Back to Journals » Infection and Drug Resistance » Volume 10
Antimicrobial susceptibility profile, treatment outcome and serotype distribution of clinical isolates of Salmonella enterica subspecies enterica: a 2-year study from Kerala, South India
Authors Harichandran D, Dinesh KR
Received 31 October 2016
Accepted for publication 23 January 2017
Published 14 March 2017 Volume 2017:10 Pages 97—101
DOI https://doi.org/10.2147/IDR.S126209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Deepa Harichandran, Kavitha Radhakrishnan Dinesh
Department of Microbiology, Amrita School of Medicine, Amrita Institute of Medical Sciences and Research Centre, Amrita Vishwa Vidyapeetham University, Kochi, Kerala, India
Background/purpose: Typhoid and paratyphoid fever continue to be important causes of illness and death in parts of Asia, being associated with poor sanitation and consumption of unsafe food and water. Antimicrobial resistance has emerged to traditional first-line drugs, namely, the fluoroquinolones, as well as to third-generation cephalosporins, posing challenges to treatment. Azithromycin has proven to be an effective alternative for treatment of uncomplicated typhoid fever. The purpose of this study was to determine the antimicrobial susceptibility, clinical outcome and serotype distribution pattern of clinical isolates belonging to Salmonella enterica subspecies enterica.
Methodology: All clinical isolates of S. enterica obtained from blood, sterile body fluids, as well as stool and urine samples at Amrita Institute of Medical Sciences and Research Centre, Kerala, India, between August 2011 and July 2013 were included in the study and processed based on standard microbiology protocols.
Results: A total of 118 isolates of Salmonella were obtained during the study period. Out of these, 79 were of S. Typhi (66.95%), followed by isolates of S. Paratyphi A (22; 18.64%) and S. Typhimurium 12 (10.17%). Five isolates could not be identified further. There was 100% susceptibility to ceftriaxone in all S. enterica subspecies. Ciprofloxacin susceptibility was 32.91% for S. Typhi and 40.90% for S. Paratyphi A as determined by the disk diffusion method. The susceptibility profile of S. Typhi isolates to different antimicrobials was as follows: chloramphenicol (94.93%), ampicillin (77.21%), cotrimoxazole (75.94%) and azithromycin (78.48%). For S. Typhi, the minimum inhibitory concentration (MIC) of ciprofloxacin required to inhibit the growth of 50% of organisms was 0.5 μg/mL (intermediate) and MIC required to inhibit the growth of 90% of organisms was 1 μg/mL (resistant). S. Typhimurium was 100% susceptible to cotrimoxazole, ampicillin, ceftriaxone, chloramphenicol, ofloxacin and azithromycin. Susceptibility to ciprofloxacin was 66.66%. Patients from whom S. Typhimurium was isolated had comorbidities with documented risk. Of the 118 patients, 3 expired. Two had typhoid fever and were in sepsis at admission. One had S. Typhimurium and was suffering from multiple myeloma.
Conclusion: S. Typhi was the predominant isolate. All isolates were susceptible to ceftriaxone. Chloramphenicol susceptibility was >90%. No multidrug-resistant Salmonella strains were isolated. Susceptibility to ciprofloxacin for S. Typhi was 33%. Recovery rate was 97%.
Keywords: Salmonella enterica, susceptibility profile, clinical isolates
Introduction
Typhoid and paratyphoid fever continue to be important causes of illness and death, particularly among children and adolescents in South-Central and Southeast Asia. Enteric fever is associated with poor sanitation and unsafe food and water. Antimicrobial resistance has sequentially emerged to traditional first-line drugs, namely, the fluoroquinolones, as well as to third-generation cephalosporins, posing challenges to treatment. Azithromycin has proven to be an effective alternative for treatment of uncomplicated typhoid fever. The availability of full-genome sequences for S. enterica serovar Typhi and S. enterica serovar Paratyphi A confirms their place as monomorphic, human-adapted pathogens vulnerable to control measures if international efforts can be redoubled.1 Not all serovars of S. enterica subspecies enterica cause disease in humans, and only a small subset causes debilitating/life-threatening disease, the most well-known being serovars Typhi, Paratyphi A–C, Enteritidis, Typhimurium and Choleraesuis.2 The purpose of this work was to study the predominant Salmonella serotypes isolated at Amrita Institute of Medical Sciences, a tertiary care hospital in Kochi, Kerala, South India, over a 2-year period. With ciprofloxacin being the traditional drug of choice for enteric fever, difference in susceptibility results of ciprofloxacin and nalidixic acid was often noted while reporting Salmonella serotypes in our clinical laboratory. The knowledge that isolates that test sensitive to ciprofloxacin and resistant to nalidixic acid on routine disk diffusion tests may have decreased ciprofloxacin susceptibility, which may not be detected unless minimum inhibitory concentration (MIC) testing is performed, propelled us to check the MIC of ciprofloxacin. Literature search did not reveal much information on isolation of S. Typhimurium from patients; this prompted us to include S. Typhimurium isolates in our study.
Methodology
All clinical isolates of S. enterica obtained from blood, sterile body fluids as well as stool and urine samples from patients treated at the Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala, India, a tertiary care center, between August 2011 and July 2013 were included in the study. The study was approved by the Thesis Protocol Review Committee (Scientific, Ethical and Financial). Samples were collected after getting written informed consent from the subjects. Briefly, motile Gram-negative bacilli that were oxidase negative and catalase positive were subjected to preliminary identification in a VITEK 2 Compact (bioMerieux, SA, France) microbial identification system and manual biochemical reactions and subsequently confirmed using the slide agglutination test with Salmonella polyvalent O antiserum groups A–E and with type-specific S. Typhi O9 and H:d, S. Paratyphi A O2 and H:a, and S. Typhimurium O4 and H:i antisera sourced from the Central Research Institute, Kasauli, Himachal Pradesh, India. Our repertoire of antisera only allowed for the identification of three serovars and isolates that were positive for Salmonella polyvalent O group A–E agglutination but gave no agglutination with type-specific antisera were reported as Salmonella species. The typing scheme followed was Grimont and Weill’s Antigenic Formulae of the Salmonella Serovars, 9th Edition.3 Antibiotic susceptibility testing was performed by Kirby–Bauer disk diffusion method using commercial antibiotic disks (Hi Media Laboratories, Mumbai, Maharashtra, India). Susceptibility to cotrimoxazole, ampicillin, ciprofloxacin, nalidixic acid, ceftriaxone, chloramphenicol, ofloxacin and azithromycin was determined.4,5 Zone diameter interpretation was based on the 2013 guidelines of Clinical and Laboratory Standards Institute. Interpretive criteria for the disk diffusion test for ciprofloxacin were as follows: susceptible ≥31 mm, intermediate 21–30 mm and resistant ≤20 mm.5 The MICs (micrograms per milliliter) for ciprofloxacin (Sigma-Aldrich, Bangalore, Karnataka, India) were determined using the microbroth dilution technique. The MIC interpretive criteria used were as follows: MIC ≥1 μg/mL as resistant, MIC 0.12–0.5 μg/mL as intermediate and MIC ≤0.06 μg/mL as susceptible.5,6 Treatment outcomes of these patients were also recorded.
Results
During the study period, 118 isolates of Salmonella were obtained. Of these, 79 were of S. Typhi (66.95%), followed by those of S. Paratyphi A 22 (18.64%) and S. Typhimurium 12 (10.17%); 5 isolates could not be identified further (Table 1). S. enterica serotype distribution in clinical samples is depicted in Table 2. The total number of Salmonella samples isolated was 118. The majority (112, 94.91%) of isolates were from the blood, 4 (3.38%) from the stool, 1 (0.84%) from the urine and 1 (0.84%) from the synovial fluid. Moreover, 78 (98.7%) S. Typhi isolates were obtained from blood. All isolates of S. Paratyphi A (22, 100%) were also from blood. Of the 12 isolates of S. Typhimurium, 8 (66%) were also from blood culture. Of the Salmonella that could not be further identified, 4 (80%) were from blood and 1 (20%) was from synovial fluid.
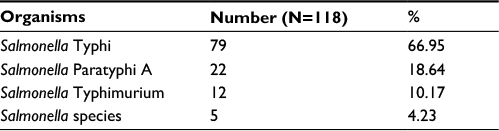 | Table 1 Isolation of Salmonella enterica subspecies enterica serotypes |
 | Table 2 Salmonella enterica serotype distribution in clinical samples (N=118) |
Percentage susceptibility results of the S. enterica isolates are presented in Table 3. The salient findings were as follows: there was 100% susceptibility to ceftriaxone in all S. enterica species. Ciprofloxacin susceptibility was 32.91% for S. Typhi and 40.90% for S. Paratyphi A as determined by the disk diffusion method. The susceptibility profile of S. Typhi isolates to antimicrobials was as follows: chloramphenicol 94.93%, ampicillin 77.21%, cotrimoxazole 75.94% and azithromycin 78.48%. Susceptibility pattern of the 22 isolates of S. Paratyphi A was as follows: 100% to ampicillin, 95.45% to cotrimoxazole, 90.90% for chloramphenicol, 81.81% to ofloxacin and 95.45% to azithromycin. S. Typhimurium was 100% susceptible to cotrimoxazole, ampicillin, ceftriaxone, chloramphenicol, ofloxacin and azithromycin. Susceptibility was 66.66% to ciprofloxacin. The MICs of all Salmonella isolates when considered together were as follows: MIC required to inhibit the growth of 50% of organisms (MIC50) =0.25 μg/mL and MIC90 =1 μg/mL. For S. Typhi alone, the values were MIC50 =0.5 μg/mL and MIC90 =1 μg/mL.
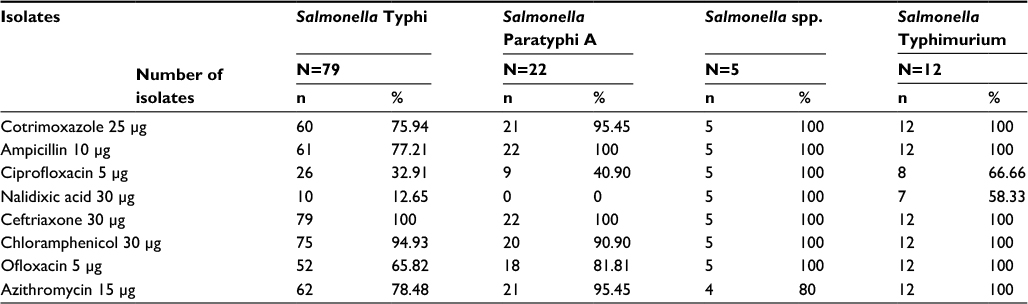 | Table 3 Percentage susceptibility of Salmonella enterica isolates (August 2011–July 2013) |
Treatment outcome
Data were available for 93 patients. All of them excluding three patients recovered. Ceftriaxone was the most common monotherapeutic agent used in 52/93 (55.91%) patients. Quinolones were used as monotherapy based on susceptibility results in 16/93 (17.2%) patients. One patient with typhoid fever was treated with azithromycin. Other agents used as monotherapy were cotrimoxazole in 1/93, cefoperazone–sulbactam in 1/93, piperacillin–tazobactam in 1/93 and amoxicillin–clavulanate in 1/93. Ten of the 12 patients in whom S. Typhimurium was detected had comorbidities with documented risk. Of the 118 patients, 3 expired. Among these, two patients had typhoid fever and were in sepsis at admission. One patient grew S. Typhimurium and was suffering from multiple myeloma.
Discussion
S. Typhi was the predominant isolate at 67%, 18% of isolates were of S. Paratyphi A and 10% were of S. Typhimurium. Isolation of S. Typhi as the most common serotype is similar to the results from other Indian studies from Chennai, Shimla, Chandigarh and New Delhi.7–11 Susceptibility of S. Typhi and S. Paratyphi A was 100% for ceftriaxone; similar susceptibility has been reported from Chennai.7 A study from Bengaluru has reported 97.50% susceptibility to ceftriaxone in S. Typhi and 100% in S. Paratyphi A.12 In our study, only 26/79 (32.9%) of S. Typhi were sensitive to ciprofloxacin. The percentage of nalidixic acid-resistant S. Typhi isolated was 87.43. The percentage of nalidixic acid-resistant S. Paratyphi A isolated was 100. A study from Chandigarh has also observed very high resistance to nalidixic acid (~86% in 2005 and 100% in 2012) and decreasing susceptibility to ciprofloxacin in S. Typhi.11
There have been many reports of multidrug-resistant (MDR) Salmonella resistant to ampicillin, trimethoprim–sulfamethoxazole and chloramphenicol in the Indian subcontinent, but we did not isolate any MDR during our study.1 A notable decline in MDR strains has been reported by Singhal et al11 in a 12-year study from Chandigarh in North India. Our observation of reemergence of susceptibility to chloramphenicol is comparable with studies by other Indian workers.7,11,13,14
S. Typhimurium was 100% susceptible to all antimicrobials tested; susceptibility to ciprofloxacin was 66.66%. Of the 12 S. Typhimurium strains isolated during the study period, 4 were from stool and 8 from blood stream; moreover, 9 patients had 3 or more comorbidities. Several comorbidities have been reported in patients with nontyphoidal salmonellosis, including malignancy, diabetes and treatment with immunotherapy agents.15,16
The lone urinary carrier of S. Typhi was a male with no history of enteric fever. He had bilateral renal calculi, obstructive uropathy, peripheral neuropathy and end-stage kidney disease. S. Typhi bacteriuria has been documented in patients with renal calculi and also in those with urinary tract abnormalities.17 The two patients who expired due to typhoid fever were septicemic; their blood cultures were positive for S. Typhi. One died a few hours after admission, and the other – despite intensive management and treatment with ceftriaxone – passed away within 48 hours of admission. On administration of appropriate antibiotic therapy in a prompt manner, typhoid fever is a short-term febrile illness with about 6 days of hospitalization. The risk of mortality is 0.2%.18 The third patient who expired grew S. Typhimurium. He was immunocompromised, suffering from multiple myeloma with renal failure and was on chemoradiation. The severity of nontyphoidal salmonellosis depends on host factors and the strain of Salmonella.18
Five isolates belonging to the genus Salmonella could not be identified further. The lack of antisera for other Salmonella serotypes and nonavailability of molecular methods for confirmatory identification were limitations of the study.
Conclusion
S. Typhi was the predominant isolate. This was followed by S. Paratyphi A. Ceftriaxone was the common monotherapeutic agent used in our hospital. All isolates of Salmonella were susceptible to ceftriaxone. Chloramphenicol susceptibility was >90%. No MDR Salmonella strains were isolated. Susceptibilty of S. Typhi to ciprofloxacin was 33%. Furthermore, 97% of patients recovered. A urinary carrier of S. Typhi was detected during the study period. There were 17 cases of nontyphoidal salmonellosis.
Acknowledgment
We gratefully acknowledge the cooperation of all the faculty members and technical staff of Department of Microbiology, Amrita School of Medicine, Kochi, India.
Disclosure
The authors report no conflicts of interest in this work.
References
Hohmann EL [homepage on the Internet]. Treatment and prevention of typhoid fever; 2016. Available from: http://www.uptodate.com. Accessed October 11, 2016. | ||
Washington CW, Stephen DA, William MJ. Koneman’s Colour Atlas and Textbook of Diagnostic Microbiology. 6th ed. Philadelphia, PA: Lippincott Williams and Wilkins; 2006. | ||
Grimont PAD, Weill F-X. Antigenic Formulae of the Salmonella serovars. WHO Collaborating Centre for Reference and Research on Salmonella. 9th ed. Paris, France: Institut Pasteur; 2007. | ||
Miles RS, Amyes SGB. Laboratory control of antimicrobial therapy. In: Collee JG, Fraser AG, Marmion BP, Simmons A, editors. Mackie & McCartney Practical Medical Microbiology. 14th ed. New Delhi: Churchill Livingstone; 2006:154–158. | ||
Clinical and Laboratory Standards Institute (CLSI) 2013. Performance Standards for Antimicrobial Susceptibility Testing; Twenty Third Informational Supplement, M100-S23. Wayne, PA: CLSI; 2013. | ||
Clinical and Laboratory Standards Institute. Methods for Dilution Antimicrobial Susceptibility Test for Bacteria that Grow Aerobically. Approved Standard M7-A8. Wayne PA: CLSI; 2009. | ||
Choudhary A, Gopalakrishnan R, Nambi PS, Ramasubramanian V, Ghafur KA, Thirunarayan MA. Antimicrobial susceptibility of Salmonella enterica serovars in a tertiary care hospital in southern India. Indian J Med Res. 2013;137(4):800–802. | ||
Verma S, Thakur S, Kanga A, Singh G, Gupta P. Emerging Salmonella paratyphi A enteric fever and changing trends in antimicrobial resistance pattern of Salmonella in Shimla. Indian J Med Microbiol. 2010;28(1):51–53. | ||
Manchanda V, Bhalla P, Sethi M, Sharma VK. Treatment of enteric fever in children on the basis of current trends of antimicrobial susceptibility of Salmonella enterica serovar typhi and paratyphi A. Indian J Med Microbiol. 2006;24(2):101–106. | ||
Mohanty S, Renuka K, Sood S, Das BK, Kapil A. Antibiogram pattern and seasonality of Salmonella serotypes in a North Indian tertiary care hospital. Epidemiol Infect. 2006;134(5):961–966. Epub 2006 Feb 14. | ||
Singhal L, Gupta PK, Kale P, Gautam V, Ray P. Trends in antimicrobial susceptibility of Salmonella Typhi from North India (2001–2012). Indian J Med Microbiol. 2014;32(2):149–152. | ||
Nagshetty K, Channappa ST, Gaddad SM. Antimicrobial susceptibility of Salmonella Typhi in India. J Infect Dev Ctries. 2010;4(2):70–73. | ||
Rudresh SM, Nagarathnamma T. Antibiotic susceptibility pattern of Salmonella enterica serovar typhi and Salmonella enterica serovar paratyphi A with special reference to quinolone resistance. Drug Dev Ther. 2015;6:70–73. | ||
Rai S, Jain S, Prasad KN, Ghoshal U, Dhole TN. Rationale of azithromycin prescribing practices for enteric fever in India. Indian J Med Microbiol. 2012;30(1):30–33. | ||
Acheson D, Hohmann EL. Nontyphoidal salmonellosis. Clin Infect Dis. 2001;32(2):263–269. | ||
WHO [webpage on the Internet]. WHO Fact sheet NO. 139. Salmonella (non-typhoidal). World Health Organisation; 2013 [cited October 17, 2016]. Available from: http://www.who.int/mediacentre/factsheets/fs139/en/. Accessed October 17, 2016. | ||
Değirmenci T, Arı A, Kozacıoğlu Z, Örs B, Günlüsoy B. Salmonella Typhi isolated from urine culture before percutaneous nephrolithotomy. Urol J. 2014;11(01):1350–1352. | ||
Lynch MF, Blanton EM, Bulens S, et al. Typhoid fever in the United States, 1999–2006. JAMA. 2009;302(8):859–865. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.