")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Application of Health Belief Model to Assess Predictors of Weight Management Behaviour Intention Among Civil Servants in Ethiopia: A Mixed Method Study
Authors Kebede N, Mohammed Y, Kasaye MD , Zewdie A
Received 18 July 2023
Accepted for publication 21 October 2023
Published 26 October 2023 Volume 2023:16 Pages 3339—3352
DOI https://doi.org/10.2147/DMSO.S431146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
Natnael Kebede,1 Yirgalem Mohammed,2 Mulugeta Desalegn Kasaye,3 Amare Zewdie4
1Department of Health Promotion, School of Public Health College of Medicine Health Sciences, Wollo University, Dessie, Ethiopia; 2Department of Health System and Policy, School of Public Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 3Department of Health Informatics, School of Public Health, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 4Department of public health, college of Medicine and health Science, Wolkite University, Wolkite, Ethiopia
Correspondence: Natnael Kebede, Email [email protected]
Introduction: This study aims to use the health belief model to identify predictors of weight management behaviour among civil servants in Ethiopia. Predictors include perceived susceptibility, severity, benefits, barriers, cues to action, and self-efficacy. The study will provide insight into potential factors that civil servants perceive as significant in weight management.
Methods: A sequential explanatory study was conducted from November 15, 2022, to January 20, 2020 among civil servants working in Dessie town, with 423 participants selected through simple random and purposive sampling techniques for the quantitative and qualitative studies, respectively. Self-administered questionnaires were used for the quantitative study, while in-depth interviews were conducted for the qualitative study. Data was verified, entered into Epi Data, and analysed using Stata for multivariable linear regression. ATLAS.ti software version 7 facilitated the qualitative data analysis process. Findings with a p-value < 0.05 at a 95% confidence interval were considered statistically significant in the final model.
Results: This study found that several factors were significantly associated with higher behavioural intention for weight management. Females had higher intention than males, and individuals with higher educational levels demonstrated higher intention. Marital status was also a factor, with being divorced associated with lower intention. The absence of an obese family member and lack of prior weight loss experience were also linked to lower intention. Perceived susceptibility and perceived benefits positively influenced intention, while higher perceived barriers were linked to lower intention.
Conclusion: The study found that a stronger inclination towards weight management was linked to being female, having higher education, no obese family member, prior weight loss experience and positive attitudes. Interventions should target those less likely to exhibit these characteristics and address negative attitudes towards weight management.
Keywords: health belief model, intention, weight management behaviour
Introduction
The health belief model, originally developed in the 1950s, is a preventive model commonly employed to address public health issues, particularly cardiovascular disease.1 In addition, this model aims to explain the lack of public engagement in health screening and prevention programs. Furthermore, The HBM comprises several key variables, including perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, and self-efficacy. These variables interact with each other to determine an individual’s intention to engage in a particular health behaviour.
To predict success in management behaviour intention, it is important to identify the specific variables that are most relevant to the behaviour in question. For example, if the behaviour is related to weight management, perceived susceptibility and severity of health problems related to obesity may be important predictors. Perceived benefits of weight loss and perceived barriers to healthy eating and exercise may also play a role. Cues to action, such as reminders or incentives to engage in healthy behaviours, can also influence behaviour intention. Finally, self-efficacy, or an individual’s belief in their ability to successfully engage in the behaviour, is a critical predictor of behaviour intention and success2,3 (Figure 1). Abnormal or excessive accumulation of fat, known as overweight or obesity, can hurt health and it’s usually measured based on high Body Mass Index (BMI).4
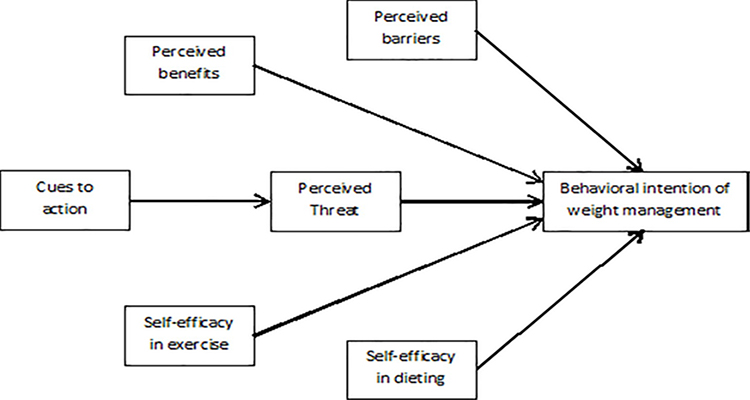 |
Figure 1 Theoretical framework adapted of health belief model applied to the behavioral intention of weight management from Glanz textbook 5th edition, showing the proposed relationship between the Independent variable and weight management behavior, Wollo University, Ethiopia, July 2023GC. |
The rapid and widespread increase in global obesity rates has emerged as a significant challenge.5 According to the World Health Organization (WHO), approximately 39% of adults worldwide are classified as overweight, with 13% being classified as obese.6 Obesity poses a critical concern for public health, as it is associated with a range of physical and psychological issues, including coronary heart disease, diabetes, and various types of cancer.7,8
In addition to its health implications, obesity places significant financial burdens on governments and individuals.9 Recent reports from the World Health Organization (WHO) indicate that overweight and obesity have become the leading causes of death globally.10,11 The worldwide burden of overweight and obesity is staggering, accounting for 2.8 million deaths per year and 35.8 million disability-adjusted life-years.12 Furthermore, overweight or obesity contributes to 44% of diabetes cases, 23% of ischemic heart diseases, and 7–41% of certain cancers.13
Across all regions in Africa, the body mass index (BMI) has shown a consistent increase over time, mirroring the global trend. Notably, the mean BMI in northern and southern Africa surpasses the global average. Projections indicate that the prevalence of overweight and obesity in Africa is expected to reach 20–50% by 2025.14 Specific country data reveals significant rates, such as 20.8% of Nigerians being overweight, 31.3% of South Africans being obese, and 37.1% and 27.8% of Ghanaians being overweight and obese, respectively.14,15 In Ethiopia, the prevalence of overweight and obesity stands at 28%.16
Overweight and obesity are strongly associated with a range of comorbidities that pose significant public health concerns, including cardiovascular diseases, type 2 diabetes, high blood pressure, high blood cholesterol, high triglycerides, certain types of cancer, and sleep apnea.17 Moreover, the impact of overweight and obesity extends beyond physical health, as it also results in compromised quality of life and imposes higher medical, psychological, and social burdens on society.18 Unhealthy eating habits and a sedentary lifestyle are major contributors to these diseases. Alarmingly, over 44% of the population does not engage in enough physical activity, while only 14% can be considered active.19 In addition, Multiple factors, including genetics, behavioural choices, and environmental influences like physical activity and dietary patterns, contribute to the development of obesity.20 To effectively address weight management, behavioural change-based strategies need to be implemented, supported by evidence-based theoretical frameworks.21 One prominent model for behavioural change in preventive programs within public health is the health belief model.
Obesity poses a significant public health challenge, with its prevalence rapidly increasing. Despite extensive efforts, successful interventions remain limited. Evidence supports that changing human behaviour and lifestyle is key to achieving weight loss and maintenance, emphasizing the importance of a comprehensive approach to weight management. Currently, there is a lack of research specifically focusing on the predictors of weight management behaviour intention among civil servants in Dessie town, Ethiopia. This gap highlights the need for a comprehensive investigation into the factors influencing weight management intentions within this specific population. By applying the health belief model, which encompasses crucial factors such as perceived susceptibility, severity, benefits, barriers, cues to action, and self-efficacy, this study fills the research gap and offers valuable insights. The mixed method approach, combining quantitative and qualitative data collection, enhances the study’s value by providing a deeper understanding of the predictors and lived experiences of civil servants, informing the development of targeted interventions to promote healthy weight management practices in this population. Hence, this study is aimed at predictors of weight management behaviour among civil servants using the health belief model as a conceptual framework.
Materials and Methods
Study Design and Period
A mixed study (sequential explanatory study) was conducted in Dessie town, which is located in the South Wollo Zone of the Amhara Region in north-central Ethiopia. The study took place from November 15 to January 20, 2022/2023 GC, and focused on civil servants in Dessie. The town is situated at a latitude and longitude of 11°8′N 39°38′E and is approximately 397 km driving distance from Addis Ababa.
Population
The source population for this study consisted of all civil servants working in Dessie town. From this source population, the study population was determined by including only those civil servants from Dessie town who met the predefined inclusion criteria.
Inclusion and Exclusion Criteria
The study included all civil servants who were present during the data collection phase. The reason why were selected since Civil servants constitute a substantial proportion of the workforce in Ethiopia and play vital roles in the public sector. Due to the nature of their work, civil servants often lead sedentary lifestyles, spending extended periods sitting at desks or engaging in minimal physical activity. However, civil servants who were unable to respond to the questionnaires due to illness were excluded from the study.
Sampling Method and Sample Size Determination
The sample size for the study was determined using the single population formula, considering the following assumptions: a 95% confidence interval (Z), a proportion of weight management behavior (P) set at 50% due to the absence of previous studies, and a margin of error (D) of 5%. Taking into account a non-response rate of 10%, the initial sample size was calculated as 384 participants. The final sample size was proposed as 423 participants. The sample size for the qualitative method was determined by the degree of saturation. This decision was based on the point where saturation was reached, as determined by adding 15 participants.
A simple random sampling method was utilized to select the participants for the quantitative study. To accomplish this, a sampling frame was prepared using the human resources data from Dessie town, and computer random generator methods were employed. On the other hand, for the qualitative study, purposive sampling was employed. Specifically, the study participants were selected using judgmental sampling, which is a type of purposive sampling technique.
Operational Definitions
Weight management behavioural intention: an indication of individual readiness/willingness/ to practice and how much effort they are planning to exert, to weight management behaviour and will be Measured five items by using a 5-point bipolar Likert scale, summed up to go the score and used as a continuous variable for further analysis.
Perceived susceptibility: Measured seven items by using a 5-point bipolar Likert scale, summed up to go the score and used as a continuous variable for further analysis.
Perceived severity: Measured eight items by using a 5-point bipolar Likert scale, summed up to go the score and used as a continuous variable for further analysis.
Perceived benefits: Measured nine items by using a 5-point bipolar Likert scale, summed up to go the score and used as a continuous variable for further analysis.
Perceived barriers: Measured five items by using a 5-point bipolar Likert scale, summed up to go the score and used as a continuous variable for further analysis.
Cues to action: Measured ten items by using a 5-point bipolar Likert scale, summed up to go the score, and used as a continuous variable for further analysis.
Self-efficacy in exercise: Measured seven items by using a 5-point bipolar Likert scale, summed up to go the score and used as a continuous variable for further analysis.
Self-efficacy in diet: Measured four items by using a 5-point bipolar Likert scale, summed up to go the score and used as a continuous variable for further analysis.
Data Collection Procedure and Quality Assurance
A self-administered questionnaire was used to collect the data. Twenty data collectors and two supervisors were recruited and they collected the data at the workplace. All data collectors were oriented for half days before the data collection period by the principal investigator on the objectives of the study and how to administer the questionnaires, the issues of verbal consent, the right not to participate in the study, and how to assist the respondents on questions that were not clear during data collection. Questionnaires were adapted from items from previous literature used.22 The questionnaires included; socio-demographic variables, Baseline characteristics of the study participants, Perceived susceptibility, perceived severity, perceived benefits, perceived barriers, cues to action, self-efficacy in exercise, and self-efficacy in diet.
For the qualitative study, the data was collected by the principal investigator using a semi-structured in-depth interview guide. After giving consent, all interviews were conducted in the Amharic language. Fifteen interviews were conducted in a private room. All interview sites were selected by the participant. The process of data collection was continued until it reached the point of saturation.
The questionnaire was initially prepared in English and then translated into Amharic. To ensure consistency, it was subsequently back-translated into English by another person. A pretest was conducted on 5% of the study population in Kombolcha town, and necessary amendments were made based on any issues related to understanding, clarity, and vocabulary. Throughout the data collection period, close supervision was maintained by supervisors. Data collectors and supervisors received one day of training on the questionnaire and the data collection process. The collected data underwent thorough checks for completeness and consistency. To enhance data quality, a double data entry method using Epidata was employed. The face validity of the questionnaire was assessed by considering the views and comments of experts in the field of health promotion. Confirmatory factor analysis was conducted to examine the convergent validity of the measurement, while reliability analysis utilizing composite reliability and Cronbach’s alpha (α) was performed to assess the internal consistency of the measurement in this study.
Rigors and Trustworthiness of the Study
Before data collection began, the researcher and advisors engaged in discussions concerning the study objectives, the confidentiality of information, the contents of the open-ended semi-structured questionnaire, and data quality management. To verify the transcription and ensure accuracy, a subset of participants was enlisted to review the transcribed data and assess if the investigator had accurately captured their perspectives. To maintain authenticity, all data were included in the final report, providing readers with a transparent understanding of the basis for the conclusions drawn. Rigor was upheld through meticulous attention to detail, adherence to procedures, and consistent accuracy throughout the research process. Peer review was conducted to enhance credibility, with trained qualitative researchers reviewing the data, analysis, interpretations, and conclusions. A session with peer researchers from similar backgrounds was conducted to ensure consistency between the data analysis and thematic development.
Throughout the data collection process, an audit trail was established, which remained intact until the member check and transcription verification was completed. Additionally, reflexivity was practiced through self-awareness and bracketing techniques. The study employed an explorative approach to gain a comprehensive understanding of the core phenomenon being investigated. To ensure dependability, meticulous documentation was maintained, minimizing spelling errors, and including all relevant documents in the final report. Transferability was addressed by providing evidence and offering a detailed description of the study, encompassing the sampling process, data analysis, and results. This comprehensive approach allows for the evaluation of the generalizability of the study’s findings.
Data Processing and Analysis
The collected data underwent thorough checks for completeness and consistency. Subsequently, the data were entered into Epidata version 4.6 and exported to Stata version 14 for analysis, conducted by the principal investigator. Descriptive analysis was employed, calculating measures such as minimum, maximum, means, and standard deviations. Simple linear regression analysis was conducted to examine the association between independent variables and weight management behaviour, preceded by tests for normality, linearity, and multicollinearity. Multiple linear regressions were performed to identify independent predictors of weight management behaviour intention, with B coefficients used to interpret effects and R2 values indicating variability in the dependent variable. Statistical significance was determined with a cut-off value of p < 0.05 and a confidence interval of 95%.
For Qualitative Data Analysis
The audio-recorded interviews were transcribed verbatim and translated into English by the principal investigator, with the translated data subsequently verified for accuracy by an independent reader. Thematic analysis was then conducted using a rigorous approach. The principal investigators meticulously reviewed the transcriptions multiple times, listening to the audio recordings repeatedly to ensure data integrity and gain a comprehensive understanding of the participants’ perspectives. Each unit of meaning was systematically labelled with a code through open coding, and similar codes were organized into meaningful categories. The data analysis process was facilitated using ATLAS.ti software version 7. The categories underwent a rigorous peer-review process and were cross-checked by the co-lead author, leading to the final creation of categories and themes. Subsequently, the report was crafted based on these categories and predefined themes aligned with the study objectives. Quotes were selectively employed to highlight each category and establish their association with respective themes. Finally, a triangulation approach was applied to integrate the quantitative findings with the qualitative findings, ensuring a comprehensive and well-rounded analysis.
Results
Confirmatory Factor Analysis of the Instrument
The results of the Confirmatory Factor Analysis (CFA) revealed the factor loadings and eigenvalues for each construct. The first construct, Intention, exhibited strong factor loadings for all its items, ranging from 0.60 to 0.71. The eigenvalue for the Intention factor was 2.16, indicating a moderate amount of variance explained by the construct. This suggests that the items related to Intention were closely associated with each other and contributed significantly to measuring the intended behaviour.
The second construct, Perceived susceptibility, demonstrated moderate factor loadings, with values ranging from 0.28 to 0.58. The eigenvalue for this construct was 1.74, indicating a relatively lower amount of variance explained compared to the other constructs. However, the items related to Perceived susceptibility still demonstrated a meaningful relationship with each other, suggesting that they collectively assessed the individual’s perception of susceptibility to a particular phenomenon.
The remaining constructs, Perceived severity, Perceived barriers, Perceived benefits, Perceived self-efficacy in dieting, and Perceived self-efficacy in exercise, all exhibited strong factor loadings for their respective items, ranging from 0.42 to 0.88. These constructs also had higher eigenvalues, ranging from 2.28 to 4.60, indicating a substantial amount of variance explained by each construct. These findings suggest that the items within these constructs were highly correlated and contributed significantly to measuring the corresponding aspects of the individual’s beliefs and perceptions. Kaiser-Meyer-Olkin Measure of Sampling Adequacy ranges from 0.81–0.95 and Bartlett’s Test of Sphericity is significant (Table 1).
 |
Table 1 Confirmatory Factor Analysis for the Components of the Application of Health Belief Model to Assess Predictors of Weight Management Behaviour Intention Among Civil Servants, Dessie Town, Ethiopia |
Reliability of the Instrument
Reliability analysis was conducted to check the internal consistency of the measurement of the health belief model using composite reliability and Cronbach’s alpha (α). The first construct, behavioural Intention, demonstrated good internal consistency with a Cronbach’s alpha coefficient of 0.79 and a composite reliability of 0.78. This indicates that the items measuring Behavioural Intention are highly reliable and consistently capture the underlying concept. The second construct, Perceived Susceptibility, also exhibited satisfactory reliability, with a Cronbach’s alpha of 0.68 and a composite reliability of 0.68. Although the reliability coefficients for Perceived Susceptibility are slightly lower than those of other constructs, they are still within an acceptable range.
Moving on to the construct of Perceived Severity, the results show strong internal consistency, as evidenced by a Cronbach’s alpha coefficient of 0.86 and a composite reliability of 0.87. This suggests that the items assessing Perceived Severity reliably measure the degree to which individuals perceive the seriousness of the health issue. Similarly, the construct of Perceived Barriers demonstrated acceptable reliability, with a Cronbach’s alpha of 0.73 and a composite reliability of 0.71. This indicates that the items capturing Perceived Barriers consistently measure the obstacles individuals perceive in adopting a particular behaviour.
Furthermore, the construct of Perceived Benefits exhibited excellent reliability, with a Cronbach’s alpha coefficient of 0.88 and a composite reliability of 0.88. This suggests that the items measuring Perceived Benefits reliably capture the advantages individuals associate with engaging in the desired behaviour. Additionally, the constructs of Perceived Self-efficacy in Dieting and Perceived Self-efficacy in Exercise both demonstrated satisfactory reliability. Perceived Self-efficacy in Dieting had a Cronbach’s alpha coefficient of 0.89 and a composite reliability of 0.90, while Perceived Self-efficacy in Exercise had a Cronbach’s alpha of 0.84 and a composite reliability of 0.82 (Table 2).
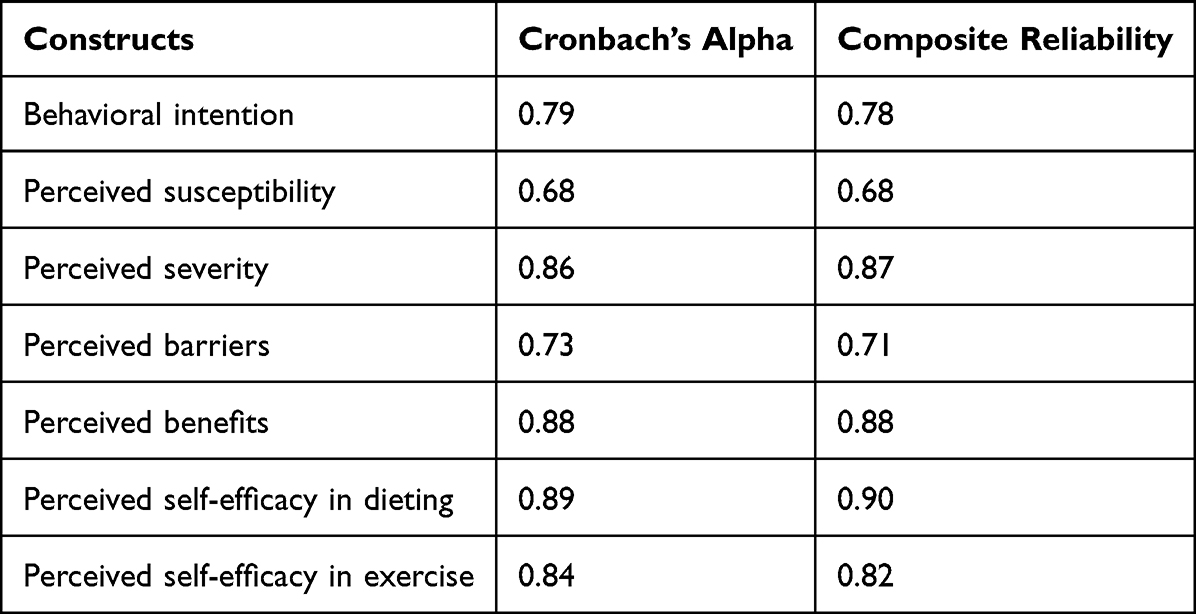 |
Table 2 Internal Consistency of Constructs of Application of Health Believe Model to Assess Predictors of Weight Management Behavior Intention Among Civil Servants, Dessie Town, Ethiopia |
Socio-Demographic Characteristics of Study Participants
A total of 410 civil servants in Dessie town participated with a response rate of 96.9%. The mean age of the respondents was 30.90 (±7.16) and the mean body mass index (BMI) of the study participants was found to be 22.98, with a standard error of 12.84. The results revealed that out of the total participants, 54.88% were male, while 45.12% were female. Regarding educational level, the majority of participants held a bachelor’s degree (68.29%), followed by a master’s degree (21.85%), and a smaller proportion had a diploma (9.86%).In terms of marital status, the participants were predominantly married (52.92%), with a considerable proportion being single (43.41%). A small percentage of participants reported being divorced (3.66%). The distribution of monthly income among the participants showed a varied range. A majority of participants had a monthly income greater than 7500 Ethiopian Birr (31.20%), followed by the income range of 2001–4000 Ethiopian Birr (27.80%). A smaller proportion had income levels ranging from 4001–7500 Ethiopian Birr (23.90%) and 1001–2000 Ethiopian Birr (13.41%) (Table 3).
 |
Table 3 Socio-Demographic Characteristics of Study Participants, Dessie Town, Ethiopia, July 2023 |
Baseline Characteristics of the Study Participants
The result revealed that among the participants, 58.54% (240 individuals) reported not having an obese family member. In terms of weight loss behavior, 52.44% (215) reported not having any prior experience, while 47.56% (195) reported having engaged in weight loss behaviour. Regarding the reasons for weight management behaviour, 48.72% (95) reported both health and better appearance as their motivation, while 43.59% (85 individuals) attributed it solely to health reasons. More half 59.76% (245) had previous exposure to diet therapy, additionally, 62.20% (255) reported having engaged in exercise therapy (Table 4).
 |
Table 4 Baseline Characteristics of the Study Participants to Application of Health Belief Model to Assess Predictors of Weight Management Behaviour Intention Among Civil Servants, Dessie Town, Ethiopia |
Descriptive Statistics for the Constructs of Health Belief Model
The mean scores and standard deviations help gauge the central tendency and variability of participants’ beliefs and attitudes toward health-related behaviours. The results indicate that the participants’ mean score for behavioural intention is 14.60, with a standard deviation of 4.42. For perceived susceptibility, the mean score is 20.26, and the standard deviation is 4.89 (Table 5).
 |
Table 5 Descriptive Statistics for the Constructs of Health Belief Model to Assess Predictors of Weight Management Behaviour Intention Among Civil Servants, Dessie Town, Ethiopia |
Predictors of the Behavioural Intention of Weight Management Behaviour
The results of the predictors of behavioural intention for weight management behaviour, based on the p-value cut-off of less than 0.05, indicate several significant associations. Females had a significantly higher behavioural intention (β = 1.27, p = 0.001) compared to males. The educational level also played a role, with individuals holding a bachelor’s degree (β = 1.80, p = 0.018) or a master’s degree (β = 2.10, p = 0.010) demonstrating higher behavioural intention than those with a diploma. Regarding marital status, being married (β = 0.43, p = 0.261) did not show a significant association with behavioural intention, while being divorced was found to have a significant negative association (β = −5.92, p = 0.000). No presence of an obese family member was significantly associated with lower behavioural intention (β = −1.50, p < 0.001). Experience in weight loss behaviour was found to be a significant predictor, with individuals without prior experience having a significantly lower behavioural intention (β = −2.241, p = 0.000) compared to those with experience. Perceived susceptibility, perceived barriers, and perceived benefits emerged as significant predictors of behavioural intention. Participants with higher levels of perceived susceptibility (β = 0.21, p = 0.000) and perceived benefits (β = 0.17, p = 0.000) had a higher intention to engage in weight management behaviours. Conversely, higher perceived barriers were associated with a lower intention (β = −0.19, p = 0.000) (Table 6).
 |
Table 6 Predictors of the Behavioural Intention of Weight Management Behaviour to Assess Predictors of Weight Management Behaviour Intention Among Civil Servants, Dessie Town, Ethiopia |
In-Depth Interview Result
The interviews revealed that individuals’ perceptions of perceived susceptibility, perceived benefits, and perceived barriers have a significant impact on their weight management behavior intention. Participants perceived themselves as susceptible to weight-related health issues and recognized the benefits of weight management. However, barriers such as time constraints and limited access to healthy options presented challenges for some participants. The presence of cues to action, such as health campaigns or social support, also played a role in triggering weight management behaviour intention.
I believe that perceived susceptibility plays a significant role in weight management behaviour intention. If individuals perceive themselves as susceptible to weight-related health issues such as diabetes or heart disease, they are more likely to prioritize weight management.
For example, one participant shared, I have a family history of diabetes, and that has made me more aware of the importance of managing my weight to prevent developing the condition. (IDP 2)
Apart from weight management, I believe these behaviours improve my physical fitness, enhance my mood, and boost my overall well-being. The idea of feeling strong, energetic, and mentally sharp drives my intention to engage in regular exercise and make healthy dietary choices. (IDI3)
I often face barriers such as temptation, particularly when I am stressed or surrounded by unhealthy food options. The availability of fast food and sugary snacks can make it difficult to stick to a healthy diet. However, I have learned to develop strategies to resist these temptations, such as planning my meals and keeping healthy snacks readily available. Despite these barriers, my weight management behaviour intention remains strong. (IDP 1)
Discussion
Weight loss maintenance has become the greatest challenge in the management of obesity. Health belief model is one of the preventive models used for public health problems such as cardiovascular disease.17 Hence, this study is aimed at predictors of weight management behaviour among civil servants using the health belief model as a conceptual framework.
The study found that females had a significantly higher behavioural intention compared to males. This finding is consistent with previous studies, conducted in Australia23 Similarly, a study conducted in the United States found that women were more likely to engage in weight loss behaviours than men24 The gender differences in behavioural intention can be influenced by cultural, social, and biological factors, which may vary across different countries. However, some studies have found no significant gender differences in weight management behaviour conducted in Iran.25
Moreover, educational level, individuals holding a bachelor’s degree or a master’s degree demonstrated higher behavioural intention compared to those with a diploma. This finding is supported by studies conducted in different countries, such as Malaysia26 and China.27 Higher educational attainment is generally associated with better health knowledge, awareness, and access to resources, which can contribute to higher behavioural intention for weight management. In contrast, a study conducted in Saudi Arabia found no significant association between educational level and weight management behaviour.28 This may be due to cultural differences or other factors specific to the Saudi Arabian population.
Being divorced was found to have a significant negative association with the behavioural intention for weight management. These findings are consistent with Studies in Japan29 found that divorced or separated individuals were less likely to engage in physical activity.
The study found that the absence of an obese family member was significantly associated with lower behavioural intention. This finding is supported by Studies in Australia30 and the United States.31 The presence of an obese family member can impact an individual’s perception of weight management, influencing their motivation and behavioural intention.
Experience in weight loss behaviour was found to be a significant predictor, with individuals without prior experience having significantly lower behavioural intention compared to those with experience. This finding aligns with a Study conducted in the United22 found that individuals with prior experience in weight loss programs were more likely to engage in weight management behaviours such as healthy eating and physical activity. Similarly, a study conducted in Australia32 found that individuals who had previously attempted weight loss were more likely to engage in physical activity and healthy eating behaviours. Previous successful weight loss attempts can enhance self-efficacy and increase motivation for continued weight management. In contrast, a study conducted in Japan33 found no significant association between prior experience in weight loss and weight management behaviour. This may be due to cultural differences or other factors specific to the Japanese population.
The study identified perceived susceptibility, perceived barriers, and perceived benefits as significant predictors of behavioural intention. These findings align with the assumptions of the Health Belief Model (HBM).34 The HBM posits that individuals are more likely to engage in health behaviors if they perceive themselves as susceptible to a health problem, believe that the benefits outweigh the barriers, and have confidence in their ability to take action. These assumptions have been supported by previous studies conducted in various countries, such as a Study conducted in the United States35 and a Study in Japan.36 This also qualitative in-depth interview of individuals’ perceptions of perceived susceptibility, perceived benefits, and perceived barriers have a significant impact on their weight management behaviour intention. Participants perceived themselves as susceptible to weight-related health issues and recognized the benefits of weight management. However, barriers such as time constraints and limited access to healthy options presented challenges for some participants. The presence of cues to action, such as health campaigns or social support, also played a role in triggering weight management behaviour intention.
Finally, the findings of this study support the policy recommendations of the World Health Organization (WHO) for weight management.37 The WHO emphasizes the importance of addressing societal, environmental, and individual factors to promote healthy lifestyles and facilitate behaviour change. The significant associations found in this study, such as gender, education, social support, experience, and perceptions, are in line with these recommendations, highlighting their relevance across different countries.
Strength and Limitation
The present study has several implications, the study utilizes a mixed-methods design, combining quantitative and qualitative methods. This comprehensive approach provides a more in-depth understanding of the predictors of weight management behaviour intention among civil servants in Dessie town, Ethiopia. Moreover, the strength of this study was the Application of Health Belief Model (HBM), the study employs the Health Belief Model, a well-established theoretical framework widely used in health behaviour research. By utilizing this model, the study provides a theoretical foundation to examine the factors influencing weight management behaviour intention. This study had some limitations, the most important of which is the cross-sectional study type, it may provide poor prediction and understanding of previous behaviour because of the time order. The study relies on self-reported data, which may be subject to recall bias or social desirability bias.
Conclusion
In summary, the study findings indicated that higher behavioural intention for weight management behaviour was associated with being female, possessing a higher educational level, no presence of an obese family member, having prior experience in weight loss behaviour, and holding favourable perceptions of susceptibility, barriers, and benefits. It is recommended that interventions and public health campaigns targeting weight management should consider these factors. Tailoring interventions to address the needs and preferences of females, individuals with higher education, those no presence of an obese family member, and individuals with prior weight loss experience, while focusing on promoting positive perceptions of susceptibility, barriers, and benefits, can potentially enhance the effectiveness of weight management programs and encourage healthier behaviours.
Abbreviations
BMI, Body Max Index; HBM, Health Belief Model; IDI, In-depth Interview.
Data Sharing Statement
All the necessary data are included in the manuscript. An English version data collection tool and detailed operational definitions of the outcome variable are accessible at a reasonable request from the corresponding author.
Ethical Approval and Consent to Participate
The current study fully complies with the ethical principles outlined in the Declaration of Helsinki. The Institutional Review Board of the School of Public Health, College of Medicine and Health Sciences at Wollo University provided ethical approval for the study. Informed consent was obtained from all participants, which included permission for publication of anonymized responses. The use of personal identification numbers and names was avoided during data collection to ensure personal anonymity. The risks, burdens, and benefits to the participants were carefully considered and were in accordance with the Declaration of Helsinki. The collected data have been kept confidential to ensure participant privacy and confidentiality. Overall, this study was conducted with high ethical standards and in accordance with the principles of the Declaration of Helsinki.
Acknowledgments
We are grateful to thank Wollo University, the College of Medicine, and the health sciences ethical review committee. Also, we want to gratify study participants and data collectors.
Funding
This investigation received no specific grant from a funding agency in the public commercial or for-profit sectors.
Disclosure
The authors declared that they have no competing interests for this work.
References
1. Zhao J, Song F, Ren S, et al. Predictors of condom use behaviors based on the health belief model (HBM) among female sex workers: a cross-sectional study in Hubei Province, China. PLoS One. 2012;7(11):e49542. doi:10.1371/journal.pone.0049542
2. Coe AB, Gatewood SB, Moczygemba LR, Beckner JO. The use of the health belief model to assess predictors of intent to receive the novel (2009) H1N1 influenza vaccine. Inov Pharm. 2012;3(2):1. doi:10.24926/iip.v3i2.257
3. Glanz K, Rimer BK, Viswanath K. Health Behavior: Theory, Research, and Practice. John Wiley & Sons; 2015.
4. Kathirvel S, Thakur JS. Sustainable development goals and noncommunicable diseases: roadmap till 2030–A plenary session of world noncommunicable diseases congress 2017. Inter J Noncommun Dis. 2018;3(1):3–8. doi:10.4103/jncd.jncd_1_18
5. Breda J, Jewell J, Keller A. The importance of the world health organization sugar guidelines for dental health and obesity prevention. Caries Res. 2019;53(2):149–152. doi:10.1159/000491556
6. Phan HD, Nguyen TNP, Bui PL, et al. Overweight and obesity among Vietnamese school-aged children: national prevalence estimates based on the world health organization and international obesity task force definition. PLoS One. 2020;15(10):e0240459. doi:10.1371/journal.pone.0240459
7. Frech A. Healthy behavior trajectories between adolescence and young adulthood. Adv Life Course Res. 2012;17(2):59–68. doi:10.1016/j.alcr.2012.01.003
8. Vella-Zarb RA, Elgar FJ. The ‘freshman 5’: a meta-analysis of weight gain in the freshman year of college. J Am Coll Health. 2009;58(2):161–166. doi:10.1080/07448480903221392
9. Tremmel M, Gerdtham U-G, Nilsson PM, Saha S. Economic burden of obesity: a systematic literature review. Int J Environ Res Public Health. 2017;14(4):435. doi:10.3390/ijerph14040435
10. Fanzo J, Hawkes C, Udomkesmalee E, et al. 2018 global nutrition report; 2019.
11. World Health Organization. World Health Organization Obesity and Overweight Fact Sheet. Geneva, Switzerland: World Health Organization; 2016.
12. Ng M, Fleming T, Robinson M, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the global burden of disease study 2013. Lancet. 2014;384(9945):766–781. doi:10.1016/S0140-6736(14)60460-8
13. World Health Organization. Women and Health: Today’s Evidence Tomorrow’s Agenda. World Health Organization; 2009.
14. Victora CG, Adair L, Fall C, et al. Maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008;371(9609):340–357. doi:10.1016/S0140-6736(07)61692-4
15. Benkeser RM, Biritwum R, Hill A. Prevalence of overweight and obesity and perception of healthy and desirable body size in urban, Ghanaian women. Ghana Med J. 2012;46(2):66–75.
16. Dagne S, Gelaw YA, Abebe Z, Wassie MM. Factors associated with overweight and obesity among adults in northeast Ethiopia: a cross-sectional study. Diabetes. 2019;391–399. doi:10.2147/DMSO.S179699
17. World Health Organization. World health organization obesity and overweight; 2011.
18. Engeland A, Bjørge T, Søgaard AJ, Tverdal A. Body mass index in adolescence in relation to total mortality: 32-year follow-up of 227,000 Norwegian boys and girls. Am J Epidemiol. 2003;157(6):517–523. doi:10.1093/aje/kwf219
19. León-Muñoz LM, Guallar-Castillón P, Graciani A, et al. Adherence to the Mediterranean diet pattern has declined in Spanish adults. J Nutr. 2012;142(10):1843–1850. doi:10.3945/jn.112.164616
20. Hruby A, Hu FB. The epidemiology of obesity: a big picture. Pharmacoeconomics. 2015;33:673–689. doi:10.1007/s40273-014-0243-x
21. Foreyt JP, Goodrick GK. Evidence for success of behavior modification in weight loss and control. Ann Intern Med. 1993;119(7_Part_2):698–701. doi:10.7326/0003-4819-119-7_Part_2-199310011-00014
22. Wadden TA, Neiberg RH, Wing RR, et al. Four‐year weight losses in the Look AHEAD study: factors associated with long‐term success. Obesity. 2011;19(10):1987–1998. doi:10.1038/oby.2011.230
23. KH-cK Y, Cornell CE, Prewitt E, et al. The WORD (Wholeness, Oneness, Righteousness, Deliverance): design of a randomized controlled trial testing the effectiveness of an evidence-based weight loss and maintenance intervention translated for a faith-based, rural, African American population using a community-based participatory approach. Contemp Clin Trials. 2015;40:63–73. doi:10.1016/j.cct.2014.11.009
24. Jeffery RW, Epstein LH, Wilson GT, Drewnowski A, Stunkard AJ, Wing RR. Long-term maintenance of weight loss: current status. Health Psychol. 2000;19(1S):5. doi:10.1037/0278-6133.19.Suppl1.5
25. Didarloo A, Shojaeizadeh D, Asl RG, Habibzadeh H, Niknami S, Pourali R. Prediction of self-management behavior among Iranian women with type 2 diabetes: application of the theory of reasoned action along with self-efficacy (etra). Iran Red Crescent Med J. 2012;14(2):86. doi:10.1016/j.diabres.2009.10.007
26. Wong JE, Yamaguchi M, Nishi N, Araki M, Wee LH. Predicting overweight and obesity status among Malaysian working adults with machine learning or logistic regression: retrospective comparison study. JMIR Format Res. 2022;6(12):e40404. doi:10.2196/40404
27. Hu L, Huang X, You C, et al. Prevalence of overweight, obesity, abdominal obesity and obesity-related risk factors in southern China. PLoS One. 2017;12(9):e0183934. doi:10.1371/journal.pone.0183934
28. Al-Rethaiaa AS, Fahmy A-EA, Al-Shwaiyat NM. Obesity and eating habits among college students in Saudi Arabia: a cross sectional study. Nutr J. 2010;9(1):1–10. doi:10.1186/1475-2891-9-39
29. Jeon CY, Lokken RP, Hu FB, Van Dam RM. Physical activity of moderate intensity and risk of type 2 diabetes: a systematic review. Diabetes Care. 2007;30(3):744–752. doi:10.2337/dc06-1842
30. Van Lippevelde W, Te Velde SJ, Verloigne M, et al. Associations between family-related factors, breakfast consumption and BMI among 10-to 12-year-old European children: the cross-sectional ENERGY-study. PLoS One. 2013;8(11):e79550. doi:10.1371/journal.pone.0079550
31. Befort CA, Nazir N, Perri MG. Prevalence of obesity among adults from rural and urban areas of the United States: findings from NHANES (2005‐2008). J Rural Health. 2012;28(4):392–397. doi:10.1111/j.1748-0361.2012.00411.x
32. Gorely T, Nevill ME, Morris JG, Stensel DJ, Nevill A. Nutrition and Physical Activity. InterJ Behav Nutrit Phys Activ. 2009;6:5. doi:10.1186/1479-5868-6-5
33. Kutsuma A, Nakajima K, Suwa K. Potential association between breakfast skipping and concomitant late-night-dinner eating with metabolic syndrome and proteinuria in the Japanese population. Scientifica. 2014;2014. doi:10.1155/2014/253581
34. Rosenstock IM. Historical origins of the health belief model. Health Educ Monogr. 1974;2(4):328–335. doi:10.1177/109019817400200403
35. Kwasnicka D, Dombrowski SU, White M, Sniehotta F. Theoretical explanations for maintenance of behaviour change: a systematic review of behaviour theories. Health Psychol Rev. 2016;10(3):277–296. doi:10.1080/17437199.2016.1151372
36. Inoue H, Yamakawa-Kobayashi K, Suzuki Y, Nakano T, Hayashi H, Kuwano T. A case study on the association of variation of bitter-taste receptor gene TAS2R38 with the height, weight and energy intake in Japanese female college students. J Nutr Sci Vitaminol. 2013;59(1):16–21. doi:10.3177/jnsv.59.16
37. Jayawardena R, Jeyakumar DT, Misra A, Hills AP, Ranasinghe P. Obesity: a potential risk factor for infection and mortality in the current COVID-19 epidemic. Diab Metab Synd. 2020;14(6):2199–2203. doi:10.1016/j.dsx.2020.11.001
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.