Back to Journals » Advances in Medical Education and Practice » Volume 16
Application of Clinical Pathway and Case-Based Learning in Residency Training of Pediatric Cardiology
Authors Shen J, Chen QC, Li JJ
Received 8 May 2025
Accepted for publication 22 August 2025
Published 28 August 2025 Volume 2025:16 Pages 1569—1578
DOI https://doi.org/10.2147/AMEP.S539059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Junjun Shen,1,2 Qin-Chang Chen,1 Jun-Jie Li1
1Department of Pediatric Cardiology, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, 510000, People’s Republic of China; 2Department of Maternal-Fetal Cardiology, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, Guangzhou, 510000, People’s Republic of China
Correspondence: Jun-Jie Li, Department of Pediatric Cardiology, Guangdong Provincial People’s Hospital (Guangdong Academy of Medical Sciences), Southern Medical University, No. 106, Zhongshan 2nd Road, Guangzhou, Guangdong, People’s Republic of China, Email [email protected]
Background: Residency training provides systematic, competency-based education for medical graduates. Although specialised knowledge and clinical skills are crucial in pediatric cardiology, training in China is often limited to 2– 3 months with lecture-heavy approaches. We explored integrating clinical pathway(CP) and case-based learning (CBL) models to enhance training efficiency.
Methods: The study involved 47 second-year pediatric trainees in Guangdong Provincial People’s Hospital (2021– 2024), randomly divided into a traditional teaching (TT) group and a CP-CBL group. Both groups underwent a 3-month training period, with no significant baseline differences (age: 21.6 ± 1.2 vs 22.1 ± 0.8 years; eight male trainees/group). The TT group received conventional lectures and ward-based learning. In the CP-CBL group, standardized instruction for common diseases was delivered through CP, whereas atypical/complex cases were taught with CBL. Both groups covered identical syllabus and duration. Outcomes were assessed through a theoretical test, case analysis, and an anonymous trainee questionnaire with a 5-point Likert scale. Group means were compared using Welch’s t-tests (α = 0.05) in R software (significance level: p < 0.05).
Results: Among 47 pediatric trainees, 24 (51.1%) were assigned to the CP-CBL group. No significant differences in age, experience, or prior CP-CBL exposure were observed between groups. All trainees completed the rotation exam. The CP-CBL group outperformed the TT group in comprehensive assessments (case analysis + theory exams), with 37.5% vs 4.3% of trainees scoring > 90 points respectively. Trainees in the CP-CBL group reported higher satisfaction with learning interest (p < 0.01) and perceived skill improvement (p < 0.01), but no significant differences in course organisation (p = 0.49) or instructor performance (p = 0.79).
Conclusion: In pediatric cardiology training, CP-CBL outperformed TT in both knowledge acquisition and learner engagement.
Keywords: pediatric education, clinical pathway, CBL teaching mode, cardiology
Key Messages
What is already known on this topic:
The limited pediatric cardiology rotation time, excessive lectures, and faculty shortage hinder training effectiveness. Innovative residency models are urgently needed.
What this study adds:
- The study established the first structured clinical pathway(CP) list for pediatric cardiology training and integrated it with case-based learning(CBL) in a detailed workflow, demonstrating its application in standardized residency education.
- It used subjective and objective evaluations to confirm CP-CBL’s effectiveness over TT.
How this study might affect research, practice, or policy:
- The study provides a validated CP-CBL training model that can standardize pediatric cardiology education and inform residency program reforms.
- Its dual focus on structured CPs and active learning offers a transferable framework for both medical training policies and practical curriculum development.
Introduction
Standardized training of resident physicians, known as “residency training”, involves systematic, competency-based education for medical trainees after they finish their formal training at accredited institutions.1,2 During training, physicians engage in comprehensive educational activities that help them effectively apply theoretical knowledge to clinical practice, enhancing their learning abilities and improving the quality of medical education. In pediatric training, cardiology is a highly specialised field that requires trainees to have a comprehensive understanding of clinical knowledge such as cardiac anatomy and hemodynamics, making clinical teaching crucial in the training process.3 However, only a few top-tier hospitals in China offer subspecialty training in pediatric cardiology, and the duration of training for residents in the department typically lasts only 2–3 months. The constrained duration of clinical rotations, compounded by excessive emphasis on didactic lectures and a shortage of qualified teaching faculty, has substantially impeded the effective achievement of training objectives. There is an urgent need for innovative residency training models to address the challenges.
While the traditional teaching(TT) model can a priori ensure homogeneous delivery of key knowledge to all trainees, it often struggles to accommodate the typically diverse backgrounds and learning abilities among trainees. Such teaching models are usually implemented through large-class lectures and didactic instruction.4 The clinical pathway (CP) provides a systematic method for creating and executing local care protocols with evidence-based clinical guidelines.5 The CP standardizes disease management and makes medical diagnosis more systematic and scientific. Since its introduction, CP has been incorporated into medical education. The CP teaching model facilitates trainees’ comprehension of clinical knowledge, promotes standardized practices, and streamlines teaching methodologies.6 CP model guides trainees in accordance with international guidelines and evidence-based medicine, facilitating more effective acquisition of new knowledge while reducing variability caused by differences in instructors, teaching methodologies, and training programs.7 Some medical education studies have demonstrated that the CP model can improve residents’ confidence and knowledge in managing specialty-specific diseases (such as in gynecology, burn care, respiratory medicine, etc) during their specialized training.8–10 Case-based learning (CBL) is a small-group teaching method using cases to learn clinical problems under teacher guidance.11 Research demonstrates that CBL significantly improves trainees’ clinical knowledge acquisition and skill development, while positively influencing their practical behaviors and teamwork competencies, thereby representing an effective pedagogical approach for adult medical education.12–16
The CP-CBL model integrates structured concept presentation with active, student-centered CBL, fostering problem-solving through real-world scenarios; research has demonstrated its effectiveness in improving trainees’ learning performance.8,9 While in TT model trainees are passive recipients of information, in CP-CBL they collaboratively analyze cases, dynamically applying concepts with instructor guidance. However, there is limited literature on the implementation of CP-CBL model in pediatric cardiology education. This study aimed to compare the efficacy of CP-CBL versus TT in clinical skill development, and evaluate whether CP-CBL’s active learning approach enhances problem-solving abilities in real-world scenarios—addressing gaps in traditional pedagogy in pediatric cardiology.
Materials and Methods
Participants
The study population comprised all eligible second-year pediatric residents undergoing standardized training at the department of Pediatric Cardiology in Guangdong Provincial People’s Hospital(GDPH) from 2021 to 2024. Participants were consecutively enrolled based on the following criteria:
Inclusion criteria: (1) Active enrollment in the pediatric residency program; (2) Completion of the rotation of 3 months; (3) No prior exposure to CP-CBL methodology; (4) Willingness to provide informed consent. Exclusion criteria: (1) Planned rotation transfers during the study period; (2) Incomplete pre- or post-assessment data.
Group allocation followed the institution’s rotation schedule. We enrolled 2–3 new pediatric residents quarterly, who were then assigned to two groups: TT group received instruction through conventional methods and the CP-CBL group received training with CP-CBL methods. We evaluated participants’ baseline familiarity with pediatric cardiology and CP-CBL model using a pre-training survey. Comparative analysis revealed no statistically significant intergroup differences.
The ethical review committee of GDPH granted approval for our research (project number KY2025-232-01). We secured written informed consent from all participants involved in this study.
Teaching Intervention
TT Model
All enrolled trainees from both study cohorts completed the standardized pediatric curriculum, which encompassed core subspecialty modules including pulmonology, gastroenterology, urology, endocrinology, rheumatology, and cardiology. Trainees typically completed 2–3 month clinical rotations in each specialty department. They received daily clinical skills instruction from attending physicians in ward settings. The TT model follows a teacher-centered approach, where instructors determine the core content of instruction based on the syllabus. The curriculum focuses on standard pediatric cardiology topics (encompassing etiological definitions, pathophysiological mechanisms, symptomatic presentations, diagnostic criteria, and therapeutic interventions). Six 45-minute didactic sessions are delivered during the clinical rotation, with no structured discussion components integrated. A full evaluation is usually performed post-rotation to assess both theoretical knowledge and clinical skills.
CP-CBL Model
The mentor team first develop a CP list based on the teaching syllabus, currently focusing on four common pediatric cardiovascular conditions: ventricular septal defect, atrial septal defect, pulmonary stenosis, and Patent Ductus Arteriosus (PDA). Upon trainees’ department orientation, mentors conduct in-depth instruction following this list, systematically covering key aspects including history taking, clinical feature analysis, diagnostic method selection, and pre-/post-operative management protocols at designated time points (Figure 1).
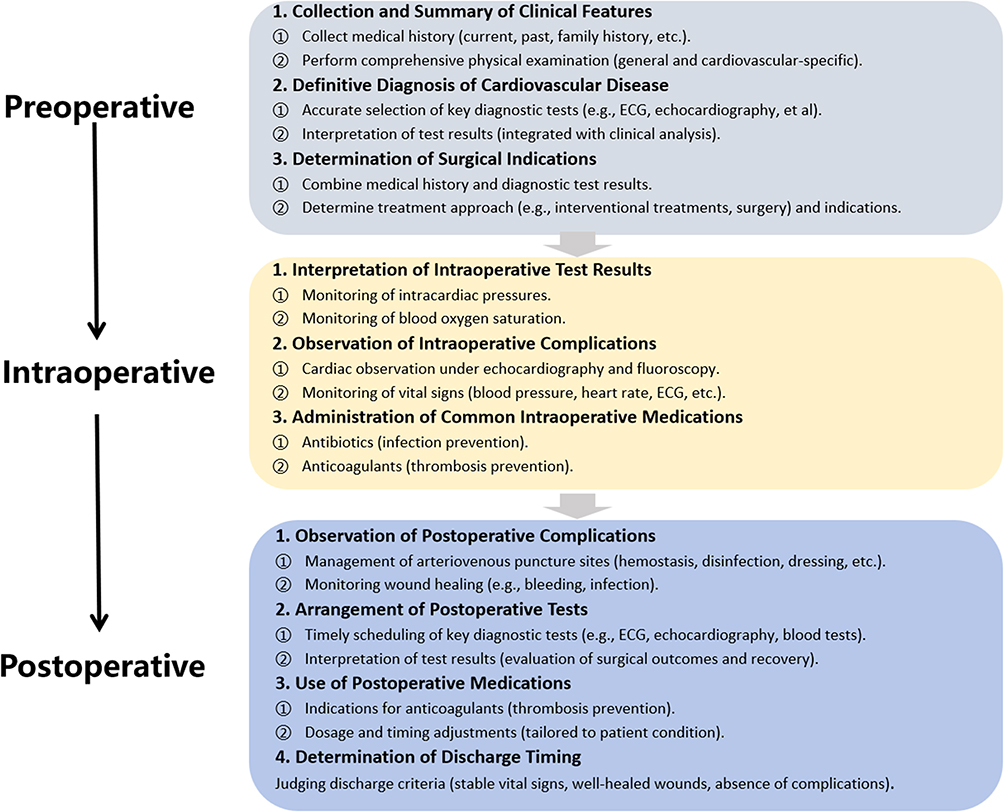 |
Figure 1 Clinical pathway list of pediatric heart disease. |
During the first month of ward rotations, trainees participated in managing cases that qualify for CPs, applying the list in practice to master standardized treatment protocols and understand routine clinical decision-making processes and evidence-based management strategies. After the second month in the department, trainees began managing more complex cases that do not qualify for standard pathways. For example, PDA with severe pulmonary hypertension, while included in the four-disease list, requires a different approach, prompting mentors to transition to CBL model.
The CBL curriculum incorporates multiple classic cases and structured modules developed through consensus among pediatric cardiologists. Instructors first pose targeted clinical questions based on current patients, following established CBL templates - for instance: “What caused this patient’s pulmonary hypertension?” “Does the patient still meet surgical criteria?” “What diagnostic tests are indicated?” Trainees then work in groups to conduct literature reviews and textbook analyses, collaboratively collecting complete medical histories, systematically documenting clinical features, and evaluating advanced diagnostic techniques like cardiac catheterization and CT angiography.
The CBL model particularly emphasizes detailed hemodynamic parameter analysis - including oxygen saturation gradients, pulmonary artery pressures, and vascular resistance measurements. Group discussions facilitate multidimensional case analysis, enabling trainees to correlate empirical findings with theoretical knowledge and collaboratively interpret complex pathophysiological mechanisms. Throughout case management, instructors organize periodic progress reviews where trainees analyze case evolution. Table S1 provides a comparison between the TT model and CP-CBL model.
Evaluation
The primary objective of assessing the CP-CBL model was to determine its comparative efficacy relative to the TT model. The evaluation included two parts: (1) a departmental stage exam for objective assessment and (2) an anonymous trainee questionnaire about the two models.
In the department rotation exam, all trainees answered the same questions. The exam included theoretical tests and case analyses, each worth 50% of the final score. Two instructors from the pediatric cardiology department, unaware of the trainees’ group, graded the exams. The theoretical tests used standardized questions and difficulty levels. The case analyses were based on specific chief complaints. Trainees asked questions from standardized patients, and instructors evaluated their performance on the basis of a scoring rubric (see Appendix 1 for details).
The anonymous questionnaire asked trainees to rate four aspects of the teaching models: satisfaction with the course arrangement, the instructors, self-perceived improvement, and interest in learning. A 10-item questionnaire was given to trainees after the course to gather feedback using a 5-point Likert scale. Detailed information about the questionnaire is available in Appendix 2. The trainees were queried regarding their overall satisfaction with the duration and format of the course. They also provided evaluations of the instructors’ teaching performance. In addition to objective test scores, we assessed the trainees’ satisfaction with their perceived improvements. The questionnaire also explored whether the course had enhanced the trainees’ enthusiasm, awareness, and interest in learning pediatric cardiology. Scores were standardized prior to comparison. Three pediatric cardiology experts evaluated the questionnaire’s content validity, with all items demonstrating excellent I-CVI scores (1.0).
Statistical Analysis
Descriptive and inferential statistical analyses were conducted to compare learning outcomes between the two experimental groups. For each target variable (theory test, case analysis, total score, satisfaction with the course arrangement, the instructors, self-perceived improvement, and interest in learning), we calculated group-wise means, standard deviations, and sample sizes. Independent samples t-tests using Welch’s approximation (to account for potential variance inequality) were employed to assess significant differences between two groups. All analyses were performed as two-tailed tests with α =0.05 using R statistical software (version 4.3.2), utilising the dplyr, tidyr, and readxl packages for data manipulation and analysis. Results are presented with t-statistics, p-values, and accompanying effect size information through group mean differences and variability measures. Statistical significance was defined as p < 0.05.
Results
Participants’ Distribution and Demographic Characteristics
From the eligible population, 47 residents met all criteria and were included in the final analysis (TT group=23, CP-CBL group=24), representing 95.9% of the target cohort (n=49). All trainees in both groups underwent training for 3 months. The remaining 2 trainees were excluded due to incomplete assessment. The two groups exhibited a balanced demographic distribution (Table 1). No significant disparities were observed in terms of age, professional tenure, or prior acquaintance with pediatric cardiology and CP-CBL models across the two groups. The mean age of trainees within the TT group was 24.25 years, closely mirroring that of the CP-CBL group. Of the participants, 66.7% were female, and all trainees in both groups exhibited greater familiarity with TT model. All participants lacked formal education in pediatric cardiology and had no prior case experience in this specialty before the rotation. The flow chart is shown in Figure 2.
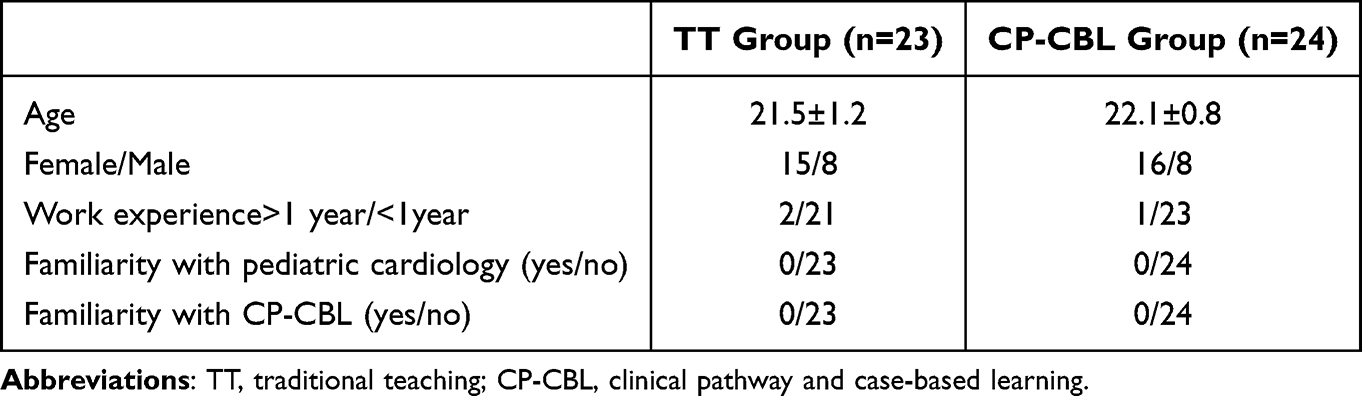 |
Table 1 Distribution and Demographic Characteristics of the Two Groups |
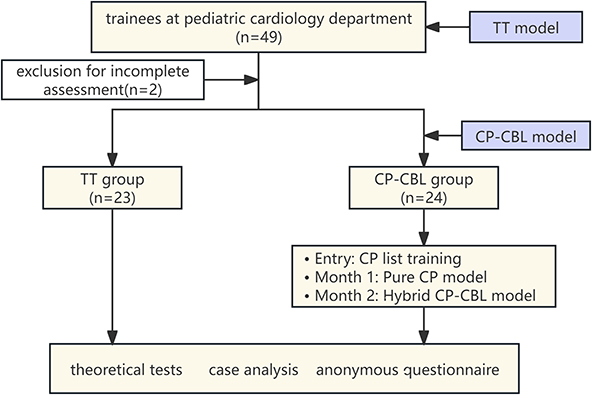 |
Figure 2 Flowchart depicting the categorization of the study population. Abbreviations: TT, traditional teaching; CP-CBL, clinical pathway and case-based learning. |
Comparison of the Examination Scores
All trainees finished the departmental rotation exam. Comparisons of the scores between the two groups are shown in Table 2 and Figure 3. The 24 trainees in the CP-CBL group had an average test score of 82.9 ± 9.9, which was significantly higher than the TT group’s average of 72.4 ± 7.8 (p < 0.01). Additionally, the CP-CBL group scored higher on both the case analysis test (32.0 ± 5.0 vs 27.6 ± 4.5, p < 0.01) and the theory examination (50.9 ± 5.3 vs 44.8 ± 7.1, p < 0.01) compared with the TT group. In the CP-CBL group, 37.5% (9/24) of the trainees scored above 90 points, while this percentage was only 4.3% in the TT group.
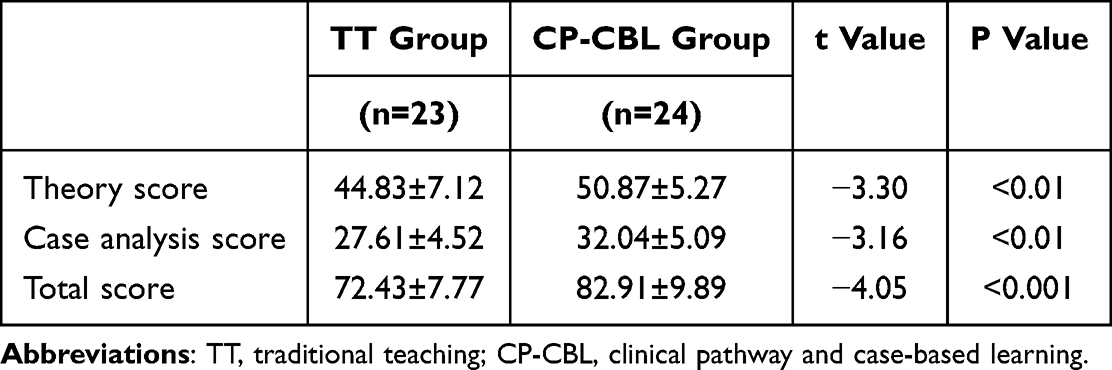 |
Table 2 Comparison of the Examination Scores Between the Two Groups |
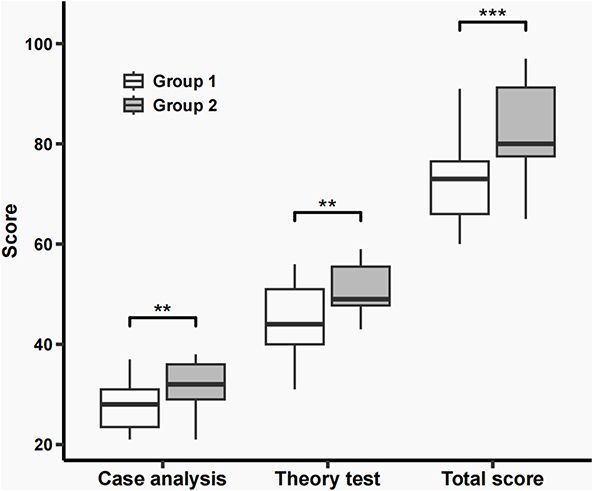 |
Figure 3 Comparison of the examination scores between the two groups. Group 1, traditional teaching group; Group 2, clinical pathway and case-based learning group. **P<0.01, ***P<0.001. |
Comparison of Satisfaction Survey Scores
Table 3 and Figure 4 show a comparison of the trainees’ subjective evaluations between the two models, both achieving a 100% survey response rate. Compared with the TT group, CP-CBL group trainees reported significantly greater satisfaction with the model’s ability to enhance their learning interest in pediatric cardiology (p < 0.01, Table 3). The CP-CBL model also resulted in a perceived significant improvement in trainees’ knowledge, skills, and ability to analyse and solve problems (p < 0.01, Table 3). However, satisfaction levels regarding course organisation (p = 0.49) and instructor performance (p = 0.79) did not differ significantly between the two groups.
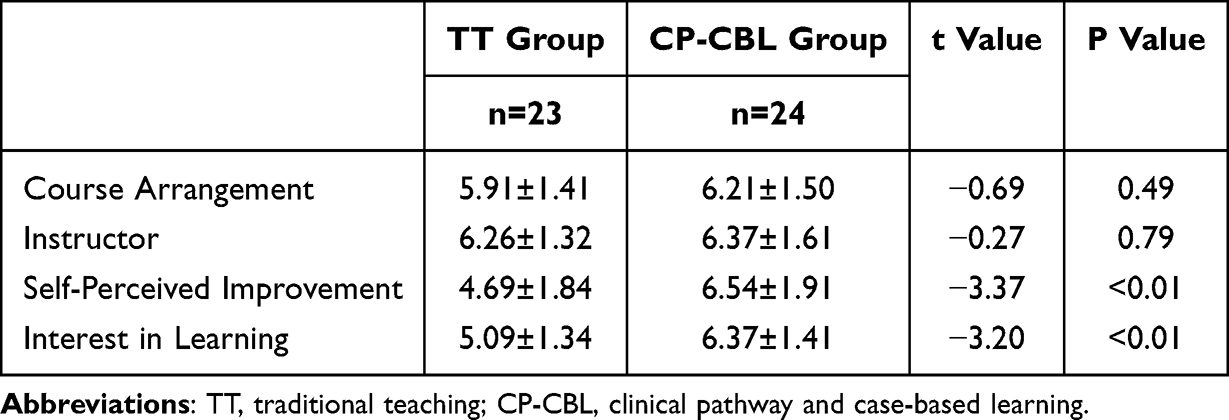 |
Table 3 Comparison of the Satisfaction Survey Scores Between the Two Groups |
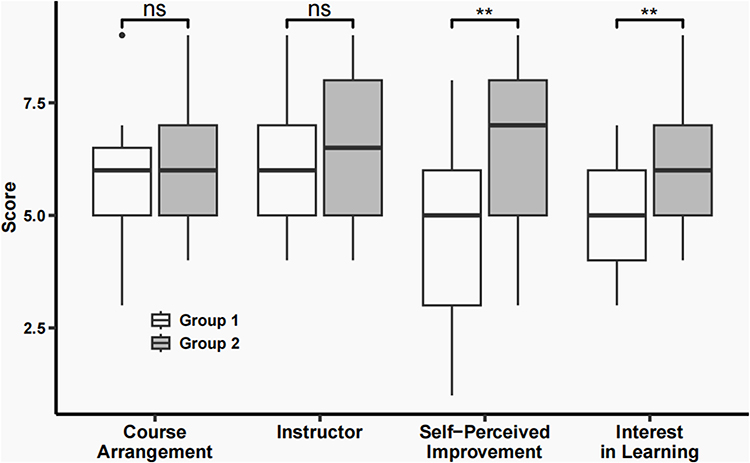 |
Figure 4 Comparison of the satisfaction survey scores between the two groups. Group 1, traditional teaching group; Group 2, clinical pathway and case-based learning group. **P<0.01. |
Discussion
The study evaluated the comparative effectiveness of the TT and CP-CBL models in pediatric cardiology residency training. The significantly higher performance scores in CP-CBL groups (Table 3) directly support our hypothesis that integrating concept presentation with CBL better achieves clinical training objectives by bridging theoretical knowledge and practical application. The educational advantage was further substantiated by significantly higher scores in theoretical assessments and case analysis evaluations among CP-CBL trainees. The results of survey demonstrated the superior efficacy of the CP-CBL model, with participants exhibiting enhanced clinical confidence, improved practical skills, and greater learning motivation compared with those in the TT group.
The CP model, while widely implemented in clinical practice and medical education, has not been systematically applied in pediatric cardiology residency training.5 Currently, 60–70% of cases in the pediatric cardiac ward are now managed through CPs. Each pathway encompasses key clinical components including medical history documentation, characteristic clinical features, diagnostic methodologies, preoperative preparations, postoperative routines, and follow-up protocols. CP-based teaching demonstrates several distinctive advantages over traditional syllabus-based instruction. First, the pathway structure provides closer integration with actual clinical practice. Second, the model incorporates a dynamic validation process where initial teaching content is continually refined through case-based verification and challenges.8 Third, the CP approach actively involves trainees in all stages of pathway development and implementation, allowing instructors to integrate critical pathways, address clinical controversies, and facilitate seamless incorporation of teaching within the CP framework.9
The implementation mechanism of the CP model follows a structured approach. Instructors utilise standardized CPs for common diseases to help residents rapidly acquire essential knowledge and clinical competencies. Trainees repeatedly review and apply diagnostic and treatment protocols in clinical settings, reinforcing their mastery of standardized procedures. The model specifically enhances trainees’ diagnostic and therapeutic capabilities for common cases, thereby boosting their confidence in routine clinical practice. The increased confidence from the CP model positively impacts both their clinical knowledge and patient interaction skills. The effectiveness of the CP model is evidenced by its ability to enhance residents’ clinical skills, critical thinking, and learning motivation, ultimately improving overall teaching outcomes.5,6,8 The benefits are supported by the current findings.
The CP-CBL model enhances traditional CP teaching by integrating complex clinical cases into the curriculum. The problem-oriented approach shifts from instructor-led to trainee-driven learning, where trainees actively solve problems through data analysis and literature review.17–20 This integrated approach not only reinforced trainees’ understanding of atypical cardiovascular presentations but also cultivated essential skills in clinical reasoning, collaborative problem-solving, and advanced diagnostic interpretation. The CP -CBL teaching methods help trainees grow into more engaged learners, boosting patient communication and clinical anomaly detection skills. The CP-CBL method also promotes continuous literature learning among trainees, boosting their professional skills. While earlier studies suggested that teacher-centred methods are more effective than CBL alone for delivering established knowledge, the current findings indicated that the integrated CP-CBL approach not only conveys knowledge effectively but also enhances clinical competencies more than traditional didactic teaching.17 In our study, questionnaire results showed the trainees in the CP-CBL model showed significant improvements in self-awareness and learning motivation. TT emphasizes knowledge acquisition, while CP-CBL prioritizes conceptual understanding and application, as demonstrated by our assessment results (Table 3). Similar observations have been noted in other studies.21,22 Effective training requires guiding trainees to recognize their limitations—an approach that extends beyond mere knowledge acquisition. A significant improvement in trainees’ self-awareness and motivation—shifting from passive instruction to active inquiry—demonstrates the efficacy of the CP-CBL model. There was no significant difference in satisfaction with course organization and instructors between CP-CBL and TT models in our study. This likely stems from trainees’ heightened motivation and their progressively more central role in the learning process.
Case analysis aims to rigorously test trainees’ practical thinking skills, observational abilities, and flexible decision-making capabilities—areas in which newly enrolled clinical trainees often lack proficiency.23–25 As shown in Table 2 and Figure 3, trainees’ scores in case analysis are generally lower than those in theoretical exams. Pediatric cardiology cases, characterised by their diversity and high level of specialisation, pose significant challenges for second-year trainees in making accurate diagnoses and treatment plans. However, a statistically significant improvement in case analysis scores was observed in the CP-CBL group compared to the TT group (32.0 ± 5.0 vs 27.6 ± 4.5, p < 0.01). The improvement may have occurred because both CP and CBL models inherently focus on repeated case-based learning, enabling trainees to approach case analysis more effectively and develop more precise diagnostic and treatment strategies.
The study had three main advantages. First, it provided a detailed description of the CP list for the first time in pediatric cardiology, integrating CPs with teaching. Second, it effectively combined the CP and CBL teaching models in the standardized training of pediatric cardiology and outlined the process in detail. Third, it employed both subjective and objective evaluations to compare the CP-CBL and TT models, confirming the effectiveness of the CP-CBL model.
The current study involved several limitations. First,despite high content validity scores of the questionnaire (I-CVI = 1.0), the study’s small sample size (n=47) constrained its statistical power. Subsequent validation studies with larger samples are needed to establish construct validity and reliability. Second, our analysis was confined to outcomes from a single clinical department within our institution, with a relatively limited sample size. While the results achieved statistical significance, future multicenter collaborations will expand recruitment to further validate the effectiveness of the CP-CBL model in specialty training programs. Third, pre-course surveys evaluated CP-CBL and pediatric cardiology awareness, but lacked objective pre-intervention knowledge assessment, warranting improvement in subsequent research. The limitations should be addressed in future research.
Conclusion
The CP-CBL model in pediatric cardiology training significantly improves teaching effectiveness compared with the TT model. The CP-CBL model motivates trainees to become more proactive and fosters their ability for independent learning, as well as enhancing their communication skills. The study provides a validated CP-CBL training model that can standardize pediatric cardiology education.
Data Sharing Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval
The current study was approved by the Institutional Review Board of the Guangdong Provincial People’s Hospital (project number KY2025-232-01). Written consent was obtained from the participants for their participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no personal or financial conflicts of interest to disclose for this work.
References
1. Zhu J, Li W, Chen L. Doctors in China: improving quality through modernisation of residency education. Lancet. 2016;388(10054):1922–1929. doi:10.1016/S0140-6736(16)00582-1
2. Deng G, Pan Y, Feng C, et al. The efficiency of residency training and health outcomes in China: based on two-stage DEA and cluster analysis. Socio-Econ Plan Sci. 2024;96:102057. doi:10.1016/j.seps.2024.102057
3. Saiydoun G, Saadé S, Jungling M, et al. Education and training of thoracic and cardiovascular surgeons: academic aspects in France. Curr Prob Surg. 2023;61(11):101611. doi:10.1016/j.cpsurg.2024.101611
4. Hu X, Li J, Wang X, et al. Medical education challenges in Mainland China: an analysis of the application of problem-based learning. Med Teach. 2024;47(4):713–728. doi:10.1080/0142159X.2024.2369238
5. Steven D, Pearson MD, Thomas H, et al. Critical Pathways as a Strategy for Improving Care: problems and Potential. Ann Internal Med. 1995;123(12):941. doi:10.7326/0003-4819-123-12-199512150-00008
6. Cui L, Dong Y, Zhang S, et al. Construction and application of procedural pathways combined with information management in nursing staff skills training system. BMC Med Educ. 2024;24(1):687. doi:10.1186/s12909-024-05593-x
7. Aspland E, Gartner D, Harper P. Clinical pathway modelling: a literature review. Health Syst. 2019;10(1):1–23. doi:10.1080/20476965.2019.1652547
8. Yao P, OuYang J, Liu C, et al. Improving burn surgery education for medical students in China. Burns. 2020;46(3):647–651. doi:10.1016/j.burns.2019.09.012
9. Wang X, Che X, Tang X, et al. Application of combined teaching method of case-based-learning and clinical pathway in practical gynecological teaching. PeerJ. 2024;12:e17813. doi:10.7717/peerj.17813
10. Kanda R, Kawamura M, Kojiro M, et al. The effectiveness of the clinical pathways for children hospitalized for the treatment of acute asthma exacerbation. Pediatr Int. 2025;67(1):e70073. doi:10.1111/ped.70073
11. Alizadeh M, Saramad A, Rafiepoor H, et al. Effect of virtual case-based learning (CBL) using the flipped class and peer instruction on the motivation to learn basic sciences. BMC Med Educ. 2024;24(1):1230. doi:10.1186/s12909-024-06229-w
12. Makwana S, Sarvaiya H, Dalsaniya V. A comparative study of case-based learning (CBL) versus the traditional teaching method for enhanced analysis and interpretation of electrocardiogram (ECG) among medical students. Cureus. 2025;17(2):e79587. doi:10.7759/cureus.79587
13. Al-Bedaery R, Baig S, Khare Y, et al. Humanising case-based learning. Med Teach. 2023;46:1348–1355. doi:10.1080/0142159X.2024.2308066
14. Harman T, Bertrand B, Greer A, et al. Case-based learning facilitates critical thinking in undergraduate nutrition education: students describe the big picture. J Acad Nutr Diet. 2014;115(3):378–388. doi:10.1016/j.jand.2014.09.003
15. Dubey S, Dubey AK. Promotion of higher order of cognition in undergraduate medical students using case-based approach. J Educ Health Promot. 2017;6:75. doi:10.4103/jehp.jehp_39_17
16. Cen XY, Hua Y, Niu S, et al. Application of case-based learning in medical student education: a meta-analysis. Eur Rev Med Pharmaco. 2021;25(8):3173–3181. doi:10.26355/eurrev_202104_25726
17. Jamkar AV, Burdick W, Morahan P, et al. Proposed model of case-based learning for training undergraduate medical students in surgery. Indian J Surg. 2007;69(5):176–183. doi:10.1007/s12262-007-0016-2
18. Yang Y, Guo Z, Guo X, et al. Enhancing postpartum hemorrhage training by integrating case-problem-based learning with simulation: a quasi experimental study. J Obstet Gynaecol. 2023;45(1):2443617. doi:10.1080/01443615.2024.2443617
19. Santhakumari BG, Vijayan S. Comparative study on the effectiveness of case-based learning over small group discussion in pediatrics among 8th semester MBBS students. Int J Res Med Sci. 2023;13:1. doi:10.18203/2320-6012.ijrms20244127
20. Shang Y, Cao KF, Yue JY, et al. Comparative effectiveness of various teaching modes, including PBL, CBL, and CTTM in pediatric medical education with combined online and offline approaches. BMC Med Educ. 2025;25(1):8. doi:10.1186/s12909-024-06267-4
21. Chen J, Gao B, Wang K, et al. WeChat as a platform for blending problem/case-based learning and paper review methods in undergraduate pediatric orthopaedics internships: a feasibility and effectiveness study. BMC Med Educ. 2023;23(1):322. doi:10.1186/s12909-023-04269-2
22. Chao J, Qingyuan S, Pei Z, et al. The application of interdisciplinary and cross-grade learning teaching method in stomatology course. J Dent Educ. 2023;88(9):1190–1197. doi:10.1002/jdd.13557
23. Ng IKS, Goh WGW, Teo DB, et al. Clinical reasoning in real-world practice: a primer for medical trainees and practitioners. Postgrad Med J. 2023;101(1191):68–75. doi:10.1093/postmj/qgae079
24. Çetinkaya L, Keser IL, Yildirim S, et al. The effect of case-based mobile virtual patient application on students’ academic achievement in clinical reasoning skills. Med Educ Online. 2023;29(1):2322223. doi:10.1080/10872981.2024.2322223
25. Jiang D, Huang D, Wan H, et al. Effect of integrated case-based and problem-based learning on clinical thinking skills of assistant general practitioner trainees: a randomized controlled trial. BMC Med Educ. 2023;25(1):62. doi:10.1186/s12909-025-06634-9
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.