")
Back to Journals » Research and Reviews in Parkinsonism » Volume 4
Applications of yoga in Parkinson's disease: a systematic literature review
Authors Roland K
Received 28 September 2013
Accepted for publication 11 November 2013
Published 9 January 2014 Volume 2014:4 Pages 1—8
DOI https://doi.org/10.2147/JPRLS.S40800
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Kaitlyn P Roland
Centre on Aging, University of Victoria, Victoria, BC, Canada
Background: Yoga may be applicable to persons with Parkinson's disease (PD). The adaptability of yoga to suit varying abilities is of significance to the PD population with its progressive mobility problems. The additional psychosocial benefits of yoga are important to the quality of life. This systematic review presents scientific evidence pertaining to the impact of yoga on physical function and psychological well-being in PD.
Methods: A literature search was conducted for randomized controlled trials (n=1), pretest–post-test design (n=3), and case studies (n=3) with the terms “yoga” and “Parkinson disease”. The study quality was assessed with a modified version of the Downs and Black Checklist and ranged from 8 to 16. The study outcomes included functional mobility (n=6), flexibility (n=4), balance (n=4), strength (n=4), depression (n=2), sleep (n=1), and quality of life (n=1).
Results: The preliminary data suggested that yoga resulted in modest improvements in functional mobility, balance, and lower-limb strength in persons with PD. This has implications for gait, postural stability, balance confidence, and functional declines related to inactivity. An improved upper- and lower-body flexibility following yoga in persons with PD is applicable to rigidity, shuffling gait, and flexed posture. The presented evidence also showed positive outcomes for mood and sleep, demonstrating yoga's benefit for self-efficacy and social support.
Conclusion: This review suggests that yoga provided an alternative method for addressing some of the reversible factors that impact motor function in PD, as well as contributing to an improved psychosocial well-being. However, limitations to the design of the studies necessitate further research to validate yoga as a therapy for PD.
Keywords: alternative therapy, adaptable, mobility, mood, quality of life, neurological disorders
Introduction
Parkinson’s disease (PD) is a progressive neurodegenerative disorder, prevalent in 1% of all individuals over the age of 60 years.1 Although considered a multineurotransmitter system disorder, the cardinal PD pathology is damage to the dopamine producing cells in the substantia nigra, which is responsible for coordinating smooth and balanced muscle movement. PD is characterized by tremor, rigidity, slowness of movement (bradykinesia), and postural instability. In addition, persons with PD face neuropsychiatric symptoms (ie, mood, sleep, psychosis, impulse control) as a result of the affected cholinergic, hypocretin, noradrenergic, and serotonergic nondopamine neurons.2 Disease management primarily focuses on pharmacotherapy (ie, dopaminergic replacement) for motor symptoms, although neuropsychiatric symptoms can play a significant role in a person’s health-related quality of life (QoL). Despite major advances in disease management and symptomatic therapy for PD, no treatment is neuroprotective. Over time, the medication loses its effectiveness, and progressing motor complications precipitate functional dependence and impair QoL. Also, the side effects of pharmacotherapy include motor fluctuations, confusion, memory problems, and psychiatric complications.3 Given this, there is a compelling need for alternative therapies to improve function and QoL in persons with PD.
Yoga may represent a particularly promising nonpharmacologic therapy for PD. A recent review on the fitness benefits of yoga for older adults proposed modest improvements in gait, balance, flexibility, lower-body strength, cardiorespiratory response, and body composition.4 The current literature has also demonstrated yoga-related improvements for chronic disease risk factors, disease management, and health-related QoL in older adults.5–11 As such, yoga may offer an alternative therapy that can be adapted to meet the needs of various neurological populations.12,13 The adaptability of yoga to suit individuals of varying abilities is of great significance to this population with its progressively increasing mobility problems. Yoga programs have been adapted to neurological disorders, such as epilepsy, multiple sclerosis, stroke, and restless leg syndrome. These programs have demonstrated improvements in stress, mood, fatigue, sleep, pain, mobility, problem solving, memory, and seizure control.14–19 The additional psychosocial benefits associated with yoga are also important to disease management and to the QoL in persons with PD, as they are often not addressed with conventional dopaminergic therapy. This paper presents a systematic review of the current scientific literature pertaining to the impact of yoga on physical function (ie, mobility, strength, flexibility) and psychological well-being (ie, mood, sleep, QoL). The potential application of yoga to PD will be defined.
Methods
Search strategy
To examine the effects of yoga for persons with PD, the electronic databases Science Direct, Medline/PubMed, CINAHL (EBSCO), PEDro, and PsychInfo were systematically searched for randomized controlled trials (RCTs), pretest–post-test design, and case studies with the terms “yoga” and “Parkinson disease” (June–July 2013).
The review was restricted to studies published in English with human subjects. Full-text articles and published abstracts were included. After the original search, titles were screened and duplicates were removed. The inclusion criteria was kept broad: 1) a hatha yoga intervention administered to a sample diagnosed with PD; and 2) any outcome measures related to physical (ie, strength, balance, gait) and psychosocial (ie, depression, QoL) well-being were included. The reviewer, who was not blinded to the purpose of the evaluation, screened the titles and appraised the abstracts to ensure they met all the inclusion criteria. An external secondary reviewer verified the search strategy and results.
Data extraction and quality assessment
Data was extracted, and a quality analysis was completed on the studies included in the systematic review. The study quality was assessed and rated according to a modified version of the Downs and Black Checklist, because of its inclusion of both randomized and nonrandomized controlled trials.20 Out of a total possible score of 20 on the modified Downs and Black Checklist, a score of 16 or better indicated a good study quality, a score from 11–15 suggested moderate quality, and a score of lower than 10 indicated poor quality. An overview of the existing evidence on the benefits of a yoga program for PD is presented, as well as potential mechanisms/applications of yoga for PD.
Results
Current evidence: yoga for Parkinson’s
The search results revealed a total of 214 articles (Figure 1). After the duplicates were removed, the titles were screened for evidence of a yoga intervention in persons with PD. The available abstracts for 43 articles were then reviewed, and – based on the inclusion criteria – a total of 18 studies were included for a full-text review. Following the full-text review, seven yoga studies specific to PD remained for data extraction and quality analysis. The reasons for exclusion at the full-text review stage included: a review paper (n=2); no yoga but other complementary or alternative therapies (n=6); or no measurable outcome/intervention (ie, only a personal report of a yoga program) (n=3). A summary of the characteristics of the seven studies is provided in Table 1. Of the studies included in this review, one was a RCT comparing yoga to a waitlist control, three were one-group pretest–post-test design, and three were case studies. The reported outcomes attributed to a yoga program in persons with PD included functional mobility (n=6; chair stand, gait), range of motion/flexibility (n=4), balance (n=4), strength (n=4), depression (n=2), sleep (n=1), and QoL (n=1). The relevant studies are summarized in the “Study quality” section.
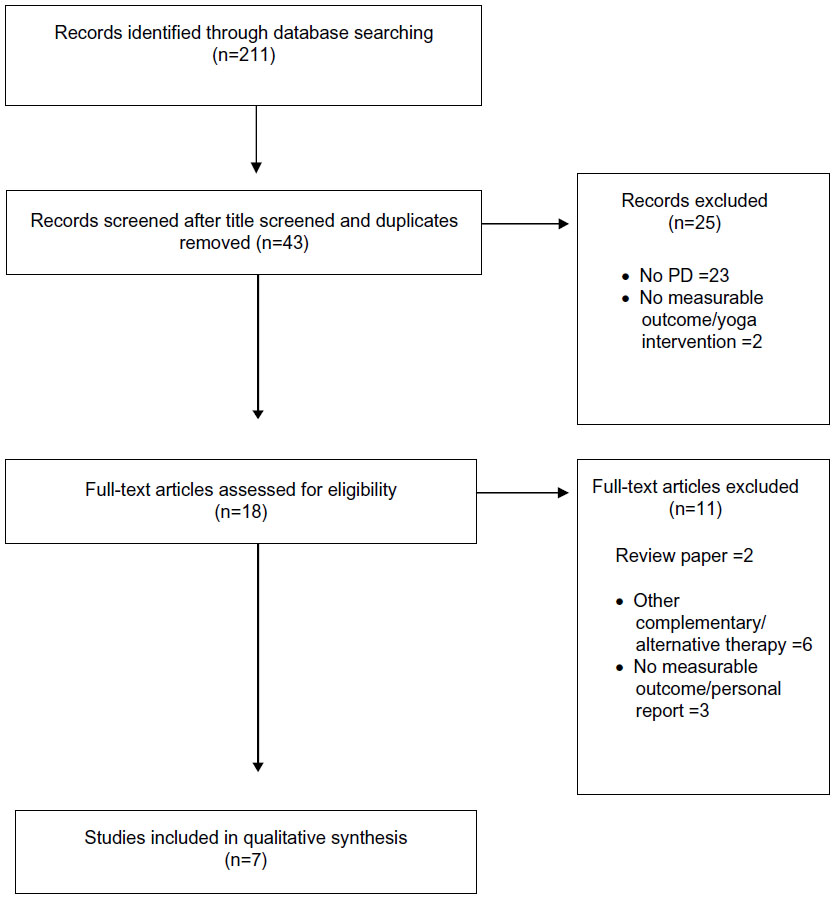 | Figure 1 Flow diagram of included and excluded studies, according to the PRISMA statement. |
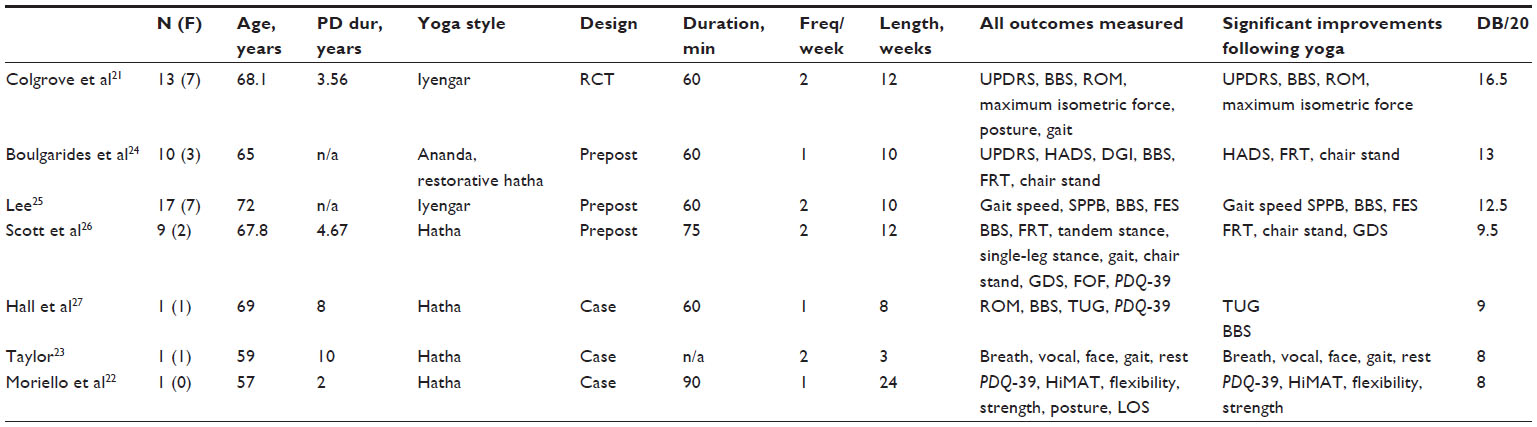 | Table 1 Literature search study characteristics |
Study quality
The study quality ranged between 8 and 16.5.21–23 Common missing information included: characteristics of participants lost to follow-up, reporting probability values, and adverse events. Reasons why study design lacked quality included: not blinded to intervention, not randomized to intervention, and insufficient power to detect statistical significance and/or clinically important events.
Study design: RCT
In the only RCT, 13 adults with PD were randomized to a 60-minute Iyengar yoga program twice a week for 12 weeks or to a waitlist control.21 Iyengar yoga is a specific tradition of hatha yoga developed by Iyengar that emphasizes detail and precision in the postural alignment. Props (ie, belts, cushions) are used to support postures. The study found that the yoga intervention group had improved scores on the motor United Parkinson’s Disease Rating Scale (UPDRS) at the first 6 weeks of intervention and maintained for the remaining 6 weeks, compared to the control (P=0.004). Improvements in the other functional measures of motor performance were demonstrated in a yoga group compared with the control – specifically, the Berg Balance Scale (BBS; P=0.04) and the gait initiation (P=0.039–0.044). Also, the improvements in contributing factors, such as hip strength (P=0.02), and hip, knee, ankle, and shoulder range of motion (P=0.003–0.033) were demonstrated in the yoga group compared to the control.21
Study design: pretest–post-test
Three one-group pretest–post-test yoga interventions were included. First, ten adults with PD participated in a 60-minute weekly hatha yoga intervention for 8 weeks to determine outcomes in functional mobility, flexibility, depression, and anxiety.24 The postintervention measurements demonstrated significant improvements in the Hospital Based Anxiety and Depression Scale (HADS, P=0.002), functional strength (30-second chair stand; P=0.03), and leg flexibility (sit-and-reach test; P=0.02). Second, 17 participants with PD completed a 10-week Iyengar yoga program.25 The program consisted of two 1-hour yoga classes and a daily 30-minute home practice. Postintervention outcome measurements demonstrated improvements in walking speed (P=0.002), Short Physical Performance Battery (SPPB; P=0.006), BBS (P=0.006), and Falls Efficacy Scale (P=0.02). The study suggested improvements in mobility (balance, gait) following yoga in PD.25 Finally, nine adults with PD participated in a twice a week hatha yoga program (75 minutes long) for 12 weeks. Following the intervention, significant improvements were seen in physical variables (chair stand, sit-and-reach test) and depression inventory, according to the Geriatric Depression Scale.26 This yoga intervention proposed improvements in both physical and affective factors relevant to PD.
Study design: case study
Three case studies were reported in the literature. First, a 57-year-old PD male participated in a 6-month program that consisted of 90 minutes of physical therapy and 90 minutes of hatha yoga each week.22 Improvements were seen in QoL (Parkinson’s Disease Questionnaire-39), mobility (High Level Mobility Assessment Tool), hamstring and hip flexor flexibility (5°–20°), and upper- and lower-body strength (20%–463%). Improved mobility and gains in flexibility meant the most to the participant as they enabled greater functional capacity in the workplace; this resulted in an improved QoL. In addition, the participant reported decreased medication dosage following the program, and results were maintained at a 6-month follow-up.22 However, due to the combination of yoga with intense physical therapy, it is difficult to attribute gains specific to the yoga program.
Second, a 59-year-old PD female participated in twice-a-week yoga classes (60-minute visits per week, total 120 minutes per week) for 3 weeks.23 Yoga postures focused on breath, core awareness, pelvic mobility, spine lengthening, twists, and the oral/facial area. Following the intervention, the participant reported increased body awareness, vocal projection, and facial awareness, confidence in gait and endurance, and fewer sleep difficulties.23
Finally, a 69-year-old PD female participated in a weekly (60-minute) 8-week yoga program focused on balance, mobility, and QoL.27 A further 5-week control phase was applied to observe any changes once the intervention was withdrawn. Trends suggested a gradual improvement on a BBS scale (3 points) and a Timed Up and Go test (1-second) at week 8; the QoL remained stable for the duration.27 These small changes make it difficult to determine clinically meaningful change; subtle improvements in functional performance require further investigation.
Discussion
This review presented evidence from seven studies of yoga for persons with PD of high (n=1), moderate (n=2), and low study quality (n=4) that met the inclusion criteria. In regards to PD, the yoga studies lacked quality due to inadequate controls and an insufficient sample size or follow-up measurements. As such, limitations to study designs necessitate further research to validate yoga as a therapy for PD. Preliminary data suggested modest improvements in functional mobility, balance, upper- and lower-limb flexibility, and lower-limb strength. By improving mobility, balance, and lower-extremity function, yoga also reduced the fear of falling and declines in strength and flexibility related to inactivity.25 Upper-body flexibility supported postural stability and improved function during daily living activities (ie, reaching). The presented evidence also showed improvements in nonphysical factors, such as mood24,26 and sleep.26
Potential mechanisms for improvement with yoga in Parkinson’s disease
Functional mobility
The issue of functional mobility has important implications for falls in PD, as sit-to-stand test and a 6 meter gait speed are valid predictors of falls in older people. In this review, improvements in mobility were seen in the UPDRS motor score,21 gait initiation,21 and gait speed.22,25 Slowed movement, or bradykinesia, is thought to most closely reflect underlying striatal dopamine depletion and predominantly impair movement execution. Yoga’s ability to improve gait initiation and speed may address bradykinesia, which affects voluntary and reactive limits of stability.22
This review also reported improvements in sit-to-stand measures in persons with PD following yoga.24,26,27 Specific improvement in the sit-to-stand ability following yoga indicated an improved functional mobility and lower-limb strength.28 Standing yoga poses (ie, chair, warrior II, tree) may be thought of as mobility focused exercises, because they simultaneously target three functionally important muscle groups that prevent the collapse of the center of mass during gait – the hip extensor, the knee extensor, and the ankle plantar flexor. More research into the biomechanical profiles of yoga postures may be used to guide the choice of poses to target the muscle groups important for functional mobility.29
Balance
In this review, three studies reported significant improvements in balance (BBS, Falls Efficacy Scale)21,25,27 and one subjective report of improved balance confidence.23 Balance training is an important component of therapy as 40% of nursing home admissions are preceded by a fall, and persons with PD fall more frequently than other older adults. Improvements in balance confidence that accompany yoga also contributed to a reduced fear of falling in PD. This is important as persons with a fear of falling decrease physical activity participation, leading to further decreases in strength, flexibility, and balance. This vicious cycle places them at a greater risk for additional falls.30
Strength
This review presented improvements in lower-body strength following yoga in persons with PD.21,22 Improved strength is important, as muscle weakness occurs in PD as a result of changes in neural drive, diminished muscle force, movement velocity, and peripheral loss of muscle function.24,26 Increased isokinetic muscular strength is most likely attributed to holding static postures and controlled systematic movement from one posture to the next. Executing specific tasks (ie, different postures) alternates the recruitment of muscle fibers from different motor units, thereby increasing muscle endurance.31 Also, the utilization of more muscle fibers, especially during one-legged balance postures, produces more force per unit of mass; this causes peripheral changes and improved muscular endurance.31 Gains in the lower extremity strength, resulting from yoga, were associated with improved postural stability and gait in PD.21
Flexibility
An improved upper- and lower-body flexibility/range of motion (ROM) was evident from this review of yoga interventions for PD.21,22,24,26 Improved flexibility is important since rigidity is a common clinical manifestation in PD. An increased range of motion is most likely due to the static stretching involved in yoga postures.9,31 Improvements in upper-body flexibility (ie, shoulder, spinal) suggested the benefits of yoga on the forward flexed (stooped) posture in PD. The stooped posture is characteristic of PD and is attributed to the shortened contractile elements of the spinal flexor muscles and lengthening and weakening of the spinal extensors.32 The shoulder and spinal flexibility supports a more upright posture, which improves the functional capacity during daily living activities (ie, reaching for objects on upper shelves). Yoga-related improvements in lower-extremity flexibility, especially the hamstring length and hip mobility demonstrated in persons with PD, are essential for regular stride length and may also translate to improvements in the PD shuffling gait.
Well-being (QoL, sleep, mood)
This review demonstrated positive outcomes for QoL22, sleep,23 and depression24,26 following yoga in PD. Yoga in a class setting offers group support, socialization, sharing a common experience, learning, and builds confidence.33 Thus, in addition to the physical benefits of yoga, socialization and self-efficacy effects are other potential mechanisms for improved QoL in PD.34 Yoga also emphasizes the importance of increased confidence and reduced social avoidance, which is of further significance, as it may indicate greater illness acceptance in PD.33 Yoga may have a calming effect by directly enhancing parasympathetic output, via stimulation of the vagus nerve, and shifting away from autonomic arousal.15,35 By showing changes toward parasympathodominance in dopamine beta-hydroxylase activity,35 yoga may attenuate pain, discomfort, and perceived stress and may promote feelings of well-being by enhancing mood, sleep, and muscle relaxation in PD.
Current evidence: yoga for other neurological conditions
While yoga and other relaxation therapies are often recommended for persons with PD, clinical trials and substantive quality evidence are lacking. However, quality studies that support the overall benefits of yoga in community-dwelling older adults and other neurologic disorders do exist. For example, there is relatively good data suggesting the utility of yoga techniques for other neurological conditions: 1) attention, mobility, speech, and fine motor coordination in persons poststroke;14,36 2) general improvements in fatigue and selective attention in multiple sclerosis;17,37 and 3) sleep quality and mood in restless leg syndrome.15 These are applicable to PD, since fatigue limits daily physical function,38 and attentional aspects of yoga may provide a nonautomatic drive for movement that serves as a compensatory mechanism to avoid the faulty basal ganglia circuitry.21,39
Considerations for program design and future research
People with PD may reduce physical activity participation as a result of symptom progression, age-related frailty, stress, depression, and concurrent medical conditions.40 This puts people at-risk for a reduced range of movement, diminished muscular and aerobic capacity, and decreased QoL. Yoga can be considered an activity that is adaptable to persons with PD who may not be able to participate in strenuous, intensive exercise. Yoga can be modified to address the needs and limitations of older populations with PD. For example, shorter time holding poses can help avoid the onset of rigidity; props can improve alignment; and modified instructions can account for cognitive impairment.41 Rigid torso muscles lead to pulmonary dysfunction in PD; this may benefit from yogic diaphragmatic maximal breathing exercises.21,42 In addition, yoga may be used in conjunction with other training modalities (ie, low-impact aerobics, strength training) to manage symptoms and to maintain independence.43 Knowledge gained from yoga is applied to perform other exercises/daily activities with more conscious thought and awareness to make safer choices and to reduce fall risks and injuries.
Research design
The current evidence suggests that yoga is acceptable to PD populations and persons may benefit; however, until study quality is improved, the discussion of the physiological and pathological benefits of yoga in PD is highly speculative. Long-term implications and dosage (frequency, intensity, timing, type [the FITT principles]) need to be determined. Other research design elements include a sufficient sample size, randomization with a suitable control group, follow-up, adherence, and control for nonspecific factors, such as social effects and attention. Outcome measures need to include not only physical strength, but also mood, cognition, and mental well-being.44 Physical, psychological, and cognitive functions are all of particular interest to the PD population and overall QoL.
Conclusion
This review evaluated the current evidence of yoga as an alternative therapy and symptom management modality in PD. Although this review provided some insight into the benefits of yoga and the application to a PD management program, most of the studies reviewed were only in the initial stages of understanding the clinical and symptomatic benefits of yoga. The evidence suggested modest improvements in physical factors, including functional mobility, balance, flexibility, and lower-limb strength. Specifically, yoga provided an alternative method for addressing some of the reversible factors that impact motor function, such as strength, flexibility, and balance. This review suggested yoga impacts fall-risk factors, including abnormal posture, gait difficulties, poor balance, and lower-body weakness. This is important, since improved physical functioning may also contribute to improved mental well-being and the capacity for independent living. The evidence also presented improvements in depression, sleep, and QoL, following yoga in persons with PD. While there is not enough research to provide strong scientific evidence for the use of yoga in PD, there is no evidence suggesting it is harmful. Yoga offers support with fewer side effects than conventional pharmaceutical treatments and may improve QoL through improved function, which is essential to the successful management of PD.
Acknowledgments
The author thanks Dr Neena L Chappell and Dr Gareth R Jones for their feedback on the review and/or comments on the manuscript.
Disclosure
The author is currently funded by the Canadian Institutes of Health Research (Gender, Work, and Health) (2012–2014) and the Michael Smith Foundation for Health Research (2013–2016) Post-Doctoral Fellowship Awards. The author reports no other conflicts of interest in this work.
References
de Lau LM, Breteler MM. Epidemiology of Parkinson’s disease. Lancet Neurol. 2006;5(6):525–535. | |
Aarsland D, Marsh L, Schrag A. Neuropsychiatric symptoms in Parkinson’s disease. Mov Disord. 2009;24(15):2175–2186. | |
Saint-Cyr JA, Taylor AE, Lang AE. Neuropsychological and psychiatric side effects in the treatment of Parkinson’s disease. Neurology. 1993;43(12 Suppl 6):S47–S52. | |
Roland KP, Jakobi JM, Jones GR. Does yoga engender fitness in older adults? A critical review. J Aging Phys Act. 2011;19(1):62–79. | |
Luskin FM, Newell KA, Griffith M, et al. A review of mind/body therapies in the treatment of musculoskeletal disorders with implications for the elderly. Altern Ther Health Med. 2000;6(2):46–56. | |
Morone NE, Greco CM. Mind-body interventions for chronic pain in older adults: a structured review. Pain Med. 2007;8(4):359–375. | |
Pilkington K, Kirkwood G, Rampes H, Richardson J. Yoga for depression: the research evidence. J Affect Disord. 2005;89(1–3):13–24. | |
Posadzki P, Ernst E, Terry R, Lee MS. Is yoga effective for pain? A systematic review of randomized clinical trials. Complement Ther Med. 2011;19(5):281–287. | |
Raub JA. Psychophysiologic effects of Hatha Yoga on musculoskeletal and cardiopulmonary function: a literature review. J Altern Complement Med. 2002;8(6):797–812. | |
Smith KB, Pukall CF. An evidence-based review of yoga as a complementary intervention for patients with cancer. Psychooncology. 2009;18(5):465–475. | |
Yang K. A review of yoga programs for four leading risk factors of chronic diseases. Evid Based Complement Alternat Med. 2007;4(4): 487–491. | |
Mishra SK, Singh P, Bunch SJ, Zhang R. The therapeutic value of yoga in neurological disorders. Ann Indian Acad Neurol. 2012;15(4): 247–254. | |
Wahbeh H, Elsas SM, Oken BS. Mind-body interventions: applications in neurology. Neurology. 2008;70(24):2321–2328. | |
Bastille JV, Gill-Body KM. A yoga-based exercise program for people with chronic poststroke hemiparesis. Phys Ther. 2004;84(1):33–48. | |
Innes KE, Selfe TK. The Effects of a Gentle Yoga Program on Sleep, Mood, and Blood Pressure in Older Women with Restless Legs Syndrome (RLS): A Preliminary Randomized Controlled Trial. Evid Based Complement Alternat Med. 2012;2012:294058. | |
Lundgren T, Dahl J, Yardi N, Melin L. Acceptance and Commitment Therapy and yoga for drug-refractory epilepsy: a randomized controlled trial. Epilepsy Behav. 2008;13(1):102–108. | |
Oken BS, Kishiyama S, Zajdel D, et al. Randomized controlled trial of yoga and exercise in multiple sclerosis. Neurology. 2004;62(11): 2058–2064. | |
Rajesh B, Jayachandran D, Mohandas G, Radhakrishnan K. A pilot study of a yoga meditation protocol for patients with medically refractory epilepsy. J Altern Complement Med. 2006;12(4):367–371. | |
Senders A, Wahbeh H, Spain R, Shinto L. Mind-body medicine for multiple sclerosis: a systematic review. Autoimmune Dis. 2012;2012: 567324. | |
Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. 1998;52(6):377–384. | |
Colgrove YS, Sharma N, Kluding P, et al. Effect of yoga on motor function in people with Parkinson’s disease: a randomized, controlled pilot study. J Yoga Phys Ther. 2012;2:112. Available from: http://www.inventi.in/Article/hls/64/12.aspx. Accessed July 4, 2013. | |
Moriello G, Denio C, Abraham M, DeFrancesco D, Townsley J. Incorporating yoga into an intense physical therapy program in someone with Parkinson’s disease: A case report. J Bodyw Mov Ther. 2013;17(4): 408–417. | |
Taylor M. Yoga therapeutics in neurological physical therapy: application to a patient with Parkinson’s disease. Journal of Neurologic Physical Therapy. 2001;25(2):55–62. | |
Boulgarides L, Coleman-Salgado B, Barakatt E, Choo D, Williams K, Morales A, et al. Effect of an 8-week adaptive yoga program on mobility, function and outlook in individuals with Parkinson’s disease. Physiotherapy. 2007;93(S1):S258. | |
Lee L. The effect of yoga exercises on balance, lower-extremity function and gait in people with Parkinson’s disease. Arch Physical Med Rehabil. 2006;87(11):E19. Available from: http://www.archives-pmr.org/article/S0003-9993(06)01010-0/fulltext. Accessed on December 6, 2013. | |
Scott M, Masterson M, Elmer L, et al. P2.160 The effects of a yoga program on Parkinson’s disease. Parkinsonism Relat Disord. 2009;15(Suppl 2):S133. | |
Hall E, Verheyden G, Ashburn A. Effect of a yoga programme on an individual with Parkinson’s disease: a single-subject design. Disabil Rehabil. 2011;33(15–16):1483–1489. | |
Tiedemann A, Shimada H, Sherrington C, Murray S, Lord S. The comparative ability of eight functional mobility tests for predicting falls in community-dwelling older people. Age Ageing. 2008;37(4): 430–435. | |
Wang MY, Yu SS, Hashish R, et al. The biomechanical demands of standing yoga poses in seniors: The Yoga empowers seniors study (YESS). BMC Complement Altern Med. 2013;13:8. | |
Schmid AA, Van Puymbroeck M, Koceja DM. Effect of a 12-week yoga intervention on fear of falling and balance in older adults: a pilot study. Arch Phys Med Rehabil. 2010;91(4):576–583. | |
Tran MD, Holly RG, Lashbrook J, Amsterdam EA. Effects of Hatha Yoga Practice on the Health-Related Aspects of Physical Fitness. Prev Cardiol. 2001;4(4):165–170. | |
Schenkman M, Butler RB. A model for multisystem evaluation treatment of individuals with Parkinson’s disease. Phys Ther. 1989;69(11): 932–943. | |
Fitzpatrick L, Simpson J, Smith A. A qualitative analysis of mindfulness-based cognitive therapy (MBCT) in Parkinson’s disease. Psychol Psychother. 2010;83(Pt 2):179–192. | |
Oken BS, Zajdel D, Kishiyama S, et al. Randomized, controlled, six-month trial of yoga in healthy seniors: effects on cognition and quality of life. Altern Ther Health Med. 2006;12(1):40–47. | |
Joseph S, Sridharan K, Patil SK, et al. Study of some physiological and biochemical parameters in subjects undergoing yogic training. Indian J Med Res. 1981;74:120–124. | |
Lynton H, Kligler B, Shiflett S. Yoga in stroke rehabilitation: a systematic review and results of a pilot study. Top Stroke Rehabil. 2007;14(4): 1–8. | |
Velikonja O, Curić K, Ozura A, Jazbec SS. Influence of sports climbing and yoga on spasticity, cognitive function, mood and fatigue in patients with multiple sclerosis. Clin Neurol Neurosurg. 2010;112(7): 597–601. | |
Grace J, Mendelsohn A, Friedman JH. A comparison of fatigue measures in Parkinson’s disease. Parkinsonism Relat Disord. 2007;13(7): 443–445. | |
Rochester L, Nieuwboer A, Baker K, et al. The attentional cost of external rhythmical cues and their impact on gait in Parkinson’s disease: effect of cue modality and task complexity. J Neural Transm. 2007;114(10):1243–1248. | |
Morris ME. Movement disorders in people with Parkinson disease: a model for physical therapy. Phys Ther. 2000;80(6):578–597. | |
Abrantes AM, Friedman JH, Brown RA, et al. Physical activity and neuropsychiatric symptoms of Parkinson disease. J Geriatr Psychiatry Neurol. 2012;25(3):138–145. | |
Sabaté M, González I, Ruperez F, Rodríguez M. Obstructive and restrictive pulmonary dysfunctions in Parkinson’s disease. J Neurol Sci. 1996;138(1–2):114–119. | |
Newell L. Combining Exercise with Yoga Postures, Breathing, and Meditation to Help Manage the Symptoms of Parkinson’s Disease. Int J Yoga Ther. 2005;15(1):81–86. Available from: http://connection.ebscohost.com/c/articles/19197206/combining-exercise-yoga-postures-breathing-meditation-help-manage-symptoms-parkinsons-disease. Accessed December 6, 2013. | |
Wang DS. Feasibility of a Yoga Intervention for Enhancing the Mental Well-Being and Physical Functioning of Older Adults Living in the Community. Act Adapt Aging. 2010;34(2):85–97. Available from: http://www.tandfonline.com/doi/abs/10.1080/01924781003773559. Accessed on December 6, 2013. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.