Back to Journals » Clinical Interventions in Aging » Volume 18
Appendicular Skeletal Muscle Mass Associated with Sarcopenia as a Predictor of Poor Functional Outcomes in Ischemic Stroke
Authors Lee SH, Choi H ![]() , Kim KY, Lee HS, Jung JM
, Kim KY, Lee HS, Jung JM
Received 23 December 2022
Accepted for publication 17 June 2023
Published 4 July 2023 Volume 2023:18 Pages 1009—1020
DOI https://doi.org/10.2147/CIA.S402548
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
Sang-Hun Lee,1 Hangseok Choi,2 Keon-Yeup Kim,1 Hyung-Soo Lee,3 Jin-Man Jung1
1Department of Neurology, Korea University Ansan Hospital, Korea University College of Medicine, Ansan, South Korea; 2Medical Science Research Center, Korea University College of Medicine, Seoul, South Korea; 3Department of Medicine, Graduate School, Kyung Hee University, Seoul, South Korea
Correspondence: Jin-Man Jung, Department of Neurology, Korea University Ansan Hospital, Korea University College of Medicine, Gojan 1-Dong, Danwon-Gu, Ansan, Gyeonggi-Do, 15355, South Korea, Tel +82-31-412-5150, Fax +82-31-412-5154, Email [email protected]
Purpose: Several studies have examined the clinical impact of poststroke and stroke-related sarcopenia on stroke recovery. However, few studies have investigated the effect of sarcopenia detected shortly after stroke on functional prognosis. We predicted functional outcomes using early screening for sarcopenia in patients with acute ischemic stroke. We also examined the effect of sarcopenia detected shortly after stroke on functional prognosis.
Patients and Methods: Patients diagnosed with acute ischemic stroke within 2 days of symptom onset were consecutively enrolled at a tertiary university hospital. Appendicular skeletal muscle mass (ASM) was measured using dual-energy X-ray absorptiometry during early hospitalization. Sarcopenia was diagnosed based on low ASM and strength criteria of the Asian Working Group for Sarcopenia (AWGS) and European Working Group on Sarcopenia in Older People (EWGSOP2). The primary outcome was poor functional outcome, defined as a modified Rankin score of 4– 6 and all-cause mortality at 3 months.
Results: Of the 653 patients, 214 (32.8%) and 174 (26.6%) had sarcopenia according to the AWGS and EWGSOP2 criteria, respectively. Irrespective of the definition, the sarcopenia group had a significantly higher proportion of patients with poor functional outcomes and all-cause mortality. Multivariate logistic regression analysis revealed that height-adjusted ASM was independently associated with poor functional outcomes (odds ratio: 0.61; 95% confidence interval: 0.40– 0.91; P < 0.005), and they were negatively correlated. However, the association between 3-month mortality, skeletal muscle mass, and sarcopenia was not sustained in multivariate analyses.
Conclusion: Height-adjusted ASM associated with sarcopenia is a potential predictor of poor functional outcomes at 3 months in patients with acute stroke. However, owing to the limitations of this study, further research is required to confirm these findings.
Keywords: stroke-related sarcopenia, skeletal muscle mass, functional outcome, prognosis
Introduction
The term “sarcopenia” was first introduced by Rosenberg to describe the progressive loss of general body muscle mass, muscle strength, and/or decreased muscle physiology associated with aging.1,2 In addition, muscle tissues play an important role in mobility and energy metabolism. Sarcopenia is associated with various adverse outcomes including frequent falls, osteoporosis, cardiovascular events, and mortality.3,4 However, variable definitions and criteria for sarcopenia using different cutoff values and measurement tools have led to difficulties in standardizing these definitions, as well as the application of sarcopenia in clinical practice. Nonetheless, in recent years, various leading groups, including the International Working Group on Sarcopenia, Asian Working Group for Sarcopenia (AWGS), and European Working Group on Sarcopenia in Older People (EWGSOP2), have attempted to create a standardized definition and diagnosis of sarcopenia. However, a unified definition and measurement tool for sarcopenia has not yet been developed.5,6
The development of sarcopenia is associated with age. Any condition or disease that reduces physical activity can lead to sarcopenia. In patients with stroke, poststroke sarcopenia can develop as a complication due to changes in muscle tissue mass and structure. Poststroke sarcopenia is also observed in approximately half of older patients with stroke.7–10 Previous studies have reported that stroke-induced disability causes sarcopenia during the recovery process, which can significantly impact activities of daily living after stroke and functional prognosis.11–13 However, these findings are mainly based on convalescent rehabilitation settings that might reflect sarcopenia after subacute or chronic stroke but not shortly after or before stroke. This could lead to biased results in that sarcopenia could result from low physical activity or poor functional outcomes attributed to stroke rather than the effect of sarcopenia itself.14–16 Furthermore, the effect of sarcopenia on functional prognosis, observed from the time of stroke onset, has rarely been investigated. In addition, the assessment of prestroke sarcopenia via a questionnaire, if any, might be limited in terms of accuracy compared to the assessment using objective tools, such as dual-energy X-ray absorptiometry (DEXA).17
Early screening for sarcopenia based on the AWGS and EWGSOP2 criteria is more appropriate for predicting clinical outcomes in patients with acute stroke to investigate the effect of sarcopenia rather than stroke-induced sarcopenia.7 Therefore, this study aimed to predict functional outcomes through early appendicular skeletal muscle mass (ASM) measurement using DEXA in patients with acute ischemic stroke.
Materials and Methods
Patients
We prospectively enrolled consecutive patients admitted to the stroke center of Korea University Ansan Hospital for ischemic stroke between March 2017 and October 2019. Patients were included in the study based on the following criteria (Figure 1): (1) admission within 2 days of symptom onset; (2) DEXA (Figure 2) examination during early hospitalization; and (3) ability to walk independently, with a modified Rankin Scale (mRS) score <2 before the index stroke. In addition, we excluded those who had difficulties in undergoing the DEXA examination (eg, ventilator application and disturbances of consciousness) and those who were previously diagnosed with musculoskeletal or neurological diseases that could cause weakness, muscle atrophy, or both. We enrolled adults aged over 19 years, and there was no upper age limit.
 |
Figure 1 Flow diagram for the inclusion and exclusion criteria. |
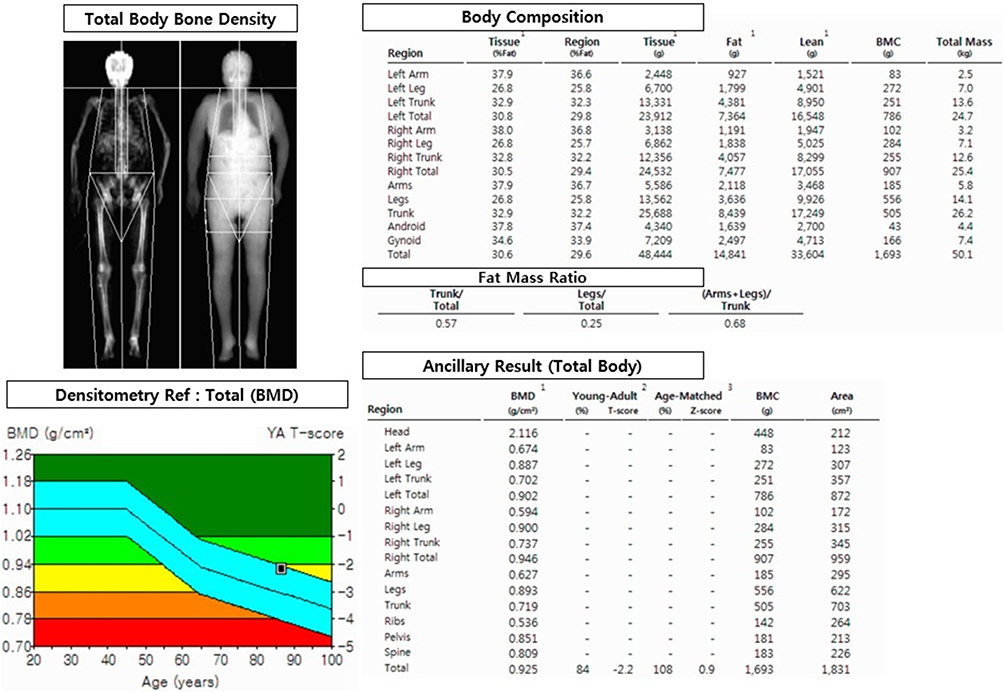 |
Figure 2 A representative dual-energy X-ray absorptiometry image used for skeletal muscle mass measurement. |
The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in a priori approval by the institution’s human research committee. Finally, this study protocol was approved by the Institutional Review Board of the Korea University (approval no. 2016AS0334). Informed consent was obtained from all participants.
Muscle Assessment and Definition of Sarcopenia
All patients included in this study underwent DEXA using a Lunar Prodigy Advance (GE Healthcare, Chicago, IL, USA) to measure whole-body and/or regional lean tissue mass, including fat, lean tissue mass, and body fat percentage. DEXA was performed during early hospitalization to reduce the impact of stroke and reflect the skeletal muscle mass before or shortly after stroke. It is one of the most frequently used techniques for body composition assessment and is considered the gold standard. However, it has some limitations.18 Previous reports show that DEXA can provide highly precise measurements of body fat, fat-free mass, and bone minerals.8,9 Total and segmental fat-free lean mass and fat mass were recorded. In addition, the height-adjusted ASM was extracted for each patient. Handgrip strength was measured during early hospitalization using a Jamar® hydraulic hand dynamometer (Model J00105, Lafayette, USA) to evaluate muscle power. The average measurement of the three trials for each hand was recorded. If there was a discrepancy in the measurement between the two hands, the larger hand was selected because patients with stroke occasionally present with hand weakness.
Sarcopenia was diagnosed based on the AWGS and EWGSOP2 criteria using both appendicular muscle mass and muscle strength.5 However, the EWGSOP2 definitions may not accurately represent racial differences because their cutoff values are based on the European population.6 Therefore, we also used the guidelines developed by the AWGS to diagnose sarcopenia, which include the differences in anthropometric, cultural, and lifestyle problems in Asians.5,6 According to the AWGS diagnostic criteria, low strength is defined as grip force <28 kg for men and <18 kg for women. The cutoff values of height-adjusted muscle mass that meet the criteria for sarcopenia are <7.0 kg/m2 in men and <5.4 kg/m2 in women.5 According to the EWGSOP2 definition, the muscle mass for DEXA was expressed as ASM/height2 with a cutoff point of <7.0 kg/m2 for men and <5.5 kg/m2 for women. The cutoff points for handgrip strength were <27 kg for men and <16 kg for women.6 It is difficult for patients with stroke to perform a comprehensive gait function evaluation; therefore, the gait speed and short physical performance battery test proposed in the EWGSOP2 were not evaluated. The definition of sarcopenia based on height-adjusted ASM and handgrip strength was adjusted in this study.
Data Collection and Measurements
The patients’ age, sex, height (cm), body weight (kg), body mass index (BMI), anthropometric parameters including mid-upper arm circumference (cm), thigh circumference (TC, cm); vascular risk factors, such as diabetes, hypertension, dyslipidemia, and atrial fibrillation; the Trial of ORG 10172 in Acute Stroke Treatment classification; the mRS score; and stroke severity score, such as the National Institute of Health Stroke Scale (NIHSS) score at the time of admission, were recorded. TC was measured at the level halfway between the anterior superior iliac spine and the apex of the patella on both the paretic and non-paretic sides.19 Laboratory findings included complete blood count, cholesterol panel, high-sensitivity C-reactive protein (hs-CRP) level, estimated glomerular filtration rate (eGFR), serum glucose, hemoglobin A1c, and homocysteine levels. In-hospital infection was defined as clinical or laboratory evidence of infection, such as fever, leukocytosis, or the use of antibiotics, irrespective of the infection site. Information regarding discharge medications, including statins, antiplatelet agents, and anticoagulants, was also collected.
Outcomes
The outcome was functional status as indicated by the mRS score at 3 months. Outcomes were grouped into dichotomous categorical variables, and a poor functional outcome was defined as an mRS score of 4–6. The primary outcome was poor functional status at 3 months. The secondary outcome was all-cause mortality at 3 months. Information on functional status was acquired via direct assessment in the outpatient clinic by stroke neurologists (JJM and LSH), or via telephone interviews conducted by an experienced nurse if the patient had not visited the hospital.
Statistical Analysis
ASM was considered a continuous and categorical variable that was divided into four groups (Q1–4) based on the quartiles of height-adjusted ASM. Q1 implied the highest value of height-adjusted ASM and Q4 implied the lowest value. Patients with sarcopenia were divided into two groups according to the EWGSOP2 and AWGS definitions. Categorical variables were analyzed using the χ2 test and Fisher’s exact test. Differences in continuous variables were assessed using the Student’s t-test, nonparametric Wilcoxon test, or Kruskal–Wallis test, depending on the normal distribution of each variable. Multivariate logistic regression analyses were performed to identify the predictive factors for each outcome. All potential predictors (P <0.05) from the univariate analyses were adjusted in the multivariate models using a backward elimination selection method. In addition, we used restricted cubic splines to examine the shape of the association between height-adjusted ASM and outcomes at 3 months after adjusting for all potential variables in the univariate analyses. The significance level was set at P <0.05. All statistical analyses were performed using R 4.0.3 and IBM SPSS Statistics for Windows (version 20.0; IBM Corp., Armonk, NY, USA).
Results
Between March 2017 and October 2019, 1760 patients were admitted to the stroke center of Korea University Ansan Hospital for ischemic stroke. In total, 916 patients who underwent DEXA were enrolled in this study. Among them, 231 patients with a prestroke mRS score ≥2, 26 with an incomplete study in which DEXA evaluation was not properly derived, and six who were lost to follow-up were excluded. In total, 653 participants were included in the analysis. The EWGSOP2 and AWGS criteria were used to identify 214 (32.8%) and 174 (26.6%) patients, respectively. Eighty-nine patients were classified into the group with poor functional outcomes at 3 months (Figure 1).
Table 1 presents the demographic characteristics of patients according to their functional outcomes. Older age; female sex; and higher rates of diabetes, atrial fibrillation, symptomatic intracerebral hemorrhage, and in-hospital infections were significantly associated with poor functional outcomes (all P < 0.05). The stroke subtype was associated with poor functional outcomes. The small-vessel occlusion group had a higher prevalence of subtypes with a good functional outcome, whereas the cardioembolic stroke group had a lower prevalence of those with a good functional outcome. The lowest quartiles of height-adjusted ASM and sarcopenia, according to the EWGSOP2 and AWGS criteria, were observed to occur significantly more in the poor-functional outcome group (all P < 0.001).
 |
Table 1 Baseline Characteristics of Study Participants |
Higher levels of white blood cells (9.14±3.23 vs 8.02±3.22, ×103/mm3), hs-CRP (0.69 [0.14–2.31] vs 0.13 [0.05–0.34], ng/mL), and homocysteine (12.8 [9.7–15.3] vs 10.9 [8.6–13.8], IU/L), and lower BMI (23.6±3.9 vs 24.5±3.4, kg/m2), eGFR (74.6±24.6 vs 89.7±27.9, mL/min/1.73 m2), handgrip strength (13.0±8.0 vs 20.1±12.3, kg), and (44.6±7.8 vs 47.8±8.9, cm) were significantly associated with the group with poor functional outcomes than the group without such outcomes (all P < 0.05) (Table 2).
 |
Table 2 Body Scales, Laboratory Findings, and Medications of Study Participants |
Figure 3A and B show the proportions of 90-day mRS scores according to whether sarcopenia was diagnosed using the AWGS and EWGSOP2 criteria. Overall, a large proportion of the patients with high mRS scores were diagnosed with sarcopenia, suggesting poor functional outcomes. When the diagnostic definition of the AWGS was applied, the proportion of patients with poor functional outcomes in the sarcopenia group was 23.5%, which was more than twice that in the non-sarcopenia group (10%). A similar pattern was observed when the EWGSOP2 diagnostic criteria were applied. Figure 3C shows the proportion of 90-day mRS scores in four groups (Q1–4) classified according to the quartiles of height-adjusted ASM. As the height-adjusted ASM score decreased, the proportion of patients with poor functional outcomes increased (Q1: 4.9%; Q2: 9.2%; Q3: 11%; Q4: 18.3%).
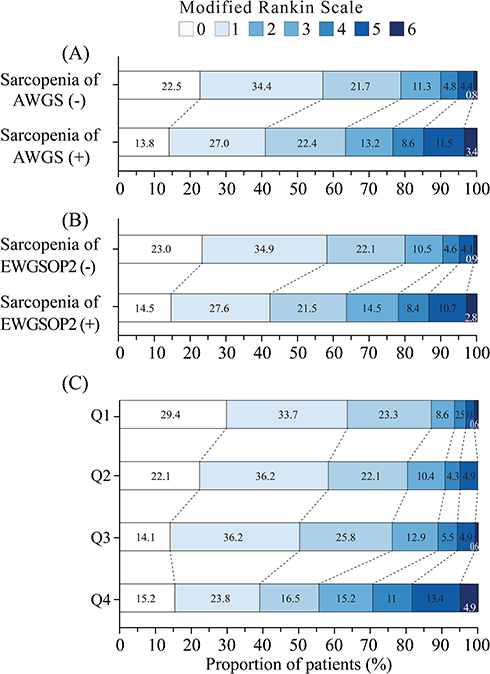 |
Figure 3 (A and B) Modified Rankin Scale scores at 90 days according to the diagnosis of sarcopenia. The distribution of scores on the modified Rankin Scale is shown. Scores ranged from 0 to 6, with 0 indicating no symptoms, 1 indicating no clinically significant disability, 2 indicating slight disability (patient is able to handle own affairs without assistance but unable to carry out all previous activities), 3 indicating moderate disability (patient requires some help but is able to walk unassisted), 4 indicating moderately severe disability (patient is unable to attend to bodily needs without assistance and is unable to walk unassisted), 5 indicating severe disability (patient requires constant nursing care and attention), and 6 indicating death. (C) Modified Rankin Scale scores at 90 days according to the quartiles of height-adjusted ASM. Categorical variables were divided into four groups (Q1–4) based on the quartiles of height-adjusted ASM. Q1 implied the highest value of height-adjusted ASM and Q4 implied the lowest value. Abbreviations: AWGS, Asian Working Group for Sarcopenia; EWGSOP2, European Working Group on Sarcopenia in Older People; ASM, appendicular skeletal muscle mass. |
Association of Muscle Mass and Sarcopenia with Patients’ Functional Outcomes at 3 Months
As the height-adjusted ASM increased, the odds of presenting with poor functional outcomes at 3 months poststroke decreased (odds ratio [OR]: 0.50; 95% confidence interval [CI]: 0.40–0.62; P <0.001) (Table 3). Regarding the height-adjusted ASM category, the groups Q2, Q3, and Q4 had a higher risk of poor functional outcomes at 3 months than the highest group (Q1 reference) (P <0.001). As the quartile of the height-adjusted ASM increased, the magnitude of the OR increased considerably. The sarcopenia group, diagnosed based on the AWGS and EWGSOP2 criteria, had a higher risk of poor functional outcomes at 3 months (OR: 2.77, 95% CI: 1.75–4.38, P <0.001; OR: 2.66, 95% CI: 1.69–4.19, P <0.001, respectively) in the univariate analyses. Multivariate logistic regression analysis revealed that height-adjusted ASM per unit increase (OR: 0.61; 95% CI: 0.40–0.91; P <0.005) was associated with a lower risk of poor functional outcomes, and there was a trend of this becoming a dose-dependent relationship when ASM was classified into quartile groups (Q1–Q4). The statistical significance of the association of the sarcopenia group, diagnosed using both the EWGSOP2 and AWGS criteria, with poor functional outcomes observed in the univariate analyses was not sustained in the multivariate analyses. In the restricted cubic spline model of the relationship between clinical outcomes (functional state and mortality) and height-adjusted ASM (Figure 4), a significant relationship was observed between poor functional outcomes (mRS scores of 4–6) and height-adjusted ASM (P = 0.008). However, there was no significant relationship between mortality and height-adjusted ASM scores (P = 0.860).
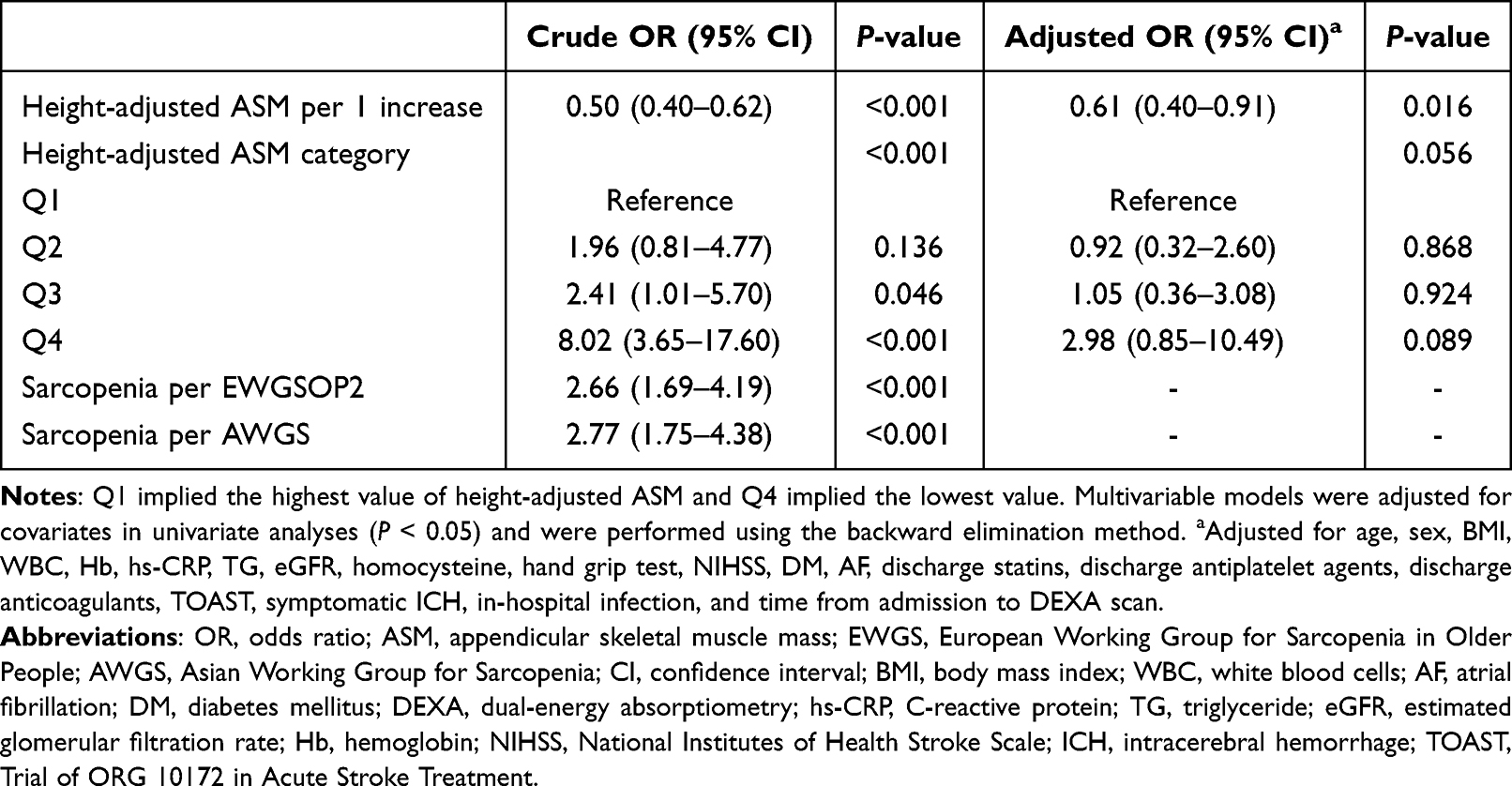 |
Table 3 Univariable and Multivariable Analyses for Poor Functional Outcome |
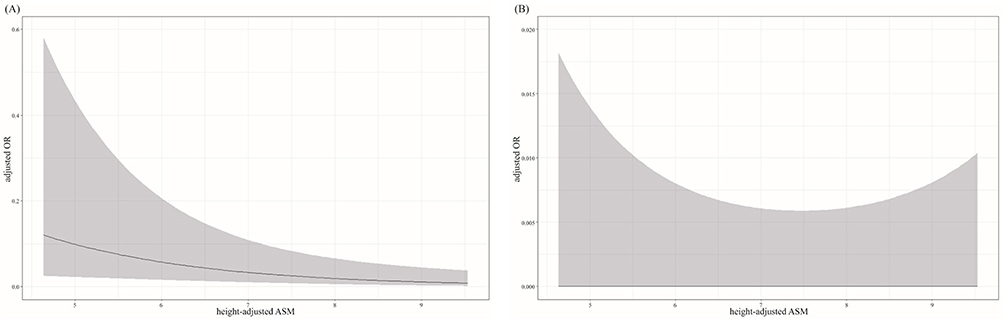 |
Figure 4 Restricted cubic spline models for the relationship between clinical outcome (poor function and mortality) and height-adjusted ASM. (A) Poor functional outcome in relation to height adjusted ASM (P = 0.008). (B) Mortality in relation to height-adjusted ASM (P = 0.860). The adjusted ORs are represented by solid lines and the 95% confidence intervals of the adjusted ORs are represented by shaded areas. The restricted cubic spline model was adjusted for age; sex; body mass index; white blood cell count; hemoglobin levels; high-sensitivity C-reactive protein level; TG; estimated glomerular filtration rate; homocysteine level; National Institute of Health Stroke Scale score; DM; AF; use of statins, antiplatelet agents, and anticoagulants; the Trial of ORG 10172 in Acute Stroke Treatment classification; symptomatic ICH; in-hospital infection; and time from admission to the dual-energy X-ray absorptiometry scan. Abbreviations: OR, odds ratio; ASM, appendicular skeletal muscle mass. |
During the 3-month period, ten patients died. Of these, six patients were diagnosed with sarcopenia, whereas four were not. The univariate analyses demonstrated a positive association between height-adjusted ASM, sarcopenia, and 3-month mortality (Supplementary Table). However, this significance was not observed in the multivariate analyses after adjusting for several confounding factors.
Discussion
In the present study, sarcopenia was investigated by measuring the initial skeletal muscle mass in patients with acute ischemic stroke. The present study investigated the prognostic effects of initial skeletal muscle mass and sarcopenia on functional outcomes and mortality in patients with acute ischemic stroke. We found that height-adjusted ASM significantly affected only poor functional outcomes and not mortality. The higher the height-adjusted ASM of the patients, the lower was their odds ratio of poor functional outcomes, suggesting a negative association between them. However, sarcopenia had a significant effect on 3-month functional outcomes and mortality in the univariate analyses, and this effect was not sustained in the multivariate analyses.
Previous studies have reported that the prevalence of sarcopenia in stroke is 14–18%, and that the increase in sarcopenia due to stroke is greater than the increase with age.20,21 The paralyzed thighs of stroke survivors have been reported to have 20–24% lower muscle area and muscle mass and 17–25% higher intramuscular fat compared to non-paretic thighs.21,22 However, there are few studies on the functional outcomes of stroke in patients with preexisting sarcopenia. A previous study reported that prestroke sarcopenia was observed in 18% of older patients with acute stroke.17
The study revealed that prestroke sarcopenia is an independent predictor of stroke severity, measured using the early NIHSS, and patients with prestroke sarcopenia had a longer hospital stay and worse prognosis than those without sarcopenia.17 However, existing studies have shown low sensitivity because in these studies, sarcopenia was diagnosed using the SARC-F questionnaire. Furthermore, there may have been selection bias because only patients with the cognitive ability to respond to the questionnaire were recruited.
A recent study by Lee et al showed that sarcopenia is independently associated with adverse functional outcomes in patients with mild acute ischemic stroke and transient ischemic attack (TIA).23 This finding is consistent with our results. However, in the study by Lee et al, appendicular skeletal muscle mass was measured using bioelectrical impedance analysis, and sarcopenia was defined according to the AWGS criteria.23 In contrast, in our study, whole-body and/or regional lean tissue mass, including fat, lean tissue mass, and percent body fat, was measured using DEXA, which is considered the gold standard for evaluating body composition.18 In addition, sarcopenia was diagnosed according to the AWGS and EWGSOP2 criteria based on the DEXA method during early hospitalization in patients with stroke, not limited to mild stroke or TIA. These suggest that the reliability and generalizability of our results are likely to be significantly higher than those of the study by Lee et al.23
Although sarcopenia was initially defined as low muscle mass, there is now a consensus that low muscle mass and low muscle function must be combined to define sarcopenia; therefore, the diagnosis of sarcopenia requires a combined measure of muscle mass, strength, and physical performance.2,6,24,25 Various indicators are related to muscle mass, such as ASM, skeletal muscle mass index, height, lower extremity skeletal muscle mass, and lower extremity skeletal muscle mass index. The ASM was adjusted using the square of the height (ASM/ht²) to compare the muscle mass of the participants. This is because previous studies have shown that the square of height in the denominator is the most common power that should be used for minimizing the correlation of the index with height across all sexes, ethnicities, age groups, and study populations.26 Furthermore, previous studies have suggested the correction of overweight/obesity with BMI or body fat mass in chronic diseases.27
Stroke-associated sarcopenia is difficult to distinguish from hemiplegia because they both affect muscle mass, strength, and body function. In a recent revision of the definition of sarcopenia, the shift in the focus of assessment from performance to strength has improved in that it can now be used to assess both non-patients and chronically ill patients.26 Before these changes, it was difficult to assess stroke-related motor dysfunction according to both physical performance and strength, owing to inherent changes in function. Some patients with stroke cannot walk independently or require the help of a gait aid because of severe hemiparesis, imbalance, or ataxia. Even in patients with stroke who can walk, neurological symptoms, such as vertigo, neglect, or sensory impairment, can affect the quality of gait, which makes the gait speed test an inappropriate tool for determining sarcopenia in these patients. Therefore, in this study, we adopted two assessments, including ASM using DEXA and isometric handgrip strength, among the three components that comprise the definition of sarcopenia.
Ryan et al reported a sarcopenia prevalence of 14–18% in stroke survivors.20 In other words, although many studies mention sarcopenia due to stroke, they focused on the cases of sarcopenia accompanying stroke and confirmed that it could seriously affect functional outcomes.20 On the other hand, our study showed a higher prevalence of sarcopenia in patients with acute stroke and a detrimental effect on their functional outcomes. Given these results, it is necessary for clinicians in the field of stroke to understand and pay attention to the clinical implications of sarcopenia as a basic or poststroke comorbidity in patients with stroke. The final step was to develop and validate customized rehabilitation treatments suitable for this condition.
Our study has some noteworthy limitations. First, this was designed as a single-hospital study. Although we prospectively collected the data to reduce bias in terms of patient selection, recording, completeness of data, and assessment of outcomes, generalizing the results of our study is challenging. These findings must be further confirmed in prospective multicenter studies with larger sample sizes. Extensive studies are needed to investigate the possible contribution of preexisting sarcopenia to the incidence, prevalence, and sequelae of stroke. Second, patients who participated in this study were enrolled within 2 days of cerebral infarction, and assessments including DEXA and handgrip tests were mostly performed within 2 days of admission to reduce the possibility of poststroke muscle derangements owing to the stroke itself. Structural changes in muscles can begin several hours after stroke onset because of disrupted synaptic transmission of motor neurons that control the muscles.28,29 The possibility of progressive muscle wasting after stroke may be intervened in rather than reflecting the prestroke muscle mass. Third, because of the difficulty in comprehensively assessing gait and motor function in patients with stroke, this study did not evaluate gait speed or the short physical performance battery test proposed by the EWGSOP2, and data such as cadence and chair stand performance were not included. Additional research is needed to incorporate comprehensive gait and motor evaluations in patients with TIA or minor stroke who have sufficient muscle strength to walk. Fourth, the purpose of this study was to evaluate the effect of basal sarcopenia after stroke, and not changes in muscle mass or follow-up measures in patients with stroke; therefore, only functional outcomes were measured without measuring muscle mass and bone density at 3 months after stroke. However, if muscle mass and bone density were additionally measured 3 months after stroke, it would provide more reliable information. Therefore, further well-designed prospective multicenter or large-sample cohort studies are needed. Finally, the association between sarcopenia and appendicular muscle mass and 3-month mortality in the univariate analyses disappeared after multivariate analyses were performed. This could be attributed to the lower power of the study due to the small event rates and short follow-up period. Therefore, further studies with large-scale sample sizes and long-term follow-up are required to confirm the predictive roles of sarcopenia and appendicular muscle mass.
Conclusion
In conclusion, according to the height-adjusted ASM, sarcopenia may play an important role as an emerging predictor of functional outcomes early after the development of acute ischemic stroke. Furthermore, these markers can help identify patients at a high risk of poor functional outcomes 3 months after ischemic stroke.
Abbreviations
ASM, appendicular skeletal muscle mass; AWGS, Asian Working Group for Sarcopenia; EWGSOP2, European Working Group on Sarcopenia in Older People; DEXA, dual-energy X-ray absorptiometry; mRS, modified Rankin Scale; BMI, body mass index; TC, thigh circumference; NIHSS, National Institute of Health Stroke Scale; s-CRP, high-sensitivity C-reactive protein; eGFR, estimated glomerular filtration rate (eGFR); TIA, transient ischemic attack.
Data Sharing Statement
All data generated or analyzed during this study are included in this article and its Supplementary Material Files. Further inquiries can be directed to the corresponding authors.
Ethics Approval and Informed Consent
The study protocol was approved by the Institutional Review Board of the Korea University (approval no. 2016AS0334). Written informed consent was obtained from all participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Science and ICT (NRF-2020R1C1C1009294) and the Ministry of Education (R2015433).
Disclosure
The authors declare that they have no competing interests.
References
1. Rosenberg IH. Epidemiologic and methodological problems in determining nutritional status of older persons: proceedings of a conference held in Albuquerque, New Mexico, October 19–21, 1988 - summary comments. Am J Clin Nutr. 1989;50:1231–1233. doi:10.1093/ajcn/50.5.1231
2. Fielding RA, Vellas B, Evans WJ, et al. Sarcopenia: an undiagnosed condition in older adults. Current consensus definition: prevalence, etiology, and consequences. International Working Group for Sarcopenia. J Am Med Dir Assoc. 2011;12:249–256. doi:10.1016/j.jamda.2011.01.003
3. Tournadre A, Vial G, Capel F, Soubrier M, Boirie Y. Sarcopenia. Joint Bone Spine. 2019;86:309–314. doi:10.1016/j.jbspin.2018.08.001
4. Pickering ME. Crosstalk between the cardiovascular disease-sarcopenia-osteoporosis triad and magnesium in humans. Int J Mol Sci. 2021;22:9102. doi:10.3390/ijms22169102
5. Chen LK, Woo J, Assantachai P, et al. Asian Working Group for Sarcopenia:2019 Consensus update on sarcopenia diagnosis and treatment. J Am Med Dir Assoc. 2020;21:300–307. doi:10.1016/j.jamda.2019.12.012
6. Cruz-Jentoft AJ, Bahat G, Bauer J, et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing. 2019;48:16–31. doi:10.1093/ageing/afy169
7. Inoue T, Maeda K, Shimizu A, et al. Calf circumference values for sarcopenia screening among older adults with stroke. Arch Gerontol Geriat. 2021;93:104290. doi:10.1016/j.archger.2020.104290
8. Matsushita T, Nishioka S, Taguchi S, Yamanouchi A. Sarcopenia as a predictor of activities of daily living capability in stroke patients undergoing rehabilitation. Geriatr Gerontol Int. 2019;19:1124–1128. doi:10.1111/ggi.13780
9. Yoshimura Y, Wakabayashi H, Nagano F, Bise T, Shimazu S, Shiraishi A. Low hemoglobin levels are associated with sarcopenia, dysphagia, and adverse rehabilitation outcomes after stroke. J Stroke Cerebrovasc Dis. 2020;29:105405. doi:10.1016/j.jstrokecerebrovasdis.2020.105405
10. Yoshimura Y, Bise T, Shimazu S, et al. Effects of a leucine-enriched amino acid supplement on muscle mass, muscle strength, and physical function in post-stroke patients with sarcopenia: a randomized controlled trial. Nutrition. 2019;58:1–6. doi:10.1016/j.nut.2018.05.028
11. Ohyama K, Watanabe M, Nosaki Y, Hara T, Iwai K, Mokuno K. Correlation between skeletal muscle mass deficit and poor functional outcome in patients with acute ischemic stroke. J Stroke Cerebrovasc. 2020;29:245.
12. Nagano F, Yoshimura Y, Bise T, Shimazu S, Shiraishi A. Muscle mass gain is positively associated with functional recovery in patients with sarcopenia after stroke. J Stroke Cerebrovasc. 2020;29:124.
13. Scherbakov N, von Haehling S, Anker SD, Dirnagl U, Doehner W. Stroke-induced sarcopenia: muscle wasting and disability after stroke. Int J Cardiol. 2013;170:89–94. doi:10.1016/j.ijcard.2013.10.031
14. Steffl M, Bohannon RW, Sontakova L, Tufano JJ, Shiells K, Holmerova I. Relationship between sarcopenia and physical activity in older people: a systematic review and meta-analysis. Clin Interv Aging. 2017;12:835–845. doi:10.2147/CIA.S132940
15. Evans WJ. Skeletal muscle loss: cachexia, sarcopenia, and inactivity. Am J Clin Nutr. 2010;91:1123s–1127s. doi:10.3945/ajcn.2010.28608A
16. Seo JH, Lee Y. Association of physical activity with sarcopenia evaluated based on muscle mass and strength in older adults: 2008–2011 and 2014–2018 Korea national Health and Nutrition Examination Surveys. BMC Geriatr. 2022;22:217. doi:10.1186/s12877-022-02900-3
17. Nozoe M, Kanai M, Kubo H, Yamamoto M, Shimada S, Mase K. Prestroke sarcopenia and functional outcomes in elderly patients who have had an acute stroke: a prospective cohort study. Nutrition. 2019;66:44–47. doi:10.1016/j.nut.2019.04.011
18. Plank LD. Dual-energy x-ray absorptiometry and body composition analysis. Curr Opin Clin Nutr. 2005;8:305–309. doi:10.1097/01.mco.0000165010.31826.3d
19. Choi Y, Im S, Park GY. Ultrasound evaluation of the rectus femoris for sarcopenia in patients with early subacute stroke. J Clin Med. 2021;10:3010. doi:10.3390/jcm10143010
20. Ryan AS, Ivey FM, Serra MC, Hartstein J, Hafer-Macko CE. Sarcopenia and physical function in middle-aged and older stroke survivors. Arch Phys Med Rehab. 2017;98:495–499. doi:10.1016/j.apmr.2016.07.015
21. Ryan AS, Dobrovolny CL, Smith GV, Silver KH, Macko RF. Hemiparetic muscle atrophy and increased intramuscular fat in stroke patients. Arch Phys Med Rehab. 2002;83:1703–1707. doi:10.1053/apmr.2002.36399
22. Ryan AS, Buscemi A, Forrester L, Hafer-Macko CE, Ivey FM. Atrophy and intramuscular fat in specific muscles of the thigh: associated weakness and hyperinsulinemia in stroke survivors. Neurorehabil Neural Repair. 2011;25:865–872. doi:10.1177/1545968311408920
23. Lee H, Lee I, Heo J, et al. Impact of sarcopenia on functional outcomes among patients with mild acute ischemic stroke and transient ischemic attack: a retrospective study. Front Neurol. 2022;13. doi:10.3389/fneur.2022.841945
24. Franzon K, Zethelius B, Cederholm T, Kilander L. The impact of muscle function, muscle mass, and sarcopenia on independent aging in very old Swedish men. BMC Geriatr. 2019;19:1–9. doi:10.1186/s12877-019-1142-y
25. Cruz-Jentoft AJ, Baeyens JP, Bauer JM, et al. Sarcopenia: European consensus on its definition and diagnosis: report of the European Working Group on sarcopenia in older people. Age Ageing. 2010;39:412–423. doi:10.1093/ageing/afq034
26. Baumgartner RN, Koehler KM, Gallagher D, et al. Epidemiology of sarcopenia among the elderly in New Mexico. Am J Epidemiol. 1998;147:755–763. doi:10.1093/oxfordjournals.aje.a009520
27. Fonseca GW, Dos Santos MR, de Souza FR, et al. Discriminating sarcopenia in overweight/obese male patients with heart failure: the influence of body mass index. Esc Heart Fail. 2020;7:85–92. doi:10.1002/ehf2.12545
28. Mas MF, Gonzalez J, Frontera WR. Stroke and sarcopenia. Curr Phys Med Rehab. 2020;8:452–460. doi:10.1007/s40141-020-00284-2
29. Arasaki K, Igarashi O, Ichikawa Y, et al. Reduction in the motor unit number estimate (MUNE) after cerebral infarction. J Neurol Sci. 2006;250:27–32. doi:10.1016/j.jns.2006.06.024
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Imaging of Sarcopenia in Type 2 Diabetes Mellitus
Wang D, Zhang G, Yu Y, Zhang Z
Clinical Interventions in Aging 2024, 19:141-151
Published Date: 26 January 2024