Back to Journals » Nature and Science of Sleep » Volume 15
App-Delivered Cognitive-Behavioral Therapy for Insomnia Among Patients with Comorbid Musculoskeletal Complaints and Insomnia Referred to 4-Week Inpatient Multimodal Rehabilitation: Protocol for a Randomized Clinical Trial
Authors Skarpsno ES ![]() , Simpson MR, Seim A, Hrozanova M, Bakøy MA, Klevanger NE, Aasdahl L
, Simpson MR, Seim A, Hrozanova M, Bakøy MA, Klevanger NE, Aasdahl L ![]()
Received 10 June 2023
Accepted for publication 20 September 2023
Published 11 October 2023 Volume 2023:15 Pages 799—809
DOI https://doi.org/10.2147/NSS.S419520
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Valentina Alfonsi
Eivind Schjelderup Skarpsno,1,2 Melanie Rae Simpson,1 Arnfinn Seim,1,3 Maria Hrozanova,1 Marthe Alida Bakøy,3 Nina Elisabeth Klevanger,1 Lene Aasdahl1,3
1Department of Public Health and Nursing, Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology, Trondheim, Norway; 2Department of Neurology and Clinical Neurophysiology, St. Olavs Hospital, Trondheim, Norway; 3Unicare Helsefort Rehabilitation Centre, Rissa, Norway
Correspondence: Eivind Schjelderup Skarpsno, Department of Public Health and Nursing, NTNU, Trondheim, Norway, Tel +47 97521297, Email [email protected]
Background: Insomnia is prevalent among patients receiving treatment for long-term musculoskeletal complaints in inpatient rehabilitation settings. Cognitive-behavioral therapy for insomnia (CBT-I) is effective for improving sleep quality in patients with pain, but a lack of therapists often limits the capacity to use this therapy in rehabilitation programs. The aim of this randomized clinical trial (RCT) is to evaluate the effectiveness of app-delivered CBT-I adjunct to inpatient multimodal rehabilitation for individuals with comorbid musculoskeletal complaints and insomnia, compared with rehabilitation (usual care) only.
Methods: This RCT has two parallel arms: 1) inpatient multimodal rehabilitation and 2) app-delivered CBT-I adjunct to inpatient multimodal rehabilitation. Patients referred to Unicare Helsefort (Norway) with long-term chronic musculoskeletal complaints are invited to the study. Eligible and consenting participants will be randomized to the intervention and usual care at a ratio of 2:1. Assessments will be carried out at baseline (prior to randomization), 6 weeks (at the end of rehabilitation), 3 months (primary outcome), as well as 6 and 12 months after the rehabilitation. The primary outcome is insomnia severity measured at 3 months. Secondary outcomes include pain intensity, health-related quality of life, fatigue, physical function, work ability, expectations about sick leave length, sick leave, and prescribed medication. Exploratory analyses are planned to identify moderators and mediators of the effect of the app-delivered intervention.
Discussion: This RCT will provide novel knowledge about the effectiveness of app-delivered CBT-I as an adjunct to usual care among patients participating in inpatient multimodal pain rehabilitation. Regardless of the results from this trial, the results will improve our understanding of the utility of dCBT-I in the field of rehabilitation and the importance of adding sleep therapy to this patient group.
Trial Registration: This trial was prospectively registered in ClinicalTrials.gov October 10, 2022 (ClinicalTrials.gov identifier: NCT05572697).
Keywords: sleep, sleeplessness, chronic pain, digital therapy
Background
Chronic musculoskeletal pain is among the highest rated causes of years lived with disability and reduced health worldwide.1 Among patients with chronic musculoskeletal pain, as many as 50% may suffer from insomnia.2–4 A growing body of evidence from different settings and methodological approaches indicates that insomnia and insufficient sleep duration can lead to a greater risk and poorer prognosis for chronic musculoskeletal pain conditions.5–9 Insomnia and chronic musculoskeletal pain have therefore become increasingly recognised as co-occurring conditions that often perpetuate and exacerbate each other.10–13
Cognitive-behavioural therapy for insomnia (CBT-I) is recommended as the first-line treatment for insomnia due to its long-term effectiveness.14 CBT-I usually consists of sleep hygiene, stimulus control, sleep restriction, cognitive therapy, and relaxation training.14 An increasing number of randomized controlled trials (RCTs) have shown that CBT-I for patients with comorbid chronic pain and insomnia is effective in reducing sleep problems,15 but with inconsistent findings for pain outcomes.15 CBT-I may also have a beneficial effect on depression, anxiety, and quality of life.16–18 Considering the interplay between insomnia, mental distress, and quality of life,19–21 high-quality sleep therapy for patients with chronic pain could potentially reduce symptoms that hamper the pain prognosis. Although inpatient rehabilitation programs incorporate principles known to be helpful for sleep quality22,23 (eg, physical exercise,24 sleep education and fixed schedules),14 constraints in resources and access to trained therapists means that high-quality individual CBT-I is rarely offered in these programs.25 Therefore, it remains uncertain whether CBT-I for patients referred to rehabilitation programs helps improve insomnia, pain intensity, physical function, and quality of life.
To increase the availability of CBT-I, self-guided, fully automated digital versions of CBT-I (dCBT-I) have been developed.26–28 An advantage of dCBT-I is that it can be an add-on to usual care and thus be more cost-efficient. dCBT-I has been evaluated in patients with insomnia,26–28 but few studies have assessed the effectiveness of dCBT-I among patients with comorbid insomnia and chronic pain.29,30 Some evidence indicates that dCBT-I is beneficial for this group, but previous studies comprised small samples in community or primary care settings.29,30 Thus, there is a lack of sufficiently powered trials examining whether app-delivered CBT-I should be recommended as an add-on to rehabilitation programs for patients with comorbid musculoskeletal pain and insomnia.
This protocol outlines a two-arm, parallel group RCT that will examine the additional benefits of app-delivered CBT-I for patients with comorbid musculoskeletal complaints and insomnia in inpatient rehabilitation compared with usual inpatient rehabilitation. The primary aim of this trial is to evaluate the effectiveness of app-delivered CBT-I on insomnia severity. The secondary aim is to evaluate the effectiveness of the intervention on pain intensity, health-related quality of life, sick leave, and prescribed sleep medication.
Methods
The protocol for the RCT follows the SPIRIT guidelines (Standard Protocol Item for Randomized Trials).31 Figure 1 shows the flow chart for the recruitment and assessments. We have uploaded a completed SPIRIT checklist.
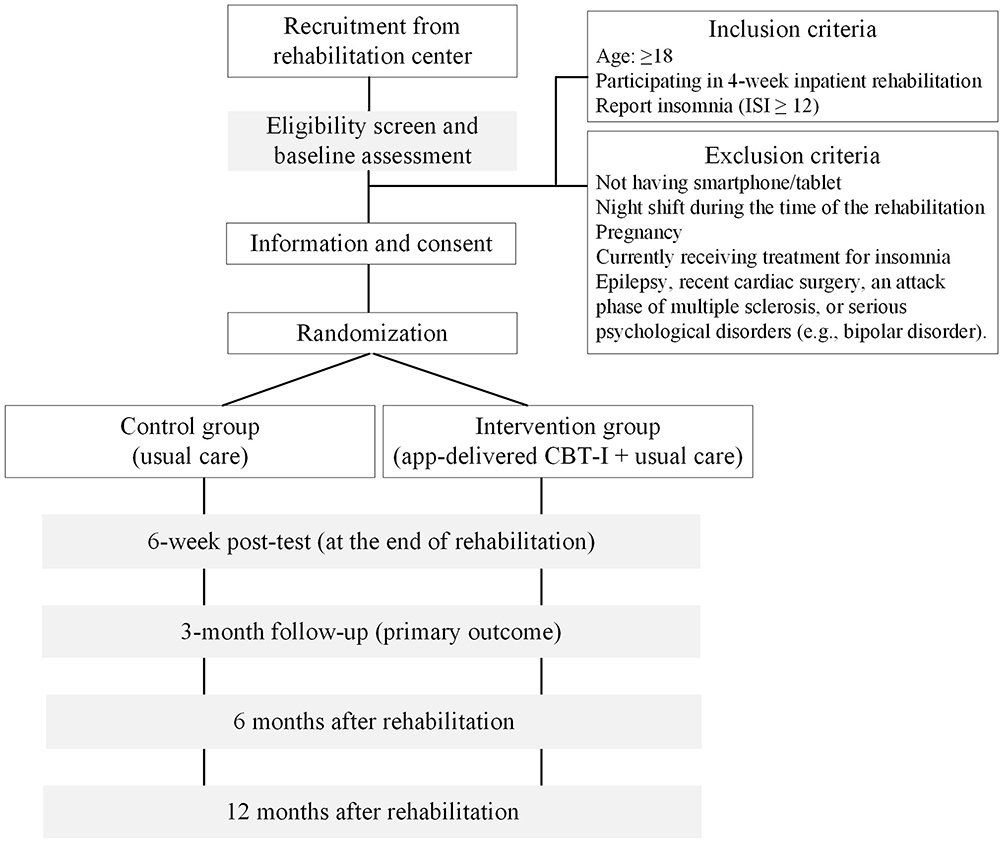 |
Figure 1 Participants’ flow chart. Abbreviations: ISI, Insomnia Severity Index; CBT-I, cognitive behavioural therapy for insomnia. |
Trial Design
This study is designed as a cluster-randomized clinical trial with two parallel groups. The trial is registered at ClinicalTrials.gov (NCT05572697). Results will be reported according to the CONSORT statement.32 The primary outcome will be insomnia severity measured by the Insomnia Severity Index (ISI)33 measured at 3 months after the baseline assessment. This timepoint was chosen to allow sufficient time to complete the digital intervention and to implement the key components of CBT-I. Secondary outcomes include pain intensity, fatigue, physical function, workability and health-related quality of life at 3 months, as well as assessment of all outcomes at 6 and 12 months after the rehabilitation to evaluate long-term gains associated with the intervention. Registry data will be used to assess the use of sleep and pain medications and sick leave during 12 months of follow-up. In addition, exploratory analyses will be carried out to identify patient and characteristics influencing the effect of the dCBT-I intervention on insomnia severity, pain intensity and quality of life.
Study Population
Potential participants are patients taking part in rehabilitation at Unicare Helsefort due to long-term musculoskeletal pain complaints. The program is group-based, and the patients are placed in groups of ~10 patients. Referrals to the rehabilitation center are done by the patients’ general practitioner or by specialist healthcare providers, mainly the pain clinic at St. Olav’s Hospital. All referrals are considered at a regional assessment unit where patients are evaluated against criteria for rehabilitation in specialist health care. Only adults are accepted for the rehabilitation program. There is no upper age limit, but most patients are of working age. The rehabilitation program lasts 4 weeks, usually 2+2 weeks with 2 weeks at home in between. For some groups, the program lasts continuously for 4 weeks, but this is an exception when necessary to run the center. Inclusion criteria for the current study are age ≥18 years, taking part in 4-week inpatient rehabilitation due to long-term musculoskeletal complaints, and Insomnia Severity Index (ISI) score ≥12. Exclusion criteria are: not having a smartphone or tablet, a work schedule that includes night shifts during the time of the intervention, pregnancy, inadequate opportunity to sleep or living circumstances that prevent modification of sleep patterns such as having an infant, currently receiving psychological treatment for insomnia, or medical history of contraindicating use of CBT-I such as epilepsy, recent cardiac surgery, an attack phase of multiple sclerosis, or serious psychological disorders (eg, bipolar disorder).
Interventions
Usual Care
Participants randomized to usual care will receive the standard inpatient rehabilitation program. This is a traditional rehabilitation program consisting of physical activity, mindfulness exercises, psychoeducation and acceptance and commitment therapy.34 Even though the program is group-based, all patients have an assigned clinician for one-to-one consultations for goal setting and creation of a rehabilitation plan. One of the consultations includes an educational session about sleep, focusing on the importance of sleep and sleep hygiene. Although its content overlaps with some of the dCBT-I intervention content, it does not include any of the interactive features of the dCBT-I intervention.
App-Delivered CBT-I
In addition to the standard rehabilitation program, participants randomized to dCBT-I will receive the sleep intervention delivered via a smartphone app. In short, the trial will use a Norwegian dCBT-I program “Assisted Self-Help”. The app is fully automated and requires no contact with healthcare personnel. It can also be assessed on computers, but in the present project participants will use the app version only. The self-managing dCBT-I program includes six modules (Table 1) consisting of sleep hygiene, stimulus control (pairing the bed with sleep), introduction to sleep restriction (reducing time in bed to increase sleep pressure), cognitive interventions (challenging dysfunctional thoughts about sleep loss), and relaxation training. The modules also consist of learning material, such as quizzes and educational information about sleep. Patients will be instructed to use the app during the 6 initial weeks of the inpatient rehabilitation. They can go through the app at their own pace but are recommended to complete one module a week. Prior to the module on sleep restriction, patients fill out a sleep diary for minimum 7 days. Patients will also receive tasks in the modules (eg, write sleep diary, try sleep restriction, and change lifestyle behavior) that facilitate self-management and focus on an active role in reducing insomnia. During rehabilitation, the patients’ assigned clinician will secure compliance with the intervention and clarify questions the patients might have.
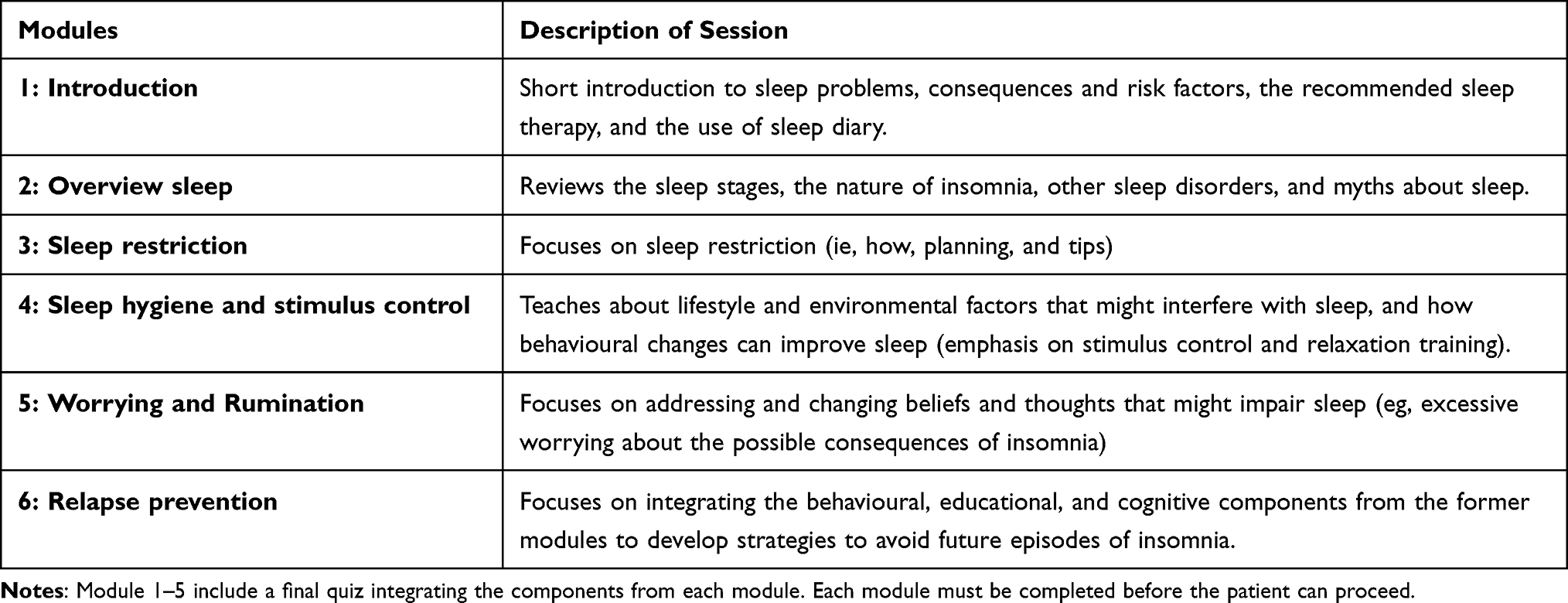 |
Table 1 Description of App-Delivered Cognitive-Behavioral Therapy for Insomnia (CBT-I) Sessions During the Intervention Period |
Recruitment and Randomization
Inclusion of patients started in October 2022. Patients will fill out questionnaires when arriving at the center (part of usual care). Patients who score ≥12 on Insomnia Severity Index (ISI) will be informed about the project by their assigned clinician and receive written information about the project. Before consenting, patients will also attend an information meeting with the researchers. Patients who consent will then be randomized to receiving usual care + dCBT-I or usual care only.
The randomization will be at group level to avoid contamination between members of the same rehabilitation group and will be performed after all eligible group members have consented to participation. Each group will be randomised using a computer-generated block randomisation provided by the Clinical Research Unit (Klinforsk) at the Faculty of Medicine and Health Sciences at the Norwegian University of Science and Technology. The research team will not be able to influence the randomization process in any way. Blinding is impossible as the participants will know whether they receive dCBT-I. Moreover, the patients’ assigned clinician will know whether the patient receive dCBT-I or not during the rehabilitation.
Assessments
Data consist of questionnaires and registry data. Questionnaire data are obtained at 5 different time points: at baseline (prior to randomization); 6 weeks (at the end of rehabilitation); 3 months (primary outcome measurement); and 6 and 12 months after rehabilitation (ie, 7.5 and 13.5 months after randomization). Self-reported measurements will be delivered by CheckWare – a survey tool developed to track patients in clinical settings and research. Participants will receive a link to the questionnaires by SMS and can answer using a smartphone, tablet, or computer. Table 2 summarizes the timing of all assessments. Participants will receive 3 reminders prompting them to complete the questionnaire at each time point if they do not respond. Registry-based data will be obtained at 12 months from national registries and contain data for the whole follow-up period. All data storage and analysis will be conducted according to regulations by the Norwegian University of Science and Technology and follow the General Data Protection Regulation. Data will not be disclosed to researchers outside the project or transferred to countries outside the European Economic Area.
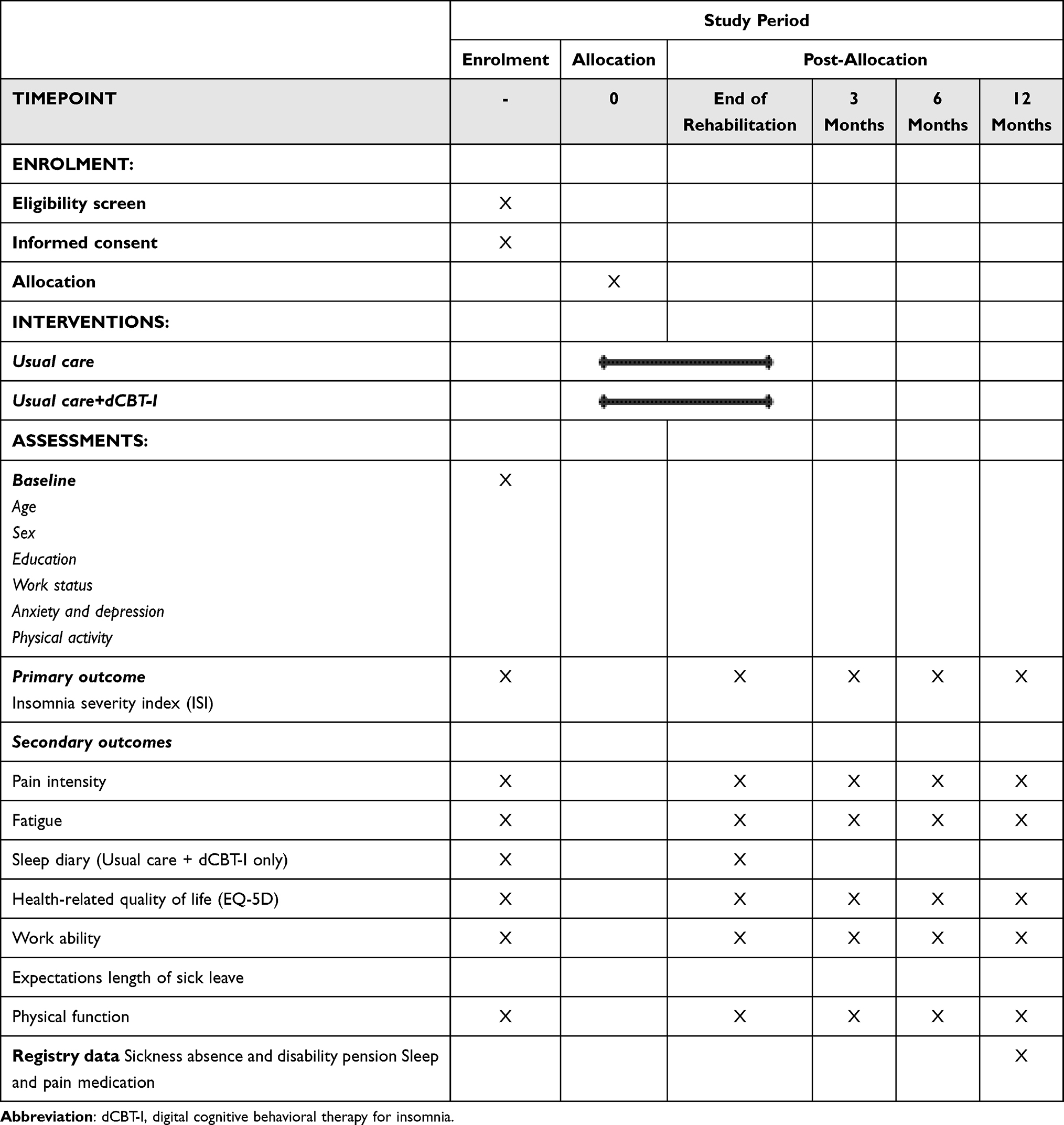 |
Table 2 The Schedule of Enrolment, Interventions, and Assessments |
Demography
As shown in Table 2, key demographic information will be assessed at baseline. The demographic questionnaire includes questions on sex, age, number of children, living situation (live alone or with someone), education level (primary school, high school, college university up to and above 4 years), work status (full time, part time, disability or retirement pension), employment fraction (percent), type of work (mostly sedentary, walking, lifting or physical demanding), whether they enjoy their work (measured on a 0–10 scale; 10 very happy) and whether they are currently receiving medical benefits (yes/no).
Sleep Measures
Primary outcome will be the ISI. ISI is the recommended outcome measure in sleep research33 and the gold standard self-report measure of insomnia severity in clinical practice, consisting of seven items assessing symptoms of insomnia such as difficulty falling or staying asleep, satisfaction with sleep, and degree of impairment with daytime functioning. The total score of ISI ranges from 0 to 28: 0 to 7 (no clinical insomnia), 8 to 14 (sub-threshold insomnia), 15 to 21 (insomnia of moderate severity), and 22 to 28 (severe insomnia). ISI has been validated and has proven sensitive to therapeutic changes.33 Patients will also be asked to digitally provide daily subjective estimates of their sleep, daily function, and pain intensity for minimum 7 consecutive days.
Measures of Somatic Symptoms and Health
Secondary outcomes will include pain scored on 0 to 100 scale (visual analogue scale), fatigue, and health-related quality of life. Fatigue in the last week will be measured using a visual analogue scale from 0 to 100. The EuroQol EQ5D-5L questionnaire35 will be used to assess health-related quality of life. The questionnaire consists of five items assessing mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Items are scored on a 5-point scale, following the format “no problems”, “slight problems”, “moderate problems”, “severe problems”, and “unable to” “extreme problems” for all items. The index value range ranges from −0.285 to 1, where lower values indicate poorer health-related quality of life.
Physical function will be measured by the Patient-Specific Functional Scale where participants are asked to identify important activities that they are unable to perform due to their pain and then to rate the current level of difficulty on a scale from 0 to 10.36 Work ability will be measured by the work ability index single item (self-assessed work ability on a 0–10 scale)37 and expectations about length of sick leave with the item “What are the chances that you are back at work in 6 months?” on a 0–10 scale.
At baseline, we will also measure symptoms of anxiety and depression using the Hopkins Symptom Checklist-25 (HSCL-25)38 and physical activity by a questionnaire adapted from the Trøndelag Health Study (HUNT Study)39,40 which consists of three questions about frequency, duration and intensity of physical activity per week.40
Registry Data
Data will be obtained from the Norwegian Prescription Database and the National Insurance Administration (NAV). From the prescription registry, we will obtain data on use of sleep and pain medications and assess the proportion of participants that obtain prescriptions of these medications during 12 months of follow-up. From NAV, we will obtain data on use of medical benefits like sickness absence, work assessment allowance and disability pensions. Sick leave outcomes will include both total number of days on sick leave during 12 months and the probability of being at work each month during the same period.
Statistical Analytical Plan
Descriptive statistics will be stratified by group allocation. Categorical and binary variables will be presented as counts and percentages, continuous variables will be presented as means and standard deviations (SD) or medians and interquartile range (IQR), as appropriate. A statistical analysis plan will be published prior to conducting the analyses.
Effect analyses of primary and secondary outcomes will be performed with an intention-to-treat (ITT) principle. The primary ITT analysis will estimate mean differences with 95% CI in ISI between the two groups at 3-month follow-up using a linear mixed model. We plan to use linear mixed model analysis to examine the change between baseline and postintervention on the primary and secondary outcome with continuous variables (ie, insomnia severity, health-related quality of life, pain intensity, fatigue, work ability and physical function). The model will include time, time–group interaction and baseline covariates.41 We do not anticipate strong cluster-level effects; however, we will conduct a sensitivity analysis including rehabilitation group in the mixed linear model with follow-up timepoints as level 1, participants as level 2, and rehabilitation group as level 3. For binary secondary outcomes (eg, clinically relevant change in ISI), logistic mixed model analysis will be used.
The main analyses will focus on the ITT analyses, but per-protocol analyses will be reported for individuals who complete ≥4 dCBT-I modules. Since we do not expect any adverse effects of the dCBT and because the patients receive medical supervision during the 4-week rehabilitation, we do not plan interim analyses.
We plan to conduct exploratory analyses identifying whether changes in pain intensity and fatigue mediate the effect of dCBT-I on insomnia severity. Likewise, we will identify whether changes in insomnia symptoms and fatigue mediate the effect on pain severity. We will follow the international, consensus-based guidance for the reporting of mediation analyses of randomized trials.42 Moreover, we will explore whether demographics (eg, age, sex), symptoms of anxiety and depression, pain intensity, and level of physical activity at baseline moderate the effect of dCBT-I on primary and secondary outcomes.
Sample Size
We anticipate that around five of 10 patients will have insomnia within each rehabilitation group and that the average ISI-score for participants completing usual treatment will be 15 (SD = 4). A 4-point improvement on the ISI score is considered clinically relevant. In order to maximize the number of participants receiving the additional treatment (dCBT-I), we will randomize the participants to the intervention and usual care at a ratio of 2:1. Recruiting 15 clusters with 2:1 randomization will achieve 80% power to detect a 4-point difference between the intervention and usual treatment group, with a conservative assumption that the intraclass correlation is 0.2 and the coefficient of variation in cluster size up to 0.7, and with a significance level of 5%. This would mean that around 150 participants will be screened to give an expected sample size of 75 (50 in dCBT-I + usual care and 25 in usual care). We expect a dropout rate of approximately 20% and that around 50% of the participants in the intervention group will complete at least four of the dCBT-I modules. Given that the per-protocol analysis is of particular interest in this study, we aim to recruit 21 clusters to account for the fact that we expect an average of four participants per cluster in the control group to complete the follow-up, and an average of two participants in the intervention group to complete at least four of the modules and attend the follow-up.
Dissemination, and Auditing
For the scientific community, results will be presented in international peer-reviewed publications and at national and international conferences. Clinicians at the rehabilitation center will be informed about the results through internal educational sessions. Results will be disseminated regardless of the magnitude or direction of the effect of the dCBT-I. Efforts will also be placed to disseminate the findings to patient representatives and the public, to guide further implementation if the intervention is shown to be effective. For the public, we will publish results in blogs and social media (eg, Twitter, Facebook). We will not use any of the data or results for commercial purposes. The investigators will adhere to international guidelines regarding authorships of manuscripts.
Trial conduct will be audited in line with NTNU’s guidelines, involving the possibility of an internal quality-assuring control where project information, data management systems, formal approvals, protocol amendments, etc. may be audited. Moreover, clinicians at the rehabilitation center will follow the data collection closely and provide support to any participants experiencing issues with the data collection.
Discussion
The utility of app-delivered CBT-I in chronic pain patients and its impact on insomnia severity, pain intensity, fatigue, physical function, health-related quality of life, sick leave, and prescribed medication is not fully understood. This article outlines the protocol for the first study to examine whether adding dCBT-I adjunct to inpatient multimodal rehabilitation confers benefits over usual care in a rehabilitation setting with chronic pain patients. Regardless of the results from this trial, the results will improve our understanding of the utility of dCBT-I in the field of rehabilitation and the importance of adding sleep therapy to this patient group.
Strengths and Limitations of This Study
The strengths of the trial include adequate power to detect changes in the primary outcome; high recruitment rate due to the availability of patients referred from the patients’ general practitioner or by specialist healthcare providers; close collaboration with physiotherapists, medical doctors, social workers, and nurses throughout the intervention period; and the inpatient setting where the patients’ assigned clinician secures compliance with the intervention. Moreover, we expect high response-rate since completion of web-based questionnaires is already part of the rehabilitation program, and because patients referred to the rehabilitation typically have high treatment adherence during the 4-week inpatient program. However, it should be noted that the effect of the therapy is limited to patients who have a smartphone and adequate digital literacy skills to engage with the intervention. Moreover, previous studies show that many patients allocated to the digital intervention do not complete the core elements of the treatment,26,28,43 and it is therefore uncertain whether this group of patients will complete all dCBT-I modules. Finally, the study will include patients referred to the rehabilitation center by general practitioners or by specialist healthcare providers and they must be willing to leave their home for 4 weeks. The included patient group might therefore be complex in terms of pain severity, insomnia severity, mental distress, and physical function. This may limit the generalizability of results to a selected group of patients with long-term pain conditions who fulfill the inclusion criteria to be referred to extensive inpatient rehabilitation programs.
If our results show benefits of adding dCBT-I to usual inpatient care, our trial will inform clinical guidelines and potentially influence the treatment of patients with chronic musculoskeletal pain who also report insomnia. Moreover, our trial will also explore whether patient characteristics influence the therapeutic response of dCBT-I, knowledge that can help to better tailor the therapy to people with different degrees of insomnia, pain intensity, and anxiety and depression. If dCBT-I is found to be efficacious, our results will provide a novel approach that health professionals can incorporate into their treatment program and thus optimize outcomes for patients in inpatient rehabilitation.
Abbreviations
CBT-I, Cognitive-behavioral therapy for insomnia; CI, Confidence interval; dCBT-I, Digital cognitive-behavioral therapy for insomnia; HSCL-25, Hopkins Symptom Checklist-25; ISI, Insomnia Severity Index; ITT, intention-to-treat; NAV, National Insurance Administration; NTNU, Norwegian University of Science and Technology; RCT, Randomized controlled trial; SD, Standard deviation.
Data Monitoring
On a monthly basis, the principal investigator, the leader of referrals and quality at Unicare Helsefort, and members of the research team will review the recruitment, enrolment, data collection, conduct of the intervention, and completion of the trial. If needed, this team will discuss appropriate actions to any inconsistencies or unexpected events.
Data Sharing Statement
Patient-level data will not be made publicly available, but anonymized patient-level data can be made available to interested investigators upon submitting a reasonable research request. Statistical codes will be added to supplementary analyses when publishing results from the trial.
Ethics Approval and Consent to Participate
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. This trial is approved by the Regional Committee for Medical and Health Research Ethics in Central Norway (reference number 496297). All participants will be informed about the study and sign a consent before study entry. They will be informed that they can withdraw from the study at any time without any consequences for their future rehabilitation. Participants receiving the intervention might experience being more tired during the day in the beginning of the intervention. However, as they are taking part in inpatient rehabilitation, there are clinicians who can answer questions. In addition, participants can contact the researchers with any questions about the project. Any amendment to the protocol that might impact the conduct of the trial will be submitted for approval to the ethical committee prior to implementation and the clinical trial registry (ClinicalTrials.gov) will be updated.
Acknowledgment
We wish to thank clinicians and staff at Unicare Rehabilitation Center for help with collecting data and carrying out the study. We would also like to thank the patient users for their valuable input to the project, and the participants who are participating in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors. No funders have been involved in designing this study.
Disclosure
Lene Aasdahl, Arnfinn Seim and Marthe A. Bakøy are employed at Unicare Helsefort. Aasdahl is the leader for research and development; Seim is a physician; and Bakøy is a quality leader. The other authors have nothing to declare for this work.
References
1. Global, regional, and national incidence, prevalence, and years lived with disability for. 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the global burden of disease study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/S0140-6736(18)32279-7
2. Kelly GA, Blake C, Power CK, O’Keeffe D, Fullen BM. The association between chronic low back pain and sleep: a systematic review. Clin J Pain. 2011;27(2):169–181. doi:10.1097/AJP.0b013e3181f3bdd5
3. Alsaadi SM, McAuley JH, Hush JM, Maher CG. Prevalence of sleep disturbance in patients with low back pain. Eur Spine J. 2011;20(5):737–743. doi:10.1007/s00586-010-1661-x
4. Tang NK, Wright KJ, Salkovskis PM. Prevalence and correlates of clinical insomnia co-occurring with chronic back pain. J Sleep Res. 2007;16(1):85–95. doi:10.1111/j.1365-2869.2007.00571.x
5. Skarpsno ES, Mork PJ, Nilsen TIL, Steingrimsdottir OA, Zwart JA, Nilsen KB. The interplay between sleeplessness and high-sensitivity C-reactive protein on risk of chronic musculoskeletal pain. longitudinal data from the Tromso study. Sleep. 2019;42(9):zsz127. doi:10.1093/sleep/zsz127
6. Skarpsno ES, Mork PJ, Hagen K, Nilsen TIL, Marcuzzi A. Number of chronic nighttime insomnia symptoms and risk of chronic widespread pain and pain-related disability: the HUNT study. Nat Sci Sleep. 2020;12:1227–1236. doi:10.2147/NSS.S284498
7. Broberg M, Karjalainen J, Ollila HM. Mendelian randomization highlights insomnia as a risk factor for pain diagnoses. Sleep. 2021;44(7):7. doi:10.1093/sleep/zsab025
8. Smith MT, Edwards RR, McCann UD, Haythornthwaite JA. The effects of sleep deprivation on pain inhibition and spontaneous pain in women. Sleep. 2007;30(4):494–505. doi:10.1093/sleep/30.4.494
9. Haack M, Sanchez E, Mullington JM. Elevated inflammatory markers in response to prolonged sleep restriction are associated with increased pain experience in healthy volunteers. Sleep. 2007;30(9):1145–1152. doi:10.1093/sleep/30.9.1145
10. Afolalu EF, Ramlee F, Tang NKY. Effects of sleep changes on pain-related health outcomes in the general population: a systematic review of longitudinal studies with exploratory meta-analysis. Sleep Med Rev. 2018;39:82–97. doi:10.1016/j.smrv.2017.08.001
11. Koffel E, Kroenke K, Bair MJ, Leverty D, Polusny MA, Krebs EE. The bidirectional relationship between sleep complaints and pain: analysis of data from a randomized trial. Health Psychol. 2016;35(1):41–49. doi:10.1037/hea0000245
12. Ho KKN, Skarpsno ES, Nilsen KB, et al. A bidirectional study of the association between insomnia, high-sensitivity C-reactive protein, and comorbid low back pain and lower limb pain. Scand J Pain. 2022;23(1):110–125. doi:10.1515/sjpain-2021-0197
13. Skarpsno ES, Mork PJ, Nilsen TIL, Nordstoga AL. Influence of sleep problems and co-occurring musculoskeletal pain on long-term prognosis of chronic low back pain: the HUNT Study. J Epidemiol Community Health. 2020;74(3):283–289. doi:10.1136/jech-2019-212734
14. Riemann D, Baglioni C, Bassetti C, et al. European guideline for the diagnosis and treatment of insomnia. J Sleep Res. 2017;26(6):675–700. doi:10.1111/jsr.12594
15. Selvanathan J, Pham C, Nagappa M, et al. Cognitive behavioral therapy for insomnia in patients with chronic pain - A systematic review and meta-analysis of randomized controlled trials. Sleep Med Rev. 2021;60:101460. doi:10.1016/j.smrv.2021.101460
16. Alimoradi Z, Jafari E, Broström A, et al. Effects of cognitive behavioral therapy for insomnia (CBT-I) on quality of life: a systematic review and meta-analysis. Sleep Med Rev. 2022;64:101646. doi:10.1016/j.smrv.2022.101646
17. Cheng P, Luik AI, Fellman-Couture C, et al. Efficacy of digital CBT for insomnia to reduce depression across demographic groups: a randomized trial. Psychol Med. 2019;49(3):491–500. doi:10.1017/S0033291718001113
18. Espie CA, Emsley R, Kyle SD, et al. Effect of digital cognitive behavioral therapy for insomnia on health, psychological well-being, and sleep-related quality of life: a randomized clinical trial. JAMA Psychiatry. 2019;76(1):21–30. doi:10.1001/jamapsychiatry.2018.2745
19. Lee S, Kim JH, Chung JH. The association between sleep quality and quality of life: a population-based study. Sleep Med. 2021;84:121–126. doi:10.1016/j.sleep.2021.05.022
20. LeBlanc M, Mérette C, Savard J, Ivers H, Baillargeon L, Incidence MMC. Risk factors of insomnia in a population-based sample. Sleep. 2009;32(8):1027–1037. doi:10.1093/sleep/32.8.1027
21. Sun X, Liu B, Liu S, et al. Sleep disturbance and psychiatric disorders: a bidirectional Mendelian randomisation study. Epidemiol Psychiatr Sci. 2022;31:e26. doi:10.1017/S2045796021000810
22. Braathen TN, Veiersted KB, Heggenes J. Improved work ability and return to work following vocational multidisciplinary rehabilitation of subjects on long-term sick leave. J Rehabil Med. 2007;39(6):493–499. doi:10.2340/16501977-0081
23. Gismervik S, Aasdahl L, Vasseljen O, et al. Inpatient multimodal occupational rehabilitation reduces sickness absence among individuals with musculoskeletal and common mental health disorders: a randomized clinical trial. Scand J Work Environ Health. 2020;46(4):364–372. doi:10.5271/sjweh.3882
24. Kredlow MA, Capozzoli MC, Hearon BA, Calkins AW, Otto MW. The effects of physical activity on sleep: a meta-analytic review. J Behav Med. 2015;38(3):427–449. doi:10.1007/s10865-015-9617-6
25. Grandner MA, Chakravorty S. Insomnia in primary care: misreported, mishandled, and just plain missed. J Clin Sleep Med. 2017;13(8):937–939. doi:10.5664/jcsm.6688
26. Ritterband LM, Thorndike FP, Ingersoll KS, et al. Effect of a web-based cognitive behavior therapy for insomnia intervention with 1-year follow-up: a randomized clinical trial. JAMA Psychiatry. 2017;74(1):68–75. doi:10.1001/jamapsychiatry.2016.3249
27. Zachariae R, Lyby MS, Ritterband LM, O’Toole MS. Efficacy of internet-delivered cognitive-behavioral therapy for insomnia – a systematic review and meta-analysis of randomized controlled trials. Sleep Med Rev. 2016;30:1–10. doi:10.1016/j.smrv.2015.10.004
28. Vedaa Ø, Kallestad H, Scott J, et al. Effects of digital cognitive behavioural therapy for insomnia on insomnia severity: a large-scale randomised controlled trial. Lancet Digit Health. 2020;2(8):e397–e406. doi:10.1016/S2589-7500(20)30135-7
29. Shaffer KM, Camacho F, Lord HR, et al. Do treatment effects of a web-based cognitive behavioral therapy for insomnia intervention differ for users with and without pain interference? A secondary data analysis. J Behav Med. 2020;43(3):503–510. doi:10.1007/s10865-019-00065-w
30. Wiklund T, Molander P, Lindner P, Andersson G, Gerdle B, Dragioti E. Internet-delivered cognitive behavioral therapy for insomnia comorbid with chronic pain: randomized controlled trial. J Med Internet Res. 2022;24(4):e29258. doi:10.2196/29258
31. Chan AW, Tetzlaff JM, Gøtzsche PC, et al. SPIRIT 2013 explanation and elaboration: guidance for protocols of clinical trials. BMJ. 2013;346:e7586. doi:10.1136/bmj.e7586
32. Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c869. doi:10.1136/bmj.c869
33. Morin CM, Belleville G, Bélanger L, Ivers H. The insomnia severity index: psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep. 2011;34(5):601–608. doi:10.1093/sleep/34.5.601
34. Hayes SC, Strosahl K, Wilson KG. Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change. New York: Guilford Press; 1999.
35. Herdman M, Gudex C, Lloyd A, et al. Development and preliminary testing of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res. 2011;20(10):1727–1736. doi:10.1007/s11136-011-9903-x
36. Stratford P, Gill C, Westaway M, Binkley J. Assessing disability and change on individual patients: a report of a patient specific measure. Physiother Can. 1995;47(4):258–263. doi:10.3138/ptc.47.4.258
37. Ahlstrom L, Grimby-Ekman A, Hagberg M, Dellve L. The work ability index and single-item question: associations with sick leave, symptoms, and health–a prospective study of women on long-term sick leave. Scand J Work Environ Health. 2010;40436.
38. Derogatis LR, Lipman RS, Rickels K, Uhlenhuth EH, Covi L. The Hopkins Symptom Checklist (HSCL): a self-report symptom inventory. Behav Sci. 1974;19(1):1–15. doi:10.1002/bs.3830190102
39. Åsvold BO, Langhammer A, Rehn TA, et al. Cohort Profile Update: The HUNT Study, Norway. Int J Epidemiol. 2022;50(6):1995–2010. doi:10.1093/ije/dyab203
40. Kurtze N, Rangul V, Hustvedt BE, Flanders WD. Reliability and validity of self-reported physical activity in the nord-trøndelag health study: HUNT 1. Scand J Public Health. 2008;36(1):52–61. doi:10.1177/1403494807085373
41. Twisk J, Bosman L, Hoekstra T, et al. Different ways to estimate treatment effects in randomised controlled trials. Contemp Clin Trials Commun. 2018;10:80–85. doi:10.1016/j.conctc.2018.03.008
42. Lee H, Cashin AG, Lamb SE, et al. A guideline for reporting mediation analyses of randomized trials and observational studies: the AGReMA statement. JAMA. 2021;326(11):1045–1056. doi:10.1001/jama.2021.14075
43. Freeman D, Sheaves B, Goodwin GM, et al. The effects of improving sleep on mental health (OASIS): a randomised controlled trial with mediation analysis. Lancet Psychiatry. 2017;4(10):749–758. doi:10.1016/S2215-0366(17)30328-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.