Back to Journals » Infection and Drug Resistance » Volume 15
Application Value of Metagenomic Next-Generation Sequencing for Bloodstream Infections in Pediatric Patients Under Intensive Care
Authors Nan X ![]() , Zhang Y
, Zhang Y ![]() , Su N, Yang L
, Su N, Yang L ![]() , Pan G
, Pan G
Received 6 January 2022
Accepted for publication 9 April 2022
Published 18 April 2022 Volume 2022:15 Pages 1911—1920
DOI https://doi.org/10.2147/IDR.S357162
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xiangzhen Nan, Yean Zhang, Nana Su, Lei Yang, Guoquan Pan
Department of Pediatric Intensive Care Unit, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China
Correspondence: Guoquan Pan, Department of Pediatric Intensive Care Unit, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Wenzhou, Zhejiang, People’s Republic of China, Email [email protected]
Purpose: This study aimed to analyze the application value of metagenomic next-generation sequencing (mNGS) as a basis for the proper adjustment of the clinical treatment of bloodstream infections (BSIs) in pediatric patients under intensive care.
Methods: We retrospectively enrolled 46 pediatric patients with clinically diagnosed BSIs who were hospitalized in the pediatric intensive care unit of the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University from June 2018 to July 2021. Blood samples were collected for cultivation and for mNGS detection of pathogens.
Results: Among the 46 children, the average turnaround time for blood culture tests was 3.2 days, and the results revealed pathogens in three children (6.5%). The average turnaround time for mNGS was 2.2 days, and pathogens were found in 30 children (65.2%). The difference in positivity rates between blood culture and mNGS was significant (p< 0.05). Blood culture tests found three pathogens, while mNGS identified 28 pathogens, indicating that mNGS detected significantly more types of pathogens than the traditional diagnostic method for pathogenic microorganisms. In some children, more than one pathogen was detected.
Conclusion: mNGS can help identify pathogenic microorganisms associated with BSI in some pediatric patients under intensive care.
Keywords: pediatric intensive care unit, bloodstream infection, next-generation sequencing, metagenomics
Introduction
A bloodstream infection (BSI) is an infectious disease in which invading pathogens grow and reproduce extensively in the bloodstream and release toxic substances harmful to tissues and organs.1 Pathogens associated with BSIs include bacteria, viruses, fungi, and parasites. The results of a 20-year study showed that Staphylococcus aureus (20.7%) and Escherichia coli (20.5%) were the most common strains causing BSIs, followed by Klebsiella pneumoniae (7.7%), Pseudomonas aeruginosa (5.3%) and Enterococcus faecalis (5.2%). Over the 20-year period, the types and proportions of pathogens detected varied by time, region and patient age, but Staphylococcus aureus and Escherichia coli remained dominant.2
BSIs are among the most serious clinical infections and can occur in people of different ages. Compared with adults, children have lower immunity and are more vulnerable to BSIs due to various innate factors, such as insufficient development of the mucocutaneous barrier and the immune system. In children, the clinical manifestations of BSIs are often atypical, and the disease often progresses rapidly. BSIs are an important cause of death in critically ill patients in the pediatric intensive care unit (PICU), with a mortality rate as high as 20–40%.3,4 In addition to high morbidity and mortality, BSIs in children have high treatment costs. Therefore, accurately diagnosing BSIs and starting effective treatment as early as possible are critical.
Metagenomic next-generation sequencing (mNGS) is a high-throughput sequencing method that directly extracts all microbial DNA from environmental/clinical samples rather than cultures from the samples and then uses a genomics research strategy to analyze all microbial genetic compositions and community functions in the sample. It can be used to extensively analyze the microbiome of clinical samples, including viruses, bacteria and fungi.5 mNGS is valuable in clinical practice due to its wide coverage, high throughput, short turnaround time, and accurate and precise sequencing results. mNGS is also unbiased because it analyzes all the genetic material that can be extracted from the sample nonspecifically. In addition, multiple samples can be analyzed by mNGS simultaneously, and bioinformatics analysis of the results can return abundant information. In this study, 46 children with clinically confirmed BSIs who were hospitalized and received mNGS tests in the PICU of the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University from June 2018 to July 2021 were retrospectively investigated to explore the application value of mNGS in children with BSI.
Subjects and Methods
Study Subjects
This retrospective summary used the clinical data for 46 pediatric patients who were hospitalized in the PICU of the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, China, from June 2018 to July 2021. The hospital is a tertiary first-class hospital that treats a variety of illnesses. The PICU treats 800–1000 inpatient annually. The inclusion criteria were as follows: (1) pediatric patients with clinically diagnosed BSIs (the diagnostic criteria for BSIs in children in this study are based on the “Experts Consensus on the Diagnosis and Treatment of Septic Shock in Children (2015 Edition)”): sepsis: fever (anal temperature >38.5°C) or hypothermia (anal temperature) temperature <35°C), tachycardia (low body temperature may not have tachycardia), accompanied by at least one of the following organ dysfunctions: altered consciousness, hypoxemia, increased serum lactic acid, or pulse beating such as full-pulse waves. The exclusion criteria were as follows: (1) patients with autoimmune diseases and (2) patients with malignant tumors. This study complies with the Declaration of Helsinki and was approved by the Medical Ethics Committee of the Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University (2021-K-114-01). This study is a retrospective study based on the examination results of previous clinical diagnosis and treatment. The exemption of informed consent will not have adverse effects on patients’ rights and health, and is also conducive to the protection of patients’ privacy. We applied to the ethics committee for an exemption from informed consent and it was granted. We state that the study complies with the Declaration of Helsinki and that patient-related data are strictly confidential.
Methods
Sample Collection
After being hospitalized, all pediatric patients underwent three routine tests on blood, urine, and stool (feces), as well as C-reactive protein (CRP), immunological, and blood chemistry tests. Sputum specimens were examined in the same hospital for 13 respiratory pathogens (mycoplasma, chlamydia, adenovirus, respiratory syncytial virus, influenza A virus (InfA), InfA/H1N1, InfA/H3N2, influenza B virus, parainfluenza virus, bocavirus, rhinovirus, metapneumovirus, and coronavirus). Blood samples were tested for IgG/IgM antibodies against Epstein–Barr virus (EBV) (viral capsid antigen, early antigen, and nuclear antigen), toxoplasmosis, rubella, cytomegalovirus (CMV), and herpes simplex virus (HSV) (TORCH) and were also subjected to two fungal assays (Aspergillus galactomannan and fungal beta-
Peripheral Blood Sample Processing and DNA Extraction (BGI Genomics Co., Ltd)
After the sample in the blood collection tube was centrifuged at 2000g for 10 minutes, 0.6 mL of blood plasma was removed and centrifuged at 16,000g for 10 minutes, and 300 µL was used for DNA extraction. DNA was extracted using a microsample genomic DNA extraction kit (DP316, Tiangen BioTech (Beijing) Co., Ltd., Beijing, China) according to the kit instructions. The extracted DNA was used for DNA library construction.6
DNA Library Construction and Sequencing
For quality control, an Agilent 2100 Bioanalyzer was used to measure and control the size of the DNA fragments to be inserted, and a Qubit dsDNA HS Assay Kit (Thermo Fisher Scientific) was used to measure and control the library DNA concentrations. Single-stranded circular DNA was first obtained through cyclization. Then, through rolling circle amplification, the cyclized library DNA was formed into DNA nanoballs, which were loaded onto sequencing slides (wafers) using the BGISEQ-50/MGISEQ-200/MGISEQ-2000 system.7
Data Analysis
Sequencing reads with low quality or a length less than 35 bp were removed. From the remaining high-quality reads, those that could be aligned against the human genome by Burrows–Wheeler alignment (http://biobwa.sourceforge.net/) were removed,8 and after removal of low-complexity reads, the rest were classified by alignment with four large microbial databases of bacteria, fungi, viruses, and parasites. Finally, according to the number of reads combined with the results from other clinical tests, the possible pathogens that had invaded the bloodstream of the patient were identified.
Blood Culture
After checking the patient’s information, the skin was disinfected at the blood collection site with iodine tincture according to the operating guidelines. Blood samples (3–5 mL) were collected from the veins of both upper limbs into culture bottles. The blood samples were sent to the laboratory within 1 hour for relevant tests and blood bacterial culture. The identification of bacterial species was completed by the French Mérieux automatic microbial identification instrument (BacT/ALERT 3D).
Statistical Analysis
SPSS 26.0 software was used for data analysis and processing. Count data are expressed as the rate (%), and the χ2 test was applied for intergroup comparisons, with p<0.05 indicating a statistically significant difference.
Results
Clinical Data
Of the 46 pediatric patients, 27 were boys, and 19 were girls. The youngest patient was 36 days old, and the oldest patient was 15 years old. Five patients were infants (28 days to <1 year), 10 were toddlers (1 to <3 years), six were preschoolers (3 to <6 years), and 25 were school age (6 to 15 years). Before admission, all 46 children had intermittent fevers with or without chills and shivers, and the highest body temperature was 43°C. Sixteen children had a fever only, while the fever was accompanied by cough and/or expectoration in nine children, vomiting in five, convulsions in five, skin rash throughout the body in four, and swollen neck lymph nodes with pain in seven. Before hospitalization, the fever lasted less than 7 days in 16 children and for 7 to <30 days in 30 children. In the latter set of patients, returning the body temperature to normal was difficult despite medication and physical cooling, and the fever often resurged. More details of the clinical data are shown in Table 1.
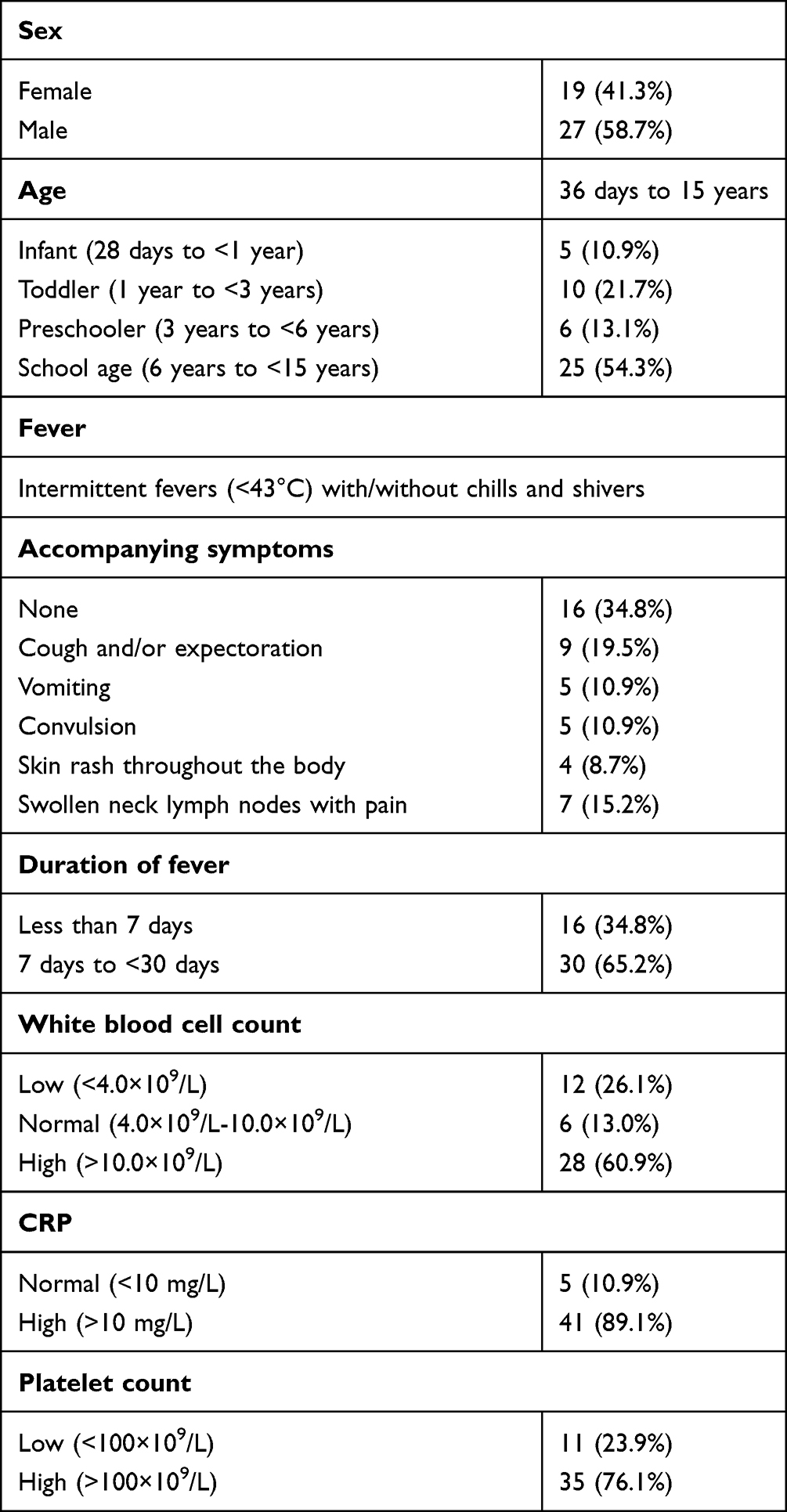 |
Table 1 The Clinical Data and Routine Blood and CRP Test Results of All Patients |
Routine Blood and CRP Test Results
All 46 children submitted blood for routine tests and the CRP test within 2 hours of admission. The white blood cell count was low in 12 children (<4.0×109/L), normal in six children (4.0×109/L-10.0×109/L), and high in 28 children (>10.0×109/L). CRP was high in 41 children (>10 mg/L, highest 263 mg/L), and the platelet count was low in 11 children (<100×109/L). More details of the blood tests are shown in Table 1.
Results of mNGS and Other Pathogen Detection Methods
All 46 children underwent a blood culture test and tests for 13 respiratory pathogens and IgG/IgM antibodies against EBV (viral capsid antigen, early antigen, and nuclear antigen) and TORCH. Blood culture tests identified one case of Candida albicans infection, one case of Escherichia coli infection, and one case of Streptococcus agalactiae infection, resulting in a positive rate of 6.5%. The average turnaround time was 3.2 days. Two children had a positive result on the tests for a respiratory pathogen; both were positive for rhinovirus, which was not considered responsible for the BSI; the two children were diagnosed with O. tsutsugamushi and S. agalactiae septicemia. One child was positive for IgG antibodies against EBV capsid antigen, early antigen, and nuclear antigen, and two children were slightly positive for IgM antibodies against EBV capsid antigen. TORCH, two fungal assays (Aspergillus galactomannan and fungal beta-
mNGS had an average turnaround time of 2.2 days and revealed positive results in 30 children, giving a positive rate of 65.2%, which was significantly higher than that of blood culture (p<0.05). The frequency of each type of organism identified by mNGS is shown in Table 2. Only three pathogens were detected in blood culture tests, while 28 pathogens were detected by mNGS. Among the 30 children with positive mNGS results, 22 were infected by a single type of pathogen (Table 3), and eight were infected by multiple types (Table 4). Both blood culture tests and mNGS detected one case of C. albicans, one case of E. coli, and one case of S. agalactiae.
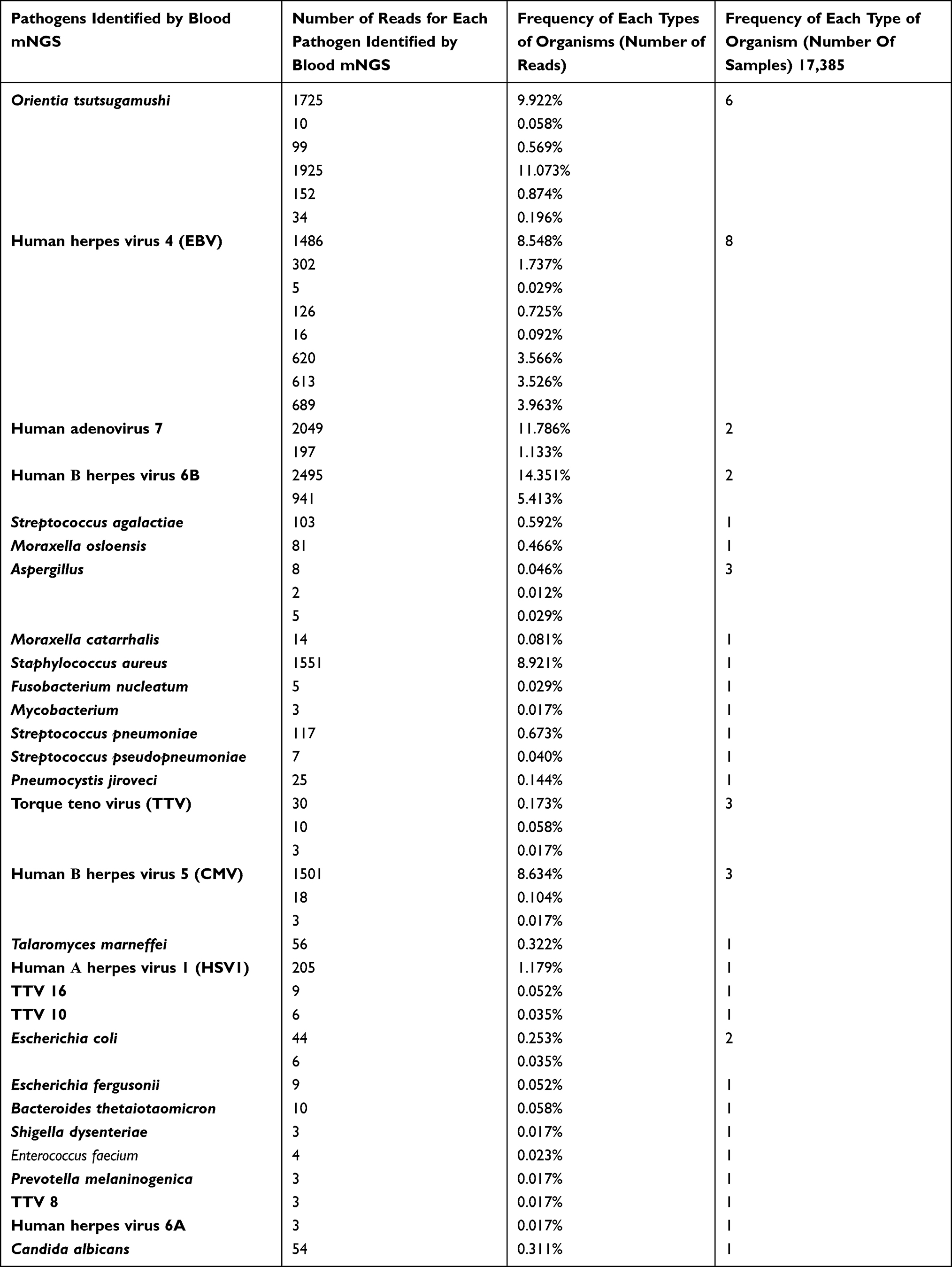 |
Table 2 Frequency of Each Type of Organism Identified by mNGS |
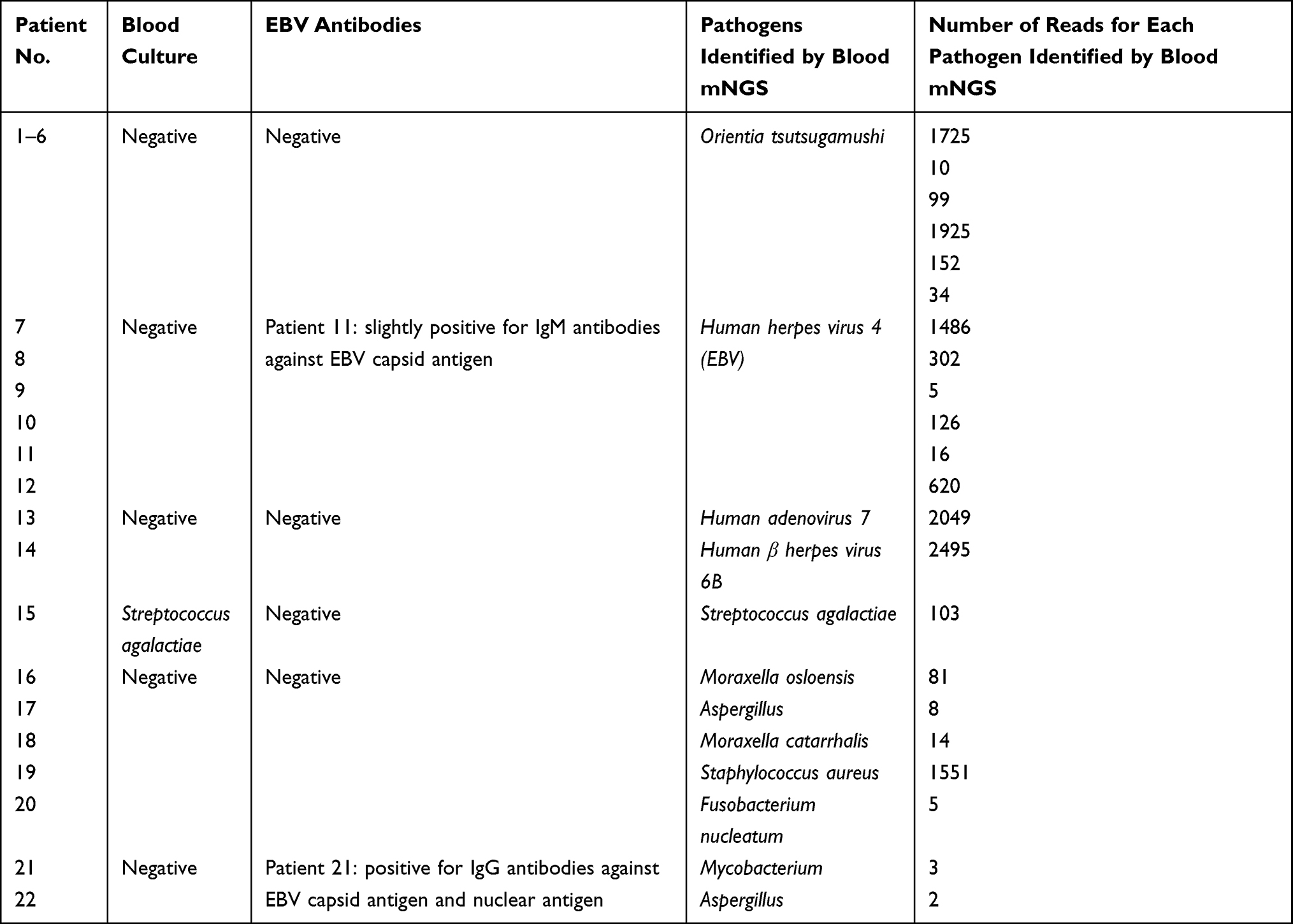 |
Table 3 Data for the 22 Patients with Single-Pathogen Infections |
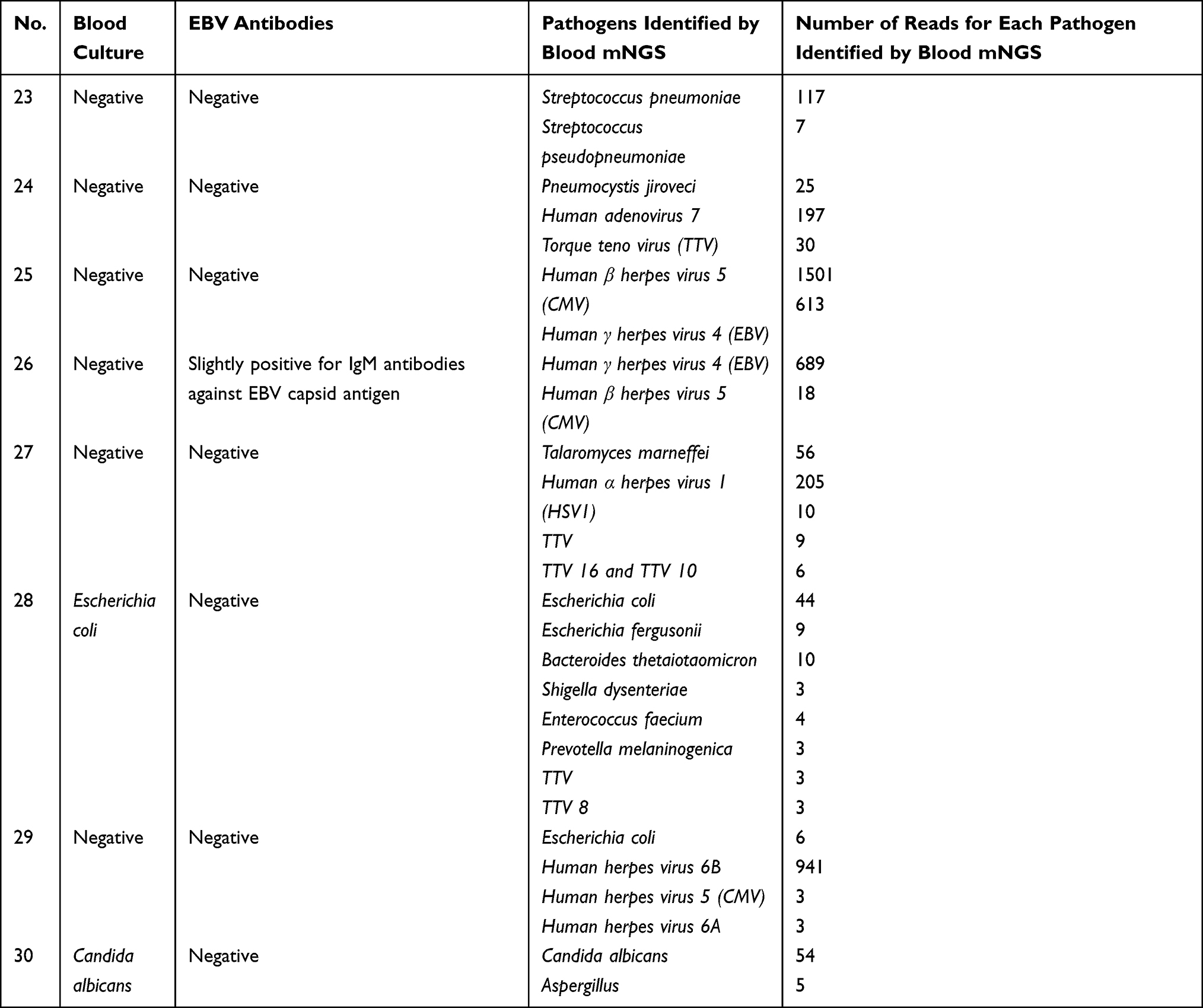 |
Table 4 Data for the Eight Patients with Multiple Pathogen Infections |
Treatment and Outcomes
All pediatric patients received empirical anti-infectious treatment and symptomatic treatment based on their medical history, clinical manifestations, and laboratory test results after admission to the hospital. Among the 30 children with positive mNGS results, antibiotic treatment was adjusted and switched to chloramphenicol in five children (patients 2–6) diagnosed with O. tsutsugamushi infection; all five children showed significant improvement and were discharged after their disease was cured. Patient 1, who had O. tsutsugamushi infection, died the day before the mNGS report. All six of these patients had negative Proteus OX19, Proteus OX2, and Proteus OXK agglutination tests and showed no eschar. Patients 7–12, 25, and 26 received additional treatment with ganciclovir injections after EBV was diagnosed. Patient 27 received additional acyclovir injections. Patients 17 and 30 received additional voriconazole injections after both were diagnosed with Aspergillus, and patient 30 was also diagnosed with C. albicans infection in blood culture tests. All the patients above showed marked improvements after treatment adjustment. In patients 21 and 22, the positive results for Mycobacterium (three reads) and Aspergillus (two reads) were considered not significant because they were inconsistent with clinical manifestations and the results from other related examinations; both patients showed improvements after empirical treatment. Patient 20 received additional metronidazole injections after Fusobacterium nucleatum was identified, and then the body temperature decreased to normal. In the remaining patients, the mNGS reports were consistent with the clinical manifestations, and the identified pathogens were already being treated by antibiotics; therefore, no treatment adjustment was made. One child with S. agalactiae infection died of septic shock the next day. Patient 17 had leukemia accompanied by Aspergillus infection, and patients 7 and 8 with EBV-associated hemophagocytic syndrome were withdrawn from treatment by their families and then died. The other 25 patients were cured and discharged after active and comprehensive treatment.
Discussion
BSI is a serious systemic infectious disease caused by the invasion of pathogenic microorganisms (including bacteria, fungi, viruses, and parasites), which can result in varying degrees of damage to tissues and organs in the human body. In this study, 11 patients (patients 1–8, 10, 12, and 25) developed hemophagocytic syndrome, including six patients with scrub typhus, and the first scrub typhus patient died of multiple-organ failure the day before the mNGS report.
Patients with BSIs often have abnormal laboratory findings, including abnormal peripheral blood white blood cell counts and neutrophil counts and elevated CRP levels and erythrocyte sedimentation rates, but these abnormalities are not specific to BSIs. Blood culture is considered the gold standard for the diagnosis of bacterial and fungal BSIs, but in vitro culture of pathogens is often time-consuming and cumbersome and is not applicable to a variety of pathogens. Other traditional methods for pathogen identification also have various limitations and cannot meet the needs of clinical diagnosis.9 Moreover, different subtypes or genotypes of pathogens vary in pathogenicity, necessitating the acquisition of genomic information about the identified pathogens to guide clinical treatment.
In recent years, NGS, which is also known as high-throughput sequencing, has been continually improved and popularized, providing a new, powerful means for pathogen diagnosis. By directly extracting and detecting all nucleic acid fragments in a sample, this sequencing technology can identify the types of nucleic acids present and acquire quantitative data by bioinformatic analysis, including the number and coverage of sequencing reads for pathogens. This technology has various advantages. First, it does not require sample culture before testing, thereby preventing missed diagnosis of pathogens that are difficult to culture. Second, all nucleic acid fragments are tested directly and nonspecifically without prior selection of a coverage range; in other words, this technology is unbiased, which minimizes the likelihood of missed diagnosis and allows the detection of host genes to facilitate diagnosis. Third, for patient follow-up, NGS can be repeated to compare the quantitative and semiquantitative data (eg, the number of reads for pathogens) before vs after treatment.
The greatest advantage of mNGS is rapid, accurate, and high-throughput detection, which provides evidence supporting early targeted anti-infective treatment. Correct interpretation is also key to reaping the benefits of mNGS. Due to the complex operation process of mNGS, contamination can easily be introduced at each step, which will interfere with the test results by making it impossible to determine if the detected pathogens are colonizing bacteria, background bacteria or pathogenic bacteria. Systematic analysis, interpretation and verification of laboratory and auxiliary examination results are necessary.10
Scrub typhus is an acute infectious disease caused by O. tsutsugamushi (family Rickettsiaceae). The primary reservoir hosts for this disease are rodents, and the disease spreads to people through bites from infected chiggers (larval mites). The clinical manifestations often include persistent high fever, toxemia, skin rash, eschars (which are often in hidden areas such as the armpit, groin, and perineum and are thus easy to miss), lymph node enlargement, and damage to the respiratory system.11,12 However, all these symptoms are atypical, and scrub typhus is therefore often misdiagnosed. At present, serosurvey remains the main laboratory method for the diagnosis of scrub typhus, and the Weil-Felix reaction is commonly used. Although the Weil-Felix reaction can be used for preliminary diagnosis due to its low cost and ease of use, this test has a high false-negative rate, which is mostly caused by the use of antibiotics in the early stage or a lack of an effective immune response due to a weak immune system. Hence, the Widal test and the Weil-Felix reaction have low sensitivity and specificity. In addition, rickettsiae grow inside cells, complicating their detection in in vitro culture tests. All these factors complicate the diagnosis of scrub typhus in patients without noticeable eschars. Moreover, scrub typhus is often complicated by hemophagocytic syndrome in children, in whom missed/delayed diagnosis and treatment are responsible for 7.8% to 25.0% of fatalities.13,14 NGS can facilitate the rapid diagnosis of scrub typhus. In this study, effective antibiotics were used after identification of a scrub typhus pathogen, which led to satisfactory prognosis, suggesting that mNGS is highly valuable in the diagnosis of scrub typhus.
At present, blood culture cannot be used to detect viruses clinically. Instead, viruses can be identified only by enzyme-linked immunosorbent assay and fluorescence quantitative detection. However, these methods have low positive rates and long turnaround times and can be used only to detect specific types of viruses. In this study, patients 11 and 26 were weakly positive for IgM antibodies against EBV capsid antigens, and patient 11 was still positive at re-examination half a month later. All other patients were negative for IgM antibodies against EBV capsid antigen, early antigen, and nuclear antigen. In a case report published by Piantadosi et al,15 Powassan virus was identified within 4 days by metagenomic sequencing in a patient with severe encephalitis who had a history of close contact with rodents such as bats. In this case, metagenomic sequencing identified the rare virus four weeks earlier than traditional methods. Therefore, we believe that mNGS can detect viruses causing BSIs in pediatric patients earlier and more accurately than serosurveys for pathogens.
In the children who were positive for bacterial or fungal infection by mNGS, the low positive rate of the traditional pathogen detection method may be attributed to the empirical antibiotic therapy administered to treat the suspected infection before blood samples were collected. In patient 19, the blood culture test was negative, but the subsequent ascitic fluid culture revealed the presence of Staphylococcus aureus, consistent with the mNGS result. Previous studies have shown that blood NGS yields results that are highly consistent with those of blood culture tests, suggesting that it is a reliable tool for pathogen detection.16 In a Chinese study, the sensitivity and specificity of NGS were 72.7% and 89.6%, respectively, when using blood culture as the gold standard; in addition, NGS provided more information than blood culture, indicating that NGS is a powerful tool to supplement blood culture.16 In another study of septic shock, the positive rate of NGS remained nearly 71% within the first 3 weeks after symptom onset, while that of blood culture reached only 33% at onset and then fluctuated between 10% and 20%.17 The newly released “Clinical Practice Expert Consensus for the Application of Metagenomic Next-Generation Sequencing”16 also recommends blood mNGS for patients with a suspected BSI but negative 3-day blood culture tests who do not respond to empirical anti-infection treatment.
Due to the high cost of mNGS examination, the sample size of this study was relatively small, and the design was not prospective. The positive rate of blood cultures may have been lower due to the treatment of some patients with antibiotics prior to hospitalization. In future research, we will design a multicenter prospective study and enroll more children with BSIs to obtain results more consistent with evidence-based medicine.
Conclusion
The results of this study show that mNGS has high sensitivity for the diagnosis of pathogens in pediatric patients with infectious diseases and can provide evidence of infections of unknown etiology or confirm a clinically suspected diagnosis. Therefore, mNGS can be used as an effective tool to supplement current clinical detection methods. mNGS also shows satisfactory performance in detecting specific pathogens, such as O. tsutsugamushi, in pediatric patients.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pliakos E, Andreatos N, Shehadeh F, Ziakas P, Mylonakis E. The cost-effectiveness of rapid diagnostic testing for the diagnosis of bloodstream infections with or without antimicrobial stewardship. Clin Microbiol Rev. 2018;31(3). doi:10.1128/CMR.00095-17
2. Diekema D, Hsueh P, Mendes R, et al. The microbiology of bloodstream infection: 20-year trends from the SENTRY antimicrobial surveillance program. Antimicrob Agents Chemother. 2019;63(7). doi:10.1128/AAC.00355-19.
3. Ziegler M, Pellegrini D, Safdar N. Attributable mortality of central line associated bloodstream infection: systematic review and meta-analysis. Infection. 2015;43(1):29–36. doi:10.1007/s15010-014-0689-y
4. Corcione S, Angilletta R, Raviolo S, et al. Epidemiology and risk factors for mortality in bloodstream infection by CP-Kp, ESBL-E, Candida and CDI: a single center retrospective study. Eur J Intern Med. 2018;48:44–49. doi:10.1016/j.ejim.2017.10.015
5. Wilson M, Naccache S, Samayoa E, et al. Actionable diagnosis of neuroleptospirosis by next-generation sequencing. N Engl J Med. 2014;370(25):2408–2417. doi:10.1056/NEJMoa1401268
6. Long Y, Zhang Y, Gong Y, et al. Diagnosis of sepsis with cell-free DNA by next-generation sequencing technology in ICU patients. Arch Med Res. 2016;47(5):365–371. doi:10.1016/j.arcmed.2016.08.004
7. Jeon Y, Zhou Y, Li Y, et al. The feasibility study of non-invasive fetal trisomy 18 and 21 detection with semiconductor sequencing platform. PLoS One. 2014;9(10):e110240. doi:10.1371/journal.pone.0110240
8. Li H, Durbin R. Fast and accurate short read alignment with Burrows-Wheeler transform. Bioinformatics. 2009;25(14):1754–1760. doi:10.1093/bioinformatics/btp324
9. Lin-Hai LI, Chen LD, Xiao B, Sun ZH. Application of metagenomic sequencing in detecting the pathogens of infectious diseases. Infect Dis Inf. 2018;31(1):15–18.
10. Miller S, Naccache S, Samayoa E, et al. Laboratory validation of a clinical metagenomic sequencing assay for pathogen detection in cerebrospinal fluid. Genome Res. 2019;29(5):831–842. doi:10.1101/gr.238170.118
11. Qu Y. [A clinical analysis of 31 cases with pulmonary damage caused by scrub typhus]. Chin J Tuberc Respir Dis. 2000;23(2):98–100. Chinese.
12. Y. DZ, Z. C, J. DX. Practice of internal medicine. Beijing: People’s Medical Publishing House; 1994.
13. Wang C, Liu S, Liu J, Chung Y, Su M, Lin M. Acute respiratory distress syndrome in scrub typhus. Am J Trop Med Hyg. 2007;76(6):1148–1152. doi:10.4269/ajtmh.2007.76.1148
14. Varghese G, Janardhanan J, Trowbridge P, et al. Scrub typhus in South India: clinical and laboratory manifestations, genetic variability, and outcome. Int J Infect Dis. 2013;17(11):e981–7. doi:10.1016/j.ijid.2013.05.017
15. Piantadosi A, Kanjilal S, Ganesh V, et al. Rapid detection of Powassan virus in a patient with encephalitis by metagenomic sequencing. Clin Infect Dis. 2018;66(5):789–792. doi:10.1093/cid/cix792
16. Diseases ECotCJoI. Clinical practice expert consensus for the application of metagenomic next generation sequencing in China. Chin J Infect Dis. 2020;38(11):681–689.
17. Grumaz S, Grumaz C, Vainshtein Y, et al. Enhanced performance of next-generation sequencing diagnostics compared with standard of care microbiological diagnostics in patients suffering from septic shock. Crit Care Med. 2019;47(5):e394–e402. doi:10.1097/CCM.0000000000003658
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.