Back to Journals » Journal of Pain Research » Volume 15
Are Pain Screening and Functional Assessment Results Associated with New Diagnoses and Treatment for Pain in Primary Care? An Observational Study
Authors Hudson Scholle S, Nguyen-Louie TT, Bifulco L ![]() , Blaz JW, Blankson ML, Channamsetty V, Anderson DR
, Blaz JW, Blankson ML, Channamsetty V, Anderson DR
Received 24 March 2022
Accepted for publication 7 July 2022
Published 5 August 2022 Volume 2022:15 Pages 2249—2261
DOI https://doi.org/10.2147/JPR.S367480
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jonathan Greenberg
Sarah Hudson Scholle,1 Tam T Nguyen-Louie,1 Lauren Bifulco,2 Jacquelyn W Blaz,1 Mary L Blankson,2 Veena Channamsetty,2 Daren R Anderson2
1National Committee for Quality Assurance, Washington, DC, USA; 2Weitzman Institute, Community Health Center, Inc., Middletown, CT, USA
Correspondence: Sarah Hudson Scholle, National Committee for Quality Assurance (NCQA), 1100 13th St. NW, Third Floor, Washington, DC, 20005, USA, Tel +1-202-955-1726, Fax +1-202-955-3500, Email [email protected]
Purpose: To determine if pain screening and functional assessment results are associated with new diagnoses and treatment for pain in primary care.
Patients and Methods: Observational study at 13 primary care sites of a statewide federally qualified health center that implemented routine screening and functional assessment for all adults in primary care. The study group included 10,091 adults aged 18+ who had an in-person visit between July 2, 2018, and June 1, 2019, where they screened positive for chronic pain and completed a 3-question functional assessment with the PEG (Pain, Enjoyment of Life, General Activity). Multivariate logistic regressions quantified associations between pain frequency, diagnosis and treatment, sociodemographics, comorbidities, and self-reported severe pain impairment with pain diagnoses and treatment documented after screening.
Results: Patients were mostly women (60.3%), Latinx (41.1%), English-speaking (80.1%), and Medicaid-insured (62.0%); they averaged 49.1 years old (SD = 13.7 years). Patients with severe pain impairment or who were Latinx were more likely to get a newly documented pain diagnosis (absolute risk difference [ARD]: 13.2% and 8.6%, ps < 0.0001), while patients with mental health/substance use or medical comorbidities were less likely (ARDs: − 20.0% to − 6.2%, ps < 0.001). Factors most consistently associated with treatment were prior treatment of the same modality (4 of 7 treatments, ARDs = 27.3% to 44.1%, ps < 0.0001), new pain diagnosis (5 of 7, ARDs = 3.2% to 27.4%, ps < 0.001), and severe impairment (4 of 7, ARDs = 2.6% to 6.5%, ps < 0.0001). A new diagnosis had the strongest association with non-opioid pain analgesics and physical medicine (ARD = 27.0% and 27.4%, p < 0.0001). Latinx patients were less likely to receive opioid analgesics and mental health/substance use medications and counseling (ARDs = − 3.3% to 7.5%, ps < 0.0001).
Conclusion: Screening and assessment with patient-reported tools may influence pain care. Care for Latinx patients differed from non-Latinx white patients.
Keywords: PEG, chronic pain, primary care, patient-reported outcome measures, federally qualified health center, equity
Plain Language Summary
Chronic pain lasts for 90 days or more and can be difficult to track, measure, and treat. We studied patterns of chronic pain care after the implementation of new processes to screen and follow-up on chronic pain in primary care. Our study took place in 2018–2019 at a federally qualified health center (FQHC), a primary care practice that treats medically underserved patients. Many are members of marginalized minority groups, are uninsured or underinsured, and/or experience poverty. We found that over 20% of the 10,091 patients who screened positive for chronic pain did not have a corresponding pain diagnosis documented in their medical record prior to screening. We also found that Latinx people and people who reported that their pain interfered severely with their lives were more likely to have a new pain diagnosis documented at the visit, and people who also had mental health, substance use, or other medical conditions were less likely. Receiving pain treatment was associated with having severe pain, receiving newly documented pain diagnoses, and having previously received treatment of the same type. Despite being more likely to receive a newly documented pain diagnosis, Latinx patients were less likely than non-Latinx patients to receive opioids, mental health medications, and substance use medications and counseling after their newly documented pain diagnosis. This information will help primary care providers understand the characteristics of patients who experience chronic pain and how information about pain interference could inform clinical care.
Introduction
The economic, social, and individual impact of chronic pain is well documented.1 In 2010, healthcare costs attributed to management of chronic pain and associated conditions were estimated to be 560 to 635 billion dollars annually.2 Patients with chronic pain are more likely to have a history of childhood or partner abuse, depression and anxiety, poor coping skills, substance use, and low employment attainment.3,4 Regardless of type, the presence of chronic pain is associated with an increased risk for suicide, especially among individuals with concomitant depression, physical disability, sleep difficulties, and multiple chronic conditions.5 In an examination of electronic health records from a California-based healthcare system between 2006 and 2015, 62% of patients with opioid use disorder experienced chronic pain before the onset of their substance use disorder.6 Despite its impact, accurate estimates of the true prevalence of chronic pain are challenged by the varied methodologies for assessment and identification, heterogeneity in etiologies, patient-perceived stigma associated with this condition, and unclear diagnostic guidelines.7 Unlike many other common chronic conditions, pain does not have good markers for disease “control” such as Hemoglobin A1c for diabetes. The commonly used eleven-point Numeric Rating Scale “pain score” has largely been shown to be of limited accuracy for assessing pain in primary care.8 The National Pain Strategy9 and other recent guidelines10 recommend that pain care decision-making should be based on function and should incorporate patient-specific functional goals for treatment. Evidence from conditions other than chronic pain suggests that the use of patient-reported outcomes could aid in care planning and lead to improvements in outcomes.11,12 The Centers for Disease Control and Prevention (CDC) guidelines for chronic pain management in outpatient primary care recommend using validated instruments, such as the PEG tool, to assess for pain’s severity and impact on quality of life and function, and to monitor patient outcomes related to chronic pain.13 The PEG is a brief, psychometrically valid three-item tool that assesses average pain intensity (P), interference with enjoyment of life (E), and interference with general activity (G) in ambulatory care.13–15 The PEG has been shown to be responsive to changes in patient-reported chronic pain over time, but its utility in informing clinical diagnosis and management of chronic pain has not been examined.
Identification and treatment of chronic pain is particularly important for primary care. In the US, over half of patients with chronic pain receive their care in a primary care setting16,17 and similar reliance on primary care is reported in other countries as well.18 Guidelines recommend that primary care practitioners assess the severity and impact of pain on functioning.10,19 But evidence suggests that primary care clinicians express low confidence in their ability to manage pain10 and may have gaps in knowledge or supports to implement evidence.20 Previous literature suggests that the prevalence of chronic pain among primary care patients varies by age and sex and often occurs with chronic illness.18,21 Also, chronic pain disproportionately affects disadvantaged populations22 and these groups are experiencing the largest increases in chronic pain prevalence.23
We previously demonstrated the feasibility of implementing a two-step process to assess the presence and impact of chronic pain at a federally qualified health center (FQHC), a primary care practice that treats medically underserved patients.24 Many of the patients served by the FQHC are members of marginalized minority groups, are uninsured or underinsured, and/or experience poverty. Patients were asked a single-item screener for presence of chronic pain,25 and patients endorsing chronic pain were administered the PEG. Nearly one-third of patients screened reported chronic pain.
Building on these findings, this study examines how the results of the screening and functional assessments, along with patient demographic and clinical characteristics, are associated with new diagnoses and treatments for pain. Based on the literature, we hypothesized that new diagnoses would be more common among women, African American and Latinx individuals, older adults, patients on Medicaid/Medicare, patients with greater physical health, mental health (MH) and substance use disorder (SUD) comorbidities, and those reporting severe pain on the PEG.3,4,18,25–27 We were uncertain as to whether new pain diagnoses and impairment identified after the new screening process would be associated with patient treatment.
Materials and Methods
Study Setting and Participants
Setting
This observational study took place at 13 sites of Community Health Center, Inc. (CHCI), Connecticut’s largest FQHC. CHCI patients are empaneled and have a designated primary care provider (PCP; a family practice physician, internist, or family nurse practitioner) working as part of a care team that includes a nurse, a medical assistant, and a co-located mental health provider. Patients may also receive on-site treatment from chiropractors and acupuncturists. Patients who require additional mental or physical health specialist care are referred for outside consultation. In addition, CHCI has a robust quality management process in place to carefully track and monitor opioid prescribing amongst its clinicians. CHCI’s screening process (described above)24 targeted all adult patients for chronic pain. All data for this study were extracted from the clinic electronic health records. Institutional Review Board (IRB) approval was obtained from the CHCI and Advarra IRBs (Protocol #1120 and Pro00022464, respectively) which also granted a waiver of consent and HIPAA authorization for this analysis of existing data. We followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline for observational studies.
Participants
The eligible population included adults aged 18+ who had an in-person primary care visit between July 2, 2018, and June 1, 2019. This study focused on patients who reported the presence of chronic pain on a screener and completed the PEG.
Data and Measures
PEG
Each item ranges from 0 to 10, with higher scores indicating greater pain intensity and/or interference, and the total score is calculated as the mean of the three. Scores of seven or higher indicate severe pain and interference.28–30
Pain Diagnoses
Pain diagnoses were grouped into nine broad International Classification of Disease version 10 (ICD-10)-based categories. Consensus on these categories was reached by a panel of eight academic and clinical experts on chronic pain who served on the project’s advisory panel.
We categorized patients into three groups based on presence and timing of the PCP assigning a pain diagnosis: 1) existing pain diagnosis (documented within one year prior to chronic pain screening); 2) newly documented pain diagnosis (no existing diagnosis and a documented pain diagnosis on the day of screening or within 90 days post-screening; 3) no documented pain diagnosis (no pain diagnosis in either period).
Mental Health (MH) and Substance Use Disorder (SUD)
MH or SUD diagnoses were categorized using the Healthcare Effectiveness Data and Information Set (HEDIS®) Mental Health Value Set and Alcohol and Other Drugs Abuse and Dependence Value Set, respectively.31
Other Chronic Medical Conditions
Other chronic medical conditions were coded using the Charlson Comorbidity Index for ICD-10 codes.32,33 A weighted score was calculated through the summation of an assigned weight of one to six for each condition. Higher weights indicate more severe morbidity.32,34
Treatment
The four types of pain treatment included onsite treatment with opioid analgesics, non-opioid analgesics, and referrals to on-site physical medicine (chiropractor, acupuncture), as well as external referrals to pain management specialist, rheumatology, orthopedic or neurological surgery, and physical therapy and rehabilitation. Three types of MH/SUD treatment included MH/SUD medications, visits to an onsite MH/SUD provider (ie, psychiatrist, psychiatric nurse, clinical psychologist, licensed clinical social worker, licensed professional counselor, marriage and family therapist, and/or alcohol and drug counselor), and external referrals to MH/SUD care.
We characterized whether treatment existed (present during the year before the screen) or was provided on the date of or within 90 days following a positive chronic pain screen.
Patient Characteristics
Demographic characteristics included age, sex, race, ethnicity, insurance, and preferred language.
Statistical Analyses
We first conducted multiple logistic regression analyses to examine 1) the association of patient-level demographics, clinical factors, and screening results with the likelihood of receiving a newly documented pain diagnosis following a positive screen, and 2) the association of patient factors and receipt of a newly documented pain diagnosis with receiving each of the seven treatment categories. All regression analyses were limited to patients without an existing pain diagnosis. In the first set of analyses, the independent variables were age, sex, race, ethnicity, insurance, preferred language, PEG severity, weighted Charlson Index, and presence of MH and SUD diagnoses. The second set of analyses also included the presence of newly documented pain diagnoses and the presence of treatment of the same modality as independent variables. For ease of interpretation, we used predictive margins to report average adjusted probability and absolute risk differences (ARDs), with 95% confidence intervals. For categorical variables, ARD represents the difference in adjusted probability of each outcome between patients with a given characteristic and the reference value. See Supplemental Table 1 for adjusted predicted probability values. Statistical analyses were performed using the R software/environment, version 3.6.3.
In addition to the primary analyses, cross-tabulations of each independent variable and Cramer’s V were evaluated to estimate strengths of relationships among categorical factors as a measure of multicollinearity. Results showed strong relationships among age, insurance type, and weighted Charlson Index, and between race and preferred language. Removing insurance type and preferred language from models resulted in minimal changes in coefficient estimates and model fit, and they were removed from final logistic regression models. Bonferroni correction was applied to analyses to account for multiple comparisons and decrease Type I error. Corrected p-values of p < 0.006 were used in the analyses to indicate significance with a family-wise error of α = 0.05.
Results
Patient Characteristics
The 10,091 adult primary care patients who reported chronic pain and completed the PEG assessment represented approximately 1/3 of the 31,600 patients screened and were on average 49.1 years old (SD = 13.7 years). The majority (60.3%) were women, Latinx (41.1%), had Medicaid insurance (62.0%), and preferred English (80.1%) as their primary language (Table 1).
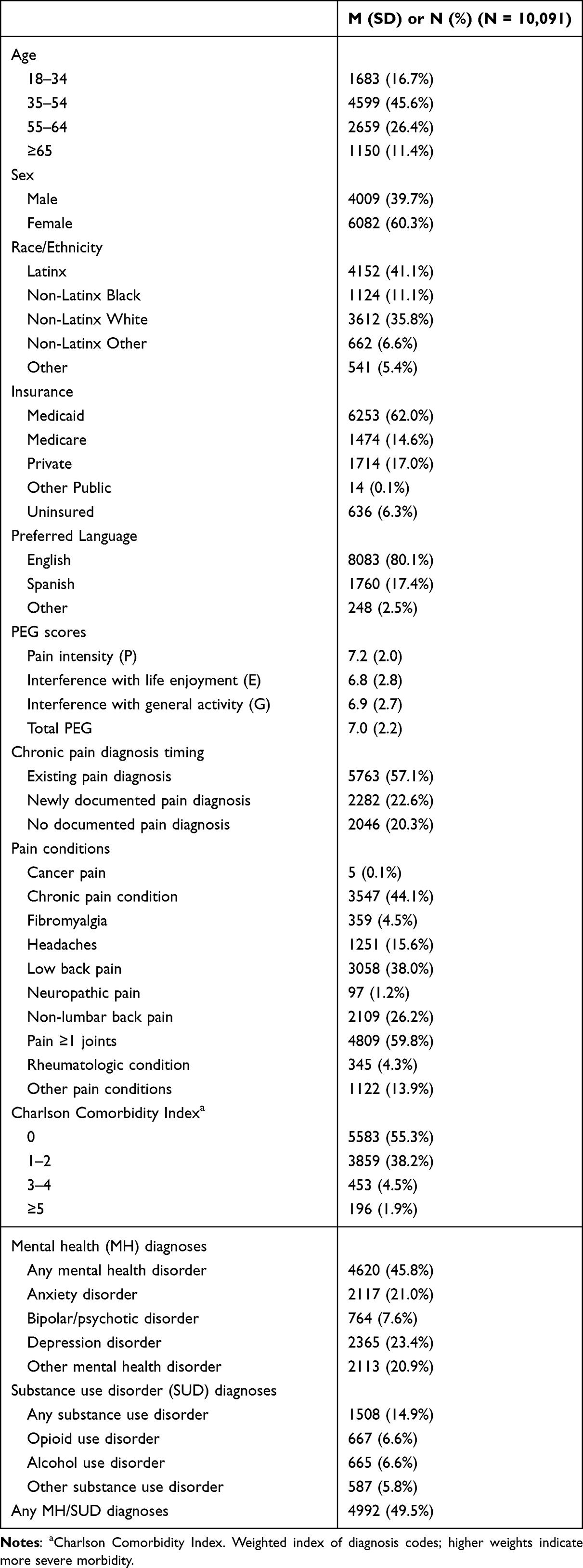 |
Table 1 Demographic and Clinical Characteristics of Patients with Self-Reported Chronic Pain (N = 10,091) |
On average, patients reported their pain severity and interference at the severe threshold (ie, PEG scores ≥7 out of 10). The majority of patients with self-reported chronic pain (57.1%) had an existing pain diagnosis documented in the prior year; 22.6% (n = 2282) had a pain diagnosis newly documented at the visit or within 90 days after, and 20.3% (n = 2046) had no pain diagnosis documented during either period. The most common pain diagnosis in the study group was pain in one or more joints (59.8%), followed by chronic pain condition (44.1%). While the majority, 55.3%, had no comorbid chronic medical conditions, half (49.5%) had at least one MH or SUD diagnosis.
Newly Documented Pain Diagnosis
Patients with severe PEG scores were more likely to receive a new pain diagnosis than patients with non-severe PEG scores (ARD = 13.2%, p < 0.0001) (Table 2). Patients with existing MH (ARD = −8.5%, p = <0.0001), SUD (ARD = −11.2%, p < 0.001), or chronic medical diagnoses (ARDs = −20.0% to −6.2%, ps <0.006) were significantly less likely to have a newly documented pain diagnosis. The only demographic factor associated with documentation of a new pain diagnosis was Latinx ethnicity; Latinx adults were more likely to receive a new pain diagnosis compared to non-Latinx White patients (ARD 8.6%, p < 0.0001). Post-hoc analyses related to this finding are detailed in Supplemental Methods and Supplemental Table 2.
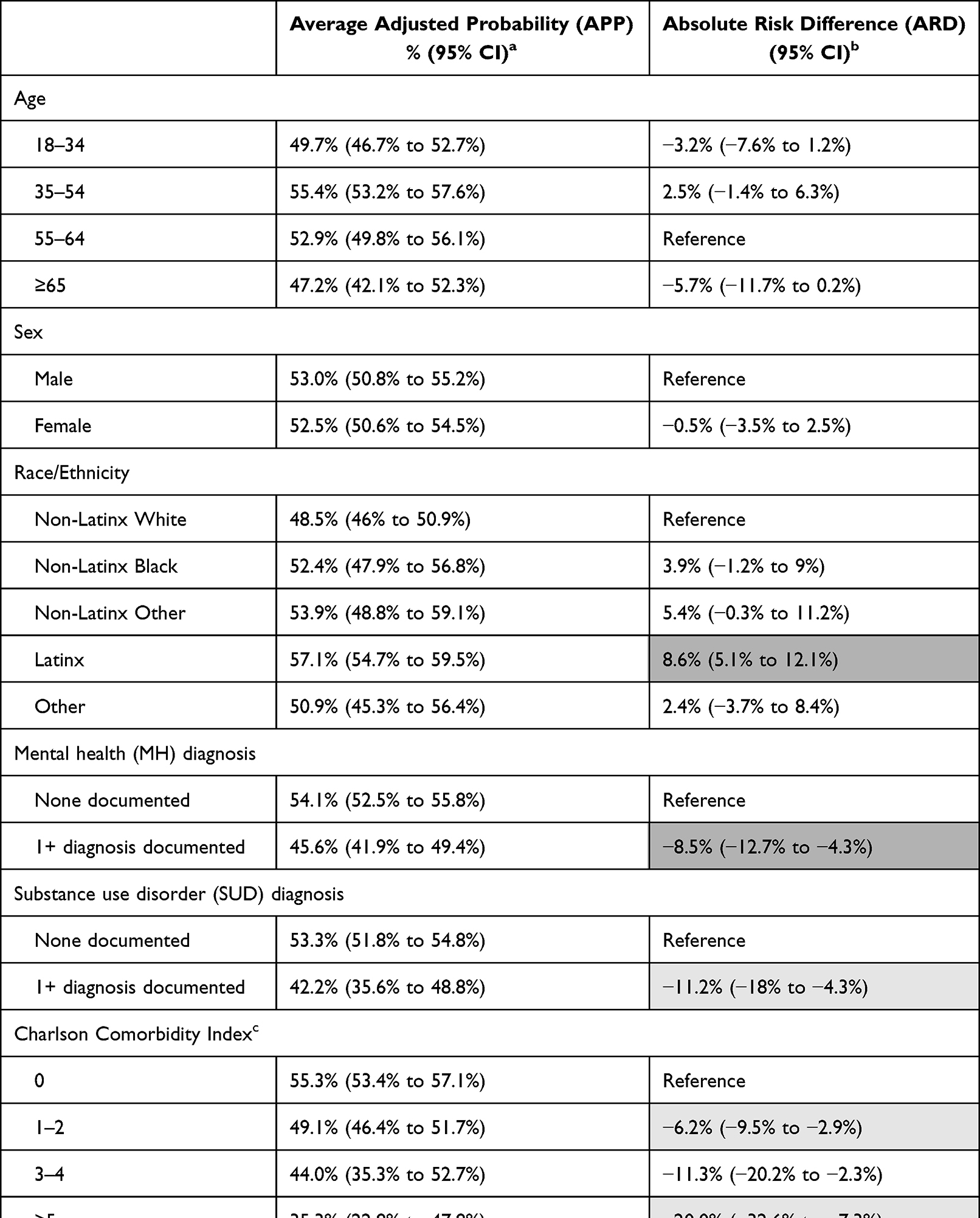 |
Table 2 Adjusted Probability of Newly Documented Pain Diagnosis Among Patients Who Self-Reported Chronic Pain and Did Not Have Existing Diagnosis (N = 4328) |
Treatment
Prevalence of Treatment Prior to and After Screening
Using unadjusted descriptive results, we found that non-opioid analgesic medications were the most common type of treatment both before and after chronic pain screening, followed by MH/SUD medications, regardless of whether patients had an existing, newly documented, or no documented pain diagnosis(Table 3). Among patients with an existing pain diagnosis, the number of individuals who received each type of treatment decreased after screening for all treatment categories (likely because the pre-screening period was a year versus only 90 days of post-screening follow-up). Among patients with a newly documented pain diagnosis, there was an increase after the screening in the number of patients receiving every type of treatment, including opioid medications.
 |
Table 3 Number of Patients Who Received Each Type of Treatment, Among Patients Who Self-Reported Chronic Pain, by Presence/Timing of Documented Pain Diagnosis (N = 10,091) |
Treatment After Screening Among Patients Without an Existing Pain Diagnosis
Adjusted results (Tables 4 and 5) show that across 4 of the 7 treatment types, prior treatment of the same modality had the largest significant association with the likelihood of receiving a specific treatment after screening (ARDs = 27.3% to 41.4%, ps <0.0001). Patients with newly documented pain diagnoses were significantly more likely to receive treatment for 5 of the 7 treatment types (ARDs = 3.2% to 27.4%, ps <0.001), with the largest magnitude for onsite physical medicine (ARD = 27.4%) and non-opioid analgesics (ARD = 27.0%). Severe PEG scores were also associated with a greater likelihood of all medical treatments and pain-related referrals (ARDs = 2.6% to 6.5%, ps<0.001).
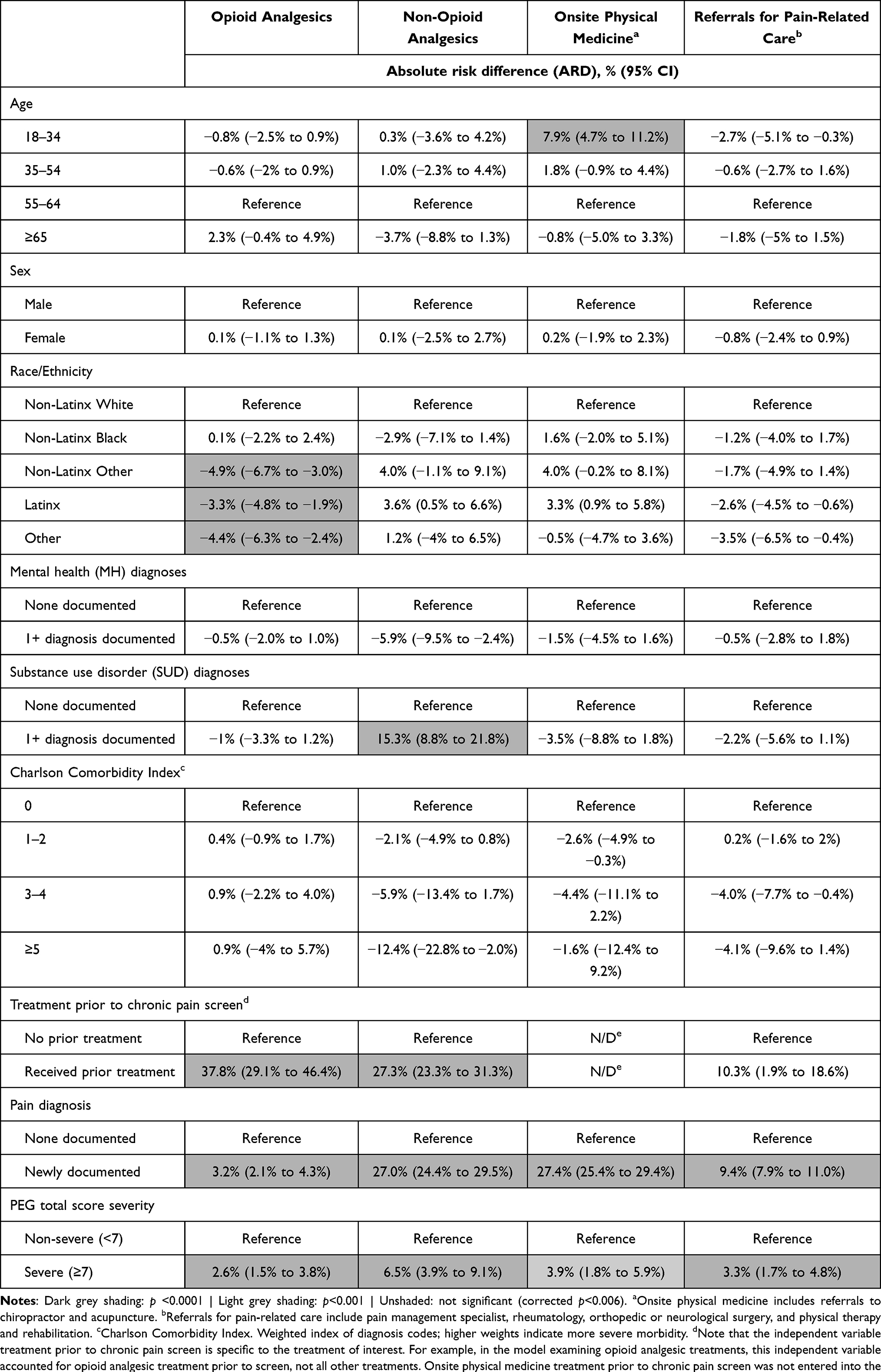 |
Table 4 Absolute Risk Difference (ARD) of Each Treatment Following Screening Among Patients with Self-Reported Chronic Pain and Without an Existing Pain Diagnosis (N = 4328) |
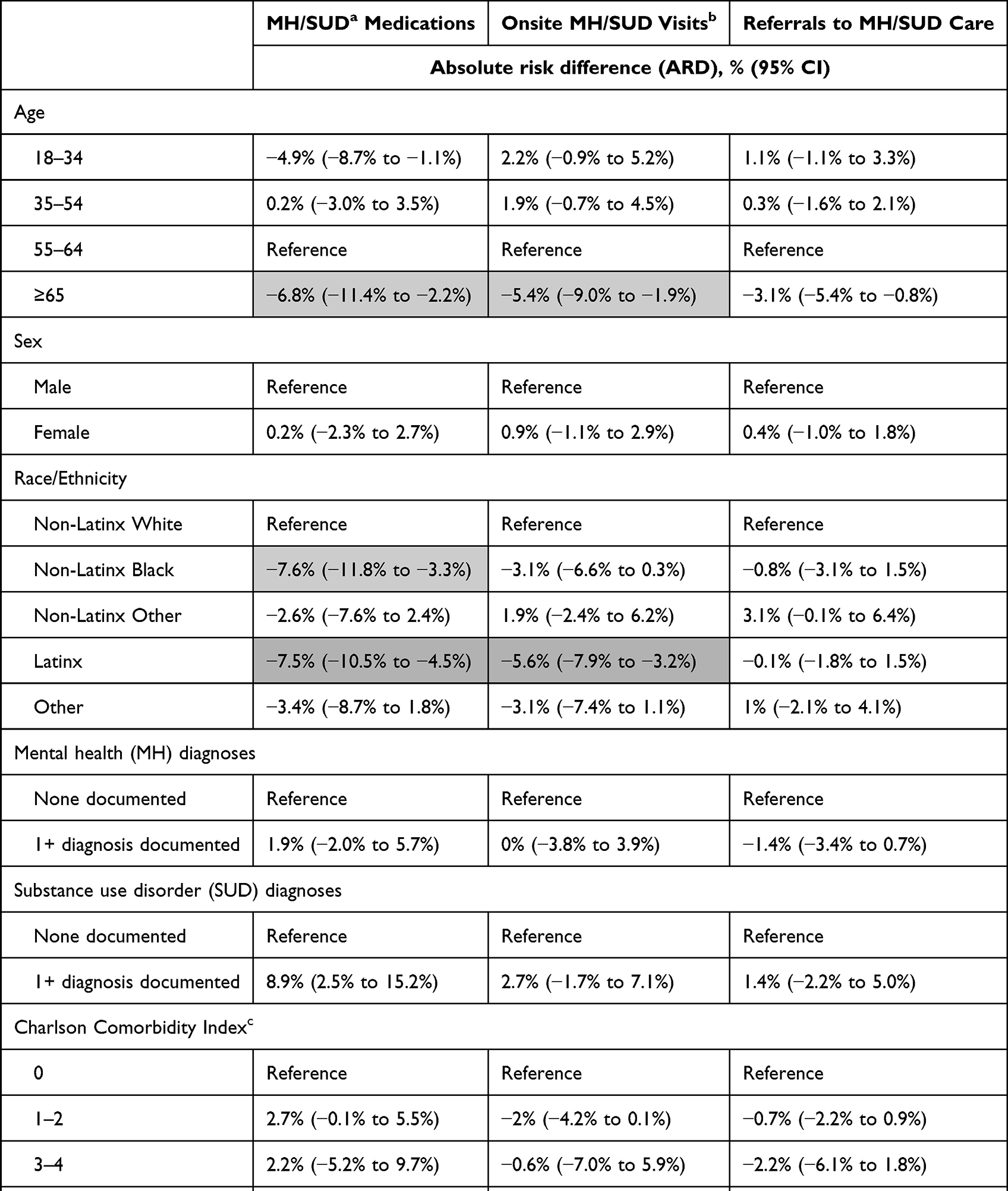 |
Table 5 Absolute Risk Difference (ARD) of Each Mental Health Treatment Following Screening Among Patients Who Self-Reported Chronic Pain on a Screener Without an Existing Pain Diagnosis (N = 4328) |
In general, demographic and other clinical factors were inconsistently associated with treatment and of comparatively smaller magnitude. Of note, Latinx patients were less likely to receive opioid medications and mental health treatments (ARDs = −7.5% to −3.3%; ps <0.001) compared to non-Latinx white patients. Post-hoc analyses related to this finding are detailed in Supplemental Table 2.
Discussion
In the context of routine screening for chronic pain with functional assessment of patients endorsing chronic pain, severe pain functional impairment was associated with the documentation of new pain diagnoses, and both pain severity and newly documented diagnoses were associated with initiation of new treatment. Approximately one in five patients with a positive chronic pain screen did not have a corresponding pain diagnosis documented prior to the screening, suggesting that the screening process helped clinicians identify and document new problems.
The indicators that had the largest and most consistent associations with treatment were clinical, not demographic, factors. While the variable with the largest effect was whether the patient previously received a given treatment prior to screening, a newly documented pain diagnosis and severe impairment on the PEG were also significantly associated with treatment. Severe overall PEG scores showed the largest association with non-opioid analgesics and mental health/SUD medications. Surprisingly, chronic medical illness comorbidities were not associated with the likelihood of receiving any type of treatment. This may reflect decreased statistical power due to zero inflation and a limited spread in the data, as over 55% of patients had no comorbid chronic illnesses, and 94% had two or fewer.
Contrary to our hypothesis, age and sex were not associated with receipt of a newly documented pain diagnosis, and the presence of MH/SUD or medical chronic conditions were inversely associated with this outcome. A reason for this unexpected finding may be that prior studies examined patients’ likelihood of reporting chronic pain, rather than their likelihood of receiving a pain diagnosis.
A notable finding was that compared to non-Latinx White patients, Latinx patients were not only more likely to have a history of documented pain diagnosis, but they were also nearly 10% more likely to receive a newly documented pain diagnosis following a positive screen. Post-hoc analyses suggested that regardless of preferred language, patients of Latinx ethnicity were more likely to report higher chronic pain severity, which increased the likelihood of receiving a newly documented pain diagnosis. Latinx patients were also less likely to receive opioid analgesics for chronic pain and were no more likely to receive any other types of treatment. These findings are in line with the literature, in which some studies have found that Latinx adults report higher pain severity compared to their non-White counterparts,35,36 but have consistently been found to be less likely to receive opioid analgesic medications.37–39 Fear of adverse outcomes39 and cultural beliefs40 have been commonly identified as contributing factors to lower opioid use among Latinxs. Our results of lower opioid analgesic treatment among Latinx patients highlight the importance of patient education and public health information to the Latinx community regarding evidence-based chronic pain treatment.
This study fills an important gap in the literature by examining the patterns of pain diagnoses and treatment in the presence of routine screening for chronic pain and assessment of functional impairment. To our knowledge, this is the largest study reporting on PEG results in a primary care setting, and uniquely focused on medically underserved populations. Another strength of the study is the examination of pain and MH in clinics with co-located mental health treatment, allowing for an accurate understanding of the nuances in the types of MH/SUD treatments received and factors most strongly associated with them.
Limitations
The study provides only observational data on the associations between screening and assessment results. The observational nature of the study limited our capability to examine whether pain-related treatments represented short-term or continuous management of symptoms. Since our list of chronic pain conditions did not include mental health conditions, which may have been comorbid with a chronic pain complaint and may have exacerbated pain, we were also unable to assess whether there was a continuous pattern of bifurcation in the treatment of chronic pain versus MH disorders. Additional longitudinal research is needed to assess this possibility. Our data are derived from patients at a single federally qualified health center treating medically underserved patients and may not be generalizable to other primary care settings.
Conclusion
In this large observational study, we examined factors most associated with newly documented pain diagnosis and treatment following chronic pain screening and functional assessment in a population of medically underserved adults in a large FQHC. Results showed that implementing patient-reported tools may influence diagnosis and treatment for patients with chronic pain, even after accounting for demographic and other clinical factors. While a comprehensive clinical assessment remains invaluable, brief screening tools, such as the PEG, offer a quick, inexpensive, reliable, and valid method to identify patients at risk for chronic pain and inform symptom management and treatment. This is especially salient in high-volume and short appointment duration settings, such as primary care clinics, where over half of patients with chronic pain receive their care.
Acknowledgments
The authors acknowledge Dr. Mary Barton (NCQA), Dr. Bennet Davis (Sierra Tucson), Dr. Antoinette Giedzinska (Sierra Tucson), Dr. Kurt Kroenke (Indiana University Center for Health Services and Outcomes Research, Regenstrief Institute, Inc.), Dr. Karl Lorenz (Stanford University), Dr. Alpa Patel (Aetna), Christin Veasley (Chronic Pain Research Alliance), and Dr. Michael VonKorff (Kaiser Permanente Washington Health Research Institute) for their important contributions as advisory panel members to the parent study. We also thank Zack Manville, BGS, at Community Health Center, Inc., for data support, and Manasi Tirodkar, PhD, MS, and Liz Hart, MPH, at the National Committee for Quality Assurance for research support, and CHCI patients for their participation in this study.
Funding
This project was supported by grant number 5R18HS025354-02 from the Agency for Healthcare Research and Quality. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality. The funding organization had no role in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; and the decision to submit the manuscript for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dueñas M, Ojeda B, Salazar A, et al. A review of chronic pain impact on patients, their social environment and the health care system. J Pain Res. 2016;9:457–467. doi:10.2147/JPR.S105892
2. Gaskin DJ, Richard P. The economic costs of pain in the United States. J Pain. 2012;13(8):715–724. doi:10.1016/j.jpain.2012.03.009
3. Gormsen L, Rosenberg R, Bach FW, et al. Depression, anxiety, health-related quality of life and pain in patients with chronic fibromyalgia and neuropathic pain. Eur J Pain. 2010;14(2):
4. Tunks ER, Weir R, Crook J. Epidemiologic perspective on chronic pain treatment. Can J Psychiatry Rev Can Psychiatr. 2008;53(4):235–242. doi:10.1177/070674370805300404
5. Racine M. Chronic pain and suicide risk: a comprehensive review. Prog Neuropsychopharmacol Biol Psychiatry. 2018;87:269–280. doi:10.1016/j.pnpbp.2017.08.020
6. Hser Y-I, Mooney LJ, Saxon AJ, et al. Chronic pain among patients with opioid use disorder: results from electronic health records data. J Subst Abuse Treat. 2017;77:26–30. doi:10.1016/j.jsat.2017.03.006
7. Dansie EJ, Turk DC. Assessment of patients with chronic pain. BJA Br J Anaesth. 2013;111(1):19–25. doi:10.1093/bja/aet124
8. Krebs EE, Carey TS, Weinberger M. Accuracy of the pain numeric rating scale as a screening test in primary care. J Gen Intern Med. 2007;22(10):1453–1458. doi:10.1007/s11606-007-0321-2
9. Interagency Pain Research Coordinating Committee (IPRCC). National Pain Strategy: A Comprehensive Population Health-Level Strategy for Pain. US Department of Health and Human Services, National Institutes of Health; 2016.
10. Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain — United States, 2016. MMWR Recomm Rep. 2016;65:1–49. doi:10.15585/mmwr.rr6501e1
11. Boyce MB, Browne JP. Does providing feedback on patient-reported outcomes to healthcare professionals result in better outcomes for patients? A systematic review. Qual Life Res. 2013;22(9):2265–2278. doi:10.1007/s11136-013-0390-0
12. Valderas JM, Kotzeva A, Espallargues M, et al. The impact of measuring patient-reported outcomes in clinical practice: a systematic review of the literature. Qual Life Res. 2008;17(2):179–193. doi:10.1007/s11136-007-9295-0
13. Krebs EE, Lorenz KA, Bair MJ, et al. Development and initial validation of the PEG, a three-item scale assessing pain intensity and interference. J Gen Intern Med. 2009;24(6):733–738. doi:10.1007/s11606-009-0981-1
14. Goldsmith ES, Taylor BC, Greer N, et al. Focused evidence review: psychometric properties of patient-reported outcome measures for chronic musculoskeletal pain. J Gen Intern Med. 2018;33(Suppl 1):61–70. doi:10.1007/s11606-018-4327-8
15. Krebs EE, Bair MJ, Damush TM, et al. Comparative responsiveness of pain outcome measures among primary care patients with musculoskeletal pain. Med Care. 2010;48(11):1007–1014. doi:10.1097/MLR.0b013e3181eaf835
16. Harle CA, Bauer SE, Hoang HQ, Cook RL, Hurley RW, Fillingim RB. Decision support for chronic pain care: how do primary care physicians decide when to prescribe opioids? A qualitative study. BMC Fam Pract. 2015;16(1):48. doi:10.1186/s12875-015-0264-3
17. Von Korff M, Scher AI, Helmick C, et al. United States national pain strategy for population research: concepts, definitions, and pilot data. J Pain. 2016;17(10):1068–1080. doi:10.1016/j.jpain.2016.06.009
18. Camilloni A, Nati G, Maggiolini P, et al. Chronic non-cancer pain in primary care: an Italian cross-sectional study. Signa Vitae. 2021;17(2):54–62.
19. Smith BH, Hardman JD, Stein A, Colvin L. Managing chronic pain in the non-specialist setting: a new SIGN guideline. Br J Gen Pract. 2014;64(624):e462–e464. doi:10.3399/bjgp14X680737
20. Militello LG, Hurley RW, Cook RL, et al. Primary care clinicians’ beliefs and strategies for managing chronic pain in an era of a national opioid epidemic. J Gen Intern Med. 2020;35(12):3542–3548. doi:10.1007/s11606-020-06178-2
21. Butchart A, Kerr EA, Heisler M, Piette JD, Krein SL. Experience and management of chronic pain among patients with other complex chronic conditions. Clin J Pain. 2009;25(4):293–298. doi:10.1097/AJP.0b013e31818bf574
22. Zelaya CE, Dahlhamer JM, Lucas JW, Connor EM. Chronic pain and high-impact chronic pain among US adults, 2019. NCHS Data Brief. 2020;2020(390):1–8.
23. Glei DA, Weinstein M, Latham-Mintus K. Disadvantaged Americans are suffering the brunt of rising pain and physical limitations. PLoS One. 2021;16(12):e0261375. doi:10.1371/journal.pone.0261375
24. Bifulco L, Anderson DR, Blankson ML, et al. Evaluation of a chronic pain screening program implemented in primary care. JAMA Netw Open. 2021;4(7):e2118495. doi:10.1001/jamanetworkopen.2021.18495
25. Dahlhamer J, Lucas J, Zelaya, C. Prevalence of chronic pain and high-impact chronic pain among adults - United States, 2016. MMWR Morb Mortal Wkly Rep. 2018;67(36):1001–1006. doi:10.15585/mmwr.mm6736a2
26. Marco CA, Nagel J, Klink E, et al. Factors associated with self-reported pain scores among ED patients. Am J Emerg Med. 2012;30(2):331–337. doi:10.1016/j.ajem.2010.12.015
27. Marco CA, Kanitz W, Jolly M. Pain scores among emergency department (ED) patients: comparison by ED diagnosis. J Emerg Med. 2013;44(1):46–52. doi:10.1016/j.jemermed.2012.05.002
28. Atkinson TM, Mendoza TR, Sit L, et al. The brief pain inventory and its “pain at its worst in the last 24 hours” item: clinical trial endpoint considerations. Pain Med. 2010;11(3):337–346. doi:10.1111/j.1526-4637.2009.00774.x
29. Jones KR, Vojir CP, Hutt E, et al. Determining mild, moderate, and severe pain equivalency across pain-intensity tools in nursing home residents. J Rehabil Res Dev. 2007;44(2):305–314. doi:10.1682/JRRD.2006.05.0051
30. Serlin RC, Mendoza TR, Nakamura Y, et al. When is cancer pain mild, moderate or severe? Grading pain severity by its interference with function. Pain. 1995;61(2):277–284. doi:10.1016/0304-3959(94)00178-H
31. NCQA. HEDIS 2019 Technical Specifications. Vol. 2. NCQA; 2019.
32. Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
33. Glasheen WP, Cordier T, Gumpina R, et al. Charlson comorbidity index: ICD-9 update and ICD-10 translation. Am Health Drug Benefits. 2019;12(4):188–197.
34. Austin SR, Wong Y-N, Uzzo RG, et al. Why summary comorbidity measures such as the Charlson Comorbidity Index and Elixhauser score work. Med Care. 2015;53(9):e65–e72. doi:10.1097/MLR.0b013e318297429c
35. Carey TS, Freburger JK, Holmes GM, et al. Race, care seeking and utilization for chronic back and neck pain: population perspectives. J Pain. 2010;11(4):343–350. doi:10.1016/j.jpain.2009.08.003
36. Portenoy RK, Ugarte C, Fuller I, et al. Population-based survey of pain in the United States: differences among white, African American, and Hispanic subjects. J Pain. 2004;5(6):317–328. doi:10.1016/j.jpain.2004.05.005
37. Hollingshead NA, Vrany EA, Stewart JC, et al. Differences in Mexican Americans’ prevalence of chronic pain and co-occurring analgesic medication and substance use relative to non-Hispanic white and black Americans: results from NHANES 1999–2004. Pain Med. 2016;17(6):1001–1009. doi:10.1093/pm/pnv003
38. Meghani SH, Byun E, Gallagher RM. Time to take stock: a meta-analysis and systematic review of analgesic treatment disparities for pain in the United States. Pain Med. 2012;13(2):150–174. doi:10.1111/j.1526-4637.2011.01310.x
39. Katz JN, Lyons N, Wolff LS, et al. Medical decision-making among Hispanics and non-Hispanic Whites with chronic back and knee pain: a qualitative study. BMC Musculoskelet Disord. 2011;12:78. doi:10.1186/1471-2474-12-78
40. Monsivais DB, Engebretson JC. “I’m just not that sick”: pain medication and identity in Mexican American women with chronic pain. J Holist Nurs. 2012;30(3):188–194. doi:10.1177/0898010112440885
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.