Back to Journals » Infection and Drug Resistance » Volume 16
Application of Mycobacterium tuberculosis RNA for the Rapid Diagnosis of Lymph Node Tuberculosis Using Different Specimens
Authors Yu G ![]() , Lin T, Yu Y, Chen P, Chen M, Zhang Y, Yang G
, Lin T, Yu Y, Chen P, Chen M, Zhang Y, Yang G
Received 2 October 2022
Accepted for publication 6 December 2022
Published 6 January 2023 Volume 2023:16 Pages 179—187
DOI https://doi.org/10.2147/IDR.S392045
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Guocan Yu,1 Ting Lin,2 Yuehui Yu,3 Peijun Chen,2 Menghan Chen,3 Ying Zhang,4,* Gaoyi Yang4,*
1Zhejiang Tuberculosis Diagnosis and Treatment Center, Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China; 2The Second Clinical Medical College, Zhejiang Chinese Medical University, Hangzhou, Zhejiang, People’s Republic of China; 3Division of Health Sciences, Hangzhou Normal University, Hangzhou, Zhejiang, People’s Republic of China; 4Department of Ultrasound, Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine, Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ying Zhang; Gaoyi Yang, Department of Ultrasound, Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine, No. 208 East Huancheng Road, Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]; [email protected]
Purpose: To evaluate the accuracy of Mycobacterium tuberculosis (MTB)-RNA in the rapid diagnosis of lymph node tuberculosis (LNTB). Moreover, the difference in the diagnostic accuracy of MTB-RNA using different specimens was determined.
Methods: We included patients with suspected LNTB who met the inclusion criteria and retrospectively analyzed their clinical data. The sensitivity, specificity, positive-predictive value (PPV), negative-predictive value (NPV), and area under the curve (AUC) of MTB-RNA and culture were calculated and its diagnostic accuracy for LNTB was evaluated in comparison with the final clinical diagnosis.
Results: Overall, 285 patients were included in the study. The overall sensitivity, specificity, PPV, NPV, and AUC of MTB-RNA were 40.6%, 100.0%, 100.0%, 17.0%, and 0.70, respectively. These values were 30.8%, 100.0%, 100.0%, 16.0%, and 0.65, respectively, for tissue specimens; 34.2%, 100.0%, 100.0%, 24.6%, and 0.67, respectively, for puncture specimens; and 57.14%, 100.0%, 100.0%, 5.3%, and 0.79, respectively, for pus specimens. These values of culture were 24.4%, 100.0%, 100.0%, 13.9%, and 0.62, respectively, for all specimens; 17.6%, 100.0%, 100.0%, 13.8%, and 0.59, respectively, for tissue specimens; 25.3%, 100.0%, 100.0%, 22.4%, and 0.63, respectively, for puncture specimens; and 31.0%, 100.0%, 100.0%, 3.3%, and 0.65, respectively, for pus specimens.
Conclusion: The diagnostic efficacy of MTB-RNA for the rapid diagnosis of LNTB was moderate, but its sensitivity was low. The lymph node pus specimens were the most sensitive for MTB-RNA testing, followed by puncture specimens; tissues were the least sensitive. Pus specimens should be preferably obtained in case only this test is to be used for diagnosis.
Keywords: LNTB, pus, puncture, tissue, sensitivity, diagnostic accuracy
Plain Language Summary
In this study, we evaluated the accuracy of using Mycobacterium tuberculosis (MTB)-RNA to rapidly diagnose lymph node tuberculosis (LNTB). The accuracy of this method using different specimens was also examined. We found that MTB-RNA exhibits moderate diagnostic efficacy for the rapid diagnosis of LNTB but with low sensitivity. Moreover, LN pus specimens were highly sensitive, whereas the tissue specimens were the least sensitive for MTB-RNA testing.
Introduction
Mycobacterium tuberculosis (MTB) infection leads to tuberculosis (TB) in humans.1 According to the site of MTB infection, TB can be broadly classified into pulmonary TB (PTB) and extrapulmonary TB (EPTB).2 Among all EPTB, lymph node TB (LNTB) has the highest incidence, and cervical LNTB is the most common type of LNTB.3 Early and rapid diagnosis of LNTB is the key to the treatment of this disease. Diagnostic delays can delay treatment, resulting in local compression, abscess formation, and sinus tract formation, which can affect the patient’s socialization ability and quality of life.4 LNTB involves different pathological stages, allowing clinicians to acquire various specimens, such as puncture, pus, and tissue biopsy specimens.5 However, invasive procedures are required for the acquisition of the specimens. Traditional classical MTB assays (acid-fast bacilli [AFB] smear and culture) are not useful for a rapid diagnosis because of their corresponding shortcomings.6
Molecular detection tests are currently majorly used for the early and rapid diagnosis of TB.7 The development of molecular tests has greatly facilitated the rapid diagnosis of TB.8 The majority of current molecular assay targets are indicated for MTB-DNA;9,10 research on molecular assays for MTB-RNA is limited.11 MTB-RNA can be detected by simultaneous amplification and testing technique, which was invented by Shanghai Rendu Biotechnology Co. and widely performed in Chinese TB laboratories.12 The application of MTB-RNA detection for TB mainly focuses on the auxiliary diagnosis of PTB and is limited to EPTB application.13,14 However, the application of MTB-RNA for the rapid diagnosis of LNTB remains to be established; moreover, the diagnostic accuracy of this method for LNTB is unclear. In addition, the difference in the diagnostic efficacy of MTB-RNA using different specimens is unknown because of the multiple specimens that can be obtained for LNTB. Therefore, this study aimed to use MTB-RNA for the diagnosis of LNTB to evaluate its accuracy in the rapid diagnosis of LNTB and compare the difference in diagnostic accuracy of MTB-RNA using different specimens to provide clinicians more information about this test for LNTB diagnosis.
Material and Methods
We retrospectively analyzed the clinical data of patients with suspected peripheral LNTB who were hospitalized at the Zhejiang TB Diagnosis and Treatment Center from March 2018 to January 2021. Patients with peripheral enlarged LNs and fever, night sweats, and other TB symptoms, those who had positive results on tuberculin-purified protein derivative tests and/or gamma interferon release assay, or those had TB at other sites were suspected to have LNTB. Patients with relevant LN specimens (such as puncture, pus, and tissue specimens) that were used for LNTB diagnosis and relevant specimens with both MTB culture and MTB-RNA test results were included in the study. Patients whose LN specimens were not obtained for relevant testing, those diagnosed with other LN diseases, those not on anti-TB therapy, and those lost to follow-up were excluded.
All patients or their guardians sign informed consent forms for LN puncture, biopsy, or abscess dissection to obtain LN puncture, tissue, or pus specimens, respectively. All patients or their guardians signed an informed consent form agreeing to the use of their relevant data in this study. The study protocol was approved by the Human Research Ethics Committee of Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine (2022-YS-142). This study complies with the Declaration of Helsinki.
The final clinical diagnosis was used as the reference standard in this study.4 The final clinical diagnosis was made based on clinical symptoms, TB immunoassay results, results of other molecular tests on LN specimens (such as Xpert MTB/RIF), results of imaging or ultrasounds, results of pathological tests, and follow-up outcomes. Based on the final clinical diagnostic criteria, patients were divided into the LNTB and non-LNTB groups. In the LNTB group, MTB was detected in the LN specimens through culturing and based on TB-related clinical symptoms, positive imaging or ultrasound results, positive pathological results, positive immunological tests, positive results of other molecular tests, and effective anti-TB treatment. In the non-LNTB group, evidence for negative MTB included ineffective anti-TB treatment and effective corresponding therapy for other pathogenic infection.
Diagnostic Specimen Collection and Handling
In the early stage of simple LN enlargement, we performed LN puncture or surgical biopsy to obtain puncture or tissue specimens according to the patients’ wish. In the stage of LN abscess formation, we performed puncture or abscess incision to obtain pus specimens for testing of the relevant assay. Fresh LN specimens were used for MTB-RNA and culture. Pus specimens could be used directly, and puncture or tissue specimens were used by grinding. N-acetyl-L-cysteine–NaOH was used for decontamination. All pretreated specimens were divided equally and used for MTB-RNA and culture.
MTB Culture
We used solid and/or liquid media for MTB culture using LN specimens obtained after preparation. 0.1 mL of the N-acetyl-L-cysteine–NaOH-treated specimen was taken and inoculated onto the medium after aseptic manipulation and incubated in a constant cabinet at 37°C. Solid or liquid culture methods were conducted following the instructions of the manufacturer. A positive result for any of the two culture methods is a positive MTB culture result.
MTB-RNA
Decontaminated relevant LN specimens were centrifuged at 13,000 ×g for 5 min, and the supernatant was discarded to retain the sediment. Subsequently, 50 µL of dilution solution was added to the sediment, mixed well, and placed in a water bath sonicator (Shanghai Shenyang Ultrasound Machines, China) for 15 min. The treated mixture was centrifuged to obtain the supernatant; 2 µL of this supernatant was added to 30 µL of the reaction solution to obtain a mixed solution. The obtained mixed solution was placed in a polymerase chain reaction (PCR) tube and pre-incubated at 60°C for 10 min and then at 42°C for 5 min. Then, 2000 units of T7 RNA polymerase (RD Bioscience, Inc., San Diego, CA, USA) and 2000 units of Moloney murine leukemia virus reverse-transcriptase were added to the incubated solution. The final mixture obtained was used for 16S rRNA amplification and analysis using a fluorescence quantitative real-time PCR instrument (SLAN-96S Real-Time PCR System, Xiamen Zeesan Biotech Co., Ltd., Xiamen, China). Finally, the test results were analyzed according to the product information pamphlet.15
Data Processing and Statistical Analysis
Microsoft Excel 2019 was used to record relevant data and calculate relevant ratio, mean, and standard deviation. IBM SPSS Statistics, version 24.0 (IBM Corp., Armonk, NY, USA), was used to calculate the true-positive, false-positive, false-negative, and true-negative values through 2×2 cross-tabulation. Based on these four values, MedCalc Statistical v15.2.2 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org) was used to calculate the sensitivity, specificity, positive-predictive value (PPV), negative-predictive value (NPV), and area under the curve (AUC) with 95% confidence interval (CI) of the test of interest and compared with the final clinical diagnosis. Differences between paired data were compared using McNemar’s test. Differences in the diagnostic efficacy of MTB-RNA using different specimens were compared using the Chi-square test or Fisher’s exact test. Different AUCs were compared using Z-test. An interactive tool (http://www.bioinformatics.com.cn/static/others/jvenn/example.html) was used to generate Venn diagrams. P < 0.05 indicated a significant difference between the two groups compared.
Results
Initial screening was performed for 322 patients, and 37 patients without culture data were excluded. As a result, 285 patients were included in the study. One LN specimen was obtained for each patient, resulting in a total of 285 specimens, including 103 tissue, 96 puncture, and 86 pus specimens (Figure 1). The mean age of the patients was 36.1 ± 16.0 years, and 157 (55.1%) of them were women. Two patients were positive for HIV. Only 36 LN specimens were tested with AFB smear, of which 3 (8.3%) were positive and the remaining 33 (91.7%) were negative.
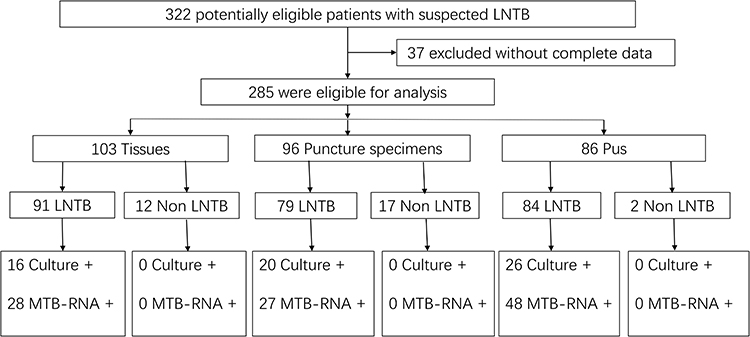 |
Figure 1 Diagnostic classification chart of included participants in different types of specimens. Abbreviations: LNTB, Lymph node tuberculosis; MTB, Mycobacterium tuberculosis. |
Among all patients, with reference to the final clinical diagnostic criteria, 254 cases were diagnosed as LNTB, including 91 tissues, 79 puncture, and 84 pus specimens, and 31 cases were diagnosed as non-LNTB, including 12 tissues, 17 puncture, and 2 pus specimens. Among all specimens in the LNTB group, 62 MTB culture were positive, including 16 tissues, 20 puncture, and 26 pus specimens, and 103 were positive for MTB-RNA, including 28 tissues, 27 puncture, and 48 pus specimens (Figure 1). In the non-LNTB group, no MTB culture and MTB-RNA-positive specimens were found. The distribution and overlap of positive MTB culture and MTB-RNA in all specimens and varying specimens are shown in Figure 2. The distribution of the MTB-RNA and culture positive results among the different sample types are shown in Figure 3.
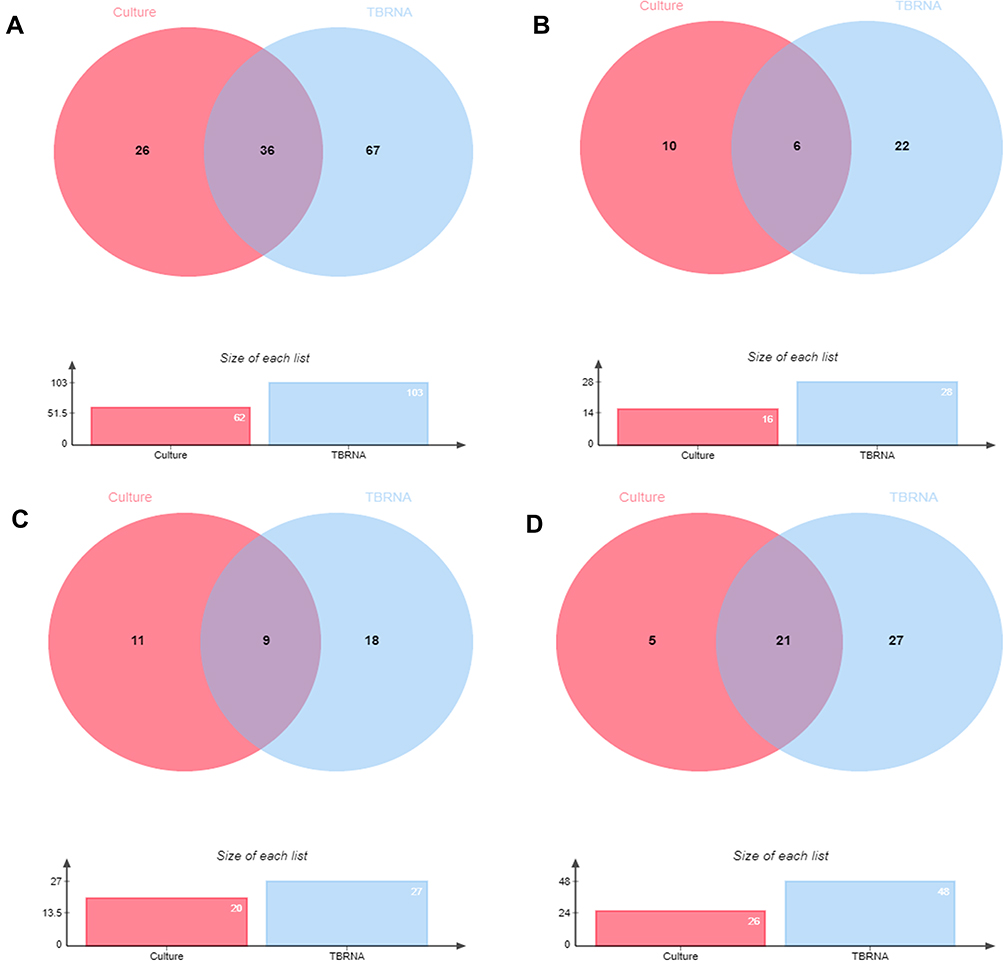 |
Figure 2 Venn diagram of positive tests. (A) all specimens. (B) tissue specimens. (C) puncture specimens. (D) pus specimens. |
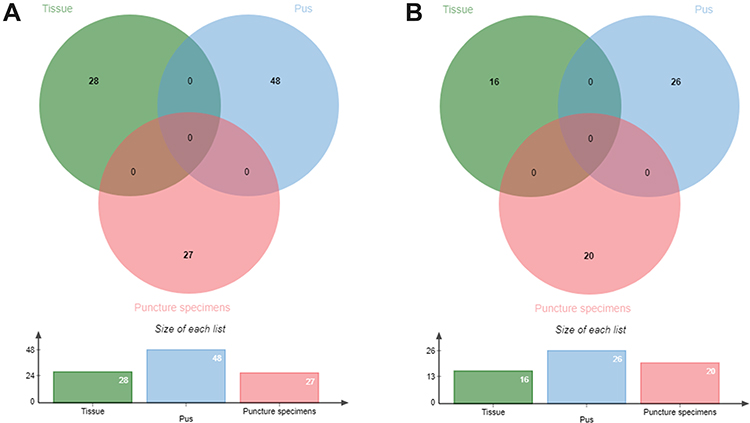 |
Figure 3 The distribution of the MTB-RNA and culture positive results among the different sample types. (A) MTB-RNA. (B) Culture. |
Diagnostic Accuracy of MTB Culture and MTB-RNA
The overall sensitivity, specificity, PPV, NPV, and AUC of MTB culture in the diagnosis of LNTB were 24.4% (95% CI, 19.3–30.2%), 100.0% (88.8–100.0%), 100.0% (94.2–100.0%), 13.9% (9.6–19.2%), and 0.62 (0.56–0.68), respectively. The overall sensitivity, specificity, PPV, NPV, and AUC of MTB-RNA were 40.6% (34.5–46.9%), 100.0% (88.8–100.0%), 100.0% (96.5–100.0%), 17.0% (11.9–23.3%), and 0.70 (0.65–0.76), respectively. These results are illustrated in Table 1.
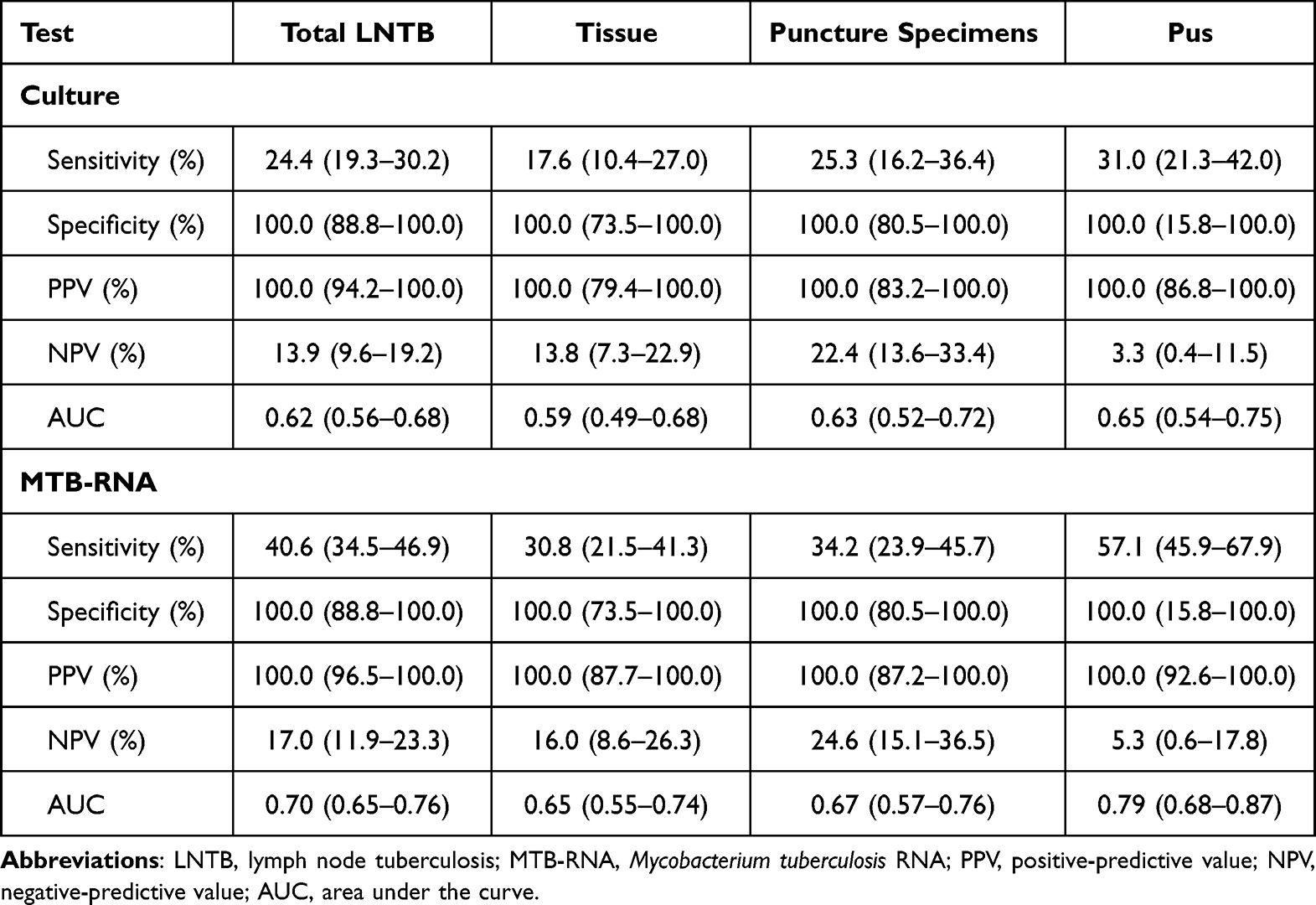 |
Table 1 Diagnostic Accuracy of Culture and MTB-RNA for Lymph Node Tuberculosis Diagnosis Using Various Specimens |
For the tissue specimens, the sensitivity, specificity, PPV, NPV, and AUC of MTB culture were 17.6% (10.4–27.0%), 100.0% (73.5–100.0%), 100.0% (79.4–100.0%), 13.8% (7.3–22.9%), and 0.59 (0.49%–0.68), and those of the MTB-RNA were 30.8% (21.5–41.3%), 100.0% (73.5–100.0%), 100.0% (87.7–100.0%), 16.0% (8.6–26.3%), and 0.65 (0.55–0.74), respectively.
For the LN puncture specimens, the sensitivity, specificity, PPV, NPV, and AUC of MTB culture were 25.3% (16.2–36.4%), 100.0% (80.5–100.0%), 100.0% (83.2–100.0%), 22.4% (13.6–33.4%), and 0.63 (0.52–0.72), respectively, and the values of MTB-RNA were 34.2% (23.9–45.7%), 100.0% (80.5–100.0%), 100.0% (87.2–100.0%), 24.6% (15.1–36.5%), and 0.67 (0.57–0.76), respectively.
For pus specimens, the sensitivity, specificity, PPV, NPV, and AUC of MTB culture were 31.0% (21.3–42.0%), 100.0% (15.8–100.0%), 100.0% (86.8–100.0%), 3.3% (0.4–11.5%), and 0.65 (0.54–0.75), respectively. The values of the MTB-RNA were 57.14% (45.9–67.9%), 100.0% (15.8–100.0%), 100.0% (92.6–100.0%), 5.3% (0.6–17.8%), and 0.79 (0.68–0.87), respectively. Table 1 summarizes the results.
Comparison of the Diagnostic Accuracy of MTB-RNA Using Different Specimens
We compared the differences in diagnostic accuracy for MTB-RNA using different specimens. The sensitivity of the MTB-RNA was the highest in pus, in comparison with LN puncture and tissue specimens (P < 0.05, Table 2). The sensitivity of the MTB-RNA was comparable to those of LN puncture and tissue specimens, and the difference was not significant (P > 0.05). The specificity of the MTB-RNA assay using different specimens was consistent (100%). The diagnostic accuracy of MTB-RNA in pus specimens was the best, but the difference did not reach significance when compared with the other two specimens (P > 0.05).
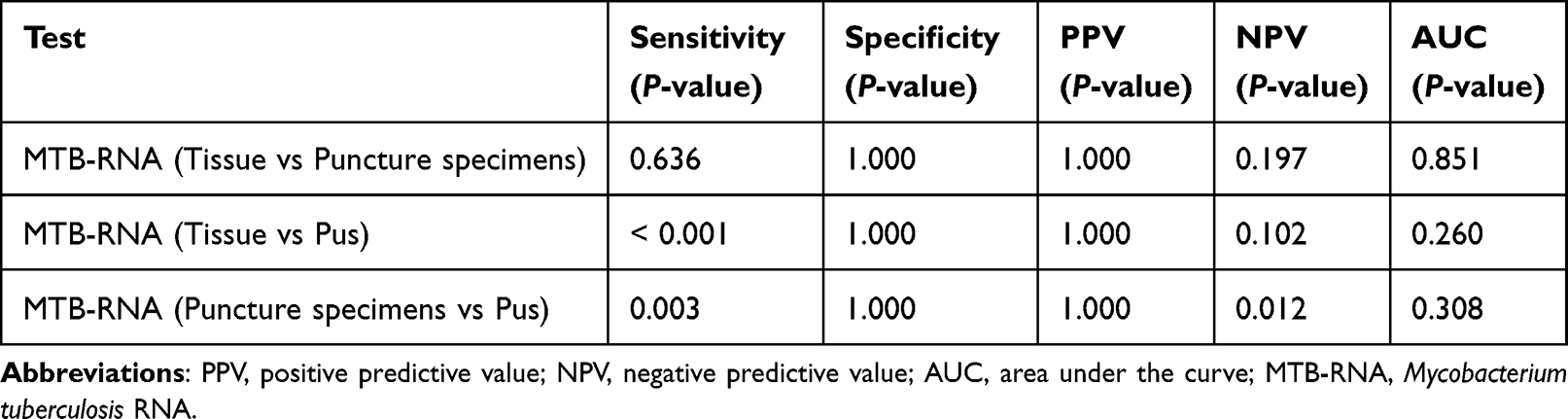 |
Table 2 Comparison of the Diagnostic Accuracy of MTB-RNA Using Different Specimen Types for the Diagnosis of Lymph Node Tuberculosis |
Discussion
In China, LNTB is the most common type of EPTB and a common cause of peripheral LN enlargement.16 The clinical presentation of LNTB is varied, presenting as a simple mass, an abscess, or a sinus tract. Different LN specimens can be obtained at each stage of LNTB development. For simple enlarged LNs, LN puncture (with or without ultrasound guidance) can be performed to obtain puncture specimens; alternatively, surgical biopsy can be performed to obtain tissue specimens. For abscess-type LNTB, pus specimens can be obtained. The acquisition of LN specimens generally involves invasive procedures, except in the case of abscess-type LNTBs that break down independently. Different LNTB stages can coexist in the same patient, especially in cases of multiple LN enlargement. However, the early and rapid diagnosis of LNTB remains challenging.17 AFB smear, although easy to perform and inexpensive, has a low efficacy in TB diagnosis and is unsuitable for the effective diagnosis of TB or LNTB.18
In this study, only 8.3% (3/36) of the specimens for which AFB smear were performed were positive, which may be related to the low MTB content in the LN specimens. This suggested that AFB smear is unsuitable for the rapid diagnosis of LNTB and is prone to missed diagnoses. MTB culture can be considered a crucial method for TB diagnosis; however, it takes a long time (up to 6 weeks) to obtain results, which may delay treatment.19 Pathological testing can guide LNTB diagnosis, but pathology does not suggest direct pathogenic evidence and remains time-consuming; therefore, it does not provide an early, rapid, and effective diagnosis of LNTB.
With it development, molecular diagnostic technology is now preferably used for the early and rapid diagnosis of TB.20 However, there may be differences between molecular diagnostic tests,21 and the efficacy of each molecular test for TB diagnosis should be evaluated separately. In EPTB, Xpert MTB/RIF is widely used for the early diagnosis of the disease, and its diagnostic accuracy is satisfactory;22,23 The loop-mediated isothermal amplification (LAMP) assay is also used for the diagnosis of EPTB, and its performance is also very good.24 Other molecular methods, such as the CapitalBio Mycobacterium real-time polymerase chain reaction (RT-PCR) and mNGS,21,25,26 have also been used in EPTB, and they have shown their own characteristics in the diagnosis of the disease. The most widely used clinical tests are molecular diagnostic tests based on MTB-DNA; molecular tests based on MTB-RNA are limited. Comparing DNA-based tests, the cost of MTB-RNA alone is low, and it is covered by basic health insurance in China, which is more friendly to low-income groups. MTB-RNA testing has relatively good diagnostic efficacy in TB diagnosis,27 but previous studies have mainly focused on PTB diagnosis. Moreover, EPTB-related studies are scarce,13 and no independent studies have reported the diagnostic accuracy for LNTB. In addition, the difference in the diagnostic efficacy of MTB-RNA in different LN specimens is unknown. Therefore, we conducted this study to evaluate the diagnostic efficacy of MTB-RNA for LNTB and its performance with different LN specimens.
In this study, the overall sensitivity and specificity of MTB-RNA for diagnosing LNTB were 40.6% and 100.0%, respectively. A previous study showed that the sensitivity and specificity of MTB-RNA in EPTB diagnosis compared with the clinical diagnosis were 41.2% and 100.0%, respectively.13 LNTB is a type of EPTB, and our findings were similar to the results of the previous study; however, that study did not report specific EPTB types and is a weaker guide to clinical practice.13 Our study clarified the overall diagnostic accuracy of the MTB-RNA assay for LNTB using larger samples, providing a more specific reference for the use of MTB-RNA assay in LNTB, a specific EPTB. The specificity of MTB-RNA for the diagnosis of LNTB was excellent but the sensitivity was low. Compared with other MTB-DNA-based molecular assays, such as the Xpert MTB/RIF,25 the sensitivity of MTB-RNA for LNTB was low in this study. This may be because RNA is less stable than DNA, with RNA degrading in approximately 7 days, whereas DNA can remain stable continuously. In addition, MTB-RNA is mainly used for PTB detection, and suitable specimens are mainly sputum and bronchoalveolar lavage fluid. The handling of LN specimens (such as tissue) may be different from that of sputum, which may affect MTB-RNA detection. However, non-head-to-head comparisons may not be credible, especially for LNTB where multiple types of specimens can be obtained, and head-to-head studies with large samples are needed to further clarify the differences in diagnostic accuracy between MTB-RNA and DNA-based tests.
The second objective of this study was to determine the diagnostic accuracy of MTB-RNA for LNTB using different LN specimens as this has not been reported by any study. For the three frequently available LN specimens of puncture, tissue, and pus, MTB-RNA showed the highest diagnostic accuracy when using pus specimens, followed by puncture specimens, and the lowest accuracy when using tissue specimens. Differences in the handling of different LN specimens may be one of the reasons for these differences in accuracy. Pus specimens are closer to sputum and are easier to handle, whereas the distribution of MTB in puncture and tissue specimens may be heterogeneous and the specimens may require grinding before processing. The differences between the three specimens were not significant; this may be related to the small sample size of each subgroup. Therefore, studies with large sample sizes are warranted to further clarify the differences.
The results of this study have important implications for the type of LN specimen to be used for MTB-RNA testing to obtain maximum benefit. For MTB-RNA, pus specimen is preferred for testing when LN abscesses are formed, and puncture specimens can be selected first for testing when no abscesses are formed because LN puncture is relatively less invasive.
This study has some limitations. First, because this was a retrospective study, patient selection may have been biased. Second, MTB-RNA is mainly applied in China and less in other regions, and it may have lower reference significance in other regions. Third, the MTB-RNA results were not compared with the results of other DNA-based tests in this study because the number of samples for simultaneous DNA and RNA testing is limited and head-to-head comparisons are difficult. Fourth, different specimens were not compared head-to-head, and the specimen volume in each group was small; thus, the results may not be reliable, and the conclusion still needs to be confirmed through head-to-head comparative studies or randomized studies with large sample sizes.
Conclusion
The diagnostic efficacy of MTB-RNA for the rapid diagnosis of LNTB was moderate, but its sensitivity was low. LN pus specimens were the most sensitive for MTB-RNA testing, followed by puncture specimens, and tissue specimens were the least sensitive. Therefore, pus specimens should be preferably obtained in case only this test is to be used for diagnosis.
Data Sharing Statement
Data will be made available on reasonable request.
Ethics Approval and Consent to Participate
All patients gave written informed consent and the study was approved by the Human Research Ethics Committee of Affiliated Hangzhou Chest Hospital, Zhejiang University School of Medicine. This study complies with the Declaration of Helsinki.
Acknowledgments
We would like to express our gratitude to the patients and their families.
Funding
Gaoyi Yang, 20190101A09, Hangzhou Science and Technology Bureau, http://kj.hangzhou.gov.cn. 2021KY911, 2022KY986, Health Commission of Zhejiang Province, https://wsjkw.zj.gov.cn/. The funders do not have a role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. World Health Organization. Global Tuberculosis Report 2021. World Health Organization; 2021.
2. Koch A, Mizrahi V. Mycobacterium tuberculosis. Trends Microbiol. 2018;26(6):555–556. doi:10.1016/j.tim.2018.02.012
3. Yu G, Zhong F, Ye B, Xu X, Chen D, Shen Y. Diagnostic accuracy of the xpert MTB/RIF assay for lymph node tuberculosis: a systematic review and meta-analysis. Biomed Res Int. 2019;2019:4878240. doi:10.1155/2019/4878240
4. Shen Y, Fang L, Ye B, Xu X, Yu G, Zhou L. The role of core needle biopsy pathology combined with molecular tests in the diagnosis of lymph node tuberculosis. Infect Drug Resist. 2022;15:335–345. doi:10.2147/IDR.S350570
5. Yao L, Xu X, Chen G, Shen Y, Jiang W. Comparison of the accuracy of two different molecular tests for the diagnosis of tuberculous lymphadenitis using core needle biopsy specimens: a diagnostic accuracy study. Int J Gen Med. 2022;15:5237–5246. doi:10.2147/IJGM.S367127
6. Fontanilla JM, Barnes A, von Reyn CF. Current diagnosis and management of peripheral tuberculous lymphadenitis. Clin Infect Dis. 2011;53(6):555–562. doi:10.1093/cid/cir454
7. Yu G, Zhong F, Zhao W, Ye B, Xu K, Chen G. Head-to-head comparison of the diagnostic value of five tests for constrictive tuberculous pericarditis: five tests for constrictive TBP. Int J Infect Dis. 2022;120:25–32. doi:10.1016/j.ijid.2022.04.018
8. Shen Y, Fang L, Xu X, Ye B, Yu G. CapitalBio Mycobacterium real-time polymerase chain reaction detection test: rapid diagnosis of Mycobacterium tuberculosis and nontuberculous mycobacterial infection. Int J Infect Dis. 2020;98:1–5. doi:10.1016/j.ijid.2020.06.042
9. Zheng H, Zhong F, Yu G, Shen Y. Comparison of the diagnostic efficacy of the CapitalBio Mycobacterium real-time polymerase chain reaction detection test and Xpert MTB/RIF in smear-negative pulmonary tuberculosis. Eur J Clin Microbiol Infect Dis. 2021;40(5):969–977. doi:10.1007/s10096-020-04113-1
10. Yu G, Shen Y, Ye B, Shi Y, Feizabadi MM. Diagnostic accuracy of Mycobacterium tuberculosis cell-free DNA for tuberculosis: a systematic review and meta-analysis. PLoS One. 2021;16(6):e0253658. doi:10.1371/journal.pone.0253658
11. Yan L, Zhang Q, Xiao H. Clinical diagnostic value of simultaneous amplification and testing for the diagnosis of sputum-scarce pulmonary tuberculosis. BMC Infect Dis. 2017;17(1):545. doi:10.1186/s12879-017-2647-7
12. Fan L, Zhang Q, Cheng L, et al. Clinical diagnostic performance of the simultaneous amplification and testing methods for detection of the Mycobacterium tuberculosis complex for smear-negative or sputum-scarce pulmonary tuberculosis in China. Chin Med J. 2014;127(10):1863–1867.
13. Li T, Shi T, Sun Y, et al. Application of real-time simultaneous amplification and testing method to accurately and rapidly detect extra-pulmonary tuberculosis. BMC Infect Dis. 2020;20(1):303. doi:10.1186/s12879-020-05036-0
14. Qiu X, Zheng S, Yang J, Yu G, Ye Y. Comparing Mycobacterium tuberculosis RNA accuracy in various respiratory specimens for the rapid diagnosis of pulmonary tuberculosis. Infect Drug Resist. 2022;15:4195–4202. doi:10.2147/IDR.S374826
15. Li QH, Zhang Y, Zhao MM, et al. Simultaneous amplification and testing method for Mycobacterium tuberculosis rRNA to differentiate sputum-negative tuberculosis from sarcoidosis. Am J Physiol Lung Cell Mol Physiol. 2019;316(3):L519–l524. doi:10.1152/ajplung.00172.2018
16. Qian X, Albers AE, Nguyen DTM, et al. Head and neck tuberculosis: literature review and meta-analysis. Tuberculosis. 2019;116s:S78–s88. doi:10.1016/j.tube.2019.04.014
17. Walzl G, McNerney R, du Plessis N, et al. Tuberculosis: advances and challenges in development of new diagnostics and biomarkers. Lancet Infect Dis. 2018;18(7):e199–e210. doi:10.1016/S1473-3099(18)30111-7
18. Sharif N, Ahmed D, Mahmood RT, et al. Comparison of different diagnostic modalities for isolation of Mycobacterium tuberculosis among suspected tuberculous lymphadenitis patients. Braz J Biol. 2021;83:e244311. doi:10.1590/1519-6984.244311
19. Gupta V, Bhake A. Assessment of clinically suspected tubercular lymphadenopathy by real-time PCR compared to non-molecular methods on lymph node aspirates. Acta Cytol. 2018;62(1):4–11. doi:10.1159/000480064
20. Machado D, Couto I, Viveiros M. Advances in the molecular diagnosis of tuberculosis: from probes to genomes. Infect Genet Evol. 2019;72:93–112. doi:10.1016/j.meegid.2018.11.021
21. Yu G, Wang L, Shen Y, et al. Comparison of the diagnostic accuracy of xpert MTB/RIF and Capitalbio Mycobacterium RT-PCR detection assay for tuberculous pericarditis. Infect Drug Resist. 2022;15:2127–2135. doi:10.2147/IDR.S360064
22. Yu G, Ye B, Chen D, et al. Comparison between the diagnostic validities of Xpert MTB/RIF and interferon-γ release assays for tuberculous pericarditis using pericardial tissue. PLoS One. 2017;12(12):e0188704. doi:10.1371/journal.pone.0188704
23. Park M, Kon OM. Use of Xpert MTB/RIF and Xpert Ultra in extrapulmonary tuberculosis. Expert Rev Anti Infect Ther. 2021;19(1):65–77. doi:10.1080/14787210.2020.1810565
24. Yu G, Shen Y, Zhong F, Ye B, Yang J, Chen G. Diagnostic accuracy of the loop-mediated isothermal amplification assay for extrapulmonary tuberculosis: a meta-analysis. PLoS One. 2018;13(6):e0199290. doi:10.1371/journal.pone.0199290
25. Yu G, Shen Y, Ye B, Chen D, Xu K. Comparison of CapitalBio™ Mycobacterium nucleic acid detection test and Xpert MTB/RIF assay for rapid diagnosis of extrapulmonary tuberculosis. J Microbiol Methods. 2020;168:105780. doi:10.1016/j.mimet.2019.105780
26. Yu G, Wang X, Zhu P, Shen Y, Zhao W, Zhou L. Comparison of the efficacy of metagenomic next-generation sequencing and Xpert MTB/RIF in the diagnosis of tuberculous meningitis. J Microbiol Methods. 2021;180:106124. doi:10.1016/j.mimet.2020.106124
27. Cui Z, Wang Y, Fang L, et al. Novel real-time simultaneous amplification and testing method to accurately and rapidly detect Mycobacterium tuberculosis complex. J Clin Microbiol. 2012;50(3):646–650. doi:10.1128/JCM.05853-11
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of the Diagnostic Performance of the LINEAR Cromatest and Laboquick URS 10-T Dipsticks Among Urinary Tract Infection Suspects in Addis Ababa, Ethiopia: A Cross-Sectional Study
Gebretensaie Y, Atnafu A, Alemu Y, Girma S, Desta K
Research and Reports in Urology 2023, 15:437-445
Published Date: 4 October 2023