Back to Journals » Infection and Drug Resistance » Volume 16
Antimicrobial Resistance Patterns of Staphylococcus aureus and Enterococcus Species at the Ethiopian Public Health Institute, Ethiopia: A Five-Year Retrospective Analysis
Authors Abdeta A ![]() , Beyene D, Negeri AA
, Beyene D, Negeri AA
Received 10 July 2023
Accepted for publication 8 September 2023
Published 13 September 2023 Volume 2023:16 Pages 6155—6166
DOI https://doi.org/10.2147/IDR.S429687
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Abera Abdeta, Degefu Beyene, Abebe Aseffa Negeri
National Clinical Bacteriology and Mycology Reference Laboratory, Ethiopian Public Health Institute, Addis Ababa, Ethiopia
Correspondence: Abera Abdeta, Tel +251911566420, Email [email protected]
Purpose: The study aimed to investigate the antimicrobial resistance patterns of Staphylococcus aureus and Enterococcus species isolated from clinical specimens over a period of five years, including resistance to methicillin and vancomycin.
Patients and Methods: Bacterial identification and antimicrobial susceptibility testing reports from 2017 to 2021 at the Ethiopian Public Health Institute were used for this retrospective study. The organisms were identified using either BD Phoenix M50, Vitek 2 compact, or conventional biochemical methods, whichever was available at the time of testing. The antimicrobial susceptibility profiles of the isolates were determined using either Kirby-Bauer disc diffusion, BD phoenix M50, or Vitek 2 compact. WHONET software was used to analyze the antimicrobial resistance patterns of both organisms. The p-values of ≤ 0.05 were considered statistically significant.
Results: During the study period, a total of 315 Staphylococcus aureus and 92 Enterococcus species were isolated. Out of 315 Staphylococcus aureus isolates, 27% and 5.1% were methicillin and vancomycin resistant, respectively. Staphylococcus aureus showed very high resistance to Penicillin G (86.7%). Out of 92 Enterococcus species recovered, 8.7% were vancomycin-resistant. Enterococcus species showed very high resistance to Penicillin G (71.4%) and tetracyclines (83.3%). Methicillin-resistant Staphylococcus aureus shows 100% resistance to penicillin followed by ciprofloxacin (50%), erythromycin (45.6%), and tetracycline (44.2%) and lower resistance to vancomycin (18.8%). All vancomycin-resistant isolates of both organisms were fully resistant (100%) to all antibiotics tested, except for linezolid and daptomycin, to which they were susceptible.
Conclusion: This study found a high prevalence of methicillin and vancomycin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus species between 2017 and 2021. However, there were no statistically significant changes in the prevalence of these organisms during the study period. This suggests that larger and more representative nationwide data is needed to show trends of these pathogens.
Keywords: antimicrobial resistance, Staphylococcus aureus, Enterococcus species, Ethiopia
Introduction
Staphylococcus aureus and Enterococcus species are both types of Gram-positive bacteria that can cause infections in humans.1,2 They have been identified by the World Health Organization (WHO) as emerging causes of nosocomial infections in recent decades, posing a significant threat to public health.3 Staphylococcus aureus is a Gram-positive, catalase, and coagulase-positive facultative anaerobic bacteria that colonizes up to 30% of the human population.4 However, certain groups, such as healthcare workers, hospitalized patients, intravenous drug users, and individuals with compromised immune systems, have higher rates of colonization (up to 80%).2 Staphylococcus aureus causes infection only if it manages to enter the bloodstream or internal tissues.5 It is a major cause of healthcare-associated infections, including bloodstream infections, surgical site infections, and pneumonia. Additionally, it can also cause community-acquired infections, such as skin and soft tissue infections and sepsis.2,6,7
Enterococci are a type of Gram-positive, facultative anaerobic bacteria that form short and medium chains of cocci that are commonly found in the gastrointestinal tract of humans and animals.1 Enterococcus faecalis and Enterococcus faecium are the most common species that cause infections in humans, and they are often associated with healthcare-associated infections, such as urinary tract infections, endocarditis, bloodstream infections, and surgical site infections.1,8,9 Enterococci are intrinsically resistant to cephalosporins, clindamycin, aminoglycosides, and trimethoprim-sulfamethoxazole.10 In addition, there have been reports of Staphylococcus aureus strains that are resistant to both methicillin (MRSA) and vancomycin (VRSA), as well as Enterococcus species that are resistant to vancomycin (VRE). This can make treatment more difficult and raise the likelihood of mortality.7,9,11 Vancomycin is primarily used to treat infections caused by MRSA and those who are allergic to semisynthetic penicillin and cephalosporins.12
In recent years, the prevalence of antimicrobial resistance among these organisms has increased significantly, highlighting the need for ongoing surveillance of their resistance patterns.13–17 A systematic analysis conducted in 2019 estimated Staphylococcus aureus is among the six leading pathogens for death-associated resistance. Particularly, Methicillin-resistant Staphylococcus aureus caused more than 100,000 deaths attributable to antimicrobial resistance. The study also reported that the Enterococcus species was responsible for between 100,000 and 250,000 deaths associated with antimicrobial resistance.18 Some studies have been conducted in Ethiopia to assess the antimicrobial resistance patterns of Staphylococcus aureus and Enterococcus species, but these studies are limited in scope, as they only analyzed a smaller number of isolates from specific geographic locations within the country. Therefore, this study aimed to determine the five-year antimicrobial resistance patterns of Staphylococcus aureus and Enterococcus species isolated from clinical specimens referred from various health facilities to the Ethiopian Public Health Institute. The findings can provide valuable insights into these bacteria’s distribution and resistance patterns in the country. Moreover, this study’s results can guide the appropriate use of antimicrobial agents in the treatment of infections caused by these bacterial pathogens, leading to better patient outcomes and reduced healthcare expenses.
Materials and Methods
Study Design and Data Extraction
In this retrospective study, we analyzed the antimicrobial resistance profiles of Staphylococcus aureus and Enterococcus species isolated from clinical specimens referred to the National Clinical Bacteriology and Mycology Reference Laboratory, Ethiopian Public Health Institute between January 1, 2017, and December 31, 2021. The laboratory was accredited by the Ethiopian Accreditation Service in 2017 for meeting the requirements of the International Organization for Standardization (ISO) 15,189: 2012. All Staphylococcus aureus and Enterococcus species isolated from all specimens with complete information were included. Identification and antimicrobial susceptibility testing results of both Staphylococcus aureus and Enterococcus species data were extracted from the bacteriology result logbook, BD Phoenix M50, and Vitek 2 compact instruments. Data from BD Phoenix M50 and Vitek 2 compact instruments were converted to a WHONET SQLite file using the WHONET backlink for analyzing the antimicrobial susceptibility pattern of Staphylococcus aureus and Enterococcus species.
Specimen Processing, Bacterial Isolation, and Identification
Specimens were sent from different healthcare facilities across the country. The specimens obtained encompassed various types of specimens, including urine, blood, wound, eye, body fluids, and other miscellaneous specimens. Only those samples that met the laboratory’s acceptance criteria were accepted and then inoculated into suitable culture media, after which they were incubated at the proper temperature and duration. Staphylococcus aureus and Enterococcus species were identified using one of the three methods: VITEK® 2 Compact (bioMérieux, France), BD phoenix M50 (Becton, Dickinson, USA), or conventional biochemical tests. Conventional biochemical tests involved macroscopic colony characterization (color, size, shape, texture, hemolysis), Gram staining, and biochemical tests (catalase test, coagulase test, L-Pyrrolidonyl Arylamidase (PYR), bile esculin agar, 6.5% sodium chloride tolerance test).
Antimicrobial Susceptibility Testing
The antimicrobial susceptibility of Staphylococcus aureus and Enterococcus species to antimicrobial agents was tested using either the BD Phoenix M50 or Vitek 2 compact systems, or the Kirby-Bauer disk diffusion method, whichever was available at the time of testing. The results were interpreted using the latest Clinical and Laboratory Standards Institute (CLSI) M100 guideline.10 The antimicrobial disks were obtained from the following manufacturers: (Oxoid Ltd., Basingstoke, Hampshire, England), (Liofilchem, Roseto degli Abruzzi, Italy), (Abtek, Liverpool, United Kingdom), and (Hardy Diagnostics, Santa Maria, California, and Springboro, Ohio, United States).
For Staphylococcus aureus, the antimicrobial agents tested and reported were as follows: Penicillin G (10 units), cefoxitin (30µg), gentamycin (10µg), ciprofloxacin (5µg), trimethoprim/sulfamethoxazole (1.25/23.75µg), clindamycin (2µg), erythromycin (30µg), linezolid (30µg), chloramphenicol (30µg), tetracycline (30µg) and Nitrofurantoin (300µg). For Enterococcus species, the following antimicrobial agents were tested and reported: Penicillin G (10 units), ampicillin (10µg), ciprofloxacin (5µg), erythromycin (30µg), linezolid (30µg), chloramphenicol (30µg), tetracycline (30µg), nitrofurantoin (300µg), and vancomycin (30µg).
Additionally, daptomycin and vancomycin susceptibility in Staphylococcus aureus and daptomycin susceptibility in Enterococcus were tested using the VITEK® 2 Compact, BD phoenix M50 systems, and vancomycin Etest (bioMérieux, France). This was necessary because disk diffusion testing of these antibiotics for these organisms is not reliable. To screen for oxacillin or methicillin-resistant Staphylococcus aureus (MRSA), a cefoxitin disk was used as a surrogate agent for oxacillin. A zone diameter of ≥22 mm was considered to be susceptible to oxacillin, while a zone diameter of ≤21 mm was considered to be resistant to oxacillin. Nitrocefin and zone edge tests were used to screen for β-lactamases in Staphylococcus aureus strains with a penicillin zone diameter of ≥29mm before reporting them as susceptible. Sharp zone edge (cliff) was considered β-lactamase positive indicating resistance to penicillin, and fuzzy zone edge (beach) was considered β-lactamase negative indicating susceptibility to penicillin.
Quality Assurance
The quality of the culture media used was checked as per CLSI M22-A3 guidelines,19 laboratories standard operating procedures, and manufacturers’ recommendations for each culture media. American-type culture collection (ATCC) strains, Escherichia coli ATCC 25922, Pseudomonas aeruginosa ATCC 27853, and Staphylococcus aureus ATCC 25923 were used to check the quality of all the antimicrobial disks used as per clinical and laboratory standards institute (CLSI) M100 Table 4A 1–2. A 15-day replicate (3x5) plan was used to check the quality of newly bought antimicrobial agents using the ATCC strains mentioned above. Once satisfactory results were obtained from daily quality controls, the quality control testing frequency was switched to weekly testing on Tuesdays of each week.
Data Analysis
The data was regularly entered into the WHONET software. The data completeness was checked using the WHONET standard report feature, and data with incomplete information were removed from the dataset. The overall antimicrobial susceptibility profile of Staphylococcus aureus and Enterococcus species to the abovementioned antimicrobial agent was analyzed to calculate the proportion of isolates resistant to different antimicrobial agents using resistance, intermediate, and susceptible (RIS) analysis type from WHONET software. Additionally, oxacillin and vancomycin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus species were selected to analyze their susceptibility profile to other antimicrobial agents. The distribution of the bacterial isolates by health facility and ward was also analyzed.
Ethical Considerations
The institutional review board (IRB) of the Ethiopian Public Health Institute (EPHI) approved this study and waived the need for informed consent because the study was retrospective and did not involve any intervention or interaction with patients. The study was assigned the IRB approval number EPHI-IRB-413-2021. Patient confidentiality was maintained by using de-identified data in the analysis. Hence, the study was conducted following the Declaration of Helsinki.
Results
Between 2017 and 2021, a total of 7110 clinical specimens were received at the National Clinical Bacteriology and Mycology Reference Laboratory of the Ethiopian Public Health Institute, after excluding 89 records due to missing information. Of these specimens, 315 Staphylococcus aureus and 92 Enterococcus species isolates were recovered. Of the 315 Staphylococcus aureus isolates, 27% were methicillin-resistant and 5.1% were vancomycin-resistant. Additionally, out of 92 Enterococcus species, 8.7% were vancomycin-resistant (Figure 1).
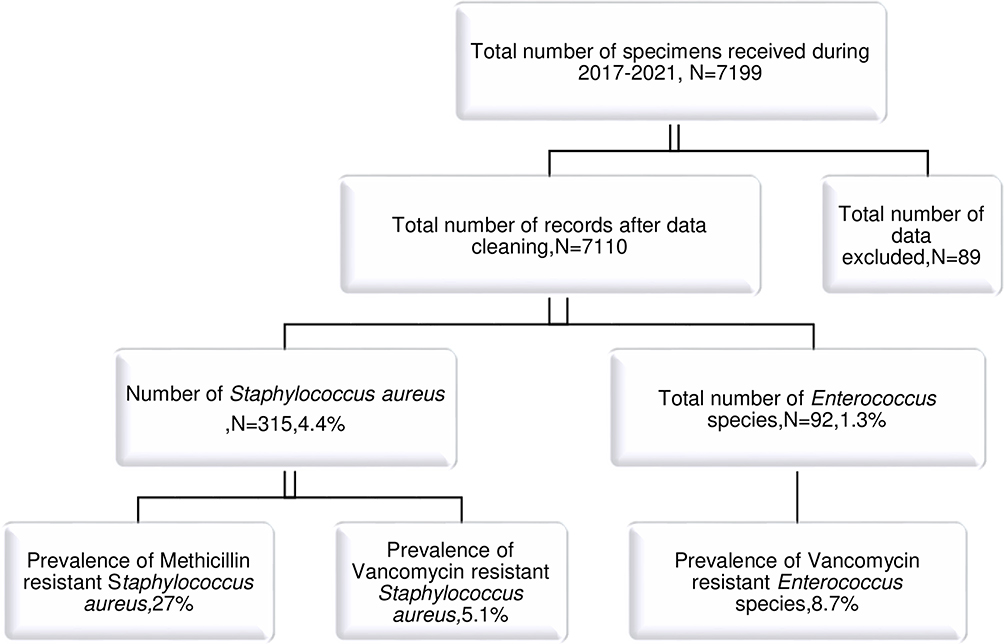 |
Figure 1 Flowchart of the data cleaning process. Abbreviation: N, number. |
Socio-Demographic Characteristics of the Patients
Table 1 summarizes the demographic characteristics of patients and the number of Staphylococcus aureus and Enterococcus species isolates obtained based on age, sex, healthcare facilities, different wards, and specimen source. Out of 407 isolates 246 and 161 were recovered from specimens obtained from males and females, respectively. The age group of 21 to 30 had 94 isolates recovered from their specimens. The majority of isolates were isolated from specimens referred from AaBET Hospital (187, representing 46% of the total). The specimens collected from patients admitted to orthopedics (102) and surgery (93) wards had the highest number of isolates, with 170 of them being Staphylococcus aureus, which represents about 87% of the total. Wound specimens had the highest number of isolates (259), with 248 of them being Staphylococcus aureus, representing 96% of the total.
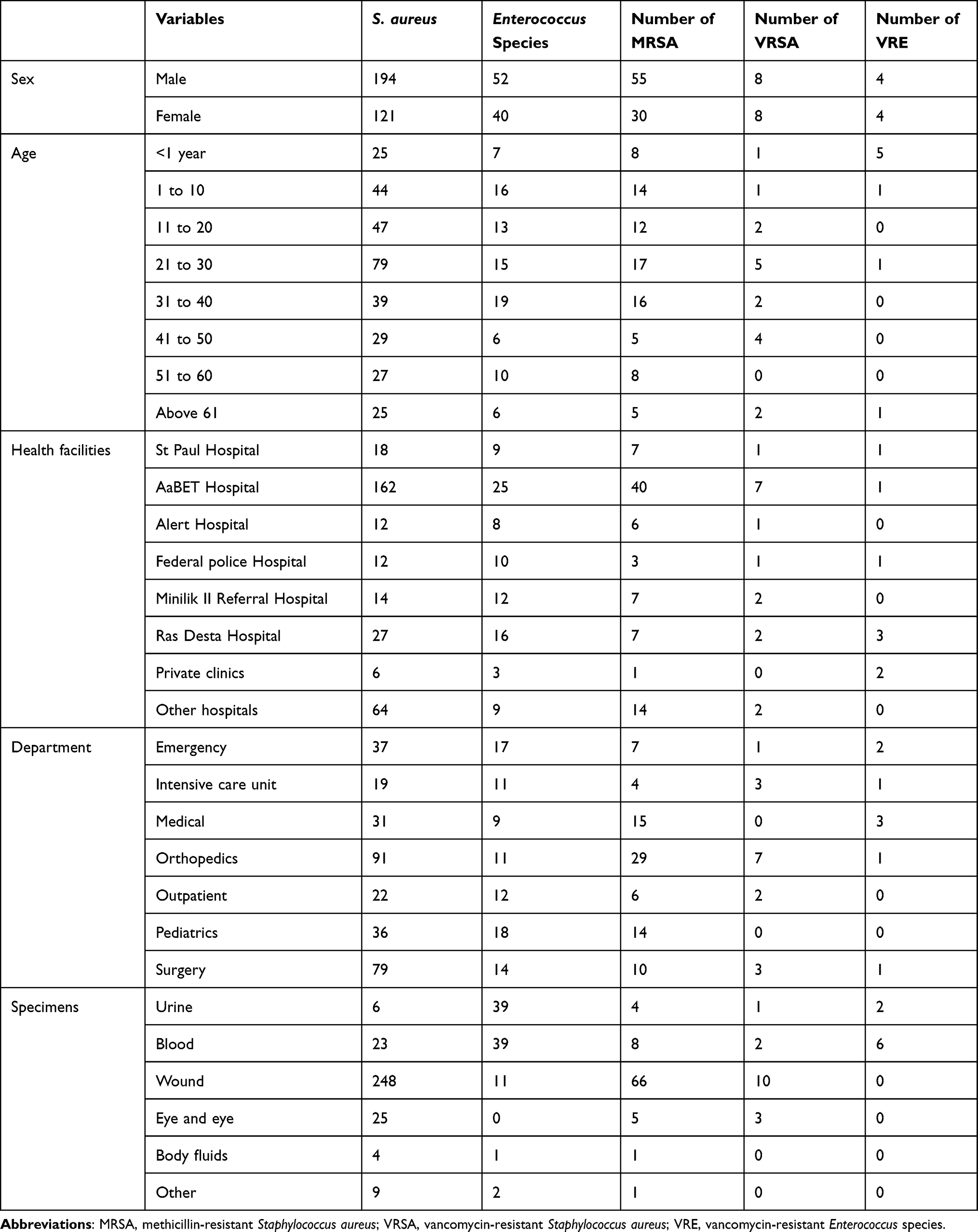 |
Table 1 Socio-Demographic Characteristics of Patients from Which Specimens Were Obtained from 2017–2021 |
Antimicrobial Susceptibility Profile
The antimicrobial susceptibility profile of Staphylococcus aureus and Enterococcus species is shown in Table 2. Out of 315 Staphylococcus aureus isolates, 85 (representing 27% of the total) and 16 (representing 5.1% of the total) were methicillin and vancomycin-resistant, respectively. Staphylococcus aureus showed very high resistance to Penicillin G (86.7%), tetracyclines (35.9%), and chloramphenicol (44.4%). The resistance rates to gentamicin and clindamycin were low at 10.3% and 10.6%, respectively. Of the 92 Enterococcus species, 8 (representing 8.7% of the total) were vancomycin-resistant. These isolates showed very high resistance to Penicillin G (71.4%), tetracyclines (83.3%), ciprofloxacin (71.9%), and erythromycin (54.5%), and lower resistance to nitrofurantoin (8%), and chloramphenicol (25%). All isolates of Staphylococcus aureus and Enterococcus species were susceptible to daptomycin and linezolid.
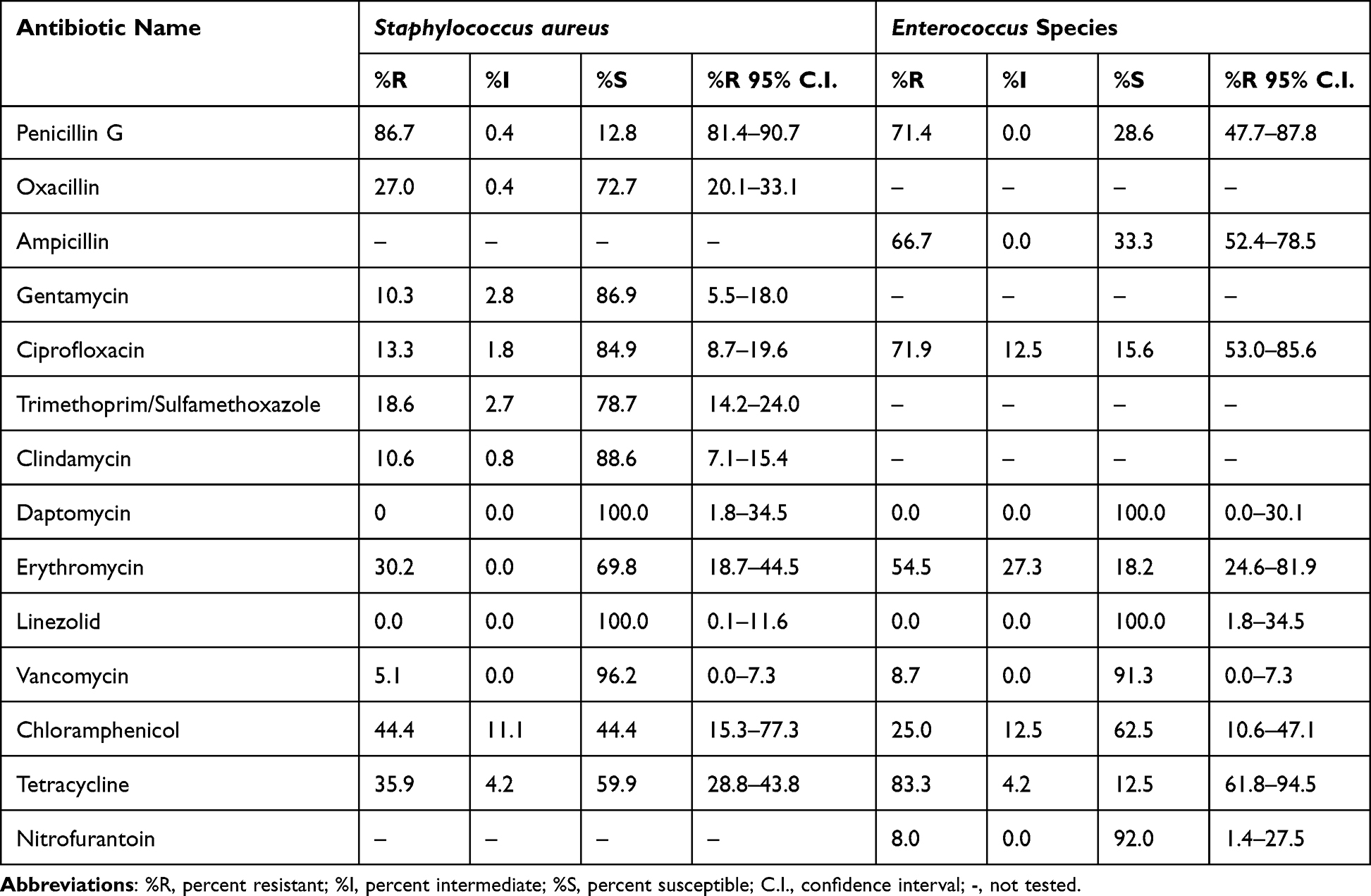 |
Table 2 Antimicrobial Susceptibility Profile of Staphylococcus aureus and Enterococcus Species |
Antimicrobial Susceptibility Profile of MRSA, VRSA, and VRE
The antimicrobial susceptibility profile of methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant Staphylococcus aureus (VRSA) and vancomycin-resistant Enterococcus species (VRE) is shown in Table 3. All of the 85 Staphylococcus aureus isolates that were resistant to methicillin also demonstrated resistance to penicillin. However, about 50%, 45.6%, and 44.2% of these isolates were found to be resistant to ciprofloxacin, erythromycin, and tetracycline, respectively. In contrast, the resistance level to vancomycin was lower, at 18.8%. Both vancomycin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus species demonstrated complete resistance to all tested antibiotics, but they exhibited no resistance to linezolid and daptomycin.
 |
Table 3 Antimicrobial Susceptibility Profile of MRSA, VRSA, and VRE |
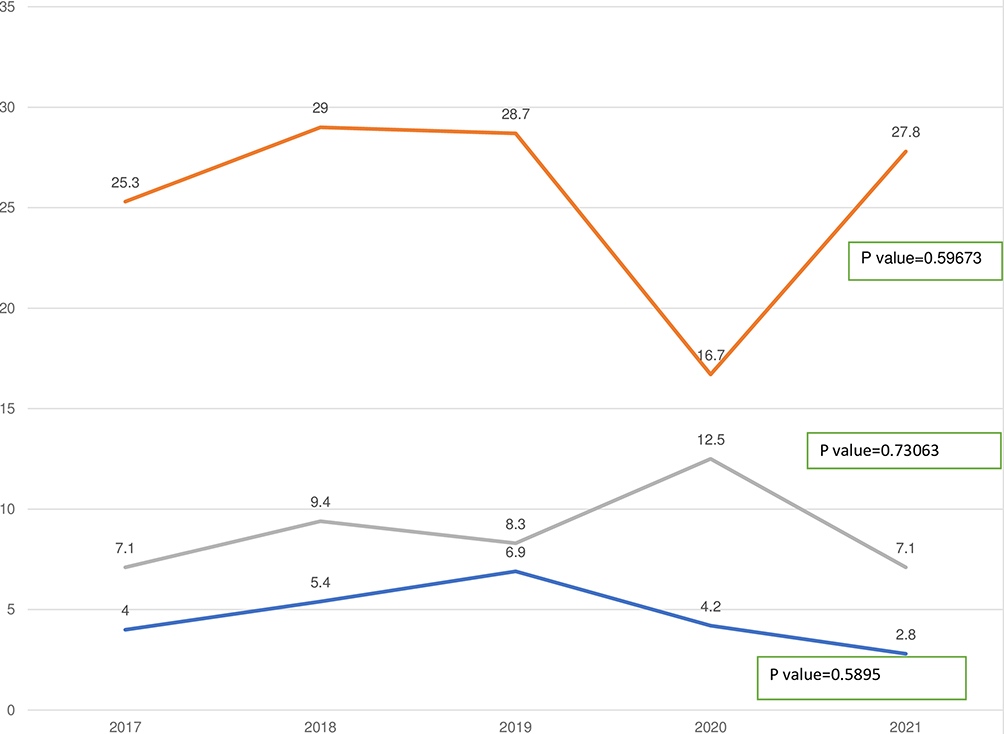
Figure 2 shows five trends in the prevalence of methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Staphylococcus aureus (VRSA), and vancomycin-resistant Enterococcus. The prevalence of methicillin-resistant Staphylococcus aureus (MRSA) was 25.3% in 2017. It increased to 29% and 28.7% in 2018 and 2019, respectively. However, it decreased to 16.7% in 2020 and then increased again to 27.8% in 2021 (p-value 0.59673). The prevalence of vancomycin-resistant Staphylococcus aureus (VRSA) was 4% in 2017. It increased slightly to 5.4%, 6.9%, and 4.2% in 2018, 2019, and 2020, respectively. However, it decreased to 2.8% in 2021 (p-value 0.5895). The prevalence of vancomycin-resistant Enterococcus species was 7.1% in 2017. It increased to 9.4%, 8.3%, and 12.5% in 2018, 2019, and 2020, respectively. It then slightly decreased back to 7.1% in 2021 (p-value 0.73063).



Discussion
In this retrospective study, we analyzed the five-year antimicrobial resistance patterns of Staphylococcus aureus and Enterococcus species isolated from clinical specimens with a special focus on methicillin and vancomycin resistance. In the present study, the highest proportion of Staphylococcus aureus, accounting for 78.7%, was obtained from wound samples. Among these isolates, 26.6% were identified as MRSA (Methicillin-Resistant Staphylococcus aureus), while 4.0% were identified as VRSA (Vancomycin-Resistant Staphylococcus aureus). These findings are consistent with the results reported in previous studies conducted at Asmara, Eritrea,20 Jimma University, Ethiopia,21 Yekatit 12 Hospital Medical College, Ethiopia,22 and Karl Referral Hospital, Ethiopia.23 The majority (84.8%) of Enterococcus isolates were obtained from blood and urine samples, of which 10.3% were identified as VRE (Vancomycin-Resistant Enterococcus). These results align with a study conducted at the University of Gondar24 and Felege Hiwot Hospital, Ethiopia,25 which reported similar findings.
In this study, the prevalence of methicillin-resistant Staphylococcus aureus was 27%, which is almost similar to the findings from Referral Hospital, Northeast Ethiopia (28.3%),26 a meta-analysis conducted in Ethiopia (32.5%).15 However, the prevalence was higher than that reported in other studies, such as Mettu Karl Referral Hospital, Ethiopia (18.8%),23 Yekatit 12 Hospital, Addis Ababa, Ethiopia (17.5%),22 Mekelle, Northern Ethiopia (2.4%),27 and Debre Markos Referral Hospital, Ethiopia (13.22%).28 Conversely, the prevalence was lower than that reported in other studies, such as Tikur Anbessa Specialized Hospital, Addis Ababa, Ethiopia (35.6%),29 Debre Markos Referral Hospital, Ethiopia (49.7%),30 Arba Minch Hospital, South Ethiopia (82.3%),31 Jimma University Specialized Hospital, Ethiopia (76.7%),21 A Multicenter Study in Asmara, Eritrea (72%),20 and a systematic review and meta-analysis in low- and lower-middle-income countries (48.4%),32 and northwest, Iran (53.7%),33 a meta-analysis, Ethiopia (47%).33 These observed differences in MRSA prevalence could be attributed to factors such as differences in study design, geographic location, sample sizes, patient populations, laboratory methods, and use of antibiotics.
In the current study, the prevalence of vancomycin resistant Staphylococcus aureus was 5.1%, which is in agreement with study from Debre Markos Referral Hospital, Ethiopia (4.1%), and28 the pooled global prevalence of 6% reported between 2000 and 2019,14 a meta-analysis, Ethiopia (5.3%),15 but lower than the prevalence reported in another meta-analysis from Ethiopia (11%).16 However, the prevalence was higher than the pooled global prevalence of VRSA 1.5%,34 and the pooled prevalence in low- and middle-income countries (0.6%).32 The different results of the studies could be due to differences in how the studies were designed, the types of samples that were used, the locations where the studies were conducted, and the policies regarding antibiotic prescription.
The prevalence of vancomycin-resistant Enterococcus species in this study was 8.7%. This is similar to the prevalence rates found in Asia (8.1%),35 Addis Ababa, Ethiopia (6.7%),36 and the SENTRY antimicrobial surveillance program (8%).37 However, it was lower than the studies from Nigeria (26.5%),38 Iran (14%),39 Egypt (26%),40 and Ethiopia (14.8%).41 Our finding was also much lower than the prevalence rates reported from Bahir Dar, Ethiopia (34.61%),25 and Gondar, Ethiopia (41.7%).24 The variation in the prevalence rates could be due to a number of factors, such as the study design, the types of samples collected, the timing of the study, differences in antibiotic prescription policies, differences in geographical locations, and other potential factors. Vancomycin is a powerful antibiotic that is used to treat infections caused by antibiotic-resistant Staphylococcus aureus and Enterococcus species with better clinical outcomes. It is important to use vancomycin wisely, as it is one of the last lines of defense against these infections. It serves as a crucial treatment option in the management of such infections, offering a reliable treatment alternative when other antibiotics fail.42–44
In the current study, methicillin-resistant Staphylococcus aureus (MRSA) showed no resistance to linezolid and daptomycin, but 18.8% resistance to vancomycin. Most studies reported zero resistance rates of MRSA to vancomycin, linezolid, and daptomycin. For instance, a study from India reported 0% resistance rates of MRSA to vancomycin,45 and North India, reported 0% resistance rates of MRSA to vancomycin and linezolid,46 Eastern India, reported 0% resistance of MRSA to vancomycin, daptomycin and linezolid,47 pooled result from Ethiopia, reported 5.3% rates of resistance to vancomycin,15 and Nairobi, Kenya, less than 5% resistance rates of MRSA to linezolid and vancomycin.48
Vancomycin has long been considered the last-resort treatment for MRSA infections and resistance to vancomycin is mediated by a vanA gene, which is transferred from vancomycin-resistant Enterococcus.34 There are multiple factors that can be directly or indirectly associated with the increasing burden of infections caused by MRSA, VRSA, and VRE strains and one of them is Excessive use of vancomycin resulted in the emergence of vancomycin-resistant Staphylococcus aureus (VRSA). These strains, in turn, lead to escalated expenses within healthcare facilities, prolonged hospital stays, heightened morbidity rates, and increased mortality rates.14,34
In the current study, all 16 vancomycin-resistant Staphylococcus aureus (VRSA) strains were susceptible to daptomycin and linezolid. This is consistent with the findings of other studies, including a review of VRSA cases that reported that VRSA were susceptible to daptomycin and linezolid,11 results of the Network on Antimicrobial Resistance in S. aureus (NARSA) Program which reported that >90% of 13 VRSA isolates were susceptible to daptomycin and linezolid,49 and a study from the United States that found that 7 out of 7 VRSA isolates were susceptible to linezolid and 6 out of 7 were susceptible to daptomycin.50
Similarly, all 8 vancomycin-resistant Enterococcus species (VRE) were susceptible to daptomycin and linezolid, which agrees with findings of the study from Ethiopia, which reported very low resistance of VRE to daptomycin and linezolid with a pooled estimate of 3.2% and 9.9%, respectively,41 and a study from Egypt between 2010 and 2022 which reported VRE resistance rate of 5.54% to linezolid.40 This is because vancomycin-resistant Staphylococcus aureus (VRSA) and vancomycin-resistant Enterococci (VRE) strains are resistant to vancomycin due to the acquisition of the vanA gene from vancomycin-resistant Enterococci (VRE). This gene encodes a modified peptidoglycan precursor that has a lower affinity for vancomycin, making the bacteria resistant to this particular antibiotic.11,35 Linezolid and daptomycin, on the other hand, have different mechanisms of action and are not affected by the modified peptidoglycan precursor. Linezolid and daptomycin target different components of the bacterial cell, hence they are effective against VRSA and VRE strains.9,33,49
The present study showed that from 2017 to 2021, the prevalence of MRSA fluctuated, which contradicts the findings of a study from the United States from 2010 to 2014 that reported decreasing rates of MRSA infections among hospitalized patients.51 It also contradicts the findings of a nationwide surveillance study (2008–2021) that reported decreasing MRSA infections.52 The study also found that the prevalence of VRSA was fluctuated, which contradicts the findings of a global pooled result of a systematic review and meta-analysis between 1997 and 2019 that reported an increase in the prevalence of VRSA from 1.2% before 2010 to 2.4% after 2010.34 Likewise, the study also found that the prevalence of VRE was fluctuated, which contradicts the findings of a three-year prospective study from India that reported increasing trends of VRE53 and the pooled results from the European Region Surveillance Network that reported decreasing trends of VRE.54 The varying trends observed in methicillin and vancomycin-resistant Staphylococcus aureus, and vancomycin Enterococcus species may be explained by the low number of each strains isolated between 2017 and 2021 at the Ethiopian Public Health Institute.
Limitations
This study has the following limitations that should be considered when interpreting the results. The first is, the study was conducted at a single institution. The second is, the study was retrospective, which means that the data were collected from records and may not reflect the current situation. The third is, we did not include information on the clinical outcomes of patients infected with these organisms. The fourth is, we did not detect resistance genes using molecular methods. The fifth is, we did not include information on the risk factors associated with antimicrobial resistance due to the retrospective nature of the work.
Conclusion
Between 2017 and 2021, 315 Staphylococcus aureus and 92 Enterococcus species were isolated, and there was a high prevalence of methicillin and vancomycin-resistant Staphylococcus aureus (MRSA and VRSA) strains, with resistance rates of 27% and 5.1%, respectively. Staphylococcus aureus showed a very high resistance to Penicillin G (86.7%). Methicillin-resistant Staphylococcus aureus showed 18.8% resistance to vancomycin. Vancomycin-resistant Enterococcus species isolates were also prevalent, with a resistance rate of 8.7%. There were no statistically significant changes in MRSA, VRSA, and VRE during the study period, which suggests that larger and more representative nationwide data is needed to show trends of these pathogens. Additionally, all Staphylococcus aureus and Enterococcus species isolates were susceptible to linezolid and daptomycin. The high prevalence of these bacteria in commonly used antibiotics necessitates the importance of strengthening the antimicrobial surveillance system, antibiotic stewardship, and infection prevention and control practices at the health facility.
Acknowledgments
We would like to thank the National Clinical Bacteriology and Mycology Reference Laboratory team for allowing us to conduct this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fiore E, van Tyne D, Gilmore MS. Pathogenicity of enterococci. Gram Positive Pathog. 2019;2007(8):378–397. doi:10.1128/9781683670131.ch24
2. Tong SYC, Davis JS, Eichenberger E, Holland TL, Fowler VG. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev. 2015;28(3):603–661. doi:10.1128/CMR.00134-14
3. Zhen X, Lundborg CS, Sun X, Hu X, Dong H. Economic burden of antibiotic resistance in ESKAPE organisms: a systematic review. Antimicrob Resist Infect Control. 2019;8(1). doi:10.1186/s13756-019-0590-7
4. Sakr A, Brégeon F, Mège JL, Rolain JM, Blin O. Staphylococcus aureus nasal colonization: an update on mechanisms, epidemiology, risk factors, and subsequent infections. Front Microbiol. 2018;9(OCT):1–15. doi:10.3389/fmicb.2018.02419
5. Lowy FD. Staphylococcus aureus infections. N Engl J Med. 1998;339(8):520–532. doi:10.1056/NEJM199808203390806
6. Rasigade JP, Vandenesch F. Staphylococcus aureus: a pathogen with still unresolved issues. Infect Genet Evol. 2014;21:510–514. doi:10.1016/j.meegid.2013.08.018
7. Boucher HW, Corey GR. Epidemiology of methicillin-resistant Staphylococcus aureus. Clin Infect Dis. 2008;46(SUPPL. 5):S344–S349. doi:10.1086/533590
8. Seby R, Kim C, Khreis M, Khreis K. Enterococcus faecalis -induced infective endocarditis: an unusual source of infection and a rare clinical presentation. J Int Med Res. 2022;50(7):030006052211120. doi:10.1177/03000605221112019
9. Levitus M, Rewane APT. Vancomycin-Resistant Enterococci. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
10. Clinical and Laboratory Standards Institute. M100 Performance Standards for Antimicrobial Susceptibility Testing. Clinical and Laboratory Standards Institute; 2022.
11. Cong Y, Yang S, Rao X. Vancomycin resistant Staphylococcus aureus infections: a review of case updating and clinical features. J Adv Res. 2020;22:21. doi:10.1016/j.jare.2019.10.005
12. Rubinstein E, Keynan Y. Vancomycin revisited - 60 years later. Front Public Heal. 2014;2(OCT):1–7. doi:10.3389/fpubh.2014.00217
13. Hasanpour AH, Sepidarkish M, Mollalo A, et al. The global prevalence of methicillin-resistant Staphylococcus aureus colonization in residents of elderly care centers: a systematic review and meta-analysis. Antimicrob Resist Infect Control. 2023;12(1):1–11. doi:10.1186/s13756-023-01210-6
14. Wu Q, Sabokroo N, Wang Y, Hashemian M, Karamollahi S, Kouhsari E. Systematic review and meta-analysis of the epidemiology of vancomycin-resistance Staphylococcus aureus isolates. Antimicrob Resist Infect Control. 2021;10(1):1–13. doi:10.1186/s13756-021-00967-y
15. Eshetie S, Tarekegn F, Moges F, Amsalu A, Birhan W, Huruy K. Methicillin resistant Staphylococcus aureus in Ethiopia: a meta-analysis. BMC Infect Dis. 2016;16(1). doi:10.1186/s12879-016-2014-0
16. Deyno S, Fekadu S, Astatkie A. Resistance of Staphylococcus aureus to antimicrobial agents in Ethiopia: a meta-analysis. Antimicrob Resist Infect Control. 2017;6(1). doi:10.1186/s13756-017-0243-7
17. Centers for Disease Control and Prevention. VRE pathogen page; 2019:2. Available from: https://www.cdc.gov/drugresistance/pdf/threats-report/vre-508.pdf.
18. Murray CJ, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0
19. Wayne P; Clinical and Laboratory Standards Institute. Quality Control for Commercially Prepared Microbiological Culture Media; Approved Standard CLSI Document M22-A3. Clinical and Laboratory Standards Institute; 2004.
20. Garoy EY, Gebreab YB, Achila OO, et al. Methicillin-resistant Staphylococcus aureus (MRSA): prevalence and antimicrobial sensitivity pattern among patients—a multicenter study in Asmara, Eritrea. Can J Infect Dis Med Microbiol. 2019;2019:1–9. doi:10.1155/2019/8321834
21. Godebo G, Kibru G, Tassew H. Multidrug-resistant bacterial isolates in infected wounds at Jimma University Specialized Hospital, Ethiopia. Ann Clin Microbiol Antimicrob. 2013;12(1). doi:10.1186/1476-0711-12-17
22. Dilnessa T, Bitew A. Prevalence and antimicrobial susceptibility pattern of methicillin resistant Staphylococcus aureus isolated from clinical samples at Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia. BMC Infect Dis. 2016;16(1). doi:10.1186/s12879-016-1742-5
23. Kejela T, Dekosa F. High prevalence of MRSA and VRSA among inpatients of Mettu Karl Referral Hospital, Southwest Ethiopia. Trop Med Int Heal. 2022;27(8). doi:10.1111/tmi.13789
24. Yilema A, Moges F, Tadele S, et al. Isolation of enterococci, their antimicrobial susceptibility patterns and associated factors among patients attending at the University of Gondar Teaching Hospital. BMC Infect Dis. 2017;17(1). doi:10.1186/s12879-017-2363-3
25. Ashagrie D, Genet C, Abera B. Vancomycin-resistant enterococci and coagulase-negative staphylococci prevalence among patients attending at Felege Hiwot Comprehensive Specialized Hospital, Bahir Dar, Ethiopia. PLoS One. 2021;16(4 April). doi:10.1371/journal.pone.0249823
26. Tsige Y, Tadesse S, G/Eyesus T, et al. Prevalence of methicillin-resistant Staphylococcus aureus and associated risk factors among patients with wound infection at referral hospital, Northeast Ethiopia. J Pathog. 2020;2020:1–7. doi:10.1155/2020/3168325
27. Gebremedhn G, Gebremariam TT, Wasihun AG, Dejene TA, Saravanan M. Prevalence and risk factors of methicillin-resistant Staphylococcus aureus colonization among HIV patients in Mekelle, Northern Ethiopia. Springerplus. 2016;5(1). doi:10.1186/s40064-016-2613-7
28. Tefera S, Awoke T, Mekonnen D. Methicillin and vancomycin resistant Staphylococcus aureus and associated factors from surgical ward inpatients at debre markos referral hospital, northwest Ethiopia. Infect Drug Resist. 2021;14. doi:10.2147/IDR.S324042
29. Tamire T, Eticha T, Gelgelu TB. Methicillin-resistant Staphylococcus aureus: the magnitude and risk factors among patients admitted to tikur anbessa specialized hospital, Addis Ababa, Ethiopia. Int J Microbiol. 2021;2021:1–7. doi:10.1155/2021/9933926
30. Kahsay A, Mihret A, Abebe T, Andualem T. Isolation and antimicrobial susceptibility pattern of Staphylococcus aureus in patients with surgical site infection at Debre Markos Referral Hospital, Amhara Region, Ethiopia. Arch Public Heal. 2014;72(1). doi:10.1186/2049-3258-72-16
31. Mama M, Aklilu A, Misgna K, Tadesse M, Alemayehu E. Methicillin- and inducible clindamycin-resistant Staphylococcus aureus among patients with wound infection attending Arba Minch Hospital, South Ethiopia. Int J Microbiol. 2019;2019:1–9. doi:10.1155/2019/2965490
32. Ayobami O, Brinkwirth S, Eckmanns T, Markwart R. Antibiotic resistance in hospital-acquired ESKAPE-E infections in low- and lower-middle-income countries: a systematic review and meta-analysis. Emerg Microbes Infect. 2022;11(1). doi:10.1080/22221751.2022.2030196
33. Ghahremani M, Jazani NH, Sharifi Y. Emergence of vancomycin-intermediate and -resistant Staphylococcus aureus among methicillin-resistant S. aureus isolated from clinical specimens in the northwest of Iran. J Glob Antimicrob Resist. 2018;14. doi:10.1016/j.jgar.2018.01.017
34. Shariati A, Dadashi M, Moghadam MT, van Belkum A, Yaslianifard S, Darban-Sarokhalil D. Global prevalence and distribution of vancomycin resistant, vancomycin intermediate and heterogeneously vancomycin intermediate Staphylococcus aureus clinical isolates: a systematic review and meta-analysis. Sci Rep. 2020;10(1). doi:10.1038/s41598-020-69058-z
35. Shrestha S, Kharel S, Homagain S, Aryal R, Mishra SK. Prevalence of vancomycin-resistant enterococci in Asia—A systematic review and meta-analysis. J Clin Pharm Ther. 2021;46(5):1226–1237. doi:10.1111/jcpt.13383
36. Ferede ZT, Tullu KD, Derese SG, Yeshanew AG. Prevalence and antimicrobial susceptibility pattern of Enterococcus species isolated from different clinical samples at black lion specialized teaching hospital, Addis Ababa, Ethiopia. BMC Res Notes. 2018;11(1). doi:10.1186/s13104-018-3898-0
37. Pfaller MA, Cormican M, Flamm RK, Mendes RE, Jones RN. Temporal and geographic variation in antimicrobial susceptibility and resistance patterns of enterococci: results From the SENTRY antimicrobial surveillance program. Open Forum Infect Dis. 2019;6(Suppl 1):S54–S62. doi:10.1093/ofid/ofy344
38. Orababa OQ, Soriwei JD, Akinsuyi SO, Essiet UU, Solesi OM. A systematic review and meta-analysis on the prevalence of vancomycin-resistant enterococci (VRE) among Nigerians. Porto Biomed J. 2021;6(1):e125. doi:10.1097/j.pbj.0000000000000125
39. Moghimbeigi A, Moghimbeygi M, Dousti M, et al. Prevalence of vancomycin resistance among isolates of enterococci in Iran: a systematic review and meta-analysis. Adolesc Health Med Ther. 2018;9:177–188. doi:10.2147/ahmt.s180489
40. Azzam A, Elkafas H, Khaled H, Ashraf A, Yousef M, Elkashef AA. Prevalence of Vancomycin ‑ resistant enterococci (VRE) in Egypt (2010 – 2022): a systematic review and meta ‑ analysis. J Egypt Public Health Assoc. 2023;9. doi:10.1186/s42506-023-00133-9
41. Melese A, Genet C, Andualem T. Prevalence of Vancomycin resistant enterococci (VRE) in Ethiopia: a systematic review and meta-analysis. BMC Infect Dis. 2020;20(1). doi:10.1186/s12879-020-4833-2
42. Katip W, Okonogi S, Oberdorfer P. The thirty-day mortality rate and nephrotoxicity associated with trough serum vancomycin concentrations during treatment of enterococcal infections: a propensity score matching analysis. Front Pharmacol. 2022;12(January):1–12. doi:10.3389/fphar.2021.773994
43. Katip W, Oberdorfer P. A monocentric retrospective study of auc/mic ratio of vancomycin associated with clinical outcomes and nephrotoxicity in patients with enterococcal infections. Pharmaceutics. 2021;13(9):1–12. doi:10.3390/pharmaceutics13091378
44. Issaranggoon Na Ayuthaya S, Katip W, Oberdorfer P, Lucksiri A. Correlation of the vancomycin 24-h area under the concentration-time curve (AUC24) and trough serum concentration in children with severe infection: a clinical pharmacokinetic study. Int J Infect Dis. 2020;92:151–159. doi:10.1016/j.ijid.2019.12.036
45. Preeja PP, Kumar SH, Shetty V. Prevalence and characterization of methicillin-resistant Staphylococcus aureus from community- and hospital-associated infections: a tertiary care center study. Antibiotics. 2021;10(2):197. doi:10.3390/antibiotics10020197
46. Article O, Malhotra R, Grover P. Antimicrobial resistance profile of Methicillin ‑ resistant Staphylococcus aureus colonizing the anterior nares of health ‑ care workers and outpatients attending the remotely India. J Lab Physicians. 2017;9:317–321. doi:10.4103/JLP.JLP
47. Mohanty S, Behera B, Sahu S, Praharaj AK. Recent pattern of antibiotic resistance in Staphylococcus aureus clinical isolates in Eastern India and the emergence of reduced susceptibility to vancomycin. J Lab Physicians. 2019;11(4):340–345. doi:10.4103/jlp.jlp_39_19
48. Wangai FK, Masika MM, Maritim MC, Seaton RA. Methicillin-resistant Staphylococcus aureus (MRSA) in East Africa: red alert or red herring? BMC Infect Dis. 2019;19(1). doi:10.1186/s12879-019-4245-3
49. Saravolatz LD, Pawlak J, Johnson LB. In vitro susceptibilities and molecular analysis of vancomycin-intermediate and vancomycin-resistant Staphylococcus aureus isolates. Clin Infect Dis. 2012;55(4):582–586. doi:10.1093/cid/cis492
50. Sievert DM, Rudrik JT, Patel JB, McDonald LC, Wilkins MJ, Hageman JC. Vancomycin-resistant Staphylococcus aureus in the United States, 2002–2006. Clin Infect Dis. 2008;46(5):668–674. doi:10.1086/527392
51. Klein EY, Mojica N, Jiang W, et al. Trends in methicillin-resistant Staphylococcus aureus hospitalizations in the United States, 2010–2014. Clin Infect Dis. 2017;65(11):1921–1923. doi:10.1093/cid/cix640
52. Renggli L, Gasser M, Buetti N, Kronenberg A. Increase in methicillin-susceptible Staphylococcus aureus bloodstream infections in Switzerland: a nationwide surveillance study (2008–2021). Infection. 2023;51(4):1025–1031. doi:10.1007/s15010-023-01980-6
53. Sivaradjy M, Gunalan A, Priyadarshi K, Madigubba H, Rajshekar D, Sastry AS. Increasing trend of vancomycin-resistant enterococci bacteremia in a tertiary care hospital, south India: a three-year prospective study. Indian J Crit Care Med. 2021;25(8):882–886. doi:10.5005/jp-journals-10071-23916
54. Ayobami O, Willrich N, Reuss A, Eckmanns T, Markwart R. The ongoing challenge of vancomycin-resistant Enterococcus faecium and Enterococcus faecalis in Europe: an epidemiological analysis of bloodstream infections. Emerg Microbes Infect. 2020;9:1180–1193. doi:10.1080/22221751.2020.1769500
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
ST7 Becomes One of the Most Common Staphylococcus aureus Clones After the COVID-19 Epidemic in the City of Wuhan, China
Gu J, Shen S, Xiong M, Zhao J, Tian H, Xiao X, Li Y
Infection and Drug Resistance 2023, 16:843-852
Published Date: 13 February 2023
Cross-sectional Hospital-based Investigation on Clinical Characteristics of Pediatric Staphylococcus aureus Isolates in a Beijing Hospital from 2013 to 2022
Wang L, Zhen JH, Dong F, Lyu ZY
Infection and Drug Resistance 2024, 17:4899-4912
Published Date: 6 November 2024