Back to Journals » Patient Preference and Adherence » Volume 19
Barriers and Facilitators in Proxy Decision-Making for Financial Support in Adolescent Idiopathic Scoliosis: A Qualitative Study of Family Caregivers Using the COM-B Model
Authors Liu S, Hu K ![]() , Rui H, Gao Y, Zhan X
, Rui H, Gao Y, Zhan X
Received 26 May 2025
Accepted for publication 19 September 2025
Published 25 September 2025 Volume 2025:19 Pages 3001—3011
DOI https://doi.org/10.2147/PPA.S538568
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Sihui Liu,1 Kaili Hu,2 Huazhen Rui,2 Yi Gao,3 Xue Zhan2
1Department of Research, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Department of Nursing, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 3Department of Thoracic, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
Correspondence: Xue Zhan, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, No. 1095 Jiefang Avenue, Hankou, Wuhan, 430030, People’s Republic of China, Email [email protected]
Purpose: This study aimed to explore the barriers and facilitators faced by family caregivers in proxy decision-Making for financial support in patients with adolescent idiopathic scoliosis (AIS).
Patients and Methods: This qualitative study utilized the Capability, Opportunity, Motivation-Behavior (COM-B) model to examine the factors that influence family caregivers’ proxy decision-Making regarding financial support for patients with AIS. Eighteen caregivers were interviewed using semi-structured interviews. The data were analyzed using MAXQDA software and Braun and Clarke’s thematic analysis.
Results: The key facilitators identified included financial relief, trust in the legitimacy and reputation of charitable organizations, and family and social support. Barriers included lack of knowledge and practical skills, emotional and physical exhaustion, privacy concerns, particularly related to the patient’s future educational opportunities, and the complexity of application procedures.
Conclusion: This study underscores the importance of addressing the barriers caregivers face, such as complex application processes and emotional stress, while enhancing facilitators like financial support and trust in organizations. Streamlining application procedures and improving transparency can enhance caregivers’ ability to access financial resources, benefiting both patients and their families.
Keywords: adolescent idiopathic scoliosis, caregivers, proxy decision-making, COM-B model, qualitative research
Introduction
Adolescent idiopathic scoliosis (AIS), a three-dimensional spinal deformity affecting 2% of adolescents in Asia, is defined by a coronal curvature greater than 10° accompanied by vertebral rotation.1–3 Severe cases (Cobb angle ≥40°) can lead to back pain, respiratory difficulties, and significant psychological and social challenges, including body image issues, emotional distress, and even suicidal tendencies.3 These multisystem effects not only diminish quality of life of patients, but also impose a heavy financial burden on families - especially when surgical treatment is required and the cost of the surgery is high.4,5
For families, the caregiving burden is further exacerbated by significant financial pressures. Previous studies have shown that more than 90% of children with AIS rely on family support for both financial and psychological assistance as well as daily activities, and caregivers frequently report moderate-to-severe emotional and physical stress,especially those without co-caregivers, and from low-income families.6,7 In addition, many families face financial difficulties and restricted access to healthcare services.8 Thus, it is essential to provide these families with professional information, policy support, and affordable, effective care services.9
To support families facing financial difficulties, the Zhishan Public Welfare Foundation launched the “China Dream – Backbone Project”,with the slogan “Stand tall, and let your dreams soar”, aiming to help children with AIS improve their posture and regain their health. Established in October 2012 and directly administered by the Ministry of Civil Affairs, the foundation is a nationally recognized charitable organization. The project employs a collaborative funding model that provides tailored assistance through multiple channels, including patient contributions, insurance reimbursement, and foundation donations. However, numerous critical challenges remain. Although caregivers play a critical role in financial proxy decision-Making processes, there is a lack of empirical research exploring the factors that enable or hinder their proxy decision-Making. Understanding these barriers and facilitators is essential to designing effective support systems that alleviate financial stress and enhance caregivers’ ability to make informed decisions.
To address this gap, we apply the COM-B model (Capability, Opportunity, Motivation–Behavior),10 proposed by Susan Michie in 2011, to analyze the factors and potential mechanisms of action that influence target behaviors, encompassing factors related to environmental, organizational, social, and cultural contexts, as well as policy and legal frameworks.10 The research findings were integrated into the COM-B model, which posits that individual behaviors are shaped by three core domains: capability (psychological or physical), opportunity (social or physical), and motivation (reflective or automatic).11 To date, a number of empirical studies have used COM-B in order to develop behavior change interventions in different contexts,12,13 but to our knowledge this has not yet been done for funding support in scoliosis population.
Utilizing a qualitative interview method, this study employed in-depth interviews to explore the barriers and facilitators faced by family caregivers of patients with AIS when seeking financial assistance through proxy decision-Making, using the COM-B model as a theoretical framework. By integrating the family perspective, the study aimed to uncover the complex interplay among psychological, social, and economic factors that shape caregivers’ proxy decision-Making processes. The findings are expected to offer empirical insights for developing targeted interventions and policies, thereby reducing caregiver burden and improving comprehensive support for families affected by AIS.
Materials and Methods
Design
This was a qualitative descriptive study that employed semi-structured interviews during the data collection phase. The face-to-face interview was chosen to capture the verbal and non-verbal responses of the participants. Since most patients with AIS primarily undergo surgery during the summer and winter vacations, all interviews were conducted in July-August 2024 and December 2024-January 2025. Findings are reported in accordance with COREQ guidelines.14
Participants and Setting
The first spinal deformity rescue center in Central China, which annually treats over 150 patients with AIS and actively engages in the “China Dream·Spinal Column Project” while consistently collaborating with charitable foundations, was selected for this study. The term “family members” in this study refers to close biological or emotional relations such as parents, spouses, adult children, siblings or close friends.15 Family members were considered eligible if they met the following criteria: (1) they were primarily responsible for applying for financial assistance or making proxy decisions to decline such applications, and the outcome of the patient’s financial assistance application had already been communicated. (2) they had the ability to speak and understand Chinese and (3) they were 18 years or older. Exclusion criteria: individuals with severe mental disabilities or significant verbal communication disorders. This study employed purposive sampling with the principle of maximum variation to select participants based on significant differences in age and education level for diverse representation.
Data Collection
Based on a literature review and expert consultation, we developed an initial interview guide. Following revisions informed by the findings of a pre-interview with two caregivers, we finalized a structured interview framework. The framework aligns with the three core components of the COM-B model. A topic guide was used during the interviews, developed in collaboration with an experienced qualitative researcher. The key questions asked included:
a) As a caregiver making decisions on behalf of the patient, how do you view the welfare fund? Please share your overall thoughts and feelings about its role in supporting patients with AIS.
b) As a proxy decision-maker for the patient, what were the key factors or motivations that influenced your decision to apply for or not apply for this financial support?
c) From your perspective as a caregiver making decisions on behalf of the patient, could you detail your experiences with the application process (or the decision not to apply)? What challenges did you face?
Interviews were conducted face-to-face in a private room within a hospital ward, based on participants’ preferences, with efforts made to ensure a quiet and undisturbed environment. All interviews were carried out by a single researcher, who was a nurse at the teaching hospital involved in the study and had no direct involvement in the care of the participants. Prior to each interview, demographic data were collected from both participants and their associated patients to provide contextual background for the research findings.
Following Francis’s recommendation,16 interviews continued until 15 participants had been interviewed, at which point no new themes emerged from the data. To further confirm data saturation, three additional interviews were conducted, bringing the total number of interviews to 18. Each interview lasted between 12 and 43 minutes. All interviews were audio-recorded and transcribed verbatim within 24 hours. After each session, the researcher completed a memo and a reflective diary entry to enhance the quality and depth of subsequent interviews.
Data Rigor
To ensure the data trustworthiness, the researchers used Guba and Lincoln’s criteria,17 which included credibility, transferability, dependability, and confirmability. Credibility was enhanced through prolonged engagement, allowing sufficient time for data collection and analysis to achieve a deeper and more accurate understanding of the data. Transferability was ensured by employing maximum variation sampling and purposive sampling, which included participants with diverse characteristics such as gender, age, socioeconomic status, and various application outcomes. Dependability was ensured through an audit trail, which provided detailed documentation of the study process. This approach ensured transparency and enabled readers to follow the methodology. Confirmability was strengthened by selecting excerpts from interviews, codes, and categories for review by two external experts in qualitative research analysis. These reviewers assessed the accuracy of data coding and provided feedback. Necessary revisions were made based on their suggestions, and the process continued until they validated the rigor and accuracy of the analysis.
Data Analysis
MAXQDA 2020 software was used to manage and analyze the data. Braun and Clarke’s six-step reflexive thematic analysis was employed to analyze the data. The approach involves (1) familiarization with the data through transcription and repeated reading, (2) generating initial codes, (3) searching for themes, (4) reviewing themes, (5) defining themes, and (6) writing the results, including using illustrative extracts.18 Following this process, key themes were collaboratively identified, clearly defined, and hierarchically organized. These themes were systematically mapped onto the COM-B model, a framework consisting of three components—capability, opportunity, and motivation—that examines behavior change. Each theme was analyzed through the lens of the COM-B model, identifying its relevance to one or more components.
Ethical Considerations
Written approval (with the code of TJ-IRB 202411080) was obtained from Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology. Informed consent was also acquired from all participants. The study was conducted in accordance with the Declaration of Helsinki. Prior to the interviews, demographic data and signed consent forms were collected from participants. Participant identification numbers were used to ensure the confidentiality of the data.
Results
Characteristics of Participants
A total of 18 parents of patients with AIS with scoliosis were interviewed. The participants’ sociodemographic characteristics are summarized in Table 1. Participants’ ages ranged from 36 to 55 years, with 7 males and 11 females. Educational backgrounds varied from primary school to a bachelor’s degree. Marital status included 16 married, 1 divorced, and 1 widowed individual. Monthly household income ranged from 2,000 to 200,000 RMB, demonstrating significant variation among participants. Regarding application outcomes, 6 cases successfully received funding, 7 did not submit an application, and 5 had their applications denied.
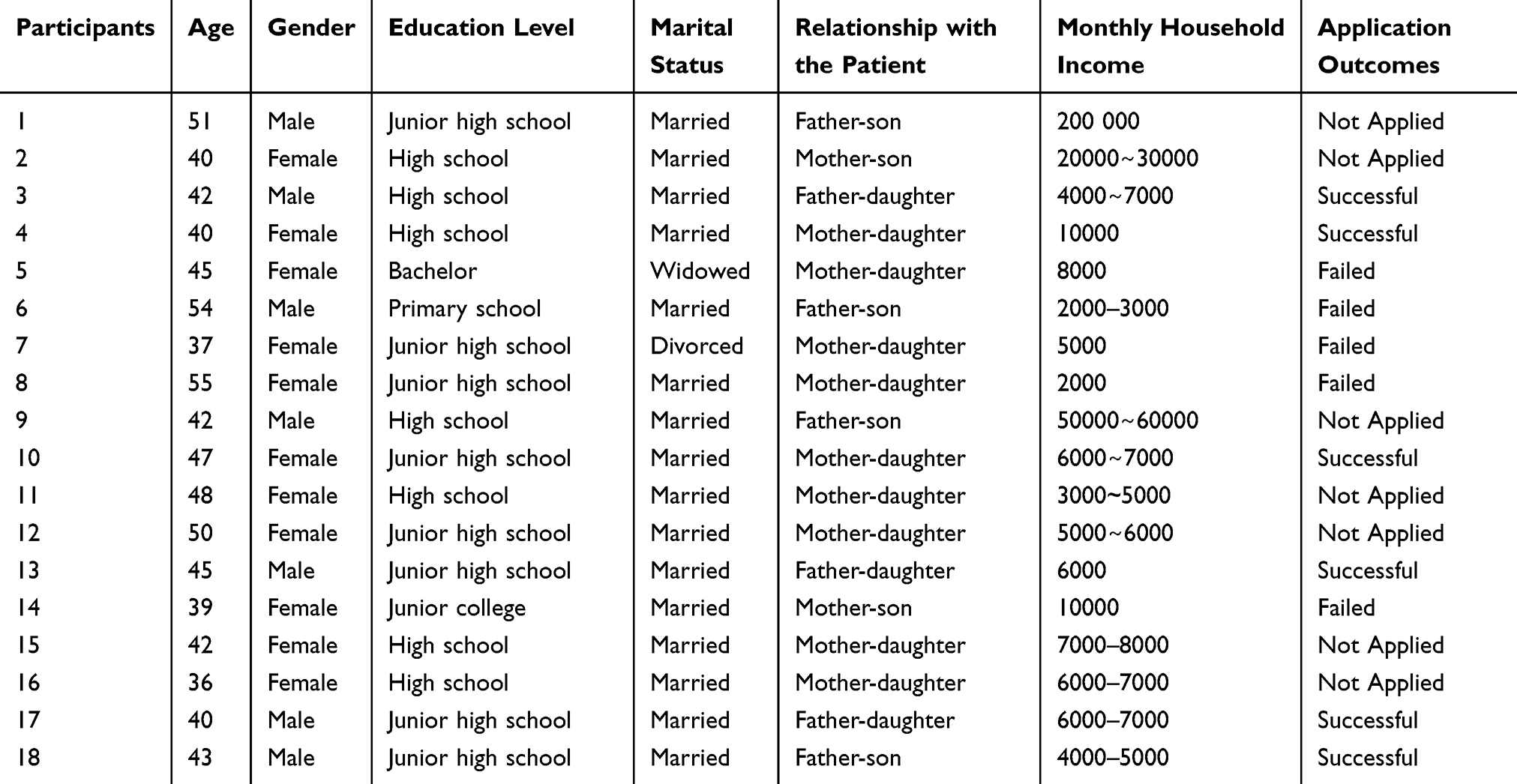 |
Table 1 Characteristic of Participants |
Factors Influencing Proxy Decision-Making Among Participants
Table 2 presents the results of applying the COM-B model to identify factors influencing proxy decision-making among family caregivers of patients with AIS. These factors are organized according to the three core components of the COM-B model: Capability, Opportunity, and Motivation, each of which encompasses specific themes derived from the interview data.
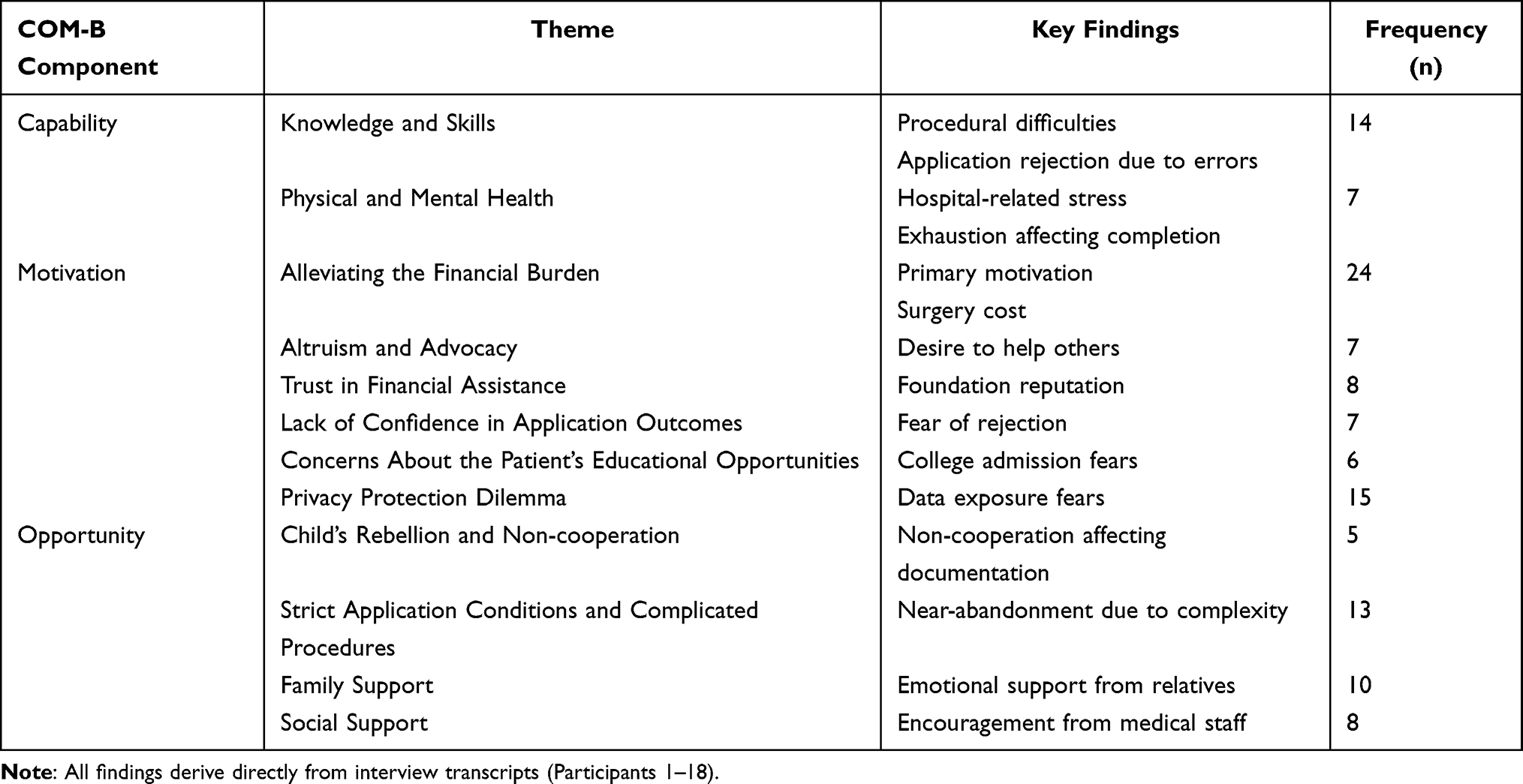 |
Table 2 Factors Influencing Proxy Decision-Making Among Family Caregivers of Patients with AIS (n=18) |
Capability
Knowledge and Skills
The lack of knowledge and practical skills emerged as a barrier for caregivers when navigating the fund application process. Participants described feeling unprepared to manage the technical and procedural requirements, often resulting in frustration and errors. Their accounts illustrate how unfamiliarity with the system and lack of guidance can hinder their ability to successfully complete applications.
I don’t know how to operate it at all, not even a bit. What am I supposed to do with this? (Participant 13, 14)
Taking photos, handling those procedures—there are so many things I don’t know how to do. (Participant 4)
Because I was unfamiliar with the process at first, I made some mistakes, and my application was rejected. (Participant 7)
Physical and Mental Health
Physical and mental health challenges were common themes among participants, who described the significant strain they faced while caring for patients with AIS, whether as caregivers or as patients themselves. The emotional toll of fear, stress, and exhaustion, combined with the physical demands of the situation, left many feeling overwhelmed and unable to focus on other responsibilities. The hospital environment further intensified these challenges, adding to the sense of pressure and distress.
I find it inconvenient to take care of my child alone. I’m a single parent, so everything depends on me. This has left me feeling both mentally and physically exhausted—though it’s mainly the mental fatigue. (Participant 7)
I was very scared at the time, and my child was also very scared. (Participant 5)
The hospital environment is definitely quite oppressive. Whether it’s her or me, we both felt a lot of inner turmoil and distress. (Participant 4)
At that time, my child was sick, and I just didn’t have the energy to handle anything. (Participant 11)
Motivation
Alleviating the Financial Burden
Financial assistance opportunities provided a critical means for families to cope with the overwhelming burden of medical expenses. For many participants, such support represented not just a reduction in financial strain but also a pathway to overcome systemic barriers to accessing necessary medical care.
Especially for a family like mine, where I’m raising a child on my own, and I also have to support my parents—both of whom are farmers with no income—it’s really tough. So, if there could be some support provided, I think it would help reduce some of my stress. (Participant 11)
The main thing is to relieve the financial pressure. We don’t have money to begin with. (Participant 17)
The real reason was that the surgery cost was too expensive, and it was a huge financial burden on the family. I couldn’t afford the surgery fee, which was over 80,000 yuan. I only paid less than 20,000 yuan myself, and the rest I borrowed from relatives and friends. (Participant 10)
Altruism and Advocacy
The opportunity to access charitable resources not only addressed participants’ immediate needs but also inspired a sense of altruism and advocacy. Many participants viewed the fund as a platform for amplifying awareness, fostering solidarity, and encouraging others to seek similar support. The desire to ensure that others in similar situations could access resources and benefit from the foundation’s support emerged as a motivating factor for their participation. These reflections underscore the broader impact of fund initiatives, extending beyond individual families to fostering a culture of mutual support and advocacy.
I hope the application will be approved, so that I can pass this on and let others know, so they can also benefit from the support of charity foundation. (Participant 13)
I hope this fund can grow larger and better, and that in the future, children facing similar difficulties will receive more help. (Participant 10)
Whether I receive help or not, the fact that it exists means it will definitely help those who need it. I think that in itself is already a great thing. (Participant 5)
Trust in Financial Assistance
The charity foundation’s established reputation and legitimacy fostered trust, which played a critical role in participants’ decision to apply. This trust alleviated hesitations and encouraged engagement with the application process. Participants emphasized the foundation’s long-standing reputation and commitment to helping those in need as key factors that alleviated their concerns and encouraged them to engage with the process. For many, confidence in the legitimacy and transparency of the organization was essential, particularly when navigating the complexities of financial assistance.
I believe this foundation has been around for so many years and has helped so many patients. Moreover, it is a legitimate organization. (Participant 4)
I trust the charity foundation. The foundation is dedicated to doing good and helping people in need. (Participant 13)
After searching and learning more online, we looked at its information and felt that this is definitely a good cause, and it can help more people. That’s basically how we think about it. (Participant 3)
I wasn’t worried, not at all. I believe in it. (Participant 3)
Lack of Confidence in Application Outcomes
While financial assistance presented a valuable opportunity, participants’ lack of confidence in the application process often hindered their ability to fully leverage this resource. Doubts about eligibility, perceived complexity, and fears of rejection were key barriers that undermined their engagement. Many caregivers expressed doubts about their eligibility and feared rejection, which discouraged them from applying. The perceived complexity of the requirements and uncertainty about the outcome contributed to their reluctance to invest time and effort into the process.
I looked at the brochure and saw the requirements for family conditions. I felt like we might not qualify, so I didn’t apply, afraid that our application would be rejected. (Participant 2)
Even if I applied, it wouldn’t necessarily be approved, and I would have put in a lot of effort. (Participant 6)
I was afraid that after applying, my application would be rejected, thinking that I might not meet their requirements. (Participant 6)
I don’t know if the application will be successful, I’m not sure about this issue. (Participant 1)
Concerns About Patients’ Educational Opportunities and Privacy Protection Dilemma
The requirement to disclose sensitive information in funding applications caused significant concern among participants. Families faced overlapping worries about privacy risks and the potential long-term effects on their child’s education and social development. Although financial aid could reduce immediate medical costs, many hesitated to fully participate due to two interconnected issues. First, caregivers feared that applying for support might harm their children’s future educational and social prospects. While economic assistance helps with short-term medical expenses, concerns about stigma or academic restrictions often discouraged full participation. Many believed that revealing personal details during the application process could negatively affect their children’s future opportunities. These fears reflect deeper anxieties about facing discrimination or institutional barriers due to program involvement. Together, these factors highlight how privacy concerns and life planning influence caregivers’ willingness to apply for funding. Second, privacy protection was a major concern. Sharing sensitive data during the application created a dilemma. Some acknowledged the need to provide accurate health information, but others worried about privacy breaches and their long-term consequences. These fears were often linked to concerns about public exposure, digital data transparency, and the impact on their child’s future. These dual concerns — about both long-term development and privacy — demonstrate the intersection of immediate data security issues and broader life-planning considerations, ultimately shaping families’ willingness to engage in funding applications.
My concern is that it will affect my child’s future life, especially when it comes to choosing a major after high school graduation. (Participant 1)
Because the child is still young, we’re worried that it might affect their education or future integration into society, so we didn’t apply. (Participant 2)
I’m afraid that if we participate, my child’s information will be exposed, and it could affect her future when applying for college. You know, some majors have certain requirements. (Participant 15)
I can understand the collection of personal information, but we are still very concerned about uploading it to the website. (Participant 15)
At first, I was worried about this because, after all, its privacy, and no one wants their personal information to be known by others. (Participant 3)
I think it’s quite normal because this information must accurately reflect her condition and health status. When it comes to illness, privacy can’t be a priority. I think this is reasonable. (Participant 5)
Privacy, well, with big data nowadays, everything is transparent. (Participant 9)
I’m worried that in the future, my child might see their information on the foundation’s website, and I don’t want to disclose their information. (Participant 16)
Opportunity
Child’s Rebellion and Non-Cooperation
For adolescents with scoliosis, their heightened sensitivity about physical appearance and a growing sense of autonomy often lead to challenges in proxy decision-Making. In the context of applying for financial support, a child’s refusal to cooperate—stemming from embarrassment, shyness, or rebellion—can create significant barriers. This non-cooperation not only hinders procedural steps, such as taking required medical photographs, but also adds an emotional burden to caregivers who are already navigating complex application processes.
At the time, my child was upset and didn’t want to take the photos because she was shy. She was around twelve or thirteen, at that sensitive age, and she felt embarrassed about taking photos without a top, so she refused to do it. (Participant 5)
My child is around thirteen or fourteen, which is the rebellious age. My feeling is that she doesn’t listen and is very unwilling to cooperate. (Participant 3)
My child is in their adolescence and is not very obedient. (Participant 6)
Strict Application Conditions and Complicated Procedures
The strict requirements and complex processes associated with fund applications often posed significant challenges for caregivers of patients with AIS. These hurdles, including the need for precise documentation and adherence to tight timelines, frequently amplified the stress experienced by families already navigating the emotional and logistical burdens of managing their loved one’s condition. For many, the combination of rigid criteria and procedural delays not only complicated the application but also created tension between prioritizing immediate medical needs and fulfilling the fund’s requirements. Such challenges highlight systemic barriers that can deter families from accessing financial assistance, ultimately influencing their willingness to engage with the process.
The procedures for the public welfare fund were quite complicated, and the amount of funding wasn’t very much, but we are still very grateful. At that time, all our energy was focused on the child, who was also in the rebellious phase. She didn’t want to have the surgery at first, and with the application process being so complicated, we almost gave up. (Participant 17)
We felt the process was quite complicated, and the application was difficult. Moreover, time was very tight. After being admitted to the hospital, we had to undergo various checks and prepare for the surgery. Each step required us to handle everything ourselves, and with such limited time, we didn’t have time to apply. (Participant 15)
If there were some minor deviations, it would be helpful to correct them in time. I think the requirements for the photos were too strict because, in the application process, if you have to resubmit, it could delay things. But when the child undergoes surgery, time doesn’t wait. Once the surgery is done, you can’t take the photos again—it’s irreversible. (Participant 5)
Family Support
Family support played a pivotal role in motivating caregivers to navigate the complexities of the fund application process. In the face of overwhelming challenges, both emotional and practical, the encouragement from relatives, friends, and colleagues provided a crucial sense of reassurance. For many participants, knowing that they were not alone in their struggles, and receiving advice and support from loved ones, helped them to persist in seeking financial assistance. This emotional backing not only offered comfort during difficult times but also acted as a motivating factor to move forward with the application, despite the uncertainties and complexities involved.
Relatives and friends would call us and say not to worry too much. they reassured us, saying, ‘You’re at such a reputable hospital, right?’ They tried to comfort us. (Participant 2)
Colleagues heard about the situation at home, and they, along with family members, were very supportive and helpful. (Participant 4)
Relatives and friends have all been comforting us, telling us to stay positive because of the child’s illness. (Participant 9)
Social Support
Social support, encompassing both emotional and practical encouragement, significantly influenced participants’ proxy decision-Making process regarding fund applications. The care and empathy provided by healthcare professionals, fellow patients, and even strangers were crucial motivators during the challenging journey of managing a scoliosis diagnosis. For many participants, the shared experiences and kindness of others acted as a source of strength, reinforcing their determination to seek financial assistance through the charity foundation.
On a mental level, the professor and his team have given us a lot of support. (Participant 16)
During our search for medical treatment, we encountered many kind-hearted people, including other patients. Since we went to Wuhan, there were people from Hubei Province and other provinces. We all helped each other and shared our situations. (Participant 7)
The doctors really prioritized the child’s health, and we definitely received some encouragement. (Participant 8)
Discussion
For caregivers of patients with AIS, proxy decision-Making regarding access to financial support is shaped by a complex interplay of multiple barriers and facilitators. This dynamic process can be systematically examined through the COM-B model. From the capability dimension perspective, caregivers encounter dual challenges: limited procedural knowledge and emotional exhaustion. At the motivational level, uncertainties about eligibility criteria and privacy concerns, particularly fears that disclosure may negatively impact the adolescent’s educational prospects, represent significant deterrents. On the opportunity dimension, obstacles are evident in the complexity of application procedures and adolescents’ reluctance to cooperate. In contrast, tangible relief provided by financial assistance, trust in charitable organizations, and robust family or social support systems have been shown to significantly enhance caregivers’ willingness to engage with support programs.
This study identifies key factors affecting proxy decision-making for financial support in family caregivers of patients with AIS. First, the “privacy-education dilemma” functions as a distinct cultural barrier. In China’s competitive, exam-driven environment, social labels or data exposure may be seen as harmful—especially for rural families who view higher education as key to upward mobility.19 The pressure within the education system intensifies caregivers’ fears that applying for financial aid could damage adolescents’ academic and social prospects. As one participant said, “We are worried this will affect their studies or future integration into society.” This concern goes beyond privacy and highlights Chinese families’ heightened sensitivity to health-related stigma. Second, adolescent autonomy plays a pivotal role in proxy decision-Making. Contrary to traditional pediatric models that emphasize parental authority, this study reveals that teenagers’ body image concerns and growing sense of self-determination often lead to non-cooperation, directly impeding the application process. For instance, one caregiver reported, “She was embarrassed and refused to take the undressed photo”, underscoring the need for funding programs to explicitly consider adolescent perspectives. Third, altruistic motivations serve as a powerful facilitator. Many caregivers perceive participation as contributing to broader social welfare.20,21 As one participant articulated, “This fund can help more children”, suggesting that framing the scholarship program as a community-building initiative, rather than a purely transactional process, can significantly enhance participation. Furthermore, established organizations with strong reputations are more likely to foster trust and motivate participation.22
Based on these findings, a set of targeted intervention strategies and policies can be developed to effectively address barriers across all dimensions. Evidence suggests that assistance programs characterized by streamlined application procedures, clear communication, and broad outreach are more likely to achieve success.23 At the capability level, healthcare settings can reduce the cognitive burden on nursing staff by implementing streamlined application procedures and deploying on-site coordinators to assist with documentation. At the motivation level, charitable organizations should sign the privacy protection agreements and adopt anonymized application systems that replace personal data with unique identifiers when processing sensitive materials (eg, spinal imaging), thereby alleviating privacy concerns and minimizing potential negative impacts on adolescents’ educational prospects.24 At the opportunity level, age-appropriate informational materials should be developed to clearly communicate the purpose of required documentation, thereby reducing adolescent non-cooperation and promoting active participation through well-designed incentive mechanisms. At the same time, establishing a transparent platform that publicly displays anonymous cases of assistance and clearly defined eligibility criteria can enhance nursing staff’s trust in the project. Furthermore, family and social support are crucial in helping caregivers make financial decisions for patients with AIS by offering emotional relief and shared responsibility, which boosts caregiver confidence and improves patient outcomes. This support enables caregivers to handle complex challenges and access essential resources more effectively.25
These findings and recommendations are not only applicable to the AIS field but also generalizable to other contexts involving chronic childhood diseases. In such contexts, economic stigma and complex treatment procedures frequently create comparable barriers.26,27 The multidimensional intervention framework proposed in this study offers empirical support for developing a more equitable and efficient family economic assistance system. For instance, in the treatment and management of children with hearing loss, providing subsidized services to alleviate economic burdens on families and streamlining diagnostic and treatment procedures to improve service accessibility can effectively support policymakers and practitioners in addressing the real-world needs of families affected by chronic pediatric conditions.
This study has several key limitations. First, the small sample size of 18 caregivers and the lack of diversity in the sample limit the generalizability of the findings across different socioeconomic, cultural, and regional backgrounds. Future research should include a larger and more diverse sample to enhance the external validity of the results. Second, while the qualitative approach provided valuable insights into caregivers’ experiences, it did not include quantitative data to assess the specific impact of various factors on the proxy decision-Making process. Future studies that combine qualitative and quantitative methods could offer a more comprehensive understanding of the factors influencing financial proxy decision-Making. Finally, this study focused only on the perspectives of caregivers, omitting the viewpoints of healthcare professionals, social workers, and other key stakeholders involved in the proxy decision-Making process. Since financial decisions often involve multiple parties, future research should incorporate a wider range of perspectives to fully understand the factors that shape these decisions.
Conclusion
Using the COM-B model, this study systematically identify key barriers (limited knowledge, emotional exhaustion, privacy-education dilemma, complex procedures) and facilitators (financial relief, institutional trust, social support) influencing caregivers’ financial proxy decision-Making for patients with AIS. The findings highlight culturally specific dynamics and the role of altruistic motivation, offering a foundation for designing targeted interventions. Furthermore, these insights provide actionable guidance for developing family-centered support systems across diverse healthcare settings, enabling caregivers to better navigate common challenges in accessing financial aid. The study also establishes a robust framework for understanding caregiver proxy decision-Making, which holds potential applicability for research on other chronic childhood conditions.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Research ethics approval (code: TJ-IRB 202411080) was obtained from Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology. All participants provided informed consent.
Acknowledgments
The authors would like to express their sincere gratitude to the participants who facilitated this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82003049), the Research Project of the Health Commission of Hubei Province (WJ2023M019), and the Tongji Hospital Nursing Special Research Foundation (2023D07).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhang X, Dai X, Chen Y, Yang H. Adolescent idiopathic scoliosis: a case report and review of experiences. Asian J Surg. 2024;47(10):4548–4549. doi:10.1016/j.asjsur.2024.07.256
2. Grauers A, Einarsdottir E, Gerdhem P. Genetics and pathogenesis of idiopathic scoliosis. Scoliosis Spinal Disord. 2016;11:45. doi:10.1186/s13013-016-0105-8
3. Kuznia AL, Hernandez AK, Lee LU. Adolescent idiopathic scoliosis: common questions and answers. Am Fam Physician. 2020;101(1):19–23.
4. Fu X, Meng S, Huang X, Li W, Ye B, Chen S. The prevalence of scoliosis among adolescents in China: a systematic review and meta-analysis. J Orthop Surg Res. 2024;19(1):585. doi:10.1186/s13018-024-05077-0
5. Malik AT, Yu E, Kim J, Khan SN. Understanding costs in a 90-day episode of care following posterior spinal fusions for adolescent idiopathic scoliosis. World Neurosurg. 2019;130:e535–e541. doi:10.1016/j.wneu.2019.06.149
6. Huang Y, Liu F, Gao D, Wang H. Family Functioning Affected by Adolescent Idiopathic Scoliosis in China: a Cross-Sectional Study. Front Pediatr. 2022;10:880360. doi:10.3389/fped.2022.880360
7. Motyer G, Dooley B, Kiely P, Fitzgerald A. Parents’ information needs, treatment concerns, and psychological well-being when their child is diagnosed with adolescent idiopathic scoliosis: a systematic review. Patient Educ Couns. 2021;104(6):1347–1355. doi:10.1016/j.pec.2020.11.023
8. Wang Y, Huang Z, Kong F. Parenting stress and life satisfaction in mothers of children with cerebral palsy: the mediating effect of social support. J Health Psychol. 2020;25(3):416–425. doi:10.1177/1359105317739100
9. Dai Q, Peng M, Li C, et al. The factors associated with the caregiving burden among family caregivers of pediatric patients with fractures: a descriptive cross-sectional study. J Pediatric Nurs. 2024;79:126–132. doi:10.1016/j.pedn.2024.08.009
10. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
11. Reid H, Smith R, Williamson W, et al. Use of the behaviour change wheel to improve everyday person-centred conversations on physical activity across healthcare. BMC Public Health. 2022;22(1):1784. doi:10.1186/s12889-022-14178-6
12. Yang Y, Gao Y, An R, Wan Q. Barriers and facilitators to exercise adherence in community-dwelling older adults: a mixed-methods systematic review using the COM-B model and Theoretical Domains Framework. Int J Nurs Stud. 2024;157:104808. doi:10.1016/j.ijnurstu.2024.104808
13. Guo S, Liu D, Bi X, et al. Barriers and facilitators to self-management among women with gestational diabetes: a systematic review using the COM-B model. Midwifery. 2024;138:104141. doi:10.1016/j.midw.2024.104141
14. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
15. Omole FS, Sow CM, Fresh E, Babalola D, Strothers H. Interacting with patients’ family members during the office visit. Am Fam Physician. 2011;84(7):780–784.
16. Francis JJ, Johnston M, Robertson C, et al. What is an adequate sample size? Operationalising data saturation for theory-based interview studies. Psychol Health. 2010;25(10):1229–1245. doi:10.1080/08870440903194015
17. Lincoln Y, Guba E. Naturalistic Inquiry. Newbury Park: Sage; 1985.
18. Braun V, Clarke V. Novel insights into patients’ life-worlds: the value of qualitative research. Lancet Psychiatry. 2019;6(9):720–721. doi:10.1016/S2215-0366(19)30296-2
19. Guo C, Guo M, Fang C, Hao X. College major decision making behavior of urban and rural students under cultural capital impact in China. Sci Rep. 2025;15(1):913. doi:10.1038/s41598-024-80664-z
20. de Waal FBM, Preston SD. Mammalian empathy: behavioural manifestations and neural basis. Nat Rev Neurosci. 2017;18(8):498–509. doi:10.1038/nrn.2017.72
21. Vickers BD, Seidler RD, Stansfield RB, Weissman DH, Preston SD. Altruistic responses to the most vulnerable involve sensorimotor processes. Front Psychiatry. 2023;14:1140986. doi:10.3389/fpsyt.2023.1140986
22. Goodman C, Flanigan A, Probst JC, Bai G. Comparison of US hospital charity care policies before vs after onset of the COVID-19 pandemic. JAMA Netw Open. 2022;5(9):e2233629. doi:10.1001/jamanetworkopen.2022.33629
23. Davidson JC. Improving the financial aid process for community college students: a literature review of FAFSA simplification, information, and verification. Commun Coll J Res Pract. 2015;39(5):397–408. doi:10.1080/10668926.2013.820157
24. Peng S, Hawk ST, Wang Y. Perceptions of parental privacy invasion and information management among Chinese adolescents: comparing between- and within-family associations. J Youth Adolesc. 2023;52(6):1287–1300. doi:10.1007/s10964-023-01771-0
25. Hu H, Hu X, Xu Y. Caring load and family caregivers’ burden in China: the mediating effects of social support and social exclusion. Front Public Health. 2023;11:1194774. doi:10.3389/fpubh.2023.1194774
26. Zussino J, Zupan B, Preston R. The barriers are plentiful. Speech-language pathologists’ perspectives of enablers and barriers to hearing assessment for children in metropolitan, regional, and rural Australia: a mixed methods study. Int J Speech-Language Pathol. 2023;26(2):289–300.
27. Rivard M, Morin M, Rochefort C, Morin D, Mello C. Barriers and facilitators to accessibility, continuity, validity, flexibility, and provider-family relationship along the diagnostic pathway in developmental disabilities. Res Dev Disabil. 2023;139:104570. doi:10.1016/j.ridd.2023.104570
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Challenges in Accessing Community-Based Rehabilitation and Long-Term Care for Older Adult Stroke Survivors and Their Caregivers: A Qualitative Study
Zeng S, Wu M, Xu L, Guo Z, Chen S, Ling K, Li H, Yu X, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:4829-4838
Published Date: 23 October 2024
A Qualitative Investigation into the Determinants of Unfulfilled Needs in Caregivers of Patients with Phenylketonuria
Zheng YJ, Hou YC, Zhao H, Wang XY, Liu YD, Li L, Yu L, Guo MM
Patient Preference and Adherence 2024, 18:2249-2259
Published Date: 8 November 2024
Perspectives of People with Type 2 Diabetes Mellitus Towards a Decision Aid Assessing Preferences of Glucose-Lowering Drugs: The Dilemma of Choosing
Roldan Munoz S, Mol PGM, de Vries F, van Dijk PR, Hillege H, Postmus D, de Vries ST
Patient Preference and Adherence 2025, 19:215-234
Published Date: 25 January 2025
Multiple Myeloma Experiences and Preferences: A Mixed Methods Study of Patients and Care Partners in the United States
Flora DR, Byrd R, Platt DA, Hlavacek P, Hoag Goldman E, Cappelleri JC, Kennedy CT, LeBlanc TW
Patient Preference and Adherence 2025, 19:963-979
Published Date: 8 April 2025
Criteria For Agreement When Conducting Local Consensus Discussions: A Qualitative Study
Pagano L, Long JC, Francis-Auton E, Hirschhorn A, Braithwaite J, Arnolda G, Sarkies MN
Journal of Healthcare Leadership 2025, 17:159-172
Published Date: 5 May 2025