Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 13
Antiretroviral Therapy and Retention in Care Experiences and Needs of Adolescents Living with HIV in Southern Ethiopia
Authors Tunje A ![]() , Jerene D
, Jerene D ![]() , Kristensson Hallström I
, Kristensson Hallström I
Received 15 September 2021
Accepted for publication 12 November 2021
Published 26 November 2021 Volume 2021:13 Pages 999—1007
DOI https://doi.org/10.2147/HIV.S339413
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Bassel Sawaya
Abayneh Tunje,1,2 Degu Jerene,1,3 Inger Kristensson Hallström1
1Child and Family Health, Department of Health Sciences, Faculty of Medicine, Lund University, Lund, Sweden; 2School of Public Health, College of Medicine and Health Sciences, Arba Minch University, Arba Minch, Ethiopia; 3KNCV Tuberculosis Foundation, The Hague, Netherlands
Correspondence: Abayneh Tunje Tel +251920011972
Email [email protected]
Background: Adolescents with HIV are faced with challenges when taking care of their medication, which affects their treatment adherence. Therefore, this study aimed to explore the experiences and needs of adolescents living with HIV regarding their antiretroviral therapy adherence and retention in care in southern Ethiopia.
Methods: An inductive qualitative study design was applied to explore adolescents’ experiences and needs regarding antiretroviral treatment adherence and retention in care in southern Ethiopia. Eighteen adolescents were selected from five HIV care and treatment facilities by purposive sampling. The interviews followed an interview guide, translated into the participants’ national language. The interviews were transcribed verbatim and the first author developed a coding frame for the analysis by using NVivo software including meaning units and codes, which were discussed by all authors. Then, sub-themes and themes were identified and analyzed by qualitative content analysis.
Results: The results were described in two themes: barriers and facilitators for treatment adherence and retention in care. Barriers were described in seven subthemes and facilitators in three subthemes. Forgetting to take medication, hiding information, or non-disclosure of HIV status, being afraid to collect treatment drugs, being in an orphanage, and school activities were described as barriers while support from health care workers, families, personal motivation to cope with medication-related problems were described as facilitators for antiretroviral therapy adherence and retention in care.
Conclusion: Adherence is a major challenge among adolescents living with HIV in Ethiopia, with barriers that are unique to this age group and their living conditions. Therefore, interventions should be targeted to address privacy barriers, stigma, and lack of support.
Keywords: antiretroviral therapy adherence, adolescents, disclosure, HIV, qualitative study, retention in care
Introduction
Adolescents, defined as persons aged between 10 and 19,1 account for about 1.7 million of all people living with the human immunodeficiency virus (HIV).2 Of these, about 1.5 million (88%) live in sub-Saharan Africa.3 Successes in the prevention of mother-to-child transmission (PMTCT) program are believed to lead to substantial reductions in new perinatal infections, whilst new sexually acquired infections among the older adolescent group seem to fuel the HIV epidemic.4 More recent global cohort data on adolescents aged 10–14 years showed that about 79% of prenatally HIV-infected adolescents were living in sub-Saharan Africa.5,6 Adolescents, as they transition from childhood to adulthood, are faced with unique challenges of taking care of themselves, which affects their treatment adherence and retention in care. Retention in care is defined as a patient’s regular engagement with medical care at a health care facility after initial entry into the system.7 Evidence from a systematic review suggests that adherence to antiretroviral treatment (ART) among adolescents was only 62.3%,8 and as adolescents get older and are under less parental supervision, adherence to their ART medication becomes a challenge.9 Other challenges related to ART adherence were: being in an orphanage,10 financial constraints,11 accessibility,12 fear of stigma,11–13 high pill burden, ART side effects,12 depression,14 and forgetfulness.15,16 For these reasons, the World Health Organization (WHO) recommends better support for adolescents to improve their adherence to treatment and retention in care.17
ART adherence is defined as the level to which a person is taking medicine as prescribed by a physician and as per medical recommendations for timing, dosing, and consistency, and correctly taking the drugs in terms of the right doses at the right time.18,19 For ART to be effective and stop the emergence of resistant strains, a strict adherence level of ≥95% is suggested.20 Failure to achieve the specified adherence level leads to accelerated progression of PLWHIV to AIDS,21 increased morbidity and mortality,22 and resistance to ART.23 In Ethiopia, 34% of out of 74% of people who were on ART had not achieved the expected level of viral load suppression.24 This low viral load suppression rate indicates poor adherence to ART and retention in care. To facilitate adherence and improve treatment outcomes in HIV-infected adolescents, an understanding of barriers and facilitators helps in planning interventions to address adherence concerns. Therefore, this study aimed to explore the experiences and needs of adolescents living with HIV regarding their ART adherence and retention in care in southern Ethiopia.
Methods
Design and Study Setting
An inductive qualitative study design was applied.25 The study was conducted at five health facilities (two health centers and three hospitals) in the Gamo, Gofa, and south Omo zones in the Southern Nations Nationalities and People’s Region (SNNPR) of Ethiopia. In this study area, there were 28 districts and seven town administrations. There are five hospitals and 71 health centers providing health services for the 2 million population, of whom 85% live in rural areas. At the time of the study, approximately 15,000 HIV patients were enrolled for ART services in the facilities. Of these, about 400 were adolescents.
Participant Recruitment and Data Collection
The adolescents were purposively recruited from August to October 2020 to get a broad variety of participants regarding age, gender, the living context through maximum variation sampling technique.26 Inclusion criteria were adolescents aged 10–19, diagnosed with HIV and on ART. The first author approached eighteen adolescents with HIV when they arrived at the ART clinic to receive routine service. Staff in the ART clinic facilitated the interview process and all those asked were willing to participate. The interviews were performed by the first author and followed a semi-structured interview guide developed after reviewing the literature, including questions about feelings when the physician told of status, disclosure, treatments, and challenging parts of the care. The interviews were performed in Amharic, one of the national languages, and lasted 20–30 minutes in a quiet and confidential area at the respective health facilities. All interviews were audio-recorded with the permission of the adolescents. The age of adolescents who participated in the interview ranged from 10–18 years and all of them could read and write. Out of the 18 interviewed adolescents, 15 were infected with HIV vertically from mother at birth, two acquired the virus through sexual contact, and one did not know the source of infection and suspected the exposure of harmful traditional uvular practice in childhood. All were aware of their HIV status. Sixteen had been in ART treatment for more than a year and two had less than a year of experience.
Data Analysis
Sixteen of the interviews were transcribed verbatim by the first author and two by an independent assistant. Then the interviews were translated from Amharic to English by the first author and checked for accuracy by one independent language expert. All authors read the transcribed interviews independently for familiarization. After that, the first author developed a coding frame for the analysis by using NVivo software including meaning units and codes, which were discussed by all authors. Preliminary sub-themes and themes were identified and reviewed, checked for accuracy with the transcripts, and discussed among all three authors until consensus was reached using thematic analysis.27 Finally, quotes from the adolescents were used to illustrate the sub-themes.
Result
The experiences and needs of adolescents living with HIV were described in two themes: barriers and facilitators for treatment adherence and retention in care. Barriers were described in seven subthemes and facilitators in three subthemes. See Table 1.
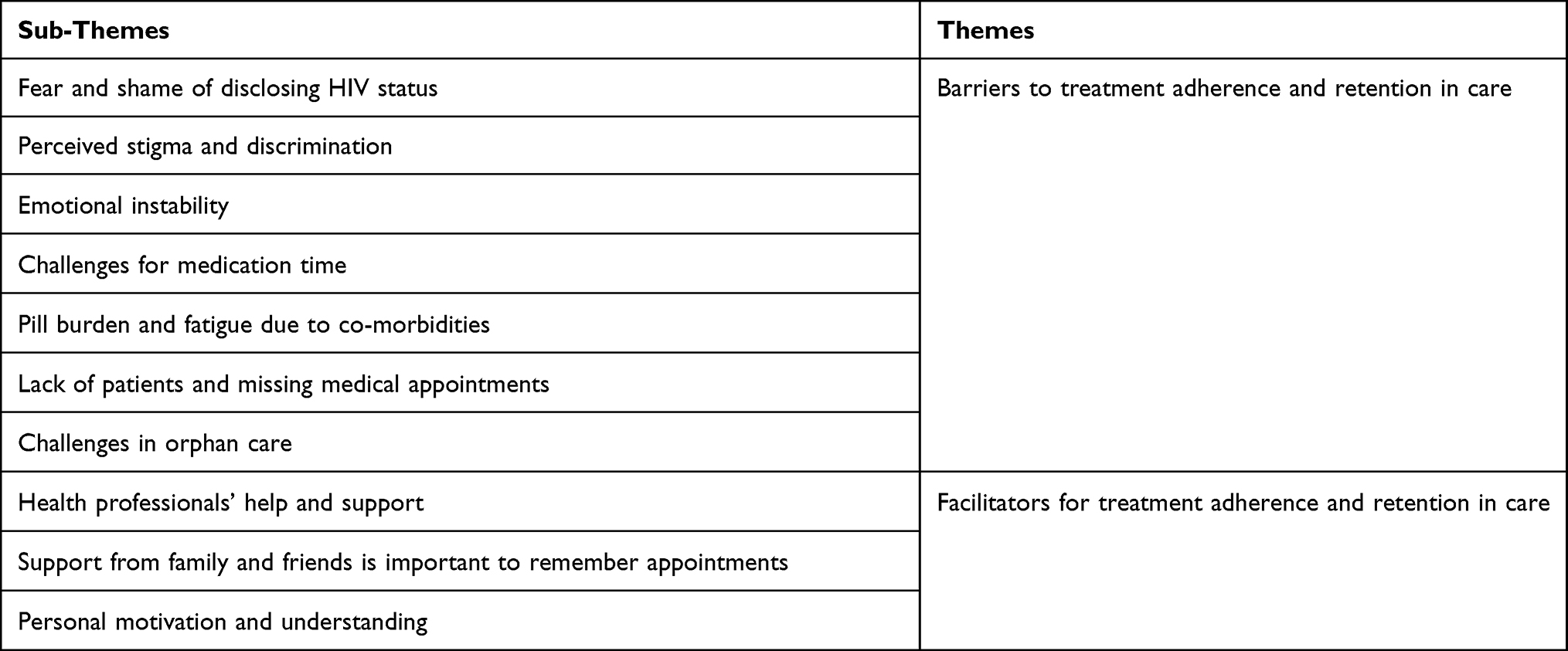 |
Table 1 Themes and Subthemes of Adolescents’ Experiences and Needs of Living with HIV in Ethiopia |
Barriers to Treatment Adherence and Retention in Care
Fear and Shame of Disclosing Their HIV Status
The adolescents described how their family kept their HIV status secret and how they were afraid to disclose their status to others. They did not want to reveal their status to anyone except some of the family members and adolescents participating in the psychosocial support group at the hospital. The adolescents believed that the information was private and they were afraid that disclosing it would end social interactions and that they would lose their close friends. To keep their HIV status secret, they hid their medication during play, studying, fasting, and prayer, while waiting for dinner and visiting friends and relatives.
So far, no one knows my history except my mother and brother. Neither my father nor anyone else knew that I have HIV. I do not want my friends to know my status. Because if they hear it, they will go to other friends and talk to them and may detach my relationship. (13 years, old Female)
Perceived Stigma and Discrimination from Family, Friends, and Society
Adolescents described how they feared being seen by others while taking medication, visiting the clinic for appointments, and collecting ART medication as they were afraid of being stigmatized. Medication times and hospital appointments were not respected due to the fear of shame from friends and the risk of disclosing their status. Adolescents described how health workers insulted them when they missed their appointments and how they stopped taking the drug because of that. Sometimes a family member or another caregiver collected their medication as they feared suffering discrimination. Adolescents described how they preferred to live alone after becoming orphans due to discrimination or lack of support from relatives.
“Students run away from me at school and I get angry and when someone makes jokes about the disease, I get very upset” (15 years old, Male).
Emotional Instability
Disclosing HIV sero-status to adolescents was described as having a negative impact on the adolescent’s emotions. The reactions to disclosure ranged from anger to expressions of a shock to a feeling of sadness and crying. They described how they became emotionally shocked, desired to commit suicide, and were anxious about dying soon when the health care provider disclosed their HIV-positive status. Some of them reported an immediate feeling of hopelessness, and disappointment about their status, and they often faced internal struggles with self-stigma and worried about the impact of HIV on their future relationships. In contrast, others reported a sense of relief when playing with peers who disclosed their HIV status.
“I am very much disappointed! I hated myself, and I was very nervous when I went to the hospital for a monthly appointment” (17 years old, Male).
“I am involved in the psycho-social support group. When we play with our peers, the anxiety is gone” (16 years old, Male).
Challenges for Medication Time
Adolescents were challenged to fit their daily ART medication into their schedules. They were most concerned about the morning dose, which was challenging for them, as they had to leave for school early in the morning before the scheduled time in order to take their ART medication and before breakfast. Sometimes they stopped taking the drug when church preachers prayed for them and said they were cured. The adolescents experienced discomfort when they took their ART medication on an empty stomach and felt sick and uncomfortable The fear of being seen taking medication led to forgetting or delaying the drug to be taken at the prescribed time.
They give me medicine to take twice a day. However, I could not take it properly. I don’t want to take it in the morning because in the morning most of the time there’s a fasting and praying program at the church so I took morning and evening medicine together in the evening. (15 years old, Male)
When I go out with friends and play, sometimes the medication hours pass. In addition, the medication time is usually delayed, especially if a guest comes to our house. Because I put the drugs on the buffet in the living room, then it’s not comfortable to swallow it in front of others. (17 years old, Male)
Pill Burden and Fatigue Due to Co-Morbidities
For the adolescents, the pill burden and treatment fatigue were described as adding to other ART-related challenges, such as side effects, emotional and physical tiredness due to internalized feelings of shame, and forgetfulness. It was not just about the burden of taking pills every day, but the adolescents also felt exhausted due to their low income, being an orphan, or other interconnected challenges such as mental health issues, stigma, and discrimination. The adolescents who had co-morbidity described the difficulty of taking multiple drugs both in the morning and in the evenings.
After my parents died, I was also infected by tuberculosis, so I was tired of taking tuberculosis and HIV drugs together, and I was fatigued by taking the drug. So some days if I take it in the morning, there is a day when I don’t take it in the evening. (17 years old, Male)
Missing Medical Appointments
Fear of going to the hospital alone or having problems with money for transportation to the hospital for appointments were described as reasons for missing hospital appointments, especially by those who came from a remote area or were orphans. The adolescents said that they sometimes felt overwhelmed by their problems or that they lacked the patience to follow the treatment adherence and retention in care properly and skipped the day of the appointment.
Sometimes I don’t go to a hospital appointment and I don’t get advice from health care providers because I don’t want anyone to see me. Even when I run out of the drug and I come to the hospital on the day of the appointment, if there is a long queue, I will return home without taking the drug. (14 years old, Female)
Keeping hospital appointments is challenging for me because since my mother is a servant at the private limited organization, sometimes the organization does not allow her to go to hospital during working hours. As a result, I have been forced to miss the appointment and drug collection because I am afraid to go to the hospital alone. (13 years old, Male)
Challenges in Orphan Care
Adolescents who were orphans and under the care of non-biological caregivers such as grandmothers, aunts, uncles, and siblings, or had parents who worked far away from home described a lack of assistance and support for adherence. They described how, in the past, people who took antiretroviral treatment would be treated free of charge if they contracted any disease. Now, other than HIV the adolescents themselves covered all medical costs. Hence, orphans who did not have enough money were not treated on time, and as a result, they described that living with an aunt or uncle, or a guardian, meant poor adherence.
I don’t have a mother, a father, a brother, or a sister. Therefore, there is no one to help me. I have been living with a caregiver who is also a drug user. Difficult to get food and to take the medication, if I don’t take food at that time, what will happen to me more than this, I need food, I may not get food when I need it. (16 years old, Male)
Facilitators for Treatment Adherence and Retention in Care
Health Professionals’ Help and Support
Health professionals were described as playing a significant role in counseling, motivating, and providing support to improve treatment adherence and retention in care. The adolescents described the patient-provider relationship as an important element in their treatment adherence and retention in care. Health care workers used home-to-home search as a strategy by sending adherence support staff to those who were lost to follow-up. Sometimes the treatment supporter collected their medicine when they were too unwell or unwilling to go to the clinic. They also described receiving psychosocial support from people engaged in religious activities. Support from religious aspects such as fasting, healing, or cures was sometimes described as positively affecting their treatment adherence and retention in care.
One adolescent described it thus:
“A nurse said that you are going to die, and she brought me to the hospital again. I finally agreed, and now I live in peace” (17 years old, female)
Support from Family and Friends
Getting support from families and friends was described as positively influencing ART treatment, and one way of optimizing adherence. When adolescents were living with their own family, they felt that their family members, including parents and siblings, generally provided a supportive environment, often reminding them to collect and take their medication. The caregivers frequently gave advice or reminded adolescents to take their medication, supervised, or watched as they took their medication. Adolescents participating in psychosocial support groups described how they were supported by their peers and how they helped them to keep up with their treatment and relieved their anxiety. Peers in psychosocial support were described as reinforcing positive behavior to increase ART adherence.
Before joining the psychosocial support group, sometimes I forgot to take my drug on time, and as a result, I was severely sick. Now I am participating in a psychosocial support group in the hospital and having a good time with my peers. Now I am using the drug properly and getting better. (18 years old, Female)
At first, it was very difficult for me to take the drug that other children did not take. But now I’m using it properly due to care and support from family and health care providers, except for the time variation in taking it. (15 years old, Female)
Personal Motivation and Understanding
Adolescents who had an understanding of poor outcomes without ART medication were motivated to adhere to their ART medication. They understood why they were receiving treatment, the gravity of missing antiretroviral therapy, and they developed and used strategies to remember their medication time. They believed that the medicine worked well and that they could live as long as HIV-negative people live. To minimize forgetting to take their medication they bought alarm clocks or programmed the times for taking medication into their cell phones, used television programs or asked families to remind them, and planned to use text messages as strategies.
I often watch a television program to remember the medication time. If the television program came, I knew it was also my medication time. When the electric power is off, I look at my watch or my sister’s phone. (15 years old, Female)
Discussion
In this study, adolescents described their experiences of their ART and retention in care in terms of barriers and facilitators. Forgetting to take medication, hiding information, or non-disclosure of HIV status to family, friends, or romantic partners were described as the main barriers to ART adherence and retention in care. As suggested in the literature from Uganda,28,29 the fear of stigma influences disclosure, disease management, and social relations and was a big hindrance to ART and retention in care. Similarly in Ghana, the fear of stigmatization after disclosure to their classmates and their friends or peers within the home environment has been reported as a barrier to adherence and retention in care.30 However, the study conducted in Uganda revealed that children were tuned in to the stigma and keeping their condition secret. As a result, the cause of non-adherence is not necessarily forgetfulness, but knowingly avoiding being seen taking their treatment.31 In the present study, forgetfulness to take medicines was reported as a serious barrier to adherence among adolescents, sometimes related to other life events such as attending church programs, going to school, playing with friends, and helping parents/guardians with trading activities. Similar findings were reported in studies from Ethiopia,32 South Africa,33 Uganda,29 Zambia, and Tanzania,34,35 showing that the clash of school activities was the main challenge to collecting ART drugs and adhering to medication time. In our study, the difficulty of getting food at medication time, or late preparation of food by the caregivers, affects adherence to medication time. Studies from Kenya, Uganda, and South Africa also showed that lack of food or food insecurity was a leading obstacle to ART adherence. As a result, adolescents without access to sufficient food reported occasionally skipping the drugs.36–38 In addition, in our study religious beliefs were identified as a barrier to ART adherence as adolescents said that they stopped taking medication in the belief that they would be cured by prayers, or by using holy water. Other studies also reported that religious beliefs and practices such as fasting, healing, or cures negatively affected ART adherence and retention in care.29,32,34,39
After the HIV disclosure, the adolescents in our study described having negative feelings such as disappointment, hopelessness, depression, difficulty accepting, and emotionally wanting to harm themselves. Similarly, a study conducted in Ethiopia revealed that the magnitude of suicidal ideation and attempts among youth attending ART follow-ups was high.40 Another study conducted in Rwanda showed that a great many adolescents were hurt and felt suffering, depressed and isolated, and fewer were motivated to take their ART after disclosure.39,41 A study from Zambia likewise found high rates of emotional difficulties and peer problems in HIV-positive adolescents.42 In addition, studies from Tanzania and Northern Thailand showed that depressive symptoms were common in vertically HIV-infected adolescents.43,44
In the present study, adolescents described how they feared being seen by others while taking medication, visiting clinics for appointments, and collecting ART medication as they were afraid of being stigmatized. Similarly, studies from Tanzania35 and Zambia34 showed that perceived stigma adversely affected collecting ART medication and led to fear of being labeled as HIV-positive. Similarly, a study conducted in the US showed that children who knew their HIV status expressed severe emotional distress, social isolation, and negative self-image.45 Whereas studies from South Africa,46 and West Africa47 have shown that disclosed HIV status improved ART adherence and retention in care.
In the present study adolescents who were orphans or under the care of non-biological caregivers such as grandmothers, aunts, uncles, and siblings or who had parents who worked far away from home described a lack of assistance and support for adherence. Moreover, accessing ART services was hindered by the shortage of money for transportation to visit the clinic because several of the adolescents lived in remote areas where they even have difficulties in getting transport to access the clinic for ART refill. Similar studies have shown that the absence of family support, distance from ART clinics, and lack of money for transportation affected adolescents’ ART adherence negatively.48,49
Support from family, friends, and health professionals was described as the main facilitator for adherence and retention in the present study. Similarly, studies from Ethiopia,11 Zambia,50 and Ghana51 showed that support from families, friends, and health professionals was viewed as an important facilitator for adherence. In addition, a study from Ghana revealed that family support, financial support, adolescents’ knowledge of their HIV status, and support from health care workers were the main facilitators for adherence to ART.30,52 Other studies from Rwanda39 and Uganda29 showed that peer support groups were important for accepting HIV status and facilitating adherence. In addition, in our study adolescents used their mobile phone alarm, mobile phone clock, television, radio, or watch as part of motivational strategies in ART medication reminders. These were also described in a study from Lesotho as the main facilitators for medication adherence.53
Conclusions
Adherence to ART is a major challenge among adolescents living with HIV in Ethiopia, with barriers that are unique to this age group and their living conditions. In exploring the adolescents’ own experiences and needs, an understanding of the difficulty and complexity of their HIV treatment and retention in care can be reached. Forgetting medication time, being afraid to collect ART drugs, being in an orphanage, and school activities have an impact on ART adherence and retention in care. In contrast, adolescents with a comprehensive understanding of ART medication seem to be motivated to adhere to their ART medication by developing motivation strategies to remind them of medication times. Giving support to the adolescents will further enable them to make life better and sustain adherence and retention in care. Therefore, interventions should be targeted to address privacy barriers, stigma, and lack of support.
Abbreviations
ART, Anti-Retroviral Treatment; HIV, Human Immunodeficiency Virus; PLWHIV, People Living With HIV; PMTCT, Prevention of Mother-To- Child Transmission; SNNPR, Southern Nations Nationalities and People’s Region; WHO, World Health Organization.
Data Sharing Statement
Data supporting the findings of this study are available from the authors on request.
Ethical Approval and Informed Consent
We conducted this study under the 1964 Declaration of Helsinki and its later amendments. The study was approved by the Swedish Ethical Review Authority (Dnr 2019-03433), National Research Ethics Review Committee in Ethiopia, and the Institutional Research Ethics Review Board in Arba Minch University. Management of the hospitals and health centers granted permission to conduct the study. Information about the study was provided to each participant. Adolescents aged 18 years and above signed their informed consent, and formal caregivers and the adolescents signed the assent for adolescents aged 10–17 years in the local language according to the National and International Guiding Principles for research involving minors.54 In addition, participants consented to the publication of their responses as long as they were kept anonymous.
Acknowledgment
The authors would like to thank the study participants and facilitators during data collection.
Author Contributions
All authors contributed to data analysis, drafting, or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The study was supported by the Swedish Research Council for Health, Working Life and Welfare Life (FORTE) (https://forte.se/en/) program support 2018–01399 and the Swedish Research Council (Vetenskapsrådet) (https://www.vr.se/english.html) program support VR 2016-05706. The funder had no role in the design of the study and collection, analysis, and interpretation of data or in writing the manuscript. The grant was awarded to IHK and DJ.
Disclosure
The authors report no competing interests in this work.
References
1. World Health Organization. Child and adolescent health and development: progress report 2006-2007: highlights. Available from: https://apps.who.int/iris/handle/10665/43862.
2. UNAIDS. Ending the AIDS epidemic 2020. Available from: https://www.unaids.org/en/resources/fact-sheet.
3. DATAU. UNAIDS epidemiological estimates; 2020. Available from: https://www.unaids.org/sites/default/files/media_asset/2020_aids-data-book_en.pdf.
4. Karim B, Baxter C. HIV incidence rates in adolescent girls and young women in sub-Saharan Africa. Lancet Global Health. 2019;7(11):e1470–e1471. doi:10.1016/S2214
5. UNAIDS. Data from: Joint United Nations Programme on HIV/AIDS (UNAIDS): distribution of new HIV infections by subpopulation. UNAIDS; 2017.
6. Slogrove ALSM, Davies MA, Williams P, Balkan S, Ben-Farhat J. Calles N The epidemiology of adolescents living with perinatally acquired HIV: a cross-region global cohort analysis. PLoSMed. 2018;15(3):
7. Horstmann BJ, Islam F, Buck J, Agins BD, Retaining HI. V-infected patients in care: where are we? Where do we go from here? Clin Infect Dis. 2010;50(5):752–761. doi:10.1086/649933
8. Kim S-H GS, Fidler S, Ward H. Adherence to antiretroviral therapy in adolescents living with HIV. Sys Rev Meta Analysis. 2014;28(13):1945–1956.
9. Marhefka SLKL, Allison S, Bachanas P, et al. Family experiences with pediatric antiretroviral therapy: responsibilities, barriers, and strategies for remembering medications. AIDS Patient Care STDs. 2008;22(8):637–647. doi:10.1089/apc.2007.0110
10. Jerene D, Tiberg I, Hallstrom I. How Can Clinical Outcomes among Adolescents Living with HIV in Ethiopia be Improved? Healthcare Professionals’ Perspectives. Compr Child Adolesc Nurs. 2021;1–10. doi:10.1080/24694193.2021.1914774
11. Achappa B, Madi D, Bhaskaran U, Ramapuram JT, Rao S, Mahalingam S. Adherence to Antiretroviral Therapy Among People Living with HIV. N Am J Med Sci. 2013;5(3):220–223. doi:10.4103/1947-2714.109196
12. WHO. Chapter 9: guidance on operations and service delivery. WHO. Available from: https://www.who.int/hiv/pub/guidelines/arv2013/operational/adherence/en/.
13. Kuhns LM, Hotton AL, Garofalo R, et al. An Index of Multiple Psychosocial, Syndemic Conditions Is Associated with Antiretroviral Medication Adherence Among HIV-Positive Youth. AIDS Patient Care STDS. 2016;30(4):185–192. doi:10.1089/apc.2015.0328
14. Morowatisharifabad M, Movahed E, Farokhzadian J, et al. Depression and physical activity among HIV-positive people: integrated care towards 90-90-90. HIV AIDS Rev Int J HIV Related Problems. 2019;18(2):131–136. doi:10.5114/hivar.2019.86377
15. Ammon NMS, Corkery J, Corkery JM. Factors impacting antiretroviral therapy adherence among human immunodeficiency virus–positive adolescents in sub-Saharan Africa: a systematic review. Public Health. 2018;15(7):20–31. doi:10.1016/j.puhe.2017.12.010
16. Williams PLSD, Montepiedra G, Nichols S, et al. Predictors of adherence to antiretroviral medications in children and adolescents with HIV infection. PEDIATRICS. 2006;118(6):15. doi:10.1542/peds.2006-0493
17. World Health Organization. HIV and adolescents: Guidance for HIV testing and counseling and care for adolescents living with HIV: recommendations for a public health approach and considerations for policy-makers and managers. World Health Organization; 2013.
18. Chaiyachati KHOO, Ogbuoji O, Price M, Suthar AB, Negussie EK, Bärnighausen,T. Interventions to improve adherence to antiretroviral therapy: a rapid systematic review. AIDS. 2014;28(2):187–204. doi:10.1097/QAD.0000000000000252
19. World Health Organization. Adherence to long-term therapies: Evidence for action. World Health Organization; 2003.
20. Paterson DLSS, Mohr J, Brester M, Vergis EN, Squier C, Wagener MM. Singh N Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med Jul. 2000;133(1):21–30. doi:10.7326/0003-4819-133-1-200007040-00004
21. Finitsis DJ, Pellowski JA, Johnson BT. Text Message Intervention Designs to Promote Adherence to Antiretroviral Therapy (ART): a Meta-Analysis of Randomized Controlled Trials. PLoS One. 2014;9(2):e88166. doi:10.1371/journal.pone.0088166
22. Hamine SG, Faulx D, Green BB, Ginsburg AS. Impact of mHealth chronic disease management on treatment adherence and patient outcomes: a systematic review. J Med Internet Res. 2015;17(2):PMC4376208. doi:10.2196/jmir.3951
23. Iacob SA. Improving the Adherence to Antiretroviral Therapy, a Difficult but Essential Task for a Successful HIV Treatment-Clinical Points of View and Practical Considerations Front Pharmacol. Nov. 2017;8:8.
24. UNAIDS. UNAIDS data; 2019. Available from: https://www.unaids.org/en/regionscountries/countries/ethiopia.
25. Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334–340. doi:10.1002/1098-240X(200008)23:4<334::AID-NUR9>3.0.CO;2-G
26. Sandelowski M. Sample size in qualitative research. Res Nurs Health. 1995;18(2):179–183. doi:10.1002/nur.4770180211
27. Braun VaC V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
28. Mutumba MBJ, Musiime V, Byaruhanga J, Francis K, Snow RC. Psychosocial challenges and strategies for coping with HIV among adolescents in Uganda: a qualitative study. AIDS Patient Care STDS. 2015;29(1):86–94. doi:10.1089/apc.2014.0222
29. Nabukeera-Barungi NEP, Asire B, Katureebe C, Lukabwe I, Namusoke E. Adherence to antiretroviral therapy and retention in care for adolescents living with HIV from 10 districts in Uganda. BMC Infect Dis. 2015;15:1–10. doi:10.1186/s12879-015-1265-5
30. Ankrah DN, Mantel-Teeuwisse AK, Arhinful DK, Agyepong IA, Lartey M. Facilitators and barriers to antiretroviral therapy adherence among adolescents in Ghana. Patient Prefer Adhere. 2016;15(3):29–37.
31. Kawuma R, Siu G, Rhodes T, Seeley J. Children will always be children: exploring perceptions and experiences of HIV-positive children who may not take their treatment and why they may not tell. Afr J AIDS Res. 2014;13(2):189–195. doi:10.2989/16085906.2014.927778
32. Bezabhe WM, Chalmers L, Bereznicki LR, Peterson GM, Bimirew MA, Kassie. DM. Barriers and facilitators of adherence to antiretroviral drug therapy and retention in care among adult HIV-positive patients: a qualitative study from Ethiopia. PLoS One. 2014;9(5):e97353. doi:10.1371/journal.pone.0097353
33. Coetzee B, Kagee A, Bland R. Barriers and facilitators to pediatric adherence to antiretroviral therapy in rural South Africa: a multi-stakeholder perspective AIDS care. AIDS Care. 2015;27(3):315–321. doi:10.1080/09540121.2014.967658
34. Denison JA, Banda H, Dennis AC. “the sky is the limit”: adhering to antiretroviral therapy and HIV self-management from the perspectives of adolescents living with HIV and their adult caregivers. J Int AIDS Soc. 2015;18(1):19358. doi:10.7448/IAS.18.1.19358
35. Nyogea D, Mtenga S, Henning L, et al. Determinants of antiretroviral adherence among HIV positive children and teenagers in rural Tanzania: a mixed-methods study. BMC Infect Dis. 2015;15:15–28. doi:10.1186/s12879-015-0753-y
36. Goudge J, Ngoma B. Exploring antiretroviral treatment adherence in an urban setting in South Africa. J Public Health Pol. 2011;32:S52–S64. doi:10.1057/jphp.2011.22
37. Jason M, Nagata R. Cohen Social determinants, lived experiences, and consequences of household food insecurity among persons living with HIV/AIDS on the shore of Lake Victoria, Kenya. AIDS Care. 2012;24(6):728–736. doi:10.1080/09540121.2011.630358
38. Weiser SDTD, Frongillo EA, Senkungu J, Mukiibi N. Bangsberg DR Food Insecurity as a Barrier to Sustained Antiretroviral Therapy Adherence in Uganda. PLoS One. 2010;5:
39. Mutwa PR, Asiimwe-Kateera B, Kestelyn E, et al. Living Situation Affects Adherence to Combination Antiretroviral Therapy in Rwanda: a HIV-Infected Adolescents Qualitative Study. PLoS One. 2013;8(4):e60073. doi:10.1371/journal.pone.0060073
40. Wonde M, Mulat H, Birhanu A. The magnitude of suicidal ideation, attempts, and associated factors of HIV positive youth attending ART follow-ups at St. Paul’s hospital Millennium Medical College and St. Peter’s specialized hospital, Addis Ababa, Ethiopia, 2018. PLoS One. 2019;14(11):e0224371. doi:10.1371/journal.pone.0224371
41. Binagwaho A. Factors associated with disclosure of HIV status among HIV-positive children in Rwanda. Rwanda Med J. 2012;69(3):154.
42. Malee K, Williams P, Montepiedra G. Medication adherence in children and adolescents with HIV infection: associations with behavioral impairment. AIDS Patient Care STDs. 2011;253:191–200. doi:10.1089/apc.2010.0181
43. Lee BCM, Oberdorfer P. Depression among Vertically HIV-Infected Adolescents in Northern Thailand. J Int Assoc Physicians AIDS Care. 2011;10(2):89–96. doi:10.1177/1545109710397892
44. Lwidiko A, Nyundo A, Mpondo BCT. Association between HIV status and depressive symptoms among children and adolescents in the Southern Highlands Zone, Tanzania: a case-control study. PLoS One. 2018;13(2):e0193145. doi:10.1371/journal.pone.0193145
45. Sl I. Perceptions of children with HIV infection when not told for so long: implications for diagnosis disclosure. J Pediatr Health Care. 2000;14(5):235–243. doi:10.1067/mph.2000.107338
46. Madiba S, Mokgatle M. Perceptions and Experiences about Self-Disclosure of HIV Status among Adolescents with Perinatal Acquired HIV in Poor-Resourced Communities in South Africa. AIDS Res Treatment. 2016.
47. Arrive´ E, Amghar H, Aka AE, et al. “HIV status disclosure and retention in care in HIV-infected adolescents on antiretroviral therapy (ART) in West Africa. PLoS One. 2012;7(3):e33690. doi:10.1371/journal.pone.0033690
48. Agwu A, Fairlie L. Antiretroviral treatment, management challenges and outcomes in perinatally HIV-infected adolescents. J Int AIDS Soc. 2013;16(1):18579. doi:10.7448/IAS.16.1.18579
49. Estripeaut D, Luciani K, García R, et al. Analysis of the social and psychosocial factors associated with adherence to antiretroviral therapy in adolescents with perinatal HIV-1 infection in Panama from a gender perspective. AIDS Care. 2016;28(2):66–72. doi:10.1080/09540121.2016.1176669
50. Mburu G, Hodgson I, Kalibala S, et al. Adolescent HIV disclosure in Zambia: barriers, facilitators and outcomes. J Int AIDS Soc. 2014;17(1):18866. doi:10.7448/IAS.17.1.18866
51. Mark D, Armstrong A, Andrade C, et al. HIV treatment and care services for adolescents: a situational analysis of 218 facilities in 23 sub-Saharan African countries. J Int AIDS Soc. 2017;20(3):21591. doi:10.7448/IAS.20.4.21591
52. Evans D, Menezes C, Mahomed K, et al. Treatment outcomes of HIV-infected adolescents attending public-sector HIV clinics across Gauteng and Mpumalanga, South Africa. AIDS Res Hum Retroviruses. 2013;29(6):892–900. doi:10.1089/aid.2012.0215
53. Axelsson JM, Hallager S, Barfod TS. Antiretroviral therapy adherence strategies used by patients of a large HIV clinic in Lesotho. J Health Popul Nutr. 2015;33(10). doi:10.1186/s41043-015-0026-9
54. OHRPPU. Guidance and Procedure: Research Involving Children and Minors, Office of Human Research Protection Program. OHRPPU; 2011.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.