy. Am J Psychiatry. 1994;151:1172–1180. doi:10.1176/ajp.151.8.1172
84. Smith S. Measurement of insomnia: assessement, diagnosis, and outcome evalutation. Aust J Psychol. 1994;54:56–57.
85. Qaseem A, Kansagara D, Forciea MA, Cooke M, Denberg TD; Clinical Guidelines Committee of the American College of Physicians. Management of chronic insomnia disorder in adults: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2016;165:125–133. doi:10.7326/M15-2175
86. Manber R, Edinger JD, Gress JL, San Pedro-Salcedo MG, Kuo TF, Kalista T. Cognitive behavioral therapy for insomnia enhances depression outcome in patients with comorbid major depressive disorder and insomnia. Sleep. 2008;31:489–495.
87. Wu JQ, Appleman ER, Salazar RD, Ong JC. Cognitive behavioral therapy for insomnia comorbid with psychiatric and medical conditions: a meta-analysis. JAMA Intern Med. 2015;175:1461–1472. doi:10.1001/jamainternmed.2015.3006
88. Geiger-Brown JM, Rogers VE, Liu W, Ludeman EM, Downton KD, Diaz-Abad M. Cognitive behavioral therapy in persons with comorbid insomnia: a meta-analysis. Sleep Med Rev. 2015;23:54–67. doi:10.1016/j.smrv.2014.11.007
89. Roehrs T, Verster JC, Koshorek G, Withrow D, Roth T. How representative are insomnia clinical trials? Sleep Med. 2018;51:118–123. doi:10.1016/j.sleep.2018.06.003
90. Ohayon MM. Epidemiology of insomnia: what we know and what we still need to learn. Sleep Med Rev. 2002;6:97–111.
91. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders.
92. Grandner MA, Patel NP, Gehrman PR, et al. Who gets the best sleep? Ethnic and socioeconomic factors related to sleep complaints. Sleep Med. 2010;11:470–478. doi:10.1016/j.sleep.2009.10.006
93. Van Straten A, Van der Zweerde T, Kleiboer A, Cuijpers P, Morin CM, Lancee J. Cognitive and behavioral therapies in the treatment of insomnia: a meta-analysis. Sleep Med Rev. 2018;38:3–16. doi:10.1016/j.smrv.2017.02.001
94. Kreuter MW, Strecher VJ, Glassman B. One size does not fit all: the case for tailoring print materials. Ann Behav Med. 1999;21:276–283. doi:10.1007/BF02895958
95. Resnicow K, Baranowski T, Ahluwalia JS, Braithwaite RL. Cultural sensitivity in public health: defined and demystified. Ethn Dis. 1999;9:10–21.
96. Shaw R, McKenzie S, Taylor T, et al. Beliefs and attitudes toward obstructive sleep apnea evaluation and treatment among blacks. J Natl Med Assoc. 2012;104:510–519.
97. Morin CM, Vallieres A, Ivers H. Dysfunctional beliefs and attitudes about sleep (DBAS): validation of a brief version (DBAS-16). Sleep. 2007;30:1547–1554.
98. Williams NJ, Jean-Louis G, Ceide ME, et al. Effect of maladaptive beliefs and attitudes about sleep among community-dwelling African American men at risk for obstructive sleep apnea. J Sleep Disord Ther. 2017;6. doi:10.4172/2167-0277
99. Grandner MA, Patel NP, Jean-Louis G, et al. Sleep-related behaviors and beliefs associated with race/ethnicity in women. J Natl Med Assoc. 2013;105:4–15.
100. Morgenthaler T, Kramer M, Alessi C, et al., American Academy of SleepMedicine. Practice parameters for the psychological and behavioral treatment of insomnia: an update. An American Academy of Sleep Medicine report. Sleep. 2006;29:1415–1419.
101. Kreuter M, Haughton L. Integrating culture into health information for African American Women. Am Behav Sci. 2006;49:794–811. doi:10.1177/0002764205283801
102. Clarke TC, Black LI, Stussman BJ, Barnes PM, Nahin RL. Trends in the use of complementary health approaches among adults: United States, 2002–2012. Natl Health Stat Report. 2015;1–16.
103. Dusek JA, Otu HH, Wohlhueter AL, et al. Genomic counter-stress changes induced by the relaxation response. PLoS One. 2008;3:e2576. doi:10.1371/journal.pone.0002576
104. Patil SG, Dhanakshirur GB, Aithala MR, Naregal G, Das KK. Effect of yoga on oxidative stress in elderly with grade-I hypertension: a randomized controlled study. J Clin Diagn Res. 2014;8:BC04–BC07. doi:10.7860/JCDR/2014/9498.4586
105. Trent NL, Miraglia M, Dusek JA, Pasalis E, Khalsa SBS. Improvements in psychological health following a residential yoga-based program for frontline professionals. J Occup Environ Med. 2018;60:357–367. doi:10.1097/JOM.0000000000001216
106. Zeichner SB, Zeichner RL, Gogineni K, Shatil S, Ioachimescu O. Cognitive behavioral therapy for insomnia, mindfulness, and yoga in patients with breast cancer with sleep disturbance: a literature review. Breast Cancer (Auckl). 2017;11:1178223417745564.
107. Kabat-Zinn J. Bringing mindfulness to medicine: an interview with Jon Kabat-Zinn, PhD. Interview by Karolyn Gazella. Adv Mind Body Med. 2005;21:22–27.
108. Haller H, Winkler MM, Klose P, Dobos G, Kummel S, Cramer H. Mindfulness-based interventions for women with breast cancer: an updated systematic review and meta-analysis. Acta Oncol. 2017;56:1665–1676. doi:10.1080/0284186X.2017.1342862
109. Williams NJ, Robbins R, Rapoport D, et al. Tailored approach to sleep health education (TASHE): study protocol for a web-based randomized controlled trial. Trials. 2016;17:585. doi:10.1186/s13063-016-1701-x
110. USDHHS. Healthy People 2020. Available from: http://www. healthypeople.gov/2020/topicsobjectives2020/objectiveslist.
111. Kaufmann CN, Spira AP, Rae DS, West JC, Mojtabai R. Sleep problems, psychiatric hospitalization, and emergency department use among psychiatric patients with Medicaid. Psychiatr Serv. 2011;62:1101–1105. doi:10.1176/ps.62.9.pss6209_1101
112. Tran D, Wallace J. Obstructive sleep apnea syndrome in a publicly funded healthcare system. J Natl Med Assoc. 2005;97:370–374.
113. Israel BA, Coombe CM, Cheezum RR, et al. Community-based participatory research: a capacity-building approach for policy advocacy aimed at eliminating health disparities. Am J Public Health. 2010;100:2094–2102. doi:10.2105/AJPH.2009.170506
114. Seixas AA, Trinh-Shevrin C, Ravenell J, Ogedegbe G, Zizi F, Jean-Louis G. Culturally tailored, peer-based sleep health education and social support to increase obstructive sleep apnea assessment and treatment adherence among a community sample of blacks: study protocol for a randomized controlled trial. Trials. 2018;19:519. doi:10.1186/s13063-018-2835-9
115. Egan KJ, Knutson KL, Pereira AC, von Schantz M. The role of race and ethnicity in sleep, circadian rhythms and cardiovascular health. Sleep Med Rev. 2017;33:70–78. doi:10.1016/j.smrv.2016.05.004
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.