Back to Journals » Patient Preference and Adherence » Volume 19
Applying the Timing It Right Framework to Caregiver Experiences and Needs in Adult Percutaneous Endoscopic Gastrostomy: A Longitudinal Qualitative Study
Authors Li X, Zhang X, Guo Y, Ruan W
Received 29 September 2025
Accepted for publication 23 December 2025
Published 31 December 2025 Volume 2025:19 Pages 4353—4367
DOI https://doi.org/10.2147/PPA.S571124
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Emma Veale
Xi Li,1,2 Xinru Zhang,1,2 Yu Guo,1 Weiqing Ruan1
1Huiqiao Medical Center, Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong, 510515, People’s Republic of China; 2School of Nursing, Southern Medical University, Guangzhou, Guangdong, 510515, People’s Republic of China
Correspondence: Weiqing Ruan, Huiqiao Medical Center, Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong, 510515, People’s Republic of China, Tel +86 13533399913, Email [email protected]
Purpose: Applying the Timing It Right (TIR) theoretical framework, we explored the evolving experiences and needs of caregivers supporting adult percutaneous endoscopic gastrostomy (PEG) patients during different cycles of PEG placement, within a Chinese cultural context.
Patients and Methods: A descriptive phenomenological research design was used to select 12 family caregivers of PEG patients in a tertiary hospital in Guangzhou from December 2024 to June 2025 through purposive sampling combined with the maximum difference strategy. Based on the TIR framework, the PEG course was divided into five stages (diagnosis, stabilization, discharge preparation, adjustment, and adaptation). Semi-structured in depth interviews were conducted with caregivers at each stage. The Colaizzi 7-step method and NVivo V.17 software were used to analyze the data and extract themes.
Results: The themes of the experiences and needs of PEG caregivers at different stages were as follows: 1. Diagnostic stage: anxiety and worry, lack of disease awareness, and passivity in medical decision-making. 2. Stabilization stage: coping with the postoperative comfort management needs of patients and sense of treatment benefit. 3. Discharge readiness stage: caregiving skills training needs and resource accessibility concerns. 4. Adjustment stage: continuity of care needs, daily care challenges (wound care needs, gastrostomy tube adjustment period), and caregiver socioeconomic role reconstruction. 5. Adaptation period: rehabilitation expectations, reality conflicts, and self-efficacy enhancement.
Conclusion: The notable variations in the demands and experiences of PEG caregivers at various phases of caregiving highlighted how crucial it was to create a staged support system that was accurate and culturally sensitive to maximize healthcare resources and effectively empower caregivers.
Keywords: experience and needs, percutaneous endoscopic gastrostomy, caregivers, timing it right theory, qualitative research
Introduction
Percutaneous endoscopic gastrostomy (PEG) is the main nutritional support for patients with long-term swallowing dysfunction.1 It has the advantages of minimal invasiveness, low risk of infection, and preservation of patient dignity.2 PEG has been increasingly used in the management of neurological disorders and head and neck tumors.3,4 According to the American College of Gastroenterology, there are about 200,000 PEG tube placements per year in the United States alone.5 Similar figures have been confirmed by studies in Taiwan.6 With the development of medical technology, the number of patients selecting PEG therapy continues to grow.
Due to primary disease limitations, most PEG patients rely on family caregivers for basic daily activities, gastrostomy tube maintenance, nutritional feeding, and management of complications.7 This leads to changes in the lifestyle of the caregiver and accumulated fatigue resulting in decreased quality of life, sleep disorders, and psychological problems.8,9 In the context of traditional Chinese culture, the concept of family and filial piety ethic has further strengthened the role of close relatives as primary caregivers,10 placing them under a heavier pressure of responsibility.11 At the same time, structural challenges such as uneven distribution of healthcare resources and weak community support systems12 exacerbate the difficulty for caregivers to access professional support.
The increased burden on caregivers not only reduces the quality of care but also hinders the recovery of patients and jeopardizes their psychological well-being13. Studies have shown that high caregiver burden is significantly associated with increased rates of medication errors and poor care practices.14 A prospective observational study showed that the severe burden on stroke caregivers threatens the sustainability of care and compromises the recovery of stroke survivors.15 Notably, the recovery cycle for PEG patients often lasts months or even years, and the experiences and needs of caregivers may change dynamically with disease stage. However, existing studies focusing on the experiences and needs of the caregivers who assist PEG patients are scarce.7,16 The unique challenges faced by these caregivers, especially in the Chinese cultural context, have not been fully explored. Moreover, they are mostly limited to static needs analysis and lack tracking of dynamic changes in the full cycle of caregiving.
The Timing It Right (TIR) theory was developed by Cameron and Gignac,17 who categorized disease trajectory into five stages: diagnosis, stabilization, readiness for discharge, adjustment, and adaptation. The theory has been effective in identifying the needs of family caregivers at different stages of a patient’s disease trajectory and has been successfully applied in care studies of patients with chronic disease, such as stroke18 and heart failure.19 This study used a phenomenological qualitative research approach, based on the TIR theoretical framework, using semi-structured interviews and Colaizzi’s phenomenological analysis method to explore the changes in the experiences of PEG caregivers at different stages of the disease. Additionally, it identified the specific needs and challenges of the caregiver throughout the PEG total care process, providing a basis for caregivers to establish a stage-specific support system.
Materials and Methods
Subjects
Family caregivers of patients who were hospitalized, received PEG for the first time, and were discharged from a tertiary care hospital in Guangzhou City from December 2024 to June 2025 were selected using the principles of purposive and maximum difference sampling methods.
Patient inclusion criteria were (1) patients who underwent PEG for the first time according to the criteria of the American Society for Gastrointestinal Endoscopy and (2) ages ≥18 years.
Patient exclusion criteria were (1) survival expectancy <3 months and (2) patients who were unable to continue treatment because their condition worsened.
Inclusion criteria for caregivers were (1) age ≥18 years; (2) caregiving hours ≥4 hours per day and more than 3 consecutive months; (3) able to read and express Chinese, with normal cognitive and communication skills; and (4) informed consent and voluntary participation in this study.
Exclusion criteria for caregivers were (1) those who had participated in PEG-related training and (2) paid caregivers, such as babysitters.
Stage Design
Based on the TIR theoretical framework and integrating the specific characteristics of the PEG procedure in consultation with experts in digestive endoscopy, rehabilitation care, and other related fields, five phases were identified: diagnosis, stabilization, discharge preparation, adjustment, and adaptation. The diagnostic period was from the day before the patient was admitted to the hospital to the day before the decision was made to undergo PEG, which usually lasted 3–7 days. The stabilization period was the time between the patient’s surgery and postoperative stabilization. This period usually lasted 1–3 days. Preparation for discharge was the period between the time the patient met the medical criteria for discharge and the time of discharge, which was usually from 3 days after surgery to the day of discharge. The adjustment period began when the patient was discharged home to 1 month after the PEG procedure. The adaptation period lasted from 1 month to 3 months after PEG.
Data Collection
Following the approval of this study by the hospital ethics committee, participants were recruited using a maximum difference strategy in purposive sampling. The purposive sampling was based on key dimensions including the caregiver’s age, gender, educational level, occupation, and place of residence, as well as the patient’s primary diagnosis, with the aim of ensuring broad sample heterogeneity.In our recruitment process, we consciously identified and invited diverse caregivers based on these dimensions to ensure the sample could capture the broadest possible range of experiences.The research team systematically reviewed the demographic and clinical data of patients who were to undergo PEG, jointly assessed the patient’s condition and family caregiver status with the attending physician and charge nurse.Prior to the formal interviews, routine nursing guidance and health education were provided to the caregivers by the attending physicians and nurses, in accordance with the hospital guidelines.After referral by the charge nurse, the researcher obtained written informed consent from the caregiver detailing the purpose of the study, voluntary participation and withdrawal rights, and confidentiality measures, such as data coded anonymously and used only for the study. Interviews were conducted in both face-to-face (inpatient/outpatient) and WeChat video (for those with limited mobility) modes. In the inpatient phase (diagnostic, stabilization, and preparation for discharge), a separate conference room was used, avoiding treatment/rest periods. In the post-discharge phase (adjustment and acclimatization), a private space in the waiting area was used to maximize opportunities for outpatient follow-up. For those unable to attend the hospital, a WeChat video interview was arranged, with the time of day being determined by the convenience of the caregiver. Each interview lasted 20–40 minutes, and a total of 12 caregivers were included (covering all five phases), with no lost cases. The outline of the interview was based on the literature review, reviewed and revised by two gastroenterologists and two senior nursing experts, and the wording and process were optimized through two pre-interviews. The interview outline is shown in Figure 1.The criterion for data saturation was two consecutive interviews with no new themes. A reflective memo was written by the researcher immediately after the interview to record nonverbal information and methodological reflections.The interview transcripts and illustrative quotes for publication were translated by two bilingual research team members, and the translations were cross-checked by the principal investigator to ensure accuracy and conceptual equivalence.
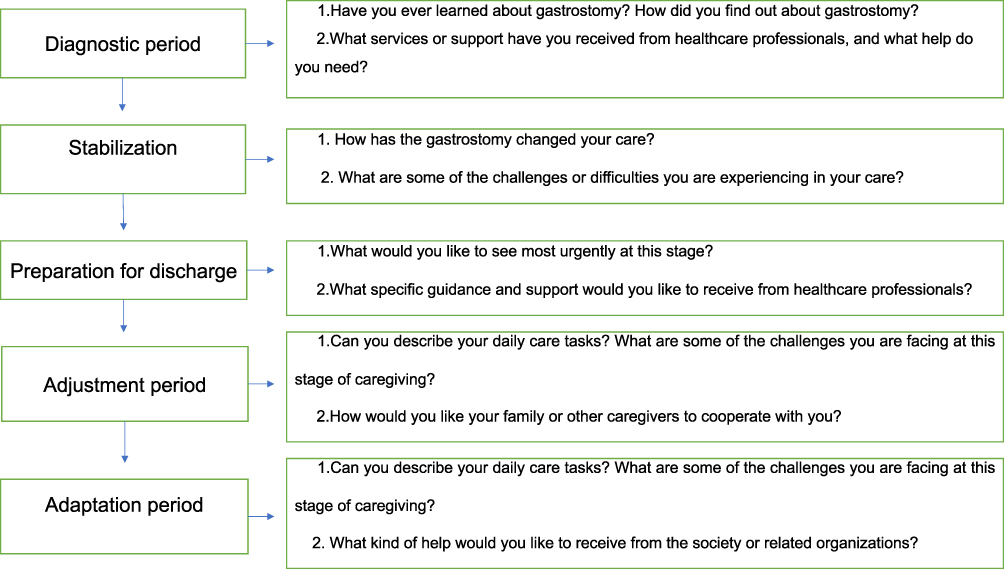 |
Figure 1 Outline of PEG caregiver interviews. |
Rigor
Researcher Background and Training: All interviews were conducted by the first author, who had received ≥40 hours of training in the qualitative research system, was the nurse-in-charge of some patients, and had established a strong foundation of trust with the patients. We communicated the purpose of the study clearly, the principle of confidentiality, and the right to voluntary participation before the interviews. After authorization, the interviews were recorded and synchronized with nonverbal behaviors, such as facial expressions, body movements, emotional fluctuations, etc. During the interviews, communication skills were used to create an open atmosphere. We used open-ended follow-up questions, such as “Can you further describe what you felt at that time?” We explored the deeper level of experience and strictly avoided induced questions. We used instant member verification, such as “I understand that you are saying. Right?” This ensured accuracy of information; ongoing reflection by the researcher on personal biases, e.g, the influence of clinical context on interpretation, and documentation through memos.
Data Analysis
Audio recordings were transcribed verbatim into text and organized within 24 hours of each interview. The data were then imported into NVivo 17 software. The Colaizzi phenomenological seven-step analysis method was used for data processing20. This proceeded as follows. (1) Immersion reading: the researcher repeatedly and intensively read all the transcribed interviews and reflective memos to initially grasp the core narrative strands. (2) Meaningful unit extraction: line-by-line annotation of meaningful statements relevant to the PEG caregiver’s experience. (3) Initial coding: open coding of the extracted statements to form an initial code base. (4) Thematic clustering: summarizing the associated codes into thematic clusters and establishing a thematic-subthematic hierarchical structure. (5) Thematic refinement and integration: cross-checking the formed thematic framework with the original transcript, resolving the dynamic associations between the themes (eg, the evolution of needs at different stages of the disease process) through team discussions. (6) Description of the nature of the phenomenon: construct a structured model of the PEG caregiver’s multi-stage experience (diagnosis → stabilization → discharge→ adjustment → adaptation), with detailed descriptions of the core themes at each stage. (7) Participant feedback and validation: Guided by the results of the thematic analysis, five participants representing the maximum variation in caregiver age, patient diagnosis, relationship to the patient, and reported caregiving challenges were identified for member checking.
Ethical Compliance
The study strictly implemented the guidelines of the Declaration of Helsinki, ethical approval number NFEC-202411-K24-01. Informed consent was obtained using double confirmation of written and verbal explanations, the interview venue ensured soundproofing, and the original recordings were stored on a password-protected standalone hard disk accessible only to the research team. Interviews were conducted anonymously and numbered instead of named to protect the privacy of the interviewees. The participants’ informed consent included publication of their anonymized responses and direct quotes.Participants were compensated with a care brochure and could request a summary of the study at any time.
Results
General Information About Participants
Twelve caregivers participated in all four interviews; eight were female and four were male, ranging in age from 28 to 61. The general profiles of the respondents are shown in Table 1 and the extracted themes are shown in Table 2.
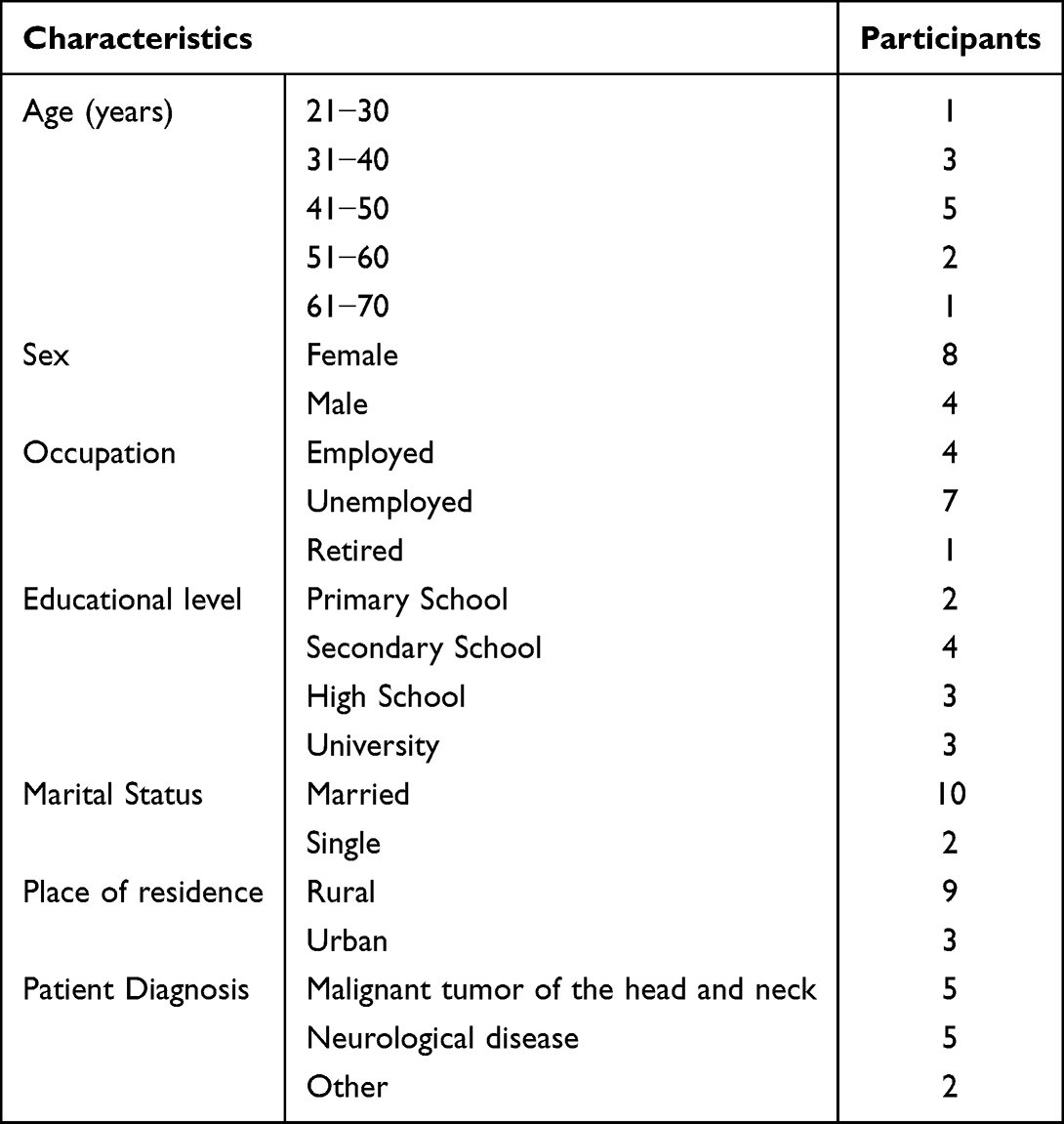 |
Table 1 General Information of the Interviewed Participants |
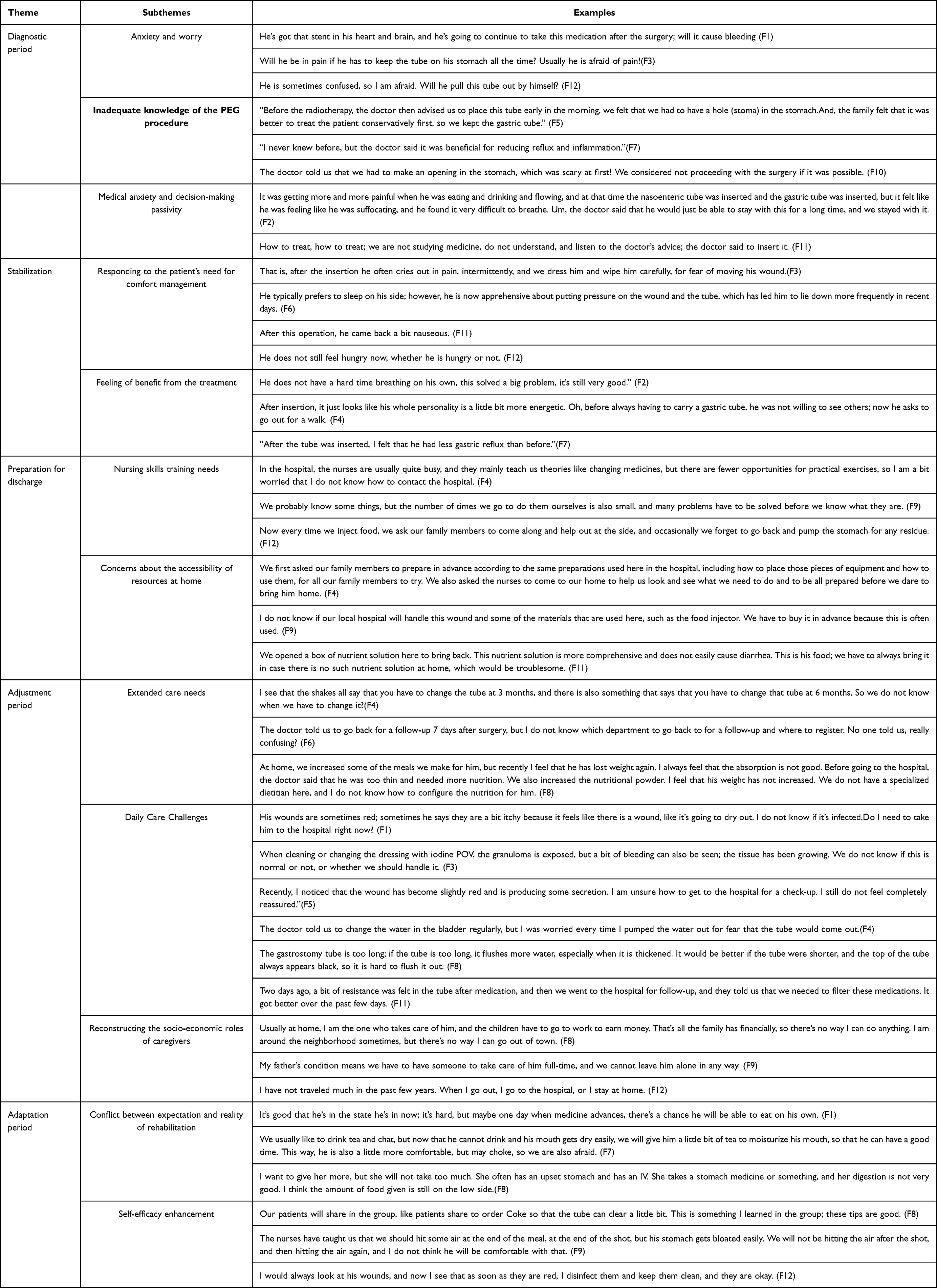 |
Table 2 Extracted Themes |
Themes
Diagnostic Period: Anxiety and Decision-Making Passivity
Subtheme 1: Anxiety and Worry
Patients who undergo PEG surgery usually need long-term medication due to the combination of other diseases (eg, cardiovascular disease, head and neck malignant tumors). Approximately 3 to 7 days before the operation, healthcare professionals will carry out relevant preoperative preparations and medication adjustments for those patients using anticoagulant medications. Consequently, caregivers may confront the risks of the operation (eg, bleeding, pain) and develop preoperative anxiety.In addition, caregivers also expressed concerns about post-procedural tube safety.
F1: He’s got that stent in his heart and brain, and he’s going to continue to take this medication after the surgery; will it cause bleeding?
F3: Will he be in pain if he has to keep the tube on his stomach all the time? Usually, he is afraid of pain!
F12: He is sometimes confused, so I’m afraid. Will he pull this tube out by himself?
Subtheme 2: Inadequate Knowledge of the PEG Procedure
Most of the caregivers had insufficient knowledge about the PEG procedure. Due to the influence of traditional Chinese culture and the concept of end-of-life body integrity, the acceptance of a permanent abdominal stoma was low.Some family members tended to choose conservative treatments (eg, nasogastric tubes) for their patients because of their fear of surgery.
F5: Before the radiotherapy, the doctor advised us to place this tube early in the morning. But at that time, we felt that we had to have a hole (stoma) in the stomach. Ah, the family felt that it was better to treat the patient conservatively first, so we kept the gastric tube.
F7: I never knew before, but the doctor said it was beneficial for reducing reflux and inflammation.
F10: The doctor told us that we had to make an opening in the stomach, which was scary at first! We considered not proceeding with the surgery if it was possible.
Subtheme 3: Passivity in Medical Decision-Making
Due to insufficient knowledge of the PEG procedure, some caregivers relied on the advice of doctors in decision-making and had a high level of trust in doctors.
F2: It was getting more and more painful when he was eating and drinking, and at that time, the nasoenteric tube was inserted, and the gastric tube was inserted, but it felt like he was suffocating, and he found it very difficult to breathe. Um, the doctor said that he would just be able to stay with this for a long time, and we stayed with it.
F11: How to treat, how to treat; we are not studying medicine, do not understand, and listen to the doctor’s advice; the doctor said to insert it.
Stabilization: Responding to Patient Comfort Management Needs and Perceived Benefits
Subtheme 1: Responding to Patient Comfort Management Needs
After PEG surgery, patients undergo a radical change in the way they eat and have abdominal wounds. Patients have wound pain and psychological and somatic perception changes after surgery. As a result, caregivers and medical teams need to provide patients with fine-tuned nursing interventions and psychological support.
F3: That is, after the insertion, he often cries out in pain, intermittently, and we dress him and wipe him carefully, for fear of moving his wound.
F6:He typically prefers to sleep on his side; however, he is now apprehensive about putting pressure on the wound and the tube, which has led him to lie down more frequently in recent days.
F11: After this operation, he came back a bit nauseous.
F12: He doesn’t feel hungry now, whether he is hungry or not.
Subtheme 2: Perceived Benefit of Treatment
Most caregivers recognized that PEG enhanced the comfort of the patient and willingness to socialize, improve nutritional intake, and increase compliance with treatment.
F2: He doesn’t have a hard time breathing on his own; this solved a big problem, it’s still very good.
F4: After insertion, it just looks like his whole personality is a little bit more energetic. Oh, before always having to carry a gastric tube, he was not willing to see others; now he asks to go out for a walk.
F7: After the tube was inserted, I felt that he had less gastric reflux than before.
Preparation for Discharge: Training Required Nursing Skills and Resource Accessibility Concerns
Subtheme 1: Training Required Nursing Skills
Most patients discharged from the hospital had incompletely healed fistulas, while healthcare professionals had limited time to train caregivers in appropriate care techniques. Caregivers lacked hands-on confidence in home care practices, such as dressing changes, sterilization procedures, and enteral nutrition infusions, especially when confronted with them for the first time. Additionally, caregivers wanted their family members to be involved in the learning process to cope with possible emergencies.
F4: In the hospital, the nurses are usually quite busy, and they mainly teach us theories like changing medicines, but there are fewer opportunities for practical exercises, so I am a bit worried that I don’t know how to contact the hospital.
F9: We probably know some things, but the number of times we do them ourselves is small, and many problems have to be solved before we know what they are.
F12: Now every time we inject food, we ask our family members to come along and help out at the side, and occasionally we forget to go back and pump the stomach for any residue.
Subtheme 2: Home Resource Accessibility Concerns
Most post-PEG patients were discharged back to their local hospitals for treatment or convalescence at home. Differences in geographic accessibility of medical supplies and nutritional preparations raised anxiety.
F4: We first asked our family members to prepare in advance according to the same preparations used here in the hospital, including how to place those pieces of equipment and how to use them, for all our family members to try. We also asked the nurses to come to our home to help us look and see what we need to do and to be all prepared before we dare to bring him home.
F9: I don’t know if our local hospital will handle this wound and some of the materials that are used here, such as the food injector. We have to buy it in advance because this is often used.
F11: We opened a box of nutrient solution here to bring back. This nutrient solution is more comprehensive and does not easily cause diarrhea. This is his food; we have to always bring it in case there is no such nutrient solution at home, which would be troublesome.
Adjustment Period: Continuum of Care Needs and Multidimensional Burden
Subtheme 1: Continuity of Care Needs
Post-PEG patients are usually required to change the wound dressing and follow-up on wound healing every 2 to 3 days after the operation until the wound heals. Nutritional assessment is also required every 3 to 6 months. A portion of the respondents indicated that healthcare professionals provided limited explanation of specific information and nutritional support in follow-up visits. Respondents reported that inadequate continuity of care after discharge exacerbated the difficulties confronting caregivers.
F4: I see that the shakes all say that you have to change the tube at 3 months, and there is also something that says that you have to change that tube at 6 months. So we don’t know when we have to change it?
F6: The doctor told us to go back for a follow-up 7 days after surgery, but I don’t know which department to go back to for a follow-up and where to register. No one told us, really confusing?
F8: At home, we increased some of the meals we make for him, but recently I feel that he has lost weight again. I always feel that the absorption is not good. Before going to the hospital, the doctor said that he was too thin and needed more nutrition. We also increased the nutritional powder. I feel that his weight has not increased. We do not have a specialized dietitian here, and I do not know how to configure the nutrition for him.
Subtheme 2: Daily Care Challenges
Some respondents indicated that patients experienced postoperative complications, including issues with wound care and tube management. A common challenge was the lack of clear guidance on recognizing complication signs and determining appropriate times to seek healthcare.
The caregivers felt helpless and confused when confronting these problems and hoped to obtain professional technical guidance.
Subtheme: Wound Care Needs
Five respondents indicated that the patient had a wound infection, and two respondents indicated that the patient had a granuloma.The question of whether and how to seek professional assistance when encountering abnormal wound symptoms often left caregivers uncertain.
F1: His wounds are sometimes red; sometimes he says they are a bit itchy because it feels like there is a wound, like it’s going to dry out. I don’t know if it’s infected.Do I need to take him to the hospital right now?
F3: When cleaning or changing the dressing with iodine POV, the granuloma is exposed, but a bit of bleeding can also be seen; the tissue has been growing. We don’t know if this is normal or not, or whether we should handle it.
F5: Recently, I noticed that the wound has become slightly red and is producing some secretion. I am unsure how to get to the hospital for a check-up. I still do not feel completely reassured.
Subtheme: Duct Maintenance and Safety Needs
Most interviewees indicated that lumen cleaning and maintaining the smoothness of the pipe were the main problems encountered in pipe maintenance.A prevalent concern among caregivers was the fear of accidental tube dislodgement.
F4: The doctor told us to change the water in the bladder regularly, but I was worried every time I pumped the water out for fear that the tube would come out.
F8: The gastrostomy tube is too long; if the tube is too long, it flushes more water, especially when it is thickened. It would be better if the tube were shorter, and the top of the tube always appears black, so it is hard to flush it out.
F11: Two days ago, a bit of resistance was felt in the tube after medication, and then we went to the hospital for follow-up, and they told us that we needed to filter these medications. It got better over the past few days.
Subtheme 3: Caregiver Socioeconomic Role Reconfiguration
Most caregivers reported that long-term care placed a significant financial and emotional strain on the family. The caregivers wanted to reduce this burden and adapt changes in their own life trajectories to cope with their relative’s illness to minimize the negative impact on the family as a whole.
F8: Usually at home, I am the one who takes care of him, and the children have to go to work to earn money. That’s all the family has financially, so there’s no way I can do anything. I am around the neighborhood sometimes, but there’s no way I can go out of town.
F9: My father’s condition means we have to have someone to take care of him full-time, and we can’t leave him alone in any way.
F12: I haven’t traveled much in the past few years. When I go out, I go to the hospital, or I stay at home.
Adaptation Period: Rehabilitation Goal Adjustment and Self-Efficacy Enhancement
Subtheme 1: Conflict Between Rehabilitation Expectations and Reality
Caregivers retain hope for the recovery of the patient. Some caregivers try risky compensatory behaviors (eg, tiny amounts of tea) in the hope of relieving the patient’s discomfort, while fearing the additional risk of exacerbating the condition.
F1: It’s good that he’s in the state he’s in now; it’s hard, but maybe one day when medicine advances, there’s a chance he’ll be able to eat on his own.
F7: We usually like to drink tea and chat, but now that he can’t drink and his mouth gets dry easily, we will give him a little bit of tea to moisturize his mouth, so that he can have a good time. This way, he is also a little more comfortable, but may choke, so we are also afraid.
F8: I want to give her more, but she won’t take too much. She often has an upset stomach and has an IV. She takes a stomach medicine or something, and her digestion is not very good. I think the amount of food given is still on the low side.
Subtheme 2: Self-Efficacy Enhancement
Some caregivers gradually optimized their care practices and developed adaptive solutions through patient support and empirical innovation.
F8: Our patients will share in the group, like patients share to order Coke so that the tube can clear a little bit. This is something I learned in the group; these tips are good.
F9: The nurses have taught us that we should hit some air at the end of the meal, at the end of the shot, but his stomach gets bloated easily. We won’t be hitting the air after the shot, and then hitting the air again, and I don’t think he will be comfortable with that.
F12: I would always look at his wounds, and now I see that as soon as they are red, I disinfect them and keep them clean, and they are okay.
Discussion
This study used a longitudinal tracking design to explore the dynamic experience and evolution of the needs of caregivers supporting patients with PEG over the full care cycle. Breaking through the limitations of previous cross-sectional studies, this longitudinal design systematically revealed differentiated core challenges and needs at each stage. These findings presented the impact of traditional Chinese cultural beliefs, family-centered medical decision-making models, and structural deficiencies in social support systems on the experiences and needs of caregivers. The specific experiences and needs at each stage will help provide a theoretical basis for constructing a precise caregiving support system.
Diagnostic Period: Optimizing Information Support and Family Collaborative Decision-Making Paths
During the diagnostic period, this study found that caregivers had difficulty in making decisions about selecting PEG due to cognitive limitations, uncertainty about surgical risks, fear of accidental tube dislodgement, and concerns about bodily integrity. This is consistent with the findings of other studies, such as Jaafa et al21. Notably, physician-patient information inequality, comprehension bias, and insufficient communication time significantly hindered the access that caregivers received to critical decision-making information. For this reason, healthcare professionals need to provide visual information support (eg, animated surgical videos and health education brochures) to optimize clinical decision pathways. Unlike the Western model of individual autonomy, Chinese families prefer the traditional model of shared family decision-making.22 It is recommended that healthcare teams allow patients, families, and healthcare professionals to discuss treatment priorities, fears, and attitudinal preferences;23 use layman’s terminology to explain surgical options and prognosis, avoiding jargon, and assess caregiver perceptions in depth. This provided caregivers with a deeper context of acceptance or rejection of PEG23. Developing evidence-based decision aids (eg, benefit-risk visualization scales) and integrating patient experience sharing helped improve the timeliness and quality of decisions. Multidisciplinary teams could be established preoperatively. There is evidence that the establishment of a multidisciplinary teamwork model supported PEG decision-making.24
Stabilization: Strengthening Psychological Adaptation and Guiding a Sense of Treatment Benefit
Patients with PEG placement often experience a transition from gastrostomy/nasal tube to PEG, during which caregivers continued to confront the multiple challenges of tube care, patient postoperative pain, nausea, and other comfort needs. These challenges significantly increased the risk of anxiety and depression in caregivers, which is consistent with the findings of a prospective cohort study.25 Studies have shown that a sense of illness benefit is effective in alleviating caregivers’ negative emotions and increasing levels of psychological resilience26,while prompting caregivers to proactively seek external support and know-how. Notably, in terms of the choice of long-term enteral nutrition, research has confirmed that PEG significantly reduces caregiver anxiety compared to other methods.8 Such evidence suggested to us that PEG itself harbored potential psychological benefits for caregivers. Therefore, healthcare professionals should help caregivers develop positive caregiving beliefs and confidence. Caregivers should recognize the specific benefits of PEG for the patient and their own caregiving, such as reducing the pain of repeated tube placement, improving feeding safety and efficiency, and improving patient comfort.27 When necessary, interventions such as cognitive-behavioral therapy and nostalgia therapy could be used to systematically enhance the caregivers’ sense of benefit from the disease therapy. Subsequently, this could alleviate their anxiety and reinforce their recognition of the value of PEG therapy.
Preparation for Discharge: Strengthening Individualized Skills Training and Care Plan Development
This study found that with the accelerated implementation of the postoperative recovery concept and diagnosis-related group payments in China, post-PEG patients had short hospital stays and quick turnarounds. The training provided during hospitalization was insufficient and brief, leading to difficulties in understanding the information. There were also reports from caregivers that the training was conducted only once or verbally and that there was a lack of hands-on experience and demonstrations, which made them less confident that they would be able to follow the nurses’ instructions on returning home. This is consistent with the findings of Sezer et al.7 Therefore, skills training for caregivers should be started as early as possible, using realistic simulation props with anatomical pieces that can be used practically and repetitively for intensive training. This would promote interaction and participation between caregivers and educational interveners, improve understanding, and ease concerns.28 Specific individualized training goals and care plans should also be set according to the self-care ability of the patient, the acquired care skills of the caregiver, and the patient’s family background. Additionally, reliable resources such as health education videos, health manuals, micro-letter platforms, and other channels should be used to provide guidance on PEG knowledge and skills.
Adjustment Period: Improvement of Continuing Care and Remote Support Mechanisms
Studies have found that post-discharge caregivers often face multiple challenges, including insufficient guidance on follow-up information, difficulties with tube maintenance and safety, wound care issues, difficulties in identifying complications, and generally significant deficits in self-coping and management skills. Unlike the well-established model of transferring these patients to specialized nursing homes in developed countries29, more than 90% of PEG patients in China return directly to their homes and are cared for by their families.30 Caregivers who lack professional support are highly vulnerable to anxiety. Ang et al31 reported that homebound PEG patients and their caregivers often experience anxiety due to a lack of knowledge about self-care and insufficient information about what to expect after tube placement. The need for ongoing professional and technical guidance to deal with the complexities of enteral feeding techniques was also noted to be cross-culturally universal. Studies have shown that the implementation of a mobile application (PEG App)32 is effective in improving the self-care knowledge and skills of homebound PEG patients, as well as significantly reducing complication rates and emergency department visits. Evidence demonstrates that telemedicine coaching is a significantly cost-effective alternative, especially in systems with constrained healthcare resources. Future directions could explore integrating PEG applications into the case management workflow of hospital systems. This could cover the entire process from hospitalization to discharge and extend to the community level for seamless linkage of information across hospital platforms. At the same time, it is proposed to implement the “1+N” radiation model in urban areas with specialized nurses as the core. One stoma therapist guides multiple communities; in rural areas, the training of care coordinators for village doctors will be strengthened. Ultimately, a closed-loop management mechanism will be constructed with the themes “Intelligent Early Warning - Initial Community Assessment- Remote Diagnosis - Family-Led Implementation”. Thereby, efficiently realizing the hospital-community-family linked integrated continuity of care model.
Adaptation Period: Building a Diversified Social Support Network and Empowerment System
Caregivers, faced with the long-term difficulty of managing a patient’s disease while hoping that the patient will be comfortable and relieved, begin to reflect on their experiences and actively seek social support. A qualitative study in South Korea33 found that the family caregivers of patients with amyotrophic lateral sclerosis who received PEG faced a variety of stresses and had insufficient social support. The study showed that adoption of the Family-Centered Empowerment Model significantly reduced caregiver burden and improved caregiving skills34. Caregivers should be encouraged and guided to take the initiative in coordinating the division of labor among family members and mobilizing other relatives to participate in caregiving. This can not only distribute specific tasks but also provide emotional resonance and understanding to the caregiver, which can significantly reduce his/her sense of isolation and fatigue. Actively building and maintaining online and offline communication platforms may assist patients and caregivers. For example, we have set up exclusive WeChat groups and online forums to facilitate instant communication, answer questions and solve problems, and ventilate emotions. Regular offline activities could be organized, such as patient association meetings, care experience sharing salons, and thematic health lectures to promote face-to-face emotional connection and practical experience transfer. The government can be urged to recognize the plight of PEG caregivers and include professional care support services in the design of social security, medical insurance, and long-term care insurance systems to provide more sustainable institutional protection.
Conclusion
Guided by the TIR theoretical framework, this study provided a systematic exploration of the dynamic experiences and evolving needs of caregivers for PEG patients at different stages of illness within the Chinese cultural context. In the diagnostic phase, caregivers showed passivity in decision-making due to anxiety about surgical risks, concerns about physical integrity, and information barriers. In the stabilization phase, they focused on coping with postoperative comfort management while perceiving the benefits of PEG. In the preparation for discharge phase, they needed urgent support for the availability of resources for hands-on skills training. During the adjustment phase, they were faced with the dual pressures of continuity of care and the reconstruction of socioeconomic roles. Finally, in the adaptation phase, patients were faced with the need to improve self-efficacy through patient support and experience innovation, but still needed to cope with the conflict between the expectations of rehabilitation and reality. The differentiated experiences and needs at different stages highlighted the urgency of establishing an accurate PEG support system that fit the Chinese cultural context. In the future, we can ensure that caregivers receive the right information and support at the right time by adopting graded intervention strategies, such as decision-making aids during the diagnostic period and remote closed-loop management during the adjustment period. This would achieve the empowerment of caregivers and the optimization of healthcare resources.
Ethics Approval and Informed Consent
This study was approved by the Ethics Committee of Nanfang Hospital, Southern Medical University (NFEC-202411-K24-01). Written informed consent was obtained from all the participants.
Acknowledgments
The authors would like to thank the participants in this study for contributing their valuable opinions.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Guangdong Science and Technology plan project (2022A1414020007).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Boullata JI, Carrera AL, Harvey L, et al. ASPEN safe practices for enteral nutrition therapy [Formula: see text]. JPEN J Parenter Enteral Nutr. 2017;41(1):15–103. doi:10.1177/0148607116673053
2. Gomes CA Jr, Andriolo RB, Bennett C, et al. Percutaneous endoscopic gastrostomy versus nasogastric tube feeding for adults with swallowing disturbances. Cochrane Database Syst Rev. 2015;2015(5):CD008096. doi:10.1002/14651858.CD008096.pub4
3. Gkolfakis P, Arvanitakis M, Despott EJ, et al. Endoscopic management of enteral tubes in adult patients - Part 2: peri- and post-procedural management. European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy. 2021;53(2):178–195. doi:10.1055/a-1331-8080
4. Tae CH, Lee JY, Joo MK, et al. Clinical Practice Guideline for Percutaneous Endoscopic Gastrostomy. Gut Liver. 2024;18(1):10–26. doi:10.5009/gnl230146
5. Friginal-Ruiz AB, Lucendo AJ. Percutaneous endoscopic gastrostomy: a practical overview on its indications, placement conditions, management, and nursing care. Gastroenterol Nurs. 2015;38(5):
6. Chang WK, Lin KT, Tsai CL, Chung CH, Chien WC, Lin CS. Trends regarding percutaneous endoscopic gastrostomy: a nationwide population-based study from 1997 to 2010. Medicine. 2016;95(24):e3910. doi:10.1097/MD.0000000000003910
7. Sezer RE, Ozdemir Koken Z, Senol Celik S. Home percutaneous endoscopic gastrostomy feeding: difficulties and needs of caregivers, qualitative study. JPEN J Parenter Enteral Nutr. 2020;44(3):525–533. doi:10.1002/jpen.1612
8. Özceylan G, Findik İ. Comparison of anxiety and depression levels in caregivers of patients with percutaneous endoscopic gastrostomy for home enteral tube feeding against other enteral nutrition methods. BMC Palliative Care. 2024;23(1):20. doi:10.1186/s12904-024-01360-3
9. Rosa E, Lussignoli G, Sabbatini F, et al. Needs of caregivers of the patients with dementia. Arch Gerontol Geriatrics. 2010;51(1):54–58. doi:10.1016/j.archger.2009.07.008
10. Hei X, Feng T, Gong C. Changes in end-of-life care models among Chinese older adults, 1998–2018: an age-period-cohort analysis. BMC Geriatr. 2025;25(1):399. doi:10.1186/s12877-025-06050-0
11. Pan Y, Chen R, Yang D. The relationship between filial piety and caregiver burden among adult children: a systematic review and meta-analysis. Geriatric Nurs. 2022;43:113–123. doi:10.1016/j.gerinurse.2021.10.024
12. Huang S, Xin L, Zheng D, et al. Mediating and moderating roles of individual resilience, caring ability and social support: a cross-sectional study on the association between family resilience and caregiving burden among primary family caregivers of cancer patients in China. BMJ Open. 2025;15(3):e093043. doi:10.1136/bmjopen-2024-093043
13. Milbury K, Badr H, Fossella F, Pisters KM, Carmack CL. Longitudinal associations between caregiver burden and patient and spouse distress in couples coping with lung cancer. Support Care Cancer. 2013;21(9):2371–2379. doi:10.1007/s00520-013-1795-6
14. Bevans M, Sternberg EM. Caregiving burden, stress, and health effects among family caregivers of adult cancer patients. JAMA. 2012;307(4):398–403. doi:10.1001/jama.2012.29
15. Wang Y, Tyagi S, Hoenig H, et al. Burden of informal care in stroke survivors and its determinants: a prospective observational study in an Asian setting. BMC Public Health. 2021;21(1):1945. doi:10.1186/s12889-021-11991-3
16. Gil E, Agmon M, Hirsch A, Ziv M, Zisberg A. Dilemmas for guardians of advanced dementia patients regarding tube feeding. Age Ageing. 2018;47(1):138–143. doi:10.1093/ageing/afx161
17. Cameron JI, Gignac MAM. “Timing It Right”: a conceptual framework for addressing the support needs of family caregivers to stroke survivors from the hospital to the home. Patient Educ Couns. 2008;70(3):305–314. doi:10.1016/j.pec.2007.10.020
18. Wang M, Wang K, Xie B, et al. Understanding the needs of family caregivers of stroke patients with disabilities: a phenomenological study using the timing it right theory. PLoS One. 2025;20(6):e0325671. doi:10.1371/journal.pone.0325671
19. Lu Q, Lu J, Zheng Y, et al. The effectiveness of mindful walking based on the timing it right framework in patients with atrial fibrillation and chronic heart failure. Front Cardiovasc Med. 2025;12:1587547. doi:10.3389/fcvm.2025.1587547
20. N T, C E, H D, N D. The application and tailoring of Colaizzi’s phenomenological approach in a hospital setting. Nurse Res. 2020;28(2). doi:10.7748/nr.2020.e1700
21. Jaafar MH, Mahadeva S, Subramanian P, Tan MP. Perceptions of healthcare professionals on the usage of percutaneous endoscopic gastrostomy in a teaching hospital from a middle-income South East Asian Country. J Nutr Health Aging. 2017;21(4):473–479. doi:10.1007/s12603-016-0774-2
22. Cong Y. Doctor-family-patient relationship: the Chinese paradigm of informed consent. J Med Philos. 2004;29(2):149–178. doi:10.1076/jmep.29.2.149.31506
23. Hogden A, Labra J, Power E. Enabling decision-making: what assists people with motor neurone disease when they consider gastrostomy insertion? Disabil Rehabil. 2025;47(10):2535–2542. doi:10.1080/09638288.2024.2395473
24. Clarke G, Galbraith S, Woodward J, Holland A, Barclay S. Should they have a percutaneous endoscopic gastrostomy? the importance of assessing decision-making capacity and the central role of a multidisciplinary team. Clin Med Lond. 2014;14(3):245–249. doi:10.7861/clinmedicine.14-3-245
25. Dong J, Dai Z, Cao F, et al. Effects of PEG in patients with esophageal squamous cell carcinoma during concurrent chemoradiotherapy: a prospective study. Gastrointest Endosc. 2023;98(6):901–910.e3. doi:10.1016/j.gie.2023.04.2094
26. Ball JQ, Ray CD. Relational maintenance behaviors mediate the relationship between alzheimer’s diagnosis severity and caregivers. Benefit Finding Health Commun. 2025:1–9. doi:10.1080/10410236.2025.2503401
27. Zhang Y, Gong Z, Cai J, Yu W, Dai Y, Wang H. Incidence of dysphagia-related safety incidents in older adults across feeding methods: a systematic review and meta-analysis. j nutr health aging. 2025;29(5):100522. doi:10.1016/j.jnha.2025.100522
28. dos SJM, Pedreira LC, Góes RP, et al. Caregivers’ mastery in handling gastrostomy at home after educational intervention: qualitative descriptive study. Healthcare. 2024;12(21):2147. doi:10.3390/healthcare12212147
29. Wong A, Sowa PM, Banks MD, Bauer JD. Home enteral nutrition in singapore’s long-term care homes-incidence, prevalence, cost, and staffing. Nutrients. 2019;11(10):2492. doi:10.3390/nu11102492
30. Farrag K, Shastri YM, Beilenhoff U, Aksan A, Stein J. Percutaneous endoscopic gastrostomy (PEG): a practical approach for long term management. BMJ. 2019;364:k5311. doi:10.1136/bmj.k5311
31. Ang SY, Lim SH, Lim ML, et al. Health care professionals’ perceptions and experience of initiating different modalities for home enteral feeding. Clin Nutr ESPEN. 2019;30:67–72. doi:10.1016/j.clnesp.2019.02.005
32. Chen BL, Lien HC, Yang SS, Wu SC, Chiang HH, Lin LC. Impact of mobile apps in conjunction with percutaneous endoscopic gastrostomy on patients’ complications, quality of life, and health-related self-care behaviors: randomized clinical trial. JMIR mhealth uhealth. 2023;
33. Chu HS, Oh J. Family caregivers’ experiences of people with amyotrophic lateral sclerosis undergoing gastrostomy tube feeding. J Neurosci Nurs. 2024;56(6):224–228. doi:10.1097/JNN.0000000000000792
34. Lin X, Fei F, Zhang X, et al. Effectiveness of the family-centred empowerment model on informal caregivers of people with chronic diseases: a systematic review and meta-analysis. J Clin Nurs. doi:10.1111/jocn.70006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Challenges in Accessing Community-Based Rehabilitation and Long-Term Care for Older Adult Stroke Survivors and Their Caregivers: A Qualitative Study
Zeng S, Wu M, Xu L, Guo Z, Chen S, Ling K, Li H, Yu X, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:4829-4838
Published Date: 23 October 2024
A Qualitative Investigation into the Determinants of Unfulfilled Needs in Caregivers of Patients with Phenylketonuria
Zheng YJ, Hou YC, Zhao H, Wang XY, Liu YD, Li L, Yu L, Guo MM
Patient Preference and Adherence 2024, 18:2249-2259
Published Date: 8 November 2024
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Multiple Myeloma Experiences and Preferences: A Mixed Methods Study of Patients and Care Partners in the United States
Flora DR, Byrd R, Platt DA, Hlavacek P, Hoag Goldman E, Cappelleri JC, Kennedy CT, LeBlanc TW
Patient Preference and Adherence 2025, 19:963-979
Published Date: 8 April 2025
Barriers and Facilitators in Proxy Decision-Making for Financial Support in Adolescent Idiopathic Scoliosis: A Qualitative Study of Family Caregivers Using the COM-B Model
Liu S, Hu K, Rui H, Gao Y, Zhan X
Patient Preference and Adherence 2025, 19:3001-3011
Published Date: 25 September 2025