Back to Journals » Patient Preference and Adherence » Volume 17
Applying Learning Principles Within Parent Education: Exploring Nurses’ Practice and Parents’ Experiences
Authors Thompson DL ![]() , May EJ, Leach MJ
, May EJ, Leach MJ ![]() , Smith CP
, Smith CP ![]() , Fereday JA
, Fereday JA ![]()
Received 15 June 2023
Accepted for publication 31 October 2023
Published 14 November 2023 Volume 2023:17 Pages 2949—2970
DOI https://doi.org/10.2147/PPA.S426043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Deryn L Thompson,1 Esther J May,1 Matthew J Leach,2 Colleen P Smith,1 Jennifer A Fereday1
1Clinical and Health Sciences, University of South Australia, Adelaide, SA, Australia; 2National Centre for Naturopathic Medicine, Southern Cross University, Lismore, NSW, Australia
Correspondence: Deryn L Thompson, Clinical and Health Sciences, University of South Australia, 108 North Terrace, Adelaide, SA, 5000, Australia, Tel +61 8 83021166, Email [email protected]
Purpose: In parent-education practice nurses use Learning Principles (LPs) when helping parents to develop the knowledge and skills required to care for their children. LPs are basic precepts of learning, comprising people’s beliefs, behaviors and reasoning processes. LPs underpin parents’ active engagement, confidence building and decision-making, as information provided becomes usable knowledge. However, the ways nurses apply LPs in parent-education practice are poorly explained in healthcare. Likewise, descriptions of parents’ learning experiences, associated with the use of LPs in nurse/parent-education interactions, are lacking. This study aimed to explore and describe nurses’ perceptions and use of LPs, and parents’ learning experiences in one healthcare organization.
Participants and Methods: Using an action research design, 25 nurses and 18 parent participants were purposively recruited across metropolitan Adelaide, Australia. Data were collected through observations and semi-structured interviews and thematically analyzed simultaneously June-December 2017.
Results: The LPs nurses used, and those important to parents’ learning experiences created three overarching themes: 1) collaborative relationships, 2) deepening learning insights, 3) the learning environment. Despite their apparent use, nurses struggled to explicitly describe how they perceived LPs, believing their knowledge and use was sub-conscious − tacit. However, tacit knowledge hinders communication and explanation of LPs used within parent-education to other nurses. The member-checking of interview data helped to stimulate the nurses’ metacognition (thinking about their thinking), unlocking their LPs awareness.
Conclusion: Nurses used LPs in practice but their knowledge was tacit. Through metacognition, nurses started to recognize the ways LPs influenced their practice and parents’ learning capabilities. Increasing healthcare constraints, including time allowed for parent-education, require nurses to optimize their use of LPs. Future research should identify ways nurses can communicate their use of LPs, potentially enhancing parents’ active learning experiences and concordance with health recommendations.
Keywords: cognition, metacognition, parent-education, nurses, knowledge, health literacy
Introduction
Parent-education encounters between health professionals (HPs), parents and families are multifaceted, collaborative, person-and family-centered (PFC) learning processes. Learners need to turn the information shared with them into knowledge they can use meaningfully, and often facilitate behavior changes, to follow health/treatment recommendations.1–3
The literature surrounding parent-education has long emphasized that HPs, especially nurses, embrace the concept of adult Learning Principles (LPs), shown in Table 1, because parents, as learners, are adults.3–6 LPs are the basic precepts comprising people’s beliefs, behaviors and reasoning processes related to learning.1,7–9 Underpinning the learning process are cognitive LPs, as shown in Table 1, which assist people to connect new information to existing knowledge and to reshape their knowledge using memory, perception and reasoning.8,9 The reshaped knowledge is then used, practiced, refined, stored, retrieved when needed, and then applied by the learner.9–11 When nurses integrate cognitive LPs into their parent-education practice, they help parents to think, reason and problem-solve − vital aspects of learning, as parents work towards developing the knowledge and skills to meet their children’s healthcare needs.3 Educational psychology research emphasizes that learning extends over a person’s lifespan, not just adulthood.3
 |
Table 1 Examples of Learning Principles |
The evidence for using adult LPs alone in parent-education is weak – a scoping review revealed that the ways nurses use adult or other LPs to facilitate parents’ learning is not overtly explained in publications.6 The adult LPs commonly cited in the literature, as shown in Table 1, were stated, but explanations of how nurses use LPs were lacking. With such explanations lacking, nurses’ knowledge development about the role of the LPs is potentially compromised. This is an important oversight, as nurses need to integrate, into their practice, those LPs that help parents to think (use cognition), reason and problem-solve.3 LPs can aid parents’ development of these vital skills needed for them to navigate the health system and meet their children’s healthcare needs and preferences.6 Currently, limited explanations on using LPs mean nurses have minimal professional practice guidance to recognize the ways they can integrate LPs into parent-education practice (in contrast to teaching strategies). This potentially impacts parents’ learning experiences.6,10
To date, research surrounding parents’ sub-optimal health-related learning experiences and their lack of concordance to care-plans/treatments have not explored those LPs linked to cognition and learning.6 Parents’ knowledge and treatment concordance shortfalls have commonly been attributed to their underserved health literacy needs, inadequacies of nurses’ practice, and time limitations, but solutions were not forthcoming.7,12–15 Researchers developed tools to address such knowledge and practice shortcomings but these tools fail to explain to parents and nurses the ways learning takes place.15 Few studies have explored parents’ insights about the aspects of their learning experiences they believe important, when parent-education is facilitated by nurses integrating LPs into practice.3,6 The objective of the study was to explore nurses’ perceptions and use of LPs while simultaneously exploring parents’ perceptions of their learning experiences during nurse/parent encounters, to describe and communicate how LPs are used within parent-education practice.
Materials and Methods
Conceptual Framework
Interpretivism and Social constructivism (SC) formed the study’s theoretical framework.16–18 When using interpretivism researchers aim to enrich understanding and interpret the multiple realities of participants by interactively exploring each one’s experiences, context and meanings they place on the situations under investigation. Collecting data in the natural setting of nursing practice and parents’ educational encounters helps create better understanding.16,18 SC further informed the study, because the premise of SC is that the individual’s mind creates and makes sense of reality within a person’s world.19 By using SC, participants’ reflection, self-questioning, discussion and interactions enabled the study to explore the multiple realities of nurses’ beliefs, comprehension and interpretations of using LPs. For parents, their versions of their learning experiences were explored, thus creating new understandings about LPs within parent-education.17,19
Research Design
The overall study employed an exploratory, practical action research design.20,21 Action Research is a cyclic process with participants’ and researchers’ collaborative involvement in the research process as they work towards identifying problems and creating change processes.20 The study’s focus was introduced to participants by DT, an experienced nurse and educator with extensive expertise in PFC education and learning.21 DT and the participants actively questioned and challenged their accepted practice, perceptions, experiences and assumptions about LPs and parents’ learning experiences within parent-education, beyond their recognized boundaries, working towards creating solutions to the issue under exploration.20–26 Stringer’s20 Look, Think and Act approach was selected for its use of everyday language terms that would resonate with both nurses and parents. In each cycle, participants and researchers explored their perceptions and use of LPs and identified problems experienced with LPs (LOOK). Data were analyzed and feedback provided on the collected, synthesized data (THINK). Participants and the researcher worked co-operatively towards creating meaningful solutions to issues surrounding the perceptions and use of LPs in practice (ACT).20 The overall study comprised three cycles, which ultimately aimed to identify, describe and develop ways to explicitly communicate the LPs that nurses used in parent-education practice and that parents considered were important to their learning experiences. This could potentiate change for nurses’ practice and parents’ learning within the healthcare organization of the participant sample.20–22 The study reported herein focuses on the first of these three cycles (shown in Figure 1). The study aimed to explore nurses’ perspectives and how they apply LPs in their parent-education practice by addressing the research questions:
- How are nurses using Learning Principles in parent-education practice?
- What is the evidence that nurses use Learning Principles in parent-education practice?
- What are parents’ experiences of learning during parent-education encounters?
 |
Figure 1 Cycle 1 of the action research process Stringer.20 |
Sample, Setting, Ethical Approval
The study was conducted within one healthcare organization in metropolitan Adelaide Australia providing hospital, ambulatory and community-based care for children 0–18 years. A purposive sample of Pediatric nurses (PNs) and Maternal Child and Family Health nurses (MCaFHNs) and parents were invited to participate following ethical approval.27 The study complied with the Declaration of Helsinki and was approved by the Human Research Ethics Committees of the Women’s and Children’s Healthcare Network (reference number: HREC/17/WCHN/41) and the University of South Australia (reference number: 200009).
Guided by sample sizes reported in other parent-education studies, the intent was to recruit 20 nurses and 20 parents.28–30 PNs are nurses commonly caring for children with health conditions, whereas MCaFHNs promote health, wellness and parenting capabilities in Australian community-care.13,31,32 Terminology addressing MCaFHNs varies globally, eg Plunkett nurses in New Zealand and home visitor nurses in United Kingdom.32 The MCaFHN acronym is used in this paper.32 Unless there is a need to differentiate between PNs and MCaFHNs, the term nurses applies hereinafter. Participant inclusion and exclusion criteria are outlined in Table 2. The study was not restricted to nurse/parent dyads due to the study’s time constraints.
 |
Table 2 Inclusion and Exclusion Criteria |
Recruitment
Following ethics approval, the nursing directors sent invitational emails, including the consent forms, to nurses working in community and hospital-based sectors of the organization.27 Study information was shared at nurses’ seminars. For parents, study information was disseminated through the organization’s health-consumer newsletter and flyers placed in waiting room areas of the healthcare network settings. After contacting the principal researcher, interested parents were sent the study details and forms.
Ethical Considerations
Written, informed consent was obtained from participants before their voluntary enrolment in the study, including their agreement that the findings may be published, but with data de-identified.27 To maintain anonymity, participants were assigned a unique identification number from a list of computer-generated numbers between 1–150, upon enrolment.27 This number, recorded on the observation field guide, stated on audio-recordings and transcripts, ensured accuracy in linking each participant’s observation and interview data, while not identifying them.27,33,34
Data Collection (Look)
Data were collected by the principal researcher (DT), between June and December 2017, using two methods ─ non-participant observations of nurse/parent-educational encounters, and semi-structured audio-recorded interviews.33,34 The tool collecting the subjective observational data was a written field-note guide, based upon other parent-education observational literature34 (Supplementary File 1). Semi-structured interview guides, one for nurses and one for parents, gathered participants’ interview data.34 These guides, informed by current literature on LPs, learning and parent-education,8,13,14,28–30 were pilot tested by three experienced nurses providing, and three parents receiving, parent-education, but who were not study participants. The few minor adjustments they suggested, along with scrutiny by the research team resulted in the interview guides seen in Table 3.
 |
Table 3 Semi-Structured Interview Guide |
Non-Participant Observations
Non-participant observations (15–120 minutes duration) enabled the researcher to identify and gain deeper insight into nurses’ behaviors regarding their use of LPs and learning facilitation skills, and of parents’ learning experiences.33 The community-based observations occurred in parents’ homes or MCaFHN clinic settings, while hospital-based observations occurred in ambulatory-care or day-procedure areas. In each encounter, data were collected on the use of LPs in practice eg how nurses (a) conveyed information to parents, (b) facilitated the information to knowledge transformation process, (c) demonstrated the skills parents needed/wanted to learn, (d) helped parents to practice the skills shown to them, (e) established that parents comprehended the information discussed, and (f) evaluated/planned to evaluate parents’ comprehension of the information. Documenting of the observational data systematically using a written field note guide also helped create reflexive awareness of the researcher about the participants.33,35
Semi-Structured Interviews
Semi-structured interviews (duration of 20–40 minutes) were conducted by DT 1–2 weeks after the observation session via telephone or face-to-face, to help maximize each participant’s recall of the observed parent-education encounter.34 For parents, the interviews captured their learning experiences with a nurse, to establish what attributes parents identified as important to their learning experiences and these descriptions also served to reveal LPs the nurses used.34 Parents’ educational levels were not sought. As the topic related to learning in a healthcare setting, the researcher did not want to inadvertently exclude potential participants from a diverse community or disadvantaged group. It was possible that asking about formal educational level could be a deterrent to participation or seen as discriminatory.36 The nurses’ interview questions asked about basic demographic data, their ways of facilitating learning within parent-education, as well as their perceptions and use of LPs.
Data Analysis (Think)
After each observation, the field note record33 with the unique participant identification number27 was transcribed by DT and imported to NVivo11®.37 Audio-recordings of the semi-structured interviews, also with the unique participant identification number,27 were transcribed verbatim by an experienced healthcare transcriber.38 The full content of all transcripts were read twice by DT, while listening again to the recordings, optimizing accurate conveyance of participants’ meaning and terms used.38 On the second examination of the data, ideas of interest or aspects linked to research questions were recorded as margin notes.39 DT then reviewed the observation fieldnotes, linked each one to the participant’s interview data, creating memos when ideas expanded any initial insights. Interview data were then entered into NVivo11® to manage and structure the data, and facilitate the thematic analysis, using Braun and Clarke’s six step approach, shown in Supplementary File 2.39,40
Coding and Themes
Each participant comprised one unit of data.41 When a participating nurse and a participating parent were in the same educational encounter, these participants were linked, forming a dyad (n=4). As the study sought to substantiate how nurses used LPs, rather than identify and compare differences between parents or the two groups of nurses, comparative analysis within these units was not undertaken.40 However, data within the dyads could potentially confirm or refute the use of LPs within a nurse’s practice or a parent’s learning experiences.40 During this initial coding run, when connections to some existing nodes were seen, tree nodes were formed. These represented a hierarchical structure of the data analysis.41 As the analysis progressed, any points of interest and evolving ideas were noted, with memo links created between nodes and the transcripts. When no new codes were needed to code the data, saturation was considered reached.39,40 As data interpretation progressed, codes with similar meanings were grouped into themes.40,41 An example of this process is shown in Figure 2.
 |
Figure 2 Example of the Themes Formed in the Data Analysis. |
Rigor
Steps to establish trustworthiness of the research were undertaken. The depth and scope of responses captured from the two methods of data collection supported the triangulation of data, assisting credibility.42,43 Convergence of data helped improve accuracy and reliability, thereby creating a credible, coherent picture of the nurses’ use of LPs and what parents saw as necessary to optimize their learning experiences.35,43 Pilot testing of the data collection tools, by nurses and parents with experiences in parent-education, but who were uninvolved in the research study, assisted study rigor.40,44 Interviewer variability was reduced by having only one interviewer (DT), and by using a semi-structured interview guide for all interviews.42 However, this created a limitation to the study – observer bias. DT’s reflexive journalling of any researcher beliefs, attitudes and preconceptions before and after observations helped to reduce this limitation.42 This form of reflexive journalling also addressed researcher positionality within the study.45,46 These journal entries were discussed with the research team regularly, to expose, discuss and address any potential biases.46
Cross-sections of the transcripts were analyzed independently by members of the research team, discussed and debated at multiple time points, until consensus was reached.40–42 Member-checking was also carried out to aid credibility, by sending a summary of the study findings to participants, who were asked to contact the researchers if they disagreed with any content.40
Results
Forty-three participants enrolled in the study: 25 nurses (14 MCaFHNs and 11 PNs) and 18 parents. Nurses’ ages ranged from 25–69 years (23 female, two male). For the parent participants (17 female, one male), ages ranged from 20–49 years and comprised 14 parents seeing a community-based MCaFHN (from herein termed CBPa) and four parents seeing a hospital-based PN (termed HBPa). Of the nurses, 11/25 (44%) had over 10 years of parent-education experience; 23/25 (92%) had post-graduate qualifications, mostly graduate or professional certificates. Participant characteristics and demographic data are shown in Tables 4 and 5.
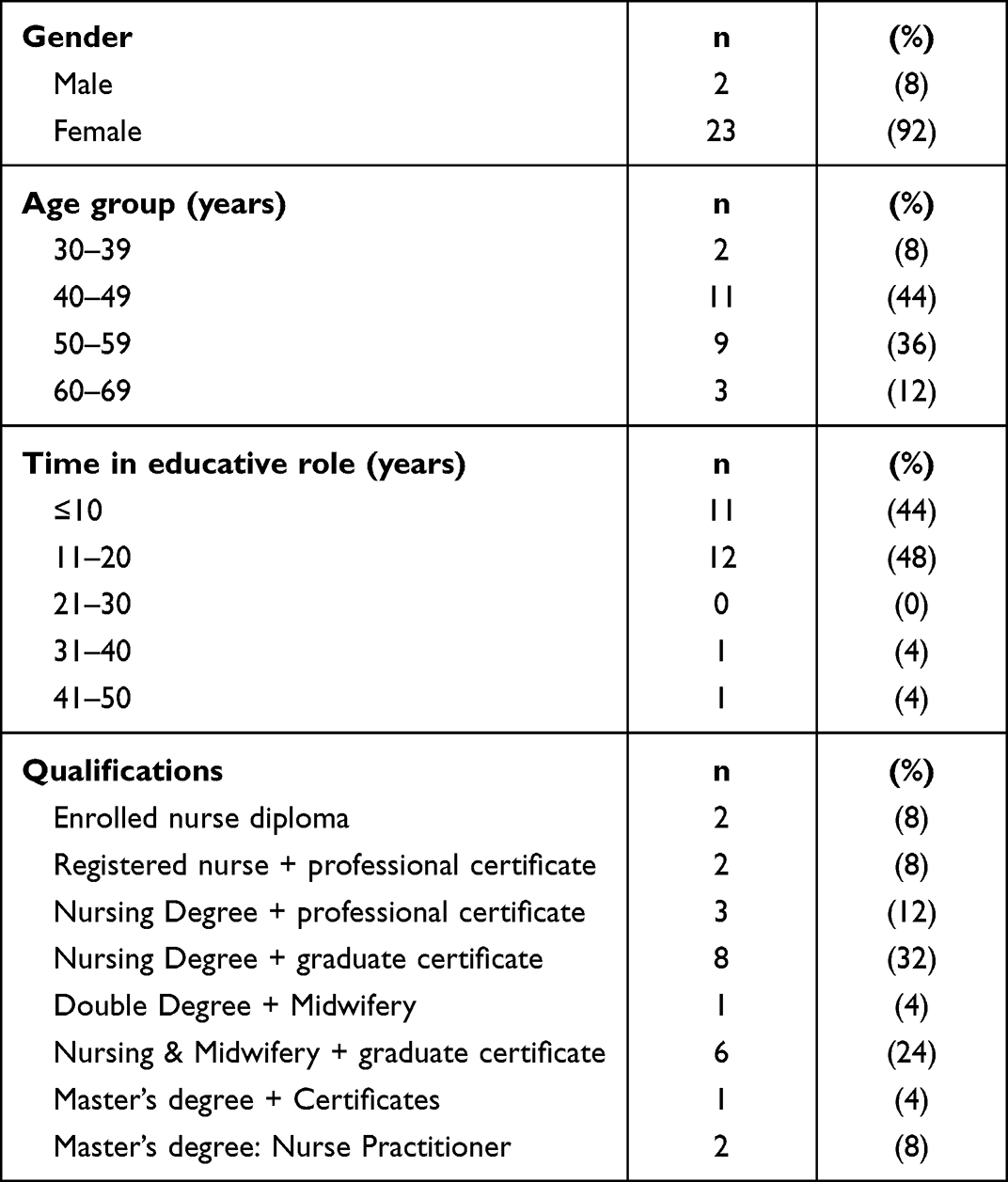 |
Table 4 Demographic Profile of Nurse Participants (n=25) |
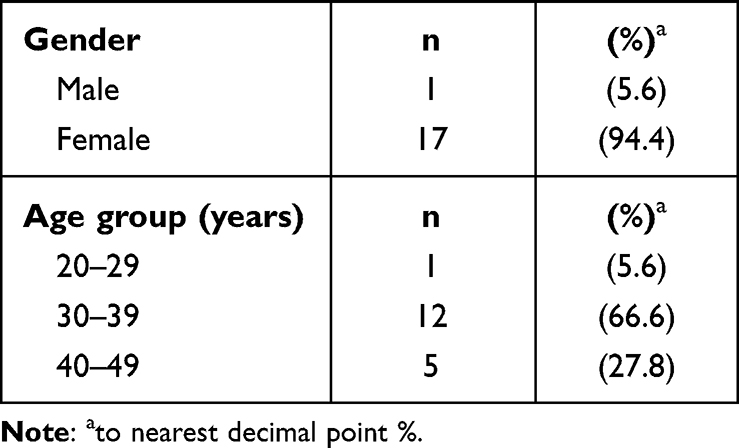 |
Table 5 Demographic Profile of Parent Participants (N=18) |
Observations
Nurses demonstrated the use of a range of LPs during observations of their educational interactions. All nurses greeted parents and their children, clarifying the child’s identifiers, required by national healthcare safety standards.47 No nurses formally identified parents’ health literacy levels, but all nurses used understandable, jargon-free terminology, and broke explanations of issues into smaller steps. Diagrams, audio-visual materials, care-plans or written resources supplemented the nurses’ discussions, promoting HBPas’ and CBPas’ active participation as the nurses explained the information. Nurses showed parents how to use equipment, such as medication devices, where applicable. Parents performed required skills, practiced what was demonstrated, with nurses observing parents’ body language to see where skills refinements were necessary. Nurses asked parents direct and indirect questions, provided cues if parents struggled to respond at times, encouraged parents to paraphrase the issues discussed and provided parents with opportunities to ask questions. Three MCaFHNs facilitated CBPas to “answer their own questions” (creating a solution themselves) by rewording parents’ initial questions. For parents who had seen a nurse before, nurses checked on progress made since the previous appointment (Box 1).
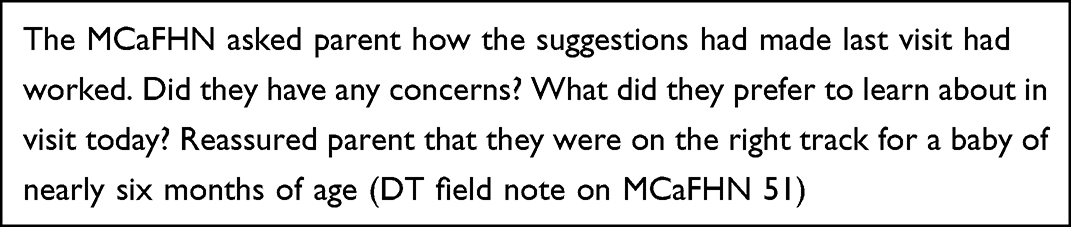 |
Box 1 Example of a Field Note in Observation Data Collection |
Two PNs created scenarios to check HBPas’ comprehension of information, asking questions to establish parents’ responses and reactions, each in contexts relevant to their family or children’s health situation. Nurses documented data in the case notes and discussed arrangements for subsequent appointments.
Semi-Structured Interviews
In the interviews, all nurses identified with being confident in their parent-education skills. Three overarching themes related to the ways the nurses used LPs and parents’ descriptions of their learning interactions became evident: 1) collaborative relationships, 2) deepening learning insights, and 3) the learning environment. A surprising finding from the interviews was the nurses’ significant struggle to explicitly describe how they used LPs when asked direct questions about using LPs. Nurses seemed unaware that within their descriptions about their successful parent-education (teaching) strategies, they had already outlined ways they were using LPs.
Theme 1: Collaborative Relationships
Collaborative relationships between nurses and parents, termed “shared care” by PNs and “partnerships-in-care” by MCaFHNs, were foundational aspects of parent-education, parent learning processes and learning outcomes. Nurses helped parents from diverse backgrounds to develop trust, feel safe, feel ready to learn, develop agency and work towards behavior changes required to capably care for their children. Nurses emphasized the importance of adopting a collaborative approach in building trust between the nurse and parent, as illustrated in this quote,
It is important to be non-judgmental, recognize people who come from different places and backgrounds…are impacted differently, even if they had similar experiences. Being there, showing people they matter is paramount…before you can make any changes. Gaining trust. Keeping the child in focus and their safety. (MCaFHN 91)
Some MCaFHNs (3/14; 21%) and PNs (2/11; 18%) “read” parents’ body language to gauge the progress of the evolving nurse/parent relationship and determine how the parent/baby relationship was developing.
MCaFHNs strove not to be seen by parents as the experts in nurse/parent collaborative relationships, believing the term “expert” implied potential nurse/parent power imbalances, which could impact learning. In contrast, all parents reported that they wanted nurses with expertise to provide them with up-to-date education and resources using straight-forward language. Parents (5/18; 27%) and MCaFHNs (5/14; 36%) concurred that continuity of care with the same MCaFHN visiting the parent in their home strengthened the nurse/parent relationship and greatly assisted with their learning, especially in the early weeks when parents were adjusting to caring for their children. These attributes represented cognitive LPs, although the nurses did not overtly use the terms. For PNs, continuity of care was less possible as rostering changes determined where and when nurses provided care and parent-education, but all HBPas preferred seeing the same nurse.
I had a lot of trust in the process…her knowledge about what she was doing, explaining why…that stuff helped the relationship…just meant that my confidence and trust in her doing and getting the test correct, so that he doesn’t have to do it again was important…my child also had confidence in her… (HBPa 77)
Theme 2: Deepening Learning Insights
As participants’ descriptions unfolded, deeper insights into the ways LPs were used within these nurses’ practice and parents’ experiences, became evident. Four sub-themes formed: i) building on strengths and achievements, ii) facilitating parents’ choices, iii) learning as a process, and iv) the nurses’ struggle to articulate LPs.
Building on Strengths and Achievements
Nurses’ Descriptions
The MCaFHNs built on parents’ achievements, helping parents set regular goals. Nurses established parents’ learning and understanding informally by observing parents’ body language (which nurses termed “cues”), asking about parents’ accomplishments at subsequent visits and asking questions to prompt parents to self-report on their progress. These examples illustrate the LP of connecting of new knowledge to existing knowledge
I always assess the situation, the parent’s intellect, for a child with chronic illness, they often know more than we do. We know technically more; they live with it… (PN 65)
PNs continually encouraged parents’ active engagement with the information provided, regardless of whether treatment /management goals were or were not achieved. All nurses respected that parents often had significant knowledge about caring for their children,
Always finding something positive to focus on and always keep reminding them of the good job they’re doing (MCaFHN 89).
Parents’ Descriptions
For CBPas the shared, interactive, strengths-based approach of the nurse placed each parent centrally in the learning interactions. This approach significantly influenced parents’ motivation in learning to meet their children’s needs and provide appropriate care, capably and confidently, even if setbacks occurred – a conducive learning environment, consistent with another key LP.
… I got my questions answered…I was not just a number… I felt my learning was on the right track…reassurance is really helpful as a new mum, that you are doing the right things… (CBPa 59).
Likewise, for HBPas, it was critical that PNs acknowledged their strengths and achievements as they learned, adapted or mastered the necessary care. HBPas needed to feel confident adhering to treatment recommendations, not only in the healthcare setting, but also once they were home and the PN was not at hand. Nurses were fundamental support mechanisms for parents, especially when nurses were contactable between visits.
… at first, we were petrified and overwhelmed…but each time we left with a bit more information, I felt I knew there were things I could do, if something happened…each time we left with a bit more confidence (HBPa 104)
…I never left feeling confused, my confidence was higher… (HBPa 104).
Facilitating Parents Having Choices
Nurses’ Descriptions
Nurses’ descriptions confirmed the observation data reflecting the use of LPs – they listened to each parent’s situation, varied their approach of providing evidence-based information to meet each parent’s psycho-socio-cultural situation, learning needs and preferences. The nurses offered parents different learning options, where possible.
I give parents choices…its helpful they realize they have choices…acknowledge what they know, help them build their confidence to use the knowledge they may have already have or are working on (MCaFHN 79).
If parents did not achieve their goals, nurses and parents collaboratively discussed alternative approaches, with nurses supporting parents’ suggestions and preferences. This assisted the development of parents’ decision-making skills:
Supporting what parents are ready, able to take on…giving parents choices…sharing of knowledge, but options of how they want to go about it…there’s no one right way unless it’s. [compromising] safety (MCaFHN 94).
As parents gained knowledge, skills and confidence, parent participation increased and nurses’ involvement in care activities decreased. For PNs, meeting parents’ preferred needs (as key LPs) was balanced by parents undertaking the required evidence-based treatments and care, relevant to each child’s condition.
I give families the opportunity to express where they are at, see what they want to achieve and to choose where possible, the direction of how the education session proceeds, for the safe management of their child’s (condition named) (PN 57)
Parents’ Descriptions
Parents appreciated those learning approaches where nurses respectfully assisted them to have choices in acquiring information and applying their learning, provided the choice posed no safety risk to the child. Sharing of parents’ peer learning experiences, in the 1–2-hour group sessions, was another learning approach choice valued by parents.
I would highly recommend it [group learning] as an option for mothers and fathers who need support. Even for a short time…it empowers them… (CBPa 52).
Parents’ descriptions aligned with the nurses’ descriptions, providing evidence of the LPs nurses used as they guided parents’ knowledge and skills development via parents’ peer interactions.
I think that confidence to know that everything’s okay…you’re doing everything right…also the process. One thing I really liked about this last visit; the nurse told me there’s choices…other options available if this doesn’t work (CBPa 59).
Learning as a Process
Nurses’ Descriptions
Most nurses perceived learning as a constructive process, unlikely to be achieved in single parent-education encounters.
It’s a process, not a one-off situation, establishing relationships with parents, seeing what needs they have, then moving through the process, involving many sorts of information. Things will change, the disease will evolve… education needs to evolve with that as well (PN 72).
However, nurses used multiple terms to describe how they established what parents knew already, what they “wanted to know”, whether any prior learning was successful and how parents were currently managing their children’s care. These included body language of the parent and the baby or child, verbal cues, a mother’s general demeanor or changes in the home environment since previous visits.
Nurses, including 9/14 (64%) MCaFHNs and 9/11 (82%) PNs, shared information with parents using a mix of verbal, web-based and/or written evidence-based “understandable” information. Two PNs equated suitable health literacy with “understandable” resources, but interview data confirmed the observation data, that no nurses used any formal process to identify parents’ specific learning needs or health literacy levels. While observations showed all nurses demonstrated and explained to parents the “how, what, when and why” of undertaking/care and treatments (fundamental cognitive LPs), only 9/25 (36%) of nurses explicitly stated that they demonstrated the treatments/required care. Commonly, the nurses described parents as “visual learners”, but some projected their own learning preferences.
I also look at whether for some people it’s appropriate to give them written material and some people they’re very visual or hands on… I actually like visual myself… I also get them all show me how they use the [device]. (PN 53).
Having parents paraphrase the information exchanged at the end of the learning encounter and noting visual cues of parents’ body-language was common practice of all nurses to “check understanding”. Seven MCaFHNs used “cues” to stimulate parents to act on the feedback in each parent-education encounter, thereby encouraging parents to create and learn solutions applicable to their situation. This practice was also seen in the observations. These examples further underline the LP that learning is a process whereby learners construct new knowledge and connect it to existing knowledge. A further three nurses encouraged parents to answer their own questions, which provided evidence they used those cognitive LPs linked to parents’ problem-solving skills development.
…I provide information, I provide visual, I chat and ask questions and try to encourage clients to feedback. Often, they answer their own questions…” (MCaFHN 98).
Overall, 64% of these nurses did not recognize that the attributes of their practice they described as parent-education strategies involved LPs, as is represented by these nurses when articulating their parent education practice, but later they were unable to describe what LPs were or how they used them:
…a mutual exchange of information-sharing… encompasses the educator finding out information, providing support…an exchange of knowledge to improve what they already know… Parent-education comes in lots of different ways, …it’s not just one off…an initial consult then…follow-up. Family and parent-education is whatever they need…to better understand the condition… (PN 69).
…the key is listening, finding out the information they want, acknowledging how much they can understand. The advice you give is achievable for them, practical. Too complex, it’s overwhelming. You have to break it down, work on something that’s more manageable. It might depend on their stress levels when they come, you work on something slowly, gain their confidence, they need to feel comfortable with me. If they feel confident, they come back…. (MCaFHN 91)
Parents’ Descriptions
All 18 parents attributed their successful knowledge and skills development to the nurses’ learning facilitation approach, with interview data supporting the observational data. Parents indicated that nurses applied LPs by using straightforward terms to convey the information and by helping parents to interpret the meaning of baby’s “cues”.
Things I was doing instinctively; things I wasn’t aware of…What constituted play for example…how to educate your child appropriate for their age.what milestones to look for. Things I mightn’t have noticed like…things I thought were, ‘I want to be fed’ cues were actually early talking cues… (CBPa 74)
…I’m not fully confident, but I’m feeling a lot more comfortable…I feel I’m able to help my child with the knowledge that I’ve been given (HBPa 10)
It was important to parents’ learning experiences that information was delivered in small amounts and supplemented with up-to-date written resources. Parents also valued being able to practice the techniques/treatments “unrushed”, until they achieved mastery. CBPas all sought reassurance from MCaFHNs that they were “getting it right”: satisfying their children’s growth, development and safety needs– attributes both nurses and parents considered important.
The Nurses’ Struggle to Articulate Learning Principles
Surprisingly, 9/25 (36%) of nurses claimed unfamiliarity with the term “Learning Principles”. Two MCaFHNs (14%) professed using adult LPs, but could not outline any principles or attribute them to any theorist. The remaining nurses struggled to articulate what LPs were and make connections to their practice, despite recognizing the term, with key examples shown in Box 2.
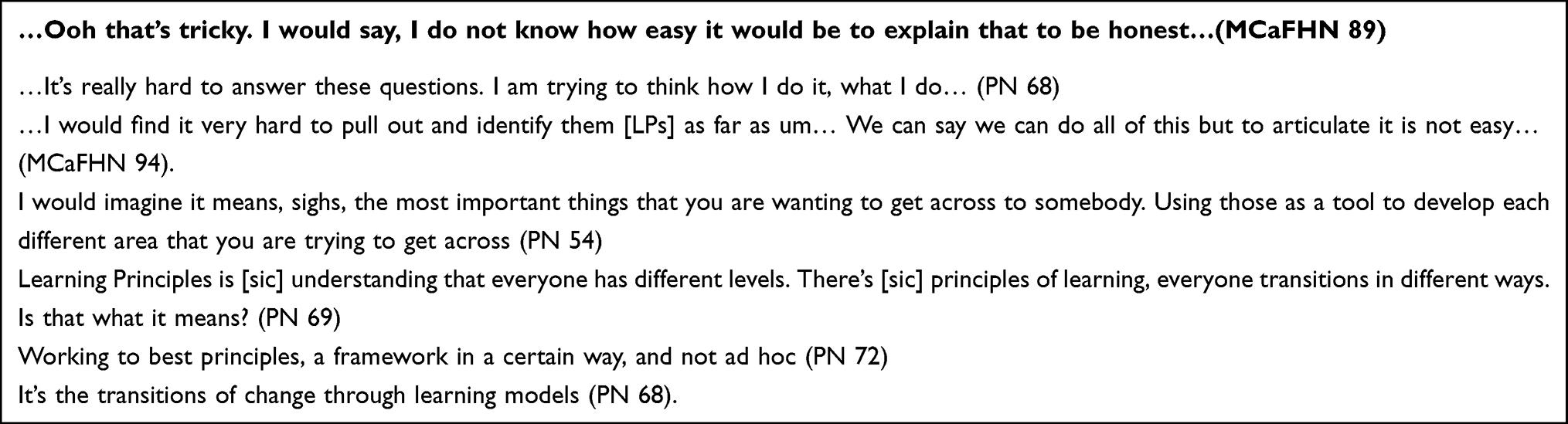 |
Box 2 Examples of Nurses’ Struggle to Articulate the LPs They Were Seen to Use in the Observations |
Despite these difficulties, nurses implicitly described using a range of LPs as they talked about their parent-education strategies− accepting information, being supportive, using listening skills, providing non-jargonistic explanations, ratifying what was said, “reading” people, encouraging self-motivation, being culturally safe, and being “open to change” to improve practice. Four MCaFHNs (29%) and 3/11 PNs (27%) expressed LPs as clinical procedures or guidelines. Although the nurses “knew” which LPs to use, they were unsure how they gained their skills in using LPs, suggesting it was likely to be intuition… “I think I do it [use Learning Principles] without knowing I do it”. (PN 53).
Theme 3: The Learning “Environment”
The learning environment refers to the locations and emotional factors influencing the nurses’ use of LPs and parents’ learning experiences. Four sub-themes evolved: i) the physical location, ii) barriers to learning processes iii) organizational influence, and iv) nurses’ self-evaluation of learning facilitation skills.
Physical Location
Nurses’ Descriptions
The hospital-based clinics required appointment scheduling within specific time limits, challenging 8/11 (73%) PNs’ use of LPs within parent-education. The busyness of clinics, parents’ stress associated with the acuity of the health situation and transport to appointments adversely affected the parents’ ability to retain and recall information shared in some educational encounters.
The open-plan clinical settings affected patient/parent/family privacy, thereby impeding parent learning for 4/11 (36%) PNs and affecting LP use.
You’re on the ward, you’re doing some form of education. There’s always a nurse or another parent interrupting…doctors or the phone…some sort of interruption or noise (PN 78)
Scheduling of the MCaFHN parent-education sessions seemed less pressured. For those parents requiring home visits, the duration for education was 1–1.5 hours and privacy was assured. MCaFHNs facilitated parent group peer-learning sessions over 1-2-hours duration, creating a “safe” learning environment for parents to share experiences.
Parents’ Descriptions
CBPas had difficulty organizing their lives in the ways they had before their baby’s birth. They valued the safety and privacy of the MCaFHNs home visits, as many parents felt vulnerable or socially anxious for several months.
It [going to the clinic] adds an extra layer of anxiety along with all the new things you’re experiencing as a parent, so you freeze up. You’re less likely to open up, and share what could be a good, valuable experience with other people. (CBPa 74).
Parents’ learning capability also fluctuated, so parents wanted MCaFHNs to repeat the information provided, demonstrate tasks frequently and vary the learning pace according to their needs at each visit.
Things I had forgotten, she fleshed out as well, gave a prompt…that helped me… (CBPa 70).
This helped build parents’ confidence and capability in caring for their baby. These parents’ (6/14, 43%) descriptions provided further evidence that MCaFHNs used cognitive LPs.
Barriers to Learning Processes
Nurses’ Descriptions
Nurses found less clinical time provided for parent-education than earlier in their careers. Moreover, 7/14 (50%) of MCaFHNs needed to adapt their approaches to meet parents’ often complex mental health needs, which affected parents’ capacity to process information provided. MCaFHNs also felt underprepared to address parents’ mental health issues.
Time can be a barrier…you’re expected to just move quickly in a consultation, from one client to the next…sometimes you’ll feel there is not enough time to really stop, listen and get a better sense of what you need to know …a client’s issues…. (MCaFHN 44).
I have to think about other ways we can deal with the issues. It impacts a lot on their learning. Once maternal anxiety or postnatal depression is dealt with, they can actually learn… (MCaFHN 56)
PNs adapted their learning approach to accommodate parents’ stresses and the emotional impact associated with their child’s health diagnosis. These nurses’ descriptions reflected their use of LPs related to readiness to learn and parents’ ability to process information at times of duress.
When I do it [parent-education for] a new diagnosis in a baby, I realized very early on, that you have to be very simple, …it’s extremely overwhelming (PN 68).
Parents’ Descriptions
Sleep deprivation and fatigue among CBPas, in the early months of their babies’ lives, made information that would have previously been informative, overwhelming. CBPas with new babies (4/14; 29%) supported the nurses’ comments, that repetition/reinforcement of the key points to know were critical to their learning. These also reflected nurses integrating LPs.
…because you’re sleep-deprived it’s hard to take in a lot of information, so just that repetitive and checking in… is welcomed… (CBPa 81)
When parents encountered different nurses in the MCaFHN clinic visits (4/14, 29%), they found inconsistencies in the information provided, which created some confusion, impacting their learning. Receiving “outdated” resources was a barrier to learning for 4/18 (22%) participating parents, who had undertaken their own research before attending the educational encounters with the nurse. One HBPa was disappointed the nurse did not explain the procedure being performed on her child. ‘the assumption we knew from tests before…but each time can be different…’(HBPa 96).
Organizational Influences
No nurses were aware of or had undertaken professional development (PD) specific to using LPs and they considered this a shortcoming of the organization. Although nurses’ practice performance was expected to meet Key Performance Indicators (KPIs) to demonstrate the organization’s quality and safety achievements, nurses believed KPIs did not factor in that parent-education and learning facilitation took considerable time to deliver. Parents’ satisfaction with their learning was impacted, which also had a bearing on nurses’ time to be able to use LPs. Furthermore, nurses (5/25; 20%) and parents (4/18; 22%) believed parents’ learning experiences were adversely affected by the tick box format for documenting evidence that parent-education occurred. Nurses expressed concern that parents’ learning and understanding may be assumed successful when a box was “ticked”, rather than the intent of showing a task had been undertaken. Parents suggested nurses ticking boxes diminished the quality of nurses’ individualized learning facilitation.
Tick-boxes are really a communication tool to say, this was discussed but not necessarily understood. Reminder, revisit this (PN 72).
…The questionnaire led the form of the session…I usually write down a few things I mean to cover, but because of that formal process of ticking off different aspects, I didn’t cover necessary aspects’ (CBPa 95).
Nurses’ Self-Evaluation of Learning Facilitation Skills
Nurses predominantly used parents’ verbal feedback, body language observations (which they termed cues) or self-reflection to self-evaluate their learning facilitation skills.
I reflect, did I get that right? Was it right for that person? I also revise and update my resources regularly, modifying them if feedback suggests they are not working…if a person’s glazing over, I think ‘you need to pull back on details…” (PN 72).
Nurses assumed their learning facilitation approach was successful when parents capably performed the care needed, returned for subsequent visits, or reported an improvement in the child’s overall condition. Additionally, 2/25 (8%) nurses perceived that parents’ responses to written consumer satisfaction surveys, tallied by the organization, reflected their satisfactory parent-education skills levels, although the surveys contained no specific parent-education questions. For 10/25 (40%) of nurses, their parent-education capabilities were professionally “evaluated” by line-manager performance reviews or in team meetings. Nurses acknowledged that such discussions lacked specific questions about nurses’ learning facilitation, use of LPs or parent-education skills capability.
Discussion
These qualitative study findings add important new insights for parent-education in nursing about the ways nurses use a range of adult and cognitive LPs. Furthermore, parents’ learning experiences, reflecting various LPs used, were revealed. Parents emphasized the fundamental importance of the nurses factoring in their individualized psycho-socio-cultural needs, beliefs and values from the outset of their learning process. Once a collaborative relationship (a parent/nurse learning partnership) was established, parents could then use the knowledge they created from the information provided, to build the skills they needed to care for their children.48 Previously, the ways LPs are used in parent-education practice have been not overtly explained in the healthcare literature.6
Three unexpected Cycle 1 findings arose:
- the ways the nurses used a range of LPs in practice was indistinguishable to them from their parent-education practice
- the nurses had difficulty articulating in any consistent professional language the ways they used a range of LPs in practice, despite being seen to do so in the observations
- the nurses believed their practice was guided by intuition − they “knew what to do” to help parents to learn and knew “what worked in practice”.
Two methods of data collection were important in Cycle 1. Parents’ accounts of important learning experiences reflected LPs the nurses used to help their learning. The observations of nurses’ practice also provided evidence of they used LPs in parent-education practice. Yet they struggled to describe, in any consistent and professional language, their perceptions and ways of using of LPs. Despite these struggles, the participants’ inconsistent terms, as shown in Table 6 under the respective themes, are not dissimilar to the adult and cognitive LPs, shown in Table 1, in the introduction of this paper. However, the nurses were not consciously aware of connections between using LPs, the learning process and their practice.
 |
Table 6 The Learning Principles Used by Nurses as Linked to the Themes |
The participating nurses had a lack of conscious awareness of their parent-education skills surrounding LPs, similar to numerous other parent-education practice research exploring parents learning needs, psychosocial barriers, nurses’ attitudes, beliefs and practices in parent-education.49–54 These studies concluded that a practice-theory gap existed, including Ghorbani et al53 where guidance on using LPs was asked for, but no solutions were forthcoming. Our findings pose new possibilities about those researchers’ theory/practice gap in nurses’ parent-education practice; the nurses in our study were factoring in features of the humanistic learning theories, although subconsciously.55 Both nurses’ and parents’ data showed the nurses recognized that learning integrated people’s life-long psychological and emotional experiences, as well as building their knowledge and skills. Positive, non-judgemental attitudes situated in the parents’ “world”, creating safe learning spaces, despite vulnerabilities and helping parents make choices, were essential for parents to feel ready and motivated to learn. These features also represent key LPs.5,7–9 These practice attributes represent evidence of nurses using LPs and aspects of learning theories in practice. They just struggled to put what they “did” into words and make conscious connections between using LPs and parent-education practice.5,7–9
These findings also demonstrate that participating nurses were addressing the important features of “interactive health literacy”, albeit unknowingly.10,55,56 A growing body of health literacy research recognizes that nurses must move beyond considering health literacy as easier written and visual materials (termed “functional health literacy”). Nurses must be cognizant that “interactional health literacy” involves them assisting learners to encode the information, link it to what they know, make meaningful connections, and then retrieve and use knowledge confidently when needed. Behavior changes can also result.10,55,56 Increasingly, researchers are recognizing the importance of people transforming information into knowledge they can use by using cognition, as well as behavior changes.56 We argue that these features align with cognitive LPs, although the term cognitive LPs seems not to be linked to health literacy publications.7,10,55,56 Health literacy researchers also recognize that those psycho-socio-cultural learning capabilities and humanistic learning theories that create safe, trusting learning environments, as mentioned above, are essential aspects for people to achieve health literacy.7,10,55,56 Our findings support these earlier findings, as the nurses actively engaging parents to connect to what they knew already, building on that knowledge with new information, explanations, demonstrations, and practicing of skills, as they integrated a range of LPs. Wolf et al10 proposed that nurses overlooked the links between the psychosocial aspects of patient/parent education and the need to help patients/parents to think (use cognition) and reason. Our findings suggest an alternative possibility. Rather than “overlooking” the psychosocial aspects of parent-education, the participating nurses were unable to consciously recognize their skills in using LPs, link them to their practice or communicate them to others. Many of the LPs used but unrecognized by the nurses align with the features of functional health literacy, suggesting that future research could explore such connections more deeply.10,55,56
The participating nurses’ beliefs that their use of LPs was “intuitive” or “automatic” and hard to talk about is likely due to LPs being invisible, subjective, non-procedural aspects of their practice.3,8,57 These findings resonate with an important body of nursing research − experienced nurses with proficient practice skills, but who struggled to describe to novice nurses what they did skillfully and automatically in practice, were shown to be using deep background knowledge.24–26 The nurses in our study also seemed to be using deep background knowledge and understanding, rather than automatic behaviors, but they were unable to see connections between their deep knowledge and their practice of using LPs.26
Our study findings also support other research findings, showing nurses’ struggles to describe the ways they use subjective (non-technical), “invisible” aspects of their practice.57–59 Peddle et al57 found subjective attributes of HPs’ practice attracted limited commentary in the national regulatory standards governing HPs’ practice in Australia, in contrast to the easily documented clinical procedures (technical skills). A French study found that the 18 nurses observed, then interviewed about their nursing practices in Therapeutic Patient Education (TPE), had similar difficulties in communicating subjective aspects of their patient-education practice.58 Authors attributed discrepancies between the nurses’ descriptions and their observations of nurses’ actions, to the lack of a common language available to nurses to convey what they “knew” they did in TPE practice. Authors termed this a “theory/practice gap”. The current study results are also similar to an earlier USA study which uncovered that nurses struggled to comprehend and articulate the “invisible” interpersonal care they performed.59 We propose that the lack of nurses’ conscious awareness about using the subjective LPs as discussed earlier, along with no standardized professional language for communicating LPs, contributes to few explicit descriptions of the role of LPs being documented in the healthcare literature.3,6,7,57–59
The nurses identified a number of challenges to helping parents to learn and using LPs, which were captured within the learning environment theme. The key organizational constraints on the time allowed for parent-education and review appointments, while parents wanted and nurses needed more time, impacted parents’ learning experiences and nurses’ practice. Time constraints in parent-education appointments are not a new problem.1,6,7,49,50,54 Interestingly, Petre et al1 who characterized HPs’ educative attitudes in another TPE research study, proposed that greater professional awareness of the learning process may enable HPs to use education facilitation time more effectively. Only further research can determine whether the nurses in the current study could become “more efficient” with time, if they developed conscious awareness of how they used LPs in practice.
The participating nurses knew of no formal PD opportunities to evaluate and build their parent-education knowledge and skills on implementing LPs. Therefore, it was unsurprising that the nurses used subjective evaluation of their parent-education practice skills (eg visual cues, parents’ verbal feedback or satisfaction surveys). Other research studies have reported nurses were evaluating their parent-education effectiveness through observing patients’/parents’ body language or using patient/parent satisfaction measures.49–52 These researchers argued, like the nurses in the current study, that incomplete PD opportunities contributed to a lack of professional guidance for nurses on ways of formally evaluating the effectiveness of parents’ learning.49–52 It is unclear how to interpret and document successful learning, while accounting for individual diversity, people’s feelings and consistent interpretations of body language. Unlike knowledge, which can be measured objectively, learning is hard to measure.60 However, a common view of the current study’s participants was that cues demonstrated by parents could, informally, show a parent did comprehend something nurses explained to them, supporting other parent-education study findings.51 We argue that while the use of LPs in practice has no consistent professional language for documentation, it will be difficult to create evaluation tools to assess parents’ learning within nurses’ parent-education practice.
Documenting parent-education with tick-boxes, as an organizational requirement, created concerns for participants. The nurses’ concerns resonate with UK researchers, who argued that tick-boxes could lead to other HPs’ erroneous assumptions of successful learning within parent-education.61,62 Nurses in the current study emphasized that ticks could not reflect the range of LPs used, whether parents turned the information provided into knowledge or parents’ comprehension of what they needed to know. Parents in our study further supported the nurses’ concerns, especially as parents suggested that tick-box documentation impacted negatively on their learning experiences. A greater concern was that tick boxes for documenting parent-education did not help nurses to develop a professional language on how they perceived and used LPs in practice.
We propose that these experienced nurses’ lack of awareness of their use of LPs and attributing LPs use to “intuition” resulted from their knowledge becoming tacit over their years of practice.24–26,63 Tacit knowledge is sub-conscious, deep-seated knowledge, embedded within a professional understanding.63 Tacit knowledge drives an individual’s behavior, but HPs are commonly challenged to explain to others “what it is” and “how you know it”, despite the knowledge being essential to clinical practice.63–65 We propose that tacit knowledge informing the participating nurses’ learning facilitation capabilities may be why their descriptions of LPs were subsumed within parent-education strategies, and seemingly unconnected to their use of LPs. This created an extra, but unsaid, barrier to the nurses communicating how they used LPs. A way needed to be found to help them make the connections. These findings created a hurdle to completing Cycle 1 of the research, and to the overall action research study.20
The original research study plan was for the collation of the anticipated explicit descriptions of LPs into a summary. This would be sent to participants, as a member-checking process, to confirm accuracy and trustworthiness of the data analysis.40 Participants could contact the researcher to discuss any points they disagreed with. Participants would then Act, in line with Stringer’s model, by reflecting on and drafting their ideas on ways to collaboratively build a resource for communicating LPs with other participants in the Cycle 2 focus groups.20,26 However, the unexpected findings of Cycle 1 created an urgent need to find ways to help the nurses to meaningfully connect with the LPs they were seen using in parent-education practice, that were tacit knowledge. Deeper reflection by the nurses was necessary.57,63
Using Metacognition to Overcome the Hurdle to ACT
The participating nurses needed help to move past accepting their practice was due to intuition,25 having evolved heuristically over years of parent-education practice.66 The nurses also needed help to gain a clearer understanding that many terms within their interview comments were LPs, but the terms were not in any concrete or deliverable form that was recognizable to the nurses themselves. A way forward for nurses to recognize their terms were key LPs, was formulated through deeper reflection – using metacognition.63–65
Deep reflection on practice is a required nursing skill, embedded in nurses’ ongoing learning and professional development, to continuously improve practice.57 A solution to this problem lay in the educational psychology literature – encouraging the nurses to use metacognition to stimulate them to deliberately think, connect with their tacit knowledge and start to link the LPs they were observed using and that parents said were important to their learning experiences.63,64,67–69
This action of metacognition was necessary to help the nurses discover ways to articulate how they used LPs, connecting what they did and why it worked.68 In undergraduate nursing, researchers stimulated third year nursing students to become aware of their clinical reasoning and decision-making skills, that had developed throughout their nursing program, but were hard to “see, describe and recall”.70 The third year students were required to explain and demonstrate to first year students their invisible nursing skills of clinical reasoning and decision-making. This approach stimulated the third year nurses to use cognition and metacognition (thinking about their thinking) to connect with their inner knowledge.70
Prompting the deliberate action of the study’s participating nurses to use metacognition (the brain taking “executive” control of the thought processes), created an opportunity for the current study nurses to actively draw out their buried thoughts and descriptions from their tacit knowledge. They could discover ways to connect the concept of LPs to what they “did”, and start to recognize why their ideas and actions led to success in their parent-education practice.68,70 By using metacognition, the nurses could potentially conceptualize, document any forthcoming ideas and then consider ways to articulate their use of LPs, ready for the Cycle 2 focus group discussions.26,71
A way to stimulate the nurses to use metacognition68–70 to connect with their tacit knowledge and start to consciously link LPs to their practice was created through the Cycle 1 data analysis member-checking summary, usually used for study rigor.72 The summary sent to participants served two purposes. Firstly for rigor, participants were asked to scrutinize the summary of their interview data analysis, reporting any discrepancies to DT. Secondly, as nurses scrutinized the summary, they were encouraged to reflect deeply on the comments to see whether reading the summary stimulated and “unlocked” knowledge about their “automatic” use of LPs developed from their years of experience. Using metacognitive or “inner” thinking created a change process within nurses’ own thinking and their assumptions, becoming the ACT of Cycle 1 (Figure 3).20,68–70 Likewise, parents were asked to think deeply about their learning experiences with a nurse, when checking the summary, with a particular emphasis on identifying attributes optimizing their learning process. It was hoped that both nurses and parents would record any ideas revealed and bring them to their focus group discussion in the next study cycle, to share, communicate and build on the ideas with other participants.71,73 The success of this strategy in unlocking participants’ tacit knowledge about LP use is further described in the PhD thesis.74
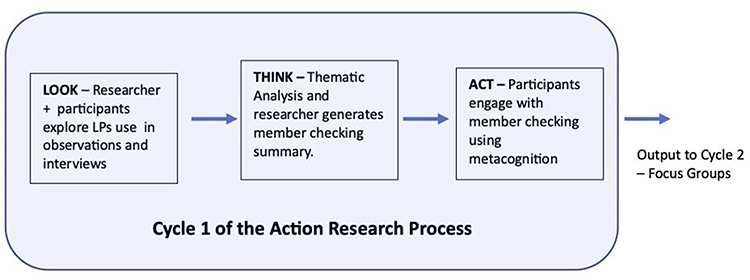 |
Figure 3 The systems approach showing participants’ ACT of cycle 1. |
Limitations and Strengths
The results of the participant sample recruited from one organization may not represent voices of PNs, MCaFHNs and parents in other sections of the organization or external healthcare organizations.46 Excluding people needing interpreter services from the study may mean findings are not representative of diverse populations of health consumers.46 Insider status can create unconscious biases of researchers. DT, as an insider, nurse educator and researcher, as well as having unconscious bias, also had the potential to mitigate changes in participants’ behaviors when observed, as well as influencing participants’ responses and actions during data collection and analysis.45 However, reflexivity by journaling and the research team discussions helped reduce researcher assumptions and bias.42,43,45 Although we aimed to stimulate nurses and parents to use metacognition for deep reflection on the member-checking summary and to record any ideas they drew upon, all participants may not have engaged with the process, potentially limiting ideas brought to the next cycle of the overall research study.42
Strengths, as outlined in the rigor section, include using two methods of data collection and representing participants’ perceptions in their social world.42,46 Observing parents’ learning experiences as well as nurses’ practice, interviewing parents and nurses helped confirm LPs links to nurses’ practice and participants’ experiences. Scrutiny of data analysis by the research team at multiple timepoints was also a study strength.35,46
Practice Implications and Future Directions
Cycle 1 findings have potential implications for nursing practice, as the descriptions uncovered can help nurses to gain awareness of the ways LPs, as subjective features of nurses’ parent-education practice, are used within a learning process. For example, from these research findings nurses can start to see the ways that the adult LPs are implemented as LPs, and how they impact upon parents’ learning experiences. Nurses could recognize if they are already implementing LPs into practice as non-technical nursing skills, but were not consciously aware of these aspects of the parent-education practice.1,57,70 To date, ways of using adult LPs have rarely been explained in the health literature.3,6 Helping nurses to see the ways LPs are used has potential to stimulate further dialogue between nurses to build a bigger picture of the ways LPs are used in practice, which may have value for parents caring for children with long-term conditions.12–15,70 Using metacognition to help nurses connect with what they believe is their “intuition” about their parent education practice has potential to help nurses to recognize and become consciously aware of their deeper inner knowledge.25,67 Nurses may then be able to start dialogues with other nurses, to put into words, describe and even document what they have assumed are automatic aspects of their parent-education practice, built on their years of experience.57,74
Conclusion
Cycle 1 of this research study makes several important contributions to the body of knowledge in nursing for PFC parent-education practice. We believe this is the first study to explore, describe and explain at greater depth the ways nurses integrate cognitive and adult LPs into practice. The role of LPs as subjective aspects of practice has been revealed. The nurses considered parents’ psycho-socio-cultural learning capabilities within collaborative learning relationships. They used humanistic learning theories, created a safe learning environment, and were actively engaging parents to connect to what they knew already, building on that knowledge with new information, explanations, demonstrations, and practicing of skills. Parents in this study concurred that these were LPs that were important to their developing of confidence and capability to create solutions to care for their children’s health needs. Deeper learning insights have been revealed about learning with parent-education practice − the nurses encouraged parents to think, use processes of reasoning and problem-solving in their learning journey.3,55 This study is the first step in helping nurses and parents to see why an awareness of cognitive LPs and their role in the learning process within parent-education must extend beyond the long-accepted nursing praxis of stating Knowles’ six core adult LPs alone.3,5,6
The study has also highlighted that tacit knowledge, rather than nurses’ intuition and automatic behaviors underlies their use of LPs and parent-education practice. Furthermore, the findings show these nurses, who lacked a common professional language to describe how people learn, were initially unable to consciously connect the LPs they were seen using in the observations to their practice. Once prompted by the novel idea of stimulating them to use metacognition, they unlocked what was their tacit knowledge, making connections between LPs and their practice. Using metacognition and deep reflection has promise for helping nurses understand better and to communicate how they use LPs as subjective (non-technical) nursing practice skills. Using LPs in parent-education practice is not “automatic” or intuitive. It is built on deeper knowledge and an awareness that LPs are the part of nursing practice that enable healthcare information to be transformed into knowledge that can be used meaningfully and adapted when necessary. Nursing is long overdue in finding a way to consistently describe and explain the ways nurses use cognitive and adult LPs in parent-education practice, and for nurses to make connections between the ways LPs when used, support parents’ learning needs and preferences. Nurses’ supportive practice builds parents’ knowledge, confidence and capability within a learning process when LPs are used. Patients/parents also need to see similar connections between their parent-education experiences and how LPs help them develop the skills to become concordant with the healthcare recommendations needed to optimize and meet their children’s healthcare needs and preferences.
Data Sharing Statement
Access to the research data from this project may be discussed with the lead and corresponding author, Deryn L. Thompson. Data management has adhered to appropriate ethical approvals and requirements.
Acknowledgments
We wish to acknowledge the participants who gave their valuable time to participate in the study and to Donna Hughes-Barton for manuscript preparation help.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This paper received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Deryn L Thompson reports personal fees from Ego Pharmaceuticals, personal fees from Loreal Pharmaceuticals, personal fees from Eczema support Australia, personal fees from Coalition of National Nursing and Midwifery Organisations of Australia, outside the submitted work. All five authors report no other conflicts of interest or financial interests in this work.
References
1. Petre B, Gagnayre R, Andrade VD, Ziegler O, Guillaume M. From therapeutic patient education principles to educative attitude: the perceptions of health care professionals – a pragmatic approach for defining competencies and resources. Patient Prefer Adherence. 2017;11:603–617. doi:10.2147/PPA.S121892
2. Delaney L. Patient-centred care as an approach to improving health care in Australia. Collegian. 2018;25(1):119–123. doi:10.1016/j.colegn.2017.02.005
3. Thompson D, May E, Leach M, Smith C, Fereday J. The invisible nature of learning: patient education in nursing. Collegian. 2021;28(3):341–345. doi:10.1016/j.colegn.2020.08.002
4. Draganov P, Andrade Carvalho A, Neves V, Sanna M. Andragogy in nursing: a literature review. Investig Educ Enferm. 2013;31(1):86–94. doi:10.17533/udea.iee.10782
5. Knowles MF, Holton ES, Swanson RA. The Adult Learner: The Definitive Classic in Adult Education and Human Resource Development.
6. Thompson D, Leach M, Smith C, Fereday J, May E. How nurses and other health professionals use learning principles in parent-education practice: a scoping review of the literature. Heliyon. 2020;6(3):1–24. doi:10.1016/j.heliyon.2020.e03564
7. Bastable S, Gramet P. Overview of education in health care. In: Bastable S, Sopczyk D, Gramet P, Jacobs K, Braungart M, editors. Health Professional as Educator : Principles of Teaching and Learning.
8. Gagne R. The Conditions of Learning and Theory of Instruction.
9. Gagne R, Wager W, Golas K, Keller J. Principles of Instructional Design.
10. Wolf M, Wilson E, Rapp D, et al. Literacy and learning in health care. Pediatrics. 2009;124(Supplement 3):S275–S281. doi:10.1542/peds.2009-1162C
11. Thompson D, Thompson M. Knowledge, instruction and behavioural change: building a framework for effective eczema education in clinical practice. J Adv Nurs. 2014;70(11):2483–2494. doi:10.1111/jan.12439
12. Smith J, Cheater FM, Bekker HL. Parents’ experiences of living with a child with a long-term condition: a rapid structured review of the literature. Health Expect. 2015;18(4):452–474. doi:10.1111/hex.12040
13. Smith J, Kendal S. Parents’ and health professionals’ views of collaboration in the management of childhood long-term conditions. J Pediatr Nurs. 2018;43:36–44. doi:10.1016/j.pedn.2018.08.011
14. Nightingale R, Friedl S, Swallow V. Parents’ learning needs and preferences when sharing management of their child’s long-term/chronic condition: a systematic review. Patient Educ Couns. 2015;98(11):1329–1338. doi:10.1016/j.pec.2015.05.002
15. Nightingale R, Wirz L, Cook W, Swallow V. Collaborating with parents of children with chronic conditions and professionals to design, develop and pre-pilot PLAnT (the Parent Learning Needs and Preferences Assessment Tool). J Pediatr Nurs. 2017;35:90–97. doi:10.1016/j.pec.2015.05.002
16. Kivunja C, Kuyini AB. Understanding and applying research paradigms in educational contexts. Int J High Educ. 2017;6(5). doi:10.5430/ijhe.v6n5p26
17. Denzin N, Lincoln Y. Introduction: the discipline and practice of qualitative research. In: Denzin N, Lincoln Y, editors. The Sage Handbook of Qualitative Research.
18. Patton M. Qualitative Evaluation and Research Methods.
19. Thomas A, Menon A, Boruff J, Rodriguez A-M, Ahmed S. Applications of social constructivist learning theories in knowledge translation for healthcare professionals: a scoping review. Implement Sci. 2014;9(1):54. doi:10.1186/1748-5908-9-54
20. Stringer ET. Action Research. Thousand Oaks (CA): SAGE Publications Inc; 2007.
21. Manfra M. Action research: exploring the theoretical divide between practical and critical approaches. J Curric Instr. 2009;3(1):32–46.
22. Gaventa J, Cornwall A. Challenging the boundaries of the possible: participation, knowledge and power. IDS Bull. 2006;37(6):122–128. doi:10.1111/j.1759-5436.2006.tb00329.x
23. Reason P, Bradbury H. Inquiry and participation in research of a world worthy of human inspiration. In: Reason P, Bradbury H, editors. The Handbook of Action Research. London: SAGE Publications Ltd; 2006:1–14.
24. Benner P. From Novice to Expert: Excellence and Power in Clinical Nursing Practice. Menlo Park (CA): Addison-Wesley; 1984.
25. Benner P. Clinical Wisdom and Interventions in Acute and Critical Care a Thinking-in-Action Approach.
26. Herbig B, Büssing A, Ewert T. The role of tacit knowledge in the work context of nursing. J Adv Nurs. 2001;34(5):687–695. doi:10.1046/j.1365-2648.2001.01798.x
27. National Health & Medical Research Council. Australian code for the responsible conduct of research. Canberra; 2007.
28. Jackson R, Baird W, Davis-Reynolds L, Smith C, Blackburn S, Allsebrook J. Qualitative analysis of parents’ information needs and psychosocial experiences when supporting children with health care needs. Health Info Libr J. 2007;25(1):31–37. doi:10.1111/j.1471-1842.2007.00736.x
29. Kelo M, Eriksson E, Eriksson I. Perceptions of patient education during hospital visit – described by school-age children with a chronic illness and their parents. Scand J Caring Sci. 2013a;27(4):894–904. doi:10.1111/scs.12001
30. Kelo M, Martikainen M, Eriksson E. Patient education of children and their families: nurses’ experiences. Pediatr Nurs. 2013b;39(2):71–79.
31. Kruske S, Barclay LM. Child health and paediatrics: more differences than similarities. Neonatal Paediatr Child Health Nurs. 2006;9(20):20–24.
32. Fraser S, Grant J, Mannix T. Maternal child and family health nurses: delivering a unique nursing speciality. Matern Child Health J. 2016;20(12):2557–2564. doi:10.1007/s10995-016-2081-2
33. McNaughton Nicholls C, Mills L, Kotecha M. Observation. In: Ritchie J, Lewis J, McNaughton Nicholls C, Ormston R, editors. Qualitative Research Practice.
34. Lewis J, McNaughton Nicholls C. Design issues. In: Ritchie J, Lewis J, McNaughton Nicholls C, Ormston R, editors. Qualitative Research Practice.
35. Guba E, Lincoln Y. Effective Evaluation: Improving the Usefulness of Evaluation Results Through Responsive and Naturalistic Approaches. San Francisco: Jossey-Bass; 1981.
36. Kripalani S, Bengtzen R, Henderson L, Jacobson T. Clinical research in low-literacy populations: using teach-back to assess comprehension of informed consent and privacy information. IRB. 2008;30(2):13–19.
37. QSR International. NVivo 11. Burlington (MA); 2017. (in Cycle 1 analysis stage of study). Available from: https://www.qsrinternational.com/nvivo-qualitative-data-analysis-software/home.
38. Halcomb EJ, Davidson P. Is verbatim transcription of interview data always necessary? Appl Nurs Res. 2006;19(1):38–42. doi:10.1016/j.apnr.2005.06.001
39. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
40. Braun V, Clarke V. Successful Qualitative Research: A Practical Guide for Beginners. London: SAGE Publications Ltd; 2013.
41. Bazeley P, Jackson K. Qualitative Data Analysis with Nvivo. London: SAGE Publications Ltd; 2013.
42. Shenton A. Strategies for ensuring trustworthiness in qualitative research projects. Educ Inf. 2004;22(2):63–75. doi:10.3233/EFI-2004-22201
43. Denzin N. The Research Act: A Theoretical Introduction to Sociological Methods.
44. Polit D, Beck C. Nursing Research Generating and Assessing Evidence for Nursing Practice.
45. Rowe W. Positionality. In: Coghlan D, Brydon-Miller M, editors. The SAGE Encyclopedia of Action Research. Thousand Oaks (CA): SAGE Publications Inc; 2014:627–628.
46. Robertson J. The three Rs of action research methodology: reciprocity, reflexivity and reflection-on-reality. Educ Action Res. 2000;8(2):307–326. doi:10.1080/09650790000200124
47. Australian Commission on Safety and Quality in Health Care. National Safety and Quality Health Service Standards. Sydney; 2017.
48. Seale B. Patients as Partners: Building Collaborative Relationships Among Professionals, Patients, Carers and Communities. The Kings Fund; 2016.
49. Lahl B, Modic B, Siedlecki B. Perceived knowledge and self-confidence of pediatric nurses as patient educators’. Clin Nurse Spec. 2013;27(4):188–193. doi:10.1097/NUR.0b013e3182955703
50. Kodjebacheva G, Sabo T, Xiong J. Interventions to improve child-parent-medical provider communication: a systematic review. Soc Sci Med. 2016;166:120–127. doi:10.1016/j.socscimed.2016.08.003
51. Gilmer C, Buchan J, Letourneau N, et al. Parent education interventions designed to support the transition to parenthood: a realist review. Int J Nurs Stud. 2016;59:118–133. doi:10.1016/j.ijnurstu.2016.03.015
52. Kääriäinen M, Kyngäs H. The quality of patient education evaluated by the health personnel: the quality of patient education. Scand J Caring Sci. 2010;24(3):548–556. doi:10.1111/j.1471-6712.2009.00747.x
53. Ghorbani R, Soleimani M, Zeinali M-R, Davaji M. Iranian nurses and nursing students’ attitudes on barriers and facilitators to patient education: a survey study. Nurse Educ Pract. 2014;14(5):551–556. doi:10.1016/j.nepr.2014.06.003
54. Livne Y, Peterfreund I, Sheps J. Barriers to patient education and their relationship to nurses’ perceptions of patient education climate. Clin Nurs Stud. 2017;5(4):65–72. doi:10.5430/cns.v5n4p65
55. Braungart M, Braungart R, Gramet P. Applying learning theories to healthcare practice. In: Bastable SB, Sopczyk D, Gramet P, Jacobs K, Braungart M, editors. Health Professional as Educator : Principles of Teaching and Learning.
56. Nutbeam D, Lloyd JE. Understanding and responding to health literacy as a social determinant of health. Annu Rev Public Health. 2021;42(1):159–173. doi:10.1146/annurev-publhealth-090419-102529
57. Peddle M, Bearman M, Radomski N, Mckenna L, Nestel D. What non-technical skills competencies are addressed by Australian standards documents for health professionals who work in secondary and tertiary clinical settings? A qualitative comparative analysis. BMJ Open. 2018;8(8):e020799–e020799. doi:10.1136/bmjopen-2017-020799
58. Vigil-Ripoche M. D’exécuter un soin à penser le soin” ou de la difficulté à “mettre en mots” la pratique infirmière [From giving care to thinking care or the difficulty of putting nursing practice “into words”]. Rech Soins Infirm. 2006;85(2):65–76. French. PMID: 16898050. doi:10.3917/rsi.085.0065
59. Laduke S. NIC puts nursing into words. Nurs Manage. 2000;31(20):43–44. doi:10.1097/00006247-200002000-00028
60. Kesänen J, Leino-Kilpi H, Arifulla D, Siekkinen M, Valkeapää K. Knowledge tests in patient education: a systematic review. Nurs Health Sci. 2014;16(2):262–273. doi:10.1111/nhs.12097
61. Grainger A. Shining a light on good practice. Nurs Manage. 2010;17(4):30–33. doi:10.7748/nm2010.07.17.4.30.c7847
62. Cleland J, Reeve J, Rosenthal J, Johnston P. Resisting the tick box culture: refocusing medical education and training. Br J Gen Pract. 2014;64(625):422–423. doi:10.3399/bjgp14X681169
63. D’Eredita M, Barreto C. How does tacit knowledge proliferate? An episode-based perspective. Organ Stud. 2006;27(12):1821–1841. doi:10.1177/0170840606067666
64. ten Cate O, Snell L, Mann K, Vermunt J. Orienting teaching toward the learning process. Acad Med. 2004;79(3):219–228. doi:10.1097/00001888-200403000-00005
65. Kothari A, Rudman D, Dobbins M, Rouse M, Sibbald S, Edwards N. The use of tacit and explicit knowledge in public health: a qualitative study. Implement Sci. 2012;7(1):20–32. doi:10.1186/1748-5908-7-20
66. Delany C, Golding C. Teaching clinical reasoning by making thinking visible: an action research project with allied health clinical educators. BMC Med Educ. 2014;14(1):1–10. doi:10.1186/1472-6920-14-20
67. Lake S, McInnes R. Exploring cognitive skill development in midwifery education. Nurse Educ Pract. 2012;12(5):264–268. doi:10.1016/j.nepr.2012.04.015
68. Kosior K, Wall T, Ferrero S. The role of metacognition in teaching clinical reasoning: theory to practice. Educ Health Prof. 2019;2(2):108–114. doi:10.4103/EHP.EHP_14_19
69. Tanner K. Promoting student metacognition. CBE Life Sci Educ. 2012;11(2):113–120. doi:10.1187/cbe.12-03-0033
70. Irvine S, Williams B, McKenna L. Near-peer teaching in undergraduate nurse education: an integrative review. Nurse Educ Today. 2018;70:60–68. doi:10.1016/j.nedt.2018.08.009
71. Lambert S, Loiselle C. Combining individual interviews and focus groups to enhance data richness. J Adv Nurs. 2008;62(2):228–237. doi:10.1111/j.1365-2648.2007.04559.x
72. Baillie L. Promoting and evaluating scientific rigour in qualitative research. Nurs Stand. 2015;29(46):36–42. doi:10.7748/ns.29.46.36.e8830
73. Tausch A, Menold N. Methodological aspects of focus groups in health research. Glob Qual Nurs Res. 2016;3:1–12. doi:10.1177/2333393616630466
74. Thompson DL. ‘I do it Without Knowing It’ Perceptions and Use of Learning Principles in Nurses’ Parent Education Practice : An Action Research Study [PhD thesis (Nursing)]. University of South Australia. UniSA Clinical Health Sciences; 2022.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Improving Nurses’ Knowledge on Sepsis Identification and Management at Mulago National Referral Hospital: A Quasi Experimental Study
Nakiganda C, Atukwatse J, Turyasingura J, Niyonzima V
Nursing: Research and Reviews 2022, 12:169-176
Published Date: 14 September 2022
Doctors’ and Nurses’ Knowledge and Perceived Barriers Regarding Acute Oxygen Therapy in a Tertiary Care Hospital in Nigeria
Desalu OO, Ojuawo OB, Adeoti AO, Oyedepo OO, Aladesanmi AO, Afolayan OJ, Ibraheem RM, Suleiman ZA, Opeyemi CM
Advances in Medical Education and Practice 2022, 13:1535-1545
Published Date: 19 December 2022
The Level of Knowledge Among Nurses Regarding Care of Patients with Hepatic Encephalopathy at Najran Hospitals, Saudi Arabia
Alwesabi SAM, Abdalla YHA, Abdulrahman EE, Osman AMA, Alkhadher MA, Alshameri FA, Hakami MS, Ahmed WA
International Journal of General Medicine 2023, 16:4719-4727
Published Date: 18 October 2023
Nurses’ Knowledge Regarding Incontinence-Associated Dermatitis
Asiri S, Alzahrani NS, Alharbi HF, Ayoub MY
Risk Management and Healthcare Policy 2024, 17:2917-2928
Published Date: 26 November 2024
Knowledge, Attitude, and Practice of Palliative Care Among Physicians and Nurses in Intensive Care Units in Shanghai, China
He X, Cai H, Zhang J, Chen W, Zhu B
Journal of Multidisciplinary Healthcare 2025, 18:2441-2449
Published Date: 1 May 2025