")
Back to Journals » International Journal of General Medicine » Volume 16
Anxiety, Depression, Quality of Life, and Family Support Among Family Caregivers of Children with Disabilities
Authors Xia C, Wei T, Tang Q, Zheng H, Sun M, Chen G, Lv J
Received 22 August 2023
Accepted for publication 20 October 2023
Published 3 November 2023 Volume 2023:16 Pages 5063—5075
DOI https://doi.org/10.2147/IJGM.S434900
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mihajlo Jakovljevic
Cong Xia,1 Ting Wei,2,3 Qi Tang,2,3 Hongying Zheng,2,3 Mei Sun,2,3 Gang Chen,2,3 Jun Lv2,3
1School of Health Management Anhui Medical University, Hefei, People’s Republic of China; 2School of Public Health, Fudan University, Shanghai, People’s Republic of China; 3China Research Center on Disability, Fudan University, Shanghai, People’s Republic of China
Correspondence: Gang Chen; Jun Lv, School of Public Health, Fudan University, 130 Dong’an Road, Xuhui District, Shanghai, 200032, People’s Republic of China, Tel +86-13661432703 ; +86-13671684324, Email [email protected]; [email protected]
Purpose: To investigate the family support, anxiety, depression, health-related quality of life (HRQoL), and their associations among parents and grandparents of children with disabilities.
Methods: This is a cross-sectional study and a total of 327 family caregivers were included. Chi-square test, Mann–Whitney U-test, and two independent t-test were used to identify the intergenerational differences in sociodemographic characteristics, received family support, anxiety, depression, and HRQoL. Eight generalized linear models were developed to examine the associations in both generations.
Results: Parents and grandparents were most in need of rehabilitation and financial support, but both populations received the least amount of financial support. 33.6% and 36.1% of family caregivers had the risk of anxiety and depression and found no significant intergenerational differences. As for HRQoL, intergenerational differences were found in the physical component score, but not found in the mental component score. Among parents, childcare support of respite care and household tasks assistance was negatively associated with their depression (p< 0.05), professional support of appropriate surgery for children (p< 0.05) and psychological support from professional psychologists (p< 0.01) were negatively associated with their anxiety and depression, psychological support from relatives and friends was negatively associated with their depression (p< 0.05) whereas was positively associated with their mental HRQoL (p< 0.01). As for grandparents, financial support for daily living expenses was negatively associated with depression (p< 0.05), and psychological support from families was negatively associated with depression (p< 0.05) whereas was positively associated with mental HRQoL (p< 0.05). However, no relationship was found between family support and anxiety among grandparents. Notably, no association was found between family support and physical HRQoL among both populations.
Conclusion: Both parents and grandparents had high risks of anxiety, depression and low levels of mental HRQoL. To efficiently improve psychological health, care providers and policymakers may consider intergenerational differences and provide targeted family support.
Keywords: mental health, health-related quality of life, family support, children with disabilities, intergenerational differences
Introduction
Childhood disability is a growing global health priority, and around 95 million children aged 0–14 live with some form of disability worldwide.1 It is also a traumatic event for the entire family, and with it comes feelings of guilt, complaint, concern, sadness, and frustration among family caregivers.2 Besides, a child with a disability usually has multiple care and rehabilitation needs, consequently requiring increased time, money, and energy from family caregivers.3 Compared with family caregivers of typically developing children, evidence showed that family caregivers of children with disabilities are chronically plagued by economic burdens, lack of practical parenting skills and information, little personal time, stigma in society, or other problems.4–6 Therefore, this population usually has more needs for information, community service, finance, and family functioning.7 According to Lazarus and Folkman, stress emerges when the needs of family caregivers exceed their resources.8 And if the family support is insufficient, stress can in turn lead to poor well-being. Specifically, researchers reported high levels of parenting stress,9 anxiety, depression,10 and low levels of health-related quality of life (HRQoL)11 among this population.
To alleviate the psychological distress of family caregivers, and facilitate the healthy development of children, it is important to satisfy the multidimensional needs of family caregivers.12,13 Family support means a set of strategies directed to the family unit with the overarching purpose to benefit the family members with disabilities, and it is one critical means of meeting family needs.14 From the perspective of sources of support, family support can be divided into formal and informal support, such as support from parents, relatives, friends, colleagues, childcare providers, and so on.15 From the perspective of types of support, family support is identified into four types: emotional, physical, material/instrumental, and informational support.16,17 It incorporates many facets of assistance associated with daily caring for a child with a disability and is one important way to enable and empower families to cope with challenges. Existing literature shows higher levels of family support are associated with better family quality of life.18 Nevertheless, internationally available research on the relationship between family support and their anxiety, depression, and HRQoL is limited.
Nowadays, besides parents, grandparents have been playing an increasingly pivotal role in childcare and family functioning, especially in families of children with disabilities.19,20 In many countries around the world, grandparents take on the responsibility of caring for grandchildren to alleviate the negative impact on their adult offspring.21 Some grandparents also describe themselves as feeling the double burden of caring for both their adult children and grandchildren.22 Therefore, grandparents may experience similar psychological distress to parents of children with disabilities. However, limited research paid attention to grandparents of children with disabilities, and little is known about their well-being and the family support they received. Previous research pointed to the discrepancies between parents and grandparents in knowledge, parenting skills, coping strategies, and so on.23,24 These indicate that grandparents may have different experiences, needs, and received different family support from parents even if they care for the same child. Therefore, this study aims to investigate the intergenerational differences in received family support, anxiety, depression, HRQoL, and their associations among family caregivers of children with disabilities.
Material and Methods
Participants and Procedure
To compare the anxiety, depression, HRQoL and their associations with received family support of grandparents to parents of children with disabilities. The cross-sectional investigation was conducted from July to August 2020 in Shanghai, China. Inclusion criteria for family caregivers were (1) they were parents or grandparents of children; (2) they were caring for children diagnosed with one or more kinds of disability aged <18 years (eg, speech disability, intellectual disability); (3) they were primary caregivers who took care of children for more than 40 hours per week; (4) they had no communication barriers and consented to participate in this investigation.
In China, children with disabilities could be easily found in rehabilitation institutions since they need to receive various kinds of therapy. Hence, we recruited family caregivers in 8 rehabilitation institutions by a convenience sampling method. In each investigation area, a three-step procedure was used to collect information. First, we contacted the staff of the rehabilitation institution to inform them of our survey purpose and the inclusion criteria of family caregivers; second, the staff of the rehabilitation institution contacted the family caregivers of children with disabilities to inform them of the study purpose, to confirm their consent, and to form a survey arrangement (including the names of family caregivers and the survey time); third, according to the survey arrangement, we arranged uniformly trained investigators from our research team to visit the rehabilitation institutions. Before investigation, investigators explained the purpose and significance of the study to family caregivers again. If they agreed to participate in the study, investigators briefly introduced the questionnaire content to participants and how to fill it out. Questionnaires were collected by the investigators directly after completion. Finally, we recruited 327 family caregivers including 238 parents and 89 grandparents.
Measures
Family Support
We used a self-designed questionnaire to investigate the family support received by family caregivers (Table 1). Items in the questionnaire were derived from literature review and expert consultation.16,17 It contains 13 items measuring the received family support from five dimensions: childcare support (2 items), rehabilitation support (2 items), financial support (3 items), psychological support (3 items), and informational support (3 items). For each item, family caregivers were asked to answer whether they had received the corresponding support, and the response was “yes” or “no”. Additionally, in order to understand family needs, this questionnaire also includes the following question: “Which of the five types of support listed in the questionnaire do you need the most?” The questionnaire reliability coefficient of Cronbach’s α was 0.818.
 |
Table 1 Content of Family Support Questionnaire |
Anxiety
We assessed anxiety levels using the Generalized Anxiety Disorder 7-item (GAD-7) Scale developed by Spitzer in 2006.25 GAD-7 consists of 7 items asking participants the frequency they have been bothered by each symptom during the last 2 weeks. Corresponding response options scored from 0 (not at all) to 3 (nearly every day), and total scores range from 0 to 21. Total scores ≤4 indicate no anxiety, total scores 5–9 indicate mild anxiety, total scores 10–14 indicate moderate anxiety and total scores ≥ 15 indicate severe anxiety. In 2010, GAD-7 was translated into Chinese and validated in the Chinese population.26 In the sample of this study, the 7-item scale reliability coefficient of Cronbach’s α was 0.916.
Depression
We used the Patient Health Questionnaire-9 (PHQ-9) to measure depression levels among family caregivers of children with disabilities. PHQ-9 was developed by Kroenke in 2001 and consists of 9 items.27 Each item asks how often they have been bothered by the specific symptom over the last 2 weeks using a four-point Likert scale. Total PHQ-9 scores range from 0 to 27 with higher scores indicating higher levels of depression. Cut points 5, 10, 15, and 20 represent mild, moderate, moderately severe, and severe depression, respectively. The Chinese version of the PHQ-9 has been validated with good reliability, validity, and efficiency for screening depression.28 In this study, the 9-item scale reliability coefficient of Cronbach’s α was 0.867.
HRQoL
HRQoL was measured by the first version of the 12-item Short Form Health Survey (SF-12v1), which was designed to be a shorter, yet valid, alternative to the MOS 36-item Short Form Health Survey (SF-36).29 It assesses physical and mental HRQOL from 8 domains: Physical Functioning (PF), Role-Physical (RP), Bodily Pain (BP), General Health (GH), Energy/Fatigue (VT), Social Functioning (SF), Role-Emotional (RE), and Mental Health (MH). And the scores are expressed as physical component score (SF-12 PCS) and mental component score (SF-12 MCS) ranging from 0–100, respectively. In 2005, a study conducted in Hong Kong showed that SF-12 was applicable to the Chinese population.30
Statistical Analysis
Chi-square test, Mann–Whitney U-test, and two independent t-test were used to identify the differences in sociodemographic characteristics, received family support, anxiety, depression, and HRQoL between parents and grandparents. To preliminarily examine the associations between sociodemographic characteristics, received family support, and family caregivers’ anxiety, depression, and HRQoL, univariate analyses were conducted. To further investigate the potential predictors of parents’ and grandparents’ anxiety, depression, and HRQoL, eight generalized linear models were developed with anxiety/depression prevalence and PCS/MCS as dependent variables. Variables in the family support questionnaire associated with anxiety/depression prevalence and PCS/MCS in univariate analyses with p<0.1 were included in the eight generalized linear models as independent variables. And variables in sociodemographic characteristics associated with anxiety/depression prevalence and PCS/MCS in univariate analyses with p<0.1 were controlled as covariates in eight generalized linear models. Adjusted odds ratios (AORs) and 95% confidence intervals (CIs) were presented in model 1 to model 4. Unstandardized coefficients (Bs) and 95% confidence intervals (CIs) were presented in model 5 to model 8. A two-tailed p<0.05 was considered statistically significant. Statistical analyses were performed using SPSS 25.0.
Ethics Declarations
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of School of Public Health Fudan University (IRB No.: 2019-10-0782). Both verbal and written informed consent were obtained from all individual participants included in the study.
Results
Sociodemographic Characteristics
In total, 327 family caregivers (Median=39.32 years, IQR=19.68) responded to the survey. Among them, 72.8% were parents, and 27.2% were grandparents. For the whole sample, 27.5% of the children they cared for were diagnosed with multiple disabilities, 25.1% were diagnosed with hearing and speech disability, and 18.7% were diagnosed with physical disability. Table 2 shows the sociodemographic characteristics of the whole sample. Most of them were female (74.6%), and 81.0% were urban residents. Additionally, 61.8% of them had a junior college degree or higher, and about half of them were unemployed (52.9%) because of retirement and child caregiving. For their health status, 29.4% of them suffered from hypertension, diabetes, arthritis, or other diseases. Significant differences (p<0.05) were found in age, education, employment status, comorbidities and the disability type of children between parents and grandparents.
 |
Table 2 Sociodemographic Characteristics† |
Family Support
As is shown in Figure 1, rehabilitation (41.9%) and finance (32.1%) were the most two types of needs among the total family caregivers, subsequently were needs for childcare (12.2%), information (8.0%), and psychology (5.8%). Specifically, rehabilitation need (43.3%) was most frequently identified by parents, whereas grandparents expressed the highest financial need (42.7%).
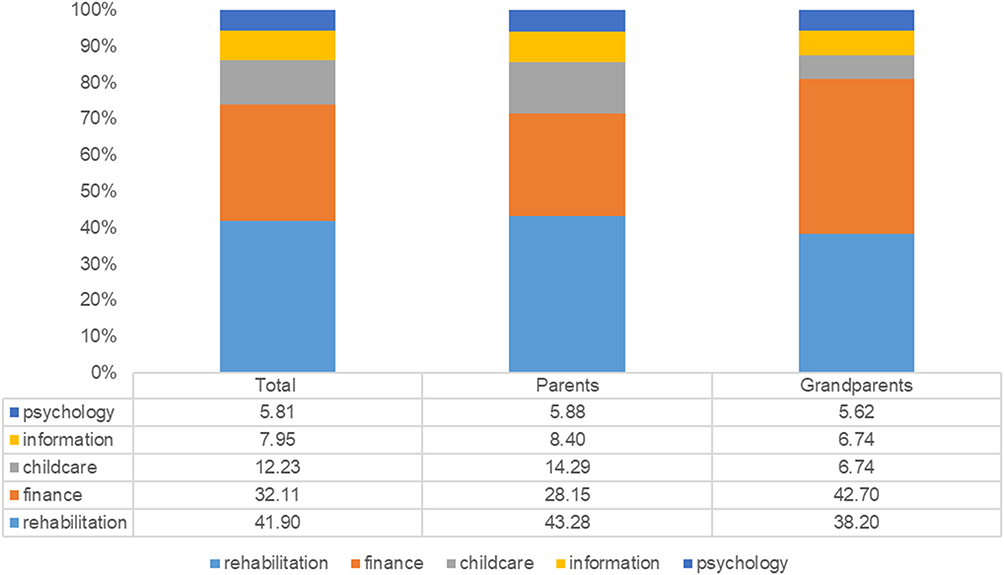 |
Figure 1 Answers to the question: what is currently most needed in your family?. |
Both parents and grandparents received rehabilitation support with the highest proportion (92.5% vs 90.5%), and received financial support with the lowest proportion (57.4% vs 66.3%). Significant differences (p<0.05) were found in FS3 (support for caregivers’ unemployment due to caregiving) and PS3 (psychological support from professional psychologists) between parents and grandparents (Table 3).
 |
Table 3 Intergenerational Differences in Family Support Received by Family Caregivers |
Anxiety, Depression, and HRQoL
Table 4 shows that the GAD-7 scores of 33.6% of family caregivers indicated possible anxiety, and the PHQ-9 scores of 36.1% of them indicated possible depression. Besides, 10.4% and 11.3% of family caregivers were screened positive for moderate to severe anxiety and depression, respectively. No significant differences were found in the risk of anxiety or depression between parents and grandparents. As for HRQoL, intergenerational differences were found in the PCS, but not found in the MCS.
 |
Table 4 Intergenerational Differences in Anxiety, Depression, and HRQoL† |
Association of Family Support with Anxiety, Depression, and HRQoL
Table 5 shows the association of family support with anxiety and depression. Model 1 shows that the support of RS2 (AOR=0.310, 95% CI=0.104, 0.919) and PS3 (AOR=0.325, 95% CI=0.152, 0.697) received by parents was significantly associated with their lower risk of anxiety. However, items of the family support questionnaire included in Model 2 were found no significant association with grandparents’ anxiety. Model 3 shows that the received support of CS1 (AOR=0.399, 95% CI= 0.187, 0.853), RS2 (AOR=0.289, 95% CI=0.093, 0.900), PS2 (AOR=0.182, 95% CI=0.038, 0.874), and PS3 (AOR=0.289, 95% CI=0.134, 0.625) were associated with lower level of depression among parents. Meanwhile, grandparents who received support of FS2 (AOR=0.141, 95% CI=0.021, 0.949) and PS1 (AOR=0.003, 95% CI=0.000,0.477) had lower risk of depression.
 |
Table 5 Intergenerational Differences in the Association of Family Support with Anxiety and Depression |
Table 6 shows the association of family support with HRQoL. Results in Model 5 and Model 6 show that there was no relationship between received family support and physical HRQoL among parents and grandparents. As for mental HRQoL, parents who received PS2 support have better mental HRQoL (B=8.986, 95% CI=2.872, 15.099). Among grandparents, the PS1 support was positively associated with their mental HRQoL (B=16.282, 95% CI=2.870, 29.695).
 |
Table 6 Intergenerational Differences in the Association of Family Support with Physical HRQoL and Mental HRQoL |
Discussion
To our knowledge, this is the first study that has explored the intergenerational differences in family support, anxiety, depression, and HRQoL, as well as their associations between parents and grandparents of children with disabilities. Overall, results indicated that: (1) parents and grandparents of children with disabilities were most in need of rehabilitation and financial support, but both populations received the least amount of financial support; (2) anxiety, depression, and mental HRQoL among parents and grandparents were not encouraging and found no significant intergenerational differences; and (3) high heterogeneities were found in the associations between family support and anxiety, depression, HRQoL among two generations.
Family caregivers of children with disabilities in this study reported the highest need for rehabilitation and financial support. This finding is consistent with some limited existing literature on the needs of family caregivers conducted in China as well as other countries. A sample of 1,390,448 Australian family caregivers reported that access to and the quality of therapy programs were a priority, and the need for financial assistance was endorsed by over 60% of respondents.31 The content analysis in one research conducted in Slovakia showed that in the current situation, finance/compensation is the most needed element for families of children with Down syndrome.3 A study conducted in Beijing and Shenyang in mainland China confirmed that financial support was necessary for families across disability categories.12 For rehabilitation support, family caregivers in our study received them frequently thanks to the rapid development of rehabilitation system for children with disabilities in China. However, family caregivers in our study received the least amount of financial support. Parenting a child with a disability has the potential to increase families’ financial pressure. On the one hand, the needs for long-term continuous rehabilitation, special examinations, and other healthcare services for children with disabilities increase family expenses.32 On the other hand, high dependency and long-term caregiving needs of children often require one parent to leave their job (approx. 40%), thereby reducing their source of family income and further increasing the financial burden.12,33 In 2018, the State Council issued the Opinions on Establishing a Rehabilitation Assistance System for Children with Disabilities, providing financial support for children’s operations, assistive devices configuration, and rehabilitation training.34,35 According to a recent statement from the China Disabled Persons’ Federation (CDPF), China offered rehabilitation assistance to 332,000 children with disabilities by the end of November 2021, nearly 50,000 more than the total of 2020.36 Unfortunately, a severe deviation between supply and demand remains,35 and the financial subsidies for each child are far from enough and need to be further adjusted.37
In the present study, 10.4% of family caregivers reported moderate to severe anxiety symptoms (scores ≥10 on GAD-7), and 11.3% reported moderate to severe depressive symptoms (scores ≥10 on PHQ-9). One study investigated the anxiety level of 5030 German population aged 14 years or older with GAD-7, and found approximately 5% of subjects had GAD-7 scores of 10 or greater.38 Another research measured the depression level of 5018 German population aged 14 years or older with PHQ-9, and found 5.6% of subjects had PHQ-9 scores of 10 or greater.39 These findings indicate that the anxiety and depression levels among family caregivers of children with disabilities are higher than the general population and should be paid urgent attention to, which is also confirmed by other previous research.40 In addition, family caregivers of children with disabilities in this study had lower MCS compared to mean scores in the general population in the United States29 and Hong Kong.30 Findings indicate that the mental HRQoL of family caregivers is poor, which is consistent with other existing literature.41 Among family caregivers in our study, approximately 30% were grandparents. Comparison results showed that no significant differences were found in the levels of anxiety, depression, and mental HRQoL between parents and grandparents, but the physical HRQoL of grandparents was found significantly poorer than parents. This finding is consistent with one comparison of HRQoL between mother and grandmother caregivers in Anhui province in China42 and highlights that the mental health of both populations should be concerned.
Providing target family support to meet the needs of family caregivers may alleviate their anxiety and depression as well as improve mental HRQoL. Among parents, the generalized linear models identified that childcare support of respite care and household tasks assistance, professional support of appropriate surgery for children, psychological support from relatives and friends, and psychological support from professional psychologists were associated with their anxiety, depression, or mental HRQoL. The results show that the four types of support are important for parents. Firstly, appropriate surgery plays a vital role in improving the health status of children with disabilities, which can reduce the concerns of parents from the source.43,44 In this study, 91.6% of parents have received the professional support of appropriate surgery for children, but their satisfaction with the treatment effect still needs to be further improved.35 Secondly, relatives and friends are salient sources of psychological support besides families, parents often experience renewed energy when relatives and friends attentively listen to their concerns, uncertainties, or frustrations.45 New friendships established with other parents of children with disabilities are also valuable as they can exchange parental experiences, as well as understand and help each other. Thirdly, only 74.4% of parents have ever received childcare support of respite care and household tasks assistance. Compared to grandparents, parents are much more educated and have a greater need for career, socialization, and leisure. However, as primary caregivers, parents sacrifice almost 24 hours a day carrying out responsibilities of children’s long-term rehabilitation, coordination of health service delivery, and assisting with daily activities (eg, eating, washing, and clothing).46 Such role restriction leads to less personnel time, freedom, possibilities to go out, and more restrictions on their chances to pursue a professional career.45 Therefore, support of respite care and household tasks assistance may partly release them from continuous caregiving and supervision and is more sensitive to parents in alleviating depressive symptoms. Finally, approximately 30% of parents have never received psychological support from professional psychologists, primary reason is that community education and service of mental health is not always available to these parents, thus interventions should be taken to improve the normalization of community services.
Among grandparents, the generalized linear models identified that financial support for daily living expenses was associated with depression, and psychological support from families was identified to have association with both depression and mental HRQoL. The phenomenon of grandparents as the primary caregivers of children with disabilities usually means that parents are unable to fulfill the parenting roles, and thus need practical or emotional support from grandparents.47 Influenced by the Confucian ethic of frugality, most grandparents view frugality and diligence as essential virtues for maintaining family functioning and could be easily influenced by the financial support for daily living expenses.48 In this study, such financial support is merely received by 51.7% of grandparents, which means that almost half of them still have a high level of unmet needs. Nowadays, financial support for daily living expenses available to families of children with disabilities in China comes from two main sources: rehabilitation assistance services and cash allowances (eg the nursing allowance for severely disabled people and the living allowance for impoverished disabled people).49 However, only three provinces, Liaoning, Shanxi, and Zhejiang, have rehabilitation assistance services covering subsistence allowances, and merely for economically disadvantaged families with children with disabilities aged 0–6. In addition, the nursing allowance and living allowance are designed for people with severe disabilities and in financial hardship, thus are inaccessible to most families with children with disabilities. The present study also examined the impact of psychological support from families on the depression and mental HRQoL of grandparents. In families with children with disabilities, grandparents assist their adult children with child caregiving and housekeeping regardless of their health. Therefore, support, recognition, and acknowledgment for dedication from other family members are important to grandparents and may motivate them to continue.45 Investigation showed that 93.3% of grandparents have received psychological support from families. Some family caregivers in one qualitative study also mentioned that their child created or enhanced a positive atmosphere in the family unit and enriched their family life, which is in line with the finding that the presence of a child with a disability can also intensify family cohesion.12
However, it is surprising to find that there was no association between family support and physical HRQoL of both parents and grandparents. Hence, associated factors should be explored from other perspectives, such as coping strategies,50 leisure and social participation,51 self-efficacy,52 etc.
Overall, the results show high heterogeneities in the associations between family support and anxiety, depression, and HRQoL among the two generations. In addition to research implications, this study implies multiple lessons on how practitioners and policymakers can help to better improve the psychological health of parents and grandparents. Firstly, to gradually improve the quality of professional rehabilitation services for children with disabilities, rehabilitation services providers should develop collaborative relationships with parents, and provide services based on children’s needs, families’ abilities, and strengths. Secondly, if parents express a need to invest more time in their interests and career, care providers could organize respite care to give parents more “breathing space”.45 Thirdly, if parents need more support from relatives or friends, care providers could help organize a series of activities to increase opportunities for interaction, and facilitate peer support. Besides, care providers should strengthen the advocacy of community education and services for mental health, to maximize its effect on families of children with disabilities or other diseases. Moreover, to increase grandparents’ feelings of competence, it seems important for care providers and other family members (especially parents) to “zoom out” their contributions, and acknowledge their efforts and perseverance. Finally, it is necessary for CDPF and relevant departments to provide higher-standard financial assistance to more children with disabilities, and to entrust third-party organizations to conduct satisfaction surveys among family caregivers to boost the quality of assistance services.
There are several limitations in our study. First, given the cross-sectional design, we would not infer causal relationships. A longitudinal design may provide more clear information on the associations of family support with family caregivers’ anxiety, depression, and HRQoL. Second, we only included a relatively small number of factors and found no statistically significant factors associated with physical HRQoL of both parents and grandparents, hence further studies should be conducted with more extensive factors. Third, children with different types of disabilities may have different impacts on the needs and well-being of their primary family caregiver. But the sample size of each type of children with disabilities in our study is small, which limits further analysis based on the type of disability. Therefore, further research should focus on specific types of disability in children to carry out in-depth exploration.
Conclusion
This study’s findings indicated the high prevalence of anxiety and depression, as well as poor mental HRQoL in both parents and grandparents of children with disabilities. To improve their psychological health, care providers and policy makers need to consider intergenerational differences that not all family caregivers have the same needs or receive the same family support when caring for children with disabilities. Specifically, interventions to improve parents’ psychological health should targeted at improving the quality of professional rehabilitation services, providing respite care and housework assistance to give parents more “breathing space”, facilitating peer support of relatives and friends, and making psychological support from professional psychologists more available. Whereas more psychological support from families and financial support for daily life expenses could alleviate the depression, and promote the mental HRQoL of grandparents. Findings in this study could also provide references for further research to identify causal relationships between the specific family support and psychological health and HRQoL among this population.
Acknowledgments
The authors would like to express our greatest appreciation to all the participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China [grant numbers 71774030 and 72274038]; National Key R&D Program of China [grant number 2021YFC2701004]; And the Major Project of National Social Science Foundation of China [grant number 17ZDA078].
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. World Report on Disability; 2011.
2. Smith M, Blamires J. Mothers’ experience of having a child with cerebral palsy. A systematic review. J Pediatr Nurs. 2022;64:64–73. doi:10.1016/j.pedn.2022.01.014
3. Slaná M, Molnárová Letovancová K, Dobríková P, Hromková M. Research into the needs of families who have children with Down syndrome (in the Slovak framework). Kontakt. 2020;22(1):60–67. doi:10.32725/kont.2020.005
4. Bian C, Peng F, Guo H, Chen K. Investigation on quality of life and economic burden of children with cerebral palsy in Changzhou. J Healthc Eng. 2022;2022:1–9. doi:10.1155/2022/1519689
5. Rayan A, Ahmad M. Psychological distress in Jordanian parents of children with autism spectrum disorder: the role of positive reappraisal coping. Arch Psychiat Nurs. 2017;31(1):38–42. doi:10.1016/j.apnu.2016.07.017
6. Liao XL, Lei XY, Li YM. Stigma among parents of children with autism: a literature review. Asian J Psychiatr. 2019;45:88–94. doi:10.1016/j.ajp.2019.09.007
7. Donald B, Bailey J, Simeonsson RJ. Assessing needs of families with handicapped infants. J Spec Educ. 1988;22(1):117–127. doi:10.1177/002246698802200113
8. Folkman S, Lazarus RS, Dunkel-Schetter C, DeLongis A, Gruenn RJ. Dynamics of a stressful encounter: cognitive appraisal, coping, and encounter outcomes. J Pers Soc Psychol. 1986;50(5):992–1003. doi:10.1037/0022-3514.50.5.992
9. Norizan A, Shamsuddin K. Predictors of parenting stress among Malaysian mothers of children with Down syndrome. JIDR. 2010;54(11):992–1003. doi:10.1111/j.1365-2788.2010.01324.x
10. Scherer N, Verhey I, Kuper H. Depression and anxiety in parents of children with intellectual and developmental disabilities: a systematic review and meta-analysis. PLoS One. 2019;(14):e219888. doi:10.1371/journal.pone.0219888
11. Guillamón N, Nieto R, Pousada M, et al. Quality of life and mental health among parents of children with cerebral palsy: the influence of self-efficacy and coping strategies. J Clin Nurs. 2013;22(11–12):1579–1590. doi:10.1111/jocn.12124
12. Wang P, Michaels CA. Chinese families of children with severe disabilities: family needs and available support. Res Pract Pers Sev D. 2009;34:21–32. doi:10.2511/rpsd.34.2.21
13. Gemikoz M, Ozgen M, Mutlu F. Anxiety, depression and quality of life levels of mothers with children with cerebral palsy. Curr Pediatr Rep. 2020;18:114–124.
14. Zeng S, Zhao H, Hu X, Lee JD, Stone-MacDonald AK, Price ZW. Are we on the same page: a dyadic analysis of parental stress, support, and family quality of life on raising children with autism spectrum disorders. J Dev Phys Disabil. 2021;33(4):599–618. doi:10.1007/s10882-020-09761-x
15. Dunst CJ, Jenkins V, Trivette CM. Family support scale: reliability and validity. J Individual Fam Comm Wellness. 1984;1:45–52.
16. Carlson JM, Miller PA. Family burden, child disability, and the adjustment of mothers caring for children with epilepsy: role of social support and coping. Epilepsy Behav. 2017;68:168–173. doi:10.1016/j.yebeh.2017.01.013
17. Kyzar KB, Turnbull AP, Summers JA, Gómez VA. The relationship of family support to family outcomes: a synthesis of key findings from research on severe disability. Res Pract Pers Sev D. 2012;37:31–44. doi:10.2511/027494812800903247
18. Zeng S, Hu X, Zhao H, Stone-MacDonald AK. Examining the relationships of parental stress, family support and family quality of life: a structural equation modeling approach. Res Dev Disabil. 2020;96:103523. doi:10.1016/j.ridd.2019.103523
19. Hank K, Buber I. Grandparents caring for their grandchildren findings from the 2004 Survey of Health, Ageing, and Retirement in Europe. J Fam Issues. 2009;30(1):53–73. doi:10.1177/0192513X08322627
20. Li XW, Liu QQ. Parent-grandparent coparenting relationship, marital conflict and parent-child relationship in Chinese parent-grandparent coparenting families. Child Youth Serv Rev. 2020;109. doi:10.1016/j.childyouth.2019.104733
21. Zakirova Engstrand R, Roll-Pettersson L, Westling Allodi M, Hirvikoski T. Needs of grandparents of preschool-aged children with ASD in Sweden. J Autism Dev Disord. 2020;50(6):1941–1957. doi:10.1007/s10803-019-03946-w
22. Margetts JK, Le Couteur A, Croom S. Families in a state of flux: the experience of grandparents in autism spectrum disorder. Child Care Health Dev. 2006;32(5):565–574. doi:10.1111/j.1365-2214.2006.00671.x
23. Glasberg BA, Harris SL. Grandparents and parents assess the development of their child with autism. Child Fam Behav Ther. 1997;19(2):17–27. doi:10.1300/J019v19n02_02
24. D’Astous V, Wright SD, Wright CA, Diener ML. Grandparents of grandchildren with autism spectrum disorders: influences on engagement. J Intergener Relatsh. 2013;11:134–147. doi:10.1080/15350770.2013.782744
25. Spitzer RL, Kroenke K, Williams JBW, Loewe B. A brief measure for assessing generalized anxiety disorder - The GAD-7. Arch Intern Med. 2006;166(10):1092–1097. doi:10.1001/archinte.166.10.1092
26. He XY, Li CB, Qian J, Cui HS, Wu WY. Reliability and validity of a generalized anxiety disorder scale in general hospital outpatients. Shanghai Arch Psychiatry. 2010;22:200–203.
27. Kroenke K, Spitzer RL, Williams JBW, Loewe B. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
28. Wang WZ, Bian Q, Zhao Y, et al. Reliability and validity of the Chinese version of the Patient Health Questionnaire (PHQ-9) in the general population. Gen Hosp Psychiat. 2014;36(5):539–544. doi:10.1016/j.genhosppsych.2014.05.021
29. Ware JE, Kosinski M, Keller SD. A 12-item short-form health survey - Construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. doi:10.1097/00005650-199603000-00003
30. Lam C, Tse E, Gandek B. Is the standard SF-12 Health Survey valid and equivalent for a Chinese population? Qual Life Res. 2005;14(2):539–547. doi:10.1007/s11136-004-0704-3
31. Burton-Smith R, McVilly KR, Yazbeck M, Parmenter TR, Tsutsui T. Service and support needs of Australian carers supporting a family member with disability at home. J Intellect Dev Dis. 2009;34(3):239–247. doi:10.1080/13668250903103668
32. Colvin MK, Poysky J, Kinnett K, et al. Psychosocial management of the patient with Duchenne Muscular Dystrophy. Pediatrics. 2018;142(Supplement_2):S99–S109. doi:10.1542/peds.2018-0333L
33. Chiu C, Turnbull AP, Summers JA. What families need: validation of the family needs assessment for Taiwanese families of children with intellectual disability and developmental delay. Res Pract Pers Sev D. 2013;38:247–258. doi:10.1177/154079691303800404
34. The State Council, the People’s Republic of China. Opinions on Establishing a Rehabilitation Assistance System for Children with Disabilities. Vol. 2022; 2018.
35. Qi CY, Wang Y. Why is rehabilitation assistance policy for children with disabilities deviated in supply-demand? A case study in mainland China. Front Public Health. 2021;9. doi:10.3389/fpubh.2021.666333.
36. CDPF. China’s Rehabilitation Assistance Services Cover More Children with Disabilities. Vol. 2022; 2021.
37. Xia C, Sun M, Li X, et al. Health-related quality of life and related factors among primary caregivers of children with disabilities in Shanghai, China: a cross-sectional study. IJERPH. 2020;17(24):9299. doi:10.3390/ijerph17249299
38. Lowe B, Decker O, Muller S, et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med Care. 2008;46(3):266–274. doi:10.1097/MLR.0b013e318160d093
39. Kocalevent R, Hinz A, Brähler E. Standardization of the depression screener Patient Health Questionnaire (PHQ-9) in the general population. Gen Hosp Psychiat. 2013;35(5):551–555. doi:10.1016/j.genhosppsych.2013.04.006
40. Fatima N, Chinnakali P, Rajaa S, Menon V, Mondal N, Chandrasekaran V. Prevalence of depression and anxiety among mothers of children with neuro-developmental disorders at a tertiary care centre, Puducherry. Clin Epidemiol Glob Health. 2021;11:100792. doi:10.1016/j.cegh.2021.100792
41. Kuhlthau K, Kahn R, Hill KS, Gnanasekaran S, Ettner SL. The Well-being of parental caregivers of children with activity limitations. Matern Child Hlth J. 2010;14(2):155–163. doi:10.1007/s10995-008-0434-1
42. Wu J, Zhang J, Hong Y. Quality of life of primary caregivers of children with cerebral palsy: a comparison between mother and grandmother caregivers in Anhui province of China. Child Care Health Dev. 2017;43(5):718–724. doi:10.1111/cch.12464
43. Hyer LC, Carpenter AM, Saraswat P, Davids JR, Westberry DE. Outcomes of patellar tendon imbrication with distal femoral extension osteotomy for treatment of crouch gait. J Pediatr Orthop. 2021;41(5):E356–E366. doi:10.1097/BPO.0000000000001793
44. DiFazio RL, Vessey JA, Miller PE, Snyder BD, Shore BJ. Health-related quality of life and caregiver burden after Hip reconstruction and spinal fusion in children with spastic cerebral palsy. Dev Med Child Neurol. 2022;64(1):80–87. doi:10.1111/dmcn.14994
45. De Clercq LE, Prinzie P, Swerts C, Ortibus E, De Pauw S. “Tell me about your child, the relationship with your child and your parental experiences”: a qualitative study of spontaneous speech samples among parents raising a child with and without autism spectrum disorder, cerebral palsy or Down syndrome. J Dev Phys Disabil. 2022;34(2):295–329. doi:10.1007/s10882-021-09800-1
46. Toledano-Toledano F, Moral De La Rubia J. Factors associated with anxiety in family caregivers of children with chronic diseases. Biopsychosoc Med. 2018;12. doi: 10.1186/s13030-018-0139-7
47. Cate IMP, Hastings RP, Johnson H, Titus S. Grandparent support for mothers of children with and without physical disabilities. Fam Soc. 2007;88(1):141–146. doi:10.1606/1044-3894.3601
48. Chen J, Bao J. Rethinking time and lifestyle migration: multiple temporalities, identity formation, and post-migration life of Chinese Houniao. Geogr J. 2020;186(2):213–223. doi:10.1111/geoj.12339
49. Wang Y, Qi CY, Zhu Y. Poverty alleviation for people with disabilities in China: policy, practice, exclusionary effects, and ways forward. Disabil Soc. 2022;37(6):1060–1065. doi:10.1080/09687599.2022.2065464
50. Tseng M, Chen K, Shieh J, Lu L, Huang C, Simeonsson RJ. Child characteristics, caregiver characteristics, and environmental factors affecting the quality of life of caregivers of children with cerebral palsy. Disabil Rehabil. 2016;38(24):2374–2382. doi:10.3109/09638288.2015.1129451
51. Rizk S, Pizur-Bamekow K, Darragh AR. Leisure and social participation and health-related quality of life in caregivers of children with autism. Otjr-Occup Part Heal. 2011;31:164–171. doi:10.3928/15394492-20110415-01
52. Isa SNI, Ishak I, Ab Rahman A, et al. Health and quality of life among the caregivers of children with disabilities: a review of literature. Asian J Psychiatr. 2016;23:71–77. doi:10.1016/j.ajp.2016.07.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.