Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
Are Real-World Mobility Patterns Early Indicators of COPD Onset? Insights from Wrist-Worn Sensors
Authors Fernandez N, Wong AY ![]() , Brodie MA, Van Schooten KS, Chan LLY, Lord SR
, Brodie MA, Van Schooten KS, Chan LLY, Lord SR
Received 25 February 2026
Accepted for publication 28 May 2026
Published 17 July 2026 Volume 2026:21 605234
DOI https://doi.org/10.2147/COPD.S605234
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Zijing Zhou
Nelida Fernandez,1 Arnold YL Wong,2 Matthew A Brodie,3 Kimberley S Van Schooten,4,5 Lloyd L Y Chan,4,6,* Stephen R Lord4,5,*
1Department of Geriatrics, Getafe University Hospital, Madrid, Spain; 2Department of Rehabilitation Sciences, The Hong Kong Polytechnic University, Hong Kong Special Administrative Region, People’s Republic of China; 3School of Biomedical Engineering, University of New South Wales, Sydney, NSW, Australia; 4Falls, Balance and Injury Research Centre, Neuroscience Research Australia, Sydney, NSW, Australia; 5School of Population Health, University of New South Wales, Sydney, NSW, Australia; 6School of Health Sciences, University of New South Wales, Sydney, NSW, Australia
*These authors contributed equally to this work
Correspondence: Lloyd L Y Chan, Falls, Balance and Injury Research Centre, Neuroscience Research Australia, 139 Barker Street, Randwick, Sydney, New South Wales, Australia, Email [email protected]
Background: Chronic Obstructive Pulmonary Disease (COPD) is a leading cause of disability and death worldwide. Early identification remains challenging, as existing prediction models largely rely on clinic-based assessments and self-report measures that are resource-intensive and prone to bias. This study aimed to determine whether real-world mobility metrics could predict incident COPD.
Methods: This prospective cohort study included 28,251 UK Biobank participants aged 60– 78 years who wore wrist-worn accelerometers. Digital gait biomarkers were derived using signal-processing and machine-learning algorithms. Incident COPD was identified via linked electronic health records. Associations between digital gait biomarkers and incident COPD were examined using Cox proportional hazards models with internal validation adjusted for age, sex, body mass index, smoking pack-years, air pollution exposure, and asthma history. Model discrimination was evaluated using Harrell’s concordance index.
Results: Among 28,251 participants, 639 (2.26%) developed COPD over a mean follow-up period of 8.5 (SD=1.3) years. Lower running duration, slower maximal walking speed, shorter walking bout duration, and a lower proportion of walks longer than 8 seconds were independently associated with incident COPD. A model incorporating these four digital gait biomarkers, and four easily collectable self-report measures, age, sex, smoking pack-years, and asthma history, achieved a Harrell’s concordance index of 0.80; comparable to existing models that require clinic-based tests and extensive self-report items.
Conclusion: Real-world mobility metrics are early indicators of incident COPD, providing an accessible and automatic approach for early risk identification in older people and enabling early intervention to delay disease progression and preserve quality of life.
Keywords: COPD, digital biomarkers, gait, sensors, aged
Introduction
Chronic obstructive pulmonary disease (COPD) is the most prevalent non-communicable respiratory disease, affecting about 4% of the global population. 1,2 Its prevalence increases progressively with age, ranging from 2–3% in younger individuals to over 15% in older people.3 However, reported prevalence rates vary widely due to factors such as high rates of underdiagnosis and misdiagnosis and varying access to healthcare across countries.3–6 In terms of mortality, COPD is the third leading cause of death worldwide, surpassed only by ischemic heart disease and stroke. It places a substantial economic burden on healthcare systems, accounting for approximately 6% of total healthcare expenditure in the European Union.1,2
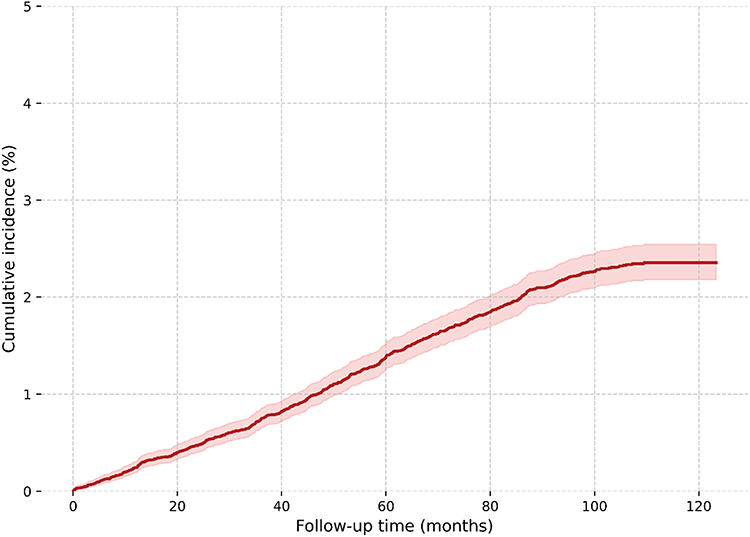 |
Figure 1 Cumulative Incidence of Incident COPD Diagnosis. |
COPD is typically diagnosed based on spirometry, indicating airflow obstruction that is irreversible or only partially reversible with bronchodilators (FEV1/FVC < 0.7). However, small airway abnormalities may develop before they are detected by this method.1 Moreover, given its insidious progression, COPD is often only diagnosed when pathophysiological changes are well-developed.7 There is a clear need, therefore, to find valid means for predicting COPD before diagnosis of manifested disease, so that early interventions can be implemented to delay disease progression and preserve people’s quality of life.
Some studies have developed predictive models utilising large databases that have included multiple medical, demographic and environmental risk factors for COPD.8,9 For example, Chen et al used a machine learning algorithm that incorporated 20 demographic, health, respiratory symptom, blood assay, and ECG variables to predict airflow limitation in the Framingham Offspring Cohort.10 Similarly, Fan et al used specific spirometry measures along with ancillary data (age, sex, chronic bronchitis and indoor biomass exposure) to predict COPD over a mean follow-up period of 3.6 years in a Chinese national cross-sectional survey.11 A recent UK Biobank study also developed a COPD risk score with 11 socioeconomic, physical activity, dietary, behavioural and environmental factors, without requiring tobacco exposure information.12 While these studies all reported good prediction accuracy, they were limited by requiring clinic/laboratory-based tests, which may be challenging to implement in daily clinical practice or telehealth settings. Further, the inclusion of many self-reported variables may introduce recall bias.13
Notably, the above prediction studies9–12 have limited emphasis on mobility and daily physical activity data, despite well-established associations between gait and balance impairments and COPD,14–19 and the growing evidence that low daily activity is an important predictor of COPD-related hospitalisations and mortality.20 Individuals with COPD usually have reduced gait speed, shorter step length, lower cadence and altered gait variability.14,15 Some papers have associated these impairments with outcomes such as mortality, disease progression or symptom severity, suggesting that they may have potential as prognostic indicators.14–21 Some studies have also used wearable sensors to evaluate gait in people with COPD, but these studies have been conducted in clinical environments, which may not reflect the real-world gait of these people.14–19 Furthermore, the sensors in these studies have been placed on the ankles and lower back, which have low participant acceptance, potentially hindering uptake and sustained use of these devices.14–19
In contrast, wrist-worn devices in the form of smartbands and smartwatches are widely accepted.22,23 Our previous study demonstrated that wrist sensor-based data provide valid measures of walking speed, quality, quantity, and bouts in everyday life.24,25 Utilising these digital gait biomarkers instead of self-reported mobility may minimise subjectivity, and recall and social desirability biases.26–28 However, the ability of objectively measured real-world walking metrics to predict incident COPD has yet to be determined.
This study aimed to establish whether: (a) digital biomarkers extracted from a wrist-worn sensor are predictive of incident COPD in a large sample of older people (over 28,000 participants from the UK Biobank database); (b) digital biomarkers provide additional value to established risk factors in predicting COPD; and (c) a COPD prediction model incorporating only digital gait biomarkers and simple self-reported measures is comparable to existing screening tools that require clinical assessments and multiple self-reported items. We hypothesized that digital biomarkers derived from wrist sensors and a few easily collectable measures would offer a valid COPD risk screening without the need for spirometry or detailed self-report health information.
Material and Methods
Participants
Data were obtained from the UK Biobank Resource (UKB), a population-based cohort study in the United Kingdom involving 500,000 participants aged 40–69 years at recruitment (2006–2010).29 Between 2013 and 2015, a sub-cohort of 236,519 participants was randomly selected and invited to wear the Axivity AX3 accelerometer (Axivity, Newcastle Upon Tyne, UK) on the dominant wrist for seven consecutive days.30 Participant information and accelerometric data were linked with the National Health Service (NHS) electronic health records, with entries retrieved in September 2023. For this study, we analysed data of participants aged 60 years or older who provided at least five days of valid accelerometric data and had not been diagnosed with COPD at the time of accelerometric data collection. All participants provided informed consent before data collection. The UK Biobank study obtained ethical approval from the NHS National Research Ethics Service (Ref: 11/NW/0382). Use of the de-identified UK Biobank dataset for the present study was acknowledged by UNSW Sydney Research Ethics & Compliance Support (RECS) (Ref: iRECS11555). Reporting in this study follows the Strengthening the Reporting of Observational studies in Epidemiology (STROBE) Statement to ensure clarity, transparency, and reproducibility.31 A STROBE statement checklist is presented in Supplementary Table 1. The participant flow chart is presented in Supplementary Figure 1.
COPD Incidence
Dates of COPD diagnoses were extracted from the NHS electronic health records in accordance with the 10th revision of the International Classification of Diseases (ICD-10, code: J44, J44.0, J44.1, J44.8, J44.9; UKB data-field #: 22,130). The number of days between accelerometric data collection and incident COPD diagnosis was extracted as the time-to-event data. Death (UKB#40000) and lost-to-follow-up (UKB#191) were set as censoring events. COPD incidence was followed up for a maximum of 9 years.
Digital Gait Biomarkers
Daily-life gait performances were extracted from the wrist-worn accelerometric data with the Watch Walk method (v2.3.0).24 In brief, acceleration signals were merged, filtered and cut into 4-second windows and classified into running, walking, stationary, and unspecified arm activities by support vector machine (SVM) algorithms. Walking activities were further divided into walking with arm swing, walking with adaptive hand positioning (eg., hands in pockets or carrying shoulder bags, briefcases, or handbags), and walking with static hand positioning (eg., hands held near the head, such as during a phone call, or held in front, such as while texting). Subsequently, 11 digital gait biomarkers were extracted with signal processing techniques and/or SVM regressions. These included step count, running duration, maximal walking speed, usual walking speed, median cadence, step time variability, step regularity, stride regularity, duration of the longest walk and the proportions of all walks that were longer than eight or sixty seconds. A detailed description has been published previously.25
Established Risk Factors
Previously reported risk factors for COPD available in the UK Biobank dataset were extracted for analysis. These included demographic information such as age (UKB#33), sex (UKB#31), and body mass index (BMI) (UKB#21001).1,3 Cumulative first-hand tobacco exposure was quantified using “pack-years of smoking” (UKB#20161), calculated by multiplying the number of cigarette packs smoked per day by the number of years smoked.1,3,32 Second-hand smoking exposure was assessed through “exposure to tobacco smoke outside home” (UKB#1279) and “exposure to tobacco smoke at home” (UKB#1269).1,3,32 Perinatal risk factor included “perinatal maternal smoking” (UKB#1787), 1,3 which is linked to diminished lung function peak during early adulthood, which predisposes to decreased lung capacity and lung diseases.1,3,32,33 Prior diagnosis of asthma (UKB#22127) was also extracted.1,3 For occupational exposure, “having worked with pesticides” (UKB#22614) was included.1,3,32 To assess air pollutant exposure, “air particulate matter PM2.5” (UKB#24006) was selected, as it represents a widely studied and clinically significant measure of air quality.1,3,32 These particles can penetrate the finest airways, potentially damaging them and triggering COPD development.1,3,32 “Total household income before tax” (UKB#738) was used as a socioeconomic factor potentially influencing indoor air quality.1,3
Statistical Analysis
Baseline Characteristics
We compared baseline characteristics of individuals who developed COPD in the follow-up period and those who did not. Categorical variables were assessed with Chi-square tests, with frequencies and proportions reported; parametric continuous variables were assessed with independent t-tests, with means and standard deviations reported; non-parametric variables were assessed with the Wilcoxon Rank Sum Test, with medians and interquartile ranges reported.
Minimally-Adjusted Cox Proportional Hazards Regression
We used Cox proportional hazards regression to examine the associations between time-to-COPD and the digital gait biomarkers, adjusting for age and sex. The proportional hazard assumptions and functional forms were assessed with weighted Schoenfeld residuals-versus-time plots and the Martingale Residual plots, respectively.34,35 Variables that violated these assumptions were transformed to ensure compliance.36
Multivariable Cox Proportional Hazards Regression
To assess whether digital gait biomarkers offer additional predictive value beyond known risk factors, we ran a multivariable Cox proportional-hazards regression. If high correlations (Pearson’s R ≥ 0.7) were identified between digital gait biomarkers, only one variable was included in the model to avoid multicollinearity. Known risk factors were entered first, followed by the digital gait biomarkers by backward elimination. Finally, a multivariable Cox proportional-hazards regression model was run to investigate the predictive value of a simplified model, where age, sex, smoking pack-years, previous diagnosis of asthma and digital gait biomarkers were selected with backward elimination.
Effect Estimates, Model Performance and Validation
Hazard ratios and the corresponding confidence intervals were reported for all Cox Proportional Hazards models. To facilitate the interpretation and comparison of effect sizes, standardized hazard ratios and 95% confidence intervals of the z-transformed biomarkers were also reported. Harrell’s concordance indices were used to assess the predictive value of the multivariable models. Its value ranges from 0.5 to 1.0, with 0.5 indicating a model no better than chance and values close to 1 indicating perfect predictive accuracy. Internal validation using 500 bootstrap resamples was conducted to assess overfitting and obtain optimism-corrected estimates of Harrell’s concordance index. The full model-building process was repeated within each resample, and bootstrap validation was used solely for performance assessment. Statistical inference was set at 0.05, and analyses were performed in SAS Enterprise 8.3 software. Missing data were imputed with the expectation-maximisation algorithm.
Results
Baseline Characteristics
Our sample comprised 28,251 individuals with a mean age of 66.7 (standard deviation, SD, 4.14) years at baseline, of which 14,533 (51.4%) were women. The average follow-up period was 8.5 years (SD = 1.3). During this period, 639 participants were diagnosed with COPD - an incidence of 2.26% (Figure 1). Table 1 presents the baseline characteristics of the participants categorised by their COPD diagnosis. Participants who developed COPD within the follow-up period were more likely to be older, have higher BMIs, have previously been diagnosed with asthma, live in lower-income households and have had greater exposure to pesticides, air pollution and all forms of tobacco use than those who did not develop COPD.
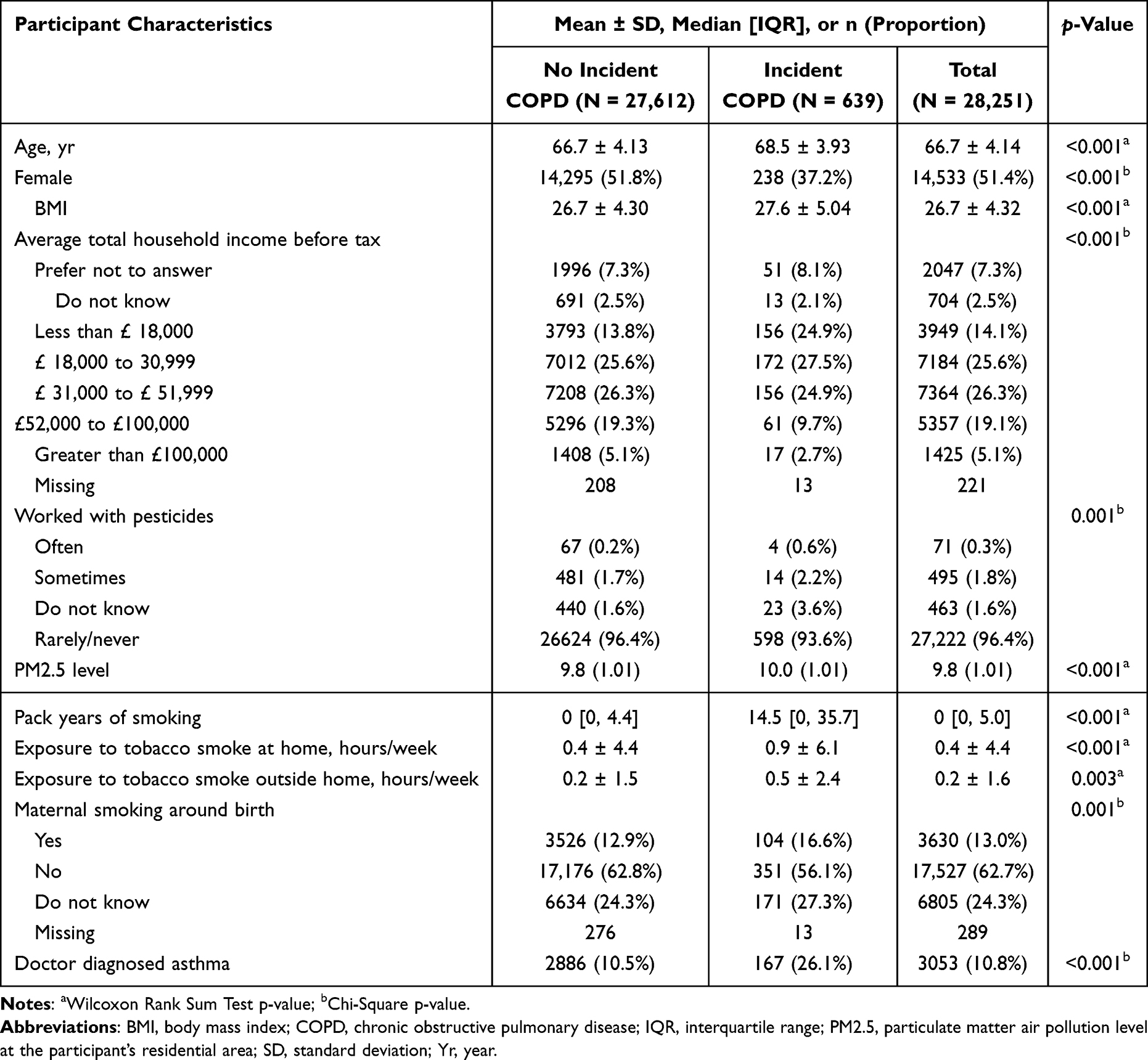 |
Table 1 Participant Characteristics by COPD Status During Follow-Up |
Minimally-Adjusted Cox Proportional Hazards Regression
Participants who developed COPD demonstrated poorer performance in all digital gait biomarkers compared to those who did not develop COPD (Supplementary Table 2). Specifically, they took fewer daily steps, had slower gait speed and cadence, increased step time variability, and ran less. All gait parameters remained significant predictors of COPD after adjusting for age and sex in the minimally adjusted Cox regression models. Running duration had the strongest association (a 45% decrease in hazard for one SD increment of the log-transformed running time). This was followed by maximal walking speed (37% decrease in hazard for one SD increment) and usual walking speed (35% decrease in hazard for one SD increment). Increased step-time variability was also associated with COPD risk (21% increase in hazard for one SD increment). Crude and standardized hazard ratios and confidence intervals for all minimally adjusted Cox regressions are shown in Supplementary Table 2.
Multivariable Cox Proportional Hazards Regression Estimates, Performance and Validation
Table 2 shows the full multivariable prediction model. This included the eleven established COPD risk factors (outlined in Table 1) entered at the initial step and four significant digital gait biomarkers (running duration, maximal walking speed, duration of longest walk and the proportion of walks longer than eight seconds) entered at step two using backward elimination. This 15-variable model had a Harrell’s concordance index of 0.81 (SE 0.01).
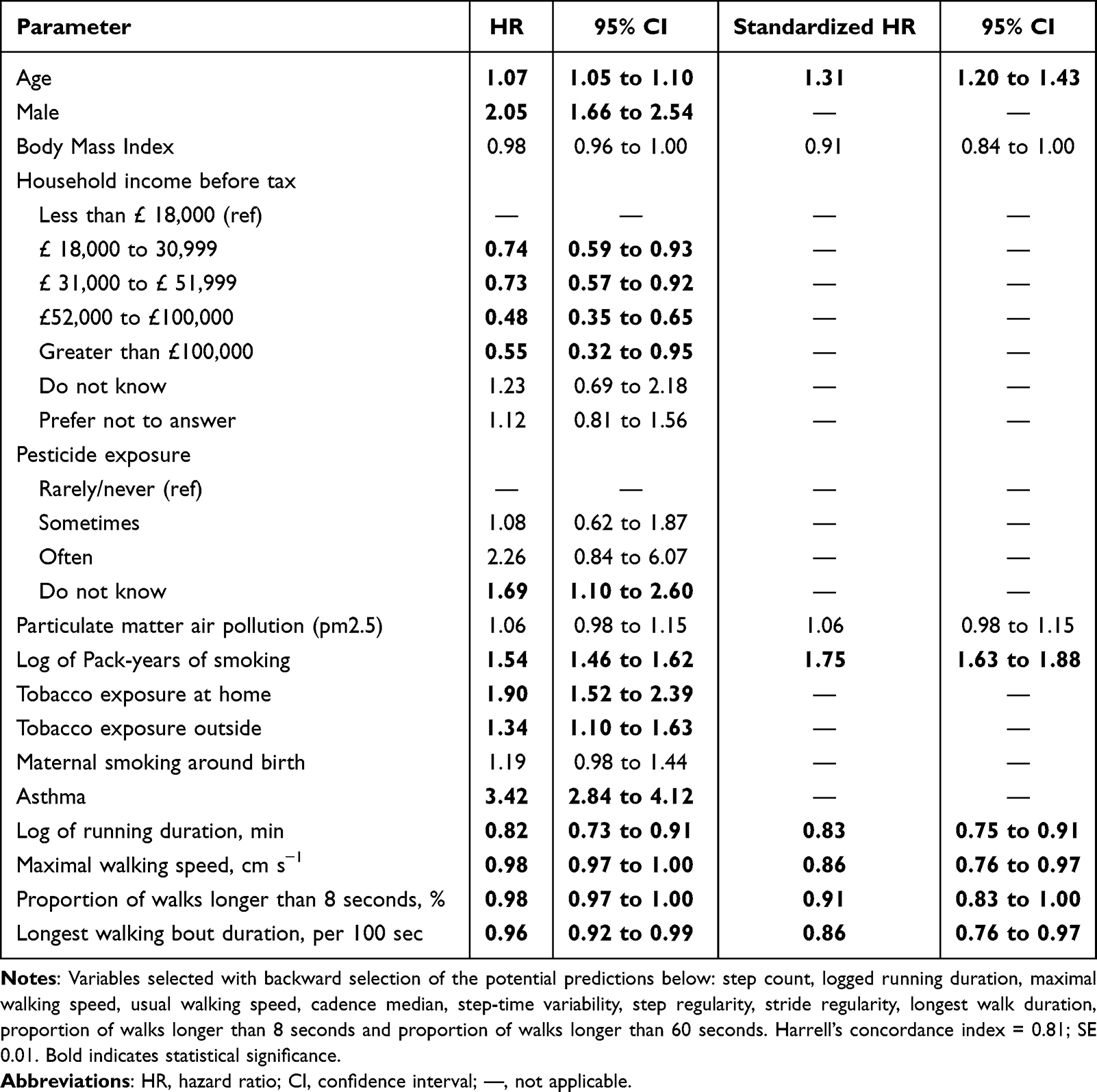 |
Table 2 Multivariable Associations Between Digital Biomarkers and Time-to-COPD via Cox Regression in the Full Model (n=28,251) |
Table 3 presents the simplified multivariable prediction, which comprised four established COPD risk factors (age, sex, smoking pack-years, and asthma history) and four digital gait biomarkers (running duration, maximal walking speed, longest walking bout duration, and proportion of walks that were longer than 8 seconds). This eight-variable model had a Harrell’s concordance index of 0.80 (standard error, SE = 0.01). Bootstrap internal validation showed negligible optimism, with a mean bootstrap C-index of 0.80, indicating stable model performance. Parameters for the prediction models fitted using Cox Regression analysis are presented in Supplementary Table 3.
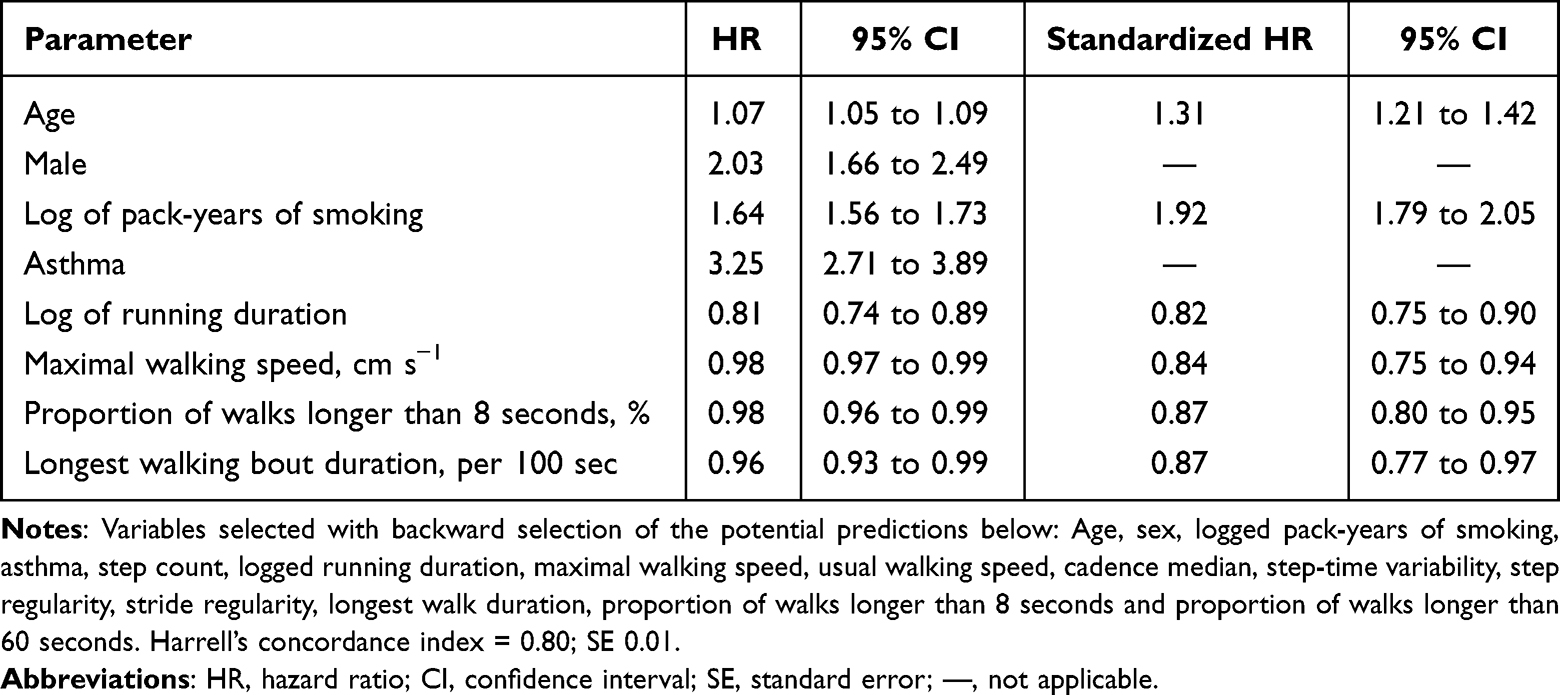 |
Table 3 Multivariable Associations Between Digital Biomarkers and Time-to-COPD via Cox Regression in the Simplified Model (n=28,251) |
Predicted Risk for Illustrative Profiles
As an illustration, a 70-year-old man with a history of asthma, a smoking exposure of one pack-year, and poor mobility (10th percentile across four digital gait biomarkers) has an estimated 5-year risk of COPD of 7.2%. In contrast, an individual with the same asthma and smoking risk factors but favourable mobility performance (90th percentile) has an estimated risk of 1.4%, representing an approximately fivefold difference in risk.
Discussion
This study is the first to investigate the association between wrist-worn sensor-acquired measures of real-world gait speed, quality and quantity and incident COPD in a large cohort of older people with up to nine years of follow-up. Participants who walked or ran less, walked slower, had less regular gait and had shorter walking bouts at baseline were more likely to develop COPD. After adjusting for established risk factors, we found that running duration, maximal walking speed, duration of the longest walk and the proportion of walks longer than 8 seconds were independent and significant predictors of COPD. On this basis, we also derived a simpler prediction model, with four self-reported variables (age, sex, smoking pack years, and asthma history) and four gait biomarkers (running duration, maximal walking speed, duration of the longest walk, and proportion of walks that were longer than 8 seconds). The clinical relevance of this model is supported by the magnitude of the observed risk differences, demonstrating that variation in key mobility measures translates into meaningful differences in predicted COPD risk. Both our comprehensive and simple models had good predictive accuracy, as indicated by Harrell’s concordance indices ≥0.80, comparable with previous models that require clinic/laboratory-based and/or several self-reported measures.9–12
Importantly, while step count was identified as a significant COPD predictor in the minimally adjusted analysis (Supplementary Table 2), it was excluded from the multivariable prediction model where established risk factors were adjusted for. This suggests that COPD risk is better predicted by other digital gait biomarkers that reflect sustained activity (longer walks) and vigour (running and fast walking speed) than physical activity volume. These biomarkers also likely better indicate poor cardiorespiratory fitness, diminished physiological capacity and impaired resilience towards physical stressors,37 which would explain their sensitivity to early COPD-related changes.
For most people, the onset of COPD is subtle and often goes unnoticed until it reaches moderate or advanced stages.38 However, COPD progressively reduces daily physical activity and leads to more sedentary behaviour,1,14 which increases the risk of hospitalisation and death.20 In recent years, concepts such as pre-COPD and Preserved Ratio Impaired Spirometry (PRISm) have gained attention,1 but due to questionable benefits, the role of spirometry in diagnosing and screening asymptomatic people is not currently recommended.1,39 However, early risk identification with a simple screening assessment may enable early diagnosis and the implementation of interventions to delay or lessen COPD progression. In this context, our findings suggest that real-world walking and running performance may serve as low-burden indicators of COPD risk, with potential application as scalable remote screening tools to identify individuals at elevated risk.
Individuals diagnosed in the pre-clinical or early stages of COPD may benefit from both pharmacological and non-pharmacological interventions.40 Bronchodilators can slow the decline in lung function in the early stages of COPD.41 They also reduce the frequency and severity of exacerbations, leading to better quality of life (QoL). However, evidence on their long-term effects in early COPD is limited.7,42 Inhaled steroids have a less significant benefit,43,44 and other less commonly used medications, such as roflumilast, macrolides, and N-acetylcysteine, still require further research.7 On the other hand, non-pharmacological treatments have shown more promising results. Smoking cessation, for example, leads to a significant reduction in COPD severity, respiratory morbidity, and mortality,45 while also improving lung function.46,47 Regular exercise and pulmonary rehabilitation can also enhance functional performance and QoL, even in the early stages.42,45,48,49 Additionally, managing other risk factors, such as exposure to air pollutants, respiratory infections, vaccination, and nutritional interventions, has been shown to play a crucial role in COPD management.7,38
This study has some notable strengths. First, the Watch Walk digital gait biomarkers have demonstrated good validity and reliability in previous research.24,25 Second, the large sample size and 9-year follow-up period provided adequate data for identifying risk factors for incident COPD. Third, the data were sourced from a comprehensive medical database with detailed sociodemographic information and reliable public health record linkage. Nonetheless, we acknowledge the limitations of this study. While our prediction model showed promising accuracy, external validation is needed to confirm its applicability across diverse demographic and healthcare settings, including different age groups, socioeconomic backgrounds, geographic locations, and ethnicities, before clinical implementation. Additionally, selecting participants who wore a wrist sensor for at least five days may have limited the generalizability of the findings to individuals with higher motivation and adherence to wearing smartwatches, which may be associated with greater engagement in health-related behaviours.
Conclusion
Real-world running and walking measures derived from wrist-worn devices, including running duration, maximal walking speed, longest walking bout duration, and the proportion of sustained walking, were independently associated with incident COPD and demonstrated good predictive discrimination (Harrell’s concordance index = 0.80). Differences in mobility were associated with meaningful differences in COPD risk. Given that these measures are easy to collect, they offer a feasible and scalable approach for identifying older people at elevated risk of COPD, facilitating earlier clinical assessment and more targeted intervention.
Abbreviations
AX3, Axivity AX3 accelerometer; BMI, Body Mass Index; CI, Confidence Interval; COPD, Chronic Obstructive Pulmonary Disease; ECG, Electrocardiogram; FEV1, Forced Expiratory Volume in one second; FVC, Forced Vital Capacity; HR, Hazard Ratio; ICD-10, International Classification of Diseases, 10th Revision; IQR, Interquartile Range; NHS, National Health Service (United Kingdom); NHMRC, National Health and Medical Research Council (Australia); PM2.5, Particulate Matter ≤2.5 µm; PRISm, Preserved Ratio Impaired Spirometry; QoL, Quality of Life; SD, Standard Deviation; SE, Standard Error; SVM, Support Vector Machine; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; UKB, UK Biobank.
Data Sharing Statement
Individual de-identified participant data underlying the results reported in this article, including data dictionaries, are available through the UK Biobank. Digital gait biomarker data processed with the Watch Walk algorithm were returned to the UK Biobank for public access in December 2023. Access is granted to researchers via the UK Biobank’s data access procedures.
Acknowledgment
This study was conducted using the UK Biobank Resource under Application Number 103840. It includes computations using the computational cluster Katana supported by Research Technology Services at UNSW Sydney.
Funding
This research received funding from the National Health and Medical Research Council (NHMRC), including an L3 Investigator Grant (Grant No. 2002096) awarded to SRL.
Disclosure
LLYC, SRL, and MAB have exclusively licensed the Watch Walk algorithms to SpaceTalk Ltd for productisation via UNSW and NeuRA. An electronic platform enabling researchers to upload wrist-worn accelerometry data and access the Watch Walk digital gait biomarkers is currently available as a non-profit initiative: https://watchwalk.neura.edu.au/. LLYC and SRL have an agreement with SpaceTalk Ltd which may result in SpaceTalk Ltd incorporating some Watch Walk algorithms in a smartwatch commercial product. The authors report no other conflicts of interest in this work.
References
1. Global Initiative for Chronic Obstructive Lung Disease. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the Diagnosis, Management, and prevention of COPD: 2024 report. 2024. Available from: https://goldcopd.org/2024-gold-report.
2. Levine SM, Marciniuk DD. Global Impact of Respiratory Disease: what Can We Do, Together, to Make a Difference? Chest. 2022;161(5):1153–11. doi:10.1016/j.chest.2022.01.014
3. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–458. doi:10.1016/s2213-2600(21)00511-7
4. Easter M, Bollenbecker S, Barnes JW, Krick S. Targeting Aging Pathways in Chronic Obstructive Pulmonary Disease. Int J Mol Sci. 2020;21(18):6924. doi:10.3390/ijms21186924
5. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: results from the Global Burden of Disease Study 2019. BMJ. 2022;378:e069679. doi:10.1136/bmj-2021-069679
6. Liu Z, Pan H, Liu B, Li L, Yang H, Shen T. Environmental and occupational risk factors for COPD and its prevalence among miners worldwide: a Mendelian randomization and meta-analysis study. Environ Sci Pollut Res. 2023;30(43):97545–97561. doi:10.1007/s11356-023-29269-z
7. Fazleen A, Wilkinson T. Early COPD: current evidence for diagnosis and management. Ther Adv Respir Dis. 2020;14:1753466620942128. doi:10.1177/1753466620942128
8. Shen X, Liu H. Using machine learning for early detection of chronic obstructive pulmonary disease: a narrative review. Respir Res. 2024;25(1):336. doi:10.1186/s12931-024-02960-6
9. Matheson MC, Bowatte G, Perret JL, et al. Prediction models for the development of COPD: a systematic review. Int J Chron Obstruct Pulmon Dis. 2018;13:1927–1935. doi:10.2147/copd.S155675
10. Chen W, Sin DD, FitzGerald JM, Safari A, Adibi A, Sadatsafavi M. An Individualized Prediction Model for Long-term Lung Function Trajectory and Risk of COPD in the General Population. Chest. 2020;157(3):547–557. doi:10.1016/j.chest.2019.09.003
11. Fan J, Fang L, Cong S, et al. Potential pre-COPD indicators in association with COPD development and COPD prediction models in Chinese: a prospective cohort study. The Lancet Regional Health - Western Pacific. 2024;44:100984. doi:10.1016/j.lanwpc.2023.100984
12. He Y, Qian DC, Diao JA, et al. Prediction and stratification of longitudinal risk for chronic obstructive pulmonary disease across smoking behaviors. Nat Commun. 2023;14(1):8297. doi:10.1038/s41467-023-44047-8
13. Ioannidis JPA. The Challenge of Reforming Nutritional Epidemiologic Research. JAMA. 2018;320(10):969–970. doi:10.1001/jama.2018.11025
14. Zago M, Sforza C, Bonardi DR, Guffanti EE, Galli M. Gait analysis in patients with chronic obstructive pulmonary disease: a systematic review. Gait Posture. 2018;61:408–415. doi:10.1016/j.gaitpost.2018.02.007
15. Buekers J, Delgado-Ortiz L, Megaritis D, et al. Gait differences between COPD and healthy controls: systematic review and meta-analysis. Eur Respir Rev. 2024;33(172):4. doi:10.1183/16000617.0253-2023
16. Iwakura M, Okura K, Shibata K, et al. Gait characteristics and their associations with clinical outcomes in patients with chronic obstructive pulmonary disease. Gait Posture. 2019;74:60–65. doi:10.1016/j.gaitpost.2019.08.012
17. Lahousse L, Verlinden VJ, van der Geest JN, et al. Gait patterns in COPD: the Rotterdam Study. Eur Respir J. 2015;46(1):88–95. doi:10.1183/09031936.00213214
18. Buekers J, Megaritis D, Koch S, et al. Laboratory and free-living gait performance in adults with COPD and healthy controls. ERJ Open Res. 2023;9(5):2. doi:10.1183/23120541.00159-2023
19. Yentes JM, Rennard SI, Schmid KK, Blanke D, Stergiou N. Patients with Chronic Obstructive Pulmonary Disease Walk with Altered Step Time and Step Width Variability as Compared with Healthy Control Subjects. Ann Am Thorac Soc. 2017;14(6):858–866. doi:10.1513/AnnalsATS.201607-547OC
20. Durheim MT, Smith PJ, Babyak MA, et al. Six-minute-walk distance and accelerometry predict outcomes in chronic obstructive pulmonary disease independent of Global Initiative for Chronic Obstructive Lung Disease 2011 Group. Ann Am Thorac Soc. 2015;12(3):349–356. doi:10.1513/AnnalsATS.201408-365OC
21. Buttery SC, Williams PJ, Alghamdi SM, et al. Investigating the prognostic value of digital mobility outcomes in patients with chronic obstructive pulmonary disease: a systematic literature review and meta-analysis. Eur Respir Rev. 2023;32(170):1. doi:10.1183/16000617.0134-2023
22. Keogh A, Dorn JF, Walsh L, Calvo F, Caulfield B. Comparing the Usability and Acceptability of Wearable Sensors Among Older Irish Adults in a Real-World Context: observational Study. JMIR mHealth uHealth. 2020;8(4):e15704. doi:10.2196/15704
23. Ambrens M, Delbaere K, Butcher K, et al. Wearable Technology in Mobility and Falls Health Care: finding Consensus on Their Clinical Utility and Identifying a Roadmap to Actual Use. J Geriatr Phys Ther. 2025. doi:10.1519/jpt.0000000000000434
24. Chan LLY, Choi TCM, Lord SR, Brodie MA. Development and large-scale validation of the Watch Walk wrist-worn digital gait biomarkers. Sci Rep. 2022;12(1):16211. doi:10.1038/s41598-022-20327-z
25. Chan LLY, Lord SR, Brodie MA. Daily-Life Walking Speed, Quality and Quantity Derived from a Wrist Motion Sensor: large-Scale Normative Data for Middle-Aged and Older Adults. Sensors. 2024;24(16). doi:10.3390/s24165159
26. Argyridou S, Zaccardi F, Davies MJ, Khunti K, Yates T. Walking pace improves all-cause and cardiovascular mortality risk prediction: a UK Biobank prognostic study. Eur J Prev Cardiol. 2020;27(10):1036–1044. doi:10.1177/2047487319887281
27. Welsh CE, Celis-Morales CA, Ho FK, et al. Grip Strength and Walking Pace and Cardiovascular Disease Risk Prediction in 406,834 UK Biobank Participants. Mayo Clin Proc. 2020;95(5):879–888. doi:10.1016/j.mayocp.2019.12.032
28. Henson J, Yates T, Bhattacharjee A, et al. Walking pace and the time between the onset of noncommunicable diseases and mortality: a UK Biobank prospective cohort study. Ann Epidemiol. 2024;90:21–27. doi:10.1016/j.annepidem.2023.10.001
29. Sudlow C, Gallacher J, Allen N, et al. UK biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 2015;12(3):e1001779. doi:10.1371/journal.pmed.1001779
30. Doherty A, Jackson D, Hammerla N, et al. Large Scale Population Assessment of Physical Activity Using Wrist Worn Accelerometers: the UK Biobank Study. PLoS One. 2017;12(2):e0169649. doi:10.1371/journal.pone.0169649
31. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370(9596):1453–1457. doi:10.1016/S0140-6736(07)61602-X
32. Ruvuna L, Sood A. Epidemiology of Chronic Obstructive Pulmonary Disease. Clinics Chest Med. 2020;41(3):315–327. doi:10.1016/j.ccm.2020.05.002
33. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
34. Grambsch PM, Therneau TM. Proportional hazards tests and diagnostics based on weighted residuals. Biometrika. 1994;81(3):515–526. doi:10.1093/biomet/81.3.515
35. Lin DY, Wei LJ, Ying Z. Checking the Cox model with cumulative sums of martingale-based residuals. Biometrika. 1993;80(3):557–572. doi:10.1093/biomet/80.3.557
36. Tukey BH, John W. Exploratory Data Analysis. Addison-Wesley Publishing Company Reading, Mass. — menlo Park, Cal. London, Amsterdam, Don Mills, Ontario, Sydney 1977, XVI, 688 S. Biometrical J. 1981;23(4):413–414. doi:10.1002/bimj.4710230408
37. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–M156. doi:10.1093/gerona/56.3.m146
38. Labonté LE, Tan WC, Li PZ, et al. Undiagnosed Chronic Obstructive Pulmonary Disease Contributes to the Burden of Health Care Use. Data from the CanCOLD Study. Am J Respir Crit Care Med. 2016;194(3):285–298. doi:10.1164/rccm.201509-1795OC
39. Mangione CM, Barry MJ, Nicholson WK, et al. Screening for Chronic Obstructive Pulmonary Disease: US Preventive Services Task Force Reaffirmation Recommendation Statement. JAMA. 2022;327(18):1806–1811. doi:10.1001/jama.2022.5692
40. Decramer M, Miravitlles M, Price D, et al. New horizons in early stage COPD--improving knowledge, detection and treatment. Respir Med. 2011;105(11):1576–1587. doi:10.1016/j.rmed.2010.12.015
41. Welte T, Vogelmeier C, Papi A. COPD: early diagnosis and treatment to slow disease progression. Int J Clin Pract. 2015;69(3):336–349. doi:10.1111/ijcp.12522
42. Agusti A, Faner R. Lung function trajectories in health and disease. Lancet Respir Med. 2019;7(4):358–364. doi:10.1016/S2213-2600(18)30529-0
43. Albers M, Schermer T, van den Boom G, et al. Efficacy of inhaled steroids in undiagnosed subjects at high risk for COPD: results of the detection, intervention, and monitoring of COPD and asthma program. Chest. 2004;126(6):1815–1824. doi:10.1378/chest.126.6.1815
44. van Grunsven P, Schermer T, Akkermans R, et al. Short- and long-term efficacy of fluticasone propionate in subjects with early signs and symptoms of chronic obstructive pulmonary disease. Results of the DIMCA study. Respir Med. 2003;97(12):1303–1312. doi:10.1016/j.rmed.2003.08.001
45. Zysman M, Mahay G, Guibert N, Barnig C, Leroy S, Guilleminault L. Impact of pharmacological and non-pharmacological interventions on mortality in chronic obstructive pulmonary disease (COPD) patients. Respir Med Res. 2023;84:101035. doi:10.1016/j.resmer.2023.101035
46. Anthonisen NR, Connett JE, Kiley JP, et al. Effects of smoking intervention and the use of an inhaled anticholinergic bronchodilator on the rate of decline of FEV1. The Lung Health Study. JAMA. 1994;272(19):1497–1505.
47. Scanlon PD, Connett JE, Waller LA, et al. Smoking cessation and lung function in mild-to-moderate chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2000;161(2):381–390. doi:10.1164/ajrccm.161.2.9901044
48. Ma Y, Chen Y, Zhang N, et al. Efficacy and safety of pulmonary rehabilitation training on lung function, quality of life, and T cell immune function in patients with stable chronic obstructive pulmonary disease: a randomized controlled trial. Ann Palliat Med. 2022;11(5):1774–1785. doi:10.21037/apm-22-451
49. Zhu Z, Muhamad AS, Omar N, Ooi FK, Pan X, Ong MLY. Efficacy of exercise treatments for chronic obstructive pulmonary disease: a systematic review. J Bodyw Mov Ther. 2024;38:106–127. doi:10.1016/j.jbmt.2024.01.019
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.