Back to Journals » Journal of Inflammation Research » Volume 19
Antineutrophil Cytoplasmic Antibody-Associated Vasculitis Overlapping with IgG4-Related Disease Accompanied by Mesangial Immunoglobulin a Deposition: A Case Report
Authors Fan YL ![]() , Han WJ, Liu Y, Hao J
, Han WJ, Liu Y, Hao J
Received 28 March 2026
Accepted for publication 8 July 2026
Published 17 July 2026 Volume 2026:19 610417
DOI https://doi.org/10.2147/JIR.S610417
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Shouya Feng
Yu-Lu Fan, Wei-Jie Han, Yang Liu, Jian Hao
Department of Medicine, Division of Nephrology, The Affiliated Hospital of Inner Mongolia Medical University, Hohhot, Inner Mongolia Autonomous Region, 010050, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jian Hao, Department of Medicine, Division of Nephrology, The Affiliated Hospital of Inner Mongolia Medical University, No. 1 North Passage Road, Huimin District, Hohhot, Inner Mongolia Autonomous Region, 010050, People’s Republic of China, Tel +8613704751021, Email [email protected]
Background: Antineutrophil cytoplasmic antibody-associated vasculitis (AAV) and immunoglobulin G4-related disease (IgG4-RD) are both systemic autoimmune disorders that can involve multiple organs; however, they exhibit distinct differences in pathogenesis, clinical manifestations, and histopathological features. Emerging evidence suggests that, in rare instances, AAV and IgG4-RD may coexist in the same patient, constituting an immunological overlap syndrome.
Case Presentation: We reported the case of a 67-year-old woman who presented with proteinuria, hematuria, and impaired renal function. After comprehensive laboratory investigations, imaging studies, and renal biopsy, the patient fulfilled the diagnostic criteria for both AAV and IgG4-RD. Renal biopsy revealed necrotizing crescentic glomerulonephritis with marked IgG4-positive plasma cell infiltration and mesangial immunoglobulin A (IgA) deposition. The patient was treated with systemic glucocorticoids combined with cyclophosphamide, leading to significant improvement in renal function.
Conclusion: The coexistence of AAV and IgG4-RD with concurrent IgA deposition is exceedingly uncommon in clinical practice. This case highlights the complexity of immune-mediated overlap syndromes and underscores the importance of careful pathological assessment, which may inform diagnostic evaluation and treatment strategies.
Keywords: antineutrophil cytoplasmic antibody-associated vasculitis, immunoglobulin G4-related disease, immunoglobulin A deposition, overlap syndrome
Introduction
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis (AAV) represents a group of systemic autoimmune disorders characterized primarily by small-vessel wall inflammation and fibrinoid necrosis.1 AAV frequently affects multiple organ systems, particularly the lungs and kidneys, and renal involvement often manifests as rapidly progressive glomerulonephritis.2 In contrast, Immunoglobulin G4-related disease (IgG4-RD) is a chronic immune-mediated fibroinflammatory condition defined by dense lymphoplasmacytic infiltration, storiform fibrosis, and obliterative phlebitis.3 The principal diagnostic features of IgG4-RD include elevated serum IgG4 concentrations and a marked increase in IgG4-positive plasma cells within affected tissue.4
AAV and IgG4-RD exhibit distinct pathogenic mechanisms and histopathological characteristics, with AAV generally classified as pauci-immune vasculitis and IgG4-RD characterized by prominent lymphoplasmacytic infiltration.5 Notably, AAV is listed among the exclusion criteria in both the 2019 ACR/EULAR classification criteria6 and the 2020 revised comprehensive diagnostic criteria for IgG4-RD,7 underscoring the diagnostic complexity of this overlap syndrome. Recent evidence from case reports and reviews suggests that AAV and IgG4-RD may coexist.8,9 Such cases constitute a rare immunological overlap syndrome that poses significant diagnostic and therapeutic challenges. In addition, a previous case has described AAV associated with IgG4-positive interstitial infiltration and IgA nephropathy.10 Furthermore, the presence of mesangial immunoglobulin A (IgA) deposition in the setting of AAV overlapping with IgG4-RD is exceedingly uncommon and further complicates pathological interpretation. Whether this finding reflects coincidental immune complex deposition or broader immune dysregulation remains uncertain.
In this report, we describe a case of AAV overlapping with IgG4-RD accompanied by mesangial IgA deposition. By analyzing the clinical course and comprehensive pathological findings, we aim to improve recognition of this complex overlap and provide insights into its diagnostic and therapeutic considerations.
Case Presentation
A 67-year-old woman with a prior history of tuberculosis was admitted on December 26, 2024, with a 6-month history of proteinuria that had progressed over the preceding two weeks, accompanied by worsening edema and gross hematuria. Proteinuria was first detected during a routine examination approximately six months prior to admission, at which time the serum creatinine was 92 μmol/L, and no further evaluation was performed. Two weeks before admission, she developed bilateral pitting edema of the lower extremities, along with gross hematuria, nocturia, and mild exertional dyspnea. There were no constitutional symptoms or features suggestive of systemic infection, rash, or arthralgia. No history of bronchial asthma, allergic rhinitis, or other allergic diseases was identified, although a history of amoxicillin allergy was reported.
Laboratory testing revealed anemia (hemoglobin 81 g/L), mildly elevated total IgG (17.1 g/L), and a positive antinuclear antibody (ANA; titer 1:320, speckled pattern). Thyroid function tests and thyroid ultrasonography revealed no evidence of Hashimoto’s thyroiditis or other thyroid diseases. Serological testing for hepatitis B virus, hepatitis C virus, HIV, and syphilis was negative. Urinalysis demonstrated marked hematuria (2318 red blood cells/μL) with dysmorphic erythrocytes on microscopy, and 24-hour urinary protein excretion was 3.86 g. However, the serum albumin level was within the normal range (39.2 g/L) at presentation. Immunological testing showed markedly elevated myeloperoxidase (MPO)-ANCA (>200 RU/mL), while proteinase 3–ANCA and anti-glomerular basement membrane antibodies were negative. Indirect immunofluorescence detected perinuclear ANCA (p-ANCA) at a titer of 1:40. Anti-double-stranded DNA antibodies were negative. Imaging studies did not demonstrate definite extrarenal organ involvement. In view of the high-titer MPO-ANCA and progressive renal impairment, AAV was initially suspected, and the patient was admitted for further evaluation.
After admission, the patient exhibited persistent hematuria and proteinuria, along with progressive renal dysfunction. The erythrocyte sedimentation rate was elevated at 68 mm/h, and serum IgG4 was notably increased at 3961 mg/L. Ultrasonography revealed enlarged lymph nodes in the bilateral inguinal and axillary regions. No constitutional symptoms suggestive of lymphoma, including fever, night sweats, or weight loss, were present. Abdominal ultrasonography showed no abnormalities of the pancreas, liver, or spleen, and no biliary dilatation. Chest CT revealed no evidence of malignancy. The patient had no prior history of hypertension; elevated blood pressure detected during hospitalization was consistent with stage 2 hypertension and was managed with antihypertensive therapy. Given the combination of progressive renal dysfunction, high-titer MPO-ANCA, markedly elevated serum IgG4, and unexplained lymphadenopathy, the possibility of AAV overlapping with IgG4-RD was considered, and oral prednisone was initiated at a dose of 40 mg/day on day 6 after admission.
Percutaneous renal biopsy was performed for diagnostic clarification. Light microscopy demonstrated extensive crescent formation, comprising cellular, fibrocellular, and fibrous crescents, along with segmental glomerulosclerosis (Figure 1A–C). Notably, significant interstitial and periglomerular fibrosis was observed (Figure 1D). Mild to moderate mesangial proliferation and arteriolar wall thickening were observed. The renal interstitium exhibited edema with focal infiltration of lymphocytes and scattered plasma cells, accompanied by fibrosis. Tubular epithelial cells showed cytoplasmic vacuolar and granular degeneration, loss of the brush border, and focal tubular atrophy. Immunofluorescence revealed no significant subepithelial or subendothelial deposits, with only sparse mesangial deposition (Figure 2), which is consistent with AAV-associated pauci-immune vasculitis. Granular IgA deposition was detected in the mesangial areas. Immunohistochemistry demonstrated more than 10 IgG4-positive plasma cells per high-power field, with an IgG4/IgG ratio >40% (Figure 3), fulfilling the pathological criteria for IgG4-RD and the 2020 revised comprehensive diagnostic criteria for IgG4-related kidney disease. Electron microscopy further confirmed the absence of significant subepithelial or subendothelial electron-dense deposits, although minor deposits were noted in the mesangial area (Figure 4). Based on the markedly elevated MPO-ANCA, significantly increased serum IgG4, and renal histopathological findings, a final diagnosis of AAV overlapping with IgG4-RD, accompanied by mesangial IgA deposition, was established.
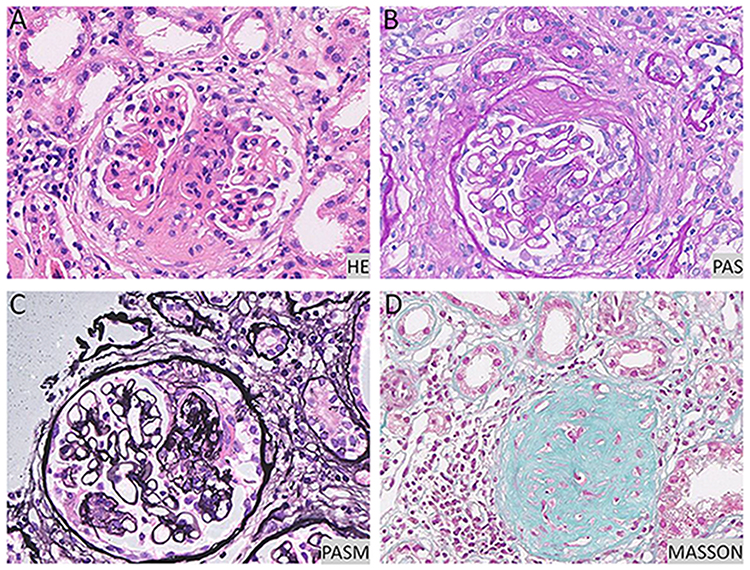 |
Figure 1 Histopathological findings by light microscopy. (A) HE staining, ×400; (B) PAS staining, ×400; (C) PASM staining, ×400; (D) Masson’s trichrome staining, ×400. Abbreviations: HE, hematoxylin and eosin; PAS, periodic acid-Schiff; PASM, Periodic acid-silver methenamine. |
 |
Figure 2 Immunofluorescence staining. (A) IgG; (B) IgA; (C) Lambda; (D) C3. Abbreviations: IgA, immunoglobin A; IgG, immunoglobin G; C3, complement component 3. |
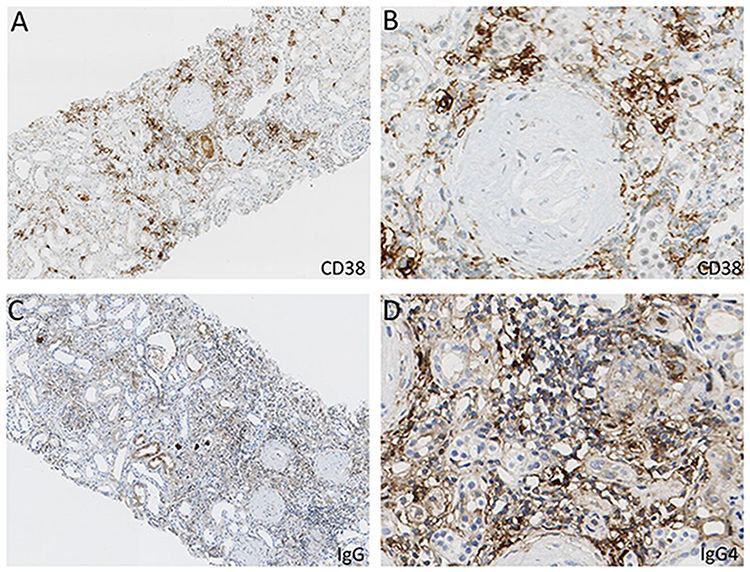 |
Figure 3 Immunohistochemical staining. (A and B) CD38 staining, ×100 and ×400, respectively; (C) IgG staining, ×100; (D) IgG4 staining, ×400. Abbreviations: IgG, immunoglobin G; IgG4, immunoglobin G4. |
 |
Figure 4 Ultrastructural findings by electron microscopy. (A) Extensive podocyte foot process effacement; (B) Thickening of the glomerular basement membrane; (C) Marked thickening of the glomerular capillary loop basement membrane accompanied by podocyte foot process effacement. |
The patient was initially treated with oral glucocorticoids in combination with intravenous cyclophosphamide for induction therapy, along with trimethoprim-sulfamethoxazole for infection prophylaxis. After a one-month hospital stay, she was discharged and continued on oral cyclophosphamide with regular outpatient follow-up. During follow-up, gradual improvements in proteinuria, hematuria, and renal function were observed, accompanied by a significant decrease in serum IgG4 levels (Figure 5). Cyclophosphamide administration was intermittently withheld due to recurrent infections and was ultimately discontinued after a cumulative dose of 6 g over a 10-month post-discharge period. Thereafter, prednisone was gradually tapered by 5 mg every 2 weeks from the initial dose of 40 mg/day to a maintenance dose of 5 mg/day (Figure 6). Notably, MPO-ANCA titers remained persistently elevated (>200 RU/mL) throughout the treatment course.
 |
Figure 5 Laboratory test results. (A) Longitudinal changes in Serum IgG4 levels (mg/L) and serum IgA levels (mg/dL) over time. Horizontal bars indicate prednisone and CTX therapy; cumulative CTX doses are shown. (B) Longitudinal changes in renal function and urinary parameters: Scr (μmol/L), urinary RBC (μL), and 24-hour UTP (g/24h). Horizontal bar shows prednisone duration; arrow indicates a clinical infection. Abbreviations: CTX, cyclophosphamide; IgG4, immunoglobin G4; RBC, red blood cells; Scr, serum creatinine; UTP, urinary protein. |
 |
Figure 6 Timeline of clinical events, diagnostic milestones, and treatments. Clinical features, laboratory results, corresponding therapies, and outcomes are presented chronologically. Abbreviations: AAV, ANCA-associated vasculitis; ANCA, antineutrophil cytoplasmic antibody; IgG4, immunoglobin G4; IgG4-RD, IgG4-related disease; MPO, myeloperoxidase; CTX, cyclophosphamide. |
Discussion
The patient in this case exhibited high-titer MPO-ANCA, and renal biopsy revealed crescentic glomerulonephritis with minimal immune complex deposition, consistent with typical renal involvement in AAV according to the 2022 American College of Rheumatology/European League Against Rheumatism classification criteria.11 Concurrently, markedly elevated serum IgG4 levels, lymphadenopathy, and renal histology showing more than 10 IgG4+ plasma cells per high-power field with an IgG4/IgG ratio >40% fulfilled the pathological criteria for IgG4-RD.6 Thus, this case represents an overlap syndrome of AAV and IgG4-RD. Although serum IgG4 elevation may occur in AAV, the present case fulfilled the 2020 revised comprehensive diagnostic criteria for IgG4-related kidney disease,7 supporting the diagnosis of AAV overlapping with IgG4-RD rather than isolated AAV with secondary IgG4 elevation. Early renal biopsy enabled precise pathological classification and guided glucocorticoid plus cyclophosphamide therapy, resulting in improved renal function and underscoring the importance of timely histopathological diagnosis.
AAV and IgG4-RD are both immune-mediated disorders but differ mechanistically: AAV is driven by ANCA-mediated neutrophil activation leading to necrotizing small-vessel inflammation, whereas IgG4-RD is characterized by Th2- and Tfh-mediated plasma cell infiltration and tissue fibrosis.12 Despite distinct mechanisms, accumulating evidence suggests that AAV and IgG4-RD can coexist,8,13,14 representing a rare immunological overlap syndrome. A European multicenter retrospective study including patients who met both AAV and IgG4-RD criteria found that several patients exhibited atypical features during the AAV course, such as prominent plasma cell infiltration or multi-organ enlargement, suggesting a concurrent IgG4-RD component.9 The study further emphasized the efficacy of rituximab in treating this overlap syndrome, particularly in relapsing cases. Clinicians should therefore consider coexistent IgG4-RD in AAV patients presenting with unexplained organ enlargement or markedly elevated IgG4.
Another notable pathological feature in this case was mesangial IgA granular deposition. IgA nephropathy (IgAN) is a disease caused by abnormal deposition of immunoglobulin A and represents the most common primary glomerulonephritis worldwide.15 While AAV is typically pauci-immune, prior studies have reported occasional IgA deposition.16,17 The coexistence of AAV and IgAN is a rare condition with low incidence, which is easily misdiagnosed or overlooked. A retrospective study of 2390 biopsy-proven IgAN patients identified 35 cases with concurrent AAV,18 indicating that although rare, the two diseases can coexist.
In IgAN patients, ANCA positivity has been associated with fewer extrarenal manifestations compared with typical AAV patients, while potentially correlating with worse renal outcomes.19 In patients with concurrent AAV and IgG4-RD, treatment with glucocorticoids combined with immunosuppressive agents has been shown to achieve favorable therapeutic responses.20
IgA deposition in AAV does not necessarily indicate concurrent IgAN; the key factor is whether the deposits are pathogenic.21 In MPO-AAV patients with IgA deposition, low-intensity deposits (≤1+) do not significantly affect renal survival, suggesting that these deposits are often non-pathogenic.22 In the present case, IgA deposition was mild, mesangial, and granular, consistent with a non-pathogenic pattern. The coexistence of IgG4-RD and IgAN is rare, with only a few reports,23,24 and IgA deposition has occasionally been observed in patients with Henoch–Schönlein purpura nephritis combined with IgG4-RD.25 Therefore, in IgG4-RD patients, evaluation of IgA deposits should be interpreted in the context of their intensity, distribution, and clinical presentation, with follow-up or repeat biopsy if warranted.
Therapeutically, both AAV and IgG4-RD are primarily treated with glucocorticoids, combined with cyclophosphamide or rituximab for intensified immunosuppression. In the present case, renal function improved following treatment with a glucocorticoid-cyclophosphamide regimen, suggesting that this therapeutic strategy is also effective in overlap diseases. Notably, the patient’s MPO-ANCA titer remained persistently high, indicating a potential dissociation between serum ANCA levels and clinical remission, as previously reported in AAV.26 Therefore, patients with this overlap syndrome require long-term follow-up with dynamic monitoring of renal function, ANCA titers, IgG4 levels, and imaging findings to assess disease activity and relapse risk.
Conclusion
This case describes an overlap of AAV and IgG4-RD with mild mesangial IgA deposition. Early renal biopsy revealed necrotizing crescentic glomerulonephritis and IgG4-positive plasma cell infiltration, enabling accurate diagnosis and guiding therapy. Glucocorticoid combined with cyclophosphamide induced marked renal function improvement, supporting the effectiveness of standard AAV regimens in overlap syndromes. Persistent high MPO-ANCA titers despite clinical remission highlight potential discordance between serology and disease activity, emphasizing the importance of longitudinal monitoring. Clinicians should consider concurrent IgG4-RD in AAV patients with elevated IgG4 or plasma cell infiltration, and evaluate the pathogenic significance of coexisting IgA deposits based on intensity and clinical context. Careful pathological assessment and long-term follow-up are crucial in managing such complex overlap cases.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Informed Consent
This study was exempted from ethical approval by the Ethics Committee of The Affiliated Hospital of Inner Mongolia Medical University, as ethical approval is not required for case reports. The study was conducted in accordance with the Declaration of Helsinki, and the CARE reporting guidelines were followed. Written informed consent was obtained from the individual participant included in the study.
Consent for Publication
Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.
Author Contributions
Yu-Lu Fan and Wei-Jie Han share first authorship.
Yu-Lu Fan and Wei-Jie Han: Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing - original draft; Yang Liu: Formal analysis, Methodology, Software, Writing - review & editing; Jian Hao: Conceptualization, Funding acquisition, Investigation, Project administration, Resources, Supervision, Writing - review & editing.
All authors gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (No. 82260146), Inner Mongolia Natural Science Foundation (No. 2022MS08036), the Program for Young Talents of Science and Technology in Universities of Inner Mongolia Autonomous Region (No. NJYT- 23-068), Medical and Health Science and Technology Plan of Health Commission of Inner Mongolia Autonomous Region (No. 202201253), and Inner Mongolia Medical University General Program (No. YKD2021MS034 and ZY20242126).
Disclosure
The authors declare that they have no competing interests.
References
1. Almaani S, Fussner LA, Brodsky S, Meara AS, Jayne D. ANCA-associated vasculitis: an update. J Clin Med. 2021;10(7):1446. doi:10.3390/jcm10071446
2. Konda R, Rajasekaran A, Rizk DV. Antineutrophil cytoplasmic antibody-associated vasculitis. Curr Opin Nephrol Hypertens. 2024;33(5):503–9. doi:10.1097/MNH.0000000000001004
3. Karadeniz H, Vaglio A. IgG4-related disease: a contemporary review. Turk J Med Sci. 2020;50(7):1616–1631. doi:10.3906/sag-2006-375
4. Lanzillotta M, Mancuso G, Della-Torre E. Advances in the diagnosis and management of IgG4 related disease. BMJ. 2020;369:m1067. doi:10.1136/bmj.m1067
5. Kitching AR, Anders H-J, Basu N, et al. ANCA-associated vasculitis. Nat Rev Dis Primers. 2020;6(1):71. doi:10.1038/s41572-020-0204-y
6. Wallace ZS, Naden RP, Chari S, et al. The 2019 American College of Rheumatology/European League against rheumatism classification criteria for IgG4-related disease. Arthritis Rheumatol. 2020;72(1):7–19. doi:10.1002/art.41120
7. Umehara H, Okazaki K, Kawa S, et al. The 2020 revised comprehensive diagnostic (RCD) criteria for IgG4-RD. Mod Rheumatol. 2021;31(3):529–533. doi:10.1080/14397595.2020.1859710
8. He R, Ma M, Luo P, Guo Q. An overlap of IgG4-related tubulointerstitial nephritis and microscopic polyangiitis-associated glomerulonephritis: a case-based review. Clin Rheumatol. 2023;42(5):1459–1467. doi:10.1007/s10067-022-06493-5
9. Danlos FX, Rossi GM, Blockmans D, et al. Antineutrophil cytoplasmic antibody-associated vasculitides and IgG4-related disease: a new overlap syndrome. Autoimmun Rev. 2017;16(10):1036–1043. doi:10.1016/j.autrev.2017.07.020
10. Galante JR, Daruwalla CP, Roberts ISD, Haynes R, Storey BC, Bottomley MJ. An unusual presentation of propylthiouracil-induced anti-MPO and PR3 positive ANCA vasculitis with associated anti-GBM antibodies, IgA nephropathy and an IgG4 interstitial infiltrate: a case report. BMC Nephrol. 2020;21(1):295. doi:10.1186/s12882-020-01964-w
11. Grayson PC, Ponte C, Suppiah R, et al. 2022 American College of Rheumatology/European Alliance of Associations for rheumatology classification criteria for eosinophilic granulomatosis with polyangiitis. Ann Rheum Dis. 2022;81(3):309–314. doi:10.1136/annrheumdis-2021-221794
12. Akiyama M, Alshehri W, Ishigaki S, Saito K, Kaneko Y. The immunological pathogenesis of IgG4-related disease categorized by clinical characteristics. Immunol Med. 2025;48(1):11–23. doi:10.1080/25785826.2024.2407224
13. Li ZY, Wang X, Xia X, et al. An overlap of antineutrophil cytoplasmic antibody (ANCA)-associated glomerulonephritis and IgG4-related kidney disease. Clin Chim Acta. 2020;501:12–19. doi:10.1016/j.cca.2019.11.030
14. Faz-Muñoz D, Hinojosa-Azaola A, Mejía-Vilet JM, et al. ANCA-associated vasculitis and IgG4-related disease overlap syndrome: a case report and literature review. Immunol Res. 2022;70(4):550–559. doi:10.1007/s12026-022-09279-8
15. Roberts IS, Cook HT, Troyanov S, et al. The Oxford classification of IgA nephropathy: pathology definitions, correlations, and reproducibility. Kidney Int. 2009;76(5):546–556. doi:10.1038/ki.2009.168
16. Bollée G, Noël LH, Suarez F, et al. Pauci-immune crescentic glomerulonephritis associated with ANCA of IgA class. Am J Kidney Dis. 2009;53(6):1063–1067. doi:10.1053/j.ajkd.2008.10.039
17. Haas M, Jafri J, Bartosh SM, Karp SL, Adler SG, Meehan SM. ANCA-associated crescentic glomerulonephritis with mesangial IgA deposits. Am J Kidney Dis. 2000;36(4):709–718. doi:10.1053/ajkd.2000.17615
18. Xie L, He J, Liu X, et al. Clinical value of systemic symptoms in IgA nephropathy with ANCA positivity. Clin Rheumatol. 2018;37(7):1953–1961. doi:10.1007/s10067-017-3931-z
19. Li W, Chen R, Chen W, Huang F, Xia X. Clinicopathological features and outcomes of IgA nephropathy with serum antineutrophil cytoplasmic autoantibody positivity. Am J Nephrol. 2023;54(9–10):416–424. doi:10.1159/000533982
20. Tota M, Donizy P, Byrska M, Krajewska M, Kusztal M. An unsuspected histopathological finding -concomitant IgA nephropathy in a patient with ANCA-associated vasculitis: a case report and literature review. Front Immunol. 2023;14:1227878. doi:10.3389/fimmu.2023.1227878
21. Haas M, Eustace JA. Immune complex deposits in ANCA-associated crescentic glomerulonephritis: a study of 126 cases. Kidney Int. 2004;65(6):2145–2152. doi:10.1111/j.1523-1755.2004.00632.x
22. Lin W, Shen C, Zhong Y, et al. Glomerular immune deposition in MPO-ANCA associated glomerulonephritis is associated with poor renal survival. Front Immunol. 2021;12:625672. doi:10.3389/fimmu.2021.625672
23. Kitazawa A, Koda R, Yoshino A, Ueda Y, Takeda T. An IgA1-lambda-type monoclonal immunoglobulin deposition disease associated with membranous features in a patient with IgG4-related kidney disease: a case report. BMC Nephrol. 2018;19(1):330. doi:10.1186/s12882-018-1133-9
24. Tian M, Luan J, Jiao C, Chang Q, Kopp JB, Zhou H. Co-occurrence of IgA nephropathy and IgG4-Tubulointersitial nephritis effectively treated with tacrolimus: a case report. BMC Nephrol. 2021;22(1):279. doi:10.1186/s12882-021-02477-w
25. Ito K, Yamada K, Mizushima I, et al. Henoch-Schönlein purpura nephritis in a patient with IgG4-related disease: a possible association. Clin Nephrol. 2013;79(03):246–252. doi:10.5414/CN107114
26. Al-Soudi A, Vegting Y, Klarenbeek PL, Hilhorst ML. Do relapses follow ANCA rises? A systematic review and meta-analysis on the value of serial anca level evaluation. Front Med. 2022;9:844112. doi:10.3389/fmed.2022.844112
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.