Back to Journals » Psychology Research and Behavior Management » Volume 16
Application of Cognitive Emotion Regulation Questionnaire in Chinese Community Elderly
Authors Ding Z, Song Q, Chu J, Zou T, Zheng K, Liu Z, Peng W, Yi J ![]()
Received 12 December 2022
Accepted for publication 4 March 2023
Published 15 March 2023 Volume 2023:16 Pages 829—839
DOI https://doi.org/10.2147/PRBM.S401087
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Zixia Ding,1,2,* Qian Song,1,2,* Jun Chu,1,2 Tao Zou,3 Kaili Zheng,1,2 Zhaoxia Liu,1,2 Wanrong Peng,1,2 Jinyao Yi1,2,4
1Medical Psychological Center, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410011, People’s Republic of China; 2Medical Psychology Institution, Central South University, Changsha, Hunan, 410011, People’s Republic of China; 3Department of Psychiatry, The Affiliated Hospital of Guizhou Medical University, Guiyang, Guizhou, 550004, People’s Republic of China; 4National Clinical Research Center for Mental Disorders, Changsha, Hunan, 410011, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jinyao Yi, Medical Psychological Center, The Second Xiangya Hospital, Central South University, Changsha, Hunan, 410011, People’s Republic of China, Email [email protected]
Background: The present study investigated the applicability of the Cognitive Emotion Regulation Questionnaire (CERQ) in the Chinese community elderly and explored the influence of cognitive emotion regulation strategies on late-life depression.
Methods: A total of 367 community elderly aged 60– 94 were deemed eligible and completed CERQ, the Perceived Stress Scale-10, the Geriatric Depression Questionnaire-15, and the State Anxiety Inventory. Confirmatory factor analysis was adopted to verify the 9-factor structure of CERQ. Cronbach’s α coefficient, Ω coefficient and split-half reliability were used to test the internal consistency of CERQ. Pearson correlations among scores of CERQ and other scales were calculated to examine its convergent validity. In addition, a structural equation model was used to further examine the effect of cognitive emotion regulation strategies on the association between perceived stress and late-life depression.
Results: All the fitting indexes of CERQ’s 9-factor model met the criterion (χ2/df= 2.26, CFI= 0.916, TLI= 0.904, RMSEA= 0.052). For the total score of CERQ, the Cronbach’s α coefficient and Ω coefficient were both 0.90, and the split-half reliability was 0.74. For the nine subscales, the α coefficients ranged from 0.66 to 0.88, and the Ω coefficients ranged from 0.69 to 0.88. Significant positive correlations were found between the maladaptive dimension of CERQ and other scales (all p < 0.001). The maladaptive emotion regulation strategies indirectly affected the effect of perceived stress on late-life depression (effect size was 21.57%).
Conclusion: With good reliability and factor validity, the CERQ showed good applicability in the Chinese elderly population. The influence of perceived stress on depression in the elderly was mediated by maladaptive emotion regulation strategies.
Keywords: cognitive emotion regulation, late-life depression, perceived stress, psychometric properties, mediating effect
Introduction
With the continuous expansion of the elderly population, the psychological health problems in the elderly have become increasingly prominent and received widespread attention. In China, depression has been one of the most common mental illnesses among the elderly, and the prevalence of depressive disorders is as high as 3.8% for those over 64 years of age.1 Depression reduces the quality of late life and increases the probability of various diseases, and severe depressive symptoms may even trigger suicide and other life-threatening behaviors.2 Abundant as the studies focusing on risk factors of depression are, little attention has been paid to the elderly population. Compared with younger groups, elderly people are faced with the decline of physical function, the transformation of social roles, and more loss events, resulting in great stress and increased risk of depression.3 Therefore, it is of great significance to explore the relevant factors and their underlying mechanism that affect depression in the elderly.
Previous research has established that the characteristics of emotion regulation have an important impact on the mental health of the elderly.4 Emotion regulation refers to the cognitive or behavioral process in which individuals consciously or unconsciously evaluate and adjust what kinds of emotions they have when they have them, and how to experience and express these emotions.5 Studies have verified that effective emotion regulation could help individuals cope with stress, adapt to the social environment, and enhance happiness,5,6 while maladaptive emotion regulation would hinder the development of mental health and has been regarded as a predisposing factor of emotional disorders.7 A meta-analysis confirmed that there is a close relationship between maladaptive emotion regulation strategies and depressive symptoms.8 For the elderly, positive reappraisal is related to mental health,9 while rumination is strongly associated with anxiety and depression.4 Therefore, it is of great significance to study the emotion regulation of the elderly to prevent their emotional problems.
Meanwhile, the prerequisite for carrying out research on emotion regulation is to take effective and precise measurements of emotion regulation. At present, there are a number of self-reported questionnaires available for measuring the characteristics of emotion regulation. For example, Gross and John divided emotion regulation into two dynamic processes, cognitive reappraisal and expression inhibition, and thus compiled the Emotion Regulation Questionnaire.5 Additionally, Gratz and Roemer designed the Difficulties in Emotion Regulation Scale to assess whether the individual has problems in understanding, regulating and accepting emotions.10 However, most tools mentioned above cannot directly and specifically measure the cognitive process of emotion regulation. Garnefski focused on the individual’s cognitive effort when adapting to external (such as criticism) or internal (such as memory) stimuli, and developed the Cognitive Emotion Regulation Questionnaire (CERQ).11 As a self-report scale assessing the individual cognitive processes under negative emotions, the CERQ includes 36 items, which is subdivided into 9 different cognitive strategies: (1) acceptance (eg, I think that I have to accept the situation); (2) positive refocusing (eg, I think about pleasant experiences); (3) refocus on planning (eg, I think of what I can do best); (4) positive reappraisal (eg, I look for the positive sides to the matter); (5) putting into perspective (eg, I tell myself that there are worse things in life); (6) self-blame (eg, I feel that I am the one to blame for it); (7) rumination (eg, I dwell upon the feelings the situation has evoked in me); (8) catastrophizing (eg, I continually think how horrible the situation has been); (9) blaming others (eg, I feel that others are to blame for it). Among them, the first 5 types are considered as adaptive dimensions (CERQ-Adaptive), and the last 4 types constitute maladaptive dimensions (CERQ-Maladaptive).
Up to now, the CERQ has been widely used and shown good psychometric characteristics in many countries, such as in Netherlands,11 the United States,12 France,13 and Spain.14 It is worth noting that only a few studies have examined the psychometric characteristics of CERQ in the elderly.14,15 In the Dutch elderly, the CERQ had good internal consistency reliability (Cronbach’s α= 0.76–0.82), and the 9 subscales explained 69.80% of the variance variation.15 In the Spanish elderly, the CERQ had good factorial validity and all CERQ subscales showed acceptable test–retest reliability, except for self-blame.14 In China, the CERQ has only been validated with good reliability and validity in samples of college students and hypertensive patients,16,17 while its psychometric properties have not been examined in the elderly population. Therefore, it is essential to verify the reliability and validity of the Chinese version of CERQ in the elderly.
Since previous studies have proved the good psychometric properties of CERQ for assessing cognitive emotion regulation in various populations,15,17 some researchers used the CERQ to explore the relationship between cognitive emotion regulation and depression.18,19 For instance, Stikkelbroek found that adolescents who tend to adopt maladaptive emotion regulation strategies had difficulty maintaining a good mental health status in stressful situations, and their risk of depression would be higher.19 Yan found that the catastrophizing (one of the maladaptive emotion regulation strategies) as a potential factor influencing the relationship between daily stress and depressive symptoms in university students.18 These findings are consistent with Raio’s opinion that acute stressful stimuli significantly would impair the efficacy of cognitive emotion regulation, which in turn might enhance individuals’ mental vulnerability.20 However, it is still not certain whether the role of cognitive emotion regulation in the relationship between stress and depression also exists in the elderly, which needs to be clarified and will help to explore the related mechanisms of late-life depression.
Hence, firstly, this study aimed to examine the reliability and validity of CERQ among the elderly in the Chinese community, which would provide an effective measurement tool for related research on cognitive emotion regulation of the elderly in China. Secondly, this study would further explore the role of cognitive emotion regulation strategies in the relationship between perceived stress and late-life depression, which might of great value for the prevention and treatment of depression in the elderly.
Materials and Methods
Participants
Elderly subjects were recruited from several communities in Guizhou and Hunan provinces of China from October to December 2019. The recruitment criteria were as follows: (1) age being or above 60 years, (2) able to understand and answer questions, (3) without neurological disease or serious physical disease of heart, liver, kidney, etc., and (4) without severe mental disorders (eg, major depression, bipolar disorder, schizophrenia).21 All recruited subjects were screened to exclude cognitive impairment by a professional clinical psychologist, and then asked to complete a series of self-report psychological scales. A total of 392 community elderly were recruited in this study, 25 of them were excluded from the final analysis (5 with cognitive impairment and 20 with more than 10% of CERQ missed). Eventually, a cohort of 367 valid samples were included in this research, their ages ranging from 60 to 94 years (mean= 69.11, SD= 6.43). The sample was composed of 115 males (31%; with mean age 70.55 ± 6.42 years) and 252 females (69%; with mean age 68.45 ± 6.33 years). The majority of the subjects reported a level of elementary and secondary education (34% primary school level, 32% junior high school level, 20% senior high school level or equivalent, 10% college level, 4% bachelor degree or above) and most participants (76%) were married. There were significant gender differences in age (t (365) = 2.91, p< 0.01) and education level (χ2= 10.50, p< 0.01), males were older and had higher education level than females (both p< 0.01).
This study was approved by the Ethics Committee of the Second Xiangya Hospital of Central South University. All the subjects participated voluntarily and signed the informed consent prior to enrollment.
Instruments
Cognitive Emotion Regulation Questionnaire (CERQ)
The CERQ is a multi-dimensional measurement instrument to evaluate the cognitive emotion regulation strategies that people adopt after experiencing negative or stressful events.11 It contains 36 items and uses a five-level scoring (1= never to 5= always). Individual subscale scores are obtained by summing the scores of their respective items. The score of each subscale represents the degree of use of a certain strategy. A higher score indicates a higher likelihood to use this strategy when coping with stressful events. The Chinese version of CERQ has shown good psychometric properties in undergraduates, and the Cronbach’s α coefficient of each subscale was between 0.76 and 0.90.17
Perceived Stress Scale-10 (PSS-10)
The PSS-10 is revision of the standard version of the Perceived Stress Scale, which assesses individual’s perceived stress level in the last month.22,23 It consists of 10 items and uses a five-level scoring (0= never to 4= always), with the total score being from 0 to 40. A higher score in the PSS-10 indicates a higher perceived stress level. The PSS-10 showed good reliability in this study (Cronbach’s α= 0.74).
Geriatric Depression Scale-15 (GDS-15)
The GDS-15 is a 15-item self-report scale that evaluates the older individuals’ severity of depression.24,25 Each item uses binary scoring (1= Yes; 0= No). The total score is between 0 and 15 points, with higher scores indicating more severe depressive symptoms. The Cronbach’s α coefficient of GDS-15 in this study was 0.74.
State Anxiety Inventory (SAI)
The SAI is a 20-item self-reported scale that assesses the degree of anxiety that an individual currently perceives.26,27 Each item is rating from 1 to 4, and the total score is ranging from 20 to 80, with higher scores indicating higher anxiety levels. In this study, the SAI obtained excellent internal consistency reliability (Cronbach’s α= 0.91).
Statistical Analyses
Preliminary analyses were performed in SPSS version 25, while confirmatory factor analysis (CFA) and structural equation model (SEM) were conducted in M-Plus version 8.3.
Firstly, to investigate the applicability of the 9-factor structure of CERQ in community elderly samples, CFA was conducted to assess the 9-factor structure of CERQ. The maximum likelihood method was adopted since the vast majority of items met the assumption of approximate normality. The Comparative Fit Index (CFI), Tucker–Lewis Index (TLI), Root Mean Square Error of Approximation (RMSEA) with a 90% Confidence Interval (CI), and Standardized Root Mean Squared Residual (SRMR) were employed to assess model fit. As recommended by Hu and Bentler, a satisfactory model should meet the following criteria: CFI and TLI being greater than 0.90, RMSEA and SRMR being less than 0.08.28 Meanwhile, the explanatory capacity of each item on latent factor was assessed through the standardized regression coefficient. If the standardized regression coefficient is greater than 0.50, the explanatory power of the factor to the variation of the observed variable is acceptable.29
To evaluate the internal consistency of CERQ, the Cronbach’s α and Omega (Ω) coefficients of the total scale and each subscale of CERQ were first calculated to test the consistency among the scores of each item, and the split-half reliability was then calculated by dividing the CERQ items into two halves.
In addition to descriptive statistics, t-tests were also performed to compare the group differences between males and females in CERQ, PSS-10, GDS-15, and SAI. Cohen’s d was used to assess the effect size of group differences. An absolute value of Cohen’s d between 0.20 and 0.50 indicates small effect size, a value between 0.50 and 0.80 represents middle effect size, while a value greater than 0.80 shows large effect size.30
Afterwards, considering the cultural specificity of emotion regulation, to explore the differences in emotional regulation characteristics of the elderly in different countries, the present study compared the Chinese sample with the Dutch sample used to develop the original version of CERQ.15 One-sample t-tests were adopted to compare mean differences between the scores of the Chinese sample and those of the Dutch sample. To examine the preference of the elderly in using cognitive emotion regulation strategies, repeated measure analysis of variance (ANOVA) was utilized with one within-subjects factor (adaptive strategies vs maladaptive strategies). Partial η2 was calculated to assess the effect size of group differences.31
Finally, to investigate the effects of emotion regulation strategies on the relationship between perceived stress and depression, Pearson correlations were performed among CERQ-Adaptive, CERQ-Maladaptive, PSS-10, GDS-15 and SAI, and a SEM was then constructed for the latent variables of emotion regulation strategies, perceived stress, and depression. Due to the high comorbidity of anxiety and depression,32 individual’s anxiety level was covaried in the model to exclude the influence of anxiety on the results. The bias corrected bootstrap confidence intervals was used to evaluate the mediation effect of emotion regulation strategies on the relationship between perceived stress and depression. If the calculated 95% confidence interval does not include 0 with repeated sampling 5000 times, the mediating effect is significant.33 The SEM fit was evaluated by the fit indices and the path coefficients, the same criterion as those of CFA.
Results
Structure Validity
The CFA results showed that the nine-factor model fitted the data well (χ2 = 1262.80, df = 558, χ2/df = 2.26, CFI = 0.916, TLI = 0.904, RMSEA = 0.052 (90% CI = 0.048–0.057), SRMR = 0.063), with all the model fit indexes being in line with the measurement standard. The standardized regression coefficients ranged from 0.53 to 0.86, except for item 2 and item 7 (both were 0.42), see Figure 1. Correlations among the nine latent factors of CERQ ranged from 0.01 to 0.80, see Table 1.
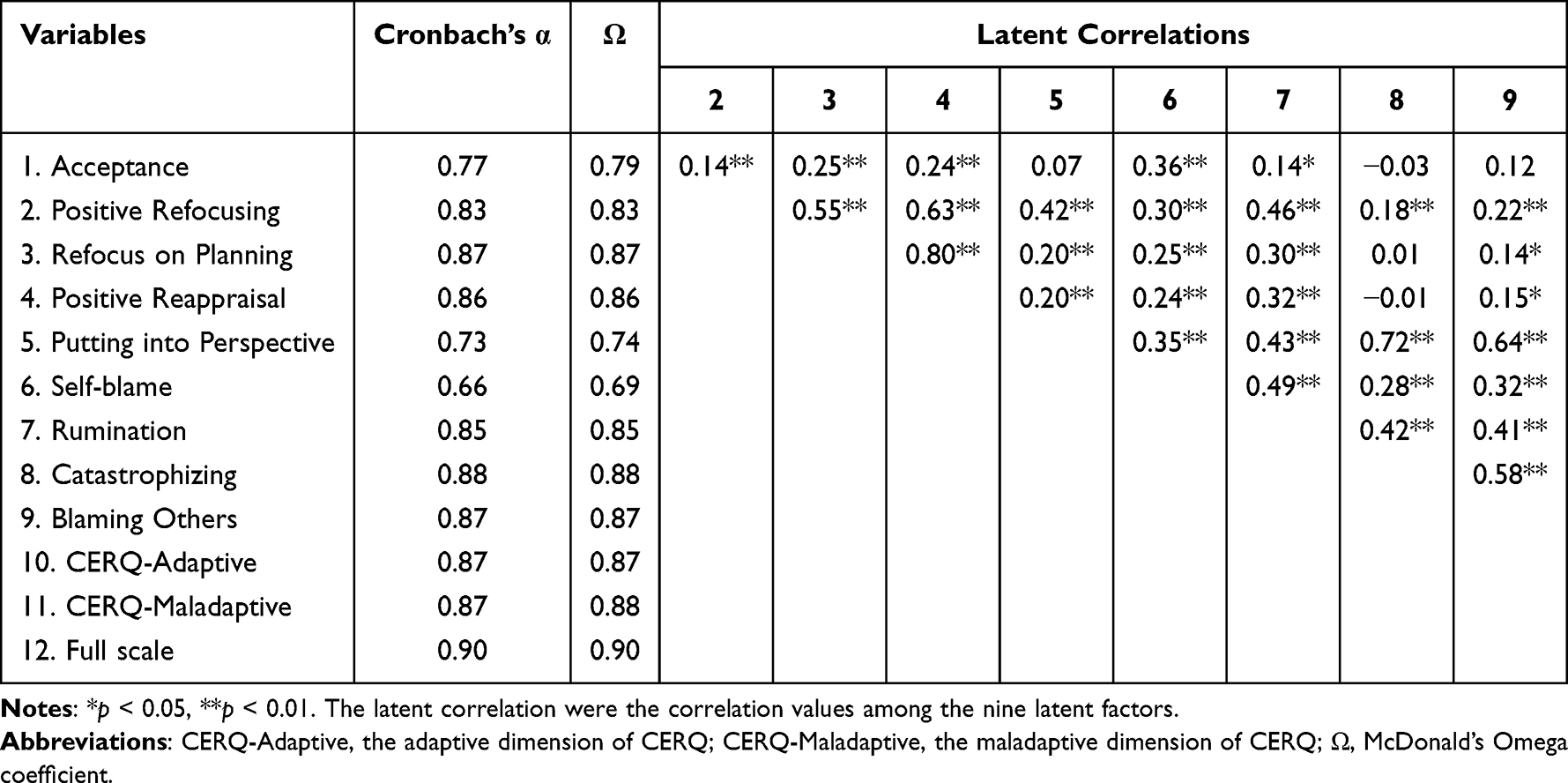 |
Table 1 Internal Consistency and Latent Correlations Between Subscales of CERQ |
 |
Figure 1 Complete standardized model for the CERQ in Chinese community elderly. Note: The scores shown on the straight line were the standardized regression coefficient of each item in their latent variable. |
Internal Reliability
As shown in Table 1, the Cronbach’s alpha coefficient of the whole scale was 0.90, and those of the subscales ranged from 0.66 to 0.88. The Ω coefficient was 0.90 for the total scale and ranged from 0.69 to 0.88 for the nine subscales. The Cronbach’s alpha coefficients of two dimensions of CERQ (CERQ-Adaptive and CERQ-Maladaptive) were both 0.87, and the Ω coefficients were 0.87 and 0.88 respectively. The split-half reliability of CERQ was 0.74.
Descriptive Statistics and Gender Differences in Psychological Variables
As shown in Table 2, elderly females got significantly higher scores in refocusing on planning, positive reappraisal and rumination than elderly males, while no significant gender differences were found in other CERQ subscales. Significant gender differences were also found in the scores of PSS-10, with elderly females scoring significantly higher than elderly males, while no significant gender differences were found in GDS-15 and SAI.
 |
Table 2 Gender Differences in Psychological Variables |
Characteristics of Cognitive Emotional Regulation in the Elderly
A comparison of the mean scores of the Chinese elderly with the mean scores of the Dutch elderly15 in the nine subscales was performed by one-sample t-tests. As shown in Figure 2, Chinese elderly reported significantly higher scores than Dutch elderly in almost all the subscales, but scored significantly lower only in putting into perspective. In addition, the scores of CERQ-Adaptive were significantly higher than those of CERQ-Maladaptive in Chinese elderly (F = 543.77, p< 0.001), with a large effect size (partial η2 = 0.60, > 0.14).
 |
Figure 2 Mean comparison in the nine subscales of CERQ between Chinese elderly and #Dutch elderly. Abbreviations: SB, self-blame; Rum, rumination; Cat, catastrophizing; OB, Other blame; Acc, acceptance; R-Plan, refocus on planning; P-Rea, positive reappraisal; PP, putting into perspective; M, mean; t, t values of one-samplet-tests; |Cohen’s d|, absolute value of Cohen’s d. Notes: #The results of Dutch elderly were quoted from the literature published by Garnefski & Kraaij (2006). ***p < 0.001. |
Correlations Between CERQ and Other Scales
As illustrated in Table 3, the CERQ-Maladaptive was positively correlated with PSS-10, GDS-15 and SAI, the PSS-10 positively correlated with GDS-15 and SAI, and the GDS-15 positively correlated with SAI. Although the CERQ-Adaptive was significantly correlated with CERQ-Maladaptive, it had no significant correlations with PSS-10, GDS-15 and SAI (p value was 0.926, 0.541 and 0.100, respectively, all > 0.05).
 |
Table 3 Pearson Correlations Between CERQ and Other Scales |
Pathway Analysis of Perceived Stress, Maladaptive Emotion Regulation and Depression
Since the CERQ-Adaptive had no significant correlations with PSS-10, GDS-15 and SAI, the SEM was just constructed among PSS-10, CERQ-Maladaptive and GDS-15, with SAI as covariate. The SEM was well fitted with the data: χ2 = 115.50, df = 40, CFI = 0.952, TLI = 0.932, SRMR = 0.046, RMSEA = 0.065 (90% CI = 0.049–0.081). In this SEM, there were two pathways through which perceived stress affected depression: the standardized pathway coefficient of “perceived stress → depression” being 0.40 (p< 0.001); the standardized path coefficient of “perceived stress → maladaptive emotion regulation → depression” being 0.55 × 0.20 = 0.11 (p = 0.029), see Figure 3.
 |
Figure 3 The mediating model of maladaptive emotion regulation between perceived stress and depression. Abbreviation: ER, emotion regulation. Notes: The anxiety was defined as covariate variable in the structural equation model. *p < 0.05, ***p < 0.001. |
The direct effect of perceived stress on depression was significant, and its mediating effect through maladaptive emotion regulation strategy on depression was also significant (95% confidence interval did not overlap with zero; Table 4), which suggested that maladaptive emotion regulation played a partial mediating role in the relationship between stress and depression. The standardized amount of indirect effect was 0.11, which accounted for 21.57% of the total effect.
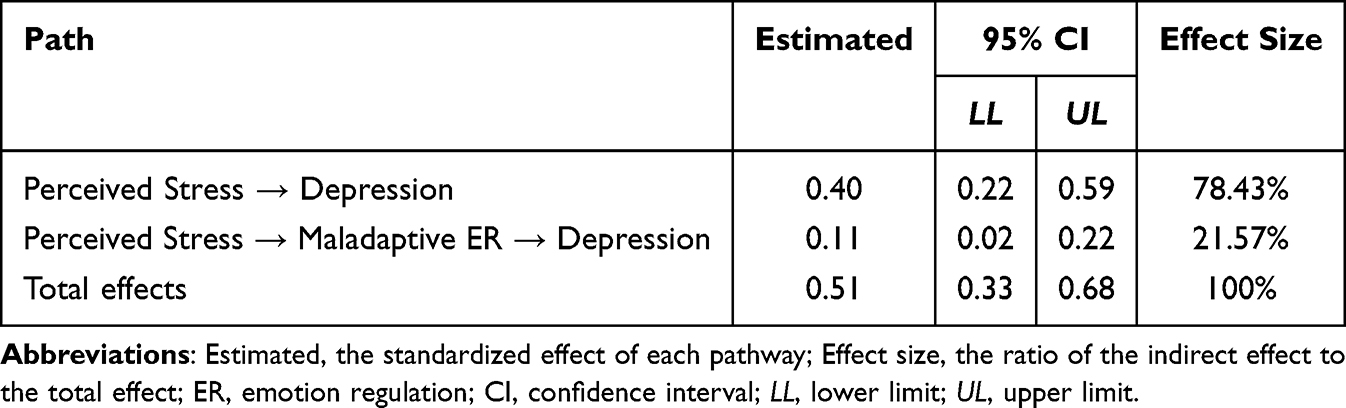 |
Table 4 Standardized Indirect Effects and 95% Confidence Intervals |
Discussion
This study is the first one to examine the reliability and validity of CERQ in the Chinese elderly population, and the first one to explore the role of cognitive emotion regulation strategies in the relationship between perceived stress and depression in the community elderly, which not only expands the population scope of application of CERQ, but also further clarifies the risk factors and influencing mechanisms of late-life depression and provides a valuable scientific basis for the prevention and treatment of depression in the elderly.
In this study, the results of CFA indicated that the 9-factor structure of CERQ had a good match with the data of the elderly sample, which further proved good structural validity of CERQ in the elderly population in China. Our results were basically consistent with the model fitting results of the 9-factor structure obtained in a sample of Chinese college students.17 Among the elderly in Spain, the 9-factor structure of CERQ has been supported repeatedly in the 36-item version and the 27-item version, respectively.14 Combined with the results of previous studies, it is suggested that the 9-factor structure of CERQ is stable and effective.
Moreover, the CERQ showed good reliability among the elderly in the Chinese community. The Cronbach’s α, Ω and split-half reliability coefficients of the total CERQ were all good. The Cronbach’s α coefficient of each subscale was acceptable, while the Cronbach’s α coefficient of self-blame was relatively low. According to the results of Zhu et al, the α coefficient of self-blame was also the lowest among the 9 subscales in the sample of Chinese college students (α= 0.76).17 In addition, the results of internal consistency of each subscale in this study were similar to those of previous studies, such as the Dutch (α= 0.66 to 0.83),11 French (α= 0.68 to 0.87),13 and English (α = 0.65 to 0.81)12 versions of CERQ. As for Ω coefficient, self-blame was only slightly less than 0.70 (Ω= 0.69). Overall, this study relatively consistently supported that the CERQ has good internal consistency reliability among the Chinese community elderly.
There were significant gender differences in the use of emotion regulation strategies. The elderly females’ scores on rumination, refocus on planning, and positive reappraisal were significantly higher than those of elderly males. Previous studies have demonstrated that women tend to pay more attention to their own emotional experiences and use more internally focused responses to their emotions than men.34,35 Our results provided further evidences for these gender differences, however, which might be somewhat limited by the uneven number of men and women in our sample (68.66% female), more studies with larger sample are needed to verify the replication of these gender differences.
As for the mean difference between the current sample and the Dutch elderly sample,15 the Chinese elderly reported significantly higher mean scores for almost all cognitive emotion regulation strategies than the Dutch elderly, which might be due to the differences in cultural values between the East and the West. Under the culture of individualism and egalitarianism, people are more likely to adjust their emotions by changing the external environment,36 while under the culture of collectivism, large power distance and high hierarchy, although people may choose to suppress emotional expression in order to maintain group harmony,37 they are also encouraged to adopt more internal adjustments to accept the imbalance of social power distribution.36 Therefore, compared with the Dutch elderly, the Chinese elderly may be more inclined to adopt cognitive and internal coping methods to regulate emotions. However, it should be noted that the difference between the Chinese elderly and the Dutch elderly might be affected by the response style, and individuals in different cultures may have different response styles to CERQ. Meanwhile, since the Dutch elderly data were published in 2006, more than a decade earlier than this study, the accuracy of these results needs to be tested in the future.
This study also found that compared with maladaptive emotion regulation strategies, the elderly was more inclined to adopt adaptive emotion regulation strategies to a large extent (partial η2= 0.60). Similar, pattern of cognitive strategies had been found in the Dutch elderly.15 One of the possible explanation is that in the experience of aging, when the elderly used adaptive emotion regulation strategies to cope with stressful events, they gradually realized the benefits and learned effective ways of using them, so that the elderly would use the adaptive cognitive coping style more frequently and effectively.9 Also, the elderly subjects in our study were all from the community and belonged to a healthier group compared with clinical subjects. According to the emotional regulation choice theory, healthy individuals generally exhibit the characteristics of selective adaptive regulation in the process of regulating emotions,38 our results provided further supports for this theory. These findings suggest that individual differences in cognitive emotion regulation selection warrant further investigation.
In this study, Pearson correlations analysis found moderate to high correlations among maladaptive emotion regulation strategies, perceived stress, depression, and anxiety. These results suggested that the maladaptive dimension of CERQ had good convergent validity, which could partially explain why individuals who use more maladaptive emotion regulation strategies would feel stronger negative emotions. Besides, previous studies found that maladaptive emotion regulation strategies (such as rumination, catastrophizing, and self-blame) were the most valuable predictors of negative mood39,40 and had stronger and more stable correlations with psychopathology than adaptive strategies did,4,9 which has been verified further in this study.
The current study confirmed that perceived stress could significantly positively predict depression in the elderly, consistent with previous studies reporting that perceived stress could increase the risk of depression.41,42 The path analysis found that perceived stress could not only directly predict depression, but also indirectly affect depression through maladaptive emotion regulation strategies. The conceptualization of maladaptive emotion regulation strategies as a potential pathway linking stress to depression vulnerability has been supported by previous findings.19,43 Generally speaking, high-stress perception may disturb the individual’s normal process of adapting to stimuli, resulting in impaired ability to process negative information and more difficulties in emotional regulation.44 Therefore, individuals with high levels of perceived stress are more likely to repeatedly and passively pay attention to negative stimuli when dealing with negative events, fall into redundant thinking, constantly blaming themselves and others, and even amplify negative effects and terrible consequences, while unable to regulate their negative emotions effectively,45 which greatly increases the risk of depression and may lead to longer lasting and more severe depressive symptoms.7,41 Our results of path analysis further supported that maladaptive emotion regulation strategies could aggravate the negative impact of perceived stress on depression in the elderly.
This study might promote the application of CERQ in identifying the habitual and rigid emotion regulation strategies in the elderly, and carry important clinical significance for the prevention and intervention of depression in the elderly. First, considering the role of perceived stress in developing and maintaining depressive symptoms, clinical interventionists should focus on relieving stress in the elderly and teaching them how to cope with or reevaluate stress. Second, maladaptive emotion regulation strategies may be the vital targets for the prevention and intervention of late-life depression. A series of emotion regulation intervention methods (such as cognitive-behavioral therapy, mindfulness-based therapy, and emotional focus therapy, etc.) should be adopted to help the elderly identify their maladaptive emotion regulation strategies and replace them with more effective strategies to prevent and slow down the occurrence and development of depression.46
Several limitations should be noted in this study. First, this study only sampled in some communities in two provinces, which may cause the results not generalizable to the rest of the Chinese elderly population. Future studies should expand the scope of sampling and strengthen the sample representativeness. Second, our sample size was relatively small, and gender of the sample was unevenly distributed, which makes it difficult to determine whether the reported difference is attributable to the actual gender difference or the different structure of measurement in different groups. Future studies should expand the sample size and perform measurement equivalence analysis of CERQ across gender. Third, this study adopted a cross-sectional design, which cannot verify the causal relationship among cognitive emotion regulation strategies and other variables. Future studies should adopt longitudinal designs and more diverse samples (ie, clinical vs community) to clarify the causal effects among these variables.
Conclusions
Overall, this study supports the good reliability and validity of CERQ in the Chinese community elderly, evidences both high-stress perception and maladaptive emotion regulation strategies being risk factors for depression in the elderly, and confirms the mediating effect of cognitive emotion regulation strategies on the relationship between perceived stress and late-life depression.
Data Sharing Statement
The datasets of this study are available from the corresponding author. Due to privacy or ethical restrictions, the datasets cannot be made public.
Ethics Approval and Informed Consent
This research was approved by the Medical Ethics Committee of the Second Xiangya Hospital, Central South University. The procedures performed were in accordance with the Declaration of Helsinki. All the subjects participated voluntarily and signed the informed consent at enrollment.
Acknowledgment
We thank all subjects for their contributions to this research.
Funding
This work was supported by the National Natural Science Foundation of China (Grant number: 81871074); and the Fundamental Research Funds for the Central Universities of Central South University (Grant number: 2022ZZTS0028, 2022ZZTS0918); and the Hunan Provincial Innovation Foundation for Postgraduate (Grant number: CX20220119).
Disclosure
The authors declare no conflict of interest.
References
1. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
2. Szanto K, Galfalvy H, Kenneally L, Almasi R, Dombrovski AY. Predictors of serious suicidal behavior in late-life depression. Eur Neuropsychopharmacol. 2020;40:85–98.
3. Yadav K, Mishra S. A study about depression and stress among older people. Res Dev. 2016;1:7–11.
4. Ramirez-Ruiz B, Quinn K, Ferreira N. Emotion-regulation strategies in older people: a systematic review. Work Old Ppl. 2020;24(1):1–18.
5. Gross JJ, John OP. Individual differences in two emotion regulation processes: implications for affect, relationships, and well-being. J Pers Soc Psychol. 2003;85(2):348–362.
6. McRae K, Mauss IB. Increasing positive emotion in negative contexts: emotional consequences, neural correlates, and implications for resilience. In: Greene JD, Morrison I, Seligman MEP, editors. Positive Neuroscience. Oxford: Oxford University Press; 2016:159–174.
7. Yoon S, Rottenberg J. Why do people with depression use faulty emotion regulation strategies? Emot Rev. 2020;12(2):118–128.
8. Visted E, Vøllestad J, Nielsen MB, Schanche E. Emotion regulation in current and remitted depression: a systematic review and meta-analysis. Front Psychol. 2018;9:765.
9. Nowlan JS, Wuthrich VM, Rapee RM. The impact of positive reappraisal on positive (and negative) emotion among older adults. Int Psychogeriatr. 2016;28(4):681–693.
10. Gratz KL, Roemer L. Multidimensional assessment of emotion regulation and dysregulation: development, factor structure, and initial validation of the difficulties in emotion regulation scale. J Psychopathol Behav Assess. 2004;26(1):41–54. doi:10.1023/B:JOBA.0000007455.08539.94
11. Garnefski N, Kraaij V, Spinhoven P. Negative life events, cognitive emotion regulation and emotional problems. Pers Individ Dif. 2001;30(8):1311–1327. doi:10.1016/S0191-8869(00)00113-6
12. Martin RC, Dahlen ER. Cognitive emotion regulation in the prediction of depression, anxiety, stress, and anger. Pers Individ Dif. 2005;39(7):1249–1260.
13. Jermann F, Van Der Linden M, D’Acremont M, Zermatten A. Cognitive Emotion Regulation Questionnaire (CERQ): confirmatory factor analysis and psychometric properties of the French translation. Eur J Psychol Assess. 2006;22(2):126–131.
14. Carvajal BP, Molina-Martínez MÁ, Fernández-Fernández V, Paniagua-Granados T, Lasa-Aristu A, Luque-Reca O. Psychometric properties of the Cognitive Emotion Regulation Questionnaire (CERQ) in Spanish older adults. Aging Ment Heal. 2020;26(2):413–422.
15. Garnefski N, Kraaij V. Relationships between cognitive emotion regulation strategies and depressive symptoms: a comparative study of five specific samples. Pers Individ Dif. 2006;40(8):1659–1669.
16. Duan S, Liu Y, Xiao J, Zhao S, Zhu X. Cognitive emotion regulation questionnaire in hypertensive patients. J Cent South Univ Med Sci. 2011;36(6):532–538.
17. Zhu X, Auerbach RP, Yao S, Abela JJRZ, Xiao J, Tong X. Psychometric properties of the cognitive emotion regulation questionnaire: Chinese version. Cogn Emot. 2008;22(2):288–307.
18. Demir Z, Böge K, Fan Y, et al. The role of emotion regulation as a mediator between early life stress and posttraumatic stress disorder, depression and anxiety in Syrian refugees. Transl Psychiatry. 2020;10(1):1–10.
19. Stikkelbroek Y, Bodden DH, Kleinjan M, Reijnders M, van Baar AL. Adolescent depression and negative life events, the mediating role of cognitive emotion regulation. PLoS One. 2016;11(8):e0161062.
20. Raio CM, Orederu TA, Palazzolo L, Shurick AA, Phelps EA. Cognitive emotion regulation fails the stress test. Proc Natl Acad Sci USA. 2013;110(37):15139–15144.
21. World Health Organization. Guidelines for the Management of Physical Health Conditions in Adults with Severe Mental Disorders. Geneva: World Health Organization; 2018.
22. Cohen S, Kamarck T, Mermelstein R, Global A. Measure of Perceived Stress. J Health Soc Behav. 1983;24(4):385–396.
23. Huang F, Wang H, Wang Z, et al. Psychometric properties of the perceived stress scale in a community sample of Chinese. BMC Psychiatry. 2020;20(1):1–7.
24. Cheng S-T, Chan ACM. A brief version of the geriatric depression scale for the Chinese. Psychol Assess. 2004;16(2):182–186.
25. Sheikh JI, Yesavage JA. Geriatric Depression Scale (GDS): recent evidence and development of a shorter version. J Aging Ment Heal. 1986;1986:1.
26. Shek DTL. Reliability and factorial structure of the Chinese version of the State-Trait Anxiety Inventory. J Psychopathol Behav Assess. 1988;10(4):303–317.
27. Speilberger CD. Manual for the State-Trait Anxiety Inventory STAI (Form Y). Palo Alto, CA: Mind Garden; 1983.
28. Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equ Model. 1999;6(1):1–55.
29. Price B, First A. Course in Factor Analysis. Technometrics. 2013;35(4):453.
30. Cohen J Quantitative methods in psychology: a power primer.
31. Richardson JTE. Eta squared and partial eta squared as measures of effect size in educational research. Educ Res Rev. 2011;6(2):135–147.
32. Groen RN, Ryan O, Wigman JTW, et al. Comorbidity between depression and anxiety: assessing the role of bridge mental states in dynamic psychological networks. BMC Med. 2020;18(1):1–17.
33. Cheung GW, Lau RS. Testing mediation and suppression effects of latent variables: bootstrapping with structural equation models. Organ Res Methods. 2008;11(2):296–325.
34. Nolen-Hoeksema S. Emotion regulation and psychopathology: the role of gender. Annu Rev Clin Psychol. 2012;8:161–187.
35. Zlomke KR, Hahn KS. Cognitive emotion regulation strategies: gender differences and associations to worry. Pers Individ Dif. 2010;48(4):408–413.
36. Matsumoto D. Individual and cultural differences on status differentiation: the status differentiation scale. J Cross Cult Psychol. 2007;38(4):413–431.
37. Su JC, Lee RM, Park IJK, et al. Differential links between expressive suppression and well-being among Chinese and Mexican American College students. Asian Am J Psychol. 2015;6(1):15–24.
38. Sheppes G. Emotion regulation choice: theory and findings. Handb Emot Regul. 2014;2:126–139.
39. Cheng M, Wang M, Chang M, Zhang R, Gu C, Zhao Y. Relationship between resilience and insomnia among the middle-aged and elderly: mediating role of maladaptive emotion regulation strategies. Psychol Heal Med. 2020;25(10):1266–1277.
40. Ludwig L, Werner D, Lincoln TM. The relevance of cognitive emotion regulation to psychotic symptoms – a systematic review and meta-analysis. Clin Psychol Rev. 2019;72:101746.
41. O’Connor DB, Thayer JF, Vedhara K. Stress and health: a review of psychobiological processes. Ann Rev Psychol. 2021;72(4):1–26.
42. Silva-Sauer L, Lima TRG, da Fonsêca ÉKG, de la Torre-Luque A, Yu X, Fernández-Calvo B. Psychological resilience moderates the effect of perceived stress on late-life depression in community-dwelling older adults. Trends Psychol. 2021;29(4):670–683.
43. Abravanel BT, Sinha R. Emotion dysregulation mediates the relationship between lifetime cumulative adversity and depressive symptomatology. J Psychiatr Res. 2015;61:89–96.
44. Tsai AC, Chi SH, Wang JY. Association of perceived stress with depressive symptoms in older Taiwanese: results of a population-based study. Geriatr Gerontol Int. 2015;15(5):535–543.
45. Brindle K, Moulding R, Bakker K, Nedeljkovic M. Is the relationship between sensory-processing sensitivity and negative affect mediated by emotional regulation? Aust J Psychol. 2015;67(4):214–221.
46. Thomas WJ, Hauson AO, Lambert JE, et al. A meta-analysis of the effectiveness of cognitive-behavioural therapies for late-life depression. Can J Couns Psychother. 2018;52(1):78–117.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.