")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Anxiety and Insomnia Mediate the Association of Fear of Infection and Fatigue: A Cross-Sectional Survey of Nurses Deployed to a COVID-19 Epicenter in China
Authors Liu Z, Zhang H, Wang N, Feng Y, Liu J, Wu L, Liu Z, Liu X, Liang L , Liu J, Wu Q , Liu C
Received 1 June 2023
Accepted for publication 11 August 2023
Published 24 August 2023 Volume 2023:16 Pages 2439—2448
DOI https://doi.org/10.2147/JMDH.S421619
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zhixin Liu,1,2,* Huanyu Zhang,1 Nan Wang,1,* Yajie Feng,1,* Junping Liu,1 Lin Wu,1 Zhaoyue Liu,1 Xinru Liu,1 Libo Liang,1 Jie Liu,3 Qunhong Wu,1 Chaojie Liu4
1Department of Social Medicine, School of Health Management, Harbin Medical University, Harbin, People’s Republic of China; 2Department of Health Policy and Management, School of Public Health, Peking University, Beijing, People’s Republic of China; 3Intensive Care Unit, The 2nd Affiliated Hospital of Harbin Medical University, Harbin, People’s Republic of China; 4Department of Public Health, School of Psychology and Public Health, La Trobe University, Melbourne, VIC, Australia
*These authors contributed equally to this work
Correspondence: Libo Liang; Jie Liu, Email [email protected]; [email protected]
Background: This study aimed to test the mediating role of anxiety and insomnia in the association between fear of infection and fatigue.
Methods: A cross-sectional questionnaire survey was conducted on the nurses deployed to Heihe. A serial multiple mediation model was established to determine the role of anxiety and insomnia in the association between fear of infection and fatigue.
Findings: Over half (53.0%) of the study participants reported experiencing fear of infection despite stringent personal protection measures. The scores of anxiety (11.87± 5.19), insomnia (16.33± 5.95), and fatigue (45.94± 12.93) were moderately correlated, with a Pearson correlation coefficient ranging from 0.501 to 0.579. Anxiety, either alone or in combination with insomnia, mediated the association between fear of infection and fatigue.
Conclusion: The findings suggest that anxiety and insomnia play a mediating role in the relationship between fear of infection and fatigue. These results emphasize the importance of implementing targeted mental health interventions and work arrangements to address the well-being of healthcare professionals.
Keywords: fear of infection, anxiety, insomnia, fatigue, COVID-19
Background
The COVID-19 pandemic caused by the novel coronavirus 2019 is an extraordinary global health crisis and a significant public health event.1 Healthcare workers, who have been at the forefront of the pandemic response, have faced immense physical and psychological stress, leading to serious mental health concerns.2 Previous research has indicated that healthcare professionals, especially those working in Emergency and Intensive Care Unit (ICU) settings, have faced various forms of distress during the COVID-19 pandemic, including depression, anxiety, post-traumatic stress disorder (PTSD), and headaches.3,4 Specifically, clinical nurses have shown a higher prevalence of emotional challenges, with around 50% of ICU nurses reporting anxiety and over 30% experiencing depression and PTSD as they confront the virus.5 Clinical nurses often bear witness to the deaths of COVID-19 patients, which intensifies their fear of infection. The heightened risk of occupational exposure to the virus further compounds the challenges faced by nurses, as their social lives are already disrupted by the outbreak of COVID-19. This situation exacerbates work-related fatigue,2 leading to decreased work capacity and performance.6 Studies have estimated that during the COVID-19 pandemic, approximately 35% to 72% of clinical nurses in China experienced moderate to high levels of work-related fatigue.7 Fatigue is recognized as a medical condition characterized by a reduced ability to perform tasks due to inadequate energy recovery.8 It poses a significant risk to occupational health and patient safety,9 manifesting in excessive daytime sleepiness, decreased productivity, and an increased likelihood of work errors and adverse events in patient care.10
Fear is a natural stress response11 and is often considered a motivator for individuals to take cautious actions, such as avoiding risky behaviors.12 However, fear can also have negative consequences.13 In the context of the COVID-19 outbreaks, fear of infection has been found to be associated with higher levels of fatigue among nurses.14,15 Even when proper personal protective equipment (PPE) and procedures are followed, the high transmissibility of the virus and direct contact with infected patients and colleagues can still lead to a strong sense of uncertainty, triggering fear of infection.16,17 Previous research has highlighted the role of psychological and cognitive factors in triggering fear of infection.18
Given the aforementioned challenges, addressing and mitigating the potential consequences of fear of infection becomes crucial. Empirical evidence indicates that fear of infection is associated with various mental factors that contribute to fatigue, including anxiety19,20 and sleep disturbance.21 Piper et al proposed that fatigue can be understood through the mechanisms of activity rhythm, sleep, and psychological states.22 Notably, insomnia is considered one of the strongest predictors of fatigue,23 with its effects extending beyond nighttime sleep and interfering with daytime activities. Anxiety, on the other hand, is also a significant predictor of fatigue24 and is closely linked to insomnia.25 According to Papadimitriou, around 60–70% of patients with generalized anxiety disorder experience sleep disturbances.26 Indeed, it has been suggested that insomnia can be considered a by-product or a consequence of anxiety.27,28
Despite extensive research on the associations among fear of infection, anxiety, insomnia, and fatigue, there is a lack of literature documenting the serial mediating effects of insomnia and anxiety on the relationship between fear of infection and fatigue. This study aims to address this gap by examining the levels of fear of infection and fatigue among nurses mobilized in emergency responses to the COVID-19 outbreak. Additionally, the study seeks to investigate the mediating role of anxiety and insomnia in the association between fear of infection and fatigue.
Methods
Study Setting and Participants
This study adopted a cross-sectional survey design and focused on nurses deployed to Heihe city, which was the epicenter of the COVID-19 outbreaks at the time in Heilongjiang province, China. These nurses were mobilized from hospitals located in Harbin, Qiqihar, and Daqing municipalities. Their primary duties involved the management of COVID-19 patients and the implementation of infection control measures. Each deployed nurse worked on the frontline for approximately 30 days. It is important to note that all participants had received full vaccination with COVID vaccines, and none of them had contracted COVID-19 prior to the survey period.
During the period from October 27 to December 9, 2021, Heihe city reported a total of 271 positive cases of COVID-19. The deployed nurses concluded their service on November 30, 2021, as the number of COVID-19 patients began to decline and the local healthcare capacity was considered adequate to manage the situation.
Data Collection
Two WeChat (a social media platform) groups were created for the deployed nurses under the guidance of the provincial manager responsible for the deployment. Permission was obtained from the manager to distribute a survey invitation through these WeChat groups. Participants were provided with a direct link and QR code to access the questionnaire, which was hosted on the “Wenjuanxing” survey platform powered by Changsha Ranxing IT Ltd. The survey was accessible from November 17 to November 28, 2021.
The survey was conducted on a voluntary and anonymous basis. Prior to completing the survey, respondents were asked to provide implied informed consent, indicating their willingness to participate. The two WeChat groups consisted of a total of 500 members. Out of these, 270 members (54% of the total group members) completed and returned a valid questionnaire.
Ethical Considerations
The study protocol complies with the Declaration of Helsinki and obtained approval from the Ethics Committee of Harbin Medical University (protocol number: HMUIRB2023017).
Measurements
Dependent Variable
Fatigue was measured as the outcome indicator using the 20-item Multidimensional Fatigue Scale (MFI-20), which was developed by Smets et al.29 The MFI-20 had been validated in various populations, including nurses.30,31 A validated Chinese version has been available since 2008.32 The MFI-20 measures five domains of fatigue: general fatigue; physical fatigue; decreased motivation; mental fatigue; and decreased activity. Each domain contains four items. Respondents were asked to rate each item on a five-point Likert scale, ranging from 1 “not at all” to 5 “completely”. The item scores were aligned in a consistent direction before calculating a summed score, where a higher score indicates a higher level of fatigue. A score of 40 or above is considered indicative of moderate to severe fatigue.33 The MFI-20 demonstrated high internal consistency as indicated by the overall Cronbach’s alpha (0.895) in this study, although the dimensional alpha ranged from 0.479 to 0.776.
Independent Variable
The association between fear of infection and fatigue was the major interest of this study. A single item was designed to measure fear of infection: “were you still worried about being infected even with head-to-toe personal protective equipment (PPE)?” Respondents were asked to rate their level of fear on a four-point scale, ranging from “not at all” to “very worried”. The responses were collapsed into two categories for data analyses: 0=not worried; 1=worried.
Mediators
The mediating effects of insomnia and anxiety on the association between fear of infection and fatigue were tested.
Insomnia was measured by the insomnia severity index (ISI) scale developed by Bastien.34 Its Chinese version (ISI-C) had been validated.35 The ISI-C contains seven items, measuring difficulty in falling asleep, difficulty in maintaining sleep, early awakening to fall asleep, dissatisfaction with sleep, impact of sleep on daytime functioning, the degree to which quality of life is affected by sleep problems, and the degree to which one worries about sleep problems, respectively. Respondents were asked to rate each item on a five-point Likert scale, ranging from 1 (not at all) to 5 (very serious). A summed score was calculated, with a higher score indicating a higher level of severity of insomnia: 7–14 normal, 15–21 subthreshold, 22–28 moderate, 29–35 severe.36 High internal consistency of the ISI-C was demonstrated in this study (Cronbach’s α = 0.907).
Anxiety was measured by the generalized anxiety disorder scale (GAD-7) developed by Robert.37 It had been widely used for assessing job-related anxiety in nurses.15 The validated Chinese version of GAD-7 contains seven items.38 Example items include “Over the last two weeks, how often have you been bothered by feeling nervous, anxious or on edge?” Respondents were asked to rate each item on a four-point scale, ranging from 1 “not at all” to 4 “nearly every day”. A summed score was calculated, with a higher score indicating a higher level of anxiety symptoms: 7–11 normal, 12–16 mild, 17–21 moderate, 22–28 severe.39 The GAD-7 demonstrated high internal consistency in this study (Cronbach’s α = 0.956).
Covariates
Sociodemographic characteristics (age and gender), work-related factors (professional title and daily working hours), and side effects associated with wearing PPE were considered as covariates that might confound the effect of fear of infection on fatigue.40,41 Seven aspects of PPE-related side effects were measured: hot, sweating, dehydration, headache, pain (face and/or behind ears), nausea/vomiting, and dizziness.42,43
Statistical Analysis
Data were analyzed using IBM SPSS 26.0 with PROCESS macro version 3.5. The frequency distribution of different characteristics of study participants was described. The level of fatigue was presented using mean value and standard deviation (SD) and compared between those with different characteristics through student t-tests. Pearson correlation analyses were performed to examine the correlations between the key constructs measured. OLS linear regression models were established to test the effect of fear of infection on fatigue with anxiety and insomnia as mediators after adjustment for variations in the covariates. The indirect effect of fear of infection on fatigue was assessed by bootstrapping (10,000 samples) with a 95% confidence interval.44
Results
Characteristics of Study Participants
The study participants had a mean age of 32.60 (SD=5.86) years. The vast majority were women (91.5%), had a junior-level professional title (63.3%), worked less than five hours per day (75.9%), and reported fewer than two PPE-related side effects (71.5%). More than half (53.0%) reported fear of infection (Table 1).
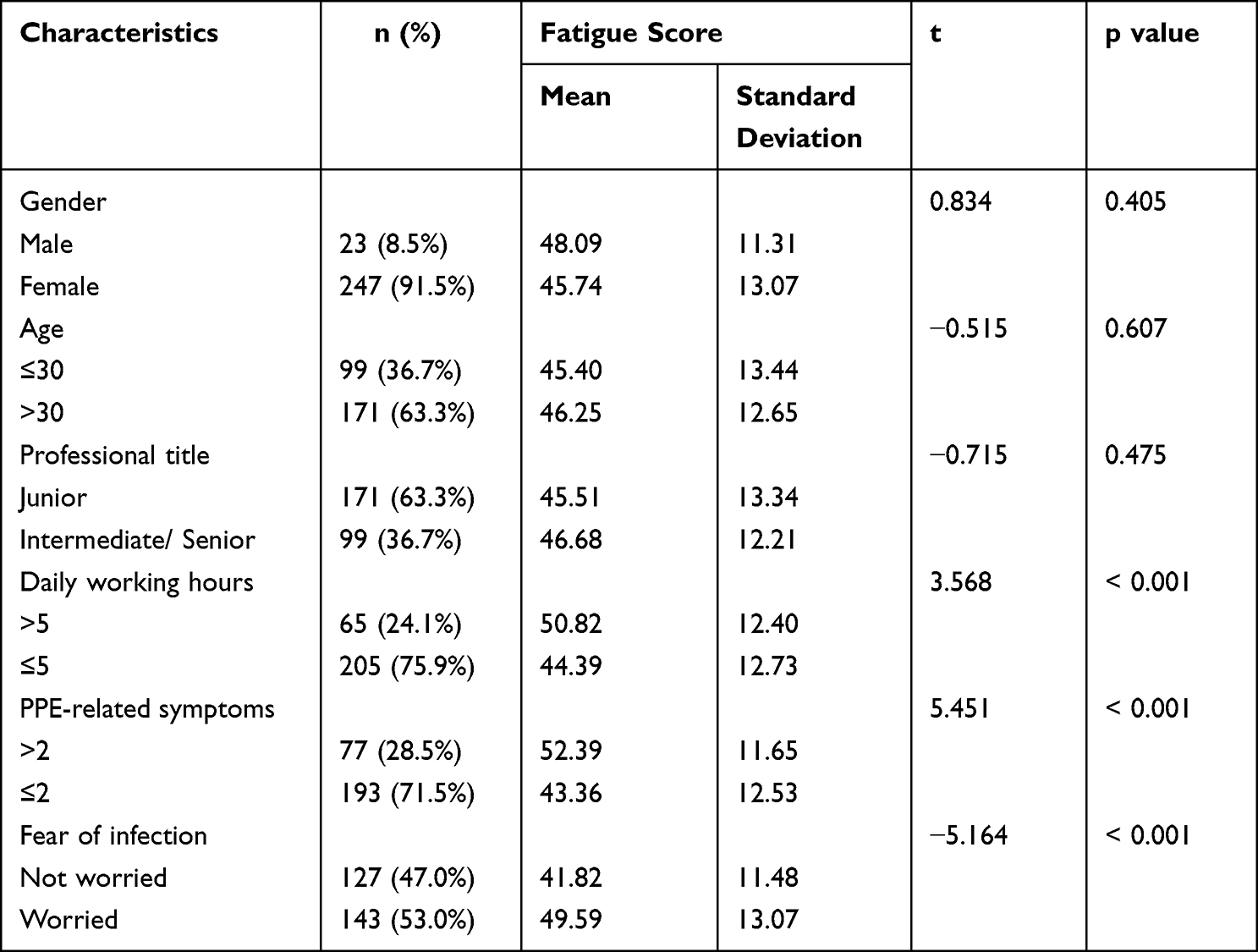 |
Table 1 Fatigue Levels of Study Participants with Different Characteristics (n=270) |
Fatigue, Anxiety, and Insomnia
The study participants reported a mean score of 45.94 (SD=12.93) in fatigue and 60% had moderate/severe levels of fatigue. Higher levels of fatigue were associated with longer daily working hours (p<0.001), more PPE-related symptoms (p<0.001), and fear of infection (p<0.001) (Table 1).
The respondents reported a mean score of 11.87 (SD=5.19) for anxiety and 16.33 (SD=5.95) for insomnia. The prevalence of moderate to severe anxiety was found to be 18.5%, while the prevalence of moderate to severe insomnia was 17.4%. Both anxiety and insomnia showed moderate correlations with each other and with fatigue (Table 2).
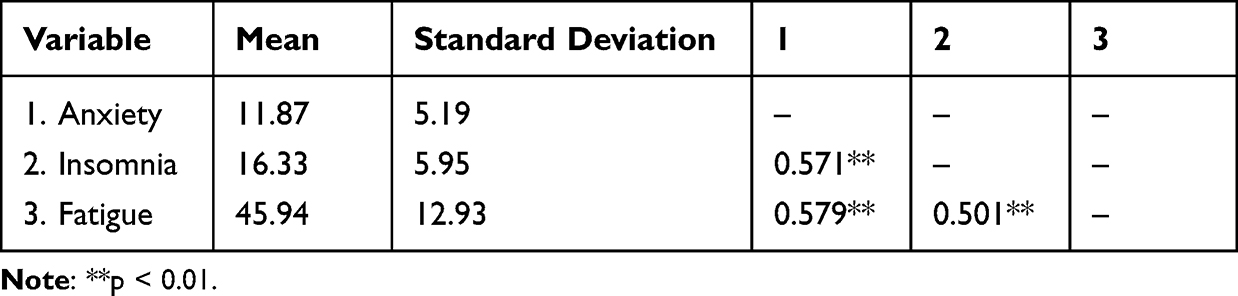 |
Table 2 Pearson Correlations Among Anxiety, Insomnia, and Fatigue (n=270) |
Mediating Effects of Anxiety and Insomnia on the Association Between Fear of Infection and Fatigue
The OLS regression models (Table 3) showed that fear of infection was a significant predictor of fatigue (β=0.280, 95% CI 0.083 to 0.478) and anxiety (β=0.421, 95% CI 0.204 to 0.639), but not for insomnia (β=−0.032, 95% CI −0.234 to 0.169). However, anxiety was significantly associated with insomnia (β=0.534, 95% CI 0.425 to 0.643). Both anxiety (β=0.378, 95% CI 0.253 to 0.502) and insomnia (β=0.225, 95% CI 0.106 to 0.344) had a direct effect on fatigue (Table 3).
 |
Table 3 Standardized OLS Regression Coefficients (95% Confidence Intervals) of Predictors on Anxiety, Insomnia and Fatigue (n=270) |
The effect of fear of infection on fatigue was mediated by anxiety (a1b1=0.159, 95% CI 0.067 to 0.280), but not by insomnia (a2b2=−0.007, 95% CI −0.055 to 0.036). The modelling also showed a significant indirect effect of fear of infection on fatigue through both anxiety and insomnia in serial (a1db2=0.051, 95% CI 0.019 to 0.094). The effect of the path through single mediation by anxiety was much stronger than that of the path through the anxiety-insomnia serial mediation (Table 4) (Figure 1).
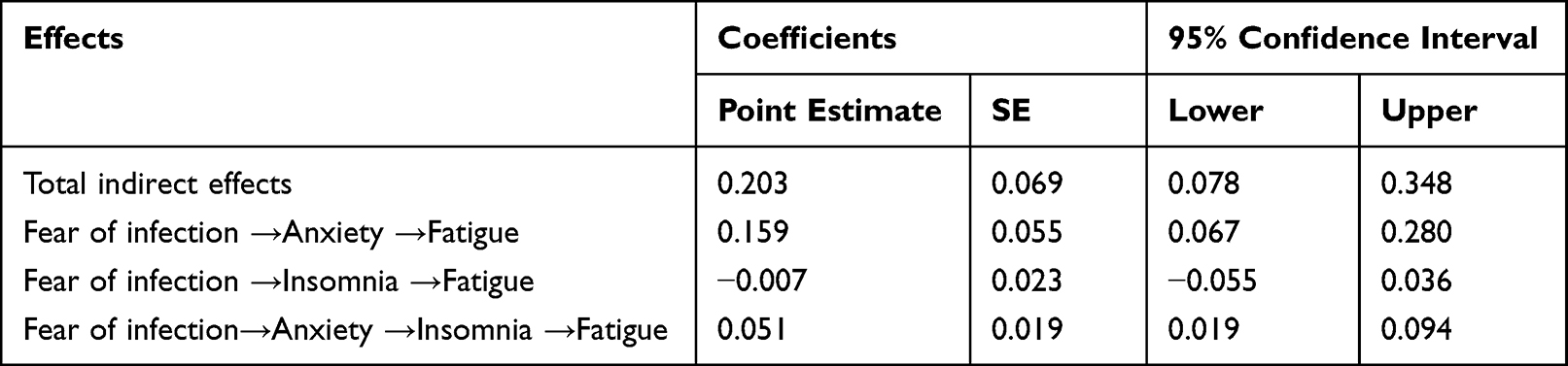 |
Table 4 Indirect Effects of Fear of Infection on Fatigue Through Anxiety and Insomnia (n=270) |
 |
Figure 1 Mediating effects of anxiety and insomnia in the association between fear of infection and fatigue after adjustment for variations of gender, age, professional title, daily working hours, and PPE-related effects. Notes: The coefficient a1 is the direct effect of fear of infection on anxiety; the coefficient a2 is the direct effect of fear of infection on insomnia; the coefficient b1 is the direct effect of anxiety on fatigue; the coefficient b2 is the direct effect of insomnia on fatigue; the coefficient d is the direct effect of anxiety on insomnia; the coefficient c is the total effect between fear of infection and fatigue, and c′ is the direct effect of fear of infection on fatigue while controlling for anxiety and insomnia in the model. Path coefficients are standardized, **p < 0.01, ***p < 0.001. |
Discussion
The current study revealed that approximately 60% of the nurses deployed for emergency responses to the COVID-19 outbreak in Heihe experienced moderate to severe levels of fatigue. This prevalence is slightly lower than what was reported by Wang et al45 for nurses deployed to Wuhan during the initial wave of the COVID-19 outbreak in China. Fatigue not only reflects the physical and mental burdens faced by healthcare workers but also poses risks to patient safety and the quality of care provided.
It is evident that the fatigue experienced by emergency responders cannot be solely attributed to heavy workloads. In our study, the vast majority (76%) of the deployed nurses worked no more than five hours per day. Fatigue is a complex and multidimensional state that encompasses emotional, physical, psychological, and cognitive exhaustion, arising from excessive work demands and insufficient energy recovery.46 Our study contributes to the existing literature by exploring the impact of fear of infection on fatigue and investigating the mediating role of anxiety and insomnia in this association.
In our study, we found that 53.0% of the deployed nurse responders reported fear of infection, while 18.5% and 17.4% experienced moderate/severe levels of anxiety and insomnia, respectively. These percentages indicate a significant decrease compared to previous studies conducted on nurse responders deployed to Wuhan during the first wave of the COVID-19 outbreak in China. In those studies, the reported percentages were higher, with 70.6% reporting fear of infection,16 44.6% experiencing moderate to severe anxiety, and 34.0% experiencing moderate to severe insomnia.39 The observed reductions in fear of infection, anxiety, and insomnia levels among the deployed nurse responders in our study are likely attributed to improved knowledge of COVID-19 and enhanced preparedness measures. Shortened working hours, for instance, were intentionally implemented to address the psychological and physical distress experienced by the nurse responders. It is crucial to acknowledge that fear of infection can also arise from concerns about transmitting the virus to loved ones.47 Nurse responders deployed to distant locations away from their families may have had fewer worries about inadvertently bringing the virus home until they were preparing to return to their households.48
According to the OLS linear regression modelling in our study, fear of infection has both direct and indirect effects on fatigue. This result is consistent with the findings of several recent studies.49 Fear can serve as a root cause for many psychological disorders. The concerns surrounding the rapidly changing work environment and uncertain outcomes during a major epidemic can create a discordant relationship between nurses and their work.50 The fear and uncertainty experienced can place significant strain on the limited resources available to nurses, resulting in “allostatic overload” when the demands on internal resources exceed their capacity.51 Fatigue emerges when nurses are no longer able to effectively manage such stress. Empirical evidence indicates that fear and stress have indeed contributed to increased fatigue among healthcare workers during the COVID-19 pandemic,50,52 and persistent fatigue can ultimately lead to burnout.53
We found that anxiety, either alone or in combination with insomnia in a series, mediates the effect of fear of infection on fatigue. This suggests that anxiety can have an impact on fatigue even in the absence of insomnia. This finding is consistent with previous studies that have highlighted the significant predictive role of anxiety in relation to fatigue among nurses.40,54 Anxiety is known to be associated with decreased personal interest, attention, work engagement, and commitment, which can contribute to feelings of fatigue.55 During the COVID-19 pandemic, fear of infection and the concern of unknowingly infecting others became significant sources of anxiety among nurses.56 It is important to note that fear of infection is an emotional reaction triggered by exposure to occupational risks, while anxiety represents the cognitive processing of that fear of infection.57 Anxiety stemming from fear can lead to elevated levels of psychological stress.
In our current study, we found that although insomnia was equally prevalent as anxiety among nurse emergency responders, it played a relatively less significant role in fatigue compared to anxiety. The results showed that anxiety alone had a stronger indirect effect (0.159) in mediating the association between fear of infection and fatigue compared to the combined effect of anxiety and insomnia (indirect effect 0.051). Previous studies have also demonstrated that psychological distress can fully mediate the relationship between fear of COVID-19 and insomnia.58 However, this does not diminish the importance of insomnia in its association with fatigue.55 Personal discomfort, restlessness, and irritability experienced due to fatigue can reasonably be attributed to poor sleep quality.59 Insomnia is a subjective complaint characterized by difficulty falling asleep, staying asleep, or experiencing non-resumption of sleep, which can significantly interfere with daily social functioning.60 In addition to genetic factors61 and personality traits,62 insomnia is closely linked to psychological disturbances. Anxiety, in particular, can induce insomnia-related symptoms through fear induction and pressure reactions.63
Our study has several limitations. Firstly, the study was conducted in a single epicenter in Heilongjiang province, China, which may limit the generalizability of the findings to other regions or populations. It is important to consider that there may be significant variations in the prevalence of COVID-19 and the response measures across different geographic locations and timeframes. Secondly, the cross-sectional study design used in this research precludes the establishment of causal relationships. Thirdly, the study focused on examining the impact of fear of infection, anxiety, and insomnia on nurses’ fatigue within a limited timeframe. Future research should incorporate longitudinal designs and follow-up studies to gain a better understanding of the recovery process of mental distress and potential long-term effects of emergency deployments, such as burnout, on the responders. In future research endeavors, it is recommended to conduct comprehensive and long-term monitoring of healthcare professionals, placing specific emphasis on investigating burnout resulting from prolonged negative emotions and fatigue experienced by healthcare workers during public health crises. This will provide a more comprehensive understanding of the long-term impacts and facilitate the development of targeted interventions to support the well-being of healthcare professionals.
Implications for Occupational Health Nursing Practice
The findings of our study have important policy and management implications, particularly in the context of emergency responses to the COVID-19 pandemic. Fear of infection, anxiety, insomnia, and fatigue are significant concerns for the occupational health and safety of healthcare workers, and they should be addressed comprehensively through a combination of job protection measures and mental health interventions.
Managers play a crucial role in demonstrating their commitment to protecting the wellbeing of healthcare workers, particularly during emergency responses. To alleviate nurses’ fear of infection, it is crucial for the government and hospitals to provide adequate prevention materials and emergency training. Ensuring that nurses have access to secure and well-equipped drop-in lounges, as well as facilitating effective information sharing about illness and self-protection, can help reduce anxiety levels.64
It is essential to recognize that each individual may have different levels of fear and anxiety, and therefore a personalized approach is preferred to address their specific needs. For individuals who exhibit high levels of anxiety or experience insomnia, more complex interventions may be necessary. These interventions could involve options such as early exit from the emergency response, medication treatments, counselling services, or even post-deployment cognitive behavioral therapy (CBT). CBT has demonstrated strong effectiveness in treating anxiety-related disorders65 as well as insomnia.66 Internet-based cognitive behavioral therapy (I-CBT) is a particularly valuable approach because it overcomes geographical limitations and time constraints67. Additionally, I-CBT eliminates the risk of disease transmission associated with face-to-face contact or treatment.68
It is crucial to incorporate mental health and wellbeing programs into occupational health and safety management practices.69 However, it is unfortunate that very few, if any, emergency response programs have included specific mental health promotion and intervention measures. This highlights a critical gap in addressing the mental health needs of healthcare workers during emergency situations.
Conclusion
In the nurses deployed for emergency responses to the COVID-19 outbreak in one of the epicenters in China, our study found a significant association between fear of infection and fatigue. Fear of infection emerged as a significant stressor, contributing to both anxiety and fatigue among the nurses. We further examined the multiple mediating roles of anxiety and insomnia in the pathway from fear of infection to fatigue. The results demonstrated that anxiety played a partial mediating role in the association between fear of infection and insomnia. In turn, insomnia partially mediated the pathway from anxiety to fatigue.
Based on these findings, we recommend strengthening interventions targeting fear of infection, anxiety, and insomnia to prevent the development of moderate to severe fatigue and potential burnout among nurses deployed for emergency responses. These interventions should encompass pre-deployment, during deployment, and post-deployment measures. It is crucial to incorporate mental health interventions into the management actions as part of the occupational health and safety system.
Data Sharing Statement
The data used in the current study are not publicly available due to privacy or ethical restrictions, but they are available from the corresponding author upon reasonable request.
Ethics Approval
The survey was voluntary and anonymous. Respondents were requested to provide implied informed consent prior to completing the survey. The study protocol complies with the Declaration of Helsinki and obtained approval from the Ethics Committee of Harbin Medical University (HMUIRB2023017).
Acknowledgments
We thank all of the participants of the survey.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (Grant Number 71974049).
Disclosure
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
1. Jarrahi A, Ahluwalia M, Khodadadi H, et al. Neurological consequences of COVID-19: what have we learned and where do we go from here? J Neuroinflammation. 2020;17(1):1–12. doi:10.1186/s12974-020-01957-4
2. Sasangohar F, Jones SL, Masud FN, Vahidy FS, Kash BA. Provider burnout and fatigue during the COVID-19 pandemic: lessons learned from a high-volume intensive care unit. Anesth Analg. 2020;131(1):106–111. doi:10.1213/ANE.0000000000004866
3. Tan YQ, Wang Z, Yap QV, et al. Psychological health of surgeons in a time of COVID-19: a global survey. Ann Surg. 2023;277(1):50. doi:10.1097/SLA.0000000000004775
4. Le XTT, Nguyen QT, Onyango B, et al. Perception toward exposure risk of COVID-19 among health workers in Vietnam: status and correlated factors. Front Public Health. 2021;9:589317. doi:10.3389/fpubh.2021.589317
5. Azoulay E, Cariou A, Bruneel F, et al. Symptoms of anxiety, depression, and peritraumatic dissociation in critical care clinicians managing patients with COVID-19. A cross-sectional study. Am J Respir Crit Care Med. 2020;202(10):1388–1398. doi:10.1164/rccm.202006-2568OC
6. Stedman T. Stedman’s Medical Dictionary. Dalcassian publishing company; 1920.
7. Labrague LJ. Pandemic fatigue and clinical nurses’ mental health, sleep quality and job contentment during the covid‐19 pandemic: the mediating role of resilience. J Nurs Manag. 2021;29:1992–2001. doi:10.1111/jonm.13383
8. Thiffault P, Bergeron J. Fatigue and individual differences in monotonous simulated driving. Pers Individ Dif. 2003;34:159–176. doi:10.1016/S0191-8869(02)00119-8
9. Sikaras C, Ilias I, Tselebis A, et al. Nursing staff fatigue and burnout during the COVID-19 pandemic in Greece. AIMS Public Health. 2021;9:94–105. doi:10.3934/publichealth.2022008
10. Rogers AE. The effects of fatigue and sleepiness on nurse performance and patient safety. In: Patient Safety and Quality: An Evidence-Based Handbook for Nurses. US: Agency for Healthcare Research and Quality; 2008.
11. Meisenhelder JB, LaCharite CL. Fear of contagion: a stress response to acquired immunodeficiency syndrome. Adv Nurs Sci. 1989;11(2):29–38. doi:10.1097/00012272-198901000-00007
12. Kish-Gephart JJ, Detert JR, Treviño LK, Edmondson AC. Silenced by fear: the nature, sources, and consequences of fear at work. Res Organ Behav. 2009;29:163–193. doi:10.1016/j.riob.2009.07.002
13. Fitzpatrick KM, Harris C, Drawve G. Fear of COVID-19 and the mental health consequences in America. Psychol Trauma. 2020;12:S17. doi:10.1037/tra0000924
14. Mulyadi M, Dedi B, Hou W-L, Huang I-C, Lee B-O. Nurses’ experiences of emergency department triage during the COVID‐19 pandemic in Indonesia. J Nurs Scholarsh. 2022;54:15–23. doi:10.1111/jnu.12709
15. Becerra-Medina LT, Meneses-La-Riva ME, Ruíz-Ruíz MT, Marcilla-Félix A, Suyo-Vega JA, Fernández-Bedoya VH. Mental health impacts of nurses caring for patients with COVID-19 in Peru: fear of contagion, generalized anxiety, and physical-cognitive fatigue. Front Psychol. 2022;13:917302. doi:10.3389/fpsyg.2022.917302
16. Lu W, Wang H, Lin Y, Li L. Psychological status of medical workforce during the COVID-19 pandemic: a cross-sectional study. Psychiatry Res. 2020;288:112936. doi:10.1016/j.psychres.2020.112936
17. Arnetz JE, Goetz CM, Arnetz BB, Arble E. Nurse reports of stressful situations during the COVID-19 pandemic: qualitative analysis of survey responses. Int J Environ Res Public Health. 2020;17(21):8126. doi:10.3390/ijerph17218126
18. Gallop RM, Lancee WJ, Taerk G, Coates RA, Fanning M. Fear of contagion and AIDS: nurses’ perception of risk. AIDS Care. 1992;4(1):103–109. doi:10.1080/09540129208251624
19. Dugas MJ, Laugesen N, Bukowski WM. Intolerance of uncertainty, fear of anxiety, and adolescent worry. J Abnorm Child Psychol. 2012;40:863–870. doi:10.1007/s10802-012-9611-1
20. Dymecka J, Machnik-Czerwik A, Filipkowski J. Fear of COVID-19, risk perception and stress level in Polish nurses during COVID-19 outbreak. J Neurol Neurosurg Nurs. 2021;10:3–9.
21. Salari N, Khazaie H, Hosseinian-Far A, et al. The prevalence of sleep disturbances among physicians and nurses facing the COVID-19 patients: a systematic review and meta-analysis. Global Health. 2020;16(1):92. doi:10.1186/s12992-020-00620-0
22. Piper BF, Lindsey AM, Dodd MJ. Fatigue mechanisms in cancer patients: developing nursing theory. Oncol Nurs Forum. 1987;14(6):17–23.
23. Zhan Y, Liu Y, Liu H, et al. Factors associated with insomnia among Chinese front‐line nurses fighting against COVID‐19 in Wuhan: a cross‐sectional survey. J Nurs Manag. 2020;28:1525–1535. doi:10.1111/jonm.13094
24. Sun N, Wei L, Shi S, et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am J Infect Control. 2020;48(6):592–598. doi:10.1016/j.ajic.2020.03.018
25. Jansson-Fröjmark M, Lindblom K. A bidirectional relationship between anxiety and depression, and insomnia? A prospective study in the general population. J Psychosom Res. 2008;64(4):443–449. doi:10.1016/j.jpsychores.2007.10.016
26. Papadimitriou GN, Linkowski P. Sleep disturbance in anxiety disorders. Int Rev Psychiatry. 2005;17(4):229–236. doi:10.1080/09540260500104524
27. Akbarpour S, Nakhostin-Ansari A, Haghighi KS, et al. COVID-19 fear association with depression, anxiety, and insomnia: a national web-based survey on the general population. Iran J Psychiatry. 2022;17:24. doi:10.18502/ijps.v17i1.8046
28. Harvey AG. A cognitive model of insomnia. Behav Res Ther. 2002;40(8):869–893. doi:10.1016/S0005-7967(01)00061-4
29. Smets EMA, Garssen B, de Bonke B, De Haes J. The Multidimensional Fatigue Inventory (MFI) psychometric qualities of an instrument to assess fatigue. J Psychosom Res. 1995;39(3):315–325. doi:10.1016/0022-3999(94)00125-O
30. Saremi M, Fallah MR. Subjective fatigue and medical errors among nurses in an educational hospital. Iran Occup Health. 2013;10:1–8.
31. Bazazan A, Dianat I, Mombeini Z, Aynehchi A, Jafarabadi MA. Fatigue as a mediator of the relationship between quality of life and mental health problems in hospital nurses. Accid Anal Prev. 2019;126:31–36. doi:10.1016/j.aap.2018.01.042
32. Miao Y, Liu X, Liu W, Xie H, Deng G. Initial revision of the Chinese version of multidimensional fatigue inventory-20 in medical staff of military basic level. Chine Ment Health J. 2008;22:658–661. Chinese.
33. Heutte N, Flechtner HH, Mounier N, et al. Quality of life after successful treatment of early-stage Hodgkin’s lymphoma: 10-year follow-up of the EORTC–GELA H8 randomised controlled trial. Lancet Oncol. 2009;10(12):1160–1170. doi:10.1016/S1470-2045(09)70258-X
34. Bastien CH, Vallières A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. doi:10.1016/S1389-9457(00)00065-4
35. Yang CM, Hsu SC, Lin SC, Chou YY, Chen YM. Reliability and validity of the Chinese version of insomnia severity index. Arch Clin Psychol. 2009;4:95–104. Chinese.
36. Agameel MM, Mohsen SAA-E, Dyab NA, Abdelwahed AY, Fakieh RA. Perceived stress, anxiety and insomnia among nursing staff in Saudi Arabia during the 2019 novel coronavirus disease pandemic. OJN. 2022;12(01):1–11. doi:10.4236/ojn.2022.121001
37. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166:1092. doi:10.1001/archinte.166.10.1092
38. Qian J, Bian C, Cui H, Wu W, Li C. Comparative study of reliability and validity between several screening scales for anxiety. J Int Med Concepts Pract. 2011;6:176–179. Chinese.
39. Lai J, Ma S, Wang Y, et al. Factors associated with mental health outcomes among health care workers exposed to Coronavirus Disease 2019. JAMA Netw Open. 2020;3:e203976. doi:10.1001/jamanetworkopen.2020.3976
40. Zhan Y, Zhao S, Yuan J, et al. Prevalence and influencing factors on fatigue of first-line nurses combating with COVID-19 in China: a descriptive cross-sectional study. Curr Med Sci. 2020;40(4):625–635. doi:10.1007/s11596-020-2226-9
41. Aloweni F, Bouchoucha SL, Hutchinson A, et al. Health care workers’ experience of personal protective equipment use and associated adverse effects during the COVID‐19 pandemic response in Singapore. J Adv Nurs. 2022;78(8):2383–2396. doi:10.1111/jan.15164
42. Kaur M, Kumar A, Kaur S, et al. Adverse effects of personal protective equipment and their self-practiced preventive strategies among the Covid-19 frontline health care workers. Hosp Top. 2022:1–12. doi:10.1080/00185868.2022.2112523
43. Ünver S, Yildirim M, Yenigun SC. Personal protective equipment related skin changes among nurses working in pandemic intensive care unit: a qualitative study. J Tissue Viability. 2022;31:221–230. doi:10.1016/j.jtv.2022.01.007
44. Hayes AF. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach. Guilford publications; 2017.
45. Wang J, Li D, Bai X, et al. The physical and mental health of the medical staff in Wuhan huoshenshan hospital during COVID-19 epidemic: a structural equation modeling approach. Eur J Integr Med. 2021;44:101323. doi:10.1016/j.eujim.2021.101323
46. Graham KC, Cvach M. Monitor alarm fatigue: standardizing use of physiological monitors and decreasing nuisance alarms. Am J Crit Care. 2010;19(1):28–34. doi:10.4037/ajcc2010651
47. Çakıcı N, Avşar G, Çalışkan N. The challenges of nurses who care for COVID-19 patients: a Qualitative Study. Holist Nurs Pract. 2021;35(6):315. doi:10.1097/HNP.0000000000000480
48. Galehdar N, Kamran A, Toulabi T, Heydari H. Exploring nurses’ experiences of psychological distress during care of patients with COVID-19: a qualitative study. BMC Psychiatry. 2020;20(1):489. doi:10.1186/s12888-020-02898-1
49. Chen H, Eyoun K. Do mindfulness and perceived organizational support work? Fear of COVID-19 on restaurant frontline employees’ job insecurity and emotional exhaustion. Int J Hosp Manag. 2021;94:102850. doi:10.1016/j.ijhm.2020.102850
50. Çalışkan E, Kargın M. The relationship between coronavirus 19 fear and occupational fatigue, burnout and recovery levels in healthcare professionals in Turkey. Arch Environ Occup Health. 2022;77(9):711–720. doi:10.1080/19338244.2021.2002796
51. Schwartz T, Pines E. Coping with fatigue, fear, and panic during a crisis. Harv Bus Rev. 2020;2020;3.
52. Yıldırım M, Solmaz F. COVID-19 burnout, COVID-19 stress and resilience: initial psychometric properties of COVID-19 burnout scale. Death Stud. 2022;46(3):524–532. doi:10.1080/07481187.2020.1818885
53. Sun T, Huang X-H, Zhang S-E, et al. Fatigue as a cause of professional dissatisfaction among Chinese nurses in intensive care unit during COVID-19 pandemic. Risk Manag Healthc Policy. 2023;Volume 16:817–831. doi:10.2147/RMHP.S391336
54. Ruggiero JS. Correlates of fatigue in critical care nurses. Res Nurs Health. 2003;26(6):434–444. doi:10.1002/nur.10106
55. Fang J, Kunaviktikul W, Olson K, Chontawan R, Kaewthummanukul T. Factors influencing fatigue in Chinese nurses. Nurs Health Sci. 2008;10(4):291–299. doi:10.1111/j.1442-2018.2008.00407.x
56. Yıldırım M, Arslan G, Özaslan A. Perceived risk and mental health problems among healthcare professionals during COVID-19 pandemic: exploring the mediating effects of resilience and coronavirus fear. Int J Ment Health Addict. 2022;20(2):1035–1045. doi:10.1007/s11469-020-00424-8
57. Porcelli P. Fear, anxiety and health-related consequences after the COVID-19 epidemic. Clin Neuropsychiatry. 2020;17:103. doi:10.36131/CN20200215
58. De Clercq D, Haq IU, Azeem MU, Khalid S. The link between fear about COVID-19 and insomnia: mediated by economic concerns and psychological distress, moderated by mindfulness. J Manag Organ. 2023;29:445–463. doi:10.1017/jmo.2021.3
59. Toker S, Laurence GA, Fried Y. Fear of terror and increased job burnout over time: examining the mediating role of insomnia and the moderating role of work support: fear of terror, insomnia, and job burnout. J Organiz Behav. 2015;36:272–291. doi:10.1002/job.1980
60. Roth T, Roehrs T. Insomnia: epidemiology, characteristics, and consequences. Clin Cornerstone. 2003;5(3):5–15. doi:10.1016/S1098-3597(03)90031-7
61. Stein MB, McCarthy MJ, Chen C-Y, et al. Genome-wide analysis of insomnia disorder. Mol Psychiatry. 2018;23(11):2238–2250. doi:10.1038/s41380-018-0033-5
62. Ho Park J, An H, Sook jang E, Chung S. The influence of personality and dysfunctional sleep-related cognitions on the severity of insomnia. Psychiatry Res. 2012;197(3):275–279. doi:10.1016/j.psychres.2011.09.018
63. Perogamvros L, Castelnovo A, Samson D, Dang-Vu TT. Failure of fear extinction in insomnia: an evolutionary perspective. Sleep Med Rev. 2020;51:101277. doi:10.1016/j.smrv.2020.101277
64. Wong TW, Yau JK, Chan CL, et al. The psychological impact of severe acute respiratory syndrome outbreak on healthcare workers in emergency departments and how they cope. Eur J Emerg Med. 2005;12:13–18. doi:10.1097/00063110-200502000-00005
65. Van Dis EA, Van Veen SC, Hagenaars MA, et al. Long-term outcomes of cognitive behavioral therapy for anxiety-related disorders: a systematic review and meta-analysis. JAMA psychiatry. 2020;77:265–273. doi:10.1001/jamapsychiatry.2019.3986
66. Soh HL, Ho RC, Ho CS, Tam WW. Efficacy of digital cognitive behavioural therapy for insomnia: a meta-analysis of randomised controlled trials. Sleep Med. 2020;75:315–325. doi:10.1016/j.sleep.2020.08.020
67. Zhang MW, Ho R. Moodle: the cost effective solution for internet cognitive behavioral therapy (I-CBT) interventions. Technol Health Care. 2017;25:163–165. doi:10.3233/THC-161261
68. Ho CS, Chee CY, Ho RC. Mental health strategies to combat the psychological impact of COVID-19 beyond paranoia and panic. Ann Acad Med Singapore. 2020;49:1–3.
69. Goetzel RZ, Roemer EC, Holingue C, et al. Mental health in the workplace: a call to action proceedings from the mental health in the workplace: public health summit. J Occup Environ Med. 2018;60:322. doi:10.1097/JOM.0000000000001271
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.